Introduction
Nephrolithiasis is a very common illness that
affects 5% of the population in the United States (1). It may result in chronic renal disease,
and ultimately end-stage kidney disease, if left untreated. In the
past two decades, owing to the technological improvements and
miniaturization of instruments, the treatment for kidney stone
disease has changed dramatically (1).
Percutaneous nephrolithotripsy (PCNL) is recommended
by guidelines on Urolithiasis as the first-line treatment for the
management of kidney stones ≥20 mm (2). Although it has been reported that PCNL
has high success rates (>95%), there are still several
significant complications associated with this procedure, including
urinary extravasation, bleeding necessitating transfusion,
postoperative fever, and septicaemia (3,4).
Retrograde intrarenal surgery (RIRS) is a procedure
that has been considered in the management of smaller stones, or
subsequently, after RIRS with a semirigid ureteroscope to
disintegrate debris in the low calyx (5). Since the procedure is involved with
long leaning curves and high rates of fiber breakage, the
complication rate and costs of the procedure are high. According to
retrospective studies, RIRS appears to be less invasive and safer
but also less effective in the treatment of kidney stones, when
compared with PCNL. Furthermore, due to the technological
improvements in the design of modern ureteroscopes, RIRS has also
been frequently considered in the treatment of larger renal stones
as an alternative to PCNL (5,6).
However, whether RIRS is superior to PCNL in the management of
renal stones remains controversial. Therefore, the present
meta-analysis was conducted to compare the efficacy and safety of
PCNL and RIRS in the treatment of renal stones.
Materials and methods
Search strategy
The following electronic databases were searched for
relevant articles without language restrictions: PubMed (ncbi.nlm.nih.gov/pubmed), Web of Science
(webofknowledge.com), Excerpta Medica
dataBASE (EMBASE; embase.com), and the Chinese
Biomedical Database (CBM; http://www.sinomed.ac.cn/).
The following search items were used: [‘Kidney
calculi’ (MeSH Terms)] OR [‘kidney’ (All Fields) AND ‘calculi’ (All
Fields)] OR [‘kidney calculi’ (All Fields)] OR [‘renal’ (All
Fields) AND ‘calculus’ (All Fields)] OR [‘renal calculus’ (All
Fields) AND retrograde (All Fields) AND intrarenal (All Fields) AND
‘surgery’ (Subheading)] OR [‘surgery’ (All Fields)] OR [‘surgical
procedures, operative’ (MeSH Terms)] OR [‘surgical’ (All Fields)
AND ‘procedures’ (All Fields) AND ‘operative’ (All Fields)] OR
[‘operative surgical procedures’ (All Fields)] OR [‘surgery’ (All
Fields)] OR [‘general surgery’ (MeSH Terms)] OR [‘general’ (All
Fields) AND ‘surgery’ (All Fields)] OR [‘general surgery’ (All
Fields) AND ‘nephrostomy, percutaneous’ (MeSH Terms)] OR
[‘nephrostomy’ (All Fields) AND ‘percutaneous’ (All Fields)] OR
[‘percutaneous nephrostomy’ (All Fields)] OR [‘percutaneous’ (All
Fields) AND ‘nephrolithotomy’ (All Fields)] OR [‘percutaneous
nephrolithotomy’ (All Fields)].
Selection criteria
Inclusion criteria that an eligible study had to
meet were as follows: i) Study design: RCT or cohort study; ii)
study population: Patients with a solitary renal stone; iii) study
intervention: Patients were treated either by RIRS or PCNL; iv) and
outcome measures: Stone-free rate, hospital stay, operation time,
and complication rate. Exclusion criteria included: i) Reviews,
letters, case report, or abstracts; ii) patients had anatomic
anomalies of kidney; iii) patients were not treated with RIRS or
PCNL; and iv) did not provide one of these interest outcomes.
Data extraction
Two independent investigators extracted the
following information for each study: First author's name, year of
publication, number of patients (RIRS group and PCNL group), mean
operation time, mean hospital stay, stone-free rate and
complication rate. A standardized Excel file was used to extract
the data. When the same trial appeared in different publications,
we chose the article with the most information or the latest data.
Disagreements between the investigators were resolved through
discussion and consensus.
Methodological assessments
We applied the Jadad scale (7) to assess the methodological quality of
RCTs. The scale consists of three items, including randomization
(0–2 points), blinding (0–2 points), and dropouts and withdrawals
(0–1 point). The total score is 5 points. Studies with a score ≥3
points are considered to be of high quality (8). For cohort studies, we used the modified
Newcastle-Ottawa Scale (NOS) (9),
which assesses studies using information on patients selection,
comparability of RIRS and PCNL group, and an assessment of the
outcomes of interest. The scale ranged from 0 to 9 stars, and
studies with a quality score of ≥6 were considered to be of high
quality (9).
Statistical analysis
All analyses were conducted using STATA version 12.0
(Stata Corp., College Station, TX, USA). Heterogeneity among the
included studies was assessed with Cochran's Q test (10) and I2 statistic
(11), in which
I2>50%, or P<0.10 was considered as
statistically significant heterogeneity (11). When significant heterogeneity was
identified, a random-effect model (DerSimonian-Laird method)
(12) was used to calculate
parameters; otherwise, a fixed-effect model (Mantel-Haenszelmethod)
(10) was used to pool data. For
dichotomous variables, including stone-free rate and incidence of
complications, the number of cases and total number of patients
were extracted from the included studies. Thereafter, they were
expressed as a risk ratio (RR) with 95% confidence intervals (CIs).
For continuous variables, including duration of hospital stay and
duration of operative time, the mean value and standard deviation
(SD) were extracted from the included studies. Thereafter, the
weighted mean difference (WMD) with 95% CIs was calculated.
Subgroup analysis was also performed based on the stone size or
study design to explore potential sources of heterogeneity.
Publication bias was evaluated by Begg's (13) and Egger's (14) tests. A P<0.05 was considered to
indicate a statistically significant difference, except when
otherwise specified.
