Introduction
Lung cancer is the leading cause of cancer death
worldwide (1). Although some
molecular-targeted drugs provide longer survival time than
cytotoxic chemotherapeutic agents (2–6),
their efficacy is limited. Earlier cancer immunotherapies such as
several types of vaccines have failed to show clinical
effectiveness because the mechanism of immunosuppression has not
been fully understood (7). Immune
checkpoint inhibitors are widely studied in cancer immunotherapy.
These agents, including cytotoxic T lymphocyte-associated antigen
(CTLA)-4, PD-1 and PD-L1 inhibitors show 10.2–24% overall response
rates in lung cancer patients in early-phase clinical trials
(8–12), several agents that target other
checkpoint proteins are now in clinical trial pipeline (13). Control of immunosuppression will be
an important aspect of effective cancer immunotherapy.
Regulatory T cells (Tregs) have been
widely studied in the context of immunosuppression (14). Tregs are characterized
by expression of transcription factor Foxp3 (15–17)
and are important in the cancer immunosuppressive mechanism. We
also reported that Treg levels significantly increase in
patients with non-small cell lung cancer (NSCLC), and high
peripheral Treg levels correlate with postoperative
disease recurrence (18). However,
how Tregs expand in cancer and how they influence tumor
immunology is unclear.
The Tregs are a heterogeneous population
and consist of at least two subsets: natural Tregs
(nTregs) and induced or adaptive Tregs
(iTregs) (19). The
nTregs originate in the thymus and are thought to
recognize self-antigens (20).
iTregs develop from conventional naïve T cell precursors
at extra-thymic sites by exposure to TGF-β and retinoic acid
(21). Because these two
Treg types are currently indistinguishable, their
relative contributions in tumor immunology are unclear. However,
expression of the transcription factor Helios, a member of the
Ikaros gene family, was recently proposed as a marker for
nTreg cells (22).
Thereafter, several reports showed iTregs also express
Helios in vitro and in vivo, which suggests that,
rather than a definite marker of nTregs, Helios could be
a marker of T cell activation (23–26).
Furthermore, Helios− Tregs reportedly display
greater suppressive capacity than do Helios+
Tregs (27). Thus, the
significance of Helios expression in Tregs is
controversial, and its clinical impact in patients with cancer is
totally unclear. The percentage of Helios+
Tregs was reported as significantly higher in peripheral
blood of patients with renal cell carcinoma (RCC) than in healthy
donors (HDs) (28). On the other
hand, in patients with premalignant respiratory papilloma (PRP),
the percentage of Helios+ Tregs was
significantly reduced among tumor infiltrating lymphocytes (TILs)
compared with blood (29).
However, to the best of our knowledge, this is the first study of
Helios+ or Helios− Tregs in
patients with lung cancer. In trying to understand the clinical
influence of Helios expression in patients with NSCLC in the
context of other investigations, we found that Helios−
Tregs were increased among peripheral Tregs
in patients with NSCLC, which implies that Helios−
Tregs in the tumor microenvironment might be clinically
important in tumor progression.
Materials and methods
Patients
We enrolled 64 patients with non-small cell lung
cancer (NSCLC) who were treated at Fukushima Medical University
Hospital in 2008, including 45 who were treated by surgery and 19
who were treated by chemotherapy because of advanced or recurrent
disease (Table I). Disease staging
was evaluated according to the International Staging System for
Lung Tumors, 7th edition (30).
 | Table IThe baseline demographics of the
patients. |
Table I
The baseline demographics of the
patients.
|
Characteristics | N=64 (%) |
|---|
| Age (years) |
| Mean ± SD | 67±8 |
| Gender |
| Female | 27 (42) |
| Male | 37 (58) |
| Pathological
stage |
| IA | 22 (34) |
| IB | 16 (25) |
| IIA | 4 (6) |
| IIB | 3 (5) |
| III | 0 (0) |
| IV (recurrence
included) |
| Chemotherapy |
| 1st line | 6 (9) |
| 2nd line | 6 (9) |
| 3rd or later
line | 7 (11) |
| Pathological
classification |
|
Adenocarcinoma | 51 (80) |
| Squamous cell
carcinoma | 10 (16) |
| Others | 3 (5) |
| EGFR mutation |
| Positive | 22 (34) |
| Negative | 31 (48) |
| Unknown | 11 (17) |
Patient specimens
Peripheral blood mononuclear cells
(PBMCs)
Peripheral blood samples were withdrawn prior to
treatment by surgery or chemotherapy. Samples were also taken from
10 HDs. PBMCs were isolated from peripheral venous blood (20–30 ml)
using Ficoll-Paque density gradient centrifugation, and then
cryopreserved at −80ºC. The PBMCs were thawed for flow cytometry,
washed in AIM-V medium (Invitrogen, Carlsbad, CA, USA), counted in
the presence of trypan blue dye to evaluate viability and used
immediately.
Tumor tissues
Tumor tissues were obtained from patients who i)
were suffering from primary NSCLC with confirmed stage (T1-T3,
pN0-pN2 and pM0); ii) underwent curative surgery but did not
receive any preoperative treatment; and iii) had available clinical
follow-up data. All patients had at least 5-year follow-up
information for the present study. As 9 patients had recurrent
diseases, we selected 9 other recurrence-free patients with matched
pathological stages (i.e., 18 patients out of the 45 treated
surgically) to examine their immunohistochemical differences in
Helios expression in the tumor microenvironment.
Flow cytometry
Cell-surface and intracellular staining procedures
were performed as previously described (31). Surfaces of 100 μl of cells
(1×106) were stained using 10 μl fluorescein
isothiocyanate-conjugated anti-CD25 and peridinin
chlorophyll-conjugated anti-CD4 (eBiosciences, San Jose, CA, USA).
Isotype control, mouse IgG1, was included in all the experiments.
For intracellular staining, cells were saponized, washed in cold
flow cytometry staining buffer and stained with
phycoerythrin-conjugated anti-human Foxp3, its isotype control rat
IgG2a (eBiosciences), Adenomatous polyposis coli
anti-mouse/human Helios, and its isotype control Armenian Hamster
IgG (BioLegend, Inc., San Diego, CA, USA). Flow cytometry was
performed using FACSCanto II (BD Biosciences). Acquisition and
analysis gates were restricted to the lymphocyte gate, as
determined by their characteristic forward and side scatter
properties. Flow data were analyzed using FlowJo software, version
7.6.5 (FlowJo, LLC, Ashland, OR, USA).
