1. Introduction
Cerebrovascular diseases (CVDs) are common in cancer
patients, significantly aggravating their condition and prognosis
(1). Approximately 15% of cancer
patients have a concomitant CVD (2,3), and
the frequency of cerebral infarcts is similar to that of cerebral
hemorrhage (3). Stroke may either
follow the initial cancer diagnosis (4) or may precede the diagnosis of
cancerous disease (5). The
prevalence of an underlying cancerous disorder is higher in
patients with ischemic stroke than in the general population
(6,7) and cancer as a comorbidity is found in
1 out of 10 hospitalized patients with ischemic stroke in the
United States (8). Patients with
cancer have been shown to have higher in-hospital post-stroke
mortality rate (1,9,10)
and patients with ischemic stroke with an active cancer have also
been found to be of younger age, with more severe and more frequent
cryptogenic strokes (1).
The connection between stroke and cancer has for
long captivated the interest of the medical community. The first
large autopsy study was conducted in 1985 by Graus et al,
showing that the most frequent complication of the central nervous
system (CNS) in cancer patients, following metastasis, was cerebral
infarction and hemorrhage. In the same study, 