Results
Identification of eligible
studies
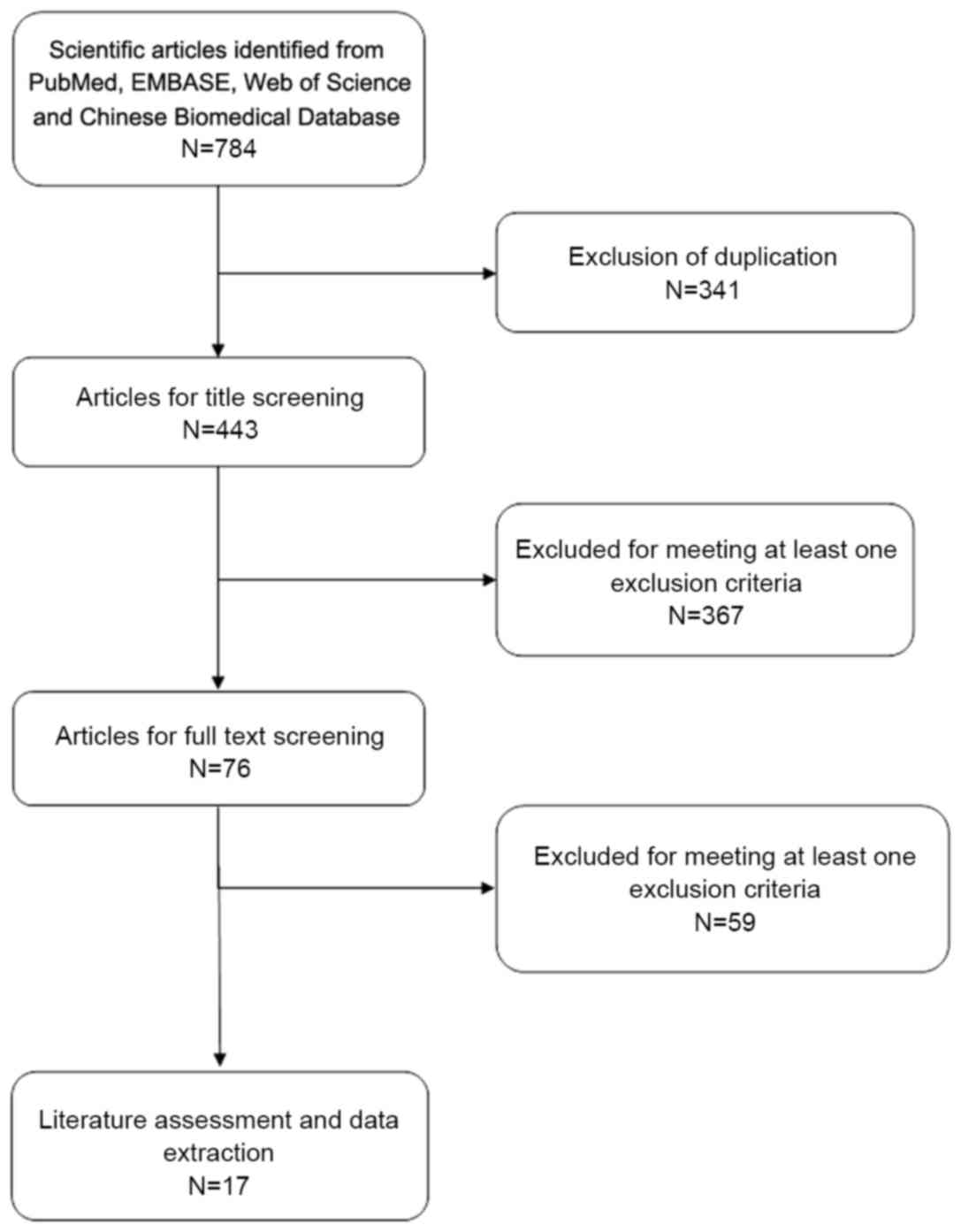
A total of 784 studies were initially retrieved in
the literature search, including 169 in PubMed, 78 in Web of
Science, 488 in EMBASE, and 49 in CBM. After checking for
duplicates, 443 publications were eligible for inclusion in the
meta-analysis. Of these, 367 studies were excluded after the
title/abstract review, and 59 studies were excluded after the
full-text review. Finally, 4 RCTs and 13 cohort studies were
included in this meta-analysis (15–31). A
flow chart of the search strategy is shown in Fig. 1.
Study characteristics
Table I presents the
main characteristics of included studies. Baseline demographics in
each study were comparable between the PCNL and RIRS groups, in
terms of age, stone size, number and the locations of stones. All
the studies were published in peer-reviewed journals between 2008
and 2015. The sample size of these studies ranged from 27 to 280.
Of the 17 studies, 4 were RCTs (16,20,21,25), and
the remaining 13 were cohort studies (15,17–19,22–24,26–31).
Although the stone sizes among these studies were variable, most
studies provided the outcome data in two groups: <2 cm group and
2–3 cm group.
 | Table I.Baseline characteristics of patients
in the trials included in the present meta-analysis. |
Table I.
Baseline characteristics of patients
in the trials included in the present meta-analysis.
| Study | Study design | Surgery | Case no. | Age, years | Stone size, mm | NOS score | (Refs.) |
|---|
| Akman et
al | Cohort | PCNL | 34 | 44.8 ±17.1 | NR | 7 | (15) |
|
|
| RIRS | 34 | 44.5 ±16.5 | NR |
|
|
| Bryniarski et
al | RCT | PCNL | 32 | 51.8 ±11.8 | >20 | 4 (Jadad
score) | (16) |
|
|
| RIRS | 32 | 53.4 ±12.4 | >20 |
|
|
| Pan et
al | Cohort | PCNL | 59 | 49.37±14.2 | 22.37±2.7 | 8 | (17) |
|
|
| RIRS | 56 | 49.32±13.7 | 22.28±2.6 |
|
|
| Hyams and Shah | Cohort | PCNL | 20 | 48 | 20–30 | 7 | (18) |
|
|
| RIRS | 19 | 56 | 20–30 |
|
|
| Li et
al | Cohort | PCNL | 30 | 26.4±5.5 | NR | 6 | (19) |
|
|
| RIRS | 24 | 26.4±5.5 | NR |
|
|
| Guo et
al | RCT | PCNL | 24 | 18–60 | 16.4±2.6 | 3 (Jadad
score) | (20) |
|
|
| RIRS | 23 | 18–60 | 15.8±2.7 |
|
|
| Cao et
al | RCT | PCNL | 123 | 20–72 | 23±9 | 3 (Jadad
score) | (21) |
|
|
| RIRS | 120 | 21–71 | 24±9 |
|
|
| Yang et
al | Cohort | PCNL | 52 | 20–50 | <20 | 7 | (22) |
|
|
| RIRS | 68 | 20–50 | <20 |
|
|
| Zhu et
al | Cohort | PCNL | 24 | 44.13±7.11 | NR | 6 | (23) |
|
|
| RIRS | 23 | 44.13±7.11 | NR |
|
|
| Yao et
al | Cohort | PCNL | 45 | 21–73 | 24±7 | 7 | (24) |
|
|
| RIRS | 64 | 21–73 | 25±9 |
|
|
| He | RCT | PCNL | 20 | 43.5±2.3 | NR | 3 (Jadad
score) | (25) |
|
|
| RIRS | 18 | 43.5±2.3 | NR |
|
|
| Yang et
al | Cohort | PCNL | 50 | 21–73 | 24±7 | 7 | (26) |
|
|
| RIRS | 67 | 21–73 | 25±9 |
|
|
| Kruck et
al | Cohort | PCNL | 108 | 53.3±14.8 | 12.6±9.5 | 7 | (27) |
|
|
| RIRS | 172 | 50±16.7 | 6.8±6.9 |
|
|
| Resorlu et
al | Cohort | PCNL | 140 | 36.4±19.7 | 17.3±3.6 | 7 | (28) |
|
|
| RIRS | 46 | 29.6±20.3 | 15.6±3.4 |
|
|
| Chung et
al | Cohort | PCNL | 15 | 58 | 10–20 | 7 | (29) |
|
|
| RIRS | 12 | 58.5 | 10–19 |
|
|
| Wiesenthal et
al | Cohort | PCNL | 43 | 52.5±15.1 | 10–20 | 7 | (30) |
|
|
| RIRS | 41 | 53.3±14.2 | 10–20 |
|
|
| Bozkurt et
al | Cohort | PCNL | 42 | 47.4±15.5 | 15–20 | 7 | (31) |
|
|
| RIRS | 37 | 41.2±13.6 | 15–20 |
|
|
Quality assessment
NOS scores for 13 cohort studies ranged from 7 to 8,
and Jadad scores for 4 RCTs ranged from 3 to 4. This indicated that
all the included studies were of high quality.