Immunohisitochemistry
We cut 3-μm microtome sections from
paraffin-embedded lung cancer specimens and performed
immunoperoxidase staining by the avidin-biotin-peroxidase complex
method. The sections were dewaxed in xylene and dehydrated through
an alcohol gradient. Endogenous peroxidase activity was quenched by
20-min incubation with 0.3% (v/v) solution of hydrogen peroxidase
(Wako Pure Chemical Industries Ltd., Osaka, Japan) in 100%
methanol. Following incubation in 5% dried skimmed milk in
phosphate-buffered saline (PBS) for 30 min at room temperature, the
sections were incubated overnight at 4ºC with primary monoclonal
antibody to Helios (1:50; GTX115629; GeneTex, Inc., Irvine, CA,
USA), to Foxp3 protein (1:100; ab20034; Abcam Inc., Tokyo, Japan),
CD4 (1:50; NCL-CD4-1F6; Leica Microsystems, Wetzlar, Germany). The
primary antibody was then detected using biotinylated secondary
anti-rabbit IgG antibody (E0431; Dako, Glostrup, Denmark), or
anti-mouse IgG antibody (BA-2000; Vector Laboratories, Burlingame,
CA, USA) by the avidin-biotin complex method. The sections were
washed several times in PBS after each step and counterstained with
Mayer's hematoxylin (Muto Pure Chemicals, Co., Ltd., Tokyo, Japan),
dehydrated through an alcohol gradient and mounted on glass
slides.
For each specimen, we took micrographs of 10
randomly selected fields with a microscope (IX73; Olympus, Co.,
Tokyo, Japan), a CCD camera (DP73; Olympus), and counted the
positively-stained lymphocytes at high-power fields (HPF, ×400). We
made sure to select the same field for each stain (CD4, Foxp3 and
Helios).
Statistical analysis
In peripheral Tregs, first we found
percentages of Foxp3+ Helios+ cells,
Foxp3+ Helios− cells in CD4+ T
cells, and Helios+ and Helios− cells among
CD4+ Foxp3+ cells. In Treg TILs,
we counted the number of CD4+ T cells
immunohistochemically. Then we counted Foxp3+ cells in
CD4+ T cells, Helios+ and Helios−
cells in CD4+ Foxp3+ cells, and analyzed
associations between Helios expressions and clinicopathological
factors, which were evaluated using Pearson's χ2 test. Differences
between groups were evaluated for statistical significance using
the Student's t-test. Survival curves were drawn according to the
Kaplan-Meier method. We compared recurrence-free survival (RFS) and
overall survival (OS) between groups of patients who expressed high
and low Helios levels among their CD4+ Foxp3+
cells by log-rank test. All analyses were performed using GraphPad
Prism 5 software (GraphPad Software Inc., La Jolla, CA, USA).
P<0.05 was considered to be statistically significant.
