Introduction
Accurate assessment of residual hepatic functional
reserve is indispensable for selecting an adequate treatment for
patients with liver cirrhosis, particularly for those with liver
tumors. Several tests have been proposed for determining residual
liver function; however, no single marker is entirely reliable for
predicting residual function, since hepatocytes possess a wide
array of different functions (1,2).
Instead of using a single marker, scoring systems using several
parameters have been developed for assessing hepatic functional
reserve and stratifying the severity of liver cirrhosis. Currently,
the Child-Pugh score is widely accepted as a method to assess liver
function during chronic liver disease, mainly cirrhosis (3,4). The
Child-Pugh scoring system employs five clinical measures; serum
albumin and bilirubin, ascites, encephalopathy and prothrombin time
(PT), while the etiology of cirrhosis is not considered. In other
words, hepatic capacity of protein synthesis is regarded as an
important aspect of the Child-Pugh scoring system, and the
evaluation system works on the assumption that every parameter
worsens in parallel according to the progression of liver fibrosis,
irrespective of the etiology. However, in a previous report
examining prediction factors for variceal hemorrhage, the form of
varices, red color sign and alcoholism were independent risk
factors, whereas Child-Pugh variables were not included as
significant factors (5). The
result indicates that for each cause of cirrhosis, the relationship
between the degree of fibrosis and clinical findings, including the
capacity for protein synthesis, may vary.
In our experience, certain cirrhotic patients
unexpectedly show high serum levels of albumin despite advanced
liver fibrosis. Certain patients with alcoholic cirrhosis who
underwent liver resection for hepatocellular carcinoma (HCC) had
severe post-operational liver failure, even though they were within
the permissible range under pre-evaluation as Child-Pugh class A
with more than 3.5 g/dl of serum albumin. This is perhaps because
the score for evaluating residual liver function was overestimated
due to their serum albumin levels. Therefore, in this study we
assessed hepatic protein synthesis capacity, including serum
albumin levels, in patients with alcoholic cirrhosis and compared
them to those in hepatitis C virus (HCV) infection-induced
cirrhotic patients, which is the most common cause of liver
cirrhosis and HCC. Platelet count was employed as a marker for
liver fibrosis, since it has been previously used for predicting
the progression of fibrosis (6,7) and
can be measured simply and non-invasively.
Materials and methods
From April 2000 to March 2006, 225 outpatients with
compensated liver cirrhosis were seen at the Department of
Hepatology and Pancreatology, Kyushu University Hospital, including
170 HCV-positive patients. We defined an alcoholic patient as one
with a daily consumption of >80 g ethanol for at least 10 years.
Prior to enrolling the patients, patients with HCC, uncontrolled
diabetes (HbA1c >6.5%) or recent appetite loss within 1 month
were excluded. Furthermore, patients who had a splenal longitudinal
size of >15 cm were also excluded. This selection was required
to minimize the influence of malnutrition and extrahepatic
destruction of platelets. After the selection, 45 alcoholic
patients and 88 non-drinkers were identified as HCV-positive
patients, while 30 alcoholic patients and 12 non-drinkers were
identified as HCV-negative patients. For the alcoholic patients,
only those who ceased drinking for at least 2 months were
enrolled.
Finally, 31 alcoholic patients with HCV infection
were enrolled (alcohol + HCV group). Stratification of patients
according to their platelet count showed that the counts were
<5.0×104/μl in 4 patients,
4.9–6.4×104/μl in 7 patients,
6.5–7.9×104/μl in 7 patients,
8.0–9.4×104/μl in 6 patients,
9.5–10.9×104/μl in 3 patients and
>11.0×104/μl in 4 patients. To set a similar
background to that of the alcohol + HCV group, we randomly selected
31 age-, gender-, body mass index (BMI)- and platelet count-matched
non-drinking HCV-positive patients (HCV group). Similarly, we
enrolled 27 HCV-negative alcoholic patients (alcohol group). All
enrolled patients were negative for hepatitis B virus, anti-nuclear
antibody and anti-mitochondrial antibody. The study protocol was
approved by the Ethics Committee of the Kyushu University
Hospital.
