Introduction
Myocarditis is a severe myocardial injury, and the
dysfunction of cardiac electrical pathway caused by myocarditis is
also one of the major causes of sudden death in young adults
(1). In the early stage of the
disease, patients only suffer from chest distress and palpitation,
so it is often ignored by them. Besides, the diagnosis of
non-specific symptoms is difficult, so the optimal treatment
opportunity is often missed (2).
Currently, the pathogenesis of myocarditis remains unclear in
clinic. Myocarditis can be caused by a variety of factors, and it
is characterized by acute onset, rapid progression, and even death
in severe cases. Therefore, the early diagnosis of myocarditis
plays a key role in clinical treatment and prevention (3).
It is very difficult to diagnose myocarditis, and
the optimal means of diagnosing the type of myocarditis and
determining its cause is an endomyocardial pathological biopsy.
However, there is psychological repellence in patients due to the
invasive examination and complications (4). C-reactive protein (CRP) is the most
commonly-used acute-phase response index in clinic, which is
involved in multiple stress responses and serves as an important
index for the diagnosis of cardiovascular and cerebrovascular
diseases (5). Hypersensitive CRP
(hs-CRP) is not affected by diet, time and corticosteroid therapy,
which can reflect the severity of cardiovascular and
cerebrovascular injury in patients more quickly and effectively
(6). Blood lactic acid (LAC) is a
product of anaerobic glycolysis closely related to the metabolism
and movement, which cannot only detect whether there are disorders
in the respiratory system and circulatory system in human body, but
also reflect the severity of disease (7). Myoglobin (Mb) is a kind of protein for
cell storage and oxygen distribution in mammals, and serves as an
important index for myocardial and skeletal muscle injury (8). However, hs-CRP and Mb are non-specific
diagnostic indexes, so the single detection has no high diagnostic
value in myocarditis. The combined detection can provide more
complete indexes for clinicians and high reference value in the
diagnosis of myocarditis, so it can be used as an effective means
for the early diagnosis and determination of risk factors for
prognosis of patients with myocarditis (9). At present, there are few studies on the
diagnosis of myocarditis via combined detection of hs-CRP, LAC and
Mb. In this study, the expression levels of hs-CRP, LAC and Mb in
patients with myocarditis were studied, and the coincidence rate,
sensitivity and specificity of single detection and combined
detection of hs-CRP, LAC and Mb in the diagnosis of myocarditis
were analyzed, so as to determine whether the single detection and
combined detection of hs-CRP, LAC and Mb can be used as diagnostic
methods for myocarditis, and provide efficient and reliable
references for the clinical treatment of patients with myocarditis
in the future.
Patients and methods
Data of patients
A total of 107 patients with suspected myocarditis
treated in the Second Nanning People's Hospital (Nanning, China)
from January 2015 to December 2017 were selected, of whom 81
patients diagnosed with myocarditis were enrolled into the research
group, and 26 non-myocarditis individuals were enrolled into the
control group. In the research group, there were 37 females and 44
males aged 22–64 years with an average of 37.91±4.72 years. In the
control group, there were 11 females and 15 males aged 19–63 years
with an average of 41.17±4.38 years. Inclusion criteria were:
patients diagnosed with suspected myocarditis via
electrocardiography, echocardiography and X-ray examination,
patients with complete data, patients aged >18 years, and
patients who did not receive relevant treatments before admission.
Exclusion criteria were: patients with other basic heart disease,
pregnant or lactating patients, patients with other severe diseases
or tumors, patients who were unwilling to undergo endomyocardial
biopsy to diagnose myocarditis, or patients with communication or
cognitive disorders.
This study was approved by the Ethics Committee of
The Second Nanning People's Hospital. All the patients and their
families signed an informed consent and cooperated with medical
workers in relevant diagnoses and treatments.
Methods and equipment
Fasting venous blood was drawn from all patients to
detect hs-CRP, LAC and Mb, and their levels were compared and
analyzed between the two groups. After fasting for 12 h, venous
blood was taken, placed at room temperature for 30 min and
centrifuged at 2,800 × g for 5 min at 20°C using a centrifugal
machine (Beijing TideRadar Technology Co., Ltd.) to separate the
serum. The hs-CRP kit was purchased from Shanghai Fanke
Biotechnology Co., Ltd. (art. no. GD-XS3103), and hs-CRP was
detected via immunoturbidimetry using the XL full-automatic
biochemical analyzer (Shanghai Yuyan Instruments Co., Ltd.). The
LAC kit was purchased from Shanghai Yubo Biological Technology Co.,
Ltd. (art. no. YB-60026), and LAC was detected via
spectrophotometry using the XL full-automatic biochemical analyzer.
