Introduction
Pancreatic ductal adenocarcinoma (PDAC) is the
fourth leading cause of cancer-associated mortality and has a
5-year survival rate of 5%. It has been predicted to become the
second leading cause of cancer-associated mortality within a decade
(1). Surgery remains the most
effective treatment for PDAC; however, only 20% of patients are
suitable for radical resection at the time of diagnosis, and a
large number of cases that undergo curative surgery develop
recurrence at a median of 10–20 months following resection
(2). In addition, treatment of
patients with recurrent or metastatic PDAC is limited to palliative
chemotherapy. Therapeutic advances, including the use of FOLFIRINOX
and gemcitabine plus nab-paclitaxel regimens, have resulted in a
modest improvement in outcome (3,4).
It is well known that cancer is a complex disease
caused by the accumulation of somatic mutations acquired by the
genome of cells. With the advent of next-generation sequencing
technologies, it is possible to detect a large number of recurring
mutations and many highly mutated genes with high resolution. In
particular, whole transcriptome massively parallel sequencing
(RNA-seq) and whole exome sequencing (WES) are powerful tools used
to detect mutations underlying carcinogenesis and to detect somatic
events, such as nucleotide substitution mutations and gene
translocations, with high resolution by sequencing the expressed
gene (cell transcriptomes) and the protein coding regions of the
genome (cell exome) (5). The
genomic characterization of PDAC via the molecular analysis of all
somatic alterations has generated much information, highlighting a
complex mutational landscape. With the exception of well-known KRAS
proto-oncogene, GTPase (KRAS), tumour protein p53 (TP53),
cyclin-dependent kinase inhibitor 2A (CDKN2A) and SMAD family
member 4 (SMAD4) alterations, which have a frequency of 71, 49, 22
and 20%, respectively, as reported in the literature, a large
number of genomic rearrangements with mutational frequency <2%
were detected (6).
The majority of single gene mutations in pancreatic
cancer can be grouped in common cellular pathways. Jones et
al identified 69 mutated gene sets in most of the 24 samples
analysed, of which 31 could be grouped into 12 core signalling
pathways. These pathways included KRAS signalling, transforming
growth factor (TGF)-β pathway, DNA damage control, apoptosis and
regulation of G1/S cell cycle transition, and other pathways, such
as Hedgehog signalling, the homophilic cell adhesion pathway,
integrin signalling, TGF-β signalling, Wnt/Notch signalling and
regulation of the invasion pathway (7).
However, at present, no prognostic or therapeutic
molecular markers are available for the better selection of
patients for surgery and therapeutic strategies.
In order to better understand PDAC biology, the
present study analysed 30 PDAC samples using either whole
transcriptome (9 samples) or exome sequencing (21 samples). A total
of 43 recurrently altered genes were identified, which are involved
in numerous pathways, including chromatin remodelling and DNA
damage repair. Subsequently, an analysis of mutational events in
known PDAC mutated genes was conducted on early stage samples (50%
of specimens), and a high number of mutations was revealed to be
significantly associated with a poor prognosis. These findings
indicated that a low level of gene mutations may predict a
favourable prognosis following surgery in patients with early stage
PDAC.
Materials and methods
Sample collection and sequencing
analysis
The present study was conducted according to the
principles expressed in the Declaration of Helsinki, and written
informed consent was obtained from all participants. The study was
approved by the Independent Ethics Committee of Sant’
Orsola-Malpighi Hospital (Bologna, Italy). A total of 30 PDAC
samples were obtained by ultrasound-guided biopsy or surgery for
either RNA or DNA extraction between January 2011 and December
2015. The tissues were collected in cryogenic tubes and were stored
at −20°C in RNAlater solution and DNAlater solution (both from
Ambion; Thermo Fisher Scientific, Inc., Waltham, MA, USA),
respectively. Nucleic acid extraction was performed using the
AllPrep RNA/DNA kit for tumour biopsies and the QiaAmp DNA Mini kit
(both from Qiagen, Inc., Valencia, CA, USA) for peripheral blood
samples of the same patients with PDAC; the results were matched
with this normal DNA to identify somatic events.
Out of the 30 samples, 9 were analysed by RNA-seq
and 21 were analysed by WES, performed at 75X2 or 100X2 bp on a
HiScanSQ Illumina platform (Illumina, Inc., San Diego, CA, USA).
Analysis was performed on a local CentOS5 Linux server by applying
a customised bioinformatics pipeline. Following the conversion of
data from binary base call (BCL) to FASTQ format (Illumina
Bcl2Fastq function), short reads were processed to clean up
sequencing adapters, and to filter or trim the reads for sequence
quality (minimum Phred quality, 10; minimum length of trimmed
sequence, 30), both of these steps were performed using
AdapterRemoval (8). The cleaned
reads were mapped to the human reference genome hg38 using
Burrows-Whealer Aligner in paired-end mode for WES data and with
the Tophat/Bowtie pipeline for RNA-seq data (9). In order to remove the optical and
polymerase chain reaction duplicates, Samtools was adopted, and
GATK was used to optimize the alignment around insertions and
deletions (InDels) (10,11). Single nucleotide variants (SNVs)
and InDels were detected using GATK (HaplotypeCaller mode), Mutect
and SNVmix2, applying manually curated quality filters (12,13).
The whole set of detected variants was refined
adopting different filtering thresholds for each sample. These
criteria were based on KRAS variant detection, which depends on the
abundance of tumour cells within a sample. Evaluation of tumour
cells was based on the presence and relative enrichment of the KRAS
mutation; only samples with >10% tumour vs. normal allele were
included in the study. Minimum depth of coverage and minimum ratio
(proportion between the depth of coverage of the mutated allele and
the total depth of coverage) were established in the range of 15–20
and 0.05–0.1, respectively. Therefore, the confidence in selecting
genuine variants was increased.
The obtained variants were annotated with 1000
Genomes allele frequencies, dbSNP 149 rsIDs, Exac and EVS, using
Annovar and Oncotator, in order to discard polymorphisms, and to
identify novel or almost rare variants (population frequency
<0.01) (14,15). Finally, to determine the pathogenic
significance of the emerging variants, previous knowledge (Catalog
of Somatic Mutations in Cancer) and bioinformatics
mutation-prediction tools (PolyPhen2, Proven and SIFT) were used
(16–18). The resulting list of variants was
analysed to distinguish between somatic and germline mutations,
according to the presence of alternative events compared with in
the normal counterpart (peripheral blood samples) using the
Samtools mpileup function. The following criteria were used: Total
depth >5 and depth of alternative base=0 (depth=1 or 2 were
admitted if the total depth was ≥15 or 30, respectively) for
inclusion of the variant in the ‘somatic’ set, otherwise the events
were marked as ‘germline’; however, if total coverage of the normal
counterpart was considered insufficiently informative (total depth
<5) the variant was classified as ‘undetermined’. The SNV and
InDels were automatically annotated with regards to the common PDAC
pathways using the Reactome database (https://reactome.org/PathwayBrowser/#TOOL=AT).
