Introduction
According to the International Diabetes Federation,
there are 425 million adults with diabetes worldwide (1). Diabetic neuropathy is the most common
complication of diabetes mellitus, becoming symptomatic after 14.5
years of chronic prolonged high blood glucose in type 1 diabetes,
and after only 8.1 years in type 2 diabetes (2). A population-based study indicated that
up to 50% of patients with either type 1 or type 2 diabetes develop
diabetic neuropathy (3), and 15–30%
of those manifestations are painful (4). Diabetic neuropathic pain (DNP) is among
the most common, expensive and disabling complications of diabetes,
affecting approximately 30% of patients with diabetes who are
hospitalized and 25% of those in the community (5,6).
DNP is characterized by sensations of numbness,
burning pain and prickling or stinging around the hands and feet,
and the pain is more severe at night (7). The more severe occurrences of DNP can
be intractable (8,9). Neuropathic pain can be constant and
accompanied by cutaneous allodynia, which significantly influences
quality of life (QOL) and prevents patients from performing their
daily activities and roles of employment. The pain may also be
associated with depression and may be a reason for withdrawal from
recreational and social life (7,10,11).
Thus, treating this debilitating condition appropriately is
important, particularly because of the impact on QOL and the
associated depression and anxiety (12).
The management of DNP is challenging and can require
a multi-modal approach involving early recognition, glycemic
control and psychological therapy, as well as therapies for
symptomatic pain relief (13–15). At
present, the pharmacological treatments for DNP include oral and
topical therapies (16). Oral
agents, such as amitriptyline, duloxetine, pregabalin and
gabapentin, are recommended as first-line drug treatments (17). However, oral therapy requires
multiple medications taken at varying times of the day and is often
associated with a significantly elevated risk of systemic side
effects, which may be severe (18).
Some patients do not tolerate these drugs and some find them
ineffective, which may cause a significant drop in patient
compliance. With the potential to provide the same level of
analgesic efficacy provided by oral analgesics, but relatively
fewer systemic adverse events and drug-drug interactions (19,20),
topical use of drugs as another treatment option for DNP is
currently gaining interest (16,21). A
variety of agents are used in the topical treatments of DNP,
including lidocaine, capsaicin, amitriptyline, clonidine, nutmeg
extracts, Citrullus colocynthis extract oil and even a
combination of various compounds, and so far offer promising
results (22–28). Given the trend towards using topical
medications to treat DNP, the present review provides an overview
of the current knowledge regarding the physiopathology of DNP and
the existing topical pharmacological treatments. A recent review,
focusing on topical treatment for localized neuropathic pain,
including post-herpetic neuralgia (PHN), complex regional pain
syndrome, diabetic peripheral neuropathy and human immunodeficiency
virus distal sensory polyneuropathy, has been published (29). In the current review, an overview is
provided of the current understanding of the pathogenesis of DNP
and the mechanism of drug action. Furthermore, the clinical data on
available agents for topical use in patients with DNP is
summarized, their potential efficacy addressed, and the potential
for use of compounded topical agents in the future is
highlighted.
Pathogenesis of DNP
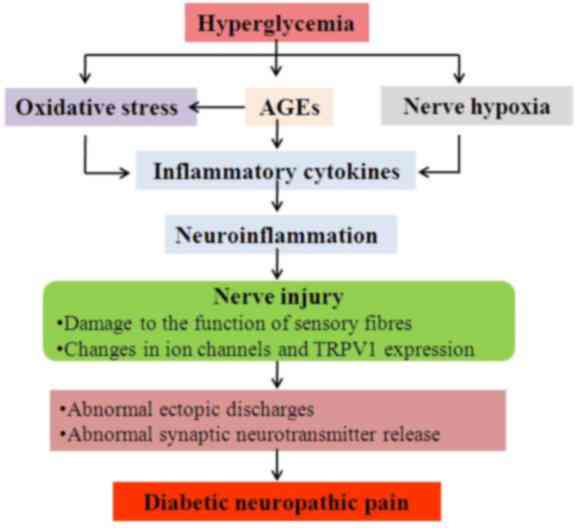
The exact pathogenic mechanisms involved in the
generation of DNP are not fully established (8). A variety of potential factors have been
postulated to elicit the pain associated with diabetic neuropathy,
including hyperglycemia, advanced glycation end-products (AGEs)/AGE
receptor (RAGE) activity, oxidative stress, neuroinflammation and
endoneural hypoxia (30,31). A schematic summarizing the potential
mechanisms underlying the pathogenesis of DNP is presented in
Fig. 1.
There is a consensus that hyperglycemia serves a
crucial role in the development of DNP (2,32–36).
Studies in non-diabetic individuals and in animals have
demonstrated that hyperglycemia can cause a decrease in pain
thresholds (34,35). Hyperglycemia is correlated with the
progression of neuropathy pain; approximately 50% of patients who
have had diabetes for more than 25 years will develop neuropathy
and the majority of symptomatic patients will complain of pain
(2,36).
Other factors besides hyperglycemia may result in
the generation of DNP (37). An
increase in AGE production and a decrease in the regeneration of
glutathione may be caused by hyperglycemia (38,39).
Depletion of glutathione could be the primary cause of oxidative
stress and related to the accumulation of toxic species (40). In addition, when the disposal of
intracellular glucose is impaired, alternate pathways are
activated, which may also lead to oxidative stress and nerve injury
(41–43). Hyperglycemia serves a key role in
oxidative stress in diabetic nerves (41). Nerve hypoxia may be evoked by
hyperglycemia, particularly in sensory nerves, altering their
function and electrical stability (44). AGEs, oxidative stress and hypoxia
thereby cause the production of inflammatory cytokines and growth
factors, which in turn cause neuroinflammation and nerve injury
(45–47). Neuropathic pain has been associated
with neurological damage to the function of sensory fibers,
including fast-conducting myelinated Aδ fibers and slow-conducting
unmyelinated C fibers, which conduct nerve impulses, and changes in
voltage-gated ion channel distribution and expression (48,49). In
addition, the upregulation of transient receptor potential
vanilloid 1 (TRPV1) expression has been identified to be associated
with neuropathic pain (50).
Hyperglycemia, AGEs, hypoxia and oxidative stress-mediated damage
in neurons and glial cells, as well as the subsequent activation of
proinflammatory cascades and crosstalk between these disease
processes, may ultimately result in abnormal ectopic discharges and
abnormal synaptic neurotransmitter release, including of serotonin
and norepinephrine (8), and thereby
trigger development of neuropathic pain (51).
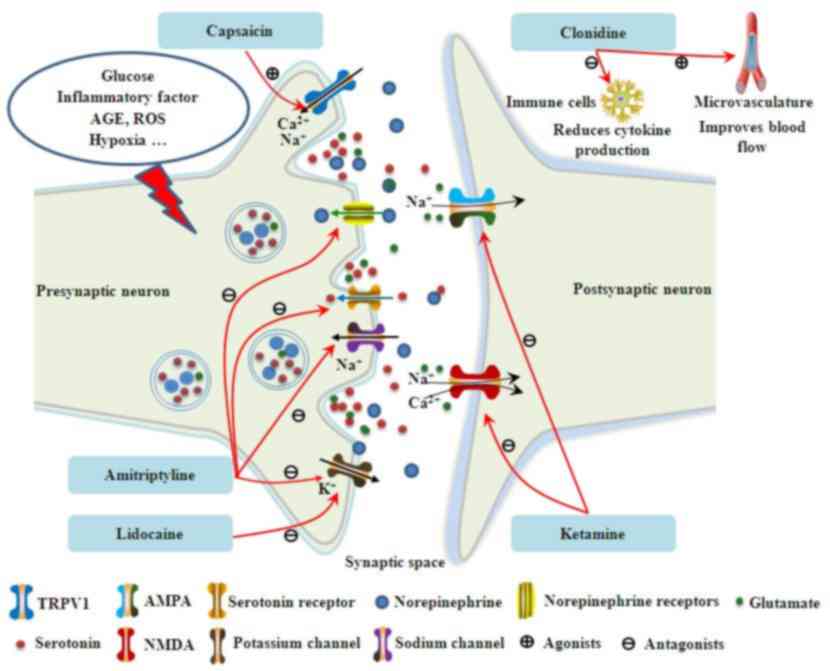
Topical pharmacological treatment of
DNP
The analgesic effect and safety of various topical
agents including lidocaine plasters and patches, capsaicin cream,
capsaicin gel, capsaicin patches, amitriptyline cream, clonidine
gel, ketamine cream, extracts from medicinal plants including
nutmeg extracts and Citrullus colocynthis extract oil, and
some compounded topical analgesics, have been assessed in patients
affected by DNP. Topical agents evaluated in clinical trials are
discussed in detail herein and their targets of action are
presented in Fig. 2.