Ethics statement
The present study was approved by the Ethics
Committee of the Fukushima Medical University (no. 2075). Written
informed consent was also obtained from all the patients.
Results
Helios expression in peripheral
Treg
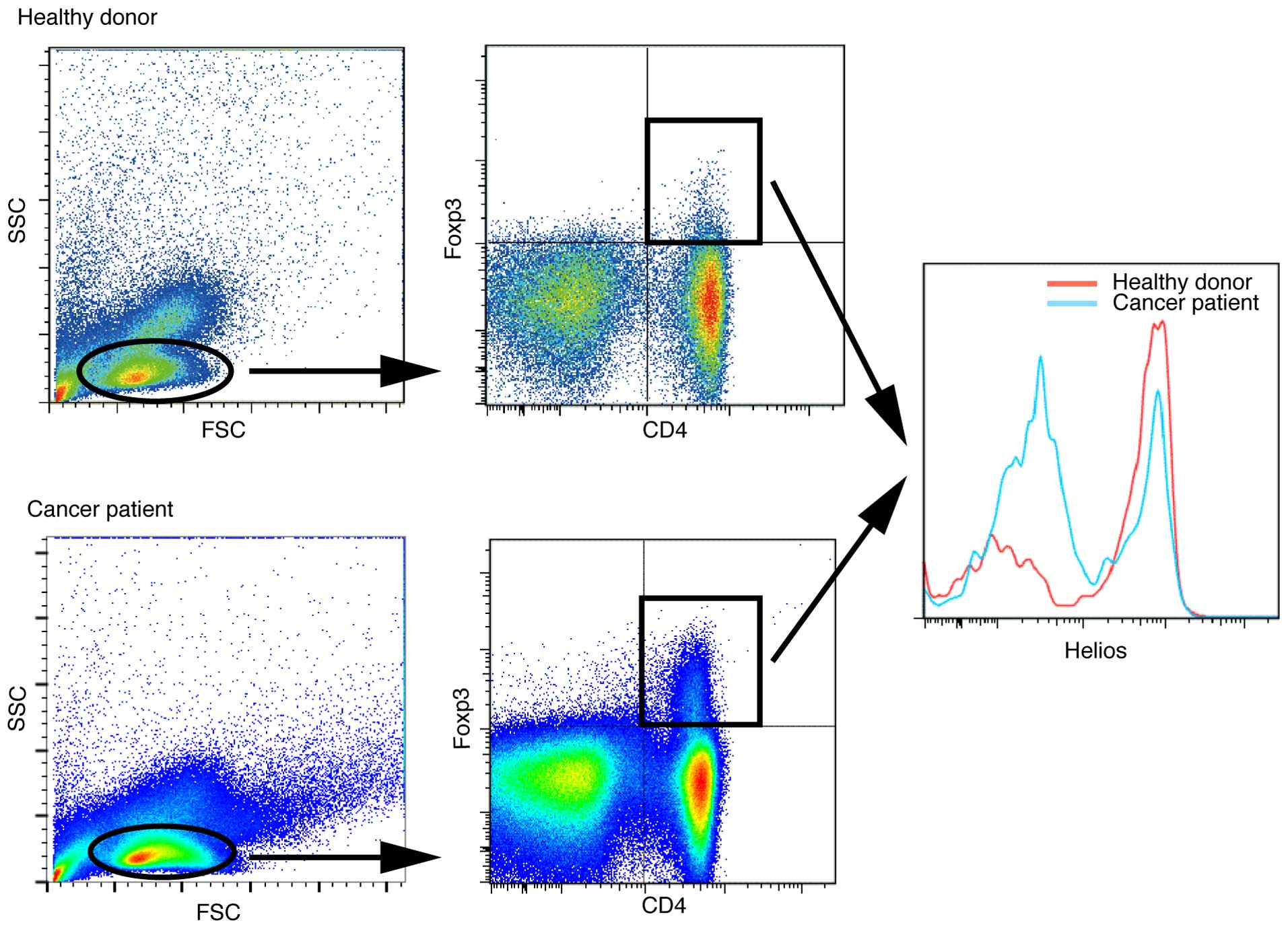
We first compared the expression of Foxp3 and Helios
among CD4+ T cells in peripheral blood of 64 patients
with NSCLC and 10 HDs. A representative flow cytometry plot of CD4,
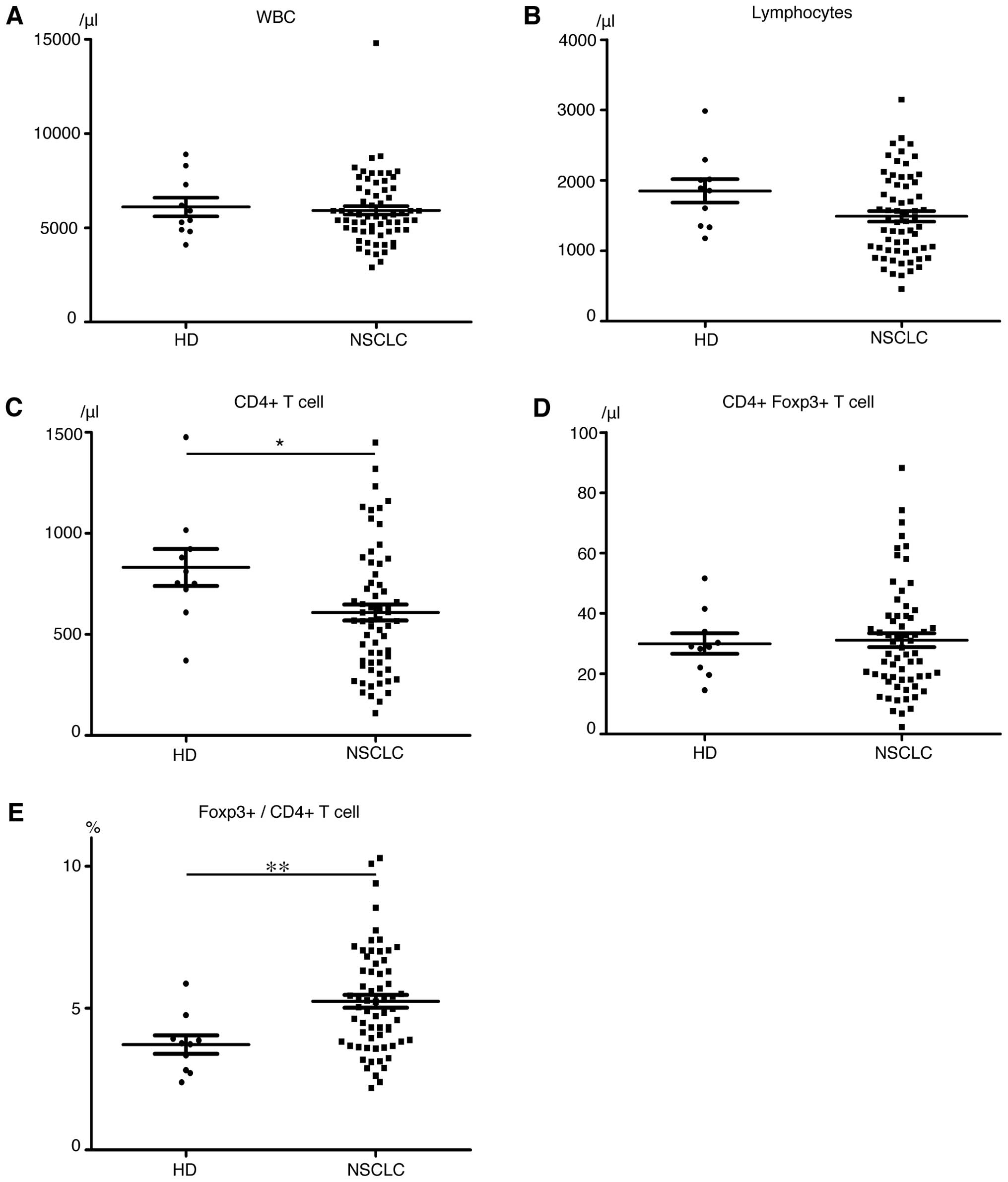
Foxp3 and Helios expression is shown in Fig. 1. The HDs and NSCLC patients had
approximately equal numbers of white blood cells (Fig. 2A) and lymphocytes (Fig. 2B), but the cancer patients had
lower CD4+ T cell levels (P=0.04, Fig. 2C). Although levels of
CD4+ Foxp3+ T cells (Fig. 2D) did not significantly differ
between patients and HDs, the percentage of Foxp3+ cells
among CD4+ T cells was significantly higher in patients
(HDs, 3.72%; patients, 5.24%; P=0.001, Fig. 2E). Helios expression in
Foxp3+ cells was 47.5±13.3% in patients and 55.9±12.3%
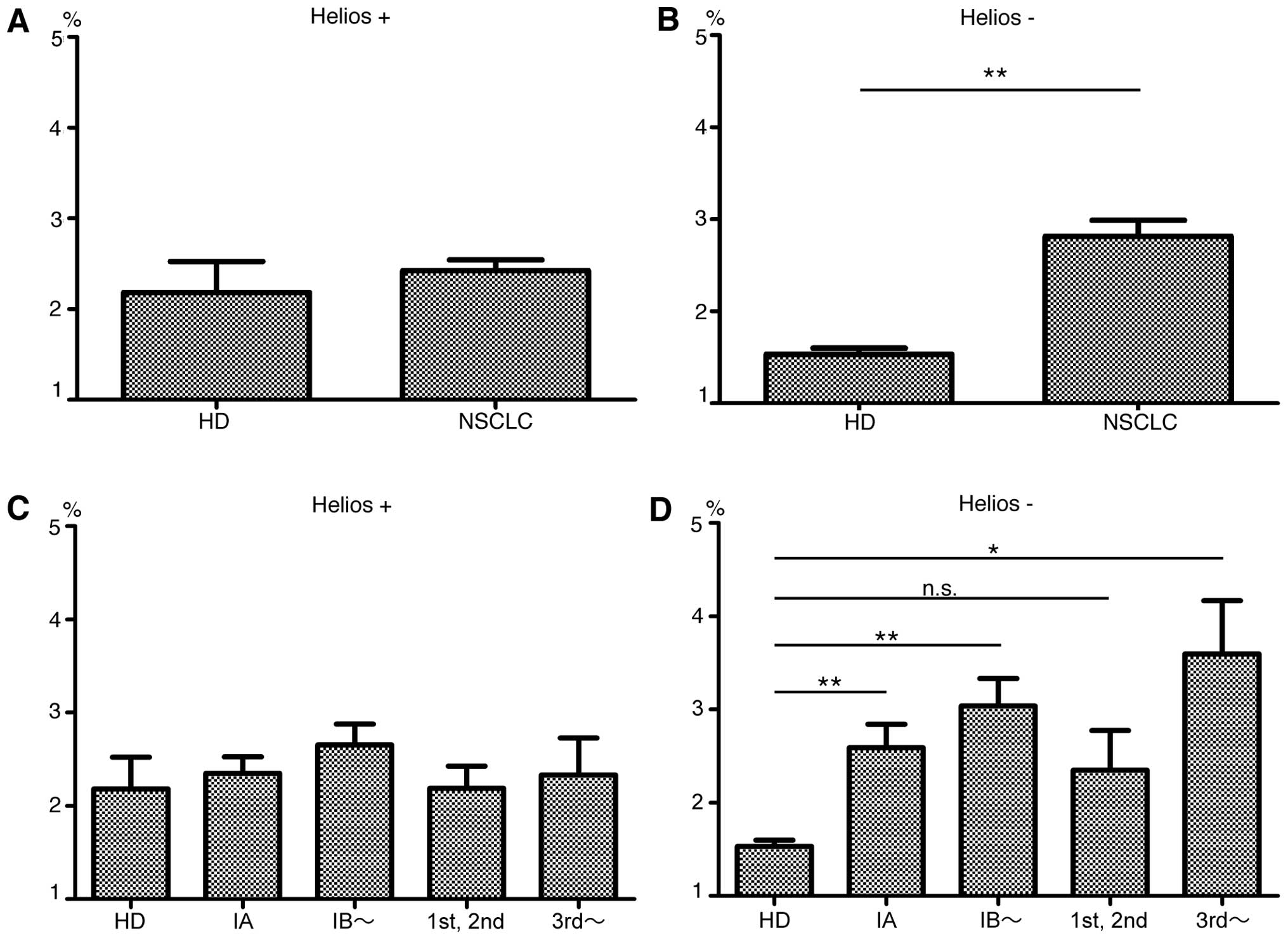
in HDs (P=0.07). Among CD4+ Foxp3+ T cells,
patients had significantly higher Helios− subpopulation
levels (P<0.0001) but Helios+ cell levels did not
significantly differ between HDs and patients (Fig. 3A and B). These results indicate
that expanded Treg levels in NSCLC patients are mainly
Helios− cells. Notably, even patients with early-stage
(stage IA) disease had significantly higher percentages of
Helios− Treg among their CD4+ T
cells than did HDs (HDs, 1.5%; all NSCLC patients, 2.4%; stage IA
patients, 2.6%; P=0.0005). The Helios− subpopulation,
but not the Helios+ subpopulation, tended to increase
with cancer progression (Fig. 3C and
D). We divided patients in high and low Helios-expressing
groups by median Helios expression among peripheral CD4+
Foxp3+ T cells (50.3%), and compared clinicopathological
features, but found no significant differences (Table II).
| Table IICharacteristics of patients with
NSCLC by levels of Helios expression in their regulatory T cells in
PBMCs (N=64) and tumor sites (N=18). |
Table II
Characteristics of patients with
NSCLC by levels of Helios expression in their regulatory T cells in
PBMCs (N=64) and tumor sites (N=18).
| PBMC Helios
expression | | TIL Helios
expression | |
|---|
|
| |
| |
|---|
|
Characteristics | High
n=32 (50%) | Low
n=32 (50%) | P-value
high vs. low | High
n=9 (50%) | Low
n=9 (50%) | P-value
high vs. low |
|---|
| Age (years) |
| <65 | 10 (31) | 14 (44) | 0.3 | 4 (44) | 1 (11) | 0.1 |
