Introduction
Burns are a common type of injury that may cause
different degrees of impairment of the body's function and
appearance, thus affecting the quality of life and placing a burden
on the affected patients and their family; depending on the extent
and degree, they may even be life-threatening. With the substantial
development of industry and transportation, the demand and use of
energy, oil and coal are rising, which increases the incidence of
burns. It is estimated that >10,000,000 individuals suffer from
burns every year in China, and, compared with the general
population, the incidence rate of burn injury is increased in the
coal, petroleum, chemical and metallurgical industries (1). According to statistics, burns are the
fourth most common type of injury in the world, ranking behind
traffic accidents, falls and intentional injuries. It is estimated
that ~100 million people are burned every year in the world, with
>10 million requiring hospitalization, and >200,000
succumbing to mortality (2).
The treatment of patients with a large total body
surface area of the burn (TBSA) or a large full-thickness burn area
is challenging. A burn is not only a type of local injury but also
a complex systemic disease that is difficult to treat, and the
associated mortality and disability rates are high. According to UK
data, there are ~13,000 hospitalized burn casualties and 300 deaths
annually in the UK, with a mortality rate of 2.31% (3). The occurrence of a burn brings great
trauma to the patient, their family and society, and the burden is
not only physical but also psychological and economic in nature. In
the previous decades, the quality of burn treatments in China has
markedly improved and the survival rate of burn patients has
significantly increased. However, reducing the incidence of burns
has also become a practical challenge (1).
Recently, numerous scholars have categorized burns
according to patient age, including pediatric burns (4) and geriatric burns (5), the cause of injury, including
electrical injury (6) and chemical
burns (7), and the location of the
burn, e.g., hand burns (8) and
auricular burns (9); however,
studies providing an overall analysis are rare, and epidemiological
data for burn patients vary between locations due to regional,
climatic and human factors.
In the present study, 9,779 burn patients
hospitalized at Southwest Hospital between January 2009 and
December 2016 were retrospectively analysed. Among them, 68 deaths
occurred, resulting in a mortality rate of 0.7%. After collecting
relevant information, the general condition, cause of injury, burn
area and complications of the burn patients were analyzed and
conclusions were drawn from these analyses. An accurate
determination of the degree of the burn may enable medical staff to
make a more objective clinical diagnosis and effective treatment.
Furthermore, a retrospective analysis of clinical cases may provide
suggestions for implementing further burn prevention strategies in
southwest China aimed at seasonal and regional characteristics.
Materials and methods
Clinical data
The data of burn patients (n=13,205) who were
admitted to the Southwest Hospital of the Army Medical University
(Chongqing, China) between January 1, 2009 and December 31, 2016
were retrieved from the hospital's Electronic Medical Record
System. Patients without acute burn injuries (i.e., those with
scarring, cosmetic problems or chronic wounds), were excluded
(n=3,426). The medical records of the hospitalized patients were
reviewed, including demographic information, causes of and factors
associated with the injury, pre-hospital and hospital treatment and
demographic data (age, gender, residential area, admission date and
discharge date), injury-associated data (condition of the burn,
etiology of burn injuries, TBSA and degree of burn), major
complications and the treatment outcomes (cure, improvement,
abandon treatment or death).
Statistical analysis
After the data were collected and listed using Excel
2007 (Microsoft Corp., Redmond, WA, USA), the statistical software
SPSS 20.0 (IBM Corp., Armonk, NY, USA) was used to perform analysis
of variance, followed by Fisher's least significant difference post
hoc test and the χ2 test between different groups. The
mean ± standard deviation or the median [interquartile range (IQR)]
was used to describe the dispersion of variables among the
statistical data. The Mann-Whitney U-test was performed to compare
two or more medians of categorical variables (age, gender, type of
burn, outcome). Multivariate logistic regression analysis was used
to screen for risk factors for burn patients. The χ2
test was used for pairwise and multi-group comparisons. P<0.05
was considered to indicate a statistically significant
difference.
Results
General analysis
During the period from 2009 to 2016, 13,205 burn
patients were admitted to the Burn Research Institute of Southwest
Hospital of the Army Medical University (Chongqing, China). After
excluding 3,426 inpatients who were not mainly treated for burns,
9,779 patients were retained. Among them, 6,560 (67.1%) were male
and 3,219 (32.9%) were female. The burn patients covered each age
group, with those aged 25–49 years accounting for the largest
proportion at 36.1%. The patients were mainly from Chongqing,
followed by Sichuan and Guizhou. The median and IQR of the length
of stay was 17 (8–33) days. The group aged 0–1 years included
almost the same number of patients as that of the group aged 2–14
years. According to a statistical analysis, the mortality rate was
only 0.7%. The medians and IQRs of the TBSA and full-thickness burn
area for all patients are presented in Table I. When formulating a burn prevention
strategy, it is required to consider not only the characteristics
of the burn itself but also the distribution, season, climate and
human factors of the local population. Male inpatients were more
common than female inpatients. The proportions of burn patients
admitted in the Spring, Summer, Autumn and Winter were 25.8, 28.3,
22.2 and 23.7%, respectively, with the proportion being slightly
higher in the Summer (Figs.
1–4).
 | Table I.General data of the hospitalized
patients (n=9,779). |
Table I.