Topical lidocaine
Lidocaine, a blocker of voltage-gated sodium
channels (particularly Nav 1.7 and 1.8), can stabilize the neuronal
membrane potential on abnormally excitable Aδ and C fibers,
resulting in a reduction of ectopic discharges (52,53).
This raises the peripheral ectopic discharge threshold and reduces
the pain transduction. Topical lidocaine has been demonstrated to
be effective in the treatment of neuropathic pain conditions,
including DNP (54–57). A network meta-analysis compared 5%
lidocaine-medicated plaster for the relief of DPN with other
relevant drugs, including amitriptyline (30, 75 and 125 mg/day),
pregabalin (300 and 600 mg/day), capsaicin (0.075% cream, four
times a day), gabapentin (≤900 and 1,200 mg/day) and placebo. It
was indicated that all interventions were effective in comparisons
with a placebo. Notably, lidocaine medicated plasters were
comparable to all of the other interventions (58).
Here, five reports that assessed the effectiveness
of topical lidocaine for DNP have been reviewed (Table I). A 4-week, randomized, open-label,
multicenter, non-inferiority study, which compared lidocaine
plaster with pregabalin in patients with DNP, was reported as an
interim analysis (59) and published
in full (52,60). The interim analysis revealed that
patients administered with 5% lidocaine plasters experienced
similar analgesic efficacy, fewer drug-related adverse events
(DRAEs; 3.9 vs. 39.2%) and substantially fewer discontinuations due
to DRAEs (1.3 vs. 20.3%) than pregabalin (59). In the full analysis the investigators
also reported results for EuroQol-5D (EQ-5D) QOL evaluation. In
line with the aforementioned results, 5% lidocaine-medicated
plaster exerted comparable efficacy, greater improvements in the
QOL based on EQ-5D, and fewer adverse events, DRAEs and related
discontinuations compared with pregabalin (52). To our knowledge this was the only
study that has assessed the lidocaine plaster as a monotherapy for
DNP. An 8-week combination phase of this study also demonstrated
additional decreases in recalled average pain intensity scores over
the previous 3 days (numeric rating scale-3 scores) (60). Another open-label study on patients
with DPN who experienced pain following a stable analgesic drug
regimen and dosages for at least a week, and presented with an
average daily pain diary rating of ≥4 on the brief pain inventory,
exhibited significant improvements in pain and QOL outcome measures
during a 3-week 5% lidocaine patch treatment period. These benefits
were maintained during an additional 5-week period with a tapering
of concomitant analgesics (56). A
further two studies also included patients with PHN or lower back
pain (55,61). The 5% lidocaine patch could
effectively reduce the intensity of pain in patients with various
pain-related conditions, including DNP. A reduction in pain
intensity was also observed with topical 5% lidocaine in a
double-blind, randomized, placebo-controlled crossover study
including patients with DNP (62).
These results of clinical trials indicated that administration with
a topical lidocaine 5% patch or plaster could relieve pain
symptoms, including in DNP.
 | Table I.Summary of clinical studies on
topical lidocaine for the treatment of DNP. |
Table I.
Summary of clinical studies on
topical lidocaine for the treatment of DNP.
| Author, year | Topical
agent(s) | Study design | No. of patients (%
male) | Age, years (mean ±
standard deviation) | Duration of
pain | Outcomes | (Refs.) |
|---|
| Comparisons with
oral pregabalin |
| Baron et al,
2009 | 5% Lidocaine
plaster | Two-stage,
adaptive, randomized, controlled, open-label, 4-week, multicenter
trial that incorporated a drug wash-out phase of up to 2 weeks
prior to the start of the comparative phase | Lidocaine: 47
(48.9) Pregabalin: 44 (54.5) | Lidocaine: 60.2±9.9
Pregabalin: 59.8±8.4 | ≥3 months | Showed similar
analgesic efficacy, fewer DRAEs (3.9% vs. 39.2%) and fewer
substantial discontinuations due to DRAEs (1.3 vs. 20.3%) than
pregabalin. | (59) |
| Baron et al,
2009 | 5% Lidocaine
plaster | Two-stage adaptive,
randomized, open-label, 4-week, multicenter, non-inferiority
study | Lidocaine: 105
(42.9) Pregabalin: 105 (46.7) | Lidocaine:
60.9±10.0 Pregabalin: 60.9±8.8 | ≥3 months | Showed comparable
efficacy, greater improvements in QOL, and fewer AEs, DRAEs and
related discontinuations compared with pregabalin. An 8-week
combination phase of this study demonstrated additional decreases
in NRS-3 scores. | (52,60) |
| Noncomparative
studies |
| Barbano et
al, 2004 | 5% Lidocaine
patch | Open-label,
flexible-dosing, 3-week study with a 5-week extension | 56 (NA) | NA | ≥3 months | Significantly
reduced pain and improved QOL. These benefits were maintained
during an additional 5 weeks with tapering of concomitant
analgesics. | (56) |
| Argoff et
al, 2004 | 5% Lidocaine
patch | Open-label,
non-randomized, prospective, 2-week study | 41 (41.5) | 56.7±12.6 | NA | Effectively reduced
the intensity of pain in patients with DNP. Well tolerated in
combination with other analgesic regimens. No serious AEs or
adverse drug interactions. | (55) |
| White et al,
2003 | 5% Lidocaine
patch | Open-label,
non-randomized, 2-week multicenter pilot trial. | 49 (46.9) | 57.7±12.6 | NA | Improved pain
intensity and pain relief scores. | (61) |
Topical capsaicin
Capsaicin, the active agent of the dried fruits or
ground powder (paprika) of chili peppers, is a naturally occurring
alkaloid (63). Capsaicin has been
used with some success in the treatment of patients with DNP
(6,64). These effects are thought to be caused
by selective binding to TRPV1 expressed on Aδ and C fibers
(65). Once capsaicin binds to the
receptor and the TRPV1 channel is opened, sodium and calcium influx
and substance P release occurs (66). Repeated TRPV1 exposure to capsaicin
causes substance P depletion and TRPV1 desensitization and
defunctionalization (7). Two forms
of capsaicin are available for DNP, a low-dose cream and a
high-dose patch, both of which should be used under specialist
supervision (67). Capsaicin creams
with concentrations of 0.025–0.250% must be applied multiple times
per day for several weeks before analgesic effects become obvious
(68). A single application of the
Qutenza patch (capsaicin patch with an 8% concentration) following
an appropriate local analgesia may provide up to 3 months of pain
relief (23). Seven double-blind
controlled studies and one open-label study of topical capsaicin in
the treatment of DNP are summarized in Table II. No study specifically examined
topical capsaicin as a monotherapy for DNP.
| Table II.Summary of clinical studies on
topical capsaicin for the treatment of DNP. |
Table II.