Stone-free rate
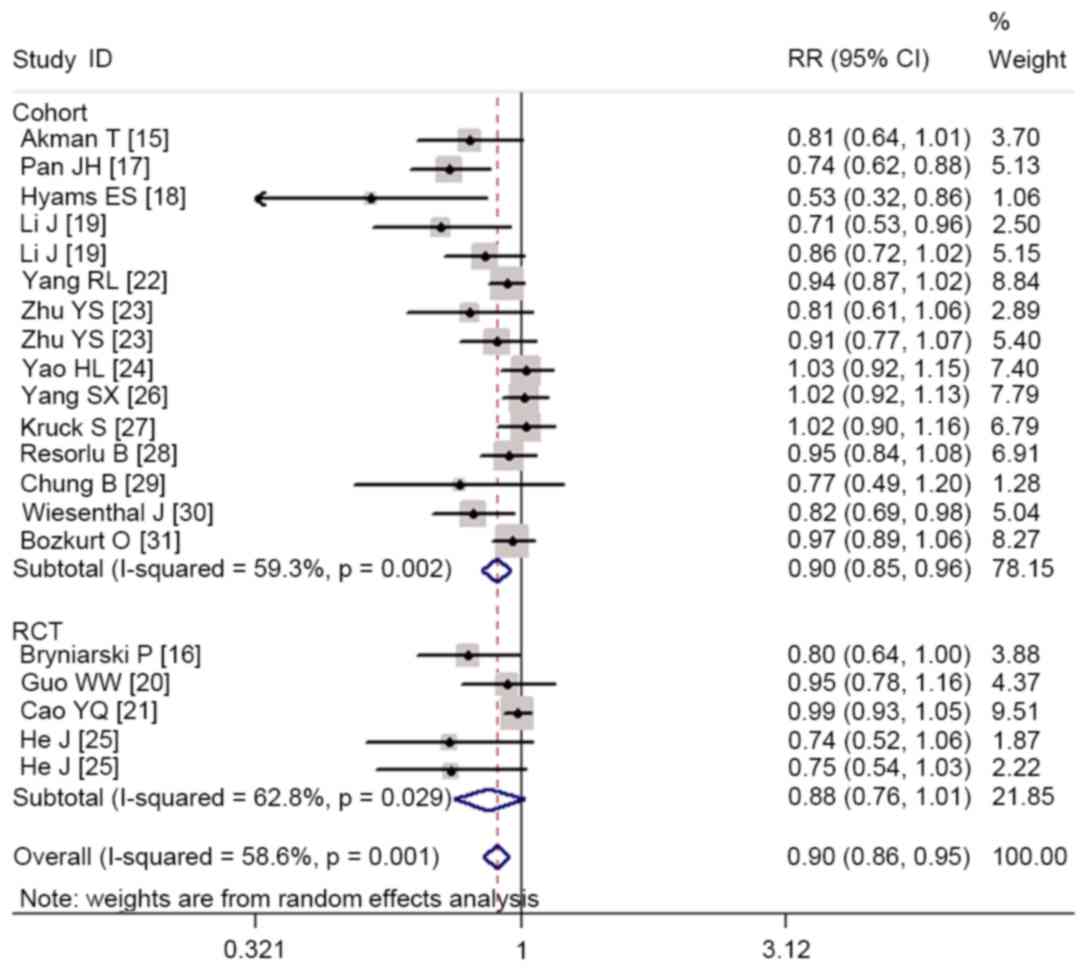
All studies reported the stone-free rate (15–31).
Pooling of all the studies using a random effects model showed that
the stone-free rate was significant lower in the RIRS group than
that in the PCNL group (RR=0.90, 95% CI: 0.86 to 0.95; P<0.001;
Fig. 2). There was statistical
heterogeneity among the included studies (heterogeneity: P=0.001,
I2=58.6%). Subsequently, we performed subgroup analysis
according to stone size and study design to explore the potential
sources of heterogeneity.
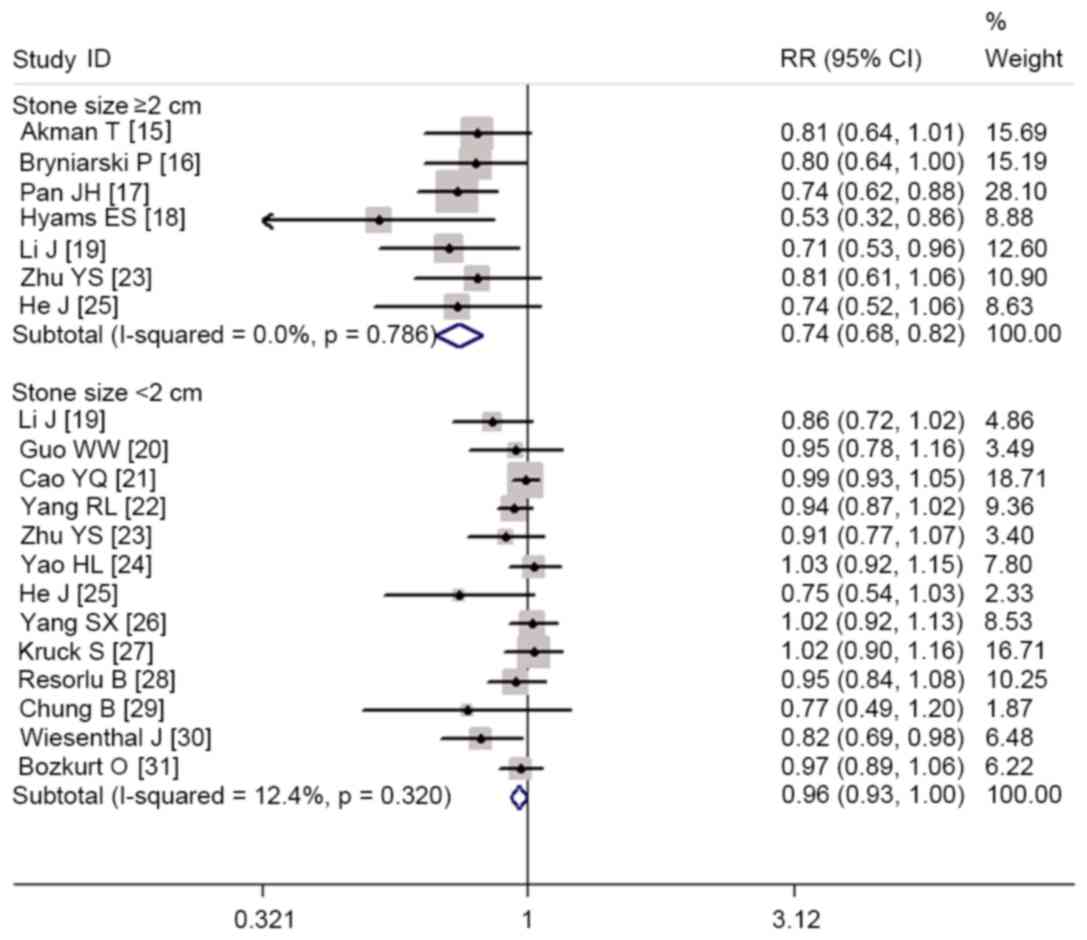
Pooled estimates suggested that RIRS had a
significant lower stone-free rate than PCNL in the treatment of
renal stones <2 cm (RR=0.96, 95% CI: 0.93 to 1.00; P=0.031) and
≥2 cm (RR=0.74, 95% CI: 0.68 to 0.82; P<0.001; Fig. 3). Subgroup analysis based on RCTs
showed that the stone-free rate was similar between the two groups
(RR=0.88, 95% CI: 0.76 to 1.01; P=0.078), whereas pooled results
from cohort studies revealed a significant higher stone-free rate
in the PCNL group than that in the RIRS group (RR=0.90, 95% CI:
0.85 to 0.96; P=0.002; Fig. 2).