All quantitative data are expressed as the means ±
standard deviation. Differences between categorical variables were
analyzed using the Chi-square test. The Student’s t-test was used
for continuous variables. We considered P-values <0.05 to denote
statistical significance.
Results
Regarding the blood testing results, significant
differences were found only for serum γ-glutamyl transpeptidase
(GGT) and albumin levels between the HCV and alcohol + HCV groups
(Table I). There were no
significant differences between the groups in terms of serum
cholinesterase (ChE) and PT, which are general indices of hepatic
protein synthesis capacity as well as albumin. In the alcohol + HCV
group, aspartate aminotransferase and alanine aminotransferase
levels were significantly lower, and the levels of GGT, ChE,
cholesterol and white blood cell counts were significantly higher
compared to the alcohol group. Platelet counts had been adjusted
among the three groups.
 | Table IPatient characteristics. |
Table I
Patient characteristics.
| Alcohol group
(alcohol+/HCV−) | HCV group
(alcohol−/HCV+) | Alcohol + HCV group
(alcohol+/HCV+) |
|---|
| No. of
patients | 27 | 31 | 31 |
| Age (years) | 67.2±7.6 | 68.2±7.9 | 64.2±9.7 |
| Gender
(male/female) | 3/24 | 4/27 | 4/27 |
| BMI
(kg/cm2) | 23.6±0.5 | 23.2±0.6 | 23.4±0.6 |
| Albumin (g/dl) | 3.7±0.1 | 3.2±0.1 | 3.6±0.1a |
| Bilirubin
(mg/dl) | 1.8±0.2 | 1.7±0.2 | 1.3±0.2 |
| AST (U/l) | 44.6±3.8c | 73.1±5.9 | 74.3±6.6 |
| ALT (U/l) | 27.3±1.9d | 57.6±5.3 | 63.4±5.8 |
| LDH (U/l) | 292.8±25.2 | 410.7±37.5 | 356.1±30.2 |
| GGT (U/l) | 195.8±34.0b | 52.7±7.0 | 103.7±15.0a |
