Introduction
Intracerebral hemorrhage (ICH), a non-traumatic and
spontaneous brain parenchymal hemorrhage, has the characteristics
of rapid onset and progression, with a high morbidity and mortality
rates (1,2). Hypertensive intracerebral hemorrhage
(HICH), is a critical disease and clinically common in middle-aged
and elderly people, it is a type of blood circulation disorder that
seriously endangers human health (3,4). The
most serious pathological change in HICH is due to mechanical
damage caused by bleeding and secondary damage to surrounding
tissues, such as cerebral ischemia and edema (5). Lakhan et al (6) suggested that the degree of brain tissue
damage caused by cerebral ischemia and edema after cerebral
hemorrhage was similar to hematoma itself. However, the patients
have a sharp increase of intracranial pressure in a short period of
time causing an extremely high mortality rates, so efficient and
timely treatment is clinically important (7). The current clinical goal of treating
HICH is to remove the hematoma, reduce intracranial pressure,
prevent or reduce the occurrence of secondary lesions after
hemorrhage, and to apply more surgical treatments. However, due to
different factors such as the severity of patients condition,
location of hematoma, volume of hematoma and the extent of damage
to the brain tissue, patients are prone to complications after
surgery. Due to the above issues it has become medically important
(8–10).
In recent years, with the improvement of clinical
technology, the mortality rate after the surgery of HICH has
decreased. However, due to the occurrence of different degrees of
dysfunction in most patients after surgery, it seriously affects
the prognosis and life quality of patients and impacts on both the
patients and their families. Some reports have shown that the
postoperative rehabilitation training has an important effect in
patients with cerebrovascular disease (11,12).
Moreover, according to the report of Li et al (13), active and effective nursing
intervention is an important means of adjuvant treatment of HICH.
It can reduce the disability rate, and improve the patients' life
quality and mental state, which plays an important role in the
clinical treatment of HICH. However, there are only a few reports
on the rehabilitation and nursing interventions for patients after
HICH surgery. Therefore, this study explored the comparison among
patients of routine treatment and routine nursing intervention
after HICH surgery with patients undergoing rehabilitation therapy
and nursing intervention, with an aim to provide reference value
for future clinical HICH treatment.
Patients and methods
Patient information
Retrospective analysis was performed of 78 patients
with severe HICH hematoma evacuation after treatment in Xuzhou No.
1 People's Hospital, Xuzhou Municipal Hospital Affiliated to Xuzhou
Medical University (Xuzhou, China) from March 2014 to July 2017.
Among them, 28 patients who received routine treatment and routine
nursing were regarded as the control group, including 19 cases of
males, 9 cases of females, average age of 68±4.67 years; 27
patients who underwent rehabilitation training based on routine
treatment and routine nursing care were regarded as the
rehabilitation training group, including 19 cases of males, 8 cases
of females, with an average age of 67.54±5.21 years. Twenty-three
patients who underwent rehabilitation training based on routine
treatment and nursing intervention were regarded as nursing
intervention group, including 14 cases of males and 9 cases of
females, with an average age of 69.95±5.06 years. Inclusion
criteria were: Patients diagnosed with HICH, and who underwent
surgery; patients with a bleeding volume between 30–50 ml; complete
medical records; not received treatment in other hospitals.
Exclusion criteria were: Patients who were unwilling to cooperate
with medical treatment; patients who have had hospitalization
transfer; patients with other hemorrhage diseases; patients with
liver, kidney, coagulopathy or other basic severe diseases;
patients with tumors; patients with mental disorders and cognitive
impairment.
All subjects and their families signed an informed
consent and cooperated with medical staff to complete relevant
medical treatment. The study was approved by the Ethics Committee
of Xuzhou No. 1 People's Hospital, Xuzhou Municipal Hospital
Affiliated to Xuzhou Medical University (Xuzhou, China).
Methods of treatment and nursing
care
All the patients in the three groups underwent
routine treatments such as nutritional brain cells, diuresis,
hemostasis, dehydration, and hypotension; both the control group
and rehabilitation group adopted routine nursing care method. On
the basis of a stable condition, rehabilitation training was given
to patients in both the rehabilitation training group and the
nursing intervention group after the cerebral edema gradually
subsided. Also targeted treatment was applied based on individual
dysfunction of the patient, the main treatments are daily life
ability training, bath technology and sports re-learning training.
