Introduction
Soft tissue sarcomas are a heterogeneous group of
solid malignant tumors which represent approximately 1% of all
malignancies (1). Liposarcomas
are the most common soft tissue sarcomas in adults, comprising
approximately 20% of all soft tissue sarcomas (2,3).
The peak incidence of liposarcomas is between 52 and 56 years of
age, and men are slightly more often affected than women (3,4).
Liposarcomas can occur throughout the body; however, 50–60% of all
liposarcomas are localized in the deep, subfascial soft tissues of
the thighs (3,5).
In patients with primary diagnosed liposarcoma
without concurrent distant metastasis, the therapy of choice
involves limb-sparing surgical resection with clear margins,
usually followed by radiation treatment to decrease local
recurrence (6,7). In this context, the achievement of
negative surgical margins in primary liposarcoma has been
determined to be an important factor for improving local disease
control (8–12). However, approximately 62–70% of
all local recurrences develop in spite of complete surgical
resection of the primary tumor with microscopically negative
margins (5,13,14).
Disseminated liposarcomas pose another therapeutic
challenge due to the limited effectivity of the currently available
treatment options. Notably, approximately 30% of all patients with
liposarcoma develop distant metastases during the course of the
disease (3,15–19). In cases of distant metastatic
disease, the median survival time is only <10 months (19). Doxorubicin, which has been the
most frequently used chemotherapeutic agent in the treatment of
metatstatic soft tissue sarcomas, only achieves response rates of
36% in liposarcoma as a whole (20). Concerning the four different
histological subsets, well-differentiated and dedifferentiated
liposarcomas display even worse response rates of 12 and 13%,
respectively (21). Pleomorphic
liposarcomas represent the most chemoresistant subentity, with
response rates of only 5% towards doxorubicin, while myxoid/round
cell liposarcomas are considered the most chemosensitive subgroup,
displaying response rates of 44–48% (22–24). The combination of doxorubicin with
ifosfamide is more effective, achieving higher response rates than
doxorubicin alone; however, it is associated with severe short-and
long-term toxicities, including cardiomyopathy and bone marrow
suppression (25–27). Unfortunately, trabectedin, which
had been approved as a promising second-line cytostatic agent in
the treatment of patients with disseminated soft tissue sarcomas,
could not achieve significant higher response rates than
doxorubicin in a recently published phase III trial (28).
Due to the rarity and heterogeneity of liposarcomas,
further investigations assessing the mechanisms leading to the
distinct chemoresistance are still lacking. In recent experimental
studies on other solid malignancies, the tumor microenvironment and
particularly, tumor-associated fibroblasts (TAFs), were identified
as a potential perpetrator of chemoresistance. Two different
mechanisms could be observed here. Firstly, TAFs can modulate the
chemosensitivity of malignant cells through the secretion of
certain cytokines. In an extensive in vitro study,
Straussman et al determined the pro-tumorigenic influence of
35 different cytokines on 45 malignant cell lines that had been
co-cultured with TAFs (29).
Interestingly, 65% of all treatment groups displayed a diminished
chemotherapeutic response that was mediated by TAF-secreted
cytokines. Since then, further in vitro studies have
revealed a similar cytokine-mediated chemoresistance in breast,
lung and pancreas carcinoma cells (30–32). A second mechanism of TAF-induced
chemoresistance was detected by Loeffler et al (33). The authors hypothesized that
chemotherapeutic drug uptake may be dictated by the interstitial
tumor pressure, which in turn is maintained by intratumoral
collagen type I. Subsequently, they targeted TAFs as a primary
source for collagen type I to decrease the interstitial tumor
pressure. By specific in vivo targeting of TAFs via
immunotherapy, doxorubicin-intake in breast carcinoma cells was
enhanced up to 70%, resulting in marked suppression of tumor growth
(33).
Apart from their influence on chemosensitivity, TAFs
have also been found to promote the growth and invasive potential
of tumor cells by the secretion of cytokines and the remodelling of
the extracellular matrix, leading to an increased malignancy in
many types of cancer, such as rhabdomyosarcoma, breast, colon and
prostate carcinoma (34–39). To date, the crosstalk between host
and cancer cells via cytokines with effects on both partners is
still unknown in liposarcoma. In the present study, we suggested
that there may be a bidirectional crosstalk between liposarcoma
cells and TAFs, which may lead to increased proliferation and
chemoresistance via soluble mediators. Therefore, we determined the
proliferation and doxorubicin sensitivity in a well-established
liposarcoma cell line (SW872) following co-culture with primary
TAFs obtained from surgically resected liposarcomas.
Materials and methods
Ethics statement
This study was reviewed and approved by the Ethics
Committee of the BG University Hospital Bergmannsheil,
Ruhr-University Bochum, Germany with the permit no. 5078-14. All
participating patients gave their written informed consent.
TAFs
Tissues for primary cultures of TAFs were collected
from one patient with an intermediate-grade myxoid/round cell
liposarcoma and a high-grade pleomorphic liposarcoma and one
patient with a high-grade pleomorphic liposarcoma that were
completely resected for curative intent at our institution. Normal
fibroblasts (NFs) were surgically obtained from the dermal layer of
both patients. The harvested tissues were minced into small
sections, washed with phosphate-buffered saline (PBS) several times
and digested with collagenase type I and hyaluronidase
(Sigma-Aldrich, St. Louis, MO, USA). Following filtration and
centrifugation at 400 × g for 5 min at 23°C, the cells were placed
in Dulbecco's modified Eagle's medium (DMEM; Biochrom GmbH, Berlin,
Germany) supplemented with 20% fetal calf serum (FCS; PAN-Biotech
GmbH, Aidenbach, Germany), 1% penicillin (100 U/ml), streptomycin
(100 µg/ml) and 1% L-glutamine (Sigma-Aldrich). The cells
were cultured in a humidified atmosphere at 37°C with 5%
CO2 in 25 cm2 flasks. The medium
was changed every second day. The experiments were conducted in
early passages (3–4 following isolation). α-smooth muscle actin
(α-SMA) is a well-established marker to detect TAFs in tumor tissue
(34,40,41). In our study, the isolated TAFs
were examined by immunofluorescence using α-SMA antibody (Abcam,
Cambridge, UK) at the second passage to confirm the fibroblastic
origin of the isolated cells.