Summary of clinical studies on
topical capsaicin for the treatment of DNP.
| Author, year | Topical
agent(s) | Study design | No. of patients (%
male) | Age, years (mean ±
standard deviation) | Duration of
pain | Outcomes | (Refs.) |
|---|
| Comparisons with
placebo or vehicle |
| Chad et al
1990 | 0.075% Capsaicin
cream | Double-blind,
4-week, multicenter, vehicle-controlled, randomized study | Capsaicin: 24 (NA)
Vehicle: 22 (NA) | NA | NA | No obvious effects
on pain relief | (74) |
| The Capsaicin Study
Group, 1991–1992 | 0.075% Capsaicin
cream | Double-blind,
8-week, multicenter, vehicle-controlled parallel randomized
study | Capsaicin: 138
(51.4) Vehicle: 139 (48.9) | Capsaicin: 60.1
(27–92)a Vehicle: 60.3
(22–81)a | NA | Well tolerated
Effective for reducing pain Improved daily activities Enhanced
QOL | (69,70) |
| Tandan et
al, 1992 | 0.075% Capsaicin
cream | Double-blind,
8-week, vehicle-controlled study with either 0.075% capsaicin cream
or vehicle cream over the painful areas | Capsaicin: 11
(54.5) Vehicle: 11 (45.5) | Capsaicin: 55.1±7.6
Vehicle: 53.3±11.8 | NA | Decreased mean pain
intensity Relieved mean pain scores No adverse effects on sensory
thresholds Approximately 50% of subjects reported improved pain
control or were cured in a follow-up open-label study | (72,73) |
| Kulkantrakorn et
al, 2013 | 0.025% Capsaicin
gel | Double-blind,
20-week, crossover, randomized, single-center study enrolling
subjects with DNP | 33 (48.5) | 58.0
(35–76)a | ≥1 month | Safe and well
tolerated Did not provide significant pain relief | (75) |
| Simpson et
al, 2017 | 8% Capsaicin
patch | Phase 3,
randomized, double-blind, 12-week, placebo-controlled, multicenter
trial | Capsaicin: 186
(61.3) Placebo: 183 (55.2) | Capsaicin:
63.9±10.6 Placebo: 62.0±10.8 | ≥1 year | Provided modest and
statistically significant improvements in pain relief Improved
sleep quality Well tolerated Did not cause any sensory
deterioration or new safety concerns | (76) |
| Comparisons with
oral amitriptyline |
| Biesbroeck et
al, 1995 | 0.075% Capsaicin
cream | Double-blind,
8-week, multicenter, parallel study compared the safety and
efficacy of topical capsaicin and oral amitriptyline in patients
with painful diabetic neuropathy | NA | NA | NA | Equally effective
Considerably safer | (71) |
| Comparisons with
SOC alone |
| Vinik et al,
2016 | 8% Capsaicin
patch | Phase 3,
multinational, open-label, randomized, controlled, 52-week safety
study | Capsaicin 8% patch
(30 min) + SOC: 156 (47.4) Capsaicin 8% patch (60 min) + SOC: 157
(50.3) SOC: 155 (45.8) | Capsaicin 8% patch
(30 min) +SOC: 60.9±10.9 Capsaicin 8% patch (60 min) +SOC:
61.0±10.3 SOC: 59.1±10.3 | ≥1 year | In patients with
PDPN, capsaicin 8% patch repeat treatment plus SOC over 52 weeks
was well tolerated with no negative functional or neurological
effects compared with SOC alone | (77) |
The action of low concentration capsaicin (0.025 or
0.075%) in the treatment of DNP was reported in a series of the
studies reviewed. The Capsaicin Study Group attempted to define the
efficacy and safety of topical 0.075% capsaicin in patients with
painful diabetic neuropathy. Improvement in pain relief, pain
intensity and daily activities, including sleeping, walking and the
ability to work and participate in recreational activities, were
observed in significantly more patients treated with capsaicin than
with a vehicle (69,70). Compared with oral amitriptyline,
topical 0.075% capsaicin cream was equally effective but
considerably safer according to the results of a comparative study
in patients with painful diabetic neuropathy (71). A double-blind, 8-week
vehicle-controlled study with either 0.075% capsaicin cream or a
vehicle cream over the painful area further confirmed the value and
safety of capsaicin for pain relief in subjects with DNP (72,73). By
contrast, Chad et al (74)
and Kulkantrakorn et al (75)
observed that low concentration topical capsaicin had little effect
in the treatment of DNP. After 4 weeks of 0.075% capsaicin cream
treatment, there was no notable difference between capsaicin and
the vehicle in terms of their beneficial effects on DNP (74). Meanwhile, 0.025% capsaicin gel was
determined safe and well tolerated, but it did not provide
significant pain relief in patients with DNP compared with a
placebo (75). Due to the
inconsistences between the aforementioned studies and their small
sample sizes, it is difficult to conclude on the efficacy of
low-concentration topical capsaicin in the treatment of DNP.
An 8% capsaicin patch, which is optimized for rapid
delivery of a high concentration of capsaicin directly to the skin,
contains 179 mg or 8% w/w capsaicin. One double-blind study that
assessed the efficacy of an 8% capsaicin patch compared with a
placebo and one open-label study that provided long-term safety and
tolerability data on patients with painful diabetic peripheral
neuropathy (PDPN) were available. In the double-blind trial that
assessed efficacy, 369 patients were randomized to an 8% capsaicin
patch (Qutenza) or a placebo patch regimen. The capsaicin patch
provided modest but statistically significant improvements in pain
relief and improved sleep quality compared with the placebo patch,
was well tolerated, and was not associated with any sensory
deterioration or new safety concerns (76). In the 52-week open safety study, 468
DNP patients were randomized to a capsaicin 8% patch repeat
treatment for 30 or 60 min plus standard of care (SOC), or SOC
alone. No worsening in sensory perception tested with sharp, cold,
warm or vibration stimuli was observed with topical capsaicin.
Compared with SOC therapy alone, SOC plus capsaicin 8% patch repeat
treatment over 52 weeks was well tolerated, had no neurological or
negative functional effects and raised no new safety concerns
(77). An article from the Drug and
Therapeutics Bulletin proposed that there is a limited role for
topical capsaicin in the treatment of DNP due to the uncertain
efficacy of low-concentration topical capsaicin and the
considerably more expensive cost of the 8% capsaicin patch compared
with oral therapies (67). However,
topical 0.075% capsaicin was recommended as a likely effective
treatment option for DNP in the American Academy of Neurology
evidence-based guidelines (78). A
network meta-analysis performed in patients with PDPN suggested
that the 8% capsaicin patch was only as effective as oral centrally
acting agents but offered superior systemic tolerability benefits
(18). Either low concentration or
high concentration capsaicin may provide a degree of pain relief to
some patients with neuropathic conditions that cause different
degrees of pain. Further developments in methods of application and
formulation may lead to improved clinical efficacy.
Topical amitriptyline
Amitriptyline is a tricyclic anti-depressant that
acts centrally by blocking Na+, K+, and
Ca2+ voltage-gated ion channels (79–81),
inhibiting neuronal reuptake of norepinephrine and serotonin. It is
effective in treating various types of neuropathic pain (82). A topical form of this drug has been
investigated in certain previous studies for the treatment of DNP
(24,62,83)
(Table III), however its adverse
effects in oral administration have limited the higher doses needed
to achieve adequate analgesia.
| Table III.Summary of clinical studies on other
topical agents for the treatment of DNP. |
Table III.