The Mb kit was purchased from Shanghai Xinfan Biotechnology Co.,
Ltd. (art. no. XFSH20581), and Mb was detected via
chemiluminescence using the XL full-automatic biochemical
analyzer.
Diagnostic criteria
According to relevant literature (9), the criteria in single detection in the
diagnosis of myocarditis are as follows: hs-CRP >10 mg/l, LAC
>100 mg/l, and Mb>80 µg/l. The criteria in combined detection
in the diagnosis of myocarditis are as follows: hs-CRP, LAC and Mb
levels are higher than the threshold value.
Statistical analysis
SPSS 18.1 (Beijing ND Times Technology Co., Ltd.)
software system was used for the statistical analysis. The basic
enumeration data of patients were expressed as percentage (%), and
Chi-square test was adopted. The expression levels of hs-CRP, LAC
and Mb were expressed as mean ± standard deviation, and t-test was
used for the difference between the two groups. P<0.05 was
considered to indicate a statistically significant difference.
Results
Comparison of clinical data of
patients
To make the experimental results accurate and
reliable, the sex, age, smoking status, alcohol consumption, chest
distress, palpitation, angina and dyspnea were compared between the
two groups, and it was found that there were no significant
differences (P>0.05), proving that patients in both groups were
comparable. The basic data of patients are shown in Table I.
 | Table I.Basic data of patients in the research
and control groups [n (%)]. |
Table I.
Basic data of patients in the research
and control groups [n (%)].
| Characteristics | Research group
(n=81) | Control group
(n=26) | χ2
value | P-value |
|---|
| Sex |
|
| 0.090 | 0.764 |
| Male | 44 (54.32) | 15 (57.69) |
|
|
|
Female | 37 (45.68) | 11 (42.31) |
|
|
| Age (years) |
|
| 0.104 | 0.747 |
|
<45 | 63 (77.78) | 21 (80.77) |
|
|
| ≥45 | 18 (22.22) | 5
(19.23) |
|
|
| Smoking status |
|
| 0.363 | 0.547 |
| Yes | 58 (71.60) | 17 (65.38) |
|
|
| No | 23 (28.40) | 9
(34.62) |
|
|
| Alcohol
consumption |
|
| 0.060 | 0.806 |
| Yes | 52 (64.20) | 16 (61.54) |
|
|
| No | 29 (35.80) | 10 (38.46) |
|
|
| Chest distress |
|
| 0.051 | 0.822 |
| Yes | 64 (79.01) | 20 (76.92) |
|
|
| No | 17 (20.99) | 6
(23.08) |
|
|
| Palpitation |
|
| 0.509 | 0.476 |
| Yes | 53 (65.43) | 15 (57.69) |
|
|
| No | 28 (34.57) | 11 (42.31) |
|
|
| Angina |
|
| 0.359 | 0.549 |
| Yes | 49 (60.49) | 14 (53.85) |
|
|
| No | 32 (39.51) | 12 (46.15) |
|
|
| Dyspnea |
|
| 0.708 | 0.400 |
| Yes | 57 (70.37) | 16 (61.54) |
|
|
| No | 24 (29.63) | 10 (38.46) |
|
|
| Pathological
type |
|
| – | – |
| Viral
myocarditis | 36 (44.44) | – |
|
|
| Bacterial
myocarditis | 15 (18.52) | – |
|
|
| Immune
response myocarditis | 12 (14.81) | – |
|
|
|
Idiopathic myocarditis | 18 (22.22) | – |
|
|
Comparison of expression levels of
hs-CRP, LAC and Mb between the two groups
The expression levels of hs-CRP, LAC and Mb in the
research group were all significantly higher than those in the
control group (10.79±1.63 mg/l vs. 9.67±1.22 mg/l, 106.24±14.08
mg/l vs. 98.15±11.43 mg/l, 82.31±7.15 µg/l vs. 77.87±5.54 mg/l),
and there were statistically significant differences (t=3.222,
2.659 and 3.372, P=0.002, 0.009 and 0.001, respectively) (Table II).
| Table II.Comparisons of expression levels of
hs-CRP, LAC and Mb between the two groups. |
Table II.