Histopathological classification
Both tumors were diagnosed by the Institute of
Pathology at the Ruhr University of Bochum. The Institute of
Pathology and the Department of Plastic Surgery are part of the
Sarcoma Reference Center at the Ruhr University of Bochum. All
pathological slides were analyzed or reviewed for consensus
diagnosis by experienced soft tissue pathologists.
Liposarcoma cell line and co-culture
The human liposarcoma cells, SW872, were purchased
from the American Type Culture Collection (ATCC, Wesel, Germany;
cell line CCI-121) and maintained in DMEM medium supplemented with
10% FCS, 1% penicillin (100 U/ml), 1% streptomycin (100
µg/ml) and 1% L-glutamine. The cells were cultured in a
humidified atmosphere at 37°C with 5% CO2 in 25
cm2 flasks. For co-culture, 5×104
SW872 cells were seeded in 12-well co-culture plates (Corning Life
Sciences, Acton, MA, USA) in DMEM medium supplemented with 10%
complete chemically defined serum substitute PANEXIN NTA
(PAN-Biotech), penicillin (100 U/ml), 1% streptomycin (100
µg/ml) and 1% L-glutamine. After 10 min Transwells with a
pore size of 0.4 µm and 12 mm diameter (Corning Life
Sciences) were inserted. Subsequently, 4×104 TAFs were
seeded in each Transwell insert and co-cultured with the SW872
cells for 48 h before the subsequent experiments were
performed.
Cell viability assay
The metabolic activity was measured via
3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT)
assay according to the standard protocol. SW872 cells were grown
for 48 h in co-culture with TAFs or NFs. Subsequently, the SW872
cells were seeded in 96-well microtiter plates (Corning Inc., New
York, NY, USA) in a concentration of 3×104 cells/well.
The following day, the cells were incubated in serum-free medium.
Thereafter, the cells were incubated in fresh medium containing MTT
solution for a further 4 h. Vital cells integrated the dye as a
sign of active metabolism (glycolysis rate). The cells were lysed
with dimethyl sulfoxide (DMSO) (Carl Roth GmbH, Karlsruhe, Germany)
and glycine buffer. The amount of integrated dye represented the
level of metabolism and was quantified at 562 nm using an Elx808
Ultra Microplate Reader (BioTek Instruments GmbH, Bad
Friedrichshall, Germany).
Cell proliferation assay
To determine and quantify the effects of TAF
co-culture on SW872 cell proliferation, a colorimetric cell
proliferation 5-bromo-2′-deoxyuridine (BrdU)-ELISA (Roche Applied
Science, Mannheim, Germany) assay was performed according to the
manufacturer's instructions. Briefly, the SW872 cells that were
grown for 48 h in co-culture were seeded at 3×104
cells/well in 96-well plates. BrdU labeling solution was added
followed by incubation for a further 4 h. Proliferating cells
integrated BrdU, a pyrimidine analogue, into their DNA. The level
of proliferation was quantified by the light emission detected
using an Orion microplate luminometer (Berthold Detection Systems
GmbH, Pforzheim, Germany).
Real-time cell analysis
For chemosensitivity analysis, the SW872 cells were
incubated in co-culture with TAFs or NFs for 48 h. Thereafter, the
SW872 cells were seeded in two 8-well plates with an integrated
microelectronic sensor array (iCELLigence Real-Time cell analyzer;
CEA Biosciences, San Diego, USA). After 24 h, the cultivated human
liposarcoma cells were incubated with doxorubicin at a
concentration of 0.25 µg/ml that exhibited strong
pro-apoptotic effects in previous a in vitro study (42). Cell proliferation and survival
were monitored real-time by measuring cell-to-electrode responses
of the seeded cells. The cell index (CI) was calculated for each
E-plate well using RTCA software 1.2 (Roche Diagnostics, Meylan,
France), as previously described (43). CI was calculated for each E-plate
well using RTCA Software. The graphs are real-time generated
outputs from the iCELLigence system.
Analysis of cell morphology
The morphology of the adherent and suspended cells
was examined and documented using a phase contrast Zeiss Axiovert
25 microscope (Carl Zeiss, Jena, Germany).
Statistical analysis
Comparisons between the experimental groups in BrdU-
and MTT-assay were performed using one-way measures of variance
(one way ANOVAs) over all time points (Tukey test). The results
were considered statistically significant for p-values ≤0.05.