Summary of clinical studies on other
topical agents for the treatment of DNP.
| Author, year | Topical
agent(s) | Study design | No. of patients (%
male) | Age, years (mean ±
standard deviation) | Duration of
pain | Outcomes | (Refs.) |
|---|
| Comparisons with
topical 5% lidocaine and placebo |
| Ho et al,
2008 | 5% Amitriptyline
cream | Double-blind,
randomized, placebo-controlled crossover study | 35 (45.7) | 57.4±13.8 | ≥6 months | No significant
change in pain intensity was observed with topical amitriptyline or
placebo Topical lidocaine and placebo each reduced pain more than
topical amitriptyline | (62) |
| Comparisons with
topical 0.75% capsaicin cream |
| Kiani et al,
2015 | 2% Amitriptyline
cream | Double-blind,
12-week, randomized, and non-inferiority trial | Amitriptyline: 51
(33.3) Capsaicin: 51 (31.4) | Amitriptyline:
57.5±10.8 Capsaicin: 55.4±10.6 | ≥3 months | Both drugs
significantly relieved pain in 12 weeks compared with baseline
values. Well tolerated | (24) |
| Comparisons with
placebo |
| Campbell et
al, 2009 and Wrzosek et al, 2015 | 0.1 and 0.2%
Clonidine gels | Double-blind,
8-week, randomized placebo-controlled trial | 0.1% clonidine: 54
(NA) 0.2% clonidine: 54 (NA) Placebo: 57 (NA) | NA | NA | The reduction in
mean aggregate pain score from week 8 to baseline in subjects who
received 0.1% gel was significantly greater compared with the
placebo group. The reduction in pain for the 0.2% group was less
impressive Adverse events were similar between the three
groups. | (25,87) |
| Campbell et
al, 2012 | 0.1% Clonidine
gel | Double-blind,
12-week, randomized, placebo-controlled, parallel-group,
multi-center trial | Clonidine: 89 (49)
Placebo: 90 (47) | Clonidine: 59.4±9.9
Placebo: 57.6±9.5 | ≥6 months | Significantly
reduced the level of pain Safe and without the problematic side
effects typically associated with systemic therapies | (88) |
| Motilal and
Maharaj, 2013 | Nutmeg extract | Double-blind,
4-week, randomized, placebo-controlled trial. | Nutmeg extract: 37
(32.4) Placebo: 37 (32.4) | Nutmeg extracts:
60.7±11.5 Placebo: 59.7±8.1 | NA | Reduced worst and
mean pain scores Improved QOL No statistically significant
differences between the groups for all outcome measures | (26) |
| Heydari et
al, 2016 | Topical
Citrullus colocynthis extract oil | Two-arm,
double-blind, randomized, placebo-controlled, parallel study | Citrullus
colocynthis extract oil: 30 (39.3) Placebo: 30 (55.6) | Citrullus
colocynthis extract oil: 57.4±10.0 Placebo: 52.7±10.5 | ≥3 months | Decreased mean pain
score Improved nerve function Improved physical domain of QOL | (27) |
| Mahoney et
al, 2012 | Topical ketamine
cream | Double-blind,
randomized, placebo-controlled, study | Ketamine: 10 (40.0)
Placebo: 7 (57.1) | Ketamine: 64.0±9.5
Placebo: 65.4±15.0 | NA | No more effective
than placebo | (100) |
| ClinicalTrials.
govNCT00476151, 2006 | Topical 4%
amitriptyline and 2% ketamine | Phase 2,
multicenter, randomized, placebo-controlled, parallel group
study | Ami/Ket: 114 (57.0)
Placebo: 112 (50.9) | Ami/Ket: 56.1±9.4
Placebo: 55.1±11.0 | ≥6 months | Showed a strong
trend toward pain reduction in painful diabetic neuropathy | (28) |
In a double-blind, randomized, placebo-controlled
crossover study, 35 patients with postsurgical neuropathic pain,
PHN or DNP were included to examine the analgesic effect of topical
5% amitriptyline. This study failed to show efficacy of topical
amitriptyline in alleviating neuropathic pain, though the results
were based on a small sample size of DNP patients (62). Inconsistent with these results, a
double-blind, 12-week, randomized and non-inferiority trial
revealed that topical 2% amitriptyline was effective in managing
DNP. The results were similar to 0.75% capsaicin cream, with fewer
adverse effects and improved patient compliance. However, the study
only measured the median pain score using the visual analogue scale
(24). In addition, two cases
treated with high doses of topical amitriptyline in neuropathic
pain have been described to record the effect of topical
amitriptyline (83). One of the
cases reported a 39-year-old patient suffering from severe
neuropathic pain in the feet and hands, due to type II diabetes
mellitus (83). Following the use of
5% amitriptyline, the pain in the hands was markedly relieved, and
following application of amitriptyline 10% to the feet, a total
reduction of pain occurred within 20 min and lasted the whole day.
These effects reportedly lasted for 7 months and the patient did
not experience any amitriptyline-related side effects (83). Amitriptyline could also improve the
quality of sleep for the patients by reducing severe pins and
needles in the feet at night (83).
Therefore, high dose topical amitriptyline at 5 and 10% may be a
useful adjunct to treat severe and intractable DNP. However at
present, the therapeutic effect of amtriptyline on DNP is still
unclear. Given the conflicting results of the reports, more studies
are required to confirm the efficacy and safety of this topical
compound as a treatment for DNP.
Topical clonidine
Clonidine is used to treat hypertension and other
conditions, including intraocular pressure rise (84) and attention deficit syndrome
(85), but it also has actions on
sensory neurons by reducing excitability, acts on the
microvasculature by improving blood flow, and acts on immune cells
by reducing cytokine production (86). It is a presynaptic α2-adrenergic
receptor agonist; thus adverse events associated with systemic use
of this drug have limited its application. As such, topical
clonidine formulations have been investigated in clinical studies.
Two randomized placebo-controlled studies for the treatment of DNP
have been conducted in the USA by Wrzosek et al (25) and Campbell et al (87) (Table
III). Both studies evaluated the efficacy and safety of topical
clonidine gel in DPDN patients. In the first of the studies, 54
patients received 0.1% clonidine gel (650 µl) and another 54
patients were treated with 0.2% clonidine gel (500 µl). The control
group (57 patients) was given a placebo gel. Participants remained
on their existing pain management treatments and these gels were
applied to both feet twice daily for 2 weeks, then 3 times daily to
a total of 8 weeks (25). Over the
8-week study interval, the reduction in mean aggregate pain score
when compared with baseline in subjects who received 0.1% gel was
significantly greater compared with the placebo group, while the
reduction in pain for the 0.2% group was less notable.
Investigators suggested the possible reason leading to such
difference was the amount applied to the skin (500 µl at 0.2% vs.
650 µl at 0.1%). Campbell et al (88) subsequently performed a 12-week study
to examine further the efficacy of topical 0.1% clonidine in
treating DNP. In the clonidine group, the decrease in average pain
from baseline to week 12 was greater than in the placebo group. For
safety, only a low concentration of clonidine (<10 pg/ml) was
aimed for in the plasma during topical application (88), and it was considerably lower than the
threshold for treating hypertension, suggesting that topical use
will be associated with few of the adverse effects of clonidine.
The results of these two clinical trials indicated that the topical
use of clonidine may relieve DNP, but it is not known from these
studies if clonidine is safe for long-term use. The use of active
treatment rather than placebo may reveal more information about the
comparative efficacy of topical clonidine vs. other drugs.
Topical nutmeg extracts
Nutmeg is the dried kernel of the broadly ovoid seed
of Myristica fragrans. Certain animal studies support nutmeg
as a potential analgesic for DNP (89,90). A
double-blind, 4-week, randomized, placebo-controlled trial further
tested the ability of topical nutmeg extracts to reduce pain or
improve QOL in patients with DNP (26) (Table
III). A total of 74 participants who met the criteria for
painful diabetic neuropathy were recruited. Subjects were
instructed to apply four sprays of either topical nutmeg extract or
placebo to the affected area 3 times a day followed by gentle
massage for 4 weeks. The topical nutmeg extract preparation
significantly reduced the worst and mean pain scores, and improved
QOL by the end of the 4-week study, but the effects were not
superior to the placebo. Due to the limited clinical research data,
it is not possible to conclude on the efficacy of topical nutmeg
extracts for the treatment of painful diabetic neuropathy.