With regards to WES data, copy number alterations
were identified using two software programs, Control-FREEC and
ADTEX (19,20). These tools compute and normalise
the copy number and β-allele frequency profiles of segments, thus
providing copy number alterations. In the present study, WES data
were analysed with the matched normal sample used as a control. The
catalogue of human genomic structural variation (Database of
Genomic Variants; http://dgv.tcag.ca/dgv/app/home) was used to remove
physiological alterations.
Mutational load
The present study restricted the analysis to the
early stage subgroup of patients (15 samples) and evaluated the
mutational load. The threshold used for overall survival (OS) was
derived from the current scientific literature, in order to
stratify the patients into long survival (>25 months) and short
survival (<25 months) groups; three early stage cases with an OS
value very close to 25 months were excluded, and only the extreme
cases were analysed (2).
A list of 365 genes previously reported in the
literature was considered somatically mutated in PDAC according to
the Catalogue of Somatic Mutations in Cancer (http://cancer.sanger.ac.uk/cosmic/browse/tissue?wgs=off&sn=pancreas&ss=NS&hn=carcinoma&sh=ductal_carcinoma&in=t&src=tissue&all_data=n).
Matching this set with the genes carrying SNVs or InDels in the
samples of the present study, the mutational load of each patient
was estimated. Using the software suite SPSS version 23 (IBM
Corporation, Armonk, NY, USA), one-way analysis of variance was
used to highlight the statistical difference in terms of OS between
the groups with high mutational load and the low mutational load,
using 25 months as the OS cut-off (Fig. 4). Finally the median OS for the two
groups of subjects was calculated according to a survival analysis
and Kaplan-Meier estimation.
Results
Sequencing analysis data
A total of 30 PDAC samples were analysed by either
whole transcriptome or exome sequencing. The patient
characteristics are summarised in Table I. After matching with normal DNA to
identify somatic events, an average of 71 coding non-synonymous
novel disease-related SNVs (ranging from 8 of the case with the
lowest number of mutation events to 304 of the one with the highest
number) and three InDels (ranging from 0 of the case with the
lowest number of mutation events to 6 of the one with the highest
number) were identified. In addition, intra- or inter-chromosomal
rearrangements were detected in the set of samples analysed by
RNA-seq. However, no recurrent fusion transcripts were
detected.
 | Table IPatient characteristics. |
Table I
Patient characteristics.
| Variable | Value |
|---|
| Age (years) | |
| Median | 74 |
| Range | 33-83 |
| Sex (%) | |
| Male | 43 |
| Female | 57 |
| Site of specimen
(%) | |
| Pancreatic
tumour | 93 |
| Hepatic
metastasis | 7 |
| Site of tumour
(%) | |