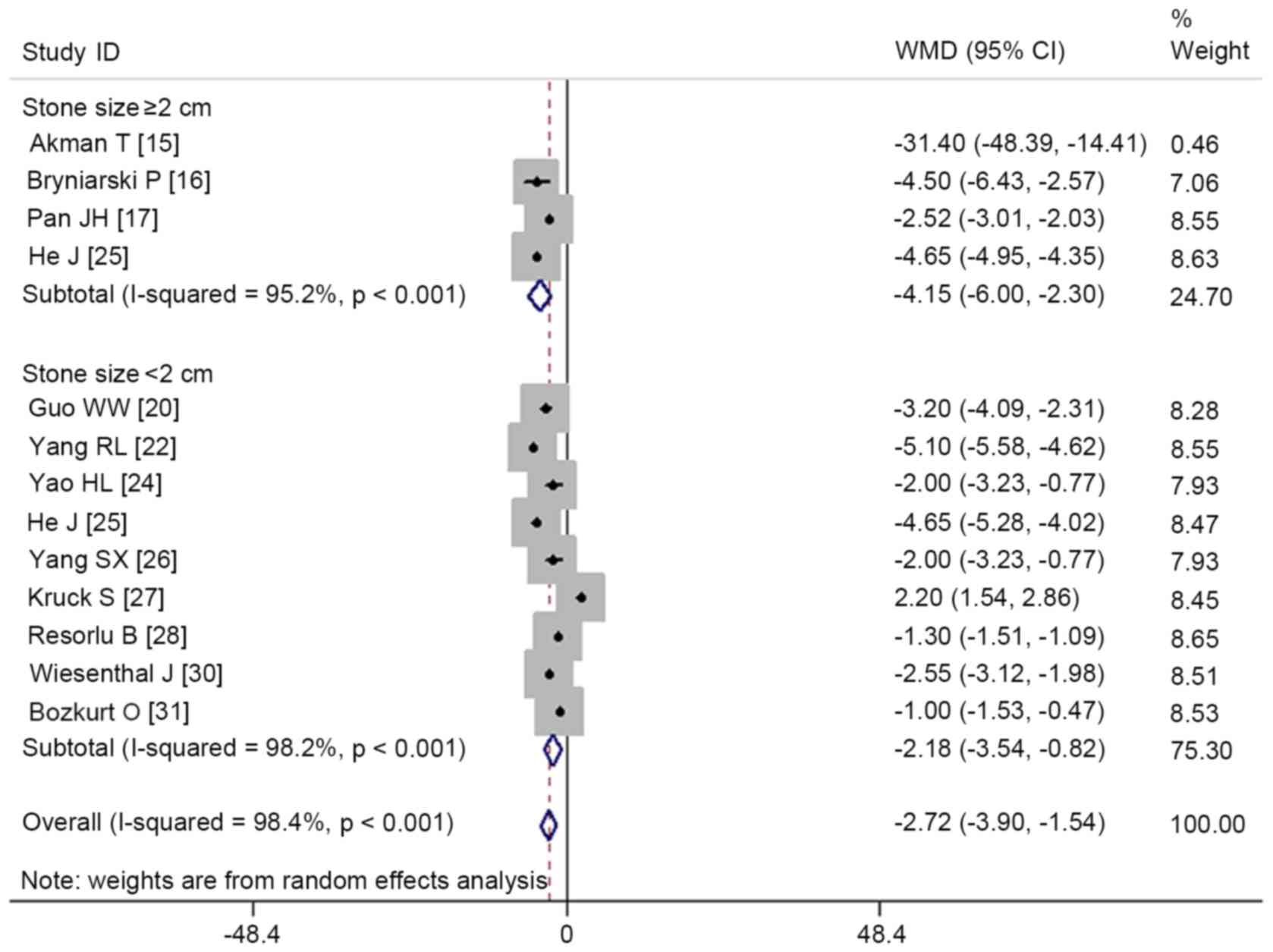
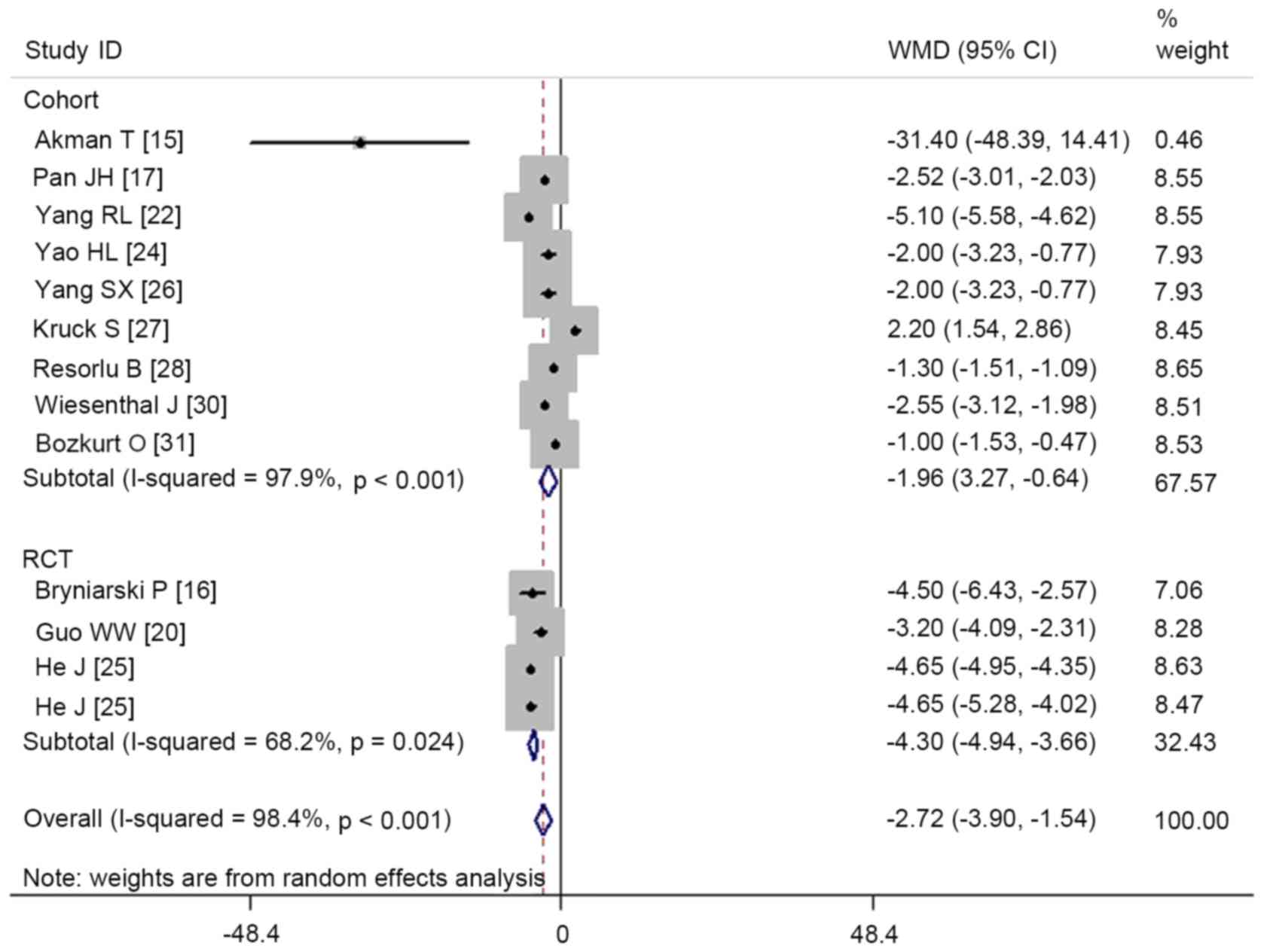
Hospital stay
In total, 12 studies presented hospital stay data
(15–17,20,22,24–28,30,31).
Aggregated results using a random effects model suggested that
patients treated with RIRS had a significantly shorter hospital
stay than those treated with PCNL (WMD=−2.72, 95% CI: −3.9 to
−1.54; P<0.001; Fig. 4). The test
for heterogeneity among the individual studies was significant
(heterogeneity: P<0.001, I2=98.4%). Therefore, we
performed subgroup analysis based on stone size and study design to
explore the potential sources of heterogeneity.