Comparisons of expression levels of
hs-CRP, LAC and Mb between the two groups.
| Factors | Research group
(n=81) | Control group
(n=26) | t value | P-value |
|---|
| hs-CRP (mg/l) | 10.79±1.63 | 9.67±1.22 | 3.222 | 0.002 |
| LAC (mg/l) | 106.24±14.08 | 98.15±11.43 | 2.659 | 0.009 |
| Mb (µg/l) | 82.31±7.15 | 77.87±5.54 | 3.372 | 0.001 |
Effectiveness analysis of single and
combined detection by hs-CRP, LAC and Mb in the diagnosis of
myocarditis
There were 107 patients with suspected myocarditis,
including 81 patients pathologically diagnosed with myocarditis and
26 non-myocarditis individuals. There were, respectively, 47, 51
and 56 cases of myocarditis diagnosed in the single detection by
hs-CRP, LAC and Mb and there were 72 cases of myocarditis diagnosed
in the combined detection. Respectively 42, 44 and 52 cases were
correctly diagnosed in the single detection by hs-CRP, LAC and Mb
(Table III–VI).
| Table III.Effectiveness of single detection by
hs-CRP. |
Table III.
Effectiveness of single detection by
hs-CRP.
| Factors | Pathological results
(+) | Pathological results
(−) | Total |
|---|
| hs-CRP diagnosis
(+) | 42 | 5 | 47 |
| hs-CRP diagnosis
(−) | 39 | 21 | 60 |
| Total | 81 | 26 | 107 |
| Table VI.Effectiveness of combined
detection. |
Table VI.
Effectiveness of combined
detection.
| Factors | Pathological
results (+) | Pathological
results (−) | Total |
|---|
| Combined diagnosis
(+) | 64 | 8 | 72 |
| Combined diagnosis
(−) | 17 | 18 | 35 |
| Total | 81 | 26 | 107 |
Analysis of coincidence rate,
sensitivity and specificity of single and combined detection by
hs-CRP, LAC and Mb in the diagnosis of myocarditis
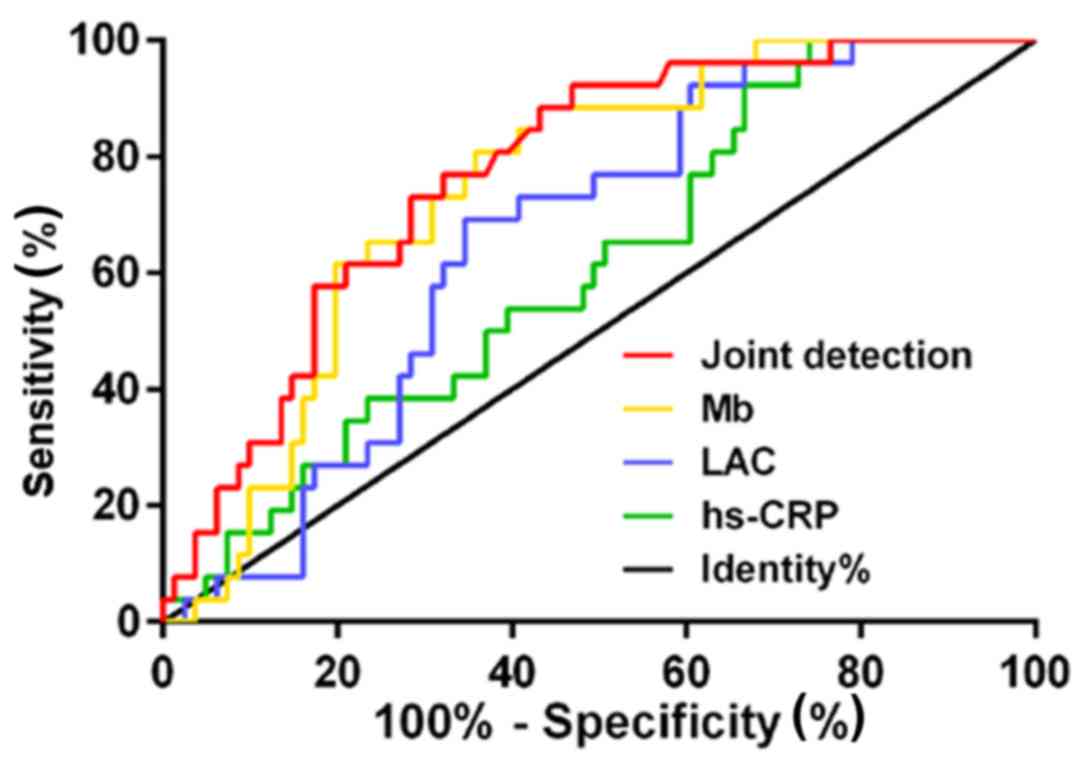
According to the receiver operating characteristic
(ROC) curve, the area under the curve (AUC), coincidence rate as
well as sensitivity and specificity, respectively, in the diagnosis
of myocarditis were 0.610 (95% CI: 0.495–0.725), 58.88, 51.85 and
80.77% for hs-CRP, 0.657 (95% CI: 0.551–0.763), 58.88, 54.32 and
73.08% for LAC, 0.747 (95% CI: 0.651–0.843), 69.16, 64.20 and
84.62% for Mb, and 0.773 (95% CI: 0.680–0.867), 76.64, 79.01 and
69.23% for combined detection (Table
VII and Fig. 1).