| Head | 63 |
| Body/tail | 37 |
| Stage (%)a | |
| I+II | 60 |
| III-LA | 13 |
| IV | 27 |
| Surgery (%) | |
| Yes | 60 |
| No | 40 |
A total of 43 recurrently mutated genes were
identified, and the high frequency of KRAS, TP53, CDKN2A and SMAD4
mutations was confirmed in PDAC; these genes were altered in 100,
74, 16 and 10% of samples, respectively. As expected, KRAS
exhibited the highest prevalence of somatic mutations; the
mutations affected the known hotspot at codon 12 (G12D, G12V, G12R
and G12C in 16, 8, 4 and 2 patients, respectively). The prevalence
of the KRAS mutation is however biased by the experimental design,
since samples were included in the present study only if a mutation
in any KRAS gene was detected, estimating the percentage of tumour
cells in the sample via quantification of the KRAS mutation in the
DNA. Somatic mutations in other genes were much less recurrent, as
summarised in Fig. 1.
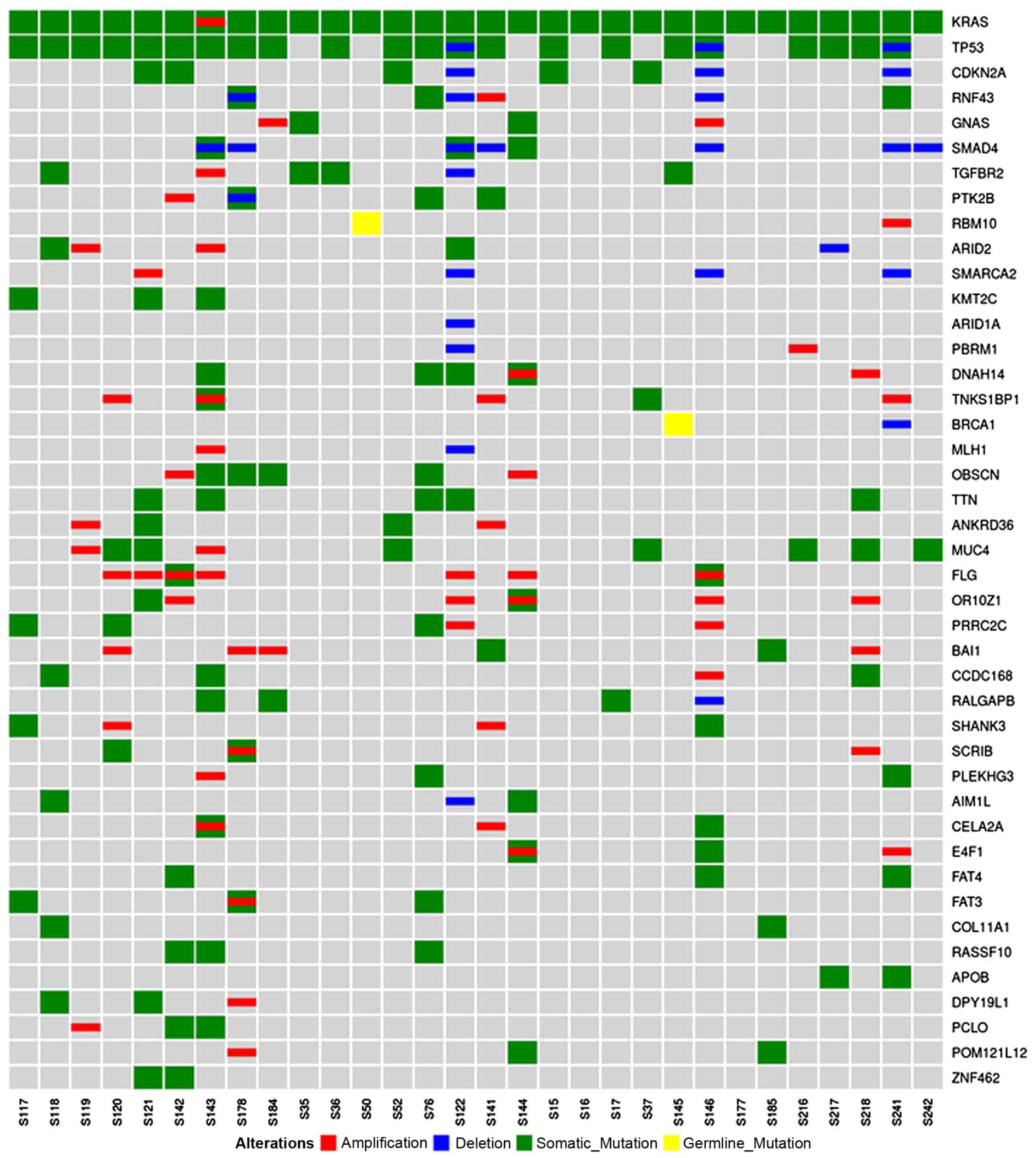 | Figure 1Alterations in the most recurrently
mutated genes. Genes are presented along the right-hand side, and
each sample is presented along the bottom. Red, amplifications;
blue, deletions; green, somatic mutations; yellow, germline
mutations. The results confirmed the high frequency of KRAS, TP53,
CDKN2A and SMAD4 mutations in pancreatic ductal adenocarcinoma;
these genes were altered in 100, 74, 16 and 10% of samples,
respectively. CDKN2A, cyclin-dependent kinase inhibitor 2A; KRAS,
KRAS proto-oncogene, GTPase; SMAD4, SMAD family member 4; TP53,
tumour protein p53. |
Pathway analysis demonstrated that the genes with a
high frequency of aberrations were clustered into the following
specific pathways: KRAS signalling, TGF-β signalling, chromatin
remodelling, Wnt signalling, DNA damage repair, cell cycle and RNA
processing (Fig. 2).
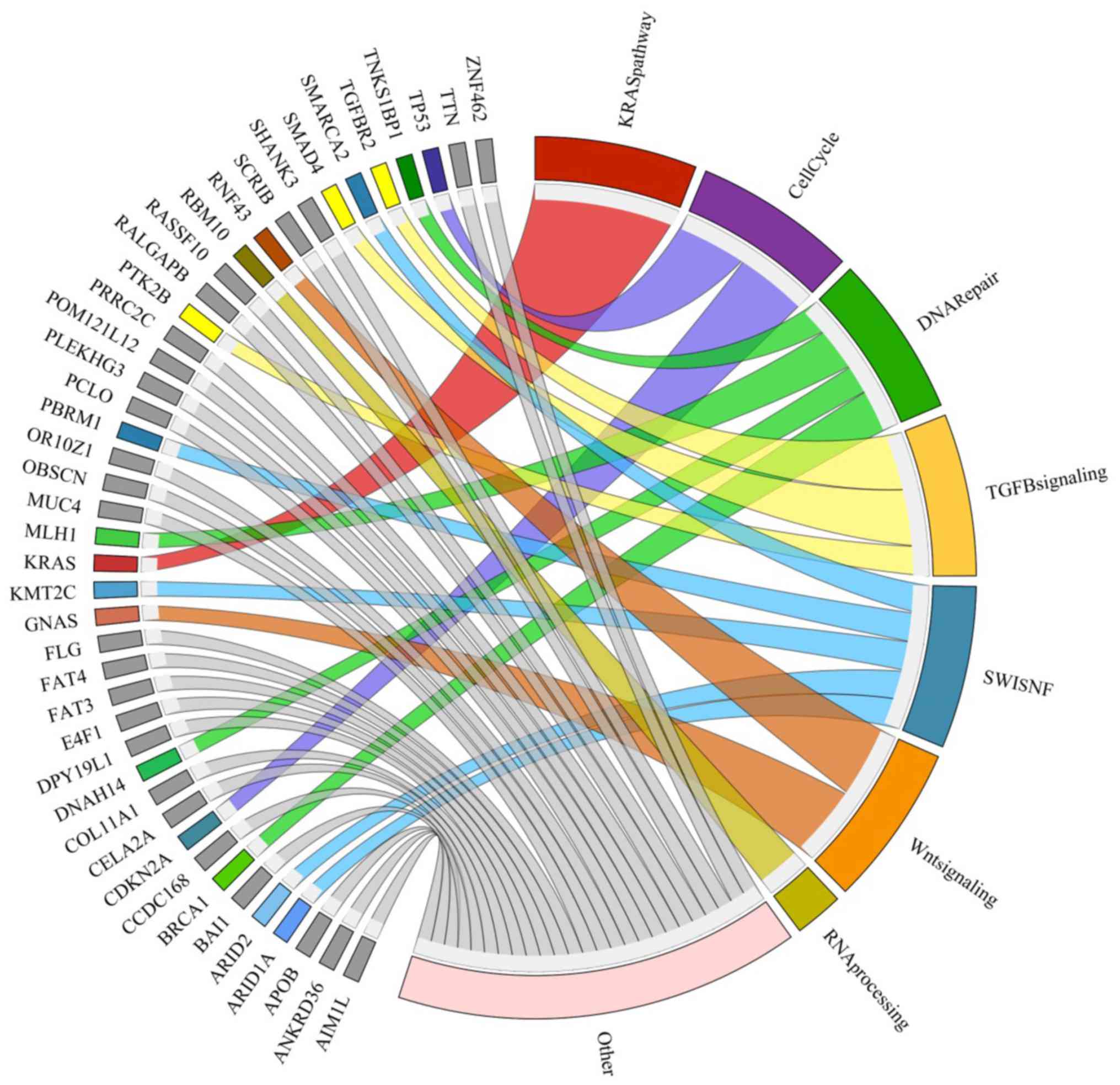 | Figure 2Genes with a high frequency of
aberrations, as presented on the left-hand side of the image, were
clustered into specific pathways, as presented on the right-hand
side. Connections are colour-coded. The most recurrently detected
pathways included KRAS signalling, TGF-β signalling, chromatin
remodelling, Wnt signalling, DNA damage repair, cell cycle and RNA
processing. KRAS, KRAS proto-oncogene, GTPase; TGF-β, transforming
growth factor-β. |
Mutational load data
In order to better understand the somatic driving
events in PDAC carcinogenesis, analysis was restricted to the early
stage subgroup of patients (50% of the samples), including only
patients with primary, operable and untreated PDAC, which underwent
pancreatectomy with curative intent. Since the RNA-seq data may
lead to biased results in the mutational load evaluation, the
present study normalised the number of mutations for the coding
sequences covered at least 10X using Samtools; therefore, it was
considered that RNA-seq data covered the transcriptome dimension.
