Introduction
Gorham-Stout syndrome (GSS) is a rare disorder
characterized by progressive osteolysis. It was first described in
1838 by Jackson who reported an 18-year-old boy with advanced
osteolysis of the humerus (1). In
1955, Gorham and Stout developed histopathological criteria of the
disease based on their own experience and the literature findings
as follows: ‘Gorhams’s disease is usually associated with an
angiomatosis of blood vessels and sometimes of lymphatic vessels,
which seemingly are responsible for it’ (2). Currently, approximately 200 cases
have been published in the literature to date (3). The majority of cases occur in
children and young adults. The clinical presentations are variable
and depend on the sites of involvement. GSS most commonly involves
the skull, shoulder and pelvic girdle. It rarely involves the bones
of the entire body. Thus, we report the case of a girl, 5 years of
age presenting with GSS and describe the clinical manifestation,
radiological features and histopathological characteristics of GSS
and discuss its pathogenetic mechanism, diagnosis and
treatment.
Case report
A 5-year-old girl was referred to a local hospital
in 2009 due to back pain with a duration of 3 months. Chest X-ray
showed the existence of hydrops in the left thoracic cavity, and
tuberculous pleuritis was diagnosed. However, treatment with
anti-tuberculosis therapy was ineffective. A soft mass with
significant tenderness was noted in the upper segment of right leg
50 days afterward. Thus, the patient presented at our hospital in
order to further obtain an accurate diagnosis and receive
treatment. X-ray revealed multiple osteolysis of the bilateral
clavicle, bilateral scapula, the 4th, 5th, 9th, 10th right ribs,
the 2th and 6th-10th left ribs, the third, fourth and fifth lumbar
vertebra, right ilium, sacrum, bilateral femur and right tibia
(Fig. 1). Laboratory test results