| ≥65 | 22 (69) | 18 (56) | | 5 (56) | 8 (89) | |
| Gender |
| Female | 14 (44) | 13 (41) | 0.8 | 6 (67) | 4 (44) | 0.3 |
| Male | 18 (56) | 19 (59) | | 3 (33) | 5 (56) | |
| Pathological
stage |
| I | 18 (56) | 20 (63) | 0.5 | 9 (100) | 4 (44) | 0.02 |
| II | 2 (6) | 2 (6) | | 0 (0) | 2 (11) | |
| III | 3 (9) | 0 (0) | | 0 (0) | 3 (17) | |
| IV (recurrence
included) | 9 (28) | 10 (31) | | 0 (0) | 0 (0) | |
| Pathology |
|
Adenocarcinoma | 26 (81) | 25 (78) | 0.8 | 7 (78) | 9 (100) | 0.2 |
| Squamous cell
carcinoma | 5 (16) | 5 (16) | | 2 (22) | 0 (0) | |
| Others | 1 (3) | 2 (6) | | 0 (0) | 0 (0) | |
| EGFR mutation |
| Positive | 15 (47) | 7 (22) | 0.1 | 4 (44) | 5 (56) | 0.3 |
| Negative | 13 (41) | 18 (56) | | 3 (33) | 4 (44) | |
| Unknown | 4 (13) | 7 (22) | | 2 (22) | 0 (0) | |
Helios expression in Treg
TILs
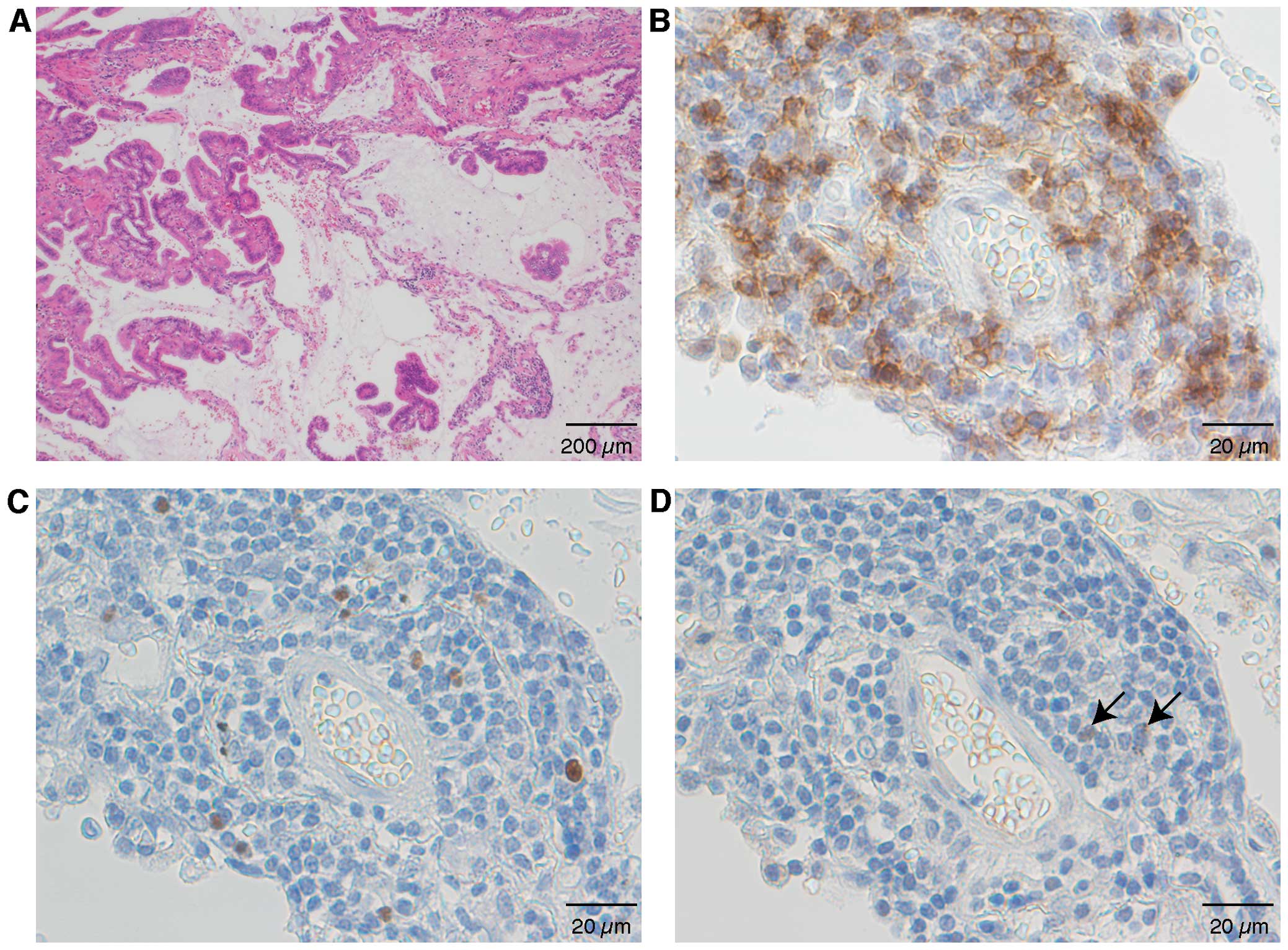
Next we evaluated Tregs in the tumor
microenvironment, and found Foxp3+ among CD4+
T cells 27.1±12.3% (mean ± SD); Helios+ among
Foxp3+ T cells: 18.1±13.4%; and Helios+
Foxp3+ among CD4+ T cells: 5.3±5.2% (Fig. 4). CD4+ T cells existed
in clusters (Fig. 4A and B), with
Foxp3+ cells scattered around the CD4+ T
cells (Fig. 4C). Few
Helios+ cells were at the same site (Fig. 4D), which indicated that most
CD4+ Foxp3+ cells at the tumor sites were
Helios−. Thus, the Helios+ Tregs
percentage was low among both TIL Tregs and peripheral
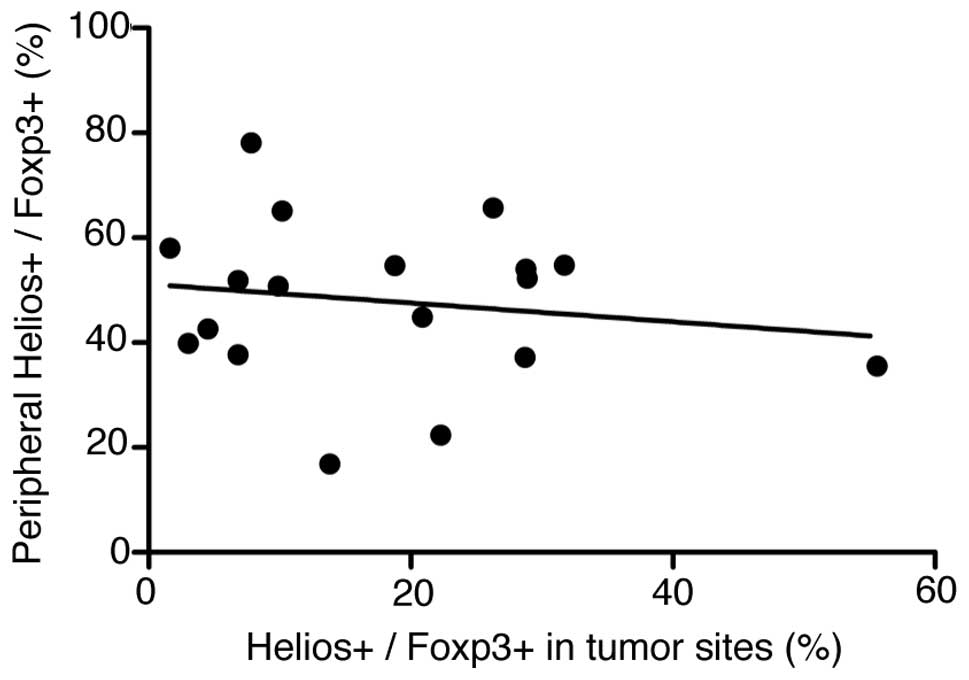
Tregs. We saw a weak but not significant relationship
between Helios expression in peripheral-blood Tregs and
that in Treg TILs (Fig.
5). Clinicopathological parameters were analyzed against TILs
(Table II). When the patients
were divided by median Helios+ percentage in their TIL
CD4+ Foxp3+ T cells (16.3%) into high- and
low-Helios expressing groups, the low Helios expressing group had
significantly more advanced-stage disease (P=0.02).
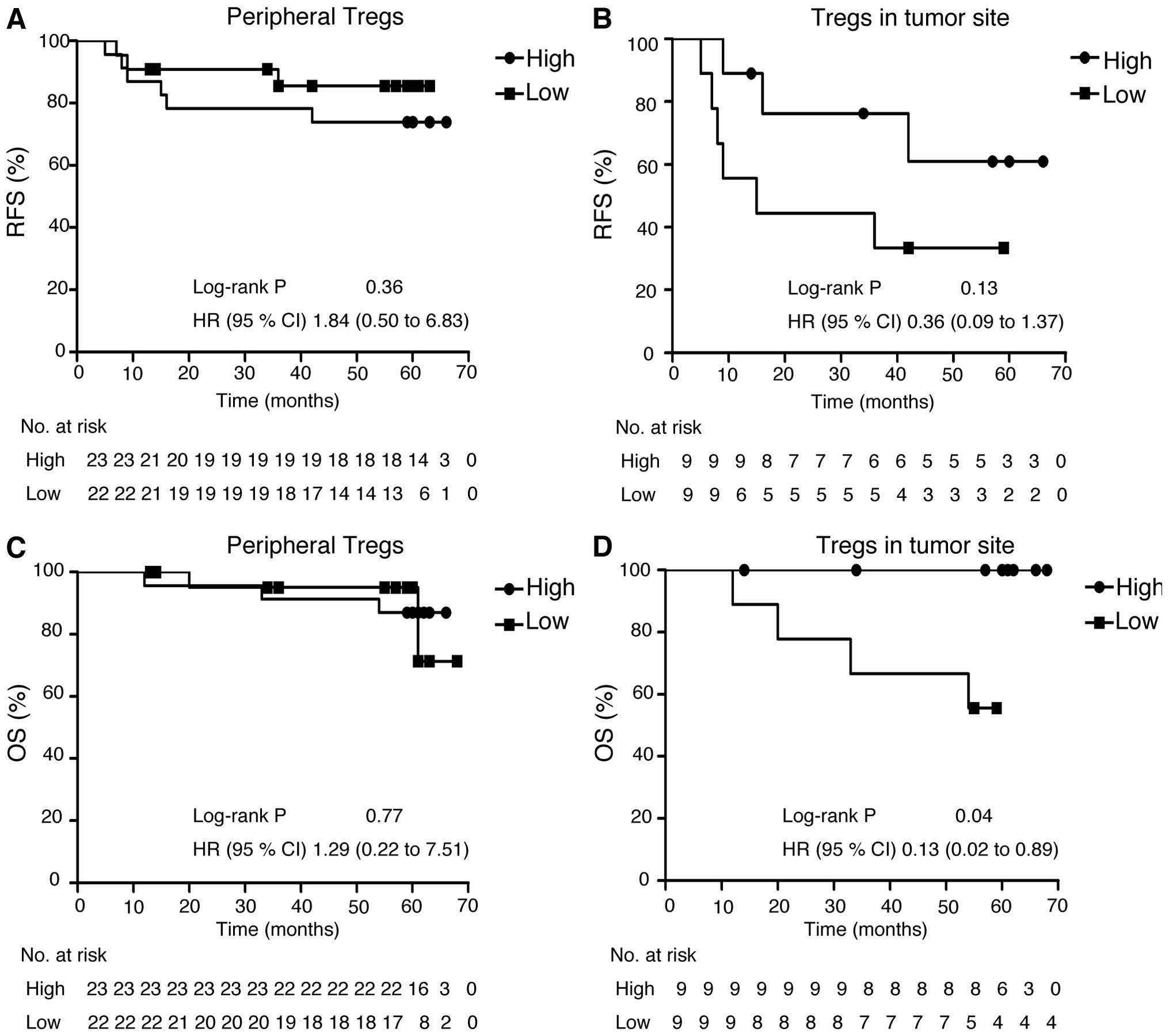
Survival analysis according to Helios
expression in Treg
We further analyzed survival outcomes for patients
with NSCLC by their Helios expression in Treg among
TILs. For the 45 patients who provided PBMCs, median follow-up was
1666 days; relapse occurred in 9 patients and 5 patients died
during follow-up. For the 18 patients who provided the specimens
for analysis of Treg TILs, the median follow-up was 1525
days; this group included the same patients who relapsed and who
died in the former group. The patients who provided tumor specimens
did not significantly differ in RFS or OS from those who provided
only PBMCs. Patients with lower Helios expression among their