In addition, of the 9 cases analysed through RNA-seq, only 5 cases
were retained for analysis of the mutational load, and these were
almost equally distributed in the two subgroups. Cohort
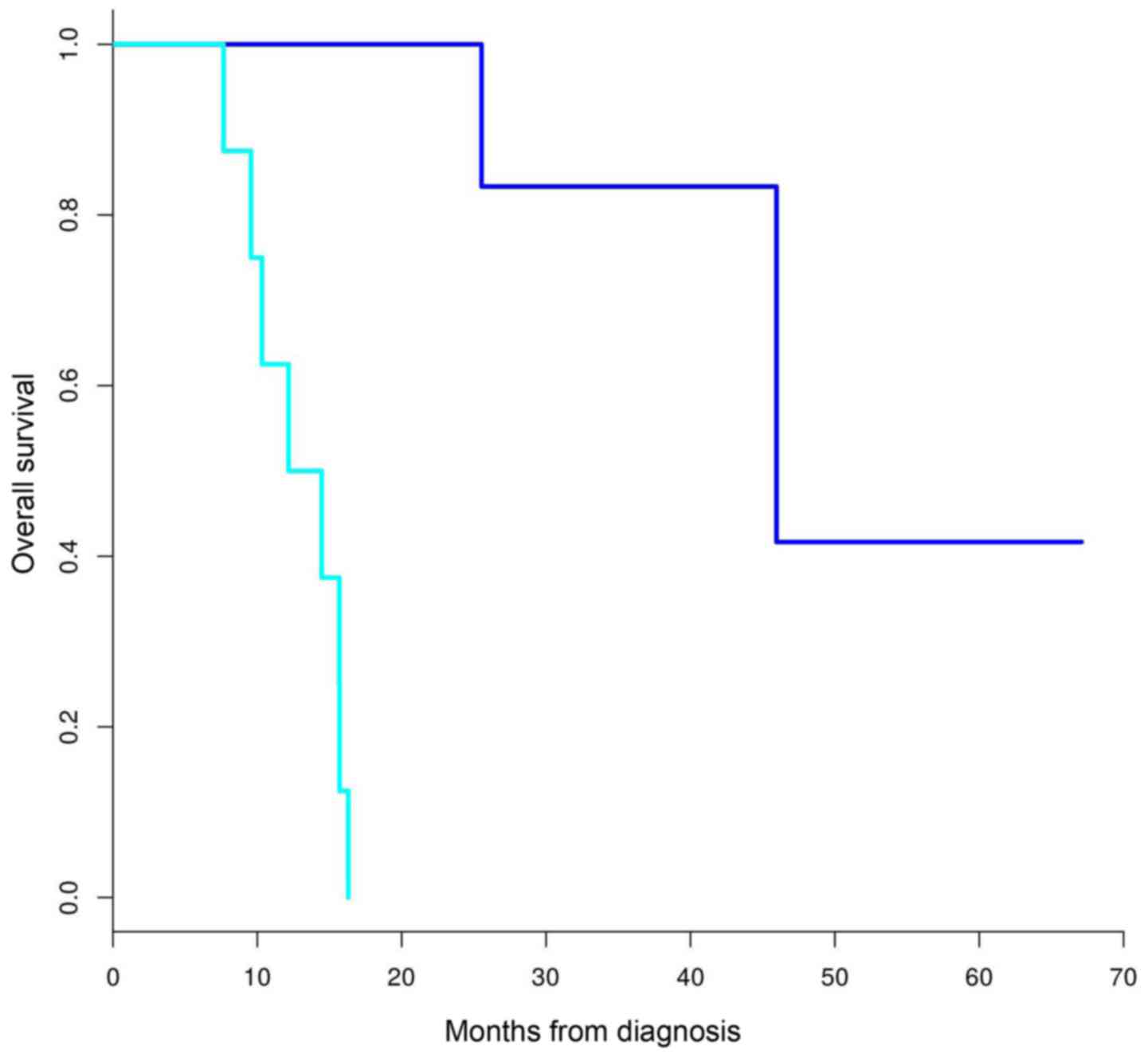
characteristics are presented in Table II. The median OS of the two
groups, as estimated using a Kaplan-Meier analysis, were 46 and 13
months for patients classified into the long and short survival
groups, respectively (Fig. 3).
| Table IIEarly-stage patient
characteristics. |
Table II
Early-stage patient
characteristics.