Topical Citrullus colocynthis (bitter
apple) extract oil
Bitter apple, or Citrullus colocynthis, is a
medicinal plant originating from Africa and Asia, where it has
traditionally been used for various medicinal purposes, including
pain relief (91). Citrullus
colocynthis has been demonstrated to have anesthetic (92), anti-oxidant (93) and anti-ulcerogenic effects (94). These properties are considered
important in the pathophysiology and/or progression of diabetic
neuropathy. Heydari et al (27) examined its efficacy and safety in DNP
patients (Table III): 60 patients
with DNP were randomized to receive topical Citrullus
colocynthis or placebo twice daily for 3 months. There was a
significantly greater decrease in mean pain score after 3 months in
the Citrullus colocynthis group than with the placebo. It
also significantly improved nerve function and the mean score in
the physical aspect of QOL (95).
Therefore, topical Citrullus colocynthis may be a potential
agent for use in the treatment of DNP and should be investigated
further in studies with larger sample sizes performed over longer
duration.
Topical ketamine
Ketamine is a non-barbiturate anesthetic agent that
acts through blocking glutamate receptors, including peripheral
N-methyl-D-aspartate receptors and
α-amino-3-hydroxy-5-methylisoxazole-4-proprionic acid (86,96–98), and
also as an inhibitor of voltage-gated Na+ and
K+ ion channels (99). A
recent study evaluated the effects of topical ketamine in relieving
DNP (Table III): 17 patients with
DNP were randomly divided into a 5% ketamine cream group or a
placebo group. The 5% topical ketamine cream was no more effective
than the placebo in relieving pain caused by diabetic neuropathy
(100). A limitation of this study
was the sample size; therefore the clinical efficacy of ketamine
needs to be further evaluated.
Compounded topical agents
Mixtures of two or more medicated forms of
compounded topical agent have been developed into potentially
valuable treatment options for DNP. The authors of the current
study concluded that these may be effective due to the multiple
complementary effects at lower doses of each individual medication.
It is apparent that only one study with compounded topical agents
has been performed in patients with DNP only (28) (Table
III); 4 other related studies also selected patients with other
types of neuropathic pain (96,101–103).
In a pilot study and its follow-up studies of mixed neuropathic
pain, including DNP, patients who were treated with topical
low-dose combinations of amitriptyline (1–2%) and ketamine (0.5–1%)
did not experience significant pain relief effect compared with
those receiving placebo for 1–3 weeks (96,101).
However, the treatment was associated with long-term perceived
analgesic effectiveness for 12 months (102). As for higher concentrations of
these combined agents (4% amitriptyline and 2% ketamine), a phase
2, multi-center, double-blind, randomized, placebo-controlled,
parallel group study indicated a trend towards pain reduction in
painful diabetic neuropathy (16,28).
Somberg and Molnar (103) conducted
a retrospective study on the analgesic activity of a topical
(TT-CTAC) cream in patients with diabetic neuropathy and other
chronic pain conditions. Two versions of TT-CTAC cream were
evaluated: cream 6B and cream 7B. Both creams contain ketamine
(10%), baclofen (2%), gabapentin (6%), amitriptyline (4%),
bupivacaine (2%) and clonidine (0.2%). Additionally, one cream (7B)
contained nifedipine (2%). Both creams provided considerable pain
relief in the majority of the patients studied and were thus
suggested to be useful modalities for pain therapy. Due to a lack
of comparative studies between compounded topical agents and single
drugs for DNP, it is not possible to conclude on the drug cost,
efficacy and side effects of compounded agent compared with
single-agent topical treatment of DNP. However, given the
advantages of formula diversity, drug economy and safety, it may be
that compounded topical agents have promising market prospects and
clinical application value.
Conclusion and perspectives
DNP is a distressing consequence of diabetes that
may be present in as many as one in five diabetic patients
(104). The pain may be severe and
management challenging. Oral treatment is the most frequently used
and among the most convenient for pain medication, but is also
associated with risk of adverse systematic effects (105,106),
particularly in vulnerable patients with multiple comorbidities and
altered pharmacokinetics and pharmacodynamics that may alter drug
metabolism (107). This may
decrease the patient's compliance. With this concern for the
systematic side effects of oral agents, topical preparations for
the treatment of DNP have gained increasing interest. Numerous
clinical studies have evaluated the analgesic effect and safety of
various topical agents, including topical anesthetic agent
lidocaine, general anesthetic agent ketamine, antidepressant agent
amitriptyline, α2 adrenergic agent clonidine, capsaicin, nutmeg
extracts, Citrullus colocynthis extract oil, and some
compounded topical analgesics. Overall topical agents are easy to
administer, offer significant improvement in patient compliance and
reduce the burden of multiple drug regimens.
For the topical treatments of DNP discussed here, a
5% lidocaine patch has been found to significantly reduce pain in
DNP patients with 2–3 weeks of treatment and the benefits were
maintained during an additional 5 weeks with tapering of
concomitant analgesics. Furthermore, the 5% lidocaine plaster was
reported to exhibit similar analgesic efficacy and fewer DRAEs
compared with oral pregabalin. It is difficult to draw conclusions
about the efficacy of low-concentration topical capsaicin in the
treatment of DNP due to the inconsistencies among related research
findings. The 8% capsaicin patch was as effective as oral centrally
acting agents but offered systemic tolerability benefits, provided
modest but statistically significant improvements in pain relief
and was well tolerated. There is conflicting evidence regarding the
effect of topical amitriptyline and it needs to be confirmed by
further studies. Topical clonidine, nutmeg extract preparation,
Citrullus colocynthis extract and some compounded topical
agents may provide significant though less notable or only
long-term improvements in pain relief. For instance, study
demonstrated that 5% topical ketamine cream was no more effective
than a placebo in relieving pain caused by diabetic neuropathy, but
the study only included 17 patients with DNP.
Since published studies suggest that these drugs
have the potential to be a valuable additional option for the
management of DNP, with adequate safety and continuous long-term
treatment efficacy, these topical drugs should be given further
consideration for the treatment of DNP. Furthermore, as described
in several studies, compounded agents are not only effective but
also safe for patients with DNP. Therefore, the use of low-dose,
complementary therapies with compounded agents is another area
worthy of further investigation. Additionally, topical drugs that
act on different targets in the process of DNP, including
anti-inflammatory and abnormal ectopic discharge therapies, or
anti-oxidant and AGE/RAGE therapies, should be studied in the
future.
Acknowledgements
Not applicable.
Funding
The authors would like to thank the Natural Science
Foundation of China (grant no. 81603171), the Natural Science
Foundation of Hunan Province (grant no. 2018JJ3743) and the
Open-End Fund for the Valuable and Precision Instruments of Central
South University (grant no. CSUZC201734) for the financial
support.
Availability of data and materials
Not applicable.
Authors' contributions
PFF, XDY and YYY designed the present study. XDY,
PFF, DXX and YYY collected the literature and performed the
literature review. XDY and YYY wrote the manuscript. YYY, PFF and
XDY revised the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors have no competing interests to
declare.
References
|
1
|
International Diabetes Federation (IDF).
IDF Diabetes Atlas (7th). 2017.
|
|
2
|
Edwards JL, Vincent AM, Cheng HT and
Feldman EL: Diabetic neuropathy: Mechanisms to management.