The main details are as follows: i) Good limb position placement
and joint passive activity training: assisting the patient to
perform appropriate passive exercise during bed rest, take the
method of alternate replacement of supine position, healthy lateral
position, the way to change lateral position and instruct the
patient to turn over on the bed; also focus on how to maintain each
joint position and the functional position, and take passive
exercise in joint activity. ii) Swallowing and speech function
training: assisting the patient in the lateral position, raising
the head of the bed 15–30°, use a syringe to inject warm water from
the corner of the healthy side into the mouth, exercise the
patient's swallowing function; also employ language and hearing
training for aphasia patients. iii) Station, walking and balance
training: Assist patients in standing and gait training according
to the patient's condition. After the patient's muscle strength
reached grade 3 or above, the patient's single leg standing balance
and normal gait training were performed. Practice the above
training 10–20 min/time, 2 times/day.
The nursing intervention group teaches patients
relevant knowledge on the basis of rehabilitation training, and
patiently answers questions and understands the patient's inner
needs. Develop an appropriate psychological guidance according to
different patient characteristics, allow patients to express their
inner depression and anxiety as much as possible, and provide
psychological guidance. Helping patients to exercise dining,
dressing and toileting and improve their self-care ability, reduce
their dependence on psychology and depression. In addition, set up
an activity room in the ward, and improve the entertainment venues
such as TV and music for patients, this helps to reduce their
depression.
Evaluation methods and criteria
The systolic blood pressure, diastolic blood
pressure, and Fugl-Meyer score among the three groups were compared
immediately after surgery (T1), 4 weeks after treatment (T2), and
12 weeks after treatment (T3). During the period of T3, the total
effective rate and adverse reactions (shoulder-hand syndrome,
hemorrhoids, depression) among the three groups of patients were
compared.
Evaluation methods of Fugl-Meyer: the scores were
taken by the same rehabilitation staff, with a total score of 100.
The higher the score, the better the recovery.
Overall efficiency criteria: Significantly
effective: The Fugl-Meyer score for patients during the period of
T3 increased by 91–100% compared with T1, with a 0 degree of
disability. Effective: During the period of T3, Fugl-Meyer score
has increased by 46–90% compared with T1, with a 1–3 degree of
disability. Progressed: Patients during the period of T3,
Fugl-Meyer score has increased by 18–45% compared with T1, with
nothing changed in the degree of disability. Non-effective:
Patients during the period of T3, Fugl-Meyer score has increased
less than 18% compared with T1. Overall efficiency = (significantly
effective number + effective number) / total number of people.
Statistical analysis
SPSS 19.1 [Bo Yi Zhixun (Beijing) Information
Technology Co. Ltd., Beijing, China] software system was applied
for statistical analysis. The enumeration data were expressed as a
percentage [n (%)], the difference between the groups was compared
by Chi-square test. Difference between multiple groups was compared
by ANOVA with LSD post hoc test. The difference between the three
groups was compared by F test. Measurement data was expressed as
mean ± standard deviation. P<0.05 was considered to indicate a
statistically significant difference.
Results
Comparison of clinical data of
patients
In order to make the experimental results accurate
and credible, the patients' sex, age, weight, condition of
psychomotor agitation, pathological changes of small arteries and
hemorrhage location were compared among the three groups, the
difference was not statistically significant (P>0.05). This
indicates that it is comparable among the three groups. Table I shows basic patient clinical
data.
 | Table I.Basic data of patients in the three
groups [n (%)]. |
Table I.