| Variable | Value |
|---|
| Age (years) | |
| Median | 67.6 |
| Range | 33-83 |
| Sex (%) | |
| Male | 53 |
| Female | 47 |
| Outcome | |
| Death (%) | 67 |
| Survival (%) | 33 |
| Median OS
(months) | 23.5 |
| Range OS
(months) | 7.66-67.09 |
| T stage (%)a | |
| T1 (1a, 1b,
1c) | 0 |
| T2 | 7 |
| T3 | 93 |
| N stage (%)a | |
| N0 | 33 |
| N1 | 20 |
| N2 | 47 |
| Grading (%) | |
| G1 | 20 |
| G2 | 60 |
| G3 | 20 |
| Margins (%) | |
| Clear | 47 |
| Involved | 53 |
| Tumour location
(%) | |
| Head | 67 |
| Body/tail | 33 |
| Type of surgery
(%) | |
| Total
pancreatectomy | 47 |
|
Pancreaticoduodenectomy | 27 |
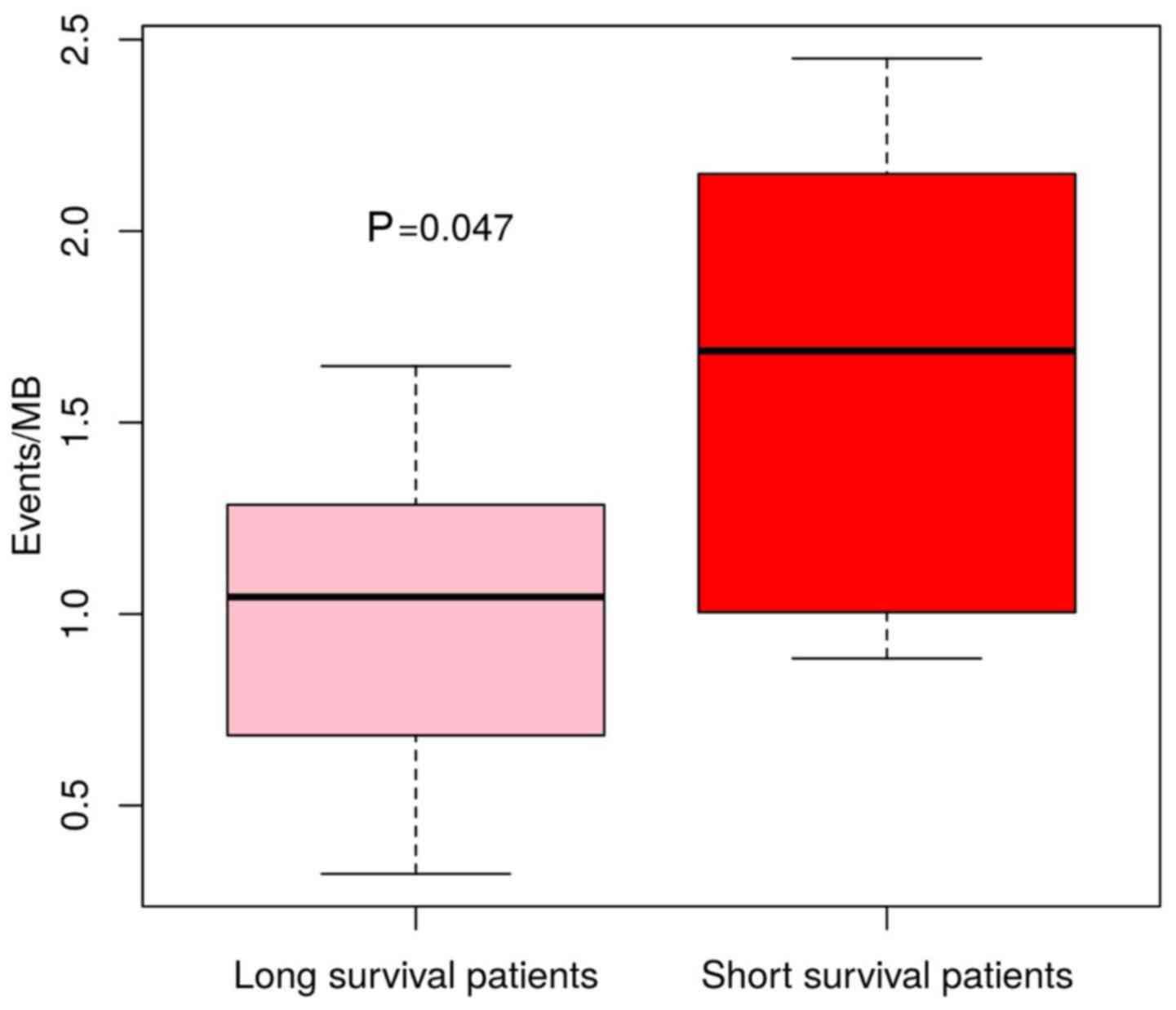
The mutational load of each patient was evaluated
and was matched to a list of 365 genes previously described as
mutated in PDAC. Among the genes carrying SNVs or InDels in the
present study samples, an average of 33 events were detected. Based
on 25 months as the cut-off value, patients were divided into two
subgroups; the subgroup with the better OS (>25 months)
harboured an average of 24 events, whereas the subgroup with the
worse OS (<25 months) presented an average of 40 mutations
(P=0.047) (Fig. 4)
The most recurrent genes altered by point mutations,
deletions or amplifications in the subgroup were KRAS (100%), TP53
(60%), mucin 4, cell surface associated (MUC4), olfactory receptor
family 10 subfamily Z member 1 (33%), CDKN2A, GNAS complex locus,
SMAD4, TGF-β receptor 2 (TGFBR2), filaggrin (27%), SWI/SNF related,
matrix associated, actin dependent regulator of chromatin,
subfamily a, member 2, dynein axonemal heavy chain 14, titin,
adhesion G protein-coupled receptor B1, Ral GTPase activating
protein non-catalytic β subunit (20%), ring finger protein 43
(RNF43), polybromo 1, obscurin, cytoskeletal calmodulin and
titin-interacting RhoGEF, proline-rich coiled-coil 2C, coiled-coil
domain-containing 168, crystalline βγ domain-containing 2, E4F
transcription factor 1 and POM121-like protein 12 (POM12L12) (13%),
as shown in Fig. 5. However, no
specific genes or pathways were correlated with OS.