| ALP (U/l) | 390.3±41.3 | 452.8±53.0 | 433.7±44.9 |
| ChE (mg/dl) | 103.3±9.1b | 70.9±6.4 | 81.3±5.4 |
| Cholesterol
(mg/dl) | 159.3±5.5b | 136.3±4.7 | 141.9±4.8 |
| PT (%) | 64.7±4.2 | 68.1±2.8 | 66.2±4.1 |
| WBC
(/μl) |
4,444.8±245.8b | 3,647.7±221.0 | 3,637.7±199.4 |
| RBC
(/μl) | 392.6±12.5 | 368.3±9.4 | 373.7±10.0 |
| Hemoglobin
(g/dl) | 12.5±0.4 | 12.0±0.4 | 12.5±0.32 |
| Platelet
(/μl) | 8.2±0.5 | 7.3±0.4 | 7.5±0.5 |
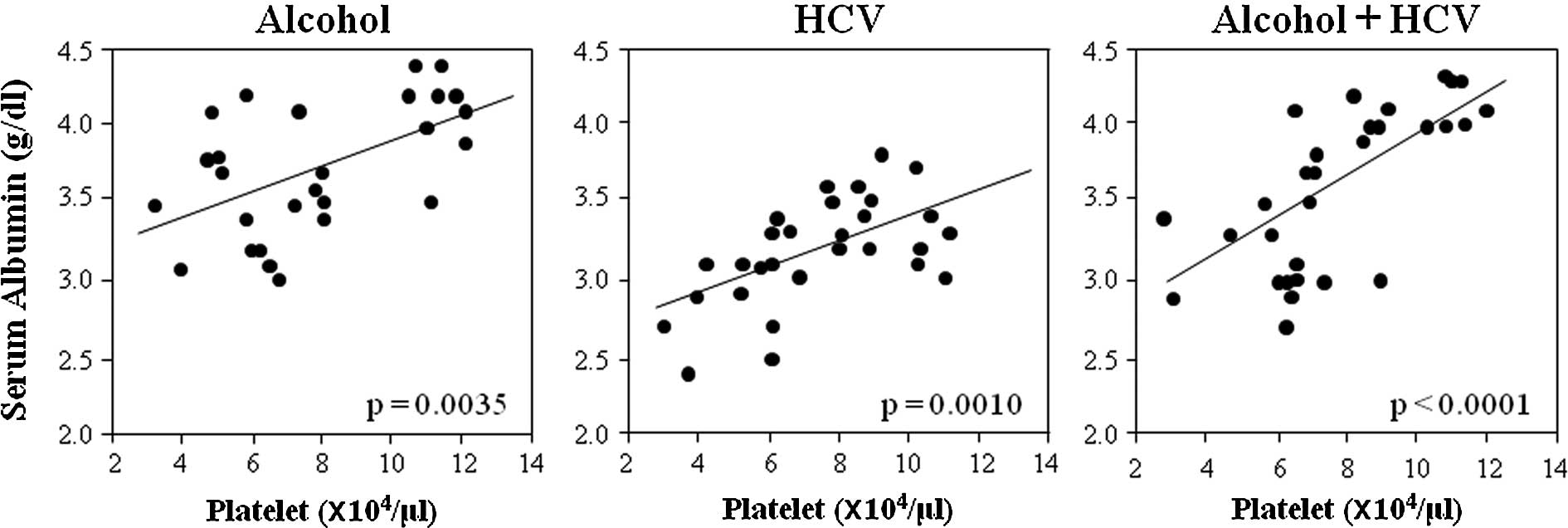
To clarify the relationship between the degree of
liver fibrosis and capacity for protein synthesis, the correlation
between serum albumin levels and platelet counts in the three
groups was examined (Fig. 1). In
each group, albumin levels significantly correlated with platelet
counts. However, albumin levels were always higher in the alcohol
group than in the HCV group, and the difference was ∼0.5 g/dl
irrespective of the platelet count. The approximate correlation
line of the alcohol + HCV group was intermediate between that of
the alcohol and HCV groups.
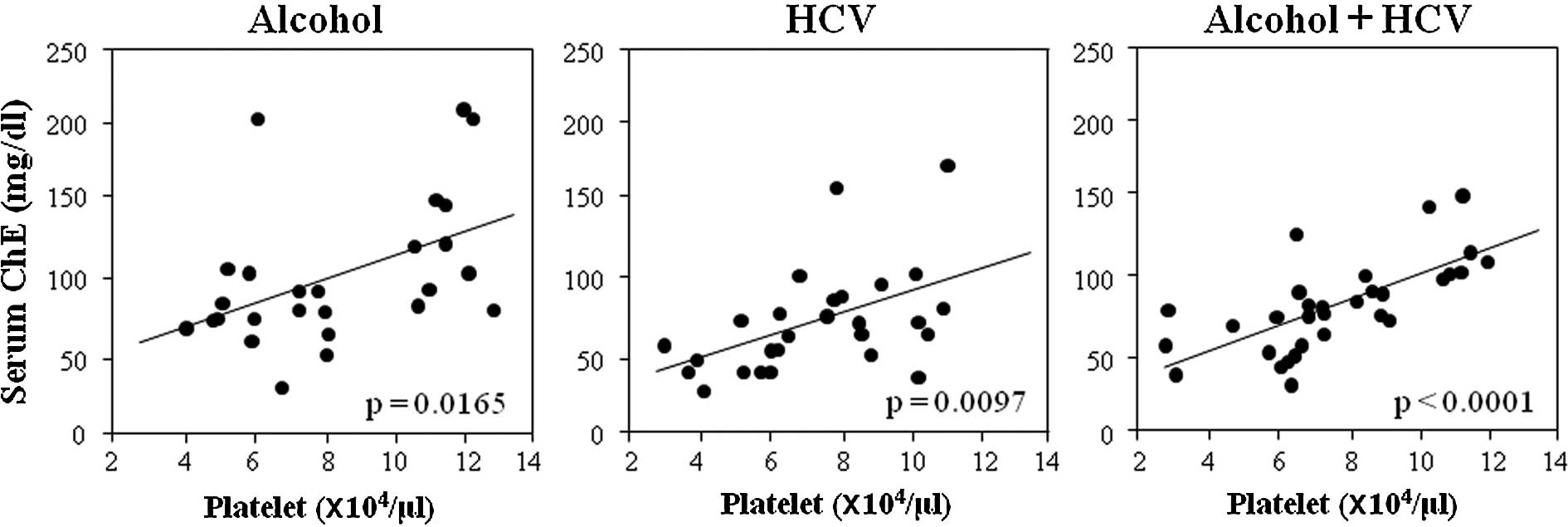
To determine whether the relationship of serum
albumin with platelet counts was also true between other proteins
produced in the liver and platelet counts, we examined the
correlation between serum ChE and platelet counts in each group
(Fig. 2). The correlation between
ChE and platelet counts was significant but, interestingly, the
levels and slope of the approximate correlation lines were almost
similar among the three groups, in contrast to the relationship
between albumin and platelet counts.