Basic data of patients in the three
groups [n (%)].
| Characteristics | Control group
(n=28) | Rehabilitation
training group n=27) | Nursing intervention
group (n=23) | Chi-square test | P-value |
|---|
| Sex |
|
|
| 0.532 | 0.766 |
| Male | 19 (67.86) | 19 (70.37) | 14 (60.87) |
|
|
|
Female | 9
(32.14) | 8
(29.63) | 9
(39.13) |
|
|
| Age (years) |
|
|
| 0.191 | 0.909 |
| ≤60 | 5
(17.86) | 6
(22.22) | 5
(21.74) |
|
|
|
>60 | 23 (82.14) | 21 (77.78) | 18 (78.26) |
|
|
| Weight (kg) |
|
|
| 0.655 | 0.721 |
| ≤60 | 13 (46.43) | 11 (40.74) | 12 (52.17) |
|
|
|
>60 | 15 (53.57) | 16 (59.26) | 11 (47.83) |
|
|
| Psychomotor
agitation |
|
|
| 1.990 | 0.370 |
| Yes | 4
(14.29) | 8
(29.63) | 6
(26.09) |
|
|
| No | 24 (85.71) | 19 (70.37) | 17 (73.91) |
|
|
| Pathological changes
of small arteries |
|
|
| 1.042 | 0.594 |
|
Glassy | 22 (78.95) | 18 (66.67) | 16 (69.57) |
|
|
|
Fibrous | 6
(21.05) | 9
(33.33) | 7
(30.43) |
|
|
| Hemorrhage
location |
|
|
| 1.659 | 0.798 |
| Basal
ganglia | 18 (64.29) | 14 (51.85) | 11 (47.83) |
|
|
|
Thalamus | 6
(21.43) | 7
(25.93) | 7
(30.43) |
|
|
|
Lobar | 4
(14.29) | 6
(22.22) | 5
(21.74) |
|
|
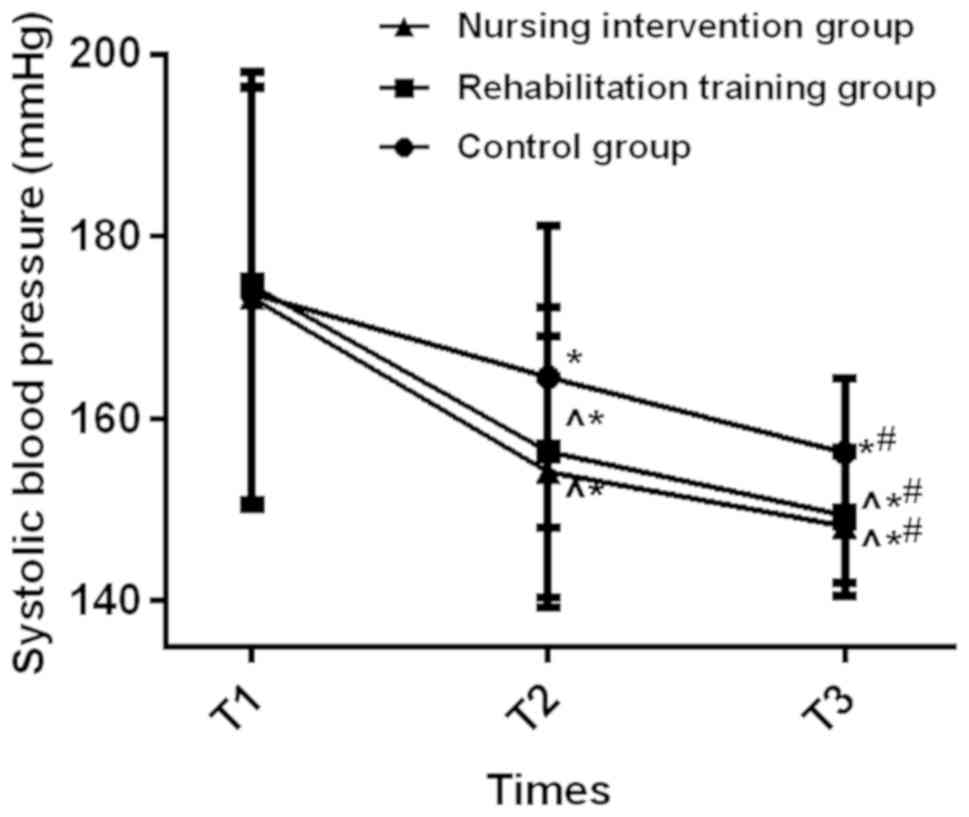
Changes of systolic blood pressure at
T1-T3 in the three groups of patients
The systolic blood pressure at T1, T2, and T3 in the
control group was 173.72±22.61, 164.56±16.57, and 156.25±8.13 mmHg.