Results
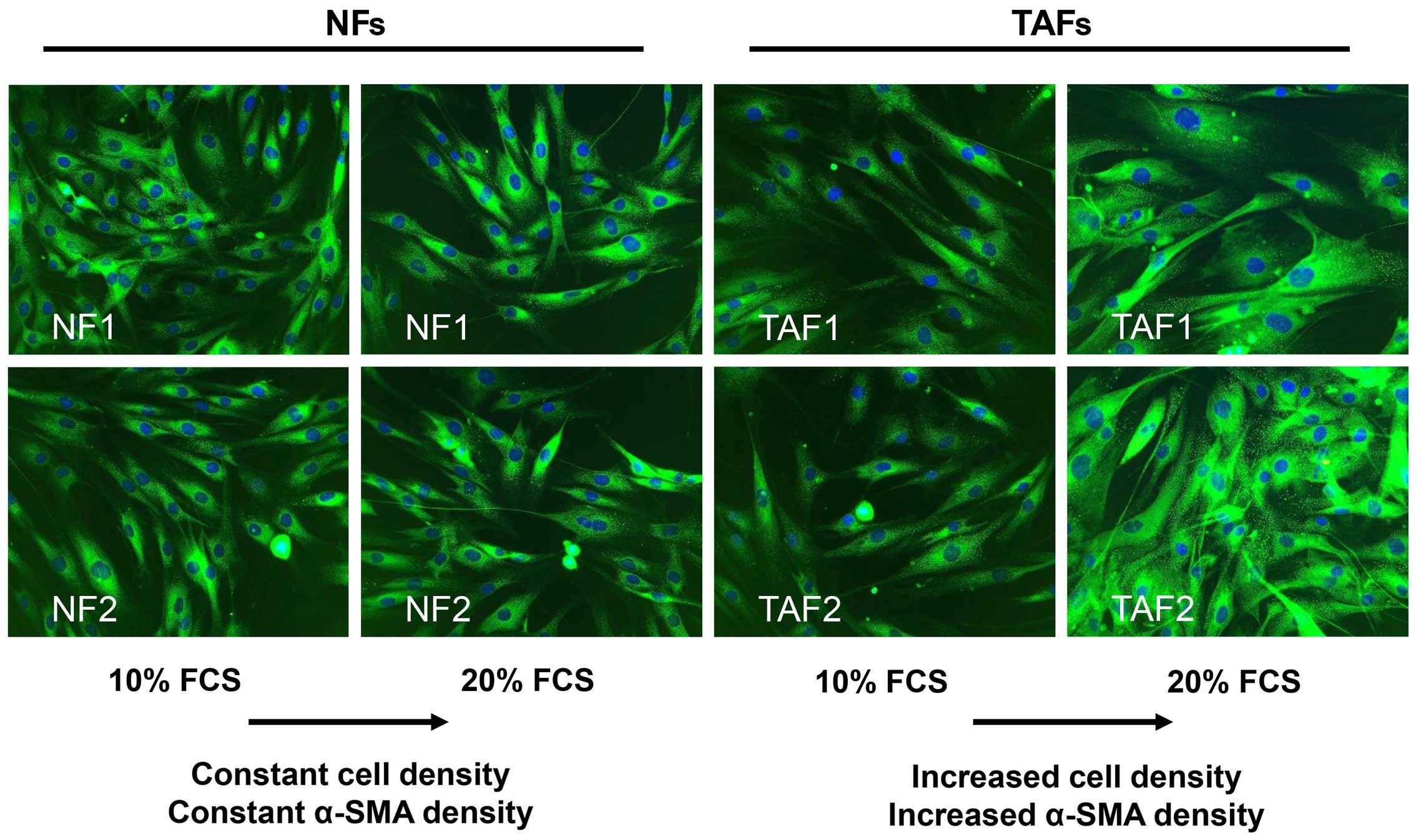
TAFs exhibit a dynamic expression of
α-SMA
Both, TAFs and NFs expressed α-SMA at the second
passage, indicating the effective isolation and cultivation of TAFs
from tumor tissue (Fig. 1). The
morphology of the TAFs obtained from intermediate-grade (TAF1) and
high-grade liposarcoma (TAF2) tumor samples did not differ from
that of the NFs. They displayed a similar spindle-shaped, elongated
and flattened phenotype with few protrusions and small lamellae.
The TAFs and NFs exhibited a comparable α-SMA expression when
cultivated with medium containing 10% FCS. Notably, the enhancement
of the FCS concentration up to 20% for 24 h led to an increase in
α-SMA expression in the TAFs, while the NFs did not respond to this
change in the FCS concentration in this short time period (Fig. 1).
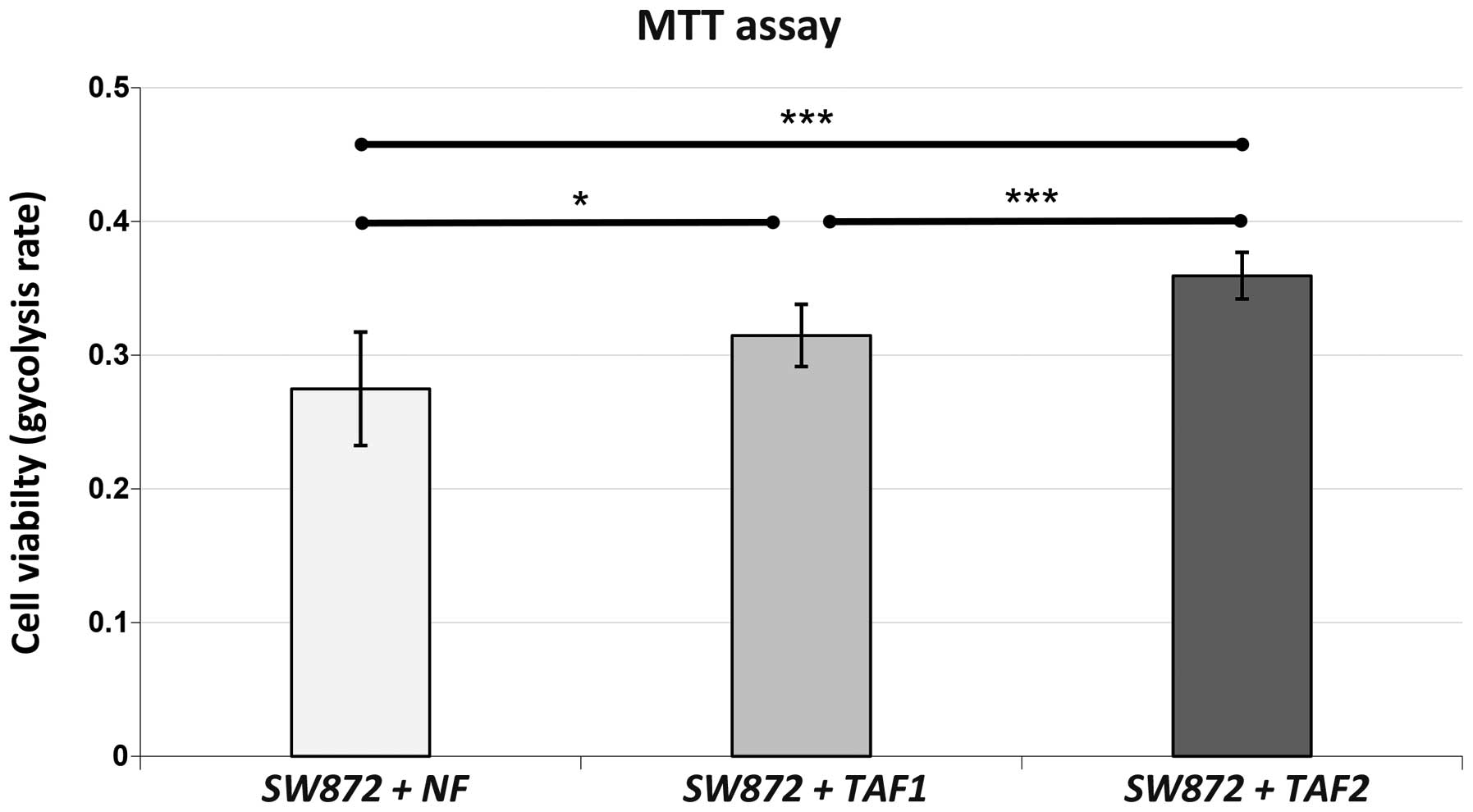
Co-culture with TAFs leads to a
significantly increased cell viability of SW872 human liposarcoma
cells
MTT assay revealed a markedly enhanced metabolic
activity of SW872 liposarcoma cells when co-cultured with TAFs
(Fig. 2). The SW872 cells that
were co-cultured with TAF2 from more malignant high-grade
liposarcoma displayed a significantly increased cell viability when
compared with the controls cultured with NFs (p<0.001) or with
the cells cultured with TAF1 (p=0.001) from less malignant
intermediate-grade liposarcoma. Nevertheless, co-culture with TAF1
was also associated with a significantly increased cell viability
when compared to co-culture with the NFs (p=0.010). Hence, both TAF
subgroups were able to enhance the viability of the SW872 cells
significantly after 48 h of co-culture.