Discussion
This study showed that serum albumin levels were
higher in patients with alcoholic cirrhosis than in those with
cirrhosis caused by HCV irrespective of platelet count. These
findings indicate that the hepatic capacity of albumin synthesis
may be affected by the etiology, alcohol or HCV, in addition to the
degree of liver fibrosis. Since protein synthesis is also
influenced by nutritional state (8), careful establishment of the
conditions for enrolling patients was required. We excluded
patients with HCC, uncontrolled diabetes or appetite loss. We also
confirmed that the BMI distribution did not differ between the
groups. Although we used platelet count as a marker of the degree
of liver fibrosis, other methods, such as indocyanine green (ICG)
tests, hyaluronic acid and pathological findings based on liver
biopsy, can also be used. Whichever parameter is used as a liver
fibrosis marker, it should be recognized that each has potential
weaknesses; for example, a decrease in platelet count can be
overestimated in patients with marked splenomegaly (9), ICG tests show higher values when a
portosystemic shunt exists (10),
serum hyaluronic acid levels cannot differentiate fibrotic stage
F1-3 (11) and liver biopsies are
invasive and associated with a risk of sampling error (12,13).
We employed the platelet count as it is a simple and non-invasive
test, and is considerably reliable in patients at an advanced
fibrotic stage (14). Patients
with enlarged spleens (long axis diameter >15 cm) were excluded
to reduce the influence of factors other than liver fibrosis and to
increase its accuracy. Under these conditions, platelet counts
probably reflect the degree of liver fibrosis, an assumption
supported by the fact that platelet counts correlated significantly
with serum albumin and ChE levels in all of the groups.
It is noteworthy that PT and serum ChE levels did
not differ and the relationship between serum ChE and the platelet
count was almost similar among the three groups, indicating that,
irrespective of the etiology, hepatocytic products other than
albumin decrease equally according to the progression of liver
fibrosis. Practically, the evaluation of the hepatic functional
reserve of the patients may not yield reliable results if only
albumin values are considered and the etiology of cirrhosis is
ignored. Our results raise questions as to why patients with
alcoholic cirrhosis would have higher serum albumin levels than
those with cirrhosis caused by HCV-infection. The role of HCV
itself can be excluded as a significant difference was observed in
albumin levels between the HCV and alcohol + HCV groups. Previous
studies have suggested that alcohol can directly influence albumin
synthesis. Annoni et al reported that patients with
alcoholic cirrhosis showed significantly higher hepatic albumin
mRNA levels than patients with a similar histological degree of
cirrhosis due to viral infection (15). However, the alcoholic patients
enrolled in the present study had stopped drinking at least 2
months prior to evaluation. Therefore, the possibility that alcohol
or its metabolic products directly influenced the expression of
albumin mRNA may be questionable. Other pathological differences
may have contributed to the disparity in albumin synthesis, for
example, the distinctive pathological characteristics of alcoholic
cirrhosis, such as pericellular and perivenular fibrosis, Mallory
bodies, steatosis and micronodular regeneration. Further
investigations are required to determine the effect of these
pathologies on albumin synthesis.