Treg TILs had significantly poorer OS (P=0.038), but not
significantly poorer RFS (Fig.
6).
Discussion
To date, very few reports have addressed Helios
expression in peripheral CD4+ Foxp3+ T cells.
According to these previous reports, the percentage of
Helios+ Tregs in patients with RCC was ~60%
(28) and in PRP was 66.1±6.5%
(29). In the present study, we
show that Helios expression among CD4+ Foxp3+
cells was 47.5±13.3% in patients with NSCLC, lower than previous
data but almost compatible. The percentage of Helios+
among CD4+ Foxp3+ T cells was significantly
lower in these patients than those of HDs (NSCLC, 47.5%; HD,
55.9%). This is the first report of Helios expression status in
Tregs from patients with NSCLC; it was significantly
decreased in patients with NSCLC than in HDs. Interestingly, even
higher percent-ages of Helios− Tregs were
seen in advanced-stage NSCLC. These results show expanded
Tregs in patients with NSCLC to be Helios−
cells, which implies that Helios− Tregs
mediate immunosuppression in NSCLC. These results are inconsistent
with the earlier reports on RCC and PRP, and suggest that the role
of these cells in immunosuppression may vary between the type of
tumor. However, these data are still limited; further studies are
needed to understand these findings.
Among TILs, Helios expression in Foxp3+
cells was 18.1±13.4% in patients with NSCLC in this series.
Helios− Tregs in tumor sites were associated
with patient prognoses. Wainwright et al reported that
Helios was expressed by almost 90% of Tregs in
glioblastoma (32), but in only
31.2±18.51% of Tregs in PRP (29). These data also imply that the
immunosuppressive status in the tumor microenvironment may depend
on the type of tumor. Our findings indicate that Helios−
Tregs have an essential role in immunosuppression, at
least in NSCLC. According to the previous study showing that Helios
could be a biomarker for nTregs (22), the present study suggests that
iTregs were mainly increased in patients with NSCLC
patients and might be induced in tumor microenvironment.
However, recent reports suggest that
nTregs from iTregs are not distinguished only
by Helios expression (25). Other
molecular markers are now under study. Several promising molecules
are epigenetic Treg-specific demethylated region (TSDR)
modifications and Neuropilin 1. Reportedly, epigenetic
modifications in the TSDR of the Foxp3 locus affect the
stability of Foxp3 (33), and are
thought to differ between nTregs from iTregs
cells (34). Neuropilin 1 is a
receptor for vascular endothelial growth factor and semaphorin