Subgroup analysis based on stone size revealed that
RIRS was associated with a significantly shorter hospital stay in
patients with stone sizes <2 cm (WMD=−2.18, 95% CI: −3.54 to
−0.82; P=0.002) and ≥2 cm (WMD=−4.15, 95% CI: −6.00 to −2.30;
P<0.001; Fig. 4). Subgroup
analysis based on study design demonstrated that both RCTs and
cohort studies demonstrated a significantly shorter hospital stay
in the RIRS group than that in the PCNL group (RCTs: WMD=−4.3, 95%
CI: −4.94 to −3.66; P<0.001; cohort studies: WMD=−1.96, 95% CI:
−3.27 to −0.64; P=0.004; Fig.
5).
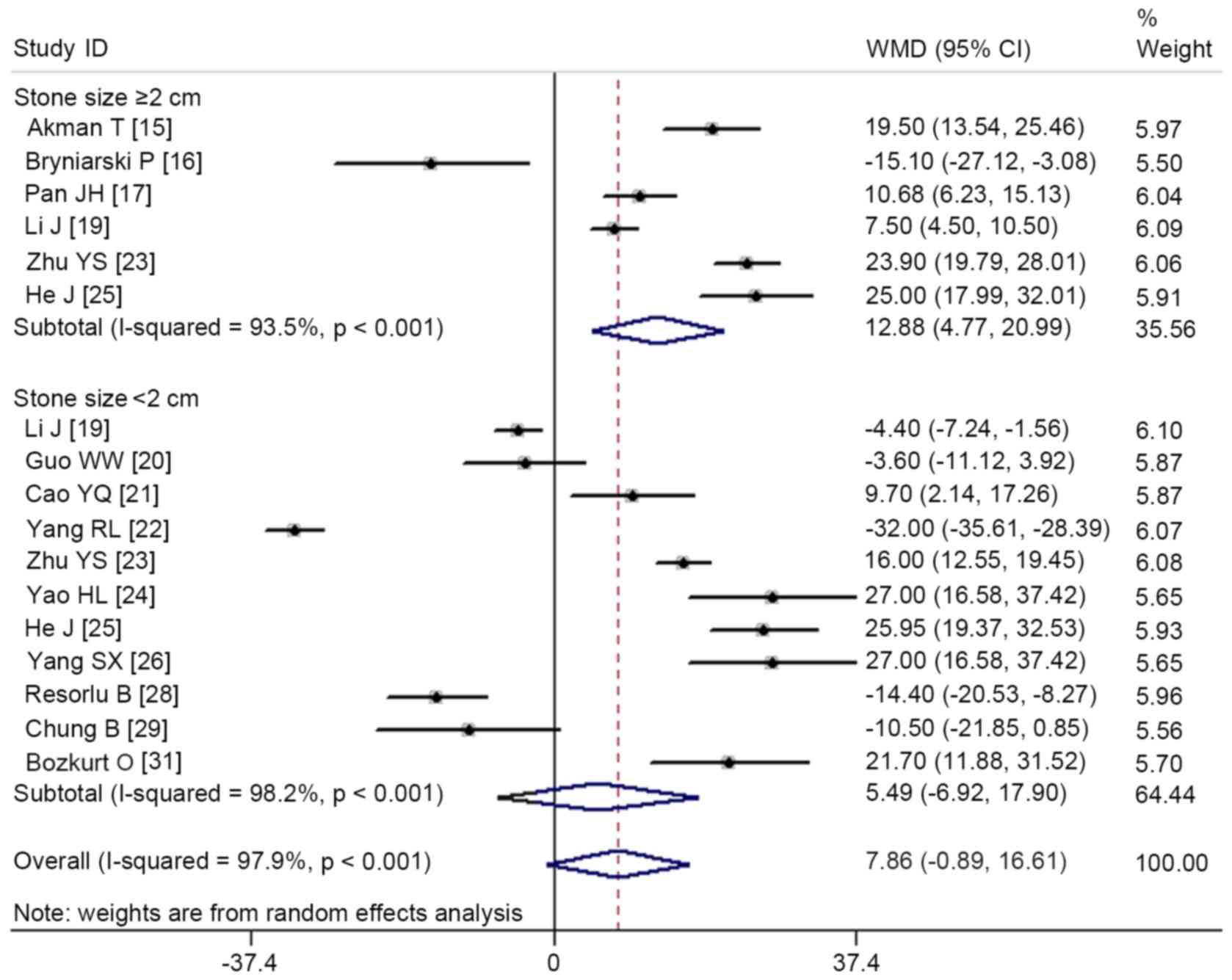
Operation time
A total of 14 studies provided operation time data
(15–17,19–26,28,29,31).
Pooled results showed that there was no significant difference in
operation time between the two groups (WMD=7.86, 95% CI: −0.89 to
16.61; P=0.078; Fig. 6). The test
for heterogeneity was significant (heterogeneity: P<0.001,
I2=97.9%). Consequently, we performed subgroup analysis
based on stone size and study design to explore the potential
sources of heterogeneity.
Subgroup-analysis based on stone size indicated that
RIRS was associated with a significantly longer operation time in
patients with stone sizes ≥2 cm (WMD=12.88, 95% CI: 4.77 to 20.99;
P=0.002), but a similar operation time in patients with stone sizes
<2 cm was found between RIRS and PCNL (WMD=5.49, 95% CI: −6.92
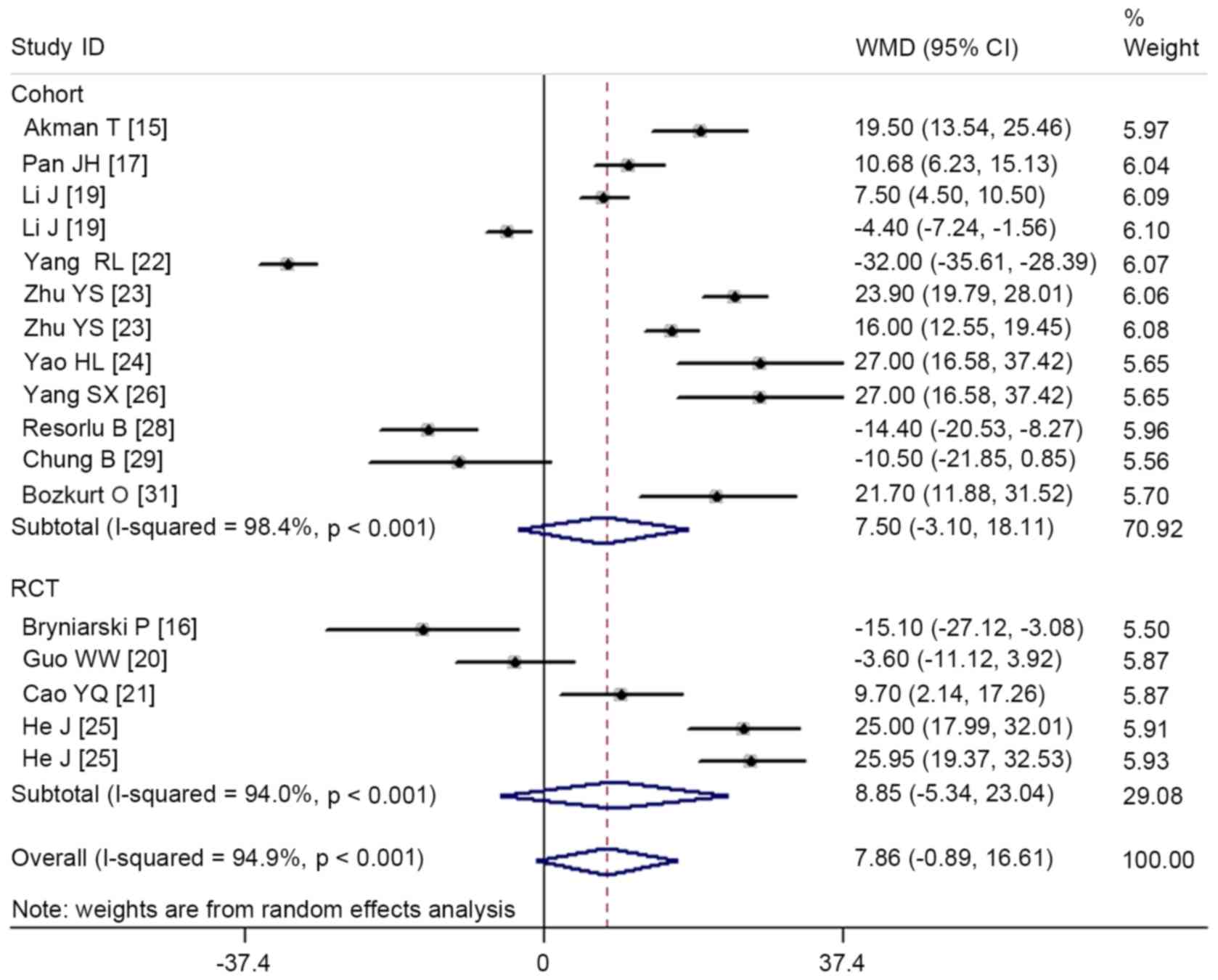
to 17.90; P=0.386; Fig. 6). Subgroup
analysis based on study design revealed that both RCTs and cohort
studies exhibited a similar operation time between the RIRS and
PCNL groups (RCTs: WMD=8.85, 95% CI: −5.34 to 23.04; P=0.222;
cohort studies: WMD=7.5, 95% CI: −3.10 to 18.11; P=0.165; Fig. 7).