The present study demonstrated that the capacity for
hepatic albumin synthesis in cirrhotic patients was differentially
affected by the etiology of alcohol. Since serum albumin levels are
commonly used as an important marker of hepatic functional reserve,
ignoring the etiology of cirrhosis may lead to an incorrect
evaluation. Serum albumin levels were present at higher levels and
Child-Pugh scoring is likely to overestimate the residual hepatic
functional reserve in patients with alcoholic cirrhosis. Therefore,
alcohol consumption should be carefully considered when evaluating
hepatic functional reserve.
Abbreviations:
|
BMI
|
body mass index;
|
|
ChE
|
cholinesterase;
|
|
GGT
|
γ-glutamyl transpeptidase;
|
|
HCC
|
hepatocellular carcinoma;
|
|
HCV
|
hepatitis C virus;
|
|
ICG
|
indocyanine green;
|
|
PT
|
prothrombin time
|
References
|
1.
|
A Di SarioG FeliciangeliE BendiaA
BenedettiDiagnosis of liver fibrosisEur Rev Med Pharmacol
Sci811182004
|
|
2.
|
EJ MullinMS MetcalfeGJ MaddernHow much
liver resection is too much?Am J
Surg1908797200510.1016/j.amjsurg.2005.01.04315972178
|
|
3.
|
J FazakasT MandliG TherEvaluation of liver
function for hepatic resectionTransplant
Proc38798800200610.1016/j.transproceed.2006.01.04816647474
|
|
4.
|
PD SchneiderPreoperative assessment of
liver functionSurg Clin North
Am84355373200410.1016/S0039-6109(03)00224-X
|
|
5.
|
DK ParkSH UmJW LeeClinical significance of
variceal hemorrhage in recent years in patients with liver
cirrhosis and esophageal varicesJ Gastroenterol
Hepatol1910421051200415304123
|
|
6.
|
X FornsS AmpurdanèsJM LlovetIdentification
of chronic hepatitis C patients without hepatic fibrosis by a
simple predictive
modelHepatology36986992200210.1053/jhep.2002.3612812297848
|
|
7.
|
CT WaiJK GreensonRJ FontanaJD
KalbfieischJA MarreroHS ConjeevaramAS LokA simple noninvasive index
can predict both significant fibrosis and cirrhosis in patients
with chronic hepatitis
CHepatology38518516200310.1053/jhep.2003.5034612883497
|
|
8.
|
F MangusoG D’AmbraA MenchiseR SollazzoL
D’AgostinoEffects of an appropriate oral diet on the nutritional
status of patients with HCV-related liver cirrhosis: a prospective
studyClin Nutr24751759200510.1016/j.clnu.2005.02.01016182039
|
|
9.
|
H WadenvikI DenforsJ KuttiSplenic blood
flow and intrasplenic platelet kinetics in relation to spleen
volumeBr J Haematol6718118519873676106
|
|
10.
|
K IzunoS FujiyamaJ ShibataK YoshidaT SatoO
ShimomuraM TakahashiTransrectal portal scintigraphy with I123
iodoamphetamine in liver
diseasesHepatogastroenterology38S8S111991
|
|
11.
|
C TatsumiM KudoK UeshimaNoninvasive
evaluation of hepatic fibrosis using serum fibrotic markers,
transient elastography (FibroScan) and real-time tissue
elastographyIntervirology512733200810.1159/000122602
|
|
12.
|
J PoniachikDE BernsteinKR ReddyLJ
JeffersME Coelho-LittleF CivantosER SchiffThe role of laparoscopy
in the diagnosis of cirrhosisGastrointest
Endosc43568571199610.1016/S0016-5107(96)70192-X8781934
|
|
13.
|
A RegevM BerhoLJ JeffersSampling error and
intra-observer variation in liver biopsy in patients with chronic
HCV infectionAm J
Gastroenterol9726142618200210.1111/j.1572-0241.2002.06038.x12385448
|
|
14.
|
RJ FontanaZG GoodmanJL
DienstagRelationship of serum fibrosis markers with liver fibrosis
stage and collagen content in patients with advanced chronic
hepatitis CHepatology47789798200810.1002/hep.2209918175357
|
|
15.
|
G AnnoniFR WeinerM ColomboMJ CzajaMA
ZernAlbumin and collagen gene regulation in alcohol- and
virus-induced human liver
diseaseGastroenterology9819720219902293578
|