included the following: white blood cell count, 8610/μl;
hemoglobin, 8.8 g/dl; platelets, 52×103/μl;
elevated inorganic phosphorus level (1.98 mmol/l). Other laboratory
biochemical and hematological tests, including alkaline
phosphatase, lactate dehydrogenase, hydroxybutyrate dehydrogenase
and cholesterin were normal. In order to further elucidate the
diagnosis, a biopsy from the right tibia was obtained and analyzed.
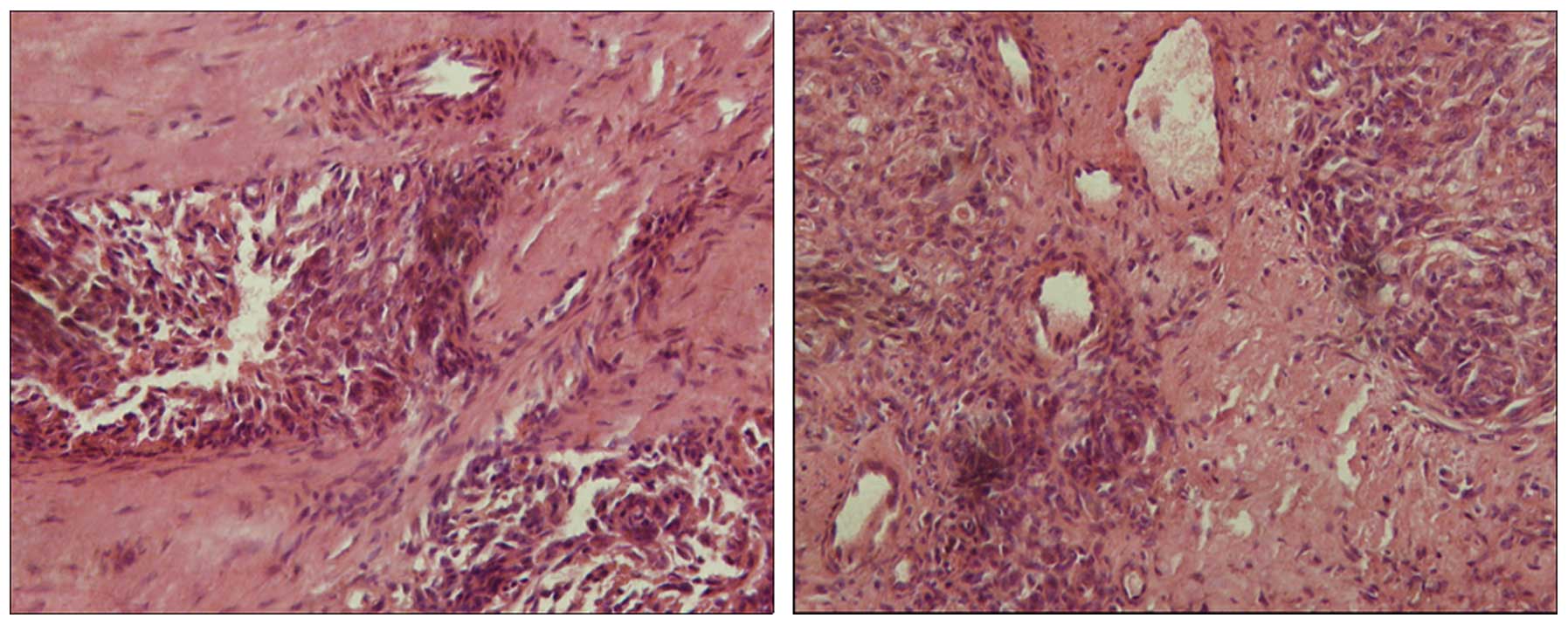
The result disclosed that the lesion was composed of hyperplastic
blood vessels and fibrous tissues (Fig. 2), and that the hyperplastic blood
vessels were divided into nested structure by fibrous tissues,
similar to hemangioma. Moreover, osseous tissues were absent. Based
on the above clinical, radiological and histopathological findings,
the clinical physician confirmed a diagnosis of Gorham-Stout
disease, and prescribed oral anti-osteoclastic medication
consisting of bisphosphonates. Three years after the initial
operation there was no evidence of new osteolysis.
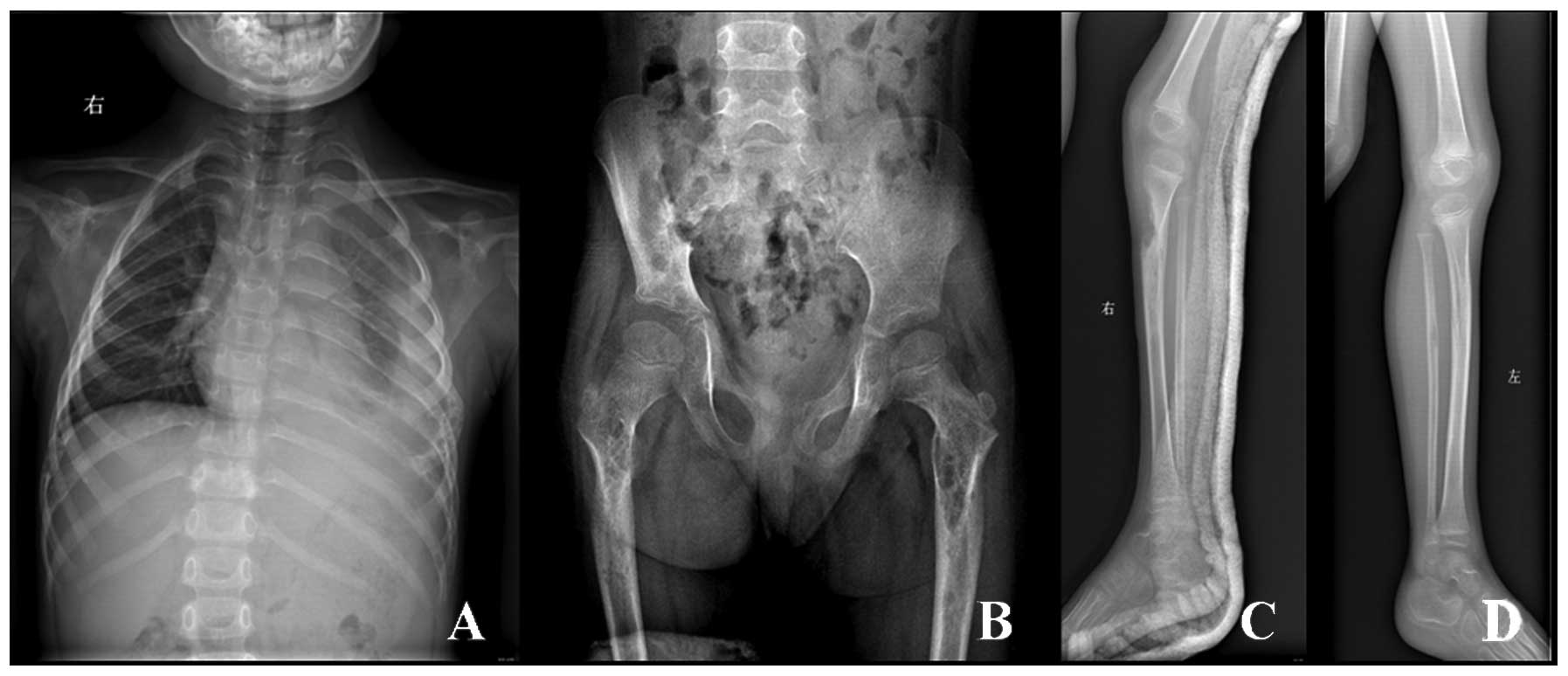 | Figure 1(A) X-ray reveals multiple osteolysis,
including bilateral clavicle, bilateral scapula, the 4th, 5th, 9th,
10th right ribs, the 2th and 6th-10th left ribs, the third, fourth
and fifth lumbar vertebra, (B) right ilium, sacrum, bilateral
femur, (C) right tibia, and (D) left tibia was normal as
control. |
Discussion
Gorham-Stout sydrome (GSS) is a rare disorder
characterized by progressive osteolysis with invasion of the
surrounding soft tissue. It can occur at any age, but is more
common in adolescents and young adults (4). There is no racial predilection
(4,5). The peak incidence is in the second
and third decades of life (5,6) and
males are more affected than females (3,6). It
may involve different regions of the skeleton, such as the pelvis,
clavicle, spine, ribs and facial skeleton. Maxillomandibular
