Introduction
Acute pulmonary embolism (PE) is a major challenge
for emergency facilities. On average, 90% of all mortalities occur
within 2 h of the onset of the symptoms (1). Therefore, the rapid treatment of
fulminant PE is a high priority. The optimization of emergency
structures has been demonstrated to significantly reduce the
mortality rate from unstable PE (2).
The reliable exclusion of PE in hemodynamically stable patients
remains an additional problem, since in a number of these patients,
the symptoms of PE are barely evident or manifest in an atypical
manner. Previous studies have shown that PE has been frequently
overlooked as a result, and that the mortality rate in such cases
is significantly increased (3,4). The
most important diagnostic method in suspected cases of PE is
computed tomography (CT) scans of the pulmonary artery (5,6).
In 2008, the European Society of Cardiology (ESC)
published guidelines for the diagnosis and management of PE
(7). These recommendations were
based on risk stratification using scores, such as the Wells and
Geneva scores (8–10). The most important consequence of the
ESC guidelines was a low-threshold indication for CT to take into
account the diagnostic uncertainty, as aforementioned. The clinical
significance of various factors within the guidelines has been
discussed controversially by certain authors (11). Furthermore, the risk of overdiagnosis
via the detection of an increasing number of clinically-unapparent
subsegmental PEs is similarly controversial.
Overall, despite the publication of ESC guidelines,
there remains uncertainty with regard to the risk assessment of PE.
Against this background, patients with a suspected PE who were
admitted to the Emergency Department of the University Medical
Center Mannheim (Mannheim, Germany) in 2010 and 2011 were
retrospectively studied and the collected data were published in a
previous study (12). The focus of
that study was on the incidence rate of PE in cases with
low-threshold CT indications and the significance of the laboratory
diagnostic markers, troponin and D-dimers (12). Patients with the cardinal symptoms of
chest pain, dyspnoea and syncope were included, since these
symptoms have been frequently observed in patients with a PE in
previous studies (13–17).
The aim of the present study was to address the
significance of PE risk factors in the patient collective, as
aforementioned. In terms of the risk profile of PE, various factors
have been proposed by previous studies, including a prior PE or a
history of deep vein thrombosis (DVT), obesity, smoking, use of
oral contraceptives, thrombophilia, recent long distance flying,
malignant disease and immobilization (18–21).
However, in general, the patient collectives studied have been
small and of heterogeneous quality. Therefore, accurate evaluation
of the risk profile in cases suspected of a PE may be important in
the context of the current ESC recommendations and in light of the
uncertainties described.
Materials and methods
Study population
In the study, the medical records of 492 patients
who were admitted to the Emergency Department of the University
Hospital of Mannheim in the period between April 2010 and July 2011
were retrospectively analyzed. Due to the retrospective nature of
the study protocol, the institutional ethical review board of the
University Medical Center Mannheim waived the requirement for
informed patient consent. All the patients presented with cardinal
symptoms of chest pain, dyspnoea or syncope, and tested positive
for the D-dimer test for PE exclusion. The patients were
hemodynamically stable and met the criteria of a low or moderate
probability of PE, according to the Wells score (10).
The specific risk profile of all the patients was
documented following their admission to the Emergency Department.
In the documentation, a number of factors, including obesity,
smoking, use of contraceptives, immobility level, history of
malignant disease and thrombophilia, family history, history of
DVT/PE, long-distance flying <1 week prior to admission and
surgery during the four preceding weeks, were recorded.
Furthermore, the diagnosis standard comprised a
physical examination and a 12-lead electrocardiography (GE MAC 1200
ST; GE Healthcare, Freiburg, Germany). As laboratory risk markers,
the levels of D-dimers (TINA-quant; Roche Diagnostics, Mannheim,
Germany), as a parameter of acute coagulation activation, and
high-sensitivity troponin (Siemens Healthcare Diagnostics,
Eschborn, Germany), a marker of cardiac cell death, were
determined. In the case of the presence of any of the described
cardinal symptoms in combination with a positive D-dimer test, a
pulmonary artery CT examination (Somatom Emotion, Siemens Medical
Solutions, Forchheim, Germany) was performed. CT was considered a
contraindication for pregnant women and patients with contrast
medium allergy, higher-grade renal insufficiency (creatinine level
of >1.5 mg/dl) or hyperthyroidism, as well as in cases of
ongoing metformin therapy. In patients with these
contraindications, no acute CT examination was performed.