General data of the hospitalized
patients (n=9,779).
| Characteristics | Value |
|---|
| Gender |
|
| Male | 6,560 (67.1) |
|
Female | 3,219 (32.9) |
| Age (years) |
|
| 0–1 | 1,807 (18.5) |
| 2–14 | 2,027 (20.7) |
|
15–24 | 806 (8.2) |
|
25–49 | 3,535 (36.1) |
| ≥50 | 1,604 (16.4) |
| Residence |
|
|
Chongqing | 7,237 (74.0) |
|
Sichuan | 1,628 (16.6) |
|
Guizhou | 518 (5.3) |
|
Others | 396 (4.0) |
| Season of burn |
|
|
Spring | 2,520 (25.8) |
|
Summer | 2,768 (28.3) |
|
Autumn | 2,173 (22.2) |
|
Winter | 2,318 (23.7) |
| Outcome |
|
|
Death | 68 (0.7) |
| Cure | 9,629 (98.5) |
| Abandon
treatment | 75 (0.8) |
|
Improvement | 7 (0.07) |
| Shock |
|
| Yes | 230 (2.4) |
| No | 9,549 (97.6) |
| Inhalation
injury |
|
| Yes | 412 (4.2) |
| No | 9,367 (95.8) |
| Complications |
|
| Yes | 141 (1.4) |
| No | 9,638 (98.6) |
| Total burn area
(%) | 8 (4–15) |
| Full-thickness burn
area (%) | 0 (0–2) |
| Length of hospital
stay (days) | 17 (9–33) |
Analysis of the burn patients
regarding gender and age
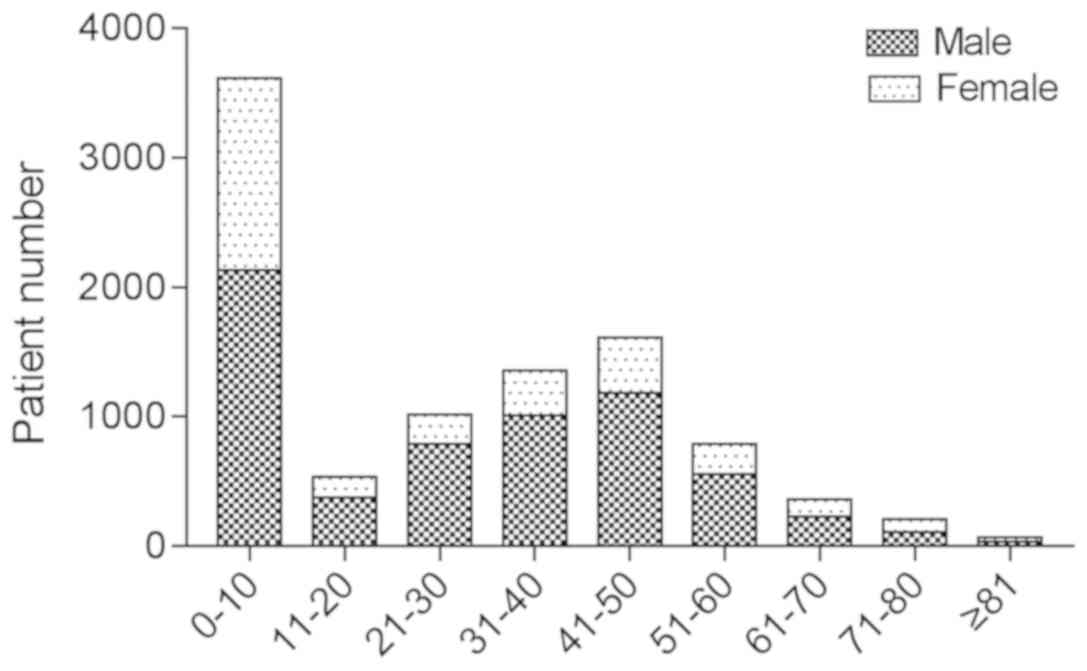
The 0–10-year-old group had the largest number of
burns and included more males than females (Fig. 1). In the 0–1-year-old age group, no
significant difference was observed among the patients in terms of
gender and causes of injury. In the group of patients aged ≥2
years, significant differences in the cause of the burn between
different genders were identified (Table II). With the increase in age, the
number of patients with burn injuries decreased. Of note, 2,637
male patients and 898 female patients were included in the
25–49-year-old group. As presented in Table II, the number of male burn patients
was higher than that of females. After dividing the patients into 5
different age groups, a significant difference in the cause of
injury by gender in the 0–1-year-old age group was identified,
while significant differences were present in the other age groups
(P<0.01; Table II). Analysis of
the TBSA by gender revealed no significant differences (P>0.05;
Table III).
| Table II.Causes of burns by gender and
age. |
Table II.
Causes of burns by gender and
age.