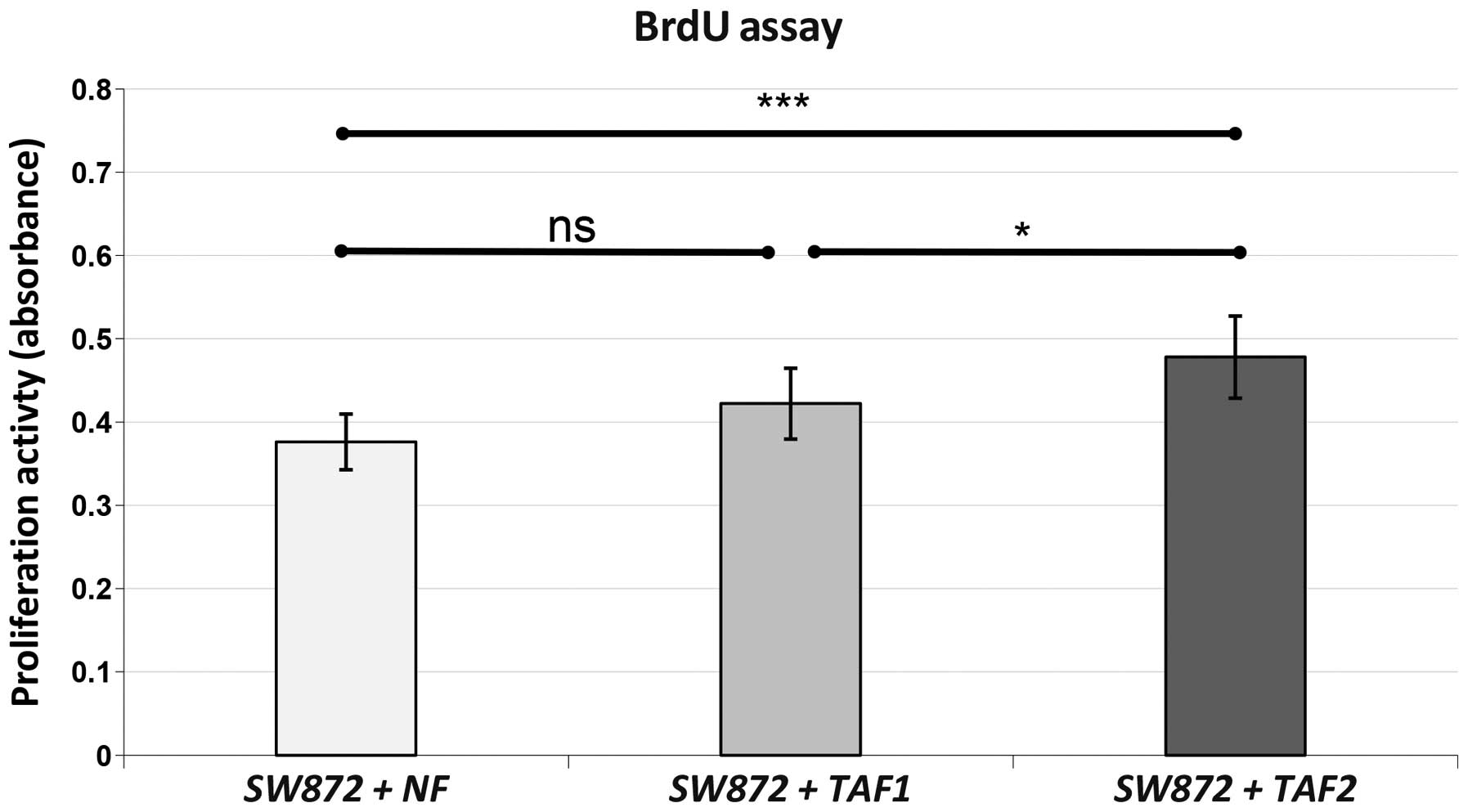
The proliferation of SW872 liposarcoma
cells is significantly enhanced following co-culture with TAFs from
high-grade liposarcoma, but not from intermediate-grade
liposarcoma
As indicated by BrdU assay, the proliferative
potency of the SW872 cells was significantly increased following
co-culture with TAF2 when compared to co-culture with NFs
(p<0.001) or TAF1 (p=0.019) (Fig.
3). Co-culture with TAF1 failed to reach a statistically
significant enhancement of proliferation compared to co-culture
with NFs (p=0.081).