Statistical analysis
For statistical analysis, JMP 9.0.0 (SAS Institute,
Inc., Cary, NC, USA), MedCalc 12.7.0 (MedCalc Software bvba,
Ostend, Belgium) and Forest Plot Viewer 1.0 (National Institute of
Environmental Health Sciences, Durham, NC, USA) software packages
were used. Nominal variables are depicted as numbers (percentages).
For each continuous variable, the Shapiro-Wilk test was applied to
assess for Gaussian distribution of the data. Parametric and
nonparametric continuous variables are expressed as the mean ±
standard deviation and as the median (1st and
3rd quartiles), respectively. Furthermore, value ranges
(minimum and maximum) were presented. As a measure for the
quantitative estimation of the risk of PE in cases with the
presence of a risk factor, the odds ratio (OR) and the 95%
confidence interval (CI) were calculated. A value of P<0.05,
based on two-sided significance testing, was considered to indicate
a statistically significant difference.
Results
Patient characteristics
Baseline characteristics of the patients are
summarized in Table I. The specific
risk profiles of the 492 patients with a suspected PE, including
the number and percentage of patients (n, %) and the single risk
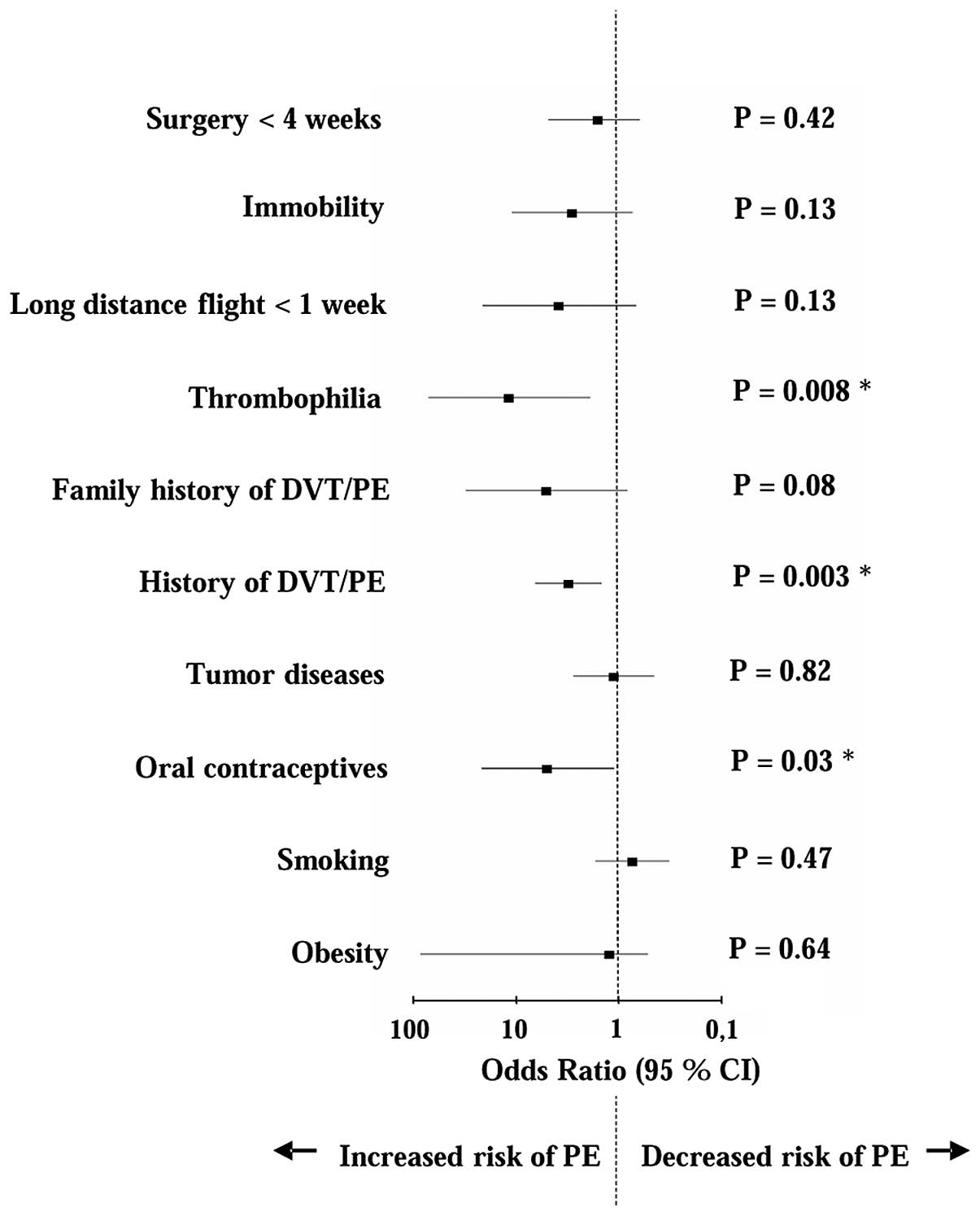
factor ORs for the presence of PE, are listed in Table II. As shown in Fig. 1, the ORs were compared in the form of
a Forest plot graph. The risk of PE was significantly increased
with each of the following factors: Thrombophilia (OR, 11.5,
P=0.008), use of contraceptives (OR, 4.9, P=0.03) and history of
DVT/PE (OR, 3.08, P=0.003). Surgery <4 weeks previously (OR,
1.58, P=0.42), immobility level (OR, 2.84, P=0.13) and
long-distance flying <1 week previously (OR, 3.78, P=0.13), as
well as family history of DVT/PE (OR, 5.03, P=0.08), neoplastic
disease (OR, 1.11, P=0.82) and obesity (OR, 1.22, P=0.64) were