The systolic blood pressure at T1, T2 and T3 in the rehabilitation
training group was 174.61±23.54, 156.35±15.94, and 149.36±7.48
mmHg. The systolic blood pressure at T1, T2, and T3 in the nursing
intervention group was 173.27±23.15, 154.16±14.86, and 148.21±7.73
mmHg.
During the period of T1, there was no statistically
significant difference in systolic blood pressure among the three
groups (P>0.050). At T2 and T3, the systolic blood pressure in
both the rehabilitation training group and the nursing intervention
group were lower than the control group, and the difference was
statistically significant (P<0.050). There was no significant
difference in systolic blood pressure between the rehabilitation
training group and the nursing intervention group (P>0.050). The
systolic blood pressure at T3 in the three groups was significantly
lower than T2 and T1, and the systolic blood pressure at T2 was
lower than T1. The difference was statistically significant
(P<0.050) (Fig. 1).
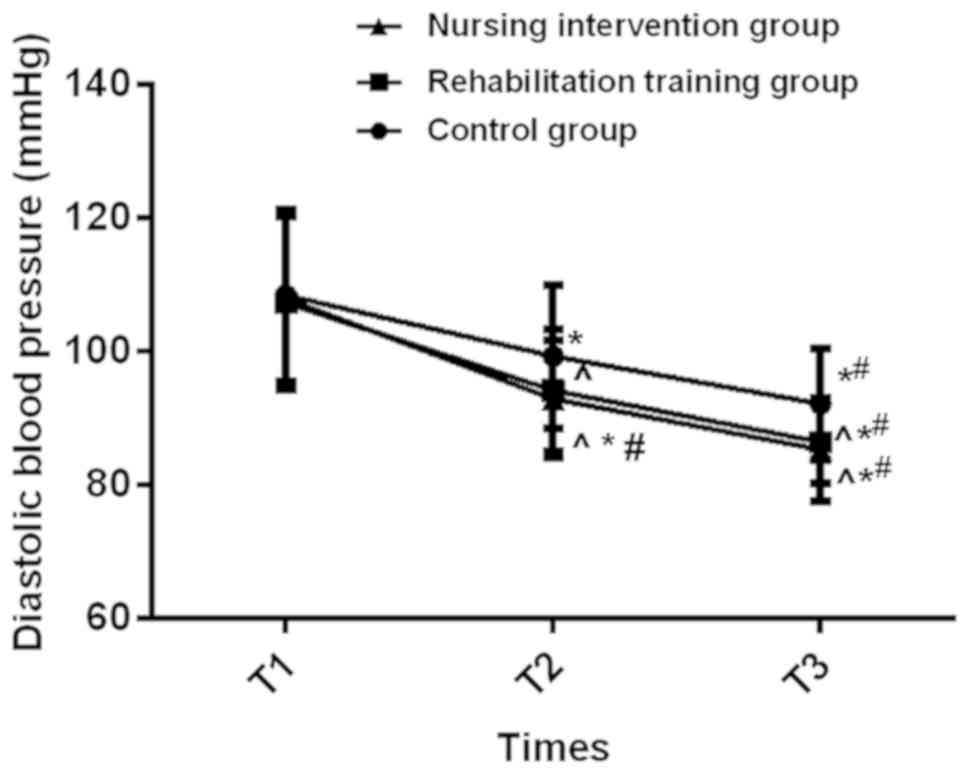
Changes of diastolic blood pressure at
T1-T3 among the three groups of patients
The diastolic blood pressures of T1, T2, and T3 in
the control group were 108.36±12.97, 99.24±10.75, and 92.08±8.36
mmHg. The diastolic blood pressure in the rehabilitation training
group at T1, T2, and T3 was respectively 107.24±13.02, 94.11±9.28,
and 86.35±6.15 mmHg. The diastolic blood pressure at T1, T2, and T3
in the nursing intervention group was 107.82±12.63, 92.86±8.84, and
85.21±7.73 mmHg.
