Introduction
In prostate cancer the bone marrow is the most
common site involved by metastatic tumors. The diagnosis of
metastatic involvement of bone marrow may therefore have a profound
effect on the prognosis and treatment of the individual patient.
However, the bone marrow may be involved by the tumor without any
abnormalities recognized in conventional imaging studies, bone
scans, serum biochemistry and/or hematological parameters.
Biochemical failure after radical prostatectomy is defined by the
NCCN 2012 guidelines (1) as a
serum prostate-specific antigen (PSA) >0.2 ng/ml, with patients
having a 100% (95% CI, 87–100) 3-year risk of PSA progression
(2). However, in men with
biochemical failure after radical prostatectomy for prostate cancer
and with a negative bone scan, treatment is often empirically
based.
The presence of PSA-positive cells in bone marrow
aspirates (BMAs) has been used to indicate the presence of
micrometastasis. There is an association with tumor stage, Gleason
score and time to biochemical failure (3–6).
However, these cells may not represent true micrometastasis
(7) and may have more in common
with circulating prostate cells (CPCs) detected in the blood. The
presence of disseminated tumor cells (DTCs) when used to define
systemic dissemination after biochemical failure has clinical
importance and is an indication for the use of systemic
therapy.
BMAs and bone marrow trephine biopsies are
considered complementary as diagnotic tests for the presence of
micro-metastatic involvement, and the use of trephine biopsies is
particularly important in cases where an adequate aspirate cannot
be obtained due to bone marrow fibrosis or densely packed bone
marrow by tumor cells (8,9). Fibrosis is considered slightly
increased in bone marrow biopsy specimens in prostate cancer in
comparison to other types of solid tumors (10).
The aim of this study was to compare the concordance
between the presence of CPCs and DTCs and micrometastasis in
patients with prostate cancer and their association in low-grade
and high-grade tumors. The phenotypic classification of the cells
using monoclonal antibodies against CD82 (a tumor-suppressor gene
product), matrix metalloproteinase-2 (MMP-2; involved in
dissemination and implantation of tumor cells) and HER-2 expression
(a marker of the resistence to androgen blockade) were also
investigated. We aimed to ascertain whether DTCs truly indicate
micrometastasis and if they exhibit the same phenotypic
characteristics as prostate cells identified in bone marrow
fragments. We also aimed to verify whether they are CPCs detected
in bone marrow rather than blood. We evaluated the clinical
implications this may have if DTCs rather than micrometastasis are
used to define systemic failure after radical prostatectomy and
possible theoretical consequences on treatment decisions.
Patients and methods
All males with histologically confirmed prostate
cancer treated at the Hospital Carabineros of Chile, the Hospital
Dipreca, Institute of Bio-Oncology and the Institute of
Radiotherapy, INRAD, Santiago, Chile and referred to the Institute
of Bio-Oncology between January 2008 and September 2011 and
fulfilling inclusion criteria were enrolled in the study. Ten women
requiring blood and bone marrow tests for hematological disorders
were included as controls.
For each patient the following clinical details were
registered: age, total serum PSA at the time of sampling, stage
according to the UICC TNM system (2002), 6th edition and Gleason
score.
The inclusion criteria were as follows. Patients i)
had biopsy confirmed prostate cancer, ii) were treated by radical
prostatectomy, iii) had treatment with or without androgen
blockade, iv) were enrolled at least 6 months post prostatectomy,
v) had negative bone scan and vi) provided written informed
consent.
Blood samples
After written informed consent a 4-ml blood sample
was collected in EDTA-containing Vacutainer® tubes
(Becton-Dickinson). Samples previously stored at 4°C were processed
within 48 h. The samples were layered onto 2 ml Histopaque
1.077® (Sigma-Aldrich) at room temperature, and the
mononuclear cells were obtained according to the manufacturer’s
instructions and finally washed 3 times in phosphate-buffered
saline pH 7.4 (PBS). The pellet was re-suspended in 100 μl
of autologous plasma and 25 μl was used to prepare each
silanized slide (Dako, USA). The slides were air dried for 24 h at
room temperature and finally fixed in a solution of 70% ethanol, 5%
formaldehyde and 25% PBS for 5 min and then washed 3 times with
PBS.
Bone marrow
BMA and biopsy samples were obtained from the
posterior superior iliac crest. Patients were sedated with 5–15 mg
of intravenous midazolam and the procedure was carried out using
5–10 ml of 2% lidocaine local anesthetic. The aspiration sample was
processed as described for the blood samples, except that the fat
was removed by centrifugation and discarded prior to gel
differential centrifugation. The bone marrow biopsy sample was used
to make 3 touch-preps using silanized slides (Dako) and both types
of samples were fixed as previously described. Touch preps were
used instead of traditional biopsy analysis, owing to the possible
destruction of epitopes during the process of the bone marrow
biopsy sample decalcification.
Immunocytochemistry
Monoclonal antibodies directed against PSA clone
28A4 (Novacastro, UK) at a concentration of 2.5 μg/ml were
used to detect prostate cells, and were identified using a
detection system based on alkaline phosphatase-anti-alkaline
phosphatase (LSAB2; Dako) with New Fuchsin as the chromogen
(according to the manufacturer’s instructions). To permit the rapid
identification of positive cells no counter-staining was carried
out with Mayer’s hematoxylin. Levisamole (Dako) was used as an
inhibitor of endogenous alkaline phosphatase, with positive and
negative controls. Positive samples underwent a second stage of
processing, using the monoclonal antibody against CD82 or MMP-2 or
HER-2 (HercepTest®) and a system of detection based on
peroxidase (LSAB2; Dako) with DAB (Dako) as the chromogen
(according to the manufacturer’s instructions). Endogenous
peroxidase was inhibited by a commercial inhibitor (Dako).