| Table VII.Analysis of coincidence rate,
sensitivity and specificity of single and combined detection by
hs-CRP, LAC and Mb in the diagnosis of myocarditis. |
Table VII.
Analysis of coincidence rate,
sensitivity and specificity of single and combined detection by
hs-CRP, LAC and Mb in the diagnosis of myocarditis.
| Factors | hs-CRP (%) | LAC (%) | Mb (%) | Combined detection
(%) |
|---|
| Diagnostic
coincidence rate | 58.88 | 58.88 | 69.16 | 76.64 |
| Sensitivity | 51.85 | 54.32 | 64.20 | 79.01 |
| Specificity | 80.77 | 73.08 | 84.62 | 69.23 |
Discussion
Myocarditis can cause severe hemodynamic damage. The
proportion of myocarditis is up to 13% in the cause of sudden death
in adolescents, and its global incidence rate is 18.27/100,000 and
prevalence rate is 21.83/100,000 (10). Pathogenesis of myocarditis has been
studied by a large number of scholars, but its clinical
manifestations are non-specific and diverse, and dependent on the
range and severity of lesion due to the different etiology, and
there may even be no clinical symptoms, making it one of the most
challenging cardiovascular diseases (11). Moreover, it is hard to conduct
multi-center large-scale experiments due to the limited incidence
rate, so myocarditis is a major challenge in the medical field
(12).
In this study, a total of 107 patients with
suspected myocarditis were retrospectively analyzed, including 81
patients pathologically diagnosed with myocarditis and 26
non-myocarditis patients. The levels of hs-CRP, LAC and Mb were
compared and analyzed between the two groups of patients, and the
coincidence rate, sensitivity and specificity of single detection
and combined detection by hs-CRP, LAC and Mb in the diagnosis of
myocarditis were also compared. The expression level of hs-CRP in
the research group was significantly higher than that in the
control group (10.79±1.63 mg/l vs. 9.67±1.22 mg/l), and there was a
statistically significant difference. There were 47 cases of
myocarditis diagnosed in the single detection by hs-CRP, and 42
cases were correctly diagnosed. According to the ROC curve, AUC,
coincidence rate, sensitivity and specificity in the diagnosis of
myocarditis, respectively, were 0.610 (95% CI: 0.495–0.725), 58.88,
51.85 and 80.77% for hs-CRP. hs-CRP is an acute-phase reactive
protein synthesized by the liver, and the changes in its expression
level can rapidly reflect the subtle changes in the circulatory
system. Besides, it is less affected by anti-inflammatory and
hormone drugs, which can reflect the severity of cardiovascular
injury more sensitively (13).
However, hs-CRP is increased in acute myocardial infarction and
stress response, so it is not a specific diagnostic index (14).