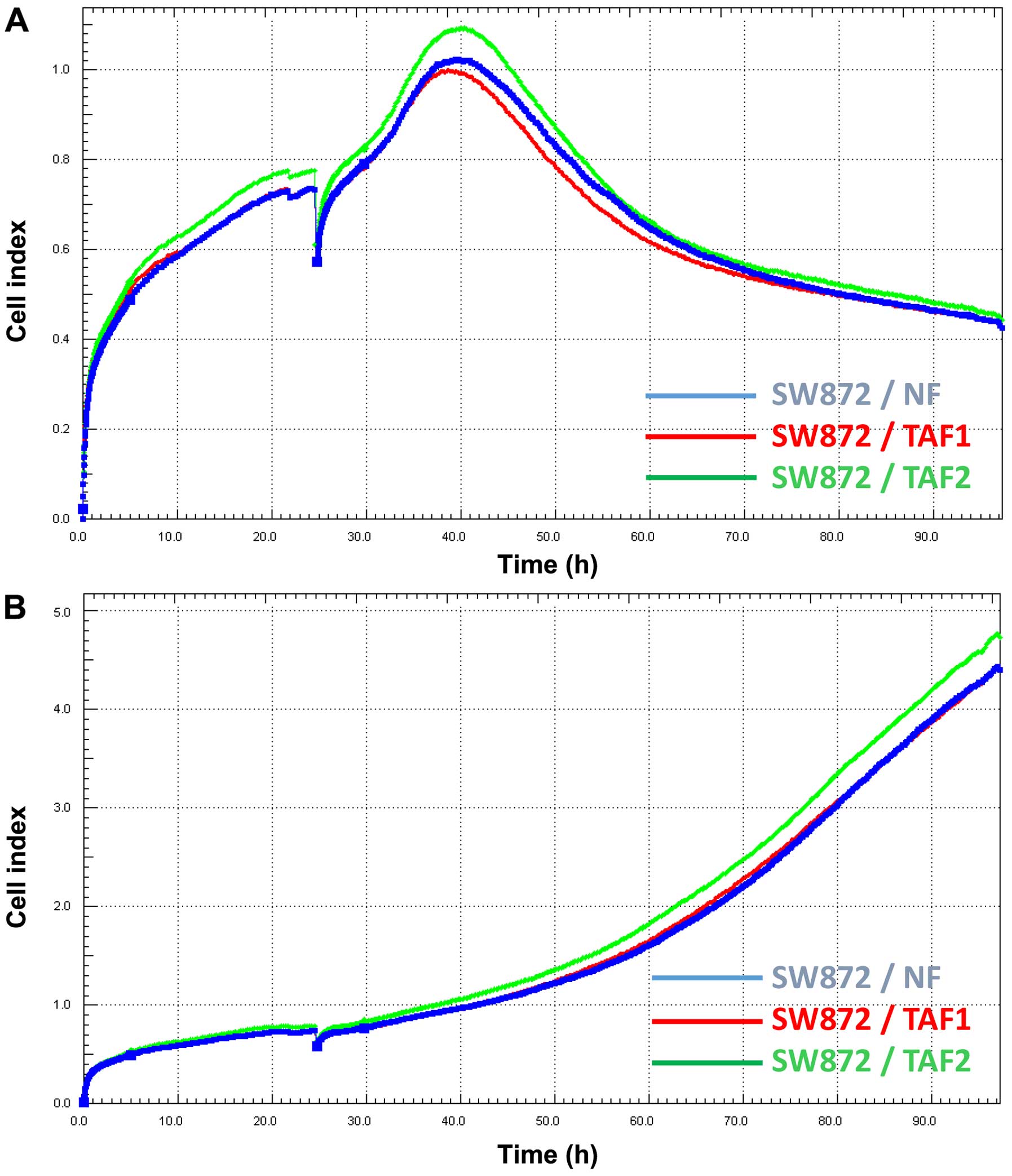
Doxorubicin treatment is less effective
in SW872 cells co-cultured with TAFs from high-grade
liposarcoma
The SW872 cells were pre-treated with different
co-cultures of NFs, TAF1 and TAF2. Thereafter, the
SW872 cells were seeded in plates with an integrated
microelectronic sensor array. After 24 h, doxorubicin was applied
to the treatment groups. The viability and proliferation of the
SW872 cells were monitored before and during doxorubicin incubation
in real-time (Fig. 4). The CI
which reflects the number of viable cells initially increased in
all treatment groups, but began to decrease after 15 h of
incubation with doxorubicin. Remarkably, the CI of the SW872 cells
which had been co-cultured previously with TAF2 diminished more
slightly than that of the cells that had been co-cultured with NFs
and TAF1. Finally, the CI of the cells co-cultured with TAF2
continuously remained at higher levels.
Discussion
Liposarcomas are rare tumors within the
heterogeneous group of soft tissue sarcomas and respond poorly to
conventional treatments, such as chemotherapy and radiation. Due to
the rarity of liposarcomas, the development of novel therapeutics
has been difficult, and the lack of novel chemotherapy protocols
remains a major obstacle. The mainstay of therapy still implies
complete surgical resection with the attainment of microscopically
negative margins (R0 resection). Nevertheless, the rates of local
recurrence in spite of complete resection are conspicuously high in
liposarcomas and cannot be explained by our current knowledge.
There have been several attempts to explain the high
rates of local recurrence (14).