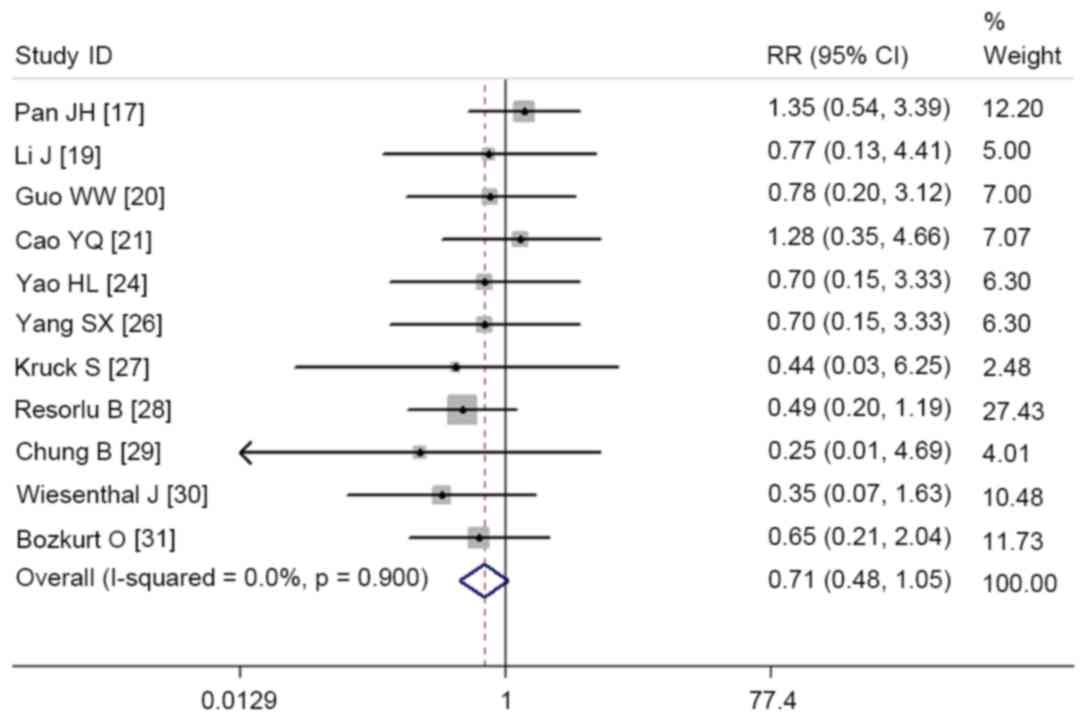
Complication rate
In total, 11 studies reported complication rate data
(17,19–21,24,26–31).
Pooled results using a fixed-effect model showed that there was no
significant difference in complication rates between the RIRS and
PCNL groups (RR=0.71, 95% CI: 0.48 to 1.05; P=0.083). The test for
heterogeneity did not indicate a significant difference
(heterogeneity: P=0.900, I2=0.0%; Fig. 8).
Publication bias
Begg's and Egger's test were used to evaluate
publication bias, and these results revealed that no potential
publication bias existed among the included studies (Egger's test,
P=0.120; Begg's test, P=0.243).
Discussion
This meta-analysis was performed with the objective
of comparing clinical outcomes between RIRS and PCNL for the
management of renal stones. Based on 17 studies, the results from
our meta-analysis suggested that PCNL was associated with a higher
stone-free rate, but a longer hospital stay, when compared with
RIRS. There was no significant difference between the two groups in
terms of operation time and complication rate. However, subgroup
analysis based on stone size showed that PCNL had a shorter
operation time than RIRS in patients with stone sizes measuring ≥2
cm. Subgroup analysis conducted on RCTs demonstrated that the
stone-free rate between the two groups was not significant.
PCNL is recommended as the first-line treatment for
kidney stones measuring >2 cm and also for complex renal stones
(32). Although this procedure has
the advantage of high stone clearance rates, it is an invasive
method that may result in serious complications. However, with the
technical improvements in flexible ureteroscope, RIRS with holmium
laser lithotripsy has become an effective and safe choice for
larger renal stones (6,33). Furthermore, since it is less invasive
than conventional PCNL, URS/laser lithotripsy has been chosen by an
increasing number of patients for the treatment of renal stones,
particularly for stones in an intermediate size range of 2–3 cm
(34). Even so, this technique has
several disadvantages, including the high retreatment rate, high
cost of flexible ureteroscopic replacement and repair (34).
The present meta-analysis demonstrated that the
stone-free rate of RIRS was lower than that of PCNL, but additional
sessions of RIRS achieved comparable stone-free rates with PCNL.
According to previous studies, the overall success rate of RIRS
ranged from 77 to 93% after additional sessions for intrarenal
calculi larger than 2 cm (6,35–39).
Breda et al (6) assessed the
efficacy and safety of ureteroscopic lithotripsy for single
intrarenal stones of sizes 20–25 mm. They found that the mean
post-procedural success rate was 93% after an average of 2.3
sessions (6). Riley et al
(37) reported that for an average
stone size of 3.0 cm, the success rate of RIRS treatment was 90.9%.
In patients with stones measuring >3 cm, 91.6% were stone-free
after an average of 1.9 procedures; patients with stones >3.5
cm, 80% were stone-free after an average of 1.8 procedures; and
patients with stones larger than 4 cm, 50% were stone-free after an
average of 2 procedures (37).
According to this meta-analysis, PCNL had
significant higher stone-free rate than RIRS. However, when the
data was pooled from RCTs, this significant difference was not
observed. Guo et al (20)
conducted a RCT to compare PCNL and flexible ureteroscope holmium
laser lithotripsy for 1–2 cm renal calculi. They reported that the
stone-free rates for the two groups were 91.7 and 86.9%,
respectively, with no significant difference. Similar results were
observed in the RCT conducted by Cao et al (21), in which PCNL and RIRS were used to
treat patients with renal calculi <3 cm in diameter; the
stone-free rates for these two groups were 95.1 and 94.2%,
respectively (21). There was no
significant difference between these values. However, in a RCT
conducted by Bryniarski et al (16), the stone-free rate in the PCNL group
(94%) was significant higher than that in the RIRS group (75%).