Gölbasi et al (15) reported that the level of hs-CRP in
patients with acute myocarditis is increased, and the ST-T changes
in more than 2 out of 4 leads (EKGI, II, aVF and V5) indicate the
increased risk of myocarditis. The expression level of LAC in the
research group was significantly higher than that in the control
group (106.24±14.08 mg/l vs. 98.15±11.43 mg/l), and there was a
statistically significant difference. There were 51 cases of
myocarditis diagnosed in a single detection of LAC, and 44 cases
were correctly diagnosed. According to the ROC curve, AUC,
coincidence rate as well as sensitivity and specificity in the
diagnosis of myocarditis, respectively, were 0.657 (95% CI:
0.551–0.763), 58.88, 54.32 and 73.08% for LAC. In patients with
myocarditis, a large number of catecholamines are secreted due to
the stimulation of inflammatory factors, thus leading to the
increased level of fasting blood glucose. Then the high-level
fasting blood glucose promotes anaerobic glycolysis, and a large
amount of LAC is produced in the body. The increase in LAC in
patients can suggest disorders in the respiratory or circulatory
system. However, LAC can be easily affected by blood glucose, so it
is not specific in the diagnosis of myocarditis (16). The expression level of Mb in the
research group was obviously higher than that in the control group
(82.31±7.15 µg/l vs. 77.87±5.54 mg/l), and the difference was
statistically significant. There were 56 cases of myocarditis
diagnosed in the single detection of Mb, and 52 cases were
correctly diagnosed. According to the ROC curve, AUC, coincidence
rate as well as sensitivity and specificity in the diagnosis of
myocarditis, respectively, were 0.747 (95% CI: 0.651–0.843), 69.16,
64.20 and 84.62% for Mb. Mb mainly exists in the striated muscle,
which is a polypeptide chain widely distributed in myocardial and
skeletal muscle tissues (17). As a
small-molecule protein containing heme, Mb can display the tissue
hypoperfusion and oxygenation dysfunction, so its level increases
in the case of shortness of breath or chest pain in patients with
myocarditis (18). Related studies
(19) have demonstrated that if
patients suffer from severe myocardial damage or ventricular
systolic dysfunction, the level of Mb is increased, which has a
significantly positive correlation with the degree of degeneration
or necrosis of myocardial cells. The above research results are
similar to this study, proving these findings. There were 72 cases
of myocarditis diagnosed in the combined detection, and 64 cases
were correctly diagnosed. According to the ROC curve, AUC,
coincidence rate as well as sensitivity and specificity in the
diagnosis of myocarditis, respectively, were 0.773 (95% CI:
0.680–0.867), 76.64, 79.01 and 69.23% for combined detection.
hs-CRP, LAC and Mb are commonly-used indexes reflecting the
myocardial damage of patients, as well as reference indexes in the
diagnosis of myocarditis (20).
According to literature (21), the
peaks of hs-CRP, LAC and Mb indicate severe myocardial damage. Berg
et al (22) conducted a
5-year follow-up study on child patients with myocarditis, and
found that hs-CRP, LAC and Mb are risk factors for prognosis of
patients. These research results can prove the conclusion in this
study that the combined detection has high value in the diagnosis
of myocarditis.
In this experiment, the sample size was small due to
the limited medical resources in the hospital, so the results may
have certain contingency. Therefore, further studies are needed for
confirmation.
In conclusion, hs-CRP, LAC and Mb are highly
expressed in the serum of patients with myocarditis, and their
combined detection has guiding significance for the prevention and
treatment of myocarditis.
Acknowledgements
Not applicable.
Funding
This study was supported by Science Foundation of
Guangxi Medical University in Nanning (GXMUYSF201536).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YaL wrote the manuscript and was also involved in
the conception and design of this study. XH and YuL detected and
analyzed hs-CRP, LAC and Mb levels. DL and JZ collected and
analyzed the general data of patients. LY and YaL were responsible
for the statistical analysis. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
The Second Nanning People's Hospital (Nanning, China). Signed
informed consents were obtained from the patients or guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Dominguez F, Kühl U, Pieske B,
Garcia-Pavia P and Tschöpe C: Update on myocarditis and
inflammatory cardiomyopathy: Reemergence of endomyocardial biopsy.