One potential explanation includes that recurring tumors derive
from micrometastases in the tissue around the original location
which were left in spite of previous R0 resection and may be
selected out from biologically more aggressive tumor cells which
display higher invasive potential and, thus, facilitating local
recurrence. Another interesting hypothesis implies that altered but
non-malignant cells at the original location, such as TAFs may
promote the growth of viable but primarily histological inapparent
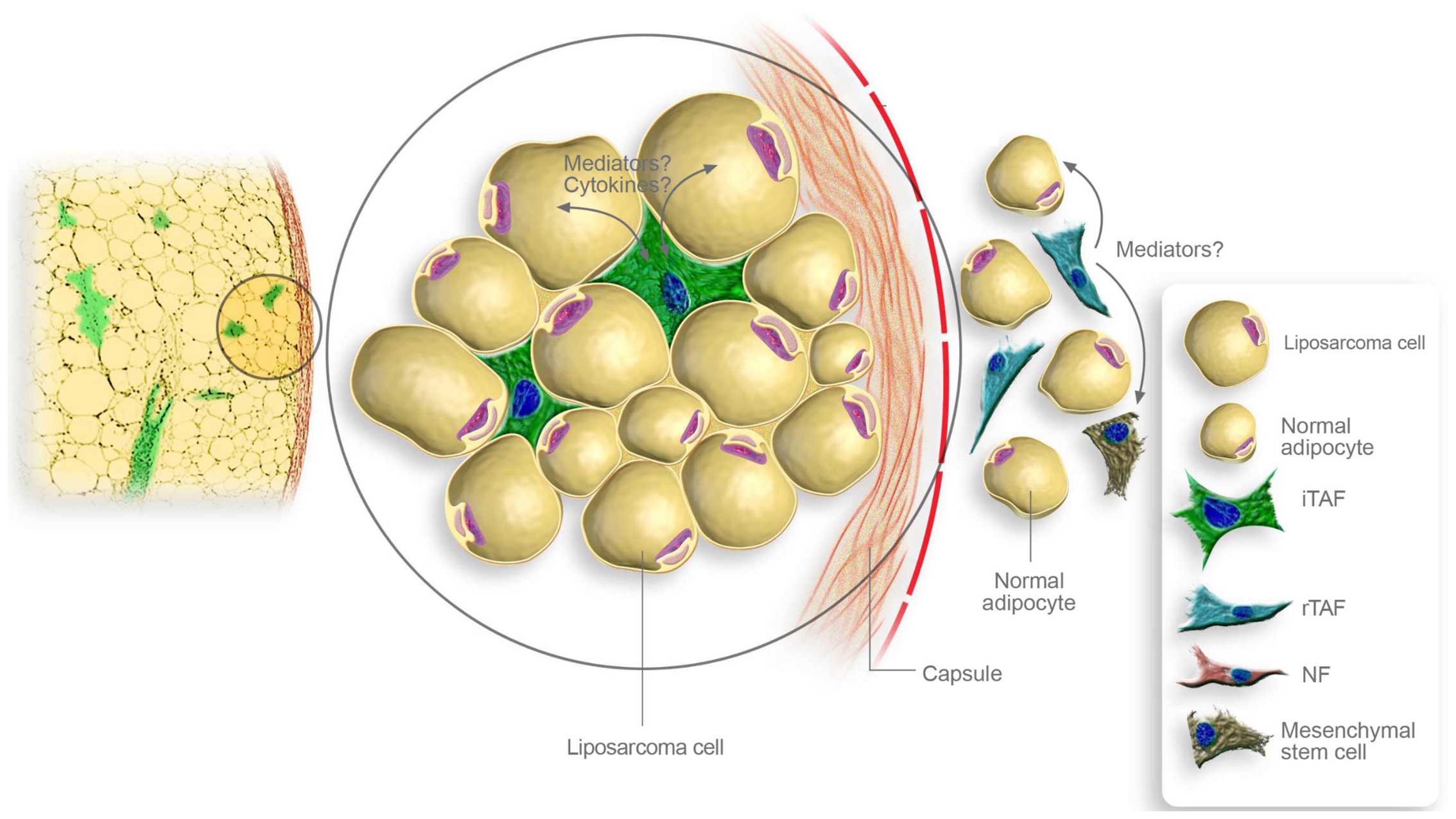
residual disease in the post-resection tumor bed. In the present
study, we demonstrated that TAFs were able to promote the
proliferation and viability of liposarcoma cells. Therefore, it
seems reasonable that TAFs may ensure the survival of remaining
liposarcoma cells in the post-resection tumor bed, leading to local
recurrence. In this context, further analyses should assess not
only the pro-tumorigenic effects of intratumoral TAFs, but also of
TAFs that were adjacent to the tumor and remain in the
post-resection tumor bed despite complete tumor resection (Fig. 5).
Interestingly, our experiments indicated that TAFs
from more malignant high-grade pleomorphic liposarcoma facilitated
the proliferation and viability of liposarcoma cells more
strikingly than TAFs from less malignant intermediate-grade
myxoid/round cell liposarcoma. Thus, histological tumor grading may
not only reflect the aggressiveness of the tumor cells, but may
also correlate with the pro-tumorigenic features of the inherent
TAFs. Vice versa, TAFs may acquire stronger tumor-promoting
properties when growing in more malignant tumor tissues.
Remarkably, TAFs from more malignant liposarcoma were able to
decrease the chemosensitivity of SW872 liposarcoma cells. Due to
our experimental design, the influence of TAFs on the
proliferation, viability and chemosensitivity of SW872 liposarcoma
cells was mediated through soluble factors that came into contact
with the liposarcoma cells during previous co-culture and led to
the sustaining alterations. Notably, NFs did not affect the
proliferation or drug resistance of liposarcoma cells, indicating a
complex bidirectional crosstalk between inherent TAFs and
liposracoma cells.
The tumor microenvironment and the involved
mediators deserve further investigation in liposarcomas. The
apparent contribution to development of drug resistance and tumor
progression make TAFs a potential therapeutic target. Present
studies are focusing on preclinical TAF-targeting approaches. In
contrast to tumor cells, TAFs represent a genetic stable target
which may be advantageous for immunotherapeutic approaches
(44,45). Further understanding of the
involved mediators also enables therapeutic intervention via
adjusted antigen body treatment (46). After identification of the
involved mediators the corresponding intracellular pathways leading
to chemoresistance and tumor progression in liposarcoma cells may
be determined and approached.
In conclusion, the present in vitro study
demonstrated that TAFs were able to promote the proliferation,
viability and drug resistance of liposarcoma cells. To our
knowledge, this is the first study that provides evidence for the
tumor-progressive influence of TAFs in liposarcoma. The encouraging
results of this study suggest experimental support for further
in vitro studies with larger cohorts involving all four
different liposarcoma subgroups.
References
|
1
|
Hoos A, Lewis JJ and Brennan MF: Soft
tissue sarcoma: prognostic factors and multimodal treatment.