During the period of T1, there was no statistically
significant difference in diastolic blood pressure among the three
groups (P>0.050). During the period of T2 and T3, the diastolic
blood pressure in the rehabilitation training group and the nursing
intervention group were lower than the control group and the
difference was statistically significant (P<0.050). There was no
significant difference in diastolic blood pressure between the
rehabilitation training group and the nursing intervention group
(P>0.050). The diastolic blood pressure at T3 in the three
groups was significantly lower than both T2 and T1. The diastolic
blood pressure at T2 was lower than T1, and the difference was
statistically significant (P<0.050) (Fig. 2).
Fugl-Meyer scores at T1-T3 time points
in the three groups of patients
During the period of T1, there was no significant
difference in Fugl-Meyer score in the three groups (P>0.050).
During the period of T2 and T3, the Fugl-Meyer scores in the
rehabilitation training group and the nursing intervention group
were higher than the control group, the difference was
statistically significant (P<0.050). There was no significant
difference in Fugl-Meyer score between the rehabilitation training
group and the nursing intervention group (P>0.050). The
Fugl-Meyer score at T3 in the three groups was significantly higher
than both T2 and T1, and the Fugl-Meyer score at T2 was higher than
T1. The difference was statistically significant (P<0.050)
(Table II).
| Table II.Comparison of Fugl-Meyer scores at
T1-T3 in the three groups of patients. |
Table II.
Comparison of Fugl-Meyer scores at
T1-T3 in the three groups of patients.
| Item | Control group
(n=28) | Rehabilitation
training group (n=27) | Nursing intervention
group (n=23) | F value | P-value |
|---|
| T1 | 26.83±5.79 | 27.19±5.54 | 27.02±6.11 |
0.027 | 0.974 |
| T2 |
34.17±8.61a |
41.59±9.03a,b |
43.07±8.67a,b |
7.825 | 0.001 |
| T3 |
43.51±8.84a,c |
58.37±10.15a–c |
60.08±10.45a–c | 23.100 | <0.001 |
| F value | 31.600 | 95.030 | 103.600 |
|
|
| P-value | <0.001 | <0.001 | <0.001 |
|
|
Comparison of overall efficiency at T3
among the three groups of patients
The number of significantly-effective, effective,
progressed and non-effective patients in the control group were 13,
8, 5, and 2, respectively. The number of significantly-effective,
effective, progressed and non-effective patients in the
rehabilitation training group was 16, 10, 1 and 0, respectively;
The number of significantly effective, effective, progressed, and
non-effective patients in the nursing intervention group was 15, 7,
1 and 0, respectively.
The total effective rate in the control group was
75.00%, the total effective rate in the rehabilitation training
group was 96.30% and the total effective rate in the nursing
intervention group was 95.65%. The total effective rate in the
rehabilitation training group and the nursing intervention group
was significantly higher than the control group, and the difference
was statistically significant (P<0.050). There was no
significant difference in total effective rate between the
rehabilitation training group and the nursing intervention group
(P>0.050) (Table III).
| Table III.Comparison of total effective rate at
T3 in the three groups of patients. |
Table III.
Comparison of total effective rate at
T3 in the three groups of patients.
| Item | Significantly
effective | Effective | Progressed | Non-effective | Total effective
rate |
|---|
| Control group
(n=28) | 13 (46.43) | 8
(28.57) | 5
(17.86) | 2 (7.14) | 21 (75.00) |
| Rehabilitation
group (n=27) | 16 (59.26) | 10 (37.03) | 1 (3.70) | 0 (0.00) | 26 (96.30) |
| Nursing
intervention group (n=23) | 15 (65.22) | 7
(30.43) | 1 (4.35) | 0 (0.00) | 22 (95.65) |
| Chi-square
test | – | – | – | – | 7.379 |
| P-value | – | – | – | – | 0.025 |
Comparison of adverse reactions at T3
in the three groups of patients
In the control group, the number of patients with
shoulder-hand syndrome, hemorrhoids, and depression was
significantly higher than both the rehabilitation training group
and the nursing intervention group, the difference was
statistically significant (P<0.050). There was no significant
difference in the number of patients with shoulder-hand syndrome
and hemorrhoids in the rehabilitation training group or nursing
intervention group (P>0.050). The number of people with
depression in the rehabilitation training group was significantly
higher than the nursing intervention group, and the difference was
statistically significant (P<0.050) (Table IV).
| Table IV.Comparison of adverse reactions in
the three groups of patients n (%)]. |
Table IV.