Immunocytochemistry was carried out at room temperature.
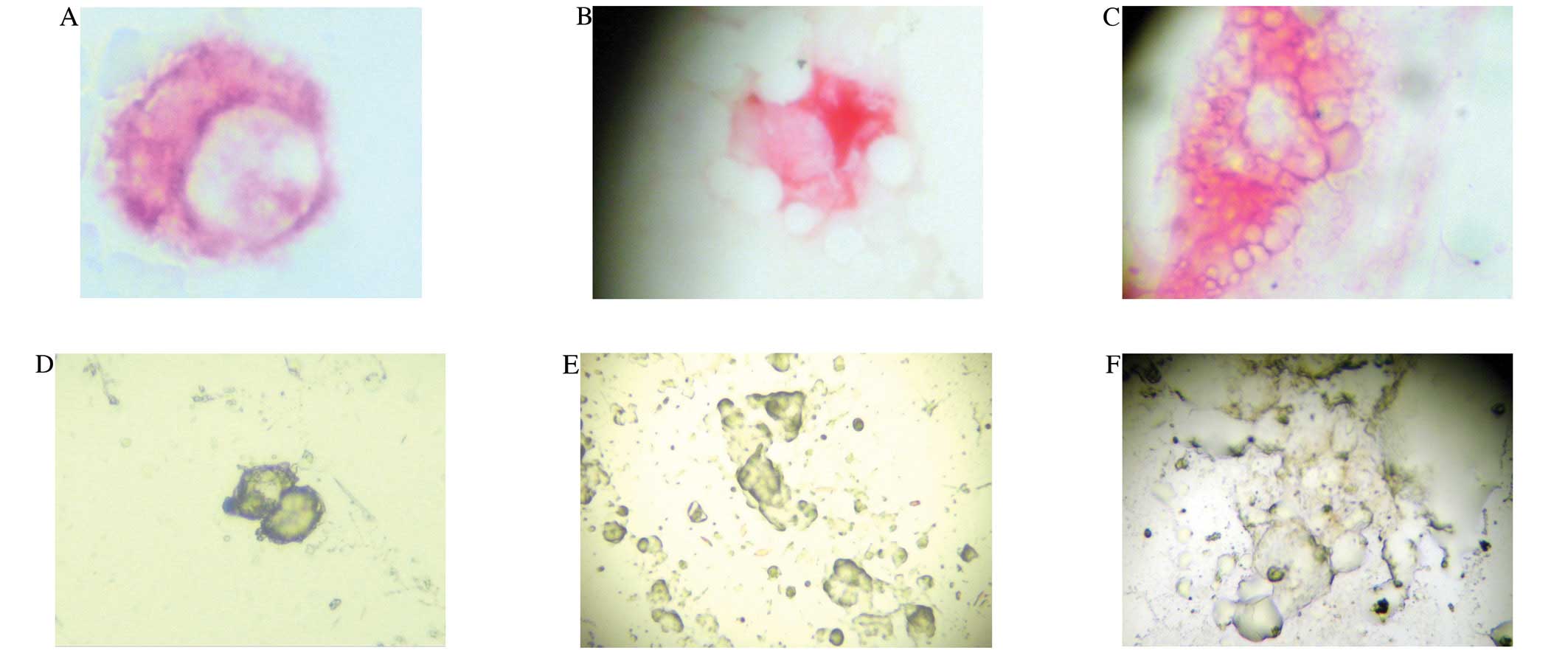
Definition of a positive sample
The definition of a CPC was based on the criteria of
ISHAGE 1999 (11): the morphology
of a cell with a nucleus and cytoplasm exhibiting positivity for
PSA. The definition of a DTC was similar with the exception that
the cell was present in the BMA and/or present in the touch prep of
the biopsy sample, but not in the micro-fragments. Micrometastasis
was defined as bone marrow fragments consisting of cells
immunostaining positive for PSA (Fig.
1A–F).