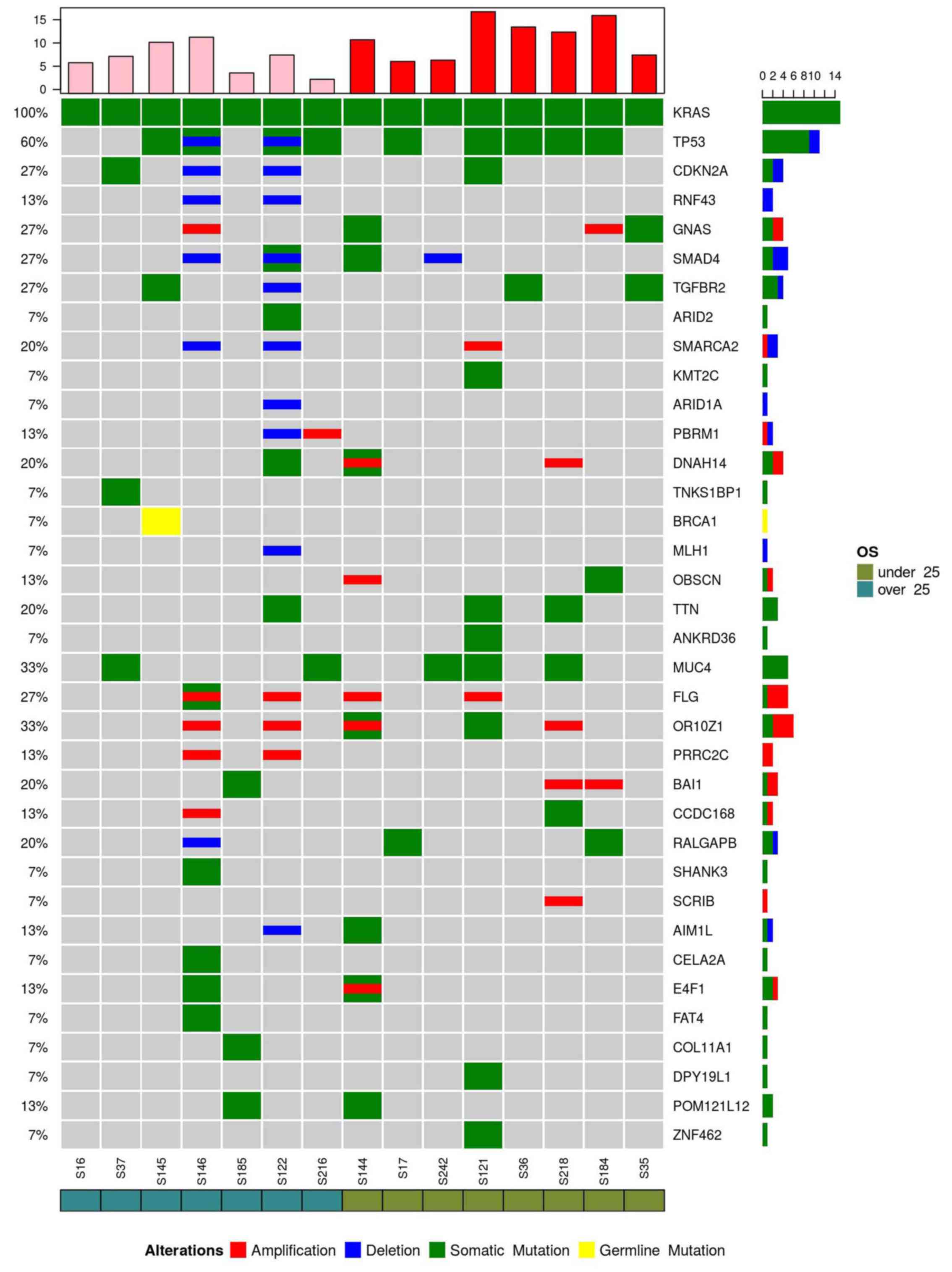 | Figure 5Recurrent genes altered by point
mutations (green), deletions (blue) or amplifications (red) in the
early stage samples are presented. A high frequency of mutations
were detected in the following genes: KRAS (100%), TP53 (60%),
MUC4, OR10Z1 (33%), CDKN2A, GNAS, SMAD4, TGFBR2, FLG (27%),
SMARCA2, DNAH14, TTN, BAI1, RALGAPB (20%), RNF43, PBRM1, OBSCN,
PRRC2C, CCDC168, AIM1L, E4F1 and POM121L12 (13%). AIM1L,
crystalline βγ domain-containing 2; BAI1, adhesion G
protein-coupled receptor B1; CCDC168, coiled-coil domain-containing
168; CDKN2A, cyclin-dependent kinase inhibitor 2A; DNAH14, dynein
axonemal heavy chain 14; E4F1, E4F transcription factor 1; FLG,
filaggrin; GNAS, GNAS complex locus; KRAS, KRAS proto-oncogene,
GTPase; MUC4, mucin 4, cell surface associated; OBSCN, obscurin,
cytoskeletal calmodulin and titin-interacting RhoGEF; OR10Z1,
olfactory receptor family 10 subfamily Z member 1; PBRM1, polybromo
1; POM121L12, POM121-like protein 12; PRRC2C, proline-rich
coiled-coil 2C; RALGAPB, Ral GTPase activating protein
non-catalytic β subunit; RNF43, ring finger protein 43; SMAD4, SMAD
family member 4; SMARCA2, SWI/SNF related, matrix associated, actin
dependent regulator of chromatin, subfamily a, member 2; TGFBR2,
transforming growth factor-β receptor 2; TP53, tumour protein p53;
TTN, titin. |
Discussion
Based on chromosome structural variation and gene
expression profiles, recent studies have classified PDAC into
various subtypes with prognostic and biological relevance. In
particular, Bailey et al (22) correlated four PDAC molecular
subtypes with specific histopathological characteristics, whereas
Waddell et al (23)
identified a subtype of PDAC that was unstable with a high
prevalence of inactivation of DNA maintenance genes, and was
associated with therapeutic responsiveness for platinum-based
chemotherapy and poly (ADP-ribose) polymerase inhibitors (21–23).
However, despite improvements regarding the
biological understanding of PDAC, there is currently no available
molecular classification able to translate the histopathological
classification into clinical practice. Molecular heterogeneity, due
to high PDAC genetic instability, hinders the identification of
prognostic or predictive biomarkers (24,25).
The present data confirmed this heterogeneous
landscape, as characterised by a high number of mutations occurring
with low frequency, with the exception of well-known mutations in
KRAS, TP53, CDKN2A and SMAD4.
As expected, KRAS mutations were the most prevalent
events detected in the present study. Numerous hotspot mutations
were identified (G12D, G12V, G12R and G12C) in KRAS, which is a key
oncogene during the onset of pancreatic cancer (26). A recent study demonstrated how
numerous subclonal KRAS mutations coexist within tumour cells,
suggesting a convergent evolution of various clones of advanced
cancer with independent KRAS mutations (6). In the present study, the majority of
single gene mutations detected in the samples can be grouped into
common cellular pathways, including KRAS signalling, TGF-β
signalling, chromatin remodelling, Wnt signalling, DNA damage
repair, cell cycle and RNA processing; these findings are
concordant with those of previous studies (7,27).
The 5-year OS of patients with surgically resected
PDAC is 20–25%, and the majority of patients develop recurrence at
a median of 10–20 months following resection (2).
By evaluating mutational load in the early stage
subgroup the present study demonstrated that samples harbouring
more genetic events were associated with worse OS, thus stressing
the urgent requirement for more molecular features to support the
clinical-pathological classification of PDAC. It may be
hypothesized that tumours with high molecular events have a more
aggressive phenotype; therefore, detection of these patients during
the early diagnostic phase may identify patients that benefit from
neoadjuvant treatment prior to surgery. However, no specific genes
or pathways were revealed to be correlated with OS in this subgroup
of patients. SMAD4 gene inactivation, which has previously been
reported to be associated with recurrence and a poorer prognosis in
patients following resection, was detected in 27% of the samples,
but was not correlated with OS correlation (28,29).
In the present study, a high prevalence of MUC4
mutation was detected in samples from patients following resection
(33%), thus confirming its importance in PDAC carcinogenesis. MUC4
is a type I membrane-bound mucin that promotes proliferation,
motility, invasiveness, epithelial-mesenchymal transition,
chemoresistance and tumour growth, the overexpression of which is
considered an early event in pancreatic carcinogenesis, and is
detected in the preneoplastic stage. Urey et al (30) investigated MUC4 expression by
immunohistochemistry and indicated that low MUC4 expression is
associated with a survival benefit in patients with resectable
pancreatic cancer receiving adjuvant gemcitabine (30,31).