lesions are more frequently described when there is associated
craniofacial involvement (7).
The exact pathogenetic mechanism of Gorham-Stout
syndrome is still unknown. There is controversy even over the
presence or absence of osteoclasts in the condition.
Heffez et al (5) concluded that osteolysis is due to an
increased number of stimulated osteoclasts, and suggested that
antiresorptive therapy, for example with bisphosphonates or
calcitonin, started in an early phase of the disease could lead to
a dramatic improvement in the treatment of progressive osteolytic
changes.
The diagnosis of GSS is difficult, particularly in
the early stage. It is often misdiagnosed as a neoplasm,
pathological fracture, chylothorax or chronic osteomyelitis due to
its rarity and bizarre clinical characteristics. GSS occurs in bone
and most commonly involves the scapula, clavicle, humerus, thoracic
vertebra and rib, and subsequently the lesion gradually involves
neighboring bone and surrounding soft tissues. Limb pain,
non-shoring physical strength and dysfunction are the main
symptoms. X-ray reveals osteolysis. The pathological process is the
replacement of normal bone by an aggressively expanding but
non-neoplastic vascular tissue, similar to a hemangioma or
lymphangioma. Widely proliferating neovascular tissue causes
massive bone loss. The clinical presentation consists of pain or
pathological fracture. The patient we present is a 5-year-old girl,
who presented initially with pain in her back, and subsequently
multifocal osteolysis was found. The biopsy revealed that the
lesion was composed of hyperplastic blood vessels and fibrous
tissues, and the hyperplastic blood vessels were divided into
nested structure by fibrous tissues, similar to hemangioma.
Moreover, laboratory test results showed that alkaline phosphatase
and calcium were normal, whereas inorganic phosphorus was elevated.