family proteins (35), and is
reported to be a possible marker for nTregs (36,37).
In spite of these studies, a definitive marker for
nTregs has not been found so far (38).
Our findings suggest that Helios−
Tregs could have an important function in NSCLC. We must
next elucidate the function of Helios− Tregs
in immunosuppression to verify their role in cancer immune
response. For such a study, we need to obtain a definitive
cell-surface marker for Helios− Tregs, as
Helios is a transcription factor. To solve this problem, Neuropilin
1 may be useful as mentioned above (35). Other cell-surface markers have been
reported. Zabransky et al reported CD103 and
glucocorticoid-induced tumor necrosis receptor (GITR) (25), and Raffin et al described
IL-1RI and CCR7 (27). Currently,
we are trying to separate Helios− Tregs from
other CD4+ T cells using IL-1RI and CCR7, which gave
70–80% specificity (data not shown). Further studies are needed to
find a definitive cell-surface marker and establish the effects of
Helios− Tregs on immunosuppression.
Successful blockades of immune checkpoints suggest
that immune escape mechanisms clearly contribute to lung cancer
progression, and also could be targets for lung cancer treatment.
To date, attempts have been made to suppress Tregs
function by using anti-CD25 antibody (39–41),
and by inhibiting the CTLA-4 pathway (12,42),
or GITR family-related proteins (43). These trials did not work well.
According to the present study, Helios− Tregs
could be both a useful prognostic biomarker in NSCLC patients and a
therapeutic target. If we can ascertain the mechanism of
immunosuppression, we may be able to establish more powerful
immunotherapy. For instance, peptide vaccine has been one of the
main streams of immunotherapy. Although peptide vaccine therapy for
NSCLC could not achieve a survival benefit in a late-phase studies
(44), other trials, such as our
multiple peptide vaccine therapy for NSCLC, have been expected to
induce strong specific T cell responses (45). Combination therapy of blockades of
immunosuppressive pathway, including immune checkpoints and/or
Tregs that target Helios− Tregs
and these peptide vaccines could be a next-generation
immunotherapy.
In summary, in the present study we demonstrated
the clinical impact of both local and systemic Helios−
Treg cells. Systemic Helios− Tregs
correlate with advanced cancer stage, and those in tumor sites are
associated with poor patient prognosis. Thus, analyzing Helios
expression levels in Tregs could be a useful marker for
disease progression and prognosis in patients with NSCLC.