However, no differences in MUC4 mutations were detected between
samples in the long and short survival groups in the present
study.
RNF43 deletion was detected in only two cases with
intraductal papillary mucinous neoplasm (IPMN)-associated PDAC in
the long survival group. Inactivating mutations of the RNF43 gene,
which encodes a protein with intrinsic U3 ubiquitin ligase
activity, have been reported in IPMN of the pancreas. According to
a previous study (32), IPMN has a
better outcome than conventional PDAC, and the present detection of
RNF43 deletions in the long survival group only supports this
hypothesis. Recent evidence has suggested that mutational
inactivation of RNF43 confers Wnt dependency, thus indicating that
the presence of RNF43 mutations may be used as a predictive
biomarker for the use of Wnt inhibitors (33).
In conclusion, the present study reaffirmed the
presence of a heterogeneous genetic landscape in PDAC, and provided
evidence to suggest that a more complex genome is correlated with a
more aggressive phenotype and poor prognosis. Further work is
required to identify molecular biomarkers that better characterise
pancreatic cancer, particularly in the early stage.
Acknowledgments
Not applicable.
Funding
The present study was supported by the Programma di
Ricerca Regione-Università, Regione Emilia Romagna, bando Giovani
Ricercatori ʻby Program Liberatiʼ 2013 to SV (grant no.
PRUA1GR-2013-00000038).
Availability of data and material
The datasets used and/or analysed during the current
study are available from the corresponding author on reasonable
request.
Authors’ contributions
EG, SD, SV, EF, GB and MDM designed and supervised
the research. CR, RC, FM, EG, CS, DS, FF, DF, FC and ADE provided
the samples. SV, SD and EG collected the specimens. SD, VI, GT and
AA performed sequencing, bioinformatics and statistical analysis.
EG, EF and MDM wrote the manuscript. All authors have read and
approved the final manuscript.
Ethics approval and consent to
participate
The present study was conducted according to the
principles expressed in the Declaration of Helsinki and written
informed consent was obtained from all participants. The study was
approved by Independent Ethics Committee of Sant’ Orsola-Malpighi
Hospital (Bologna, Italy).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Vogelzang NJ, Benowitz SI, Adams S,
Aghajanian C, Chang SM, Dreyer ZE, Janne PA, Ko AH, Masters GA,
Odenike O, et al: Clinical cancer advances 2011: Annual Report on
Progress Against Cancer from the American Society of Clinical
Oncology. J Clin Oncol. 30:88–109. 2012. View Article : Google Scholar
|
|
2
|
Katz MH, Wang H, Fleming JB, Sun CC, Hwang
RF, Wolff RA, Varadhachary G, Abbruzzese JL, Crane CH, Krishnan S,
et al: Long-term survival after multidisciplinary management of
resected pancreatic adenocarcinoma. Ann Surg Oncol. 16:836–847.
2009. View Article : Google Scholar
|
|
3
|
Conroy T, Desseigne F, Ychou M, Bouché O,
Guimbaud R, Bécouarn Y, Adenis A, Raoul JL, Gourgou-Bourgade S, de
la Fouchardière C, et al Groupe Tumeurs Digestives of Unicancer;
PRODIGE Intergroup: FOLFIRINOX versus gemcitabine for metastatic
pancreatic cancer. N Engl J Med. 364:1817–1825. 2011. View Article : Google Scholar
|
|
4
|
Von Hoff DD, Ervin T, Arena FP, Chiorean
EG, Infante J, Moore M, Seay T, Tjulandin SA, Ma WW, Saleh MN, et
al: Increased survival in pancreatic cancer with nab-paclitaxel
plus gemcitabine. N Engl J Med. 369:1691–1703. 2013. View Article : Google Scholar
|
|
5
|
Meyerson M, Gabriel S and Getz G: Advances
in understanding cancer genomes through second-generation
sequencing. Nat Rev Genet. 11:685–696. 2010. View Article : Google Scholar
|
|
6
|
Cancer Genome Atlas Research Network:
Electronic address: andrew_aguirre@dfci.harvard.eduCancer Genome
Atlas Research Network: Integrated Genomic Characterization of
Pancreatic Ductal Adenocarcinoma. Cancer Cell. 32:185–203.e13.
2017. View Article : Google Scholar
|
|
7
|
Jones S, Zhang X, Parsons DW, Lin JC,
Leary RJ, Angenendt P, Mankoo P, Carter H, Kamiyama H, Jimeno A, et
al: Core signaling pathways in human pancreatic cancers revealed by
global genomic analyses. Science. 321:1801–1806. 2008. View Article : Google Scholar
|
|
8
|
Schubert M, Lindgreen S and Orlando L:
AdapterRemoval v2: Rapid adapter trimming, identification, and read
merging. BMC Res Notes. 9:882016. View Article : Google Scholar
|
|
9
|
Lang B, Trapnell C, Pop M and Salzberg L:
Ultrafast and memory-efficient alignment of short DNA sequences to
the human genome. Genome Biol. 10:R252009. View Article : Google Scholar
|
|
10
|
Li H, Handsaker B, Wysoker A, Fennell T,
Ruan J, Homer N, et al: 1000 Genome roject Data Processing
Subgroup. The SequenceAlignment/Map format and SAMtools.
Bioinformatics. 25:2078–2079. 2009. View Article : Google Scholar
|
|
11
|
McKenna A, Hanna M, Banks E, Sivachenko A,
Cibulskis K, Kernytsky A, Garimella K, Altshuler D, Gabriel S, Daly
M, et al: The Genome Analysis Toolkit: A MapReduce framework for
analyzing next-generation DNA sequencing data. Genome Res.
20:1297–1303. 2010. View Article : Google Scholar
|
|
12
|
Cibulskis K, Lawrence MS, Carter SL,
Sivachenko A, Jaffe D, Sougnez C, Gabriel S, Meyerson M, Lander ES
and Getz G: Sensitive detection of somatic point mutations in
impure and heterogeneous cancer samples. Nat Biotechnol.