Thus, hyperparathyroidism caused by the developmental and metabolic
disorder of calcium and phosphorus should not be considered. In
addition, according to the following diagnostic criteria suggested
by Heffez et al (5) which
include i) a positive biopsy for angiomatous tissue; ii) absence of
cellular atypia; iii) minimal or no osteoblastic response and
absence of dystrophic calcification; iv) evidence of local
progressive osseous resorption; v) nonexpansile, nonulcerative
lesion; vi) absence of visceral involvement; vii) an osteolytic
radiographic pattern; and viii) negative hereditary, metabolic,
neoplastic, immunologic, or infectious etiology, the diagnosis of
Gorham-Stout disease was confirmed. Of course, other diseases,
including disuse atrophy, acute inflammatory atrophy associated
with trauma, primary and metastatic tumors and osteomyelitis, may
be excluded based on clinical history, laboratory test results,
radiological examination and histopathological findings.
There is no standard therapy available for GSS. A
number of different treatments have been proposed, with a huge
variation in long-term results (9–12).
The prognosis is highly variable and unpredictable, ranging from
minimal disability to mortality, depending on the site of
involvement, extent of the disease and presence of complications.
At present, the treatment for GSS includes radiation therapy,
anti-osteoclastic medications (bisphosphonates) and α-2b
interferon. Lehmann et al (8) reported that long-term bisphosphonate
therapy for over 17 years was feasible and could contribute to
clinical stabilization in GSS. Moreover, surgical treatment options
include resection of the lesion and reconstruction using grafts
and/or prostheses. Our patient continued to receive oral
anti-osteoclastic medication consisting of bisphosphonates. Three
years after the initial operation, there is no evidence of new
osteolysis. The patient attends school normally.
Acknowledgements
This study was supported by the
National Natural Science Foundation of China (30800417).
References
|
1.
|
Escande C, Schouman T, Françoise G, et al:
Histological features and management of a mandibular Gorham
disease: a case report and review of maxillofacial cases in the
literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod.
106:e30–e37. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2.
|
Gorham LW and Stout AP: Massive osteolysis
(acute spontaneous absorption of bone, phantom bone, disappearing
bone): its relation to hemangiomatosis. J Bone Joint Surg Am.
37:985–1004. 1955.PubMed/NCBI
|
|
3.
|
Hagberg H, Lamberg K and Astrom G:
Alpha-2b interferon and oral clodronate for Gorham’s disease.
Lancet. 350:1822–1823. 1997.PubMed/NCBI
|
|
4.
|
Hammer F, Kenn W, Wesselmann U, et al:
Gorham-Stout disease: stabilization during bisphosphonate
treatment. J Bone Miner Res. 20:350–353. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5.
|
Heffez L, Doku HC, Carter BL, et al:
Perspectives on massive osteolysis: report of a case and review of
literature. Oral Surg Oral Med Oral Pathol. 55:331–343. 1983.
View Article : Google Scholar : PubMed/NCBI
|
|
6.
|
Holroyd I, Dillon M, Roberts GJ, et al:
Gorham’s disease: a case (including dental presentation) of
vanishing bone disease. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod. 89:125–129. 2000.
|
|
7.
|
Jackson JBS: A boneless arm. Boston Med
Surg J. 18:368–369. 1838.
|
|
8.
|
Lehmann G, Pfeil A, Böttcher J, et al:
Benefit of a 17-year long-term bisphosphonate therapy in a patient
with Gorham-Stout syndrome. Arch Orthop Trauma Surg. 129:967–972.
2009.PubMed/NCBI
|
|
9.
|
Moller G, Priemel M, Amling M, et al: The
Gorham-Stout syndrome (Gorham’s massive osteolysis), a report of
six cases with histopathological findings. J Bone Joint Surg Br.
81:501–506. 1999.
|
|
10.
|
Oujilal A, Lazrak A, Benhalima H, et al:
Massive lytic osteodystrophy or Gorham-Stout disease of the
craniomaxillofacial area. Rev Laryngol Otol Rhinol (Bord).
121:255–260. 2000.PubMed/NCBI
|
|
11.
|
Paley MD, Lloyd CJ and Penfold CN: Total
mandibular reconstruction for massive osteolysis of the mandible
(Gorham-Stout syndrome). Br J Oral Maxillofac Surg. 43:166–168.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
12.
|
Patel DV: Gorham’s disease or massive
osteolysis. Clin Med Res. 3:65–74. 2005.
|