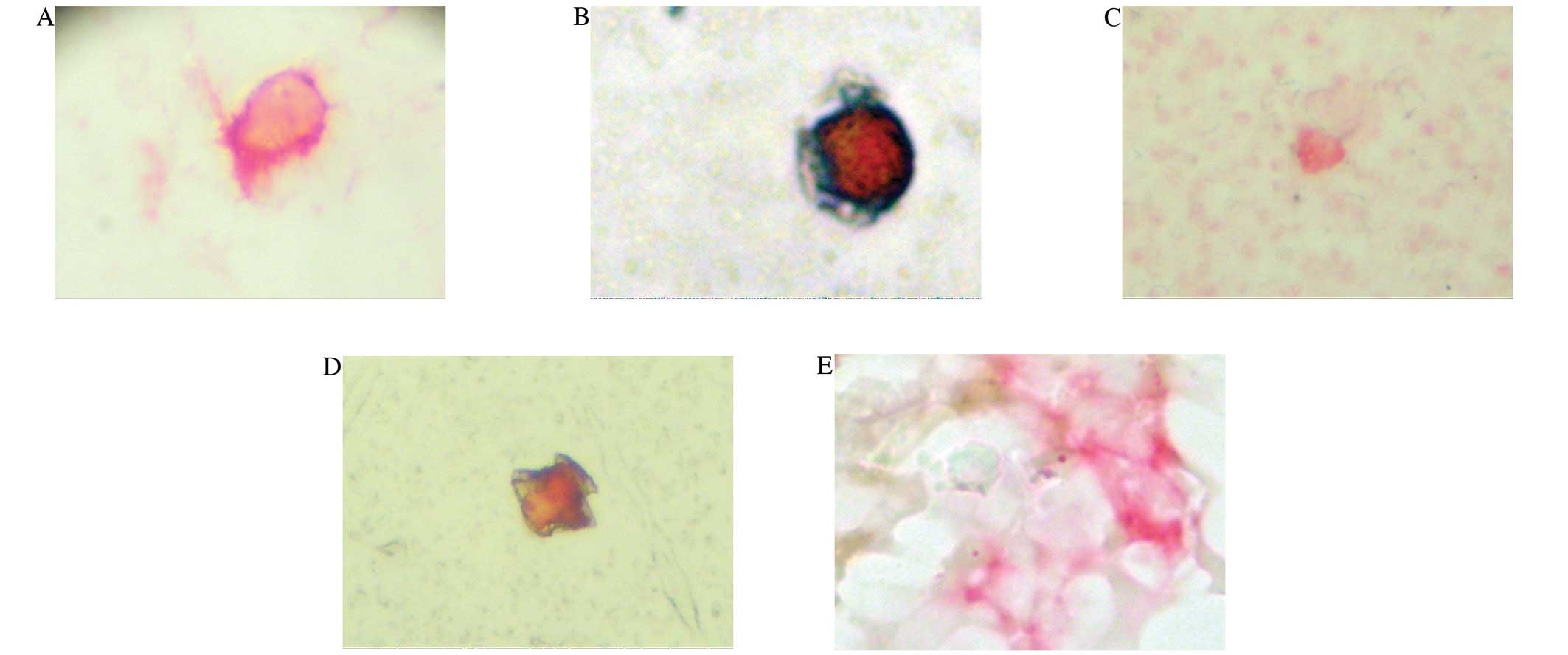
Immunophenotype
CD82 expression was scored using a semi-quantative
scale (Fig. 2A–E): 0, no
expression; 1+, part of the cell membrane is CD82 positive; 2+, all
of the cell membrane weakly expresses CD82; 3+, all of the cell
membrane strongly expresses CD82. Samples with 10% of cell staining
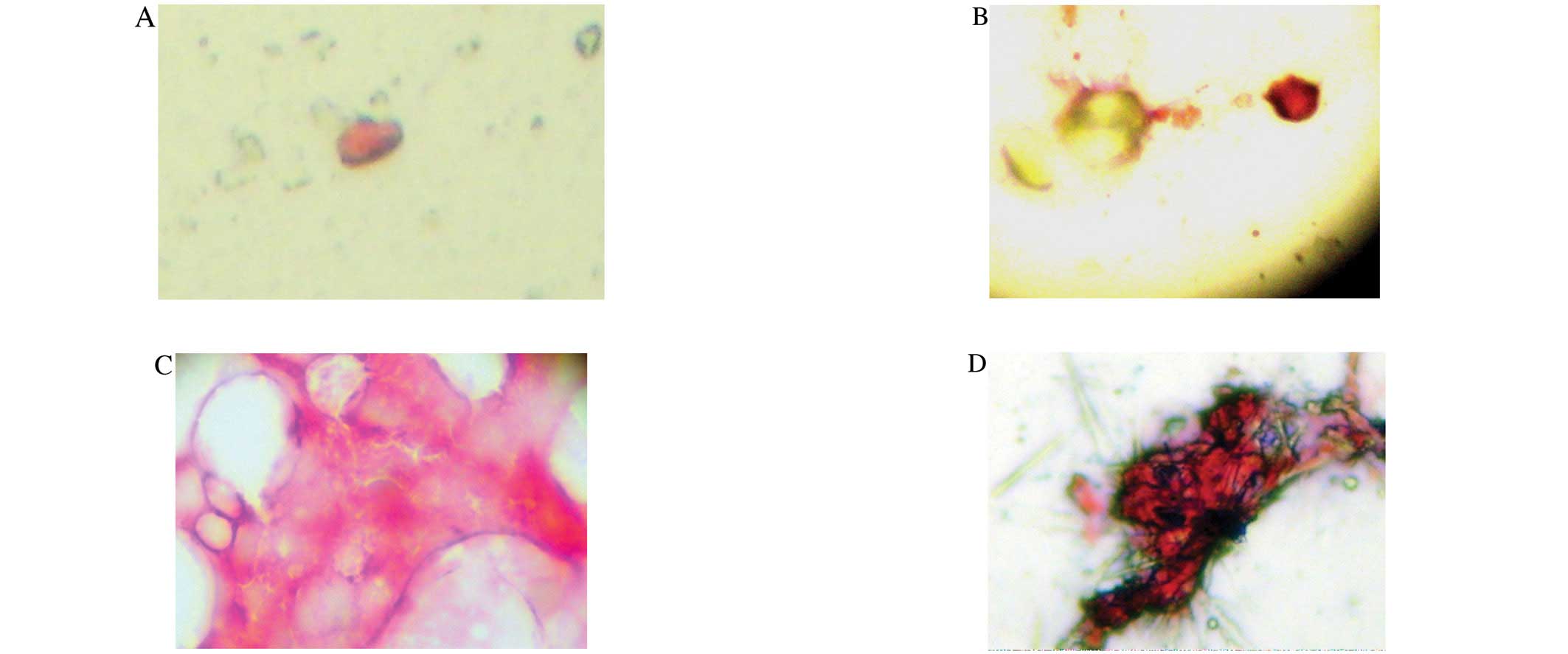
2+ and/or 3+ were considered positive for CD82 expression (18). MMP-2 expression was scored using a
semi-quantative scale. A sample containing >10% of cells
positive for MMP-2 was considered positive (12) (Fig.