Furthermore, it also could be a novel therapeutic target for
various cancers. Further study is needed to understand the function
of Helios− Tregs in immune suppression, and
to develop therapeutic modality targeting cancer-specific
Tregs.
Acknowledgements
We thank E. Ohtomo, Y. Kikuta and Y. Yuda for their
excellent technical assistance.
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Mitsudomi T, Morita S, Yatabe Y, Negoro S,
Okamoto I, Tsurutani J, Seto T, Satouchi M, Tada H, Hirashima T, et
al; West Japan Oncology Group. Gefitinib versus cisplatin plus
docetaxel in patients with non-small-cell lung cancer harbouring
mutations of the epidermal growth factor receptor (WJTOG3405): An
open label, randomised phase 3 trial. Lancet Oncol. 11:121–128.
2010. View Article : Google Scholar
|
|
3
|
Maemondo M, Inoue A, Kobayashi K, Sugawara
S, Oizumi S, Isobe H, Gemma A, Harada M, Yoshizawa H, Kinoshita I,
et al; North-East Japan Study Group. Gefitinib or chemotherapy for
non-small-cell lung cancer with mutated EGFR. N Engl J Med.
362:2380–2388. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Zhou C, Wu YL, Chen G, Feng J, Liu XQ,
Wang C, Zhang S, Wang J, Zhou S, Ren S, et al: Erlotinib versus
chemotherapy as first-line treatment for patients with advanced
EGFR mutation-positive non-small-cell lung cancer (OPTIMAL,
CTONG-0802): A multicentre, open-label, randomised, phase 3 study.
Lancet Oncol. 12:735–742. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Solomon BJ, Mok T, Kim DW, Wu YL, Nakagawa
K, Mekhail T, Felip E, Cappuzzo F, Paolini J, Usari T, et al;
PROFILE 1014 Investigators. First-line crizotinib versus
chemotherapy in ALK-positive lung cancer. N Engl J Med.
371:2167–2177. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Shaw AT, Yeap BY, Solomon BJ, Riely GJ,
Gainor J, Engelman JA, Shapiro GI, Costa DB, Ou SH, Butaney M, et
al: Effect of crizotinib on overall survival in patients with
advanced non-small-cell lung cancer harbouring ALK gene
rearrangement: A retrospective analysis. Lancet Oncol.
12:1004–1012. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Rosenberg SA, Yang JC and Restifo NP:
Cancer immunotherapy: Moving beyond current vaccines. Nat Med.
10:909–915. 2004. View
Article : Google Scholar : PubMed/NCBI
|
|
8
|
Brahmer JR, Tykodi SS, Chow LQM, Hwu WJ,
Topalian SL, Hwu P, Drake CG, Camacho LH, Kauh J, Odunsi K, et al:
Safety and activity of anti-PD-L1 antibody in patients with
advanced cancer. N Engl J Med. 366:2455–2465. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Garon E, Balmanoukian A, Hamid O, Hui R,
Gandhi L and Leighi N: Preliminary clinical safety and activity of
MK-3475 monotherapy for the treatment of previously treated
patients with non-small cell lung cancer. In: IASLC 15th World
Conference on Lung Cancer; 27–31 October; Sydney, Australia.
2013
|
|
10
|
Herbst RS, Gordon MS and Fine GD: A study
of MPDL3280A, an engineered PD-L1 antibody in patients with locally
advanced or metastatic tumors. J Clin Oncol. 31:30002013.
|
|
11
|
Horn L, Herbst R and Spiegel D: An
analysis of the relationship of clinical activity to baseline EGFR
status PD-L1 expression and prior treatment history in patients
with non-small cell lung cancer (NSCLC) following PD-L1 blockade
with MPDL3280A (anti-PDL1). In: IASLC 14th World Conference on Lung
Cancer; July 3–7; Amsterdam, The Netherlands. 2012
|
|
12
|
Lynch TJ, Bondarenko I, Luft A,
Serwatowski P, Barlesi F, Chacko R, Sebastian M, Neal J, Lu H,
Cuillerot JM, et al: Ipilimumab in combination with paclitaxel and
carboplatin as first-line treatment in stage IIIB/IV non-small-cell
lung cancer: Results from a randomized, double-blind, multicenter
phase II study. J Clin Oncol. 30:2046–2054. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Creelan BC: Update on immune checkpoint
inhibitors in lung cancer. Cancer Control. 21:80–89. 2014.
|
|
14
|
deLeeuw RJ, Kost SE, Kakal JA and Nelson
BH: The prognostic value of FoxP3+ tumor-infiltrating
lymphocytes in cancer: A critical review of the literature. Clin
Cancer Res. 18:3022–3029. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hori S, Nomura T and Sakaguchi S: Control
of regulatory T cell development by the transcription factor Foxp3.
Science. 299:1057–1061. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Fontenot JD, Gavin MA and Rudensky AY:
Foxp3 programs the development and function of
CD4+CD25+ regulatory T cells. Nat Immunol.
4:330–336. 2003. View
Article : Google Scholar : PubMed/NCBI
|
|
17
|
Khattri R, Cox T, Yasayko SA and Ramsdell
F: An essential role for Scurfin in CD4+CD25+
T regulatory cells. Nat Immunol. 4:337–342. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hasegawa T, Suzuki H, Yamaura T, Muto S,
Okabe N, Osugi J, Hoshino M, Higuchi M, Ise K and Gotoh M:
Prognostic value of peripheral and local forkhead box
P3+ regulatory T cells in patients with non-small-cell
lung cancer. Mol Clin Oncol. 2:685–694. 2014.PubMed/NCBI
|
|
19
|
Curotto de Lafaille MA and Lafaille JJ:
Natural and adaptive foxp3+ regulatory T cells: More of
the same or a division of labor? Immunity. 30:626–635. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Apostolou I, Sarukhan A, Klein L and von
Boehmer H: Origin of regulatory T cells with known specificity for
antigen. Nat Immunol. 3:756–763. 2002.PubMed/NCBI
|
|
21
|
Bilate AM and Lafaille JJ: Induced CD4
Foxp3 regulatory T cells in immune tolerance. Annu Rev Immunol.
30:733–758. 2012. View Article : Google Scholar
|
|
22
|
Thornton AM, Korty PE, Tran DQ, Wohlfert
EA, Murray PE, Belkaid Y and Shevach EM: Expression of Helios, an
Ikaros transcription factor family member, differentiates
thymic-derived from peripherally induced Foxp3+ T
regulatory cells. J Immunol. 184:3433–3441. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Akimova T, Beier UH, Wang L, Levine MH and
Hancock WW: Helios expression is a marker of T cell activation and
proliferation. PLoS One. 6:e242262011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gottschalk RA, Corse E and Allison JP:
Expression of Helios in peripherally induced Foxp3+
regulatory T cells. J Immunol. 188:976–980. 2012. View Article : Google Scholar
|
|
25
|
Zabransky DJ, Nirschl CJ, Durham NM, Park
BV, Ceccato CM, Bruno TC, Tam AJ, Getnet D and Drake CG: Phenotypic
and functional properties of Helios+ regulatory T cells.