| Age
(years)/gender | Scalds | Flame | Electric | Solid
materials | Steam | Explosion | Others |
χ2 | P-value |
|---|
| 0–1 |
|
|
|
|
|
|
|
|
|
|
Male | 951 (9.72) | 76 (0.78) | 6 (0.06) | 13 (0.13) | 4 (0.04) | 0 (0.00) | 28 (0.29) | 0.544 | 0.995 |
|
Female | 641 (6.55) | 53 (5.42) | 5 (0.51) | 10 (1.02) | 2 (0.20) | 0 (0.00) | 18 (1.84) |
|
|
| 2–14 |
|
|
|
|
|
|
|
|
|
|
Male | 734 (7.51) | 298 (3.05) | 87 (0.89) | 15 (0.15) | 7 (0.07) | 12 (0.12) | 46 (0.47) | 31.919 | <0.001 |
|
Female | 599 (6.13) | 150 (1.53) | 31 (0.32) | 12 (0.12) | 5 (0.05) | 4 (0.04) | 27 (0.28) |
|
|
| 15–24 |
|
|
|
|
|
|
|
|
|
|
Male | 95 (0.97) | 199 (2.03) | 179 (1.83) | 41 (0.42) | 8 (0.08) | 5 (0.05) | 71 (0.73) | 85.87 | <0.001 |
|
Female | 74 (0.76) | 79 (0.81) | 4 (0.04) | 14 (0.14) | 6 (0.06) | 3 (0.03) | 28 (0.29) |
|
|
| 25–49 |
|
|
|
|
|
|
|
|
|
|
Male | 266 (2.72) | 808 (8.26) | 890 (9.10) | 277 (2.83) | 33 (0.34) | 30 (0.31) | 333 (3.41) | 520.113 | <0.001 |
|
Female | 319 (3.26) | 326 (3.33) | 44 (0.45) | 39 (0.40) | 21 (0.21) | 6 (0.06) | 143 (1.46) |
|
|
| ≥50 |
|
|
|
|
|
|
|
|
|
|
Male | 169 (1.73) | 417 (4.26) | 228 (2.33) | 72 (0.74) | 15 (0.15) | 12 (0.12) | 135 (1.38) | 170.027 | <0.001 |
|
Female | 220 (2.25) | 226 (2.31) | 22 (0.22) | 18 (0.18) | 8 (0.08) | 1 (0.01) | 61 (0.62) |
|
|
| Total |
|
|
|
|
|
|
|
|
|
|
Male | 2,215 (22.65) | 1,798 (18.39) | 1,390 (14.21) | 418 (4.27) | 67 (0.69) | 59 (0.60) | 613 (6.27) | 807.114 | <0.001 |
|
Female | 1,853 (18.95) | 834 (8.53) | 106 (1.08) | 93 (0.95) | 42 (0.43) | 14 (0.14) | 277 (2.83) |
|
|
| Table III.Burn TBSA by gender and age
group. |
Table III.
Burn TBSA by gender and age
group.
|
Parameters | TBSA |
χ2 | P-value |
|---|
| Gender |
|
|
|
|
Male | 8 (4–15) | −0.440 | 0.660 |
|
Female | 8 (4–15) |
|
|
| Age (years) |
|
|
|
|
0–1 | 8 (5–13) | 57.309 | <0.001 |
|
2–14 | 8 (5–15) |
|
|
|
15–24 | 6 (2–15) |
|
|
|
25–49 | 8 (3–17) |
|
|
|
≥50 | 7 (2–16) |
|
|
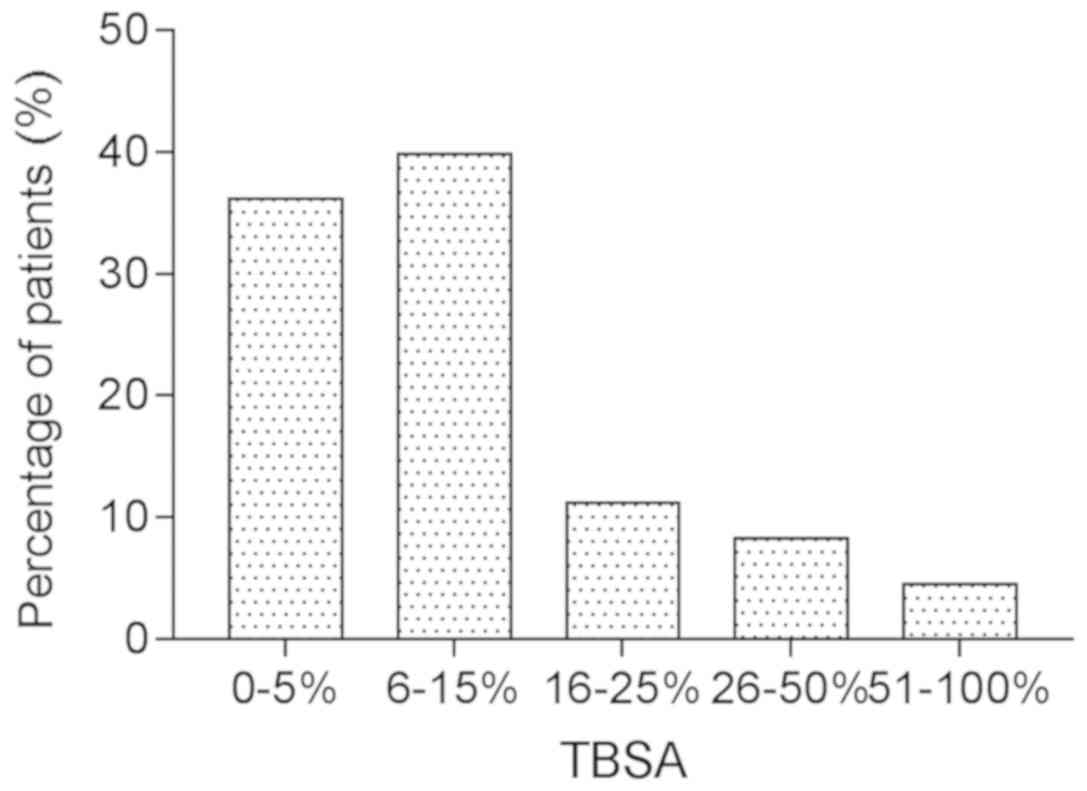
Analysis of the TBSA
Among all of the hospitalized patients, the minimum
TBSA was 0.1% and the maximum TBSA was 100%. The groups with a TBSA
of 0–5 and 6–15% included more burn victims but fewer deaths
compared with those in the groups with a higher TBSA. With the
increase in the TBSA, the number of deaths increases gradually
(Table IV). The number of deaths
increased significantly when the TBSA was >50%, although the
number of cases in that group was lower than that in the groups
with a lower TBSA.
| Table IV.Outcome of burns by sex and total
burn area. |
Table IV.