3A–D). HER-2-positive cells were classified according to the
HercepTest® scale for breast cancer and approved by the
FDA. A score of 2+ or 3+ was classified as positive and 0 or 1+ as
negative according to the criteria of Osman et al (13) (Fig.
4A–C).
Definition of biochemical failure
Biochemical failure was defined according to
recommendations of the NCCN 2012 guidelines as a serum PSA >0.2
ng/ml.
Definition of type of relapse, local or
systemic
Micrometastasis or systemic relapse was defined as
the presence of fragments positive for PSA irrespective of the
presence or absence of circulating cells in the blood or bone
aspirate. Local recurrence was defined as the presence of negative
fragments with the absence of prostate cells in the blood or bone
marrow. Local recurrence with a risk of micrometastasis was defined
as the presence of negative fragments but with circulating cells in
the blood and/or aspirate samples. For each specimen
photomicrographs were captured with a digital camera, Samsung
Digimax D73, and processed with the Digimax program for Windows
98.
Ethical considerations
The study was carried out in full accordance with
the Declaration of Helsinki and the Hospital Ethics Committees.
Statistical analysis
Descriptive statistics were used for demographic
variables, expressed as the mean ± standard deviation in the case
of continuous variables with a normal distribution. In the event of
asymmetrical distribution the median and interquartile range (IQR)
values were used. Non-contiguous variables were presented as
frequencies. The Student’s t-test was used to compare continuous
variables with a normal distribution and Chi-square, Kruskal-Wallis
and log regression for the differences in frequency. The kappa test
was used to analyze concordance.
Results
Table I shows the
demographic characteristics of the 185 men who participated in the
study. The presence of CPCs in BMAs and in bone marrow of prostate
cancer patients was analyzed by determining PSA protein expression.
CPCs were detected in 62.7%, DTCs in 62.2% and micrometastasis in
71.4% of the patients.
 | Table IDemographic characteristics of the
study group. |
Table I
Demographic characteristics of the
study group.
| No. of patients,
n | 185 |
| Mean age ± SD,
years | 72.2±9.0 |
| Median serum PSA
(IQR), ng/ml | 1.32
(0.40–5.77) |
| Median Gleason
score (IQR) | 6 (5–7) |
| Median stage (TMN)
(IQR) | 3 (2–3) |
| Median time from
diagnosis (IQR), years | 3 (1–7) |
| Detection of
prostate cells, % (n) | |
| CPCs | 62.7 (116) |
| DTCs | 62.2 (115) |
|
Micrometastasis | 71.4 (132) |
| Post prostatectomy,
% (n) | 81.1 (150) |
Table II shows the
PSA protein expression in cells present in blood, BMA and biopsy of
cancer patients in comparison with the Gleason score. There was no
difference in the detection of cells in relation to age or serum
PSA levels or the time from diagnosis to test time. Patients with
higher Gleason scores had significantly higher stage disease. There
were no differences in the frequency of detection of CPCs and DTCs
with regards to the Gleason score. However, the frequency of
detection of micrometastasis was significantly lower in patients
with Gleason 4 in comparison with higher Gleason scores
(Kruskal-Wallis, P<0.001).
| Table IIDemographic variables according to
Gleason score. |
Table II
Demographic variables according to
Gleason score.
| Gleason 4 | Gleason 5+6 | Gleason 7 | Gleason 8+9 | P-value |
|---|
| No. of patients,
n | 28 | 106 | 31 | 20 | |
| Mean age ± SD,
years | 71.1±8.7 | 73.2±9.4 | 70±8.9 | 71.7±6.7 | NSe |
| Median serum PSA
(IQR), ng/ml | 1.0 (0.5–4.8) | 1.68 (0.5–5.5) | 0.57
(0.1–10.0) | 1.68
(0.32–28.7) | NSf |
| Median stage
(IQR) | 2
(1–2)a–c | 3
(2–3)a,d | 3
(2–3)b | 3
(3–4)c,d |
<0.001a–a,f |
| | | | |
<0.001b–b,f |
| | | | |
<0.001c–c,f |
| | | | |
<0.002d–d,f |
| | | | | Significant
<0.004f |
| Median time from
diagnosis (IQR), years | 2 (1–4) | 4 (1–8) | 3 (1–5) | 2 (1–5) | NSf |
| Presence of
prostate cells, % (n) | | | | | |
| CPCs | 46.4 (13) | 63.2 (67) | 64.5 (20) | 80 (16) | P=0.0123g |
| DTCs | 35.7 (10) | 65.1 (69) | 67.7 (21) | 75 (15) | P=0.015g |
|
Micrometastasis | 32.1 (9) | 77.4 (82) | 77.4 (24) | 85 (17) | P=0.001g |
| Prostatectomy %
(n) | 82 (23) | 75.5 (80) | 90.3 (28) | 95 (19) | NSf |
Table III shows
the expression of the markers MMP-2, the tumor suppressor CD82 and
HER-2 in patients positive for prostate cells in blood (n=116),
BMAs (n=115) and bone marrow biopsy (n=132). MMP-2 expression was
commonly limited to the edge of the bone marrow fragment (Fig. 3D).