Chirurg. 71:787–794. 2000.In German. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Mack TM: Sarcomas and other malignancies
of soft tissue, retroperitoneum, peritoneum, pleura, heart,
mediastinum, and spleen. Cancer. 75(Suppl 1): 211–244. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Dalal KM, Kattan MW, Antonescu CR, Brennan
MF and Singer S: Subtype specific prognostic nomogram for patients
with primary liposarcoma of the retroperitoneum, extremity, or
trunk. Ann Surg. 244:381–391. 2006.PubMed/NCBI
|
|
4
|
Kransdorf MJ: Malignant soft-tissue tumors
in a large referral population: distribution of diagnoses by age,
sex, and location. AJR Am J Roentgenol. 164:129–134. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Stojadinovic A, Leung DH, Hoos A, Jaques
DP, Lewis JJ and Brennan MF: Analysis of the prognostic
significance of microscopic margins in 2,084 localized primary
adult soft tissue sarcomas. Ann Surg. 235:424–434. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kaushal A and Citrin D: The role of
radiation therapy in the management of sarcomas. Surg Clin North
Am. 88:629–646. viii2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Singer S, Demetri GD, Baldini EH and
Fletcher CD: Management of soft-tissue sarcomas: an overview and
update. Lancet Oncol. 1:75–85. 2000. View Article : Google Scholar
|
|
8
|
Collin C, Godbold J, Hajdu S and Brennan
M: Localized extremity soft tissue sarcoma: an analysis of factors
affecting survival. J Clin Oncol. 5:601–612. 1987.PubMed/NCBI
|
|
9
|
Pisters PW and Pollock RE: Staging and
prognostic factors in soft tissue sarcoma. Semin Radiat Oncol.
9:307–314. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gaynor JJ, Tan CC, Casper ES, Collin CF,
Friedrich C, Shiu M, Hajdu SI and Brennan MF: Refinement of
clinicopathologic staging for localized soft tissue sarcoma of the
extremity: a study of 423 adults. J Clin Oncol. 10:1317–1329.
1992.PubMed/NCBI
|
|
11
|
Pisters PW, Leung DH, Woodruff J, Shi W
and Brennan MF: Analysis of prognostic factors in 1,041 patients
with localized soft tissue sarcomas of the extremities. J Clin
Oncol. 14:1679–1689. 1996.PubMed/NCBI
|
|
12
|
Matsumoto S, Ahmed AR, Kawaguchi N, Manabe
J and Matsushita Y: Results of surgery for malignant fibrous
histiocytomas of soft tissue. Int J Clin Oncol. 8:104–109. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lewis JJ, Leung D, Heslin M, Woodruff JM
and Brennan MF: Association of local recurrence with subsequent
survival in extremity soft tissue sarcoma. J Clin Oncol.
15:646–652. 1997.PubMed/NCBI
|
|
14
|
Daigeler A, Zmarsly I, Hirsch T, Goertz O,
Steinau HU, Lehnhardt M and Harati K: Long-term outcome after local
recurrence of soft tissue sarcoma: a retrospective analysis of
factors predictive of survival in 135 patients with locally
recurrent soft tissue sarcoma. Br J Cancer. 110:1456–1464. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Spillane AJ, Fisher C and Thomas JM:
Myxoid liposarcoma – the frequency and the natural history of
nonpulmonary soft tissue metastases. Ann Surg Oncol. 6:389–394.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ghadimi MP, Al-Zaid T, Madewell J, Peng T,
Colombo C, Hoffman A, Creighton CJ, Zhang Y, Zhang A, Lazar AJ, et
al: Diagnosis, management, and outcome of patients with
dedifferentiated liposarcoma systemic metastasis. Ann Surg Oncol.
18:3762–3770. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hoffman A, Ghadimi MP, Demicco EG,
Creighton CJ, Torres K, Colombo C, Peng T, Lusby K, Ingram D,
Hornick JL, et al: Localized and metastatic myxoid/round cell
liposarcoma: clinical and molecular observations. Cancer.
119:1868–1877. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Billingsley KG, Lewis JJ, Leung DH, Casper
ES, Woodruff JM and Brennan MF: Multifactorial analysis of the
survival of patients with distant metastasis arising from primary
extremity sarcoma. Cancer. 85:389–395. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Billingsley KG, Burt ME, Jara E, Ginsberg
RJ, Woodruff JM, Leung DH and Brennan MF: Pulmonary metastases from
soft tissue sarcoma: analysis of patterns of diseases and
postmetastasis survival. Ann Surg. 229:602–610; discussion 610–612.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Van Glabbeke M, van Oosterom AT,
Oosterhuis JW, Mouridsen H, Crowther D, Somers R, Verweij J,
Santoro A, Buesa J and Tursz T: Prognostic factors for the outcome
of chemotherapy in advanced soft tissue sarcoma: an analysis of
2,185 patients treated with anthracycline-containing first-line
regimens - a European Organization for Research and Treatment of
Cancer Soft Tissue and Bone Sarcoma Group Study. J Clin Oncol.
17:150–157. 1999.PubMed/NCBI
|
|
21
|
Italiano A, Toulmonde M, Cioffi A, Penel
N, Isambert N, Bompas E, Duffaud F, Patrikidou A, Lortal B, Le
Cesne A, et al: Advanced well-differentiated/dedifferentiated
liposarcomas: role of chemotherapy and survival. Ann Oncol.
23:1601–1607. 2012. View Article : Google Scholar
|
|
22
|
Italiano A, Garbay D, Cioffi A, Maki RG
and Bui B: Advanced pleomorphic liposarcomas: clinical outcome and
impact of chemotherapy. Ann Oncol. 23:2205–2206. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Jones RL, Fisher C, Al-Muderis O and
Judson IR: Differential sensitivity of liposarcoma subtypes to
chemotherapy. Eur J Cancer. 41:2853–2860. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Patel SR, Burgess MA, Plager C,
Papadopoulos NE, Linke KA and Benjamin RS: Myxoid liposarcoma.
Experience with chemotherapy. Cancer. 74:1265–1269. 1994.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Brodowicz T, Schwameis E, Widder J, Amann
G, Wiltschke C, Dominkus M, Windhager R, Ritschl P, Pötter R, Kotz
R and Zielinski CC: Intensified adjuvant IFADIC chemotherapy for
adult soft tissue sarcoma: a prospective randomized feasibility
trial. Sarcoma. 4:151–160. 2000. View Article : Google Scholar
|
|
26
|
Frustaci S, Gherlinzoni F, De Paoli A,
Bonetti M, Azzarelli A, Comandone A, Olmi P, Buonadonna A, Pignatti
G, Barbieri E, et al: Adjuvant chemotherapy for adult soft tissue
sarcomas of the extremities and girdles: results of the Italian
randomized cooperative trial. J Clin Oncol. 19:1238–1247.