Pharmacol Ther. 120:1–34. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Harati Y: Diabetic neuropathies:
Unanswered questions. Neurol Clin. 25:303–317. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Farmer KL, Li C and Dobrowsky RT: Diabetic
peripheral neuropathy: Should a chaperone accompany our therapeutic
approach? Pharmacol Rev. 64:880–900. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Spallone V, Lacerenza M, Rossi A, Sicuteri
R and Marchettini P: Painful diabetic polyneuropathy: Approach to
diagnosis and management. Clin J Pain. 28:726–743. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Snyder MJ, Gibbs LM and Lindsay TJ:
Treating painful diabetic peripheral neuropathy: An update. Am Fam
Physician. 94:227–234. 2016.PubMed/NCBI
|
|
7
|
Schreiber AK, Nones CF, Reis RC, Chichorro
JG and Cunha JM: Diabetic neuropathic pain: Physiopathology and
treatment. World J Diabetes. 6:432–444. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tesfaye S, Vileikyte L, Rayman G, Sindrup
SH, Perkins BA, Baconja M, Vinik AI and Boulton AJ: Toronto Expert
Panel on Diabetic Neuropathy: Painful diabetic peripheral
neuropathy: Consensus recommendations on diagnosis, assessment and
management. Diabetes Metab Res Rev. 27:629–638. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Jane SW, Lin MS, Chiu WN, Beaton RD and
Chen MY: Prevalence, discomfort and self-relief behaviours of
painful diabetic neuropathy in Taiwan: A cross-sectional study. BMJ
Open. 6:e118972016. View Article : Google Scholar
|
|
10
|
Tesfaye S, Boulton AJ and Dickenson AH:
Mechanisms and management of diabetic painful distal symmetrical
polyneuropathy. Diabetes Care. 36:2456–2465. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gore M, Brandenburg NA, Dukes E, Hoffman
DL, Tai KS and Stacey B: Pain severity in diabetic peripheral
neuropathy is associated with patient functioning, symptom levels
of anxiety and depression, and sleep. J Pain Symptom Manage.
30:374–385. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Vileikyte L, Leventhal H, Gonzalez JS,
Peyrot M, Rubin RR, Ulbrecht JS, Garrow A, Waterman C, Cavanagh PR
and Boulton AJ: Diabetic peripheral neuropathy and depressive
symptoms: The association revisited. Diabetes Care. 28:2378–2383.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sadosky A, McDermott AM, Brandenburg NA
and Strauss M: A review of the epidemiology of painful diabetic
peripheral neuropathy, postherpetic neuralgia, and less commonly
studied neuropathic pain conditions. Pain Pract. 8:45–56. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ziegler D: Painful diabetic neuropathy:
Treatment and future aspects. Diabetes Metab Res Rev. 24 Suppl
1:S52–S57. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kaku M, Vinik A and Simpson DM: Pathways
in the diagnosis and management of diabetic polyneuropathy. Curr
Diab Rep. 15:6092015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Sawynok J and Zinger C: Topical
amitriptyline and ketamine for post-herpetic neuralgia and other
forms of neuropathic pain. Expert Opin Pharmacother. 17:601–609.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ziegler D and Fonseca V: From guideline to
patient: A review of recent recommendations for pharmacotherapy of
painful diabetic neuropathy. J Diabetes Complications. 29:146–156.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
van Nooten F, Treur M, Pantiri K, Stoker M
and Charokopou M: Capsaicin 8% patch versus oral neuropathic pain
medications for the treatment of painful diabetic peripheral
neuropathy: A systematic literature review and network
meta-analysis. Clin Ther. 39:787–803.e18. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Argoff CE: Topical analgesics in the
management of acute and chronic pain. Mayo Clin Proc. 88:195–205.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Jorge LL, Feres CC and Teles VE: Topical
preparations for pain relief: Efficacy and patient adherence. J
Pain Res. 4:11–24. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Derry S, Rice AS, Cole P, Tan T and Moore
RA: Topical capsaicin (high concentration) for chronic neuropathic
pain in adults. Cochrane Database Syst Rev.
1:CD0073932017.PubMed/NCBI
|
|
22
|
Mick G and Correa-Illanes G: Topical pain
management with the 5% lidocaine medicated plaster-a review. Curr
Med Res Opin. 28:937–951. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Mou J, Paillard F, Turnbull B, Trudeau J,
Stoker M and Katz NP: Qutenza (capsaicin) 8% patch onset and
duration of response and effects of multiple treatments in
neuropathic pain patients. Clin J Pain. 30:286–294. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kiani J, Ahmad Nasrollahi S, Esna-Ashari
F, Fallah P and Sajedi F: Amitriptyline 2% cream vs. capsaicin
0.75% cream in the treatment of painful diabetic neuropathy (Double
blind, randomized clinical trial of efficacy and safety). Iran J
Pharm Res. 14:1263–1268. 2015.PubMed/NCBI
|
|
25
|
Wrzosek A, Woron J, Dobrogowski J,
Jakowicka-Wordliczek J and Wordliczek J: Topical clonidine for
neuropathic pain. Cochrane Database Syst Rev.
8:CD0109672015.PubMed/NCBI
|
|
26
|
Motilal S and Maharaj RG: Nutmeg extracts
for painful diabetic neuropathy: A randomized, double-blind,
controlled study. J Altern Complement Med. 19:347–352. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Heydari M, Homayouni K, Hashempur MH and
Shams M: Topical Citrullus colocynthis (bitter apple) extract oil
in painful diabetic neuropathy: A double-blind randomized
placebo-controlled clinical trial. J Diabetes. 8:246–252. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
A study of the efficacy and safety of
amitriptyline/ketamine topical cream in patients with diabetic
peripheral neuropathy. simpleClinicalTrials.govNCT00476151. 2006
|
|
29
|
Casale R, Symeonidou Z and Bartolo M:
Topical treatments for localized neuropathic pain. Curr Pain
Headache Rep. 21:152017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Sloan G, Shillo P, Selvarajah D, Wu J,
Wilkinson ID, Tracey I, Anand P and Tesfaye S: A new look at
painful diabetic neuropathy. Diabetes Res Clin Pract. 144:177–191.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Dewanjee S, Das S, Das AK, Bhattacharjee
N, Dihingia A, Dua TK, Kalita J and Manna P: Molecular mechanism of
diabetic neuropathy and its pharmacotherapeutic targets. Eur J
Pharmacol. 833:472–523. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Dobretsov M, Hastings SL, Romanovsky D,
Stimers JR and Zhang JM: Mechanical hyperalgesia in rat models of
systemic and local hyperglycemia. Brain Res. 960:174–183. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Oyibo SO, Prasad YD, Jackson NJ, Jude EB
and Boulton AJ: The relationship between blood glucose excursions
and painful diabetic peripheral neuropathy: A pilot study. Diabet
Med. 19:870–873. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Morley GK, Mooradian AD, Levine AS and
Morley JE: Mechanism of pain in diabetic peripheral neuropathy.
Effect of glucose on pain perception in humans. Am J Med. 77:79–82.
1984. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Lee JH, Cox DJ, Mook DG and McCarty RC:
Effect of hyperglycemia on pain threshold in alloxan-diabetic rats.
Pain. 40:105–107. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Dyck PJ, Litchy WJ, Lehman KA, Hokanson
JL, Low PA and O'Brien PC: Variables influencing neuropathic
endpoints: The rochester diabetic neuropathy study of healthy
subjects. Neurology. 45:1115–1121. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Romanovsky D, Wang J, Al-Chaer ED, Stimers
JR and Dobretsov M: Comparison of metabolic and neuropathy profiles
of rats with streptozotocin-induced overt and moderate
insulinopenia. Neuroscience. 170:337–347. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Peppa M, Stavroulakis P and Raptis SA:
Advanced glycoxidation products and impaired diabetic wound
healing. Wound Repair Regen. 17:461–472. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Babizhayev MA, Strokov IA, Nosikov VV,
Savel'Yeva EL, Sitnikov VF, Yegorov YE and Lankin VZ: The role of
oxidative stress in diabetic neuropathy: Generation of free radical
species in the glycation reaction and gene polymorphisms encoding
antioxidant enzymes to genetic susceptibility to diabetic
neuropathy in population of type i diabetic patients. Cell Biochem
Biophys. 71:1425–1443. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Oates PJ: Polyol pathway and diabetic
peripheral neuropathy. Int Rev Neurobiol. 50:325–392. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Obrosova IG: How does glucose generate
oxidative stress in peripheral nerve Int Rev Neurobiol. 50:3–35.