| Table IIIExpression of MMP-2, CD82 and HER-2
in patients according to Gleason score. |
Table III
Expression of MMP-2, CD82 and HER-2
in patients according to Gleason score.
| Gleason 4 %
(n) | Gleason 5+6 %
(n) | Gleason 7 %
(n) | Gleason 8+9 %
(n) | P-value
(statistical test-log regression) |
|---|
| Total 100%
(n=185) | 15.1 (28) | 57.3 (106) | 16.8 (31) | 10.8 (20) | |
| CPC-positive 62.7%
(n=116) | 46.4 (13) | 63.2 (67) | 64.5 (20) | 80.0 (16) | NS |
| MMP-2 | 100.0 (13) | 100.0 (67) | 100.0 (20) | 100.0 (16) | NS |
| CD82 | 61.5a
(8) | 1.9a
(2) | 0 | 0 |
<0.001a–a |
| HER-2 | 23.1b,c
(3) | 20.9d,e
(14) | 60.0b,d
(12) | 63.5c,e
(10) |
<0.02b–b |
| | | | |
<0.005c–c |
| | | | |
<0.005d–d |
| | | | |
<0.002e–e |
| DTC-positive 62.5%
(n=115) | 35.7 (10) | 65.1 (69) | 67.7 (21) | 75.0 (15) | |
| MMP-2 | 100.0 (10) | 100.0 (69) | 100.0 (21) | 100.0 (15) | NS |
| CD82 | 79.0f
(7) | 4.4f
(3) | 0 | 0 |
<0.001f–f |
| HER-2 | 20.0g,h
(2) | 21.8i,j
(15) | 52.4g,i
(22) | 60.0h,j
(9) |
<0.017g–g |
| | | | |
<0.006h–h |
| | | | |
<0.01i–i |
| | | | |
<0.002j–j |
| MM-positive 71.4%
(n=132) | 32.1 (9) | 77.4 (82) | 77.4 (22) | 85.0 (17) | |
| MMP-2 |
0k–m | 14.6k,n
(11) | 20.8l
(5) | 41.1m,n
(7) |
<0.002k–k |
| | | | |
<0.002l–l |
| | | | |
<0.002m–m |
| | | | |
<0.002n–n |
| | | | | Trend
Chi-squared |
| | | | | P=0.031 |
| CD82 | 0 | 0 | 0 | 0 | |
| HER-2 | 22.2o,p
(2) | 25.6q,r
(21) | 58.3o,q
(14) | 58.8p,r
(10) | NS |
| | | | |
<0.004o–o |
| | | | |
<0.003p–p |
| | | | |
<0.006q–q |
| | | | |
<0.006r–r |
Table IV shows the
concordance among CPCs, DTCs and micrometastasis using kappa
statistics. For all Gleason scores there was moderate to good
concordance between the detection of CPCs and DTCs. There was low
concordance between CPCs and micrometastasis in patients with
Gleason 4–7 but moderate concordance in patients with Gleason 8 and
9. There was good concordance between DTCs and micrometastasis in
patients with Gleason 4, 8 and 9 but low concordance with Gleason
5, 6 and 7.
| Table IVConcordance among detection of CPCs,
DTCs and micrometastasis according to Gleason score. |
Table IV
Concordance among detection of CPCs,
DTCs and micrometastasis according to Gleason score.
| κ-values
between | Gleason 4 | Gleason 5+6 | Gleason 7 | Gleason 8+9 |
|---|
| CPC + DTC | 0.64 | 0.55 | 0.78 | 0.57 |
| CPC + MM | 0.27 | 0.32 | 0.23 | 0.48 |
| DTC + MM | 0.60 | 0.39 | 0.44 | 0.69 |
Table V shows the
concordance among CPCs, DTCs and micrometastasis for the expression
of MMP-2, CD82 and HER-2, respectively. There was complete
concordance for the expression of HER-2. MMP-2 was concordant with
CPCs and DTCs, but neither was concordant with micrometastasis; a
similar result was found for the CD82 expression for Gleason 4 and
5.
| Table VConcordance between CPCs, DTCs and
micrometastasis for the expression of MMP-2, CD82 and HER-2. |
Table V
Concordance between CPCs, DTCs and
micrometastasis for the expression of MMP-2, CD82 and HER-2.