shown to increase the risk of PE; however, the difference was not
statistically significant. In the comprised collective, smoking was
not found to be associated with an increased risk of PE (OR, 0.73,
P=0.47).
 | Table I.Baseline characteristics of 492
patients with a suspected pulmonary embolism. |
Table I.
Baseline characteristics of 492
patients with a suspected pulmonary embolism.
| Characteristic | All patients
(n=492) |
|---|
| Age, years |
|
| Mean
±SD | 68±17 |
|
Range | 19–105 |
| Gender, n (%) |
|
| Male | 218 (44) |
|
Female | 274 (56) |
| Symptoms, n (%) |
|
| Chest
pain | 257 (52) |
|
Dyspnoea | 281 (57) |
|
Syncope | 81 (16) |
| Heart rate, bpm |
|
| Mean ±
SD | 86±22 |
|
Range | 49–175 |
| Systolic blood
pressure, mmHg |
|
| Mean ±
SD | 147±29 |
|
Range | 90–290 |
| Diastolic blood
pressure, mmHg |
|
| Mean ±
SD | 80±15 |
|
Range | 40–150 |
| Oxygen saturation,
% |
|
| Mean ±
SD | 96±4 |
|
Range | 70–100 |
| Table II.Risk factors in patients (n=492) with
a suspected PE. |
Table II.
Risk factors in patients (n=492) with
a suspected PE.
| Risk factor | Cases, n (%) | OR | 95% CI | P-value |
|---|
| Obesity | 50 (10.2) | 1.22 | 0.52–85 | 0.64 |
| Smoking | 74 (15.0) | 0.73 | 0.32–1.69 | 0.47 |
| Oral
contraceptives | 8 (1.6) | 4.90 | 1.11–21.59 | 0.03a |
| Tumor diseases | 46 (9.3) | 1.11 | 0.45–2.75 | 0.82 |
| History of
DVT/PE | 41 (8.3) | 3.08 | 1.45–6.54 | 0.003a |
| Family history of
DVT/PE | 5 (1.0) | 5.03 | 0.82–30.74 | 0.08 |
| Thrombophilia | 5 (1.0) | 11.50 | 1.89–70.60 | 0.008a |
| Long distance flight
<1 week | 6 (1.2) | 3.78 | 0.67–21.01 | 0.13 |
| Immobility | 11 (2.2) | 2.84 | 0.73–11.04 | 0.13 |
| Surgery <4
weeks | 23 (4.7) | 1.58 | 0.62 to 4.83 | 0.42 |
Discussion
In hemodynamically stable patients, the optimal
workflow for the exclusion of a PE remains subject to uncertainty.