Outcome of burns by sex and total
burn area.
| TBSA (%) | Sex | Discharged (n) | Death (n) | Percentage
death |
|---|
| 0–5 | Male | 2,464 | 0 | 0.00 |
|
| Female | 1,187 | 2 | 0.17 |
| 6–15 | Male | 2,510 | 1 | 0.04 |
|
| Female | 1,307 | 1 | 0.08 |
| 16–25 | Male | 702 | 1 | 0.14 |
|
| Female | 374 | 0 | 0.00 |
| 26–50 | Male | 541 | 8 | 1.48 |
|
| Female | 243 | 2 | 0.82 |
| 51–60 | Male | 92 | 2 | 2.17 |
|
| Female | 43 | 0 | 0.00 |
| 61–70 | Male | 63 | 3 | 4.76 |
|
| Female | 19 | 1 | 5.26 |
| ≥71 | Male | 132 | 41 | 31.06 |
|
| Female | 34 | 6 | 17.65 |
Association of TBSA with the cause of
burns and length of hospital stay (LOS)
Scalding, flame and electricity were the major
causes of burn injury, followed by solid materials and hot steam. A
significant difference was identified in the TBSA between different
burn types and in-hospital mortality (Table V). Other causes of burns mainly
included infrared, ultraviolet and high-temperature dust (data not
shown). Among all causes of burn injury, the death rate of patients
with chemical burns was highest, as the burn degree was deeper and
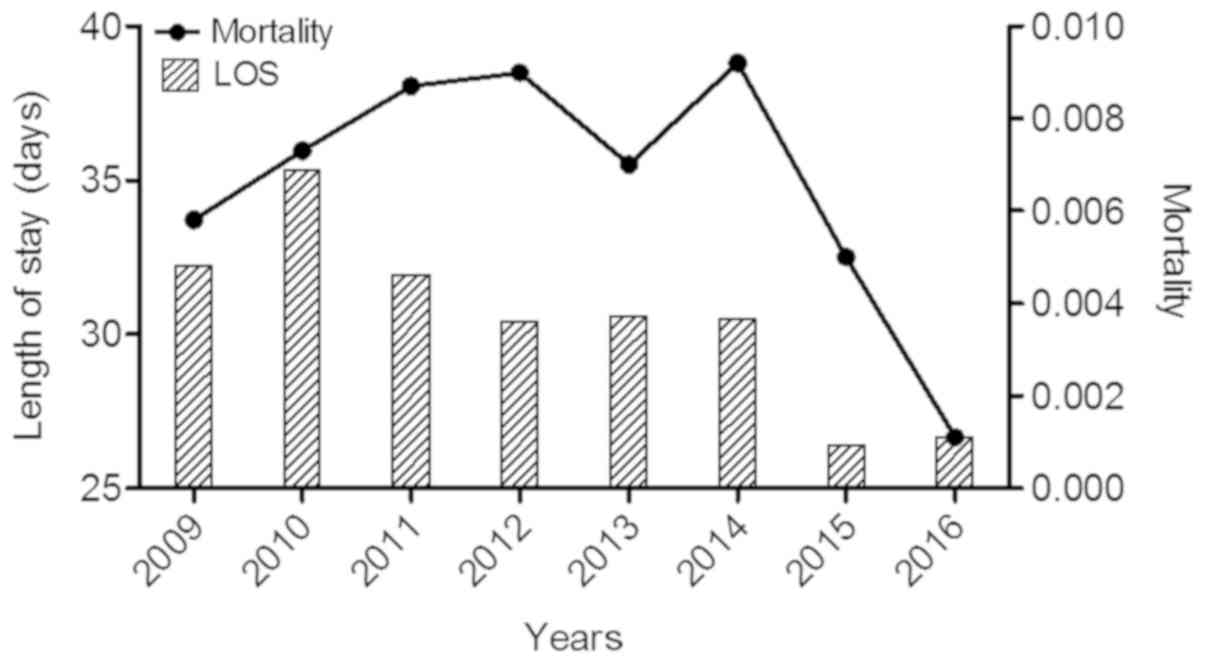
the complications were more serious (results not shown) (10). Recently, with the renewal of
treatment concepts and the refinement of the management of burn
patients, the importance of the LOS of burn patients has gradually
been emphasized These new treatment concepts and patient management
contribute to the shorter LOS and lower mortality in 2015 and 2016
(Fig. 5).
| Table V.Total burn area by burn type and
in-hospital mortality. |
Table V.
Total burn area by burn type and
in-hospital mortality.
| Item | TBSA |
χ2 | P-value |
|---|
| Cause of burn |
|
|
|
|
Scalds | 8 (5–15) | 1,016.876 | <0.001 |
|
Flame | 10 (5–25) |
|
|
|
Electric | 5 (2–10) |
|
|
| Solid
materials | 2 (1–7) |
|
|
|
Steam | 7 (3–15) |
|
|
|
Explosion | 10 (5–56) |
|
|
|
Others | 3 (1–12) |
|
|
| Outcome |
|
|
|
|
Death | 85 (61–94) | −2.690 | 0.007 |
|
Cure | 8 (4–15) |
|
|
| Abandon
treatment | 10 (5–52) |
|
|
|
Improvement | 35 (10–83) |
|
|
Analysis of the causes of death
Clinicians face numerous difficulties when treating
burns. The factors that may affect the survival of burn patients
include widespread complications, patient age, burn area and
tolerance to injury. As determining the sole cause of death for a
patient is difficult, the present study focused on the patients who
succumbed to mortality and aimed to identify what factors might
increase their risk of death.