2001.PubMed/NCBI
|
|
27
|
Judson I, Verweij J, Gelderblom H,
Hartmann JT, Schöffski P, Blay JY, Kerst JM, Sufliarsky J, Whelan
J, Hohenberger P, et al: European Organisation and Treatment of
Cancer Soft Tissue and Bone Sarcoma Group: Doxorubicin alone versus
intensified doxorubicin plus ifosfamide for first-line treatment of
advanced or metastatic soft-tissue sarcoma: a randomised controlled
phase 3 trial. Lancet Oncol. 15:415–423. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Blay JY, Casali P, Nieto A, Tanović A and
Le Cesne A: Efficacy and safety of trabectedin as an early
treatment for advanced or metastatic liposarcoma and
leiomyosarcoma. Future Oncol. 10:59–68. 2014. View Article : Google Scholar
|
|
29
|
Straussman R, Morikawa T, Shee K,
Barzily-Rokni M, Qian ZR, Du J, Davis A, Mongare MM, Gould J,
Frederick DT, et al: Tumour micro-environment elicits innate
resistance to RAF inhibitors through HGF secretion. Nature.
487:500–504. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Rong G, Kang H, Wang Y, Hai T and Sun H:
Candidate markers that associate with chemotherapy resistance in
breast cancer through the study on Taxotere-induced damage to tumor
microenvironment and gene expression profiling of
carcinoma-associated fibroblasts (CAFs). PLoS One. 8:e709602013.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wang W, Li Q, Yamada T, Matsumoto K,
Matsumoto I, Oda M, Watanabe G, Kayano Y, Nishioka Y, Sone S and
Yano S: Crosstalk to stromal fibroblasts induces resistance of lung
cancer to epidermal growth factor receptor tyrosine kinase
inhibitors. Clin Cancer Res. 15:6630–6638. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Hwang RF, Moore T, Arumugam T,
Ramachandran V, Amos KD, Rivera A, Ji B, Evans DB and Logsdon CD:
Cancer-associated stromal fibroblasts promote pancreatic tumor
progression. Cancer Res. 68:918–926. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Loeffler M, Krüger JA, Niethammer AG and
Reisfeld RA: Targeting tumor-associated fibroblasts improves cancer
chemotherapy by increasing intratumoral drug uptake. J Clin Invest.
116:1955–1962. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
34
|
Orimo A, Gupta PB, Sgroi DC,
Arenzana-Seisdedos F, Delaunay T, Naeem R, Carey VJ, Richardson AL
and Weinberg RA: Stromal fibroblasts present in invasive human
breast carcinomas promote tumor growth and angiogenesis through
elevated SDF-1/CXCL12 secretion. Cell. 121:335–348. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Lee YS, Choi I, Ning Y, Kim NY,
Khatchadourian V, Yang D, Chung HK, Choi D, LaBonte MJ, Ladner RD,
et al: Interleukin-8 and its receptor CXCR2 in the tumour
microenvironment promote colon cancer growth, progression and
metastasis. Br J Cancer. 106:1833–1841. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Olumi AF, Grossfeld GD, Hayward SW,
Carroll PR, Tlsty TD and Cunha GR: Carcinoma-associated fibroblasts
direct tumor progression of initiated human prostatic epithelium.
Cancer Res. 59:5002–5011. 1999.PubMed/NCBI
|
|
37
|
Kalluri R and Zeisberg M: Fibroblasts in
cancer. Nat Rev Cancer. 6:392–401. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Tarnowski M, Grymula K, Liu R, Tarnowska
J, Drukala J, Ratajczak J, Mitchell RA, Ratajczak MZ and Kucia M:
Macrophage migration inhibitory factor is secreted by
rhabdomyosarcoma cells, modulates tumor metastasis by binding to
CXCR4 and CXCR7 receptors and inhibits recruitment of
cancer-associated fibroblasts. Mol Cancer Res. 8:1328–1343. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Mishra P, Banerjee D and Ben-Baruch A:
Chemokines at the crossroads of tumor-fibroblast interactions that
promote malignancy. J Leukoc Biol. 89:31–39. 2011. View Article : Google Scholar
|
|
40
|
Augsten M: Cancer-associated fibroblasts
as another polarized cell type of the tumor microenvironment. Front
Oncol. 4(62)2014. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Sugimoto H, Mundel TM, Kieran MW and
Kalluri R: Identification of fibroblast heterogeneity in the tumor
microenvironment. Cancer Biol Ther. 5:1640–1646. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Harati K, Chromik AM, Bulut D, Goertz O,
Hahn S, Hirsch T, Klein-Hitpass L, Lehnhardt M, Uhl W and Daigeler
A: TRAIL and taurolidine enhance the anticancer activity of
doxorubicin, trabectedin and mafosfamide in HT1080 human
fibrosarcoma cells. Anticancer Res. 32:2967–2984. 2012.PubMed/NCBI
|
|
43
|
Koval OA, Sakaeva GR, Fomin AS, Nushtaeva
AA, Semenov DV, Kuligina EV, Gulyaeva LF, Gerasimov AV and Richter
VA: Sensitivity of endometrial cancer cells from primary human
tumor samples to new potential anticancer peptide lactaptin. J
Cancer Res Ther. 11:345–351. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Kakarla S, Song XT and Gottschalk S:
Cancer-associated fibroblasts as targets for immunotherapy.
Immunotherapy. 4:1129–1138. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Underwood TJ, Hayden AL, Derouet M, Garcia
E, Noble F, White MJ, Thirdborough S, Mead A, Clemons N, Mellone M,
et al: Cancer-associated fibroblasts predict poor outcome and
promote periostin-dependent invasion in oesophageal adenocarcinoma.
J Pathol. 235:466–477. 2015. View Article : Google Scholar :
|
|
46
|
Togo S, Polanska UM, Horimoto Y and Orimo
A: Carcinoma-associated fibroblasts are a promising therapeutic
target. Cancers (Basel). 5:149–169. 2013. View Article : Google Scholar
|