The ESC guidelines for PE published in 2008 took this into account
by recommending a low-threshold CT indicator for patients with a
suspected PE. However, this strategy is considered controversially
with regard to the possibility of overdiagnosis of patients, such
as by the detection of unapparent subsegmental PEs. Therefore,
relevant criteria for further optimization of the risk assessment
of these patients is required.
Traditionally, risk factors play an important role
in the diagnostic workup of patients with cardiovascular disease.
In acute coronary syndrome, for example, the risk factors of
coronary heart disease are mapped by relevant scores, such as the
Thrombolysis In Myocardial Infarction score (criterion, ≥3 risk
factors) (22). Similarly, with
regard to PE, a number of risk factors are known, as previously
described. However, the Wells score considers only the factors of
immobilization or surgery <4 weeks previously, prior history of
DVT or PE and malignant disease <6 months previously (10). In addition, the Geneva score only
includes the criteria of a prior history of DVT or PE, surgery or
fracture <4 weeks previously and active malignancy (9). Other parameters, including obesity,
smoking, use of oral contraceptives, thrombophilia and recent long
distance flying, are described in the literature; however, are not
included into the scores recommended by the ESC (18–21).
Therefore, the predictive value of considering these risk factors
in the context of modern PE diagnostics is yet to be
determined.
The aim of the present study was to re-evaluate the
risk factors of PE in their entirety, and particularly in synopsis
with the ESC recommendations published in 2008 and updated in 2014.
The current study met the low-threshold indicators for CT, as
demanded by the ESC, and thus the modern requirements of PE
diagnosis. The results of the present study demonstrated a
significant risk of PE for the criterion of contraceptive use and a
highly significant risk of PE for the parameters of a history of
DVT/PE and thrombophilia. History of DVT/PE is included in the two
previously mentioned scoring systems within the ESC guidelines. By
contrast, the factors of contraceptive use and thrombophilia are
not included in the Wells or Geneva scores. This diagnostic
deficiency is, however, difficult to assess. The association
between oral contraceptives and PE is established, although only a
limited number of studies address the issue (20,23). Of
these, the study by Lauque et al comprised only 11 case
reports and is not recent (20).
Significantly more data exist with regard to the association
between DVT and contraceptive use. A meta-analysis by Manzoli et
al included a considerable number of studies and confirmed a
significantly increased risk of thrombosis with oral contraceptive
use (23). Despite the wealth of
data, the results concerning DVT cannot be transferred directly to
PE. Nevertheless, the association between oral contraceptives and
PE remains undisputed. With regard to the association between
thrombophilia and PE, the data of the Lauque et al study are
similarly weak. Data from a large retrospective study by Wu et
al indicated a significantly increased risk of PE associated
with different thrombophilia subgroups; the risk increased further
upon concomitant intake of contraceptives (24). Thus, the risk factors of
contraceptive use and thrombophilia, in addition to a history of
DVT/PE, are of significant importance in the context of PE.
In conclusion, the results of the present study
demonstrate that emphasis should be focused on the risk factors of
contraceptive use, thrombophilia and a history of DVT/PE, in
addition to previously used diagnostic parameters, such as D-dimer
testing, in the overall assessment of PE risk. Patients with a
suspected PE and at least one of the aforementioned risk factors
should be referred for CT diagnosis even in the absence of elevated
levels of D-dimers, since a number of PE cases that tested negative
for D-dimer have been reported (25).
References
|
1
|
Walther A and Böttiger BW: Pulmonary
embolism. Wien Med Wochenschr. 158:610–614. 2008.[(In German)].
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Horlander KT, Mannino DM and Leeper KV:
Pulmonary embolism mortality in the United States, 1979–1998: an
analysis using multiple-cause mortality data. Arch Intern Med.
163:1711–1717. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Goldhaber SZ: Pulmonary embolism. Lancet.
363:1295–1305. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kline JA, Hernandez-Nino J, Jones AE, Rose
GA, Norton HJ and Camargo CA Jr: Prospective study of the clinical
features and outcomes of emergency department patients with delayed
diagnosis of pulmonary embolism. Acad Emerg Med. 14:592–598. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mullins MD, Becker DM, Hagspiel KD and
Philbrick JT: The role of spiral volumetric computed tomography in
the diagnosis of pulmonary embolism. Arch Intern Med. 160:293–298.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Perrier A, Howarth N, Didier D, et al:
Performance of helical computed tomography in unselected
outpatients with suspected pulmonary embolism. Ann Intern Med.