| A, Concordance
between the expression of MMP-2 in CPCs, DTCs and micrometastasis
according to Gleason score. |
|
| kappa: MMP-2 | Gleason 4 | Gleason 5+6 | Gleason 7 | Gleason 8+9 |
|
| CPCs + DTCs | 0.64 | 0.59 | 0.78 | 0.57 |
| CPCs + MM | 0 | 0.14 | 0.19 | 0.23 |
| DTCs + MM | 0 | 0.13 | 0.17 | 0.30 |
|
| B, Concordance
between the expression of CD82 in CPCs, DTCs and micrometastasis
according to Gleason score. |
|
| kappa: CD82 | Gleason 4 | Gleason 5+6 | | |
|
| CPCs + DTCs | 0.55 | 0.80 | | |
| CPCs + MM | 0 | 0 | | |
| DTCs + MM | 0 | 0 | | |
|
| C, Concordance
between the expression of HER-2 in CPCs, DTCs and micrometastasis
according to Gleason score. |
|
| kappa: HER-2 | Gleason 4 | Gleason 5+6 | Gleason 7 | Gleason 8+9 |
|
| CPCs + DTCs | 0.78 | 0.88 | 0.93 | 0.90 |
| CPCs + MM | 0.78 | 0.69 | 0.87 | 0.80 |
| DTCs + MM | 1.00 | 0.67 | 0.80 | 0.90 |
We aimed to evaluate the clinical implications for
defining micrometastasis using DTCs vs. micrometastasis (Table VI). Of the total population of 185
men, 13 were positive for DTCs and negative for micrometastasis and
20 were negative for DTCs and positive for micrometastasis. Thus,
17.8% of cases were misclassified when only DTCs were used to
define micro-metastasis. Of 115 men with biochemical failure, 7
were positive for DTCs and negative for micrometastasis and 16 were
negative for DTCs and positive for micrometastasis representing a
misclassification of 20% of the cases.
| Table VIType of dissemination defined by the
presence of CPCs, DTCs and micrometastasis. |
Table VI
Type of dissemination defined by the
presence of CPCs, DTCs and micrometastasis.
| All negative | CPCs (+) | CPCs (+) | All positive | CPCs (−) | CPCs (−) |
|---|
| DTCs (−) | DTCs (+) | DTCs (+) | DTCs (−) |
|---|
| MM (−) | MM (−) | MM (+) | MM (+) |
|---|
| All patients
(n=185) | 36 | 6 | 13 | 94 | 16 | 20 |
| Patients with BF
(n=115) | 20 | 1 | 7 | 60 | 11 | 16 |
| Classification | None/local | Local with
dissemination | Local with
dissemination | Systemic with
dissemination | Systemic with
dissemination | Systemic |
Discussion
This study analyzed the presence of prostate cells
in BMAs and biopsy samples and compared their presence and
phenotypic characteristics with those of CPCs found in the blood of
men with histologically confirmed prostate cancer.
There was no relation with age, serum PSA level or
from the time of diagnosis as previously reported (5), and the finding that patients with
higher Gleason scores had cancer of a more advanced stage is
consistent with the natural history of the disease.
The detection of CPCs and DTCs were independent of
the Gleason score suggesting they may be similar in nature (i.e.,
circulating tumor cells), especially since the presence of
micrometastasis was significantly lower in low-grade Gleason 4
tumors.
There was a good concordance between the presence of
CPCs and DTCs for all Gleason scores, differing from that of
micrometastasis. There was a low concordance between CPCs and
micrometastasis except for high-grade Gleason 8 and 9 tumors. This
suggests that they represent different types of cells, that
micrometastasis is not necessarily associated with actively
disseminating cells (CPCs). CPCs may have disseminated from the
local disease that is confirmed to the prostate bed or lymph nodes
or from systemic bone disease. The presence of CPCs alone does not
allow the differentiation between local relapse and systemic
relapse. The low concordance between DTCs and micrometastasis for
patients with Gleason 5, 6 and 7 suggests there is a difference in
their physiological/oncological role. In high-grade Gleason 8 and 9
there was good concordance which may be explained on the basis of
rheological studies and the nature of the test itself. Research
(5) has shown that prostate
cancer micrometastasis has a low proliferation index thus it would
be expected that the cells remain adherent to the endosteum and are
not present in the intertrabecular spaces, that is the results are
usually aspirate-negative but biopsy-positive. This suggests that
BMAs may not truly represent micrometastatic disease due to bone
marrow cell kinetics. This may help to explain why patients
frequently have disease relapse even with a negative BMA. It is
postulated that a BMA, by its nature, provides either a sample of
cells that are in transit or a sample that is removed from the
endosteum. The cells in transit may be circulating from the
original tumor, or are detached from a proliferating
micrometastatic site.
There are no studies of in vivo tumor cell
rheology in the bone marrow. However, there are in vivo
optical imaging studies in laboratory animals demonstrating the
mechanisms of tumor cell attachment to the endosteum that are
similar to stem cell engraftment (14,15). Topological and chronological
patterns of stem cell seeding have shown that most cells drift
within the bone marrow space, then are gradually found close to the
endosteal surface. The center of the bone marrow space seems to be
the site of proliferation of transplanted cells and not the
endosteal surface (16). Further
studies have shown that the adherent cells are viable, whereas
cells in transit contain a percentage of dead or dying cells
(17). Experimental data suggest
that adhesion is the rate limiting determinant of homing and early
seeding and a crucial event that preserves the viability of cells
towards successful engraftment (17). The fact that cells attached to the
endosteal surface are not usually detected may explain why all
patients with positive BMA do not develop metastasis. Conversely,
patients with negative BMA may have cancer cells attached to the
endosteal surface that may eventually develop into metastasis.