2002.PubMed/NCBI
|
|
42
|
Obrosova IG: Diabetes and the peripheral
nerve. Biochim Biophys Acta. 1792:931–940. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Schemmel KE, Padiyara RS and D'Souza JJ:
Aldose reductase inhibitors in the treatment of diabetic peripheral
neuropathy: A review. J Diabetes Complications. 24:354–360. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Fuchs D, Birklein F, Reeh PW and Sauer SK:
Sensitized peripheral nociception in experimental diabetes of the
rat. Pain. 151:496–505. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Bachewal P, Gundu C, Yerra VG, Kalvala AK,
Areti A and Kumar A: Morin exerts neuroprotection via attenuation
of ROS induced oxidative damage and neuroinflammation in
experimental diabetic neuropathy. Biofactors. 44:109–122. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Tobon-Velasco JC, Cuevas E and
Torres-Ramos MA: Receptor for AGEs (RAGE) as mediator of NF-kB
pathway activation in neuroinflammation and oxidative stress. CNS
Neurol Disord Drug Targets. 13:1615–1626. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Gao X, Wu B, Fu Z, Zhang Z and Xu G:
Carvedilol abrogates hypoxia-induced oxidative stress and
neuroinflammation in microglial BV2 cells. Eur J Pharmacol.
814:144–150. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Dworkin RH: An overview of neuropathic
pain: Syndromes, symptoms, signs, and several mechanisms. Clin J
Pain. 18:343–349. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Djouhri L, Fang X, Koutsikou S and Lawson
SN: Partial nerve injury induces electrophysiological changes in
conducting (uninjured) nociceptive and nonnociceptive DRG neurons:
Possible relationships to aspects of peripheral neuropathic pain
and paresthesias. Pain. 153:1824–1836. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Aslam A, Singh J and Rajbhandari S:
Pathogenesis of painful diabetic neuropathy. Pain Res Treat.
2014:4120412014.PubMed/NCBI
|
|
51
|
Rahman MH, Jha MK and Suk K: Evolving
insights into the pathophysiology of diabetic neuropathy:
Implications of malfunctioning glia and discovery of novel
therapeutic targets. Curr Pharm Des. 22:738–757. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Baron R, Mayoral V, Leijon G, Binder A,
Steigerwald I and Serpell M: 5% lidocaine medicated plaster versus
pregabalin in post-herpetic neuralgia and diabetic polyneuropathy:
An open-label, non-inferiority two-stage RCT study. Curr Med Res
Opin. 25:1663–1676. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Krumova EK, Zeller M, Westermann A and
Maier C: Lidocaine patch (5%) produces a selective, but incomplete
block of Aδ and C fibers. Pain. 153:273–280. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Herrmann DN, Barbano RL, Hart-Gouleau S,
Pennella-Vaughan J and Dworkin RH: An open-label study of the
lidocaine patch 5% in painful idiopathic sensory polyneuropathy.
Pain Med. 6:379–384. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Argoff CE, Galer BS, Jensen MP, Oleka N
and Gammaitoni AR: Effectiveness of the lidocaine patch 5% on pain
qualities in three chronic pain states: Assessment with the
neuropathic pain scale. Curr Med Res Opin. 20 Suppl 2:S21–S28.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Barbano RL, Herrmann DN, Hart-Gouleau S,
Pennella-Vaughan J, Lodewick PA and Dworkin RH: Effectiveness,
tolerability, and impact on quality of life of the 5% lidocaine
patch in diabetic polyneuropathy. Arch Neurol. 61:914–918. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Devers A and Galer BS: Topical lidocaine
patch relieves a variety of neuropathic pain conditions: An
open-label study. Clin J Pain. 16:205–208. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Wolff RF, Bala MM, Westwood M, Kessels AG
and Kleijnen J: 5% lidocaine medicated plaster in painful diabetic
peripheral neuropathy (DPN): A systematic review. Swiss Med Wkly.
140:297–306. 2010.PubMed/NCBI
|
|
59
|
Baron R, Mayoral V, Leijon G, Binder A,
Steigerwald I and Serpell M: Efficacy and safety of 5% lidocaine
(lignocaine) medicated plaster in comparison with pregabalin in
patients with postherpetic neuralgia and diabetic polyneuropathy:
Interim analysis from an open-label, two-stage adaptive,
randomized, controlled trial. Clin Drug Investig. 29:231–241. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Baron R, Mayoral V, Leijon G, Binder A,
Steigerwald I and Serpell M: Efficacy and safety of combination
therapy with 5% lidocaine medicated plaster and pregabalin in
post-herpetic neuralgia and diabetic polyneuropathy. Curr Med Res
Opin. 25:1677–1687. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
White WT, Patel N, Drass M and Nalamachu
S: Lidocaine patch 5% with systemic analgesics such as gabapentin:
A rational polypharmacy approach for the treatment of chronic pain.
Pain Med. 4:321–330. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Ho KY, Huh BK, White WD, Yeh CC and Miller
EJ: Topical amitriptyline versus lidocaine in the treatment of
neuropathic pain. Clin J Pain. 24:51–55. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Zheng J, Zheng S, Feng Q, Zhang Q and Xiao
X: Dietary capsaicin and its anti-obesity potency: From mechanism
to clinical implications. Biosci Rep. 37(pii): BSR20170286.
2017.
|
|
64
|
Musharraf MU, Ahmad Z and Yaqub Z:
Comparison of topical capsaicin and topical turpentine Oil for
treatment of painful diabetic neuropathy. J Ayub Med Coll
Abbottabad. 29:384–387. 2017.PubMed/NCBI
|
|
65
|
Mitchell K, Bates BD, Keller JM, Lopez M,
Scholl L, Navarro J, Madian N, Haspel G, Nemenov MI and Iadarola
MJ: Ablation of rat TRPV1-expressing Adelta/C-fibers with
resiniferatoxin: Analysis of withdrawal behaviors, recovery of
function and molecular correlates. Mol Pain. 6:942010. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Fattori V, Hohmann MS, Rossaneis AC,
Pinho-Ribeiro FA and Verri WA: Capsaicin: Current understanding of
its mechanisms and therapy of pain and other pre-clinical and
clinical uses. Molecules. 21(pii): E8442016. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
What role for capsaicin in diabetic
peripheral neuropathy? Drug Ther Bull. 54:90–93. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Rosenberg CJ and Watson JC: Treatment of
painful diabetic peripheral neuropathy. Prosthet Orthot Int.
39:17–28. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Treatment of painful diabetic neuropathy
with topical capsaicin. A multicenter, double-blind,
vehicle-controlled study. The Capsaicin Study Group. Arch Intern
Med. 151:2225–2229. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Effect of treatment with capsaicin on
daily activities of patients with painful diabetic neuropathy. The
Capsaicin Study Group. Diabetes Care. 15:159–165. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Biesbroeck R, Bril V, Hollander P, Kabadi
U, Schwartz S, Singh SP, Ward WK and Bernstein JE: A double-blind
comparison of topical capsaicin and oral amitriptyline in painful
diabetic neuropathy. Adv Ther. 12:111–120. 1995.PubMed/NCBI
|
|
72
|
Tandan R, Lewis GA, Badger GB and Fries
TJ: Topical capsaicin in painful diabetic neuropathy. Effect on
sensory function. Diabetes Care. 15:15–18. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Tandan R, Lewis GA, Krusinski PB, Badger
GB and Fries TJ: Topical capsaicin in painful diabetic neuropathy.
Controlled study with long-term follow-up. Diabetes Care. 15:8–14.
1992. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Chad DA, Aronin N, Lundstrom R, McKeon P,
Ross D, Molitch M, Schipper HM, Stall G, Dyess E and Tarsy D: Does
capsaicin relieve the pain of diabetic neuropathy? Pain.