Comparison of adverse reactions in
the three groups of patients n (%)].
| Groups | Control group
(n=28) | Rehabilitation
training group (n=27) | Nursing
intervention group (n=23) | Chi-square
test | P-value |
|---|
| Shoulder-hand
syndrome | 21 (75.00) | 3
(11.11)a | 4
(17.39)a | 29.240 | <0.001 |
| Decubitus | 13 (46.43) | 5
(18.52)a | 4
(17.39)a |
7.171 | 0.028 |
| Depression | 23 (82.14) | 14
(51.85)a | 5
(21.74)a,b | 18.600 | <0.001 |
Discussion
According to statistics, in industrialized
countries, cerebrovascular disease is the leading cause of death
among women. Also the second leading cause of death in men,
cerebrovascular disease is also an important cause of cognitive
impairment and dementia (14,15).
HICH is a parenchymal hemorrhage caused by rupture of small
arteries when blood pressure rises suddenly. The incidence of HICH
has increased significantly in recent years. It has a high
disability and mortality rate, the mortality rate is approximately
35–52% (16). HICH is the main cause
of functional disability, most patients with cerebral hemorrhage
have neurological sequelae after treatment, and cannot restore the
same level of daily living activities as before the disease
(17,18). The number of patients with HICH
worldwide is gradually declining due to early control of risk
factors. However, many patients still require a long-term care
after surgery, this has caused a great burden on the patient's
family and society, therefore, early intervention is crucial
(19,20). This study analyzed 78 patients with
severe HICH hematoma evacuation after treatment in Xuzhou No. 1
People's Hospital. The efficacy and adverse reactions of different
postoperative intervention methods were compared to provide
reference for clinical diagnosis and treatment of HICH
patients.
In this study, we found that the systolic blood
pressure, diastolic blood pressure, Fugl-Meyer score, total
effective rate and the number of patients with shoulder-hand
syndrome and decubitus were not statistically significant in either
the rehabilitation training group or the nursing intervention
group. This indicates that there was no significant difference in
the effect of postoperative intervention between the groups.
However, the number of people with depression in the rehabilitation
training group was significantly higher than the nursing
intervention group. Lack of social support, disability and chronic
diseases are the poor prognostic factors for depression, and has
increased the mortality rate in patients (21). Scientific and effective care with
positive and accurate clinical treatment are the key to improving
the prognosis condition and cure rate. Traditional and conventional
nursing models cannot fully adapt to patients in different
situations because of their backward concepts and ways of thinking.
This has caused less than ideal prognosis for patients, especially
in the emotional direction of patients (22). Therefore, we need to be more focused
on the emotional side of HICH patients. Some documentaries have
shown that it is important to let cardiovascular patients know the
relevant knowledge, further supporting our point view (23).
In this study, we also found that patients in the
rehabilitation training group and the nursing intervention group
had undergone rehabilitation training, so the systolic blood
pressure, diastolic blood pressure, and the number of patients with
shoulder-hand syndrome and decubitus were significantly lower than
the control group. However, the Fugl-Meyer score and the overall
effective rate were significantly higher than the control group.
This indicates that each index of the patients who underwent
rehabilitation training after HICH is better than those who did not
undergo rehabilitation training. Some documents have shown that for
patients with ischemic or cerebral vascular hemorrhage, should take
therapeutic exercise, task-oriented training, gait training,
balance training, restrictive exercise therapy, shoulder treatment
and other rehabilitation training (24). According to a study by Bai et
al (25) on patients with
hemorrhagic stroke, it was found that the improvement of Fugl-Myere
score in the rehabilitation group was significantly higher than the
control group, and this further support our research results.