Thus, in high-grade cancer, the interchange between cells between
the bone and intertrabecular space may be sufficiently high,
suggesting that the presence of DTCs is equivalent to the presence
of micrometastasis. However in intermediate grade cancer, with a
lower interchange rate this relationship does not appear to remain
valid. However, this would not explain why there was good
concordance between the presence of DTCs and micrometastasis in
low-grade Gleason 4 cancer. The concordance was confined to
patients with stage 3 disease. These patients experienced
biochemical failure, had MMP-2-negative micrometastasis and CPCs
and DTCs were detected. One explanation is that the CPCs and DTCs
originated from a local failure near to the prostate bed and the
micrometastasis was in a dormant state in the bone marrow. This
needs to be further investigated with a larger group of
patients.
Phenotypically CPCs and DTCs were identical, but
differed from micrometastasis. The lack of CD82 expression in
micro-metastasis suggests that the expression of this
tumor-suppressor protein present in low-grade tumors inhibits
implantation of CPCs (CPCs and DTCs), as was suggested previously
(18). HER-2 expression increased
significantly with an increasing Gleason score, without significant
differences between CPCs, DTCs and micrometastasis. This is
explained by the fact that men with androgen blockade had higher
Gleason scores as was previously reported (19).
The differential expression of MMP-2 may explain in
part the differences in the concordance among CPCs, DTCs and
micrometastasis. The differential expression of MMP-2 in bone
marrow micrometastasis, where the absence of MMP-2 detected by
immunocytochemistry is common, suggests the inhibition of MMP-2.
The stromal microenvironment plays a critical role in determining
tumor cell behavior in primary tumors; the stromal cells increasing
MMP-2 expression in tumor cells (20,21). To the best of our knowledge, we
describe for the first time in prostate cancer that bone marrow
stromal cells produce the opposite reaction, that of inhibition of
MMP-2 expression. That the expression is different to that in CPCs
and DTCs, is supportive evidence that prostate cells detected in
BMAs are different and are not true micrometastasis (7), but represent circulating tumor cells
in the bone marrow compartment. It has been shown that the bone
marrow microenvironment is composed of specific niches that provide
support for the proliferation and maintenance of hematopoietic stem
cells (22). Interactions between
the stem cells and their microenvironment regulate their
maintenance, proliferation, differentiation and migration into the
blood circulation. Distinct niches have been anatomically and
physiologically defined within the bone marrow (23,24). In the endosteal region,
osteoblasts and other mesenchymal derived stromal cells such as
reticular cells, fibroblasts and adipocytes constitute the
osteoblastic niche that supports the maintenance of hematopoietic
stem cells in a quiescent and undifferentiated state, by adhesion
and humoral factors (25).
We propose that the expression of MMP-2 is inhibited
by bone marrow stromal cells, in a process similar to that noted in
hematopoietic stem cells, possibly by TIMP-2. Other inhibitors
modulating this function cannot be excluded.
The inhibition of MMP-2 decreases the ability of
cancer to migrate from its new site, but does not inhibit
proliferation directly. However, the decreased release of growth
factors produced by MMP-2 and decreased initiation of angiogenesis
by MMP-9 induced in part by MMP-2 (26) may limit the growth potential of
microfoci. However, in high-grade cancer, such as Gleason 9, tumor
cells of the micrometastasis continue to proliferate. As they
divide and expand towards the inter-trabecular surface, the
inhibition by stromal cells decreases. This permits the
reappearance of MMP-2 expression, as noted in the microfragment
borders but not in the centre of the fragment, where MMP-2
suppression continues. This in turn allows the cells to escape and
to disseminate, forming 2 CPCs. This theory would explain our
results demonstrating the concordance between DTCs and
micrometastasis for Gleason scores 5–9.
Using the presence of conventional DTCs rather than
micro-metastasis as a biomarker for systemic disease and to
indicate systemic treatment after biochemical failure, 20% of
patients would be erroneously classified.
Thus, this study suggests that DTCs in intermediate
grade cancer do not indicate micrometastasis and are simply
circulating tumor cells in the bone marrow compartment. They are
phenotypically different and if used to define systemic
micro-metastatic disease misclassification of patient would occur
in 20% of the cases. Due to the phenotypic differences, various
treatments may be necessary in order to eliminate DTCs,
particularly when considering targeted therapy.
Acknowledgements
We gratefully thank Mrs. Ana Maria
Palazuelos for her assistance in this study.
References
|
1.
|
NCCN prostate cancer guidelines 2012.