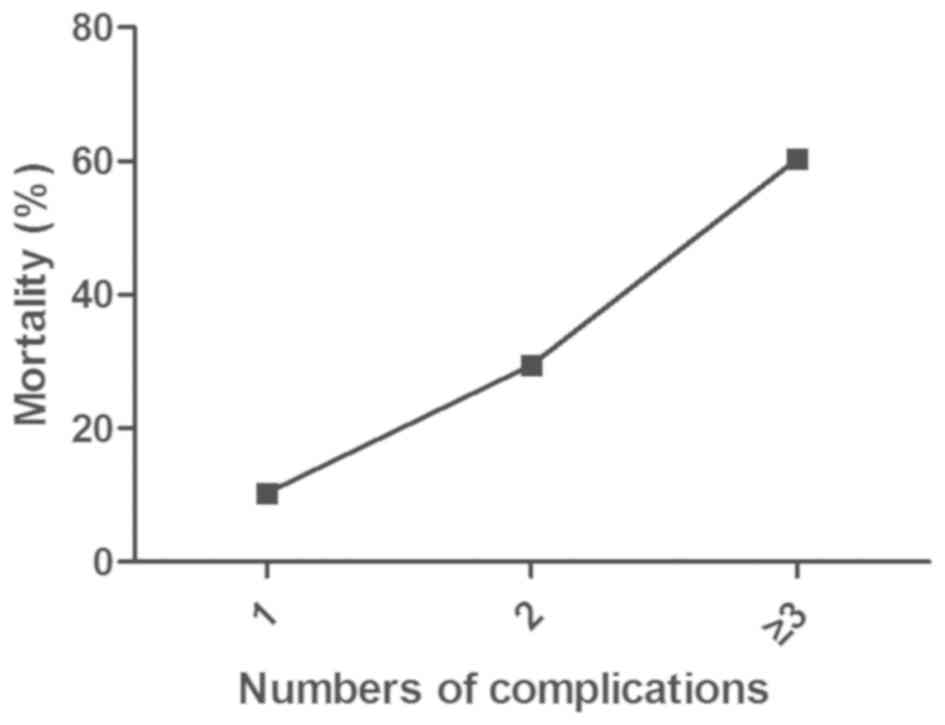
Among all of the cases that resulted in death,
sepsis and organ complications (internal organ failure and
bleeding) were the most common and major causes, although in
certain cases, death occurred due to mild inhalation injury and
shock. Statistical analysis indicated that the patients with more
complications also had higher mortality rates. For instance, 29.41%
of the burn patients with two types of complication died, while the
mortality rate was 60.29% for the burn patients with three types of
complication (Fig. 6). However, with
the improvement in medical treatment and the high quality of
nursing technology, a decline in the number of deaths induced by
sepsis and organ complications has been observed.
Risk factors for death of burn
patients
The three major complications in burn patients are
inhalation injury, shock and infection. In the present study, shock
was selected as an index for multivariate analysis. Infection is
mainly a matter that requires the attention of medical staff. In
addition, certain studies have expressed doubt regarding inhalation
injury as a prognostic factor in burn patients; prior to the
popularization of the fibrotic bronchoscope at our institution, the
diagnosis of inhalation injury mainly relied on the clinician's
experience, this subjective assessment can sometimes be
controversial (11). Therefore,
inhalation injuries as an index affecting the risk of mortality of
burn patients were not included.
First, single-factor analysis was used to screen and
reassign multiple variables associated with death. Subsequently,
the variables were subjected to analysis with multivariate logistic
regression models. Next, the fitting method was used to screen six
risk factors associated with burn-associated death. After sorting
the factors according to their odds ratio, it was revealed that
explosion, shock, age, TBSA and full-thickness burn area were risk
factors for burn injury-associated death (Table VI). As presented in Table VII, patients injured by an
explosion had the highest OR. Therefore, the mortality rate of
these patients is higher (12–14);
indeed, the mortality rate of burn patients injured by explosions
was reported to be 38.46% (15).
With the increased LOS, the patient mortality decreased (regression
coefficient, −0.020; P<0.001).
| Table VI.Univariate logistic regression
analysis of factors associated with mortality. |
Table VI.
Univariate logistic regression
analysis of factors associated with mortality.
| Variables | Regression
coefficient | Standard error | Wald | P-value | OR (95% CI) |
|---|
| Age | 0.659 | 0.121 | 29.456 | <0.001 | 1.932
(1.523–2.451) |
| Explosion | 4.988 | 0.510 | 95.519 | <0.001 | 146.683
(53.943–398.868) |
| Total burn
area | 0.077 | 0.005 | 247.429 | <0.001 | 1.08
(1.07–1.09) |
| Full-thickness burn
area | 0.080 | 0.004 | 325.271 | <0.001 | 1.083
(1.074–1.092) |
| LOS | −0.008 | 0.005 | 2.183 | 0.140 | 0.992
(0.982–1.003) |
| Shock | 2.062 | 0.134 | 237.148 | <0.001 | 7.865
(6.049–10.226) |
| Table VII.Multivariate logistic regression
analysis of factors associated with mortality. |
Table VII.
Multivariate logistic regression
analysis of factors associated with mortality.
| Variables | Regression
coefficient | Standard error | Wald | P-value | OR (95% CI) |
|---|
| Age | 0.530 | 0.181 | 8.530 | 0.003 | 1.699
(1.190–2.424) |
| Explosion | 2.835 | 0.751 | 14.264 | <0.001 | 17.033
(3.911–74.182) |
| Total burn
area | 0.046 | 0.008 | 31.242 | <0.001 | 1.047
(1.030–1.064) |
| Full-thickness burn
area | 0.033 | 0.009 | 12.456 | <0.001 | 1.034
(1.015–1.053) |
| LOS | −0.020 | 0.005 | 13.737 | <0.001 | 0.980
(0.970–0.991) |
| Shock | 0.920 | 0.185 | 24.638 | <0.001 | 2.509
(1.745–3.609) |
Discussion
There are certain limitations of the present study.
For example, the protocol did not assess the degree of the burns.