Since the stone size in these RCTS was variable, further
well-performed, high-homogeneity RCTs are required to evaluate
whether PCNL has higher stone-free rate than RIRS.
The main reason for the lower disintegration rate in
RIRS compared with PCNL is that larger fragments fall back into the
lower calix where they cannot be accessed with a semirigid
ureteroscope. A flexible ureteroscope was then used by the
urologists to disintegrate them; however, most urologists failed to
leave the kidneys without any stone debris. Notably, Smith et
al (40) described a technique
to avoid such failure. At the beginning of procedure, they filled
the lower calix with autologous blood, meaning that the stone
debris would not fall back there during disintegration (40). Since few studies using this technique
to manage patients with renal stone have been published, further
studies are warranted to identify whether this technique would
increase the disintegration rate.
In this meta-analysis, we found that there was no
significant difference in operation time between the two groups.
The mean operation times for PCNL and RIRS group were 61.49±14.17
and 69.37±16.89 min, respectively. Previous studies have reported
that prolonged operation time was associated with several
complications. Akman et al (41) found that operative time longer than
58 min would increase 2.82 times risk of needing for blood
transfusion when patients were managed with PCNL. Moreover, Kukreja
et al (42) reported that
diabetes mellitus, a multiple access tract procedure and prolonged
operative time, were associated with blood loss during the PCNL
procedure (42). However, whether
prolonged operative time in RIRS would increase the risk of
bleeding remains unknown.
This meta-analysis found that RIRS had a shorter
hospital stay than the PCNL. This result was observed in all of the
included studies. In most western countries, RIRS is considered as
an outpatient procedure in which patients are discharged after 24
h; whereas, PCNL usually requires 2 days of hospitalization. Of the
included studies, Bryniarski et al (16) reported the longest hospital stay, in
which the hospital stays for the PCNL and RIRS group were 11.3±4.4
and 6.8±3.4 days, respectively. The authors explained the prolonged
hospitalization. Firstly, the approach they used from the
procedural causes was different, thus patients required a longer
hospital stay; secondly, they used a wide ureteroscope for RIRS
(16). In order to avoid potential
strictures, patients were required to remain in hospital for longer
to ensure the ureters were able to recover with ureteral stents
inserted (16).
With regards to the complications, no significant
difference between the PCNL and RIRS group was found in this
meta-analysis. Despite this, several complications related with
PCNL or RIRS should not be ignored. Percutaneous access is the main
reason for the complications. Severe complications would result in
damage to the renal parenchyma and adjacent structures. The PCNL
procedure is associated with several complications, including
bleeding requiring blood transfusion, septicaemia, colonic injury,
fever and urinary infection (43,44).
Bleeding requiring transfusion is one of the most important
complications, the incidence of which has been reported to range
from 0.8 to 45% in the PCNL literature (43–45).
Urosepsi is one of the most important complications related with
RIRS. Takazawa et al (46)
reported that 15% of the patients with renal stones measuring ≥2 cm
presented a high-grade fever with urosepsis when they were treated
with flexible ureteroscopic lithotripsy (46). This severe complication could be
explained by two main reasons: Intrarenal reflux-containing
bacteria from infectious stones during fragmentation, and a long
operative time (46).
There are several potential limitations to this
meta-analysis that should be considered. Firstly, of the 17
studies, only 4 were RCTs, and the remaining 13 were cohort
studies. Despite the reasoning that cohort studies may reflect the
real-world and further support the conclusion, cohort data are
associated with bias due to patient selection. Secondly, 10 of the
studies included had a relatively small sample size (n<100).
Although all of these studies were well-performed, high-quality
trials, our conclusions should be interpreted with caution because
studies with small sample size are more likely to overestimate the
treatment effect than those with larger sample sizes. Thirdly, the
characteristics (age, sex, stone number, stone localization and
stone size), and study designs varied considerably among the
included studies. These factors may increase the heterogeneity and
affect the pooled estimates. Therefore, physicians should interpret
our findings with caution when applying them to clinical
practice.
In conclusion, the findings of the present
meta-analysis indicated that PCNL had a higher stone-free rate, but
longer hospital stay, in comparison with RIRS. Operation time and
complication rate between the two groups were comparable.
Therefore, we propose that RIRS may be an alternative therapy to
PCNL, with acceptable efficacy and complication rates for renal
stones. However, considering the potential limitations of this
study, further large-scale, well-conducted RCTs are required to
verify our findings.
Acknowledgements
The present study was supported by the Medical
Scientific Research Foundation of Zhejiang Province, China (grant
nos. 2015DTA017 and 2016ZHA005).
References
|
1
|
Stamatelou KK, Francis ME, Jones CA,
Nyberg LM and Curhan GC: Time trends in reported prevalence of
kidney stones in the United States: 1976–1994. Kidney Int.
63:1817–1823. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Preminger GM, Assimos DG, Lingeman JE,
Nakada SY, Pearle MS and Wolf JS Jr; AUA Nephrolithiasis Guideline
Panel, : Chapter 1: AUA guideline on management of staghorn
calculi: Diagnosis and treatment recommendations. J Urol.
173:1991–2000. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Michel MS, Trojan L and Rassweiler JJ:
Complications in percutaneous nephrolithotomy. Eur Urol.
51:899–906. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
de la Rosette J, Assimos D, Desai M,
Gutierrez J, Lingeman J, Scarpa R and Tefekli A; CROES PCNL Study
Group, : The clinical research office of the endourological society
percutaneous nephrolithotomy global study: Indications,
complications, and outcomes in 5,803 patients. J Endourol.
25:11–17. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Traxer O, Dubosq F, Jamali K, Gattegno B
and Thibault P: New-generation flexible ureterorenoscopes are more
durable than previous ones. Urology. 68:276–281. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Breda A, Ogunyemi O, Leppert JT, Lam JS
and Schulam PG: Flexible ureteroscopy and laser lithotripsy for
single intrarenal stones 2 cm or greater-is this the new frontier?
J Urol. 179:981–984. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Jadad AR, Moore RA, Carroll D, Jenkinson
C, Reynolds DJ, Gavaghan DJ and McQuay HJ: Assessing the quality of
reports of randomized clinical trials: Is blinding necessary?
Control Clin Trials. 17:1–12. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kjaergard LL, Villumsen J and Gluud C:
Reported methodologic quality and discrepancies between large and
small randomized trials in meta-analyses. Ann Intern Med.
135:982–989. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wells G, Shea B, O'connell D, Peterson J
and Welch V: The Newcastle-Ottawa Scale (NOS) for assessing the
quality of nonrandomized studies in meta-analyses. 3rd Symposium on
Systematic Reviews: Beyond the Basics. 3–5. 2000.
|
|
10
|
DerSimonian R and Laird N: Meta-analysis
in clinical trials. Control Clin Trials. 7:177–188. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Higgins JP, Thompson SG, Deeks JJ and
Altman DG: Measuring inconsistency in meta-analyses. BMJ.
327:557–560. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Mantel N and Haenszel W: Statistical
aspects of the analysis of data from retrospective studies of
disease. J Natl Cancer Inst. 22:719–748. 1959.PubMed/NCBI
|
|
13
|
Begg CB and Mazumdar M: Operating
characteristics of a rank correlation test for publication bias.