31:213–219. 2013. View
Article : Google Scholar
|
|
13
|
Goya R, Sun MGF, Morin RD, Leung G, Ha G,
Wiegand KC, Senz J, Crisan A, Marra MA, Hirst M, et al: SNVMix:
Predicting single nucleotide variants from next-generation
sequencing of tumors. Bioinformatics. 26:730–736. 2010. View Article : Google Scholar
|
|
14
|
Wang K, Li M and Hakonarson H: ANNOVAR:
Functional annotation of genetic variants from high-throughput
sequencing data. Nucleic Acids Res. 38:e1642010. View Article : Google Scholar
|
|
15
|
Ramos AH, Lichtenstein L, Gupta M,
Lawrence MS, Pugh TJ, Saksena G, Meyerson M and Getz G: Oncotator:
Cancer variant annotation tool. Hum Mutat. 36:E2423–E2429. 2015.
View Article : Google Scholar
|
|
16
|
Adzhubei IA, Schmidt S, Peshkin L,
Ramensky VE, Gerasimova A, Bork P, et al: Catalog of Somatic
Mutations in Cancer and bioinformatics mutation-prediction tools
PolyPhen2. Nat Methods. 7:248–249. 2010. View Article : Google Scholar
|
|
17
|
Choi Y and Chan AP: PROVEAN web server: A
tool to predict the functional effect of amino acid substitutions
and indels. Bioinformatics. 31:2745–2747. 2015. View Article : Google Scholar
|
|
18
|
Ng PC and Henikoff S: SIFT: Predicting
amino acid changes that affect protein function. Nucleic Acids Res.
31:3812–3814. 2003. View Article : Google Scholar
|
|
19
|
Boeva V, Popova T, Bleakley K, Chiche P,
Cappo J, Schleiermacher G, Janoueix-Lerosey I, Delattre O and
Barillot E: Control-FREEC: A tool for assessing copy number and
allelic content using next-generation sequencing data.
Bioinformatics. 28:423–425. 2012. View Article : Google Scholar
|
|
20
|
Amarasinghe KC, Li J, Hunter SM, Ryland
GL, Cowin PA, Campbell IG and Halgamuge SK: Inferring copy number
and genotype in tumour exome data. BMC Genomics. 15:7322014.
View Article : Google Scholar
|
|
21
|
Collisson EA, Sadanandam A, Olson P, Gibb
WJ, Truitt M, Gu S, Cooc J, Weinkle J, Kim GE, Jakkula L, et al:
Subtypes of pancreatic ductal adenocarcinoma and their differing
responses to therapy. Nat Med. 17:500–503. 2011. View Article : Google Scholar
|
|
22
|
Bailey P, Chang DK, Nones K, Johns AL,
Patch AM, Gingras MC, Miller DK, Christ AN, Bruxner TJ, Quinn MC,
et al Australian Pancreatic Cancer Genome Initiative: Genomic
analyses identify molecular subtypes of pancreatic cancer. Nature.
531:47–52. 2016. View Article : Google Scholar
|
|
23
|
Waddell N, Pajic M, Patch AM, Chang DK,
Kassahn KS, Bailey P, Johns AL, Miller D, Nones K, Quek K, et al
Australian Pancreatic Cancer Genome Initiative: Whole genomes
redefine the mutational landscape of pancreatic cancer. Nature.
518:495–501. 2015. View Article : Google Scholar
|
|
24
|
Di Marco M, Astolfi A, Grassi E,
Vecchiarelli S, Macchini M, Indio V, Casadei R, Ricci C, D’Ambra M,
Taffurelli G, et al: Characterization of pancreatic ductal
adenocarcinoma using whole transcriptome sequencing and copy number
analysis by single-nucleotide polymorphism array. Mol Med Rep.
12:7479–7484. 2015. View Article : Google Scholar
|
|
25
|
Samuel N and Hudson TJ: The molecular and
cellular heterogeneity of pancreatic ductal adenocarcinoma. Nat Rev
Gastroenterol Hepatol. 9:77–87. 2011. View Article : Google Scholar
|
|
26
|
Collins MA and Pasca di Magliano M: Kras
as a key oncogene and therapeutic target in pancreatic cancer.
Front Physiol. 4:4072014. View Article : Google Scholar
|
|
27
|
Biankin AV, Waddell N, Kassahn KS, Gingras
MC, Muthuswamy LB, Johns AL, Miller DK, Wilson PJ, Patch AM, Wu J,
et al Australian Pancreatic Cancer Genome Initiative: Pancreatic
cancer genomes reveal aberrations in axon guidance pathway genes.
Nature. 491:399–405. 2012. View Article : Google Scholar
|
|
28
|
Blackford A, Serrano OK, Wolfgang CL,
Parmigiani G, Jones S, Zhang X, Parsons DW, Lin JC, Leary RJ,
Eshleman JR, et al: SMAD4 gene mutations are associated with poor
prognosis in pancreatic cancer. Clin Cancer Res. 15:4674–4679.
2009. View Article : Google Scholar
|
|
29
|
Shin SH, Kim HJ, Hwang DW, Lee JH, Song
KB, Jun E, Shim IK, Hong SM, Kim HJ, Park KM, et al: The DPC4/SMAD4
genetic status determines recurrence patterns and treatment
outcomes in resected pancreatic ductal adenocarcinoma: A
prospective cohort study. Oncotarget. 8:17945–17959. 2017.
View Article : Google Scholar
|
|
30
|
Urey C, Andersson B, Ansari D, Sasor A,
Said-Hilmersson K, Nilsson J and Andersson R: Low MUC4 expression
is associated with survival benefit in patients with resectable
pancreatic cancer receiving adjuvant gemcitabine. Scand J
Gastroenterol. 52:595–600. 2017. View Article : Google Scholar
|
|
31
|
Jonckheere N, Lahdaoui F and Van Seuningen
I: Targeting MUC4 in pancreatic cancer: miRNAs. Oncoscience.
2:799–800. 2015.
|
|
32
|
Koh YX, Chok AY, Zheng HL, Tan CS and Goh
BK: Systematic review and meta-analysis comparing the surgical
outcomes of invasive intraductal papillary mucinous neoplasms and
conventional pancreatic ductal adenocarcinoma. Ann Surg Oncol.
21:2782–2800. 2014. View Article : Google Scholar
|
|
33
|
Jiang X, Hao HX, Growney JD, Woolfenden S,
Bottiglio C, Ng N, Lu B, Hsieh MH, Bagdasarian L, Meyer R, et al:
Inactivating mutations of RNF43 confer Wnt dependency in pancreatic
ductal adenocarcinoma. Proc Natl Acad Sci USA. 110:12649–12654.
2013. View Article : Google Scholar
|
|
34
|
Brierley JD, Gospodarowicz MK and
Wittekind C: UICC TNM Classification of Malignant Tumours. 8th
edition. Wiley-Blackwell; Oxford: 2016
|