135:88–97. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Torbicki A, Perrier A, Konstantinides S,
et al: ESC Committee for Practice Guidelines (CPG): Guidelines on
the diagnosis and management of acute pulmonary embolism: the Task
Force for the Diagnosis and Management of Acute Pulmonary Embolism
of the European Society of Cardiology (ESC). Eur Heart J.
29:2276–2315. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Douma RA, Mos IC, Erkens PM, et al:
Performance of 4 clinical decision rules in the diagnostic
management of acute pulmonary embolism: a prospective cohort study.
Ann Intern Med. 154:709–718. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Le Gal G, Righini M, Roy PM, Sanchez O,
Aujesky D, Bounameaux H and Perrier A: Prediction of pulmonary
embolism in the emergency department: the revised Geneva score. Ann
Intern Med. 144:165–171. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wells PS, Anderson DR, Rodger M, et al:
Derivation of a simple clinical model to categorize patients
probability of pulmonary embolism: increasing the models utility
with the SimpliRED D-dimer. Thromb Haemost. 83:416–420.
2000.PubMed/NCBI
|
|
11
|
Young MD, Daniels AH, Evangelista PT, et
al: Predicting pulmonary embolus in orthopedic trauma patients
using the wells score. Orthopedics. 36:e642–e647. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gruettner J, Walter T, Bolte M, Haghi D,
Sudarski S and Henzler T: Incidence of pulmonary embolism in an
emergency department cohort evaluated with a simple symptom-based
diagnostic algorithm. In Vivo. 27:215–220. 2013.PubMed/NCBI
|
|
13
|
Calvo-Romero JM, Pérez-Miranda M and
Bureo-Dacal P: Syncope in acute pulmonary embolism. Eur J Emerg
Med. 11:208–209. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Castelli R, Tarsia P, Tantardini C,
Pantaleo G, Guariglia A and Porro F: Syncope in patients with
pulmonary embolism: comparison between patients with syncope as the
presenting symptom of pulmonary embolism and patients with
pulmonary embolism without syncope. Vasc Med. 8:257–261. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Koutkia P and Wachtel TJ: Pulmonary
embolism presenting as syncope: case report and review of the
literature. Heart Lung. 28:342–347. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Miniati M, Prediletto R, Formichi B, et
al: Accuracy of clinical assessment in the diagnosis of pulmonary
embolism. Am J Respir Crit Care Med. 159:864–871. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wolfe TR and Allen TL: Syncope as an
emergency department presentation of pulmonary embolism. J Emerg
Med. 16:27–31. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Goldhaber SZ, Grodstein F, Stampfer MJ, et
al: A prospective study of risk factors for pulmonary embolism in
women. JAMA. 277:642–645. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kline JA and Miller DW: Risk
stratification for acute pulmonary embolism. J Natl Compr Canc
Netw. 9:800–810. 2011.PubMed/NCBI
|
|
20
|
Lauque D, Mazières J, Rouzaud P, et al:
Pulmonary embolism in patients using estrogen-progestagen
contraceptives. Presse Med. 27:1566–1569. 1998.[(In French)].
PubMed/NCBI
|
|
21
|
Lehmann R, Suess C, Leus M, et al:
Incidence, clinical characteristics and long-term prognosis of
travel-associated pulmonary embolism. Eur Heart J. 30:233–241.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Antman EM, Cohen M, Bernink PJ, et al: The
TIMI risk score for unstable angina/non-ST elevation MI: A method
for prognostication and therapeutic decision making. JAMA.
284:835–842. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Manzoli L, De Vito C, Marzuillo C, Boccia
A and Villari P: Oral contraceptives and venous thromboembolism: a
systematic review and meta-analysis. Drug Saf. 35:191–205.
2012.PubMed/NCBI
|
|
24
|
Wu O, Robertson L, Twaddle S, et al:
Screening for thrombophilia in high-risk situations: systematic
review and cost-effectiveness analysis. The thrombosis: risk and
economic assessment of thrombophilia screening (TREATS) study.
Health Technol Assess. 10:100–110. 2006. View Article : Google Scholar
|
|
25
|
Breen ME, Dorfman M and Chan SB: Pulmonary
embolism despite negative ELISA D-dimer: a case report. J Emerg
Med. 37:290–292. 2009. View Article : Google Scholar : PubMed/NCBI
|