Biometrics. 50:1088–1101. 1994. View
Article : Google Scholar : PubMed/NCBI
|
|
14
|
Egger M, Davey Smith G, Schneider M and
Minder C: Bias in meta-analysis detected by a simple, graphical
test. BMJ. 315:629–634. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Akman T, Binbay M, Ozgor F, Ugurlu M,
Tekinarslan E, Kezer C, Aslan R and Muslumanoglu AY: Comparison of
percutaneous nephrolithotomy and retrograde flexible
nephrolithotripsy for the management of 2–4 cm stones: A
matched-pair analysis. BJU Int. 109:1384–1389. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Bryniarski P, Paradysz A, Zyczkowski M,
Kupilas A, Nowakowski K and Bogacki R: A randomized controlled
study to analyze the safety and efficacy of percutaneous
nephrolithotripsy and retrograde intrarenal surgery in the
management of renal stones more than 2 cm in diameter. J Endourol.
26:52–57. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Pan J, Chen Q, Xue W, Chen Y, Xia L, Chen
H and Huang Y: RIRS versus mPCNL for single renal stone of 2–3 cm:
Clinical outcome and cost-effective analysis in Chinese medical
setting. Urolithiasis. 41:73–78. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hyams ES and Shah O: Percutaneous
nephrostolithotomy versus flexible ureteroscopy/holmium laser
lithotripsy: Cost and outcome analysis. J Urol. 182:1012–1017.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Li J, Wang J, Li Y, Tong F, Zhai C and Ye
L: Comparative study of transurethral flexible ureteroscope
lithotripsy and minimally invasive percutaneous nephrolithotomy in
treatment of renal calyceal calculi. J Kunming Med Univ.
36:134–136. 2015.
|
|
20
|
Guo W, Yan R, Wang L, Zhang J and Liu C:
Percutaneous nephrolithotomy versus flexible ureteroscope holmium
laser lithotripsy for renal calculi. Int Med Health Guidance News.
21:1520–1524. 2015.(In Chinese).
|
|
21
|
Cao Y, Jiang Z and Shi L: Comparison of
the clinical efficacy of percutaneous nephrolithotomy and
ureteroscopy for the treatment of renal calculi. Int J Urol
Nephrol. 34:805–808. 2014.
|
|
22
|
Yang R, Kang J and Chen D: Flexible
ureteroscopy and percutaneous nephrolithotomy holmium laser
lithotripsy for renal calculi (<2 cm) clinical effect
comparison. Med Infor. 28:37–38. 2015.
|
|
23
|
Zhu Y, Su H and Deng Q: Comparative
efficacy analysis of flexible ureteroscopic lithotripsy and
percutaneous nephrolithotomy for treatment of renal calyceal
stones. J Luzhou Med Col. 382–383. 2013.
|
|
24
|
Yao H, Song C and Liu L: Comparison of
therapeutic effects of renal calculi witll ureteroscopic holminum
laser fithotripsy versus percutaneous nephrostofithotripsy. J Clin
Surg. 21:802–803. 2013.
|
|
25
|
He J: Comparison of the clinical efficacy
of percutaneous nephrolithotomy and ureteroscopy for the treatment
of renal calculi. Med Aesthetics Cosmetol. 6972015.
|
|
26
|
Yang S, Song C, Liu L, et al: Management
of renal calculi: Retrograde ureteroscopic holminum laser versus
percutaneous nephrolithotripsy. Chin J Urol. 34:666–669. 2013.
|
|
27
|
Kruck S, Anastasiadis AG, Herrmann TR,
Walcher U, Abdelhafez MF, Nicklas AP, Hölzle L, Schilling D, Bedke
J, Stenzl A and Nagele U: Minimally invasive percutaneous
nephrolithotomy: An alternative to retrograde intrarenal surgery
and shockwave lithotripsy. World J Urol. 31:1555–1561. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Resorlu B, Unsal A, Ziypak T, Diri A, Atis
G, Guven S, Sancaktutar AA, Tepeler A, Bozkurt OF and Oztuna D:
Comparison of retrograde intrarenal surgery, shockwave lithotripsy
and percutaneous nephrolithotomy for treatment of medium-sized
radiolucent renal stones. World J Urol. 31:1581–1586. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Chung BI, Aron M, Hegarty NJ and Desai MM:
Ureteroscopic versus percutaneous treatment for medium-size
(1–2-cm) renal calculi. J Endourol. 22:343–346. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wiesenthal JD, Ghiculete D, D'A Honey RJ
and Pace KT: A comparison of treatment modalities for renal calculi
between 100 and 300 mm2: Are shockwave lithotripsy, ureteroscopy,
and percutaneous nephrolithotomy equivalent? J Endourol.
25:481–485. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Bozkurt OF, Resorlu B, Yildiz Y, Can CE
and Unsal A: Retrograde intrarenal surgery versus percutaneous
nephrolithotomy in the management of lower-pole renal stones with a
diameter of 15 to 20 mm. J Endourol. 25:1131–1135. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Tiselius HG, Alken P and Buck C:
Guidelines on urolithiasis. http://www.uroweb.org/fileadmin/user_upload/Guidelines/Urolithiasis.pdf2010
|
|
33
|
Mariani AJ: Combined electrohydraulic and
holmium:YAG laser ureteroscopic nephrolithotripsy of large (greater
than 4 cm) renal calculi. J Urol. 177:168–173. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Hyams ES, Munver R, Bird VG, Uberoi J and
Shah O: Flexible ureterorenoscopy and holmium laser lithotripsy for
the management of renal stone burdens that measure 2 to 3 cm: A
multi-institutional experience. J Endourol. 24:1583–1588. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
El-Anany FG, Hammouda HM, Maghraby HA and
Elakkad MA: Retrograde ureteropyeloscopic holmium laser lithotripsy
for large renal calculi. BJU Int. 88:850–853. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Grasso M, Conlin M and Bagley D:
Retrograde ureteropyeloscopic treatment of 2 cm. or greater upper
urinary tract and minor Staghorn calculi. J Urol. 160:346–351.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Riley JM, Stearman L and Troxel S:
Retrograde ureteroscopy for renal stones larger than 2.5 cm. J
Endourol. 23:1395–1398. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Mariani AJ: Combined electrohydraulic and
holmium:yag laser ureteroscopic nephrolithotripsy for 20 to 40 mm
renal calculi. J Urol. 172:170–174. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Breda A, Ogunyemi O, Leppert JT and
Schulam PG: Flexible ureteroscopy and laser lithotripsy for
multiple unilateral intrarenal stones. Eur Urol. 55:1190–1196.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Smith R, Khoubehi B and Fuchs G: Occlusion
of the lower calyx by autologuos blood prevents accumulation of
stone fragments at this site after retrograde intra-renal surgery.
Eur Urol. (Suppl 264):2005. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Akman T, Binbay M, Sari E, Yuruk E,
Tepeler A, Akcay M, Muslumanoglu AY and Tefekli A: Factors
affecting bleeding during percutaneous nephrolithotomy: Single
surgeon experience. J Endourol. 25:327–333. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Kukreja R and Desai M, Patel S, Bapat S
and Desai M: Factors affecting blood loss during percutaneous
nephrolithotomy: Prospective study. J Endourol. 18:715–722. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Segura JW, Patterson DE, LeRoy AJ,
Williams HJ Jr, Barrett DM, Benson RC Jr, May GR and Bender CE:
Percutaneous removal of kidney stones: Review of 1,000 cases. J
Urol. 134:1077–1081. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Stoller ML, Wolf JS Jr and St Lezin MA:
Estimated blood loss and transfusion rates associated with
percutaneous nephrolithotomy. J Urol. 152:1977–1981. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Liatsikos EN, Kapoor R, Lee B, Jabbour M,
Barbalias G and Smith AD: ‘Angular percutaneous renal access’.
Multiple tracts through a single incision for staghorn calculous
treatment in a single session. Eur Urol. 48:832–837. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Takazawa R, Kitayama S and Tsujii T:
Successful outcome of flexible ureteroscopy with holmium laser
lithotripsy for renal stones 2 cm or greater. Int J Urol.
19:264–267. 2012. View Article : Google Scholar : PubMed/NCBI
|