PLoS One. 7:e345472012. View Article : Google Scholar
|
|
26
|
Getnet D, Grosso JF, Goldberg MV, Harris
TJ, Yen HR, Bruno TC, Durham NM, Hipkiss EL, Pyle KJ and Wada S: A
role for the transcription factor Helios in human
CD4+CD25+ regulatory T cells. Mol Immunol.
47:1595–1600. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Raffin C, Pignon P, Celse C, Debien E,
Valmori D and Ayyoub M: Human memory Helios−
FOXP3+ regulatory T cells (Tregs) encompass induced
Tregs that express Aiolos and respond to IL-1β by downregulating
their suppressor functions. J Immunol. 191:4619–4627. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Elkord E, Sharma S, Burt DJ and Hawkins
RE: Expanded subpopulation of FoxP3+ T regulatory cells
in renal cell carcinoma co-express Helios, indicating they could be
derived from natural but not induced Tregs. Clin Immunol.
140:218–222. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Hatam LJ, Devoti JA, Rosenthal DW, Lam F,
Abramson AL, Steinberg BM and Bonagura VR: Immune suppression in
premalignant respiratory papillomas: Enriched functional
CD4+Foxp3+ regulatory T cells and
PD-1/PD-L1/L2 expression. Clin Cancer Res. 18:1925–1935. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Goldstraw P, Crowley J, Chansky K, Giroux
DJ, Groome PA, Rami-Porta R, Postmus PE, Rusch V and Sobin L;
International Association for the Study of Lung Cancer
International Staging Committee; Participating Institutions. The
IASLC Lung Cancer Staging Project: Proposals for the revision of
the TNM stage groupings in the forthcoming (seventh) edition of the
TNM Classification of malignant tumours. J Thorac Oncol. 2:706–714.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Roncador G, Brown PJ, Maestre L, Hue S,
Martínez-Torrecuadrada JL, Ling KL, Pratap S, Toms C, Fox BC,
Cerundolo V, et al: Analysis of FOXP3 protein expression in human
CD4+CD25+ regulatory T cells at the
single-cell level. Eur J Immunol. 35:1681–1691. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Wainwright DA, Sengupta S, Han Y and
Lesniak MS: Thymus-derived rather than tumor-induced regulatory T
cells predominate in brain tumors. Neuro Oncol. 13:1308–1323. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Polansky JK, Schreiber L, Thelemann C,
Ludwig L, Krüger M, Baumgrass R, Cording S, Floess S, Hamann A and
Huehn J: Methylation matters: Binding of Ets-1 to the demethylated
Foxp3 gene contributes to the stabilization of Foxp3 expression in
regulatory T cells. J Mol Med Berl. 88:1029–1040. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Kim YC, Bhairavabhotla R, Yoon J, Golding
A, Thornton AM, Tran DQ and Shevach EM: Oligodeoxynucleotides
stabilize Helios-expressing Foxp3+ human T regulatory
cells during in vitro expansion. Blood. 119:2810–2818. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Rossignol M, Pouysségur J and Klagsbrun M:
Characterization of the neuropilin-1 promoter; gene expression is
mediated by the transcription factor Sp1. J Cell Biochem.
88:744–757. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Yadav M, Louvet C, Davini D, Gardner JM,
Martinez-Llordella M, Bailey-Bucktrout S, Anthony BA, Sverdrup FM,
Head R, Kuster DJ, et al: Neuropilin-1 distinguishes natural and
inducible regulatory T cells among regulatory T cell subsets in
vivo. J Exp Med. 209:1713–1722. s1711–1719. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Weiss JM, Bilate AM, Gobert M, Ding Y,
Curotto de Lafaille MA, Parkhurst CN, Xiong H, Dolpady J, Frey AB,
Ruocco MG, et al: Neuropilin 1 is expressed on thymus-derived
natural regulatory T cells, but not mucosa-generated induced Foxp3
T reg cells. J Exp Med. 209:1723–1742. s17212012. View Article : Google Scholar :
|
|
38
|
Lin X, Chen M, Liu Y, Guo Z, He X, Brand D
and Zheng SG: Advances in distinguishing natural from induced
Foxp3+ regulatory T cells. Int J Clin Exp Pathol.
6:116–123. 2013.
|
|
39
|
Onizuka S, Tawara I, Shimizu J, Sakaguchi
S, Fujita T and Nakayama E: Tumor rejection by in vivo
administration of anti-CD25 (interleukin-2 receptor alpha)
monoclonal antibody. Cancer Res. 59:3128–3133. 1999.PubMed/NCBI
|
|
40
|
Gallimore A and Sakaguchi S: Regulation of
tumour immunity by CD25+ T cells. Immunology. 107:5–9.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Morse MA, Hobeika AC, Osada T, Serra D,
Niedzwiecki D, Lyerly HK and Clay TM: Depletion of human regulatory
T cells specifically enhances antigen-specific immune responses to
cancer vaccines. Blood. 112:610–618. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Sutmuller RP, van Duivenvoorde LM, van
Elsas A, Schumacher TN, Wildenberg ME, Allison JP, Toes RE,
Offringa R and Melief CJ: Synergism of cytotoxic T
lymphocyte-associated antigen 4 blockade and depletion of
CD25+ regulatory T cells in antitumor therapy reveals
alternative pathways for suppression of autoreactive cytotoxic T
lymphocyte responses. J Exp Med. 194:823–832. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Ko K, Yamazaki S, Nakamura K, Nishioka T,
Hirota K, Yamaguchi T, Shimizu J, Nomura T, Chiba T and Sakaguchi
S: Treatment of advanced tumors with agonistic anti-GITR mAb and
its effects on tumor-infiltrating
Foxp3+CD25+CD4+ regulatory T
cells. J Exp Med. 202:885–891. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
GlaxoSmithKline plc. Update on phase III
clinical trial of investigational MAGE-A3 antigen-specific cancer
immunotherapeutic in non-small cell lung cancer [Internet].
02–April. 2014, [cited 2015 March 24] Available from http://www.gsk.com/en-gb/media/press-releases/2014/update-on-phase-iii-clinical-trial-of-investigational-mage-a3-antigen-specific-cancer-immunother-apeutic-in-non-small-cell-lung-cancer/.
|
|
45
|
Suzuki H, Fukuhara M, Yamaura T, Mutoh S,
Okabe N, Yaginuma H, Hasegawa T, Yonechi A, Osugi J, Hoshino M, et
al: Multiple therapeutic peptide vaccines consisting of combined
novel cancer testis antigens and anti-angiogenic peptides for
patients with non-small cell lung cancer. J Transl Med. 11:972013.
View Article : Google Scholar : PubMed/NCBI
|