Accessed www.nccn2012.org
|
|
2.
|
SJ FreedlandME SutterF DoreyWJ
AronsonDefining the ideal cutpoint for determining PSA recurrence
after radical prostatectomy: prostate specific
antigenUrology61365369200310.1016/S0090-4295(02)02268-912597949
|
|
3.
|
DP WoodM BanerjeePresence of circulating
prostate cells in the bone marrow of patients undergoing radical
prostatectomy is predictive of disease free survivalJ Clin
Oncol153451345719979396397
|
|
4.
|
ML CherJG De OliveiraAA BeamanJA NemethM
HussainDP Wood JrCellular proliferation and prevalence of
micro-metastatic cells in the bone marrow of patients with
clinically localized prostate cancerClin Cancer
Res524212425199910499613
|
|
5.
|
R ObernederR RiesenbergM
KreigmairImmunocytochemical detection and phenotypic
characterization of micrometastatic tumor cells in bone marrow of
patients with prostate cancerUrol Res2238199410.1007/BF00431541
|
|
6.
|
K PantelC AignherrJ KollermannJ CapranoG
RiethmullerMW KollermannImmunocytochemical detection of isolated
tumor cells in bone marrow of patients with untreated stage C
prostate cancerEur J
Cancer31A1627A1632199510.1016/0959-8049(95)00290-Y7488413
|
|
7.
|
NP MurrayGM CalafL BadinezPresence of
prostate cells in bone marrow biopsies as a sign of micrometastasis
in cancer patientsOncol Rep21571575200919212613
|
|
8.
|
JD BeardenGA RatkinCA ColtmanComparison of
the diagnostic value of bone marrow biopsy and bone marrow
aspiration in neoplastic diseaseJ Clin
Pathol27738740197210.1136/jcp.27.9.7384426982
|
|
9.
|
A BjorneklettP SlavernK ElgioRelative
value of sterna aspiration, iliac crest biopsy and biopsy imprint
in the diagnosis of secondary cancer involvement of the bone
marrowActa Med
Scand203279281197810.1111/j.0954-6820.1978.tb14873.x645440
|
|
10.
|
F MoidL DePalmaComparison of relative
value of bone marrow aspirates and bone marrow trephine biopsies in
the diagnosis of solid tumor metastasis and Hodgkin lymphomaArch
Pathol Lab Med129497501200515794673
|
|
11.
|
E BorgenB NaumeJM NeslandE KvalheinK
BeiskeO FodstedStandardization of the immunocytochemical detection
of cancer cells in bone marrow and blood: I. establishment of objec
tive criteria for the evaluation of immunostained
cellsCytotherapy5377388199910.1080/003247203100014128320426539
|
|
12.
|
D TrudelY FradetF MeyerF HarelB
TetuSignificance of MMP-2 expression in prostate cancerCancer
Res6385118515200314679018
|
|
13.
|
I OsmanHI ScherM DrobnjakD VerbelM MorrisD
AgusHER-2/neu (p185neu) protein expression in the natural or
treated history of prostate cancerClin Cancer
Res726432647200111555574
|
|
14.
|
N AskenasyDL FarkasOptical imaging of
PKH-labeled hematopoietic cells in recipient bone marrow in
vivoStem Cells20501513200210.1634/stemcells.20-6-50112456958
|
|
15.
|
PJ QuesenberryPS BeckerStem cell homing:
rolling, crawling and nestingProc Natl Acad Sci
USA951515515157199810.1073/pnas.95.26.151559860935
|
|
16.
|
JL ChristensenDE WrightAJ WagersIL
WeissmanCirculation and chemotaxis of fetal hematopoietic stem
cellsPLoS Biol2E75200410.1371/journal.pbio.002007515024423
|
|
17.
|
IB MazoUH Von AndrianAdhesion and homing
of blood-borne cells in bone marrow microvesselsJ Leukoc
Biol662532199910410986
|
|
18.
|
NP MurrayL BadínezO BadínezN OrellanaR
DueñasE ReyesC FuentealbaExpresión del supresor tumoral CD82 en
células prostáticas primarias y secundarias en la circulación
sanguínea (CPCs) de pacientes con cáncer prostáticoRev Mex
Urol7092962010(In Spanish)
|
|
19.
|
NP MurrayL BadinezR DueñasN OrellanaP
TapiaPositive HER-2 protein expression in circulating prostate
cells and micro-metastasis, resistant to androgen blockage but not
diethylstilbestrolIndian J
Urol27200207201110.4103/0970-1591.8283821814310
|
|
20.
|
LW ChungA BasemanV AssikisHE ZhauMolecular
insights into prostate cancer progression: the missing link of
tumor microenvironmentJ
Urol1731020200510.1097/01.ju.0000141582.15218.1015592017
|
|
21.
|
T SatoT SakaiY NoguvhiM TakitaS HirakawaA
ItoTumor stromal cell contact promotes invasion of human cervical
carcinoma cells by augmenting the expression and activation matrix
metalloproteinasesGynecol
Oncol924756200410.1016/j.ygyno.2003.09.01214751137
|
|
22.
|
B HeissigY OhkiY SatoS RafiiZ WerbK
HattoriA role for niches in hematopoietic cell
developmentHematology10247253200510.1080/1024533050006724916019473
|
|
23.
|
I YanivJ SteinDL FarkasN AshenasyThe tale
of early hematopoietic cell seeding in the bone marrow nicheStem
Cells Dev15416200610.1089/scd.2006.15.4
|
|
24.
|
RN KaplanB PsailaD LydenNiche to niche
migration of bone marrow derived cellsTrends Mol
Med137281200710.1016/j.molmed.2006.12.00317197241
|
|
25.
|
RS TaichmannBlood and bone: two tissues
whose fates are intertwined to create the hematopoietic cell stem
nicheBlood10526312639200510.1182/blood-2004-06-248015585658
|
|
26.
|
G BergersR BrekkenG McMahonTH VuT ItohK
TamakiMatrix metalloproteinase-9 triggers the angiogenic switch
during carcinogenesisNat Cell
Biol2737744200010.1038/3503637411025665
|