Secondly the study only analyzed a single burn treatment center,
thus the analysis results may only represent the situation of burns
in a certain area. Whether the findings can be popularized and used
nationwide remains to be discussed.
Retrospective analysis of patients' medical records
from a hospital's database may not only provide summaries to
improve the treatment technology, but also a reference for the
formulation of burn prevention strategies in the future. Of note,
the present study indicated that the number of male burn patients
was higher than that of females, which may be due to differences
between male and female occupations and activities. Therefore, when
formulating burn prevention strategies, age factors should also be
distinguished. After 2 years of age, children begin to attend early
childhood classes and kindergartens, and teachers should perform
burn prevention education as a strategy to reduce the number of
burn injuries. Furthermore, the present study indicated that the
proportion of burn patients in the 25–49 year-old group was higher
than the other four groups, perhaps due to the greater exposure of
these people to certain heat sources and the resulting increase in
the probability of contracting burn injuries, whereas the number of
children with scalds was much higher, and therefore, enforcement of
post-school safety education is particularly important. In
addition, a risk factor analysis may provide guidance for clinical
treatment (16).
In the present study, statistical analysis of the
clinical data suggested that the patients hospitalized at Southwest
Hospital (Chongqing, China) mostly lived in Chongqing and Sichuan
province of China. Chongqing is also known as the ‘mountain city’;
the resident population is mainly composed of individuals native to
this area. Previous epidemiological studies on burn injuries in
southwest China, which has unique climatic characteristics, are
relatively rare. The Burn Research Institute of Southwest Hospital
(Chongqing, China) is the largest burn treatment center in
southwest China and has treated a large number of cases that
basically reflect the epidemiological characteristics of burn
patients in this area (8,17). Therefore, the present study provided
an epidemiological analysis of inpatients with burns in southwest
China treated from 2009 to 2016 in order to provide suggestions for
the further improvement in the treatment as well as the prevention
of burns.
With increases in the TBSA, complications were more
serious, and the treatment difficulty and the mortality rate
gradually increased. Among all of the inpatients treated from 2009
to 2016, the mortality rate was 0.7%, which indicated a significant
decline compared with that of mortality rates reported previously
(18). With the increase of years,
the number of severely burned patients exhibited a downward trend.
This result suggests that with recent improvements in burn
treatment technology and in the meticulous care of burn patients,
the effect of treatment and the overall survival rate have
improved. Simultaneously, due to the popularization of knowledge
about burns and first-aid techniques, intervention (e.g. cooling)
may occur in a more timely manner, leading to a reduction in the
severity of burns and the mortality rate.
The mortality of hospitalized burn patients in
developing countries, except China, is inconsistent, but overall,
it is significantly higher than that in developed countries.
Statistics indicate that the fatality rate of hospitalized burn
patients ranges from 25.9–43.9% in Iran to 28.4% in Kuwait, 33.5%
in Turkey, 27% in Sri Lanka, 7.4% in Saudi Arabia, 16% in
Afghanistan, 19.7% in India and 62% in Pakistan (19,20).
According to recent statistics from a Turkish study, the overall
fatality rate of 2,713 burn patients admitted to their unit was
only 0.9% (19). In 2000, the
burn-associated mortalities was ~1.36/10 million for males and
1.28/10 million for females (20).
Differences in mortality of burn patients based on gender were
observed due to males and females having significantly different
burn tolerances. More importantly, men are more commonly exposed to
heat sources than women, and men engage in more dangerous
occupations and tend to be less cautious, suggesting that gender is
a factor that accounts for burns (21).
Analysis of the causes of the burn injuries revealed
that the majority of injuries were caused by different types of
flame burns and hot liquids or vapor (~40%), followed by chemical
burns (liquefied gas explosion); these results are similar to those
of a previous study (22). Patients
aged <15 years may have experienced burns mostly due to their
curious behavior and poor self-control, or due to the negligence of
adults. With the increase in age, the number of patients with burn
injuries decreased, likely due to the growing awareness of the risk
of burns. In addition, scalds, which accounted for the largest
proportion of burns in this age group, mainly resulted from hot
liquids, including hot water, rice porridge and soup (23). Although the incidence rate was high
for children, the mortality rate was relatively low. Patients who
died of burns were mostly aged 18–59 years, while children and
elderly patients less frequently contracted deadly burns. This
result may have been due to the fact that individuals aged 18–59
years are more likely to encounter complex environments with an
increased risk of being burned. Therefore, the majority of severe
burn patients included young adults and middle-aged individuals,
and the mortality rate was higher in the young and middle-aged
group than that in children and elderly individuals (22).
The present results indicated that children are a
major high-risk group in terms of severe burns, which is similar to
previous results regarding severe burns in Europe (24). Children with poor self-protection
ability and insufficient protection provided by caregivers
frequently suffer burns, which should attract widespread attention.
Children mainly suffer scalding burns from hot liquids, including
hot water, porridge or soup due to curiosity and a poor
self-control ability regarding touching objects of interest.
Furthermore, the group of 31–50 year-old males with burns comprised
a large risk group due to their complex daily living and working
environment, which may have increased the possibility of
contracting burns. With the increase in age, particularly for
middle-aged patients, the function of tissues and organs of the
whole body gradually decreased. When the TBSA was <50%, more
burn patients affected and fewer deaths were noted. When the TBSA
was >50%, the risk of poor outcome was higher. Furthermore, when
complications were present, the proportion of deaths was
significantly increased, indicating that the methods used to treat
patients with a large TBSA or large full-thickness burn area
require to be improved (22).