42:387–388. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Kulkantrakorn K, Lorsuwansiri C and
Meesawatsom P: 0.025% capsaicin gel for the treatment of painful
diabetic neuropathy: A randomized, double-blind, crossover,
placebo-controlled trial. Pain Pract. 13:497–503. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Simpson DM, Robinson-Papp J, Van J, Stoker
M, Jacobs H, Snijder RJ, Schregardus DS, Long SK, Lambourg B and
Katz N: Capsaicin 8% patch in painful diabetic peripheral
neuropathy: A randomized, double-blind, placebo-controlled study. J
Pain. 18:42–53. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Vinik AI, Perrot S, Vinik EJ, Pazdera L,
Jacobs H, Stoker M, Long SK, Snijder RJ, van der Stoep M, Ortega E
and Katz N: Capsaicin 8% patch repeat treatment plus standard of
care (SOC) versus SOC alone in painful diabetic peripheral
neuropathy: A randomised, 52-week, open-label, safety study. BMC
Neurol. 16:2512016. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Bril V, England J, Franklin GM, Backonja
M, Cohen J, Del Toro D, Feldman E, Iverson DJ, Perkins B, Russell
JW, et al: Evidence-based guideline: Treatment of painful diabetic
neuropathy: Report of the American academy of neurology, the
American association of neuromuscular and electrodiagnostic
medicine and the American academy of physical medicine and
rehabilitation. PM R. 3:345–352. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Pancrazio JJ, Kamatchi GL, Roscoe AK and
Lynch CR III: Inhibition of neuronal Na+ channels by antidepressant
drugs. J Pharmacol Exp Ther. 284:208–214. 1998.PubMed/NCBI
|
|
80
|
Nicholson GM, Blanche T, Mansfield K and
Tran Y: Differential blockade of neuronal voltage-gated Na(+) and
K(+) channels by antidepressant drugs. Eur J Pharmacol. 452:35–48.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Joshi PG, Singh A and Ravichandra B: High
concentrations of tricyclic antidepressants increase intracellular
Ca2+ in cultured neural cells. Neurochem Res. 24:391–398. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Watson CP: The treatment of neuropathic
pain: Antidepressants and opioids. Clin J Pain. 16 (2
Suppl):S49–S55. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Kopsky DJ and Hesselink JM: High doses of
topical amitriptyline in neuropathic pain: Two cases and literature
review. Pain Pract. 12:148–153. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Zeraatian S, Zakeri H, Boroojeny SB,
Hourang MH, Ghaffarpasand F and Fard MM: Effect of oral clonidine
on acute intraocular pressure rise after phacoemulsification: A
prospective double-blind, randomized, clinical trial. J Ocul
Pharmacol Ther. 27:293–297. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Otasowie J, Castells X, Ehimare UP and
Smith CH: Tricyclic antidepressants for attention deficit
hyperactivity disorder (ADHD) in children and adolescents. Cochrane
Database Syst Rev. 9:CD0069972014.
|
|
86
|
Sawynok J: Topical analgesics for
neuropathic pain: Preclinical exploration, clinical validation,
future development. Eur J Pain. 18:465–481. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Campbell C, Campbell J, Schmidt W, Brady K
and Stouch B: Topical clonidine gel reduces pain caused by diabetic
neuropathy: Results of a multicenter, placebo-controlled clinical
trial. J Pain. 10 Suppl:S552009. View Article : Google Scholar
|
|
88
|
Campbell CM, Kipnes MS, Stouch BC, Brady
KL, Kelly M, Schmidt WK, Petersen KL, Rowbotham MC and Campbell JN:
Randomized control trial of topical clonidine for treatment of
painful diabetic neuropathy. Pain. 153:1815–1823. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Grover JK, Khandkar S, Vats V, Dhunnoo Y
and Das D: Pharmacological studies on myristica
fragrans-antidiarrheal, hypnotic, analgesic and hemodynamic (blood
pressure) parameters. Methods Find Exp Clin Pharmacol. 24:675–680.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Hayfaa AA, Sahar AM and Awatif MA:
Evaluation of analgesic activity and toxicity of alkaloids in
myristica fragrans seeds in mice. J Pain Res. 6:611–615. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Forouzanfar F and Hosseinzadeh H:
Medicinal herbs in the treatment of neuropathic pain: A review.
Iran J Basic Med Sci. 21:347–358. 2018.PubMed/NCBI
|
|
92
|
Ramanathan T, Gurudeeban S and Satyavani
K: Local anesthetic effect of citrullus colocynthis on rana
hexadactyla. Res J Med Plant. 5:338–342. 2011. View Article : Google Scholar
|
|
93
|
Kumar S, Kumar D, Manjusha, Saroha K,
Singh N and Vashishta B: Antioxidant and free radical scavenging
potential of citrullus colocynthis (L.) schrad. Methanolic fruit
extract. Acta Pharm. 58:215–220. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Reddy VP, Sudheshna G, Shaik A, Saran SS,
Kumar SN, Ram CR and Reddy KR: Evaluation of antiulcer activity of
Citrullus colocynthis fruit against pylorus ligation induced ulcers
in male Wistar rats. Int J Pharm Pharm Sci. 4:446–451. 2012.
|
|
95
|
Nedjat S, Montazeri A, Holakouie K,
Mohammad K and Majdzadeh R: Psychometric properties of the Iranian
interview-administered version of the world health organization's
quality of life questionnaire (WHOQOL-BREF): A population-based
study. BMC Health Serv Res. 8:612008. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Lynch ME, Clark AJ, Sawynok J and Sullivan
MJ: Topical 2% amitriptyline and 1% ketamine in neuropathic pain
syndromes: A randomized, double-blind, placebo-controlled trial.
Anesthesiology. 103:140–146. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Hocking G and Cousins MJ: Ketamine in
chronic pain management: An evidence-based review. Anesth Analg.
97:1730–1739. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Niesters M, Martini C and Dahan A:
Ketamine for chronic pain: Risks and benefits. Br J Clin Pharmacol.
77:357–367. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Mion G and Villevieille T: Ketamine
pharmacology: An update (pharmacodynamics and molecular aspects,
recent findings). Cns Neurosci Ther. 19:370–380. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Mahoney JM, Vardaxis V, Moore JL, Hall AM,
Haffner KE and Peterson MC: Topical ketamine cream in the treatment
of painful diabetic neuropathy: A randomized, placebo-controlled,
double-blind initial study. J Am Podiatr Med Assoc. 102:178–183.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Lynch ME, Clark AJ and Sawynok J: A pilot
study examining topical amitriptyline, ketamine, and a combination
of both in the treatment of neuropathic pain. Clin J Pain.
19:323–328. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Lynch ME, Clark AJ, Sawynok J and Sullivan
MJ: Topical amitriptyline and ketamine in neuropathic pain
syndromes: An open-label study. J Pain. 6:644–649. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Somberg JC and Molnar J: Retrospective
study on the analgesic activity of a topical (TT-CTAC) cream in
patients with diabetic neuropathy and other chronic pain
conditions. Am J Ther. 22:214–221. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Javed S, Petropoulos IN, Alam U and Malik
RA: Treatment of painful diabetic neuropathy. Ther Adv Chronic Dis.
6:15–28. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Stanos SP and Galluzzi KE: Topical
therapies in the management of chronic pain. Postgrad Med. 125 (4
Suppl):S25–S33. 2013. View Article : Google Scholar
|
|
106
|
Barkin RL: The pharmacology of topical
analgesics. Postgrad Med. 125 (4 Suppl 1):S7–S18. 2013. View Article : Google Scholar
|
|
107
|
Pickering G, Martin E, Tiberghien F,
Delorme C and Mick G: Localized neuropathic pain: An expert
consensus on local treatments. Drug Des Devel Ther. 11:2709–2718.
2017. View Article : Google Scholar : PubMed/NCBI
|