However, according to Stern et al (26) in patients with non-traumatic
subarachnoid hemorrhage, they found that rehabilitation physicians
have developed the most appropriate rehabilitation program for
these patients with the latest developments and potential
complications, this can reduce the mortality rate in patients.
However, there is currently only a few documents on the
rehabilitation therapy in HICH patients. Therefore, this has made
our study more innovative and valuable.
There are still some shortcomings in our
investigation due to limited experimental conditions, such as small
sample size; so statistical analysis of large data could not be
performed. Also our research subjects were quite uniform, so there
may be differences in the performance among different
ethnicities.
Overall, rehabilitation therapy and nursing
intervention are better than routine treatment and nursing for
postoperative recovery of HICH patients, also there are less
adverse reactions post-operatively, thus it is worthy of promotion
clinically.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
XL and PZ were responsible for methods of treatment
and nursing care. CG and JX collected and analyzed general data of
patients. MH wrote the initial draft manuscript and helped with
statistical analysis. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Xuzhou No. 1 People's Hospital, Xuzhou Municipal Hospital
Affiliated to Xuzhou Medical University (Xuzhou, China). Patients
who participated in this research had complete clinical data.
Signed informed consents were obtained from the patients or the
guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Hemphill JC III, Greenberg SM, Anderson
CS, Becker K, Bendok BR, Cushman M, Fung GL, Goldstein JN,
Macdonald RL, Mitchell PH, et al American Heart Association Stroke
Council; Council on Cardiovascular and Stroke Nursing and Council
on Clinical Cardiology, : Guidelines for the management of
spontaneous intracerebral hemorrhage: A guideline for healthcare
professionals from the American Heart Association/American Stroke
Association. Stroke. 46:2032–2060. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wang J, Wang G, Yi J, Xu Y, Duan S, Li T,
Sun XG and Dong L: The effect of monascin on hematoma clearance and
edema after intracerebral hemorrhage in rats. Brain Res Bull.
134:24–29. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Qureshi AI and Qureshi MH: Acute
hypertensive response in patients with intracerebral hemorrhage
pathophysiology and treatment. J Cereb Blood Flow Metab.
38:1551–1563. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hong D, Stradling D, Dastur CK, Akbari Y,
Groysman L, Al-Khoury L, Chen J, Small SL and Yu W: Resistant
hypertension after hypertensive intracerebral hemorrhage is
associated with more medical interventions and longer hospital
stays without affecting outcome. Front Neurol. 8:1842017.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zhang XQ, Zhang ZM, Yin XL, Zhang K, Cai H
and Ling F: Exploring the optimal operation time for patients with
hypertensive intracerebral hemorrhage: Tracking the expression and
progress of cell apoptosis of prehematomal brain tissues. Chin Med
J (Engl). 123:1246–1250. 2010.PubMed/NCBI
|
|
6
|
Lakhan SE, Kirchgessner A, Tepper D and
Leonard A: Matrix metalloproteinases and blood-brain barrier
disruption in acute ischemic stroke. Front Neurol. 4:322013.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ropper AE and Chi JH: Treatment of
traumatic brain injury without direct intracranial pressure
monitoring. Neurosurgery. 72:N19–N20. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Gavito-Higuera J, Khatri R, Qureshi IA,
Maud A and Rodriguez GJ: Aggressive blood pressure treatment of
hypertensive intracerebral hemorrhage may lead to global cerebral
hypoperfusion: Case report and imaging perspective. World J Radiol.