According to the cause of injury analysis, the major
causes of burns were flames and hot liquids (~69%), followed by
electricity, chemical burns and explosions; these results were
similar to those reported by previous epidemiological studies
(25). The incidence of burns was
increased in Spring and Summer; one possible reason for this is
that thin clothes are worn in the warm weather associated with
these seasons, and the cooling time for scalds solutions is
prolonged, which may lead to more exposure and a larger burn area
after contact with heat and flames. Through further analysis of the
causes of burn incidents, we found that more mosquitoes are present
in mainland China in the Summer, and mosquito repellent incense is
commonly used to repel mosquitoes, which may accidentally ignite
clothing, furniture and electrical equipment, and eventually lead
to the occurrence of burns.
As an active advocate for the prevention of burns
and contributor to the advancement of burn treatments, China has
published a similar epidemiological analysis of burn patients to
that provided by the present study (26). However, the present study is
different from the previous one and has provided novel insight into
the epidemiology of burn injury and the efficacy of burn wound
management. First of all, the present study contains more data,
leading to higher statistical power and allowing for more objective
conclusions. Compared with the previous study, further parameters
were analyzed; in addition to a summary and analysis of
clinicopathological patient characteristics, including patient age,
sex, burn area and LOS, the present study also assessed the
influence of shock, inhalation injury and complications on the
outcome. Furthermore, the present study indicated that there was no
statistically significant difference in the causes of burns between
males and females in the group aged 0–1 years, but in the group
aged ≥2 years, there was a statistically significant difference in
the causes of burns between males and females. In addition, the
proportion of burn patients in the 25–49 year-old group was higher
than the other four groups, which may be helpful to formulate
prevention and treatment strategies for burns. In addition,
significant differences in the TBSA were identified between
patients of different ages, which may also provide clues for
developing a strategy to prevent burns. At last, in the analysis of
risk factors, it was revealed that shock was positively associated
with the risk of death of patients with burn injury, while the LOS
was a protective factor for the death of burned patients.
Furthermore, it is indicated that in 2015/16, the LOS was low and
the mortality also, but this was due to different treatment/patient
management. It may be reasonable to state that this association
cannot be fully proven based on the present data due to
inhomogeneous treatment and that this may require elucidation in
the future.
In the present study, the clinical data of burn
patients treated at Southwest Hospital (Chongqing, China) were
retrospectively analyzed. A logistic regression analysis model was
used to identify factors associated with death. Explosion, shock,
age, TBSA and full-thickness burn area were identified as risk
factors for death from a burn. For burn patients after admission,
it is therefore important to actively control and deal with the
above risk-factors to reduce the incidence of burn-associated
mortality. Since the present study is a single burn center study,
it has certain shortcomings. Thus, further studies with a larger
sample size at multiple centers and levels are required in the
future.
According to analyses of the causes of death in
recent years, sepsis, single or multiple organ failure and
inhalation injury remain the three leading causes of death due to
burns. Apart from injuries to the skin or other deeper tissues,
burn patients also suffer from inhalation injuries and pathological
or physiological disorders that may impair the normal function of
organs, which increases the difficulty of clinical treatment
(27). Most burn patients suffer
from mucosal damage, congestion, edema or lung parenchymal damage
due to thermal factors and smoke. In addition, head and neck skin
injuries lead to subcutaneous tissue swelling and pressure
accompanied by mild inhalation injury or shock, which aggravate the
severity of the illness (28). With
the increased understanding of inhalation injury and shock, and the
improvement of prevention and control measures, great progress has
been made in the overall treatment quality, and these injuries are
no longer the direct cause of death due to burns (16). However, these complications may cause
body tissue ischemia, internal disorders and immune dysfunction
resulting in organ failure, which largely hinders the improvement
and recovery of burn patients and may even be life-threatening.
Under such circumstances, vasoactive substances should be
immediately applied to these patients to improve the condition of
visceral organs (29). The airways
and lungs of burn patients are frequently damaged; failure to clear
off exfoliated or necrotic mucosa and secretions may induce severe
lung infection due to pathogenic bacteria commonly present in
hospitals, including Staphylococcus aureus, Pseudomonas
aeruginosa and Escherichia coli. The healing times for
patients with severe burn wounds are prolonged due to their
exposure to the environment, which increases the risk of infection
and threatens the lives of patients (30). Therefore, the reasonable use of
antibiotics as effective anti-infection treatment methods is
important, which is also supported by the results of the present
study. In addition to rescue during the shock period, the focus of
clinical work should include improvement of the treatment of
infection and subsequent complications to reduce the mortality rate
of severe burn patients.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
G-X L and GL conceived the study and provided
guidance regarding the analyses; RZ, WQ, TY and LS collected the
clinical data; YZ sorted and analyzed the data.
Ethics approval and informed consent
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors have no competing interests to
declare.
References
|
1
|
Andrews CJ and Cuttle L: Comparing the
reported burn conditions for different severity burns in porcine
models: A systematic review. Int Wound J. 14:1199–1212. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf
|
|
3
|
Page F, Hamnett N, D'Asta F and Jeffery S:
Epidemiology of U.K. Military Burns 2008–2013. J Burn Care Res.
38:e269–e276. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hashemi SS, Sharhani A, Lotfi B,
Ahmadi-Juibari T, Shaahmadi Z and Aghaei A: A systematic review on
the epidemiology of pediatric burn in Iran. J Burn Care Res.
38:e944–e951. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Emami SA, Motevalian SA, Momeni M and
Karimi H: The epidemiology of geriatric burns in Iran: A national
burn registry-based study. Burns. 42:1128–1132. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Saaiq M: Epidemiology and outcome of
childhood electrical burn injuries at Pakistan Institute of Medical
Sciences Islamabad, Pakistan. J Burn Care Res. 37:e174–e180. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Akhtar MS, Ahmad I, Khurram MF and Kanungo
S: Epidemiology and outcome of chemical burn patients admitted in
burn unit of JNMC hospital, Aligarh Muslim University, Aligarh,
Uttar Pradesh, India: A 5-year experience. J Family Med Prim Care.
142:106–109. 2015. View Article : Google Scholar
|
|
8
|
Wang KA, Sun Y, Wu GS, Wang YR and Xia ZF:
Epidemiology and outcome analysis of hand burns: A 5-year
retrospective review of 378 cases in a burn center in Eastern
China. Burns. 41:1550–1555. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kraenzlin FS, Mushin OP, Ayazi S, Loree J
and Bell DE: Epidemiology and outcomes of auricular burn injuries.
J Burn Care Res. 39:326–331. 2018.PubMed/NCBI
|
|
10
|
Sheppard NN, Hemington-Gorse S, Shelley
OP, Philp B and Dziewulski P: Prognostic scoring systems in burns.
A review. Burns. 37:1288–1295. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kim Y, Kym D, Hur J, Yoon J, Yim H, Cho YS
and Chun W: Does inhalation injury predict mortality in burns
patients or require redefinition? PLoS One. 12:e01851952017.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Feng JY, Chien JY, Kao KC, Tsai CL, Hung
FM, Lin FM, Hu HC, Huang KL, Yu CJ and Yang KY: Predictors of early
onset multiple organ dysfunction in major burn patients with
ventilator support: Experience from a mass casualty explosion. Sci
Rep. 8:109392018. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wang TH, Jhao WS, Yeh YH and Pu C:
Experience of distributing 499 burn casualties of the June 28, 2015
Formosa Color Dust Explosion in Taiwan. Burns. 43:624–631. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Tekin A, Namias N, O'Keeffe T, Pizano L,
Lynn M, Prater-Varas R, Quintana OD, Borges L, Ishii M, Lee S, et
al: A burn mass casualty event due to boiler room explosion on a
cruise ship: Preparedness and outcomes. Am Surg. 71:210–215.
2005.PubMed/NCBI
|
|
15
|
Zhang YH, Guo GH, Shen GL, Han W, Zhao XY,
Lin W, Huang CH, Xu J, Fan SW and Qian HG: Analysis on treatment of
extremely severe burn patients with severe inhalation injury in
August 2nd Kunshan factory aluminum dust explosion accident.
Zhonghua Shao Shang Za Zhi. 34:455–458. 2018.(In Chinese).
PubMed/NCBI
|
|
16
|
Schaefer TJ and Nunez Lopez O: Burns,
resuscitation and management, treasure Island (FL). StatPearls
Publishing; 2018, 01
|
|
17
|
Ho WS and Ying SY: An epidemiological
study of 1063 hospitalized burn patients in a tertiary burns centre
in Hong Kong. Burns. 27:119–123. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Huang Y, Zhang L, Lian G, Zhan R, Xu R,
Huang Y, Mitra B, Wu J and Luo G: A novel mathematical model to
predict prognosis of burnt patients based on logistic regression
and support vector machine. Burns. 42:291–299. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Albayrak Y, Temiz A, Albayrak A, Peksöz R,
Albayrak F and Tanrıkulu Y: A retrospective analysis of 2713
hospitalized burn patients in a burns center in Turkey. Ulus Travma
Acil Cerrahi Derg. 24:25–30. 2018.PubMed/NCBI
|
|
20
|
Lionelli GT, Pickus EJ, Beckum OK,
Decoursey RL and Korentager RA: A three decade analysis of factors
affecting burn mortality in the elderly. Burns. 31:958–963. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ederer IA, Hacker S, Sternat N, Waldmann
A, Salameh O, Radtke C and Pauzenberger R: Gender has no influence
on mortality after burn injuries: A 20-year single center study
with 839 patients. Burns. Aug 28–2018.(Epub ahead of print).
PubMed/NCBI
|
|
22
|
Cheng WF, Zhao DX, Shen ZA, Zhang HY, Tu
JJ, Yuan ZQ, Duan P and Song GD: An epidemiological investigation
of pediatric patients under 14 with large area burns: A multicenter
study. Zhonghua Yi Xue Za Zhi. 97:462–467. 2017.(In Chinese).
PubMed/NCBI
|
|
23
|
Hussain A and Dunn K: Burn related
mortality in greater manchester: 11-year review of regional
coronial department data. Burns. 41:225–234. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Dĕdovic Z, Brychta P, Koupilová I and
Suchánek I: Epidemiology of childhood burns at the burn centre in
brno, Czech Republic. Burns. 22:125–129. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Liu HF, Zhang F and Lineaweaver WC:
History and advancement of burn treatments. Ann Plast Surg. 78 (2
Suppl 1):S2–S8. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Li H, Yao Z, Tan J, Zhou J, Li Y, Wu J and
Luo G: Epidemiology and outcome analysis of 6325 burn patients: A
fve-year retrospective study in a major burn center in Southwest
China. Sci Rep. 7:460662017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Hettiaratchy S and Dziewulski P: ABC of
burns: Pathophysiology and types of burns. BMJ. 328:1427–1429.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Schaefer T and Burns NLO: Resuscitation
and management. 2017.
|
|
29
|
Klein MB, Hayden D, Elson C, Nathens AB,
Gamelli RL, Gibran NS, Herndon DN, Arnoldo B, Silver G, Schoenfeld
D and Tompkins RG: The association between fluid administration and
outcome following major burn: A multicenter study. Ann Surg.
245:622–628. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Toussaint J and Singer AJ: The evaluation
and management of thermal injuries: 2014 update. Clin Exp Emerg
Med. 1:8–18. 2014. View Article : Google Scholar : PubMed/NCBI
|