Rev Esp Cardiol (Engl Ed). 69:178–187. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bowles NE and Towbin JA: Molecular aspects
of myocarditis. Curr Opin Cardiol. 13:179–184. 1998.PubMed/NCBI
|
|
3
|
Heymans S, Eriksson U, Lehtonen J and
Cooper LT Jr: The quest for new approaches in myocarditis and
inflammatory cardiomyopathy. J Am Coll Cardiol. 68:2348–2364. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Johnson DB, Balko JM, Compton ML, Chalkias
S, Gorham J, Xu Y, Hicks M, Puzanov I, Alexander MR, Bloomer TL, et
al: Fulminant myocarditis with combination immune checkpoint
blockade. N Engl J Med. 375:1749–1755. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Guo JG: Detection of cardiac troponin and
high-sensitivity C reactive protein in children with viral
myocarditis. Nan Fang Yi Ke Da Xue Xue Bao. 28:1076–1077. 2008.(In
Chinese). PubMed/NCBI
|
|
6
|
Sata N, Hamada N, Horinouchi T, Amitani S,
Yamashita T, Moriyama Y and Miyahara K: C-reactive protein and
atrial fibrillation. Is inflammation a consequence or a cause of
atrial fibrillation? Jpn Heart J. 45:441–445. 2004.PubMed/NCBI
|
|
7
|
Garlotta D: A literature review of
poly(lactic acid). J Polym Environ. 9:63–84. 2001. View Article : Google Scholar
|
|
8
|
Kottwitz J, Berg J, Baltensperger N,
Elhassan M, Kissel CK, Lovrinovic M, Patriki D, Scherff F, Schmied
C, Templin C, et al: Myoglobin is a strong predictor of extent of
late gadolinium enhancement on cardiac magnetic resonance imaging
in patients with acute myocarditis. Circulation. 136 (Suppl
1):A151562017.
|
|
9
|
Huang GY, Zhang LY, Long-Le MA and Wang
LX: Clinical characteristics and risk factors for peripartum
cardiomyopathy. Afr Health Sci. 12:26–31. 2012.PubMed/NCBI
|
|
10
|
Sinagra G, Anzini M, Pereira NL, Bussani
R, Finocchiaro G, Bartunek J and Merlo M: Myocarditis in clinical
practice. Mayo Clin Proc. 91:1256–1266. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Rose NR: Viral myocarditis. Curr Opin
Rheumatol. 28:383–389. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Huber SA: Viral myocarditis and dilated
cardiomyopathy: etiology and pathogenesis. Curr Pharm Des.
22:408–426. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Henningsen KM, Nilsson B, Bruunsgaard H,
Chen X, Pedersen BK and Svendsen JH: Prognostic impact of hs-CRP
and IL-6 in patients undergoing radiofrequency catheter ablation
for atrial fibrillation. Scand Cardiovasc J. 43:285–291. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Fett JD: Inflammation and virus in dilated
cardiomyopathy as indicated by endomyocardial biopsy. Int J
Cardiol. 112:125–126. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gölbasi Z, Uçar O, Keles T, Sahin A, Cagli
K, Camsari A, Diker E and Aydogdu S: Increased levels of high
sensitive C-reactive protein in patients with chronic rheumatic
valve disease: Evidence of ongoing inflammation. Eur J Heart Fail.
4:593–595. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Donald KW, Gloster J, Harris EA, Reeves J
and Harris P: The production of lactic acid during exercise in
normal subjects and in patients with rheumatic heart disease. Am
Heart J. 62:494–510. 1961. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Al Shamkhani W, Ajaz Y, Saeed Jafar N and
Roy Narayanan S: Myocarditis and rhabdomyolysis in a healthy young
man caused by salmonella gastroenteritis. Case Rep Infect Dis.
2015:9549052015.PubMed/NCBI
|
|
18
|
Odum EP and Young EE: Elevated cardiac
troponin I, creatine kinase and myoglobin and their relationship
with cardiovascular risk factors in patients with type 2 diabetes.
Diabetes Metab Syndr. 12:141–145. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Shorie M, Kumar V, Priyanka S and Ganguli
AK: Carbon quantum dots-mediated direct fluorescence assay for the
detection of cardiac marker myoglobin. Curr Sci. 108:1595–1596.
2015.
|
|
20
|
Khan R, Pal M, Kuzikov AV, Bulko T, Suprun
EV and Shumyantseva VV: Impedimetric immunosensor for detection of
cardiovascular disorder risk biomarker. Mater Sci Eng C. 68:52–58.
2016. View Article : Google Scholar
|
|
21
|
Thomas KN, Cotter JD, Williams MJ and van
Rij AM: Diagnosis, incidence, and clinical implications of
perioperative myocardial injury in vascular surgery. Vasc
Endovascular Surg. 50:247–255. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Berg J, Kottwitz J, Baltensperger N,
Kissel CK, Lovrinovic M, Mehra T, Scherff F, Schmied C, Templin C,
Lüscher TF, et al: Cardiac magnetic resonance imaging in
myocarditis reveals persistent disease activity despite
normalization of cardiac enzymes and inflammatory parameters at
3-month follow-up. Circ Heart Fail. 10:102017. View Article : Google Scholar
|