9:448–453. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Manno EM, Atkinson JL, Fulgham JR and
Wijdicks EF: Emerging medical and surgical management strategies in
the evaluation and treatment of intracerebral hemorrhage. Mayo Clin
Proc. 80:420–433. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
10
|
Inamasu J, Nakae S, Adachi K and Hirose Y:
Angiotensin II receptor blockers following intravenous nicardipine
administration to lower blood pressure in patients with
hypertensive intracerebral hemorrhage: A prospective randomized
study. Blood Press Monit. 22:34–39. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Knecht S, Roßmüller J, Unrath M, Stephan
KM, Berger K and Studer B: Old benefit as much as young patients
with stroke from high-intensity neurorehabilitation: Cohort
analysis. J Neurol Neurosurg Psychiatry. 87:526–530. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Shimamura N, Katagai T, Kakuta K, Matsuda
N, Katayama K, Fujiwara N, Watanabe Y, Naraoka M and Ohkuma H:
Rehabilitation and the Neural Network After Stroke. Transl Stroke
Res. 8:507–514. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Li W, Gao J, Wei S and Wang D: Application
values of clinical nursing pathway in patients with acute cerebral
hemorrhage. Exp Ther Med. 11:490–494. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Phipps MS, Jastreboff AM, Furie K and
Kernan WN: The diagnosis and management of cerebrovascular disease
in diabetes. Curr Diab Rep. 12:314–323. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kalaria RN: Cerebrovascular disease and
mechanisms of cognitive impairment: Evidence from
clinicopathological studies in humans. Stroke. 43:2526–2534. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Soustiel JF, Sviri GE, Mahamid E, Shik V,
Abeshaus S and Zaaroor M: Cerebral blood flow and metabolism
following decompressive craniectomy for control of increased
intracranial pressure. Neurosurgery. 67:65–72. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Xu X, Chen X, Li F, Zheng X, Wang Q, Sun
G, Zhang J and Xu B: Effectiveness of endoscopic surgery for
supratentorial hypertensive intracerebral hemorrhage: A comparison
with craniotomy. J Neurosurg. 128:553–559. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Biffi A, Anderson CD, Battey TW, Ayres AM,
Greenberg SM, Viswanathan A and Rosand J: Association between blood
pressure control and risk of recurrent intracerebral hemorrhage.
JAMA. 314:904–912. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yu SX, Zhang QS, Yin Y, Liu Z, Wu JM and
Yang MX: Continuous monitoring of intracranial pressure for
prediction of postoperative complications of hypertensive
intracerebral hemorrhage. Eur Rev Med Pharmacol Sci. 20:4750–4755.
2016.PubMed/NCBI
|
|
20
|
Li F and Chen QX: Risk factors for mental
disorders in patients with hypertensive intracerebral hemorrhage
following neurosurgical treatment. J Neurol Sci. 341:128–132. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lee LC and Tsai AC: Mini-nutritional
assessment predicts functional decline of elderly Taiwanese: Result
of a population-representative sample. Br J Nutr. 107:1707–1713.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Waguchi H, Hidaka K, Shinoki K, Matsuoka
M, Mito S, Doi S, Hata A, Ibata T, Komuro R and Iijima S:
Coordination to assist with hospital-to-home discharge after
cerebral hemorrhage - perspectives of a patient's family and nurse.
Gan To Kagaku Ryoho. 40 (Suppl 2):216–218. 2013.(In Japanese).
PubMed/NCBI
|
|
23
|
Raitakari OT, Juonala M, Kähönen M,
Taittonen L, Laitinen T, Mäki-Torkko N, Järvisalo MJ, Uhari M,
Jokinen E, Rönnemaa T, et al: Cardiovascular risk factors in
childhood and carotid artery intima-media thickness in adulthood:
The Cardiovascular Risk in Young Finns Study. JAMA. 290:2277–2283.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Cavallo S, Brosseau L, Toupin-April K,
Wells GA, Smith CA, Pugh AG, Stinson J, Thomas R, Ahmed S, Duffy
CM, et al: Ottawa panel evidence-based clinical practice guidelines
for structured physical activity in the management of juvenile
idiopathic arthritis. Arch Phys Med Rehabil. 98:1018–1041. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Bai Y, Hu Y, Wu Y, Zhu Y, He Q, Jiang C,
Sun L and Fan W: A prospective, randomized, single-blinded trial on
the effect of early rehabilitation on daily activities and motor
function of patients with hemorrhagic stroke. J Clin Neurosci.
19:1376–1379. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Stern M, Chang D, Odell M and Sperber K:
Rehabilitation implications of non-traumatic subarachnoid
haemorrhage. Brain Inj. 20:679–685. 2006. View Article : Google Scholar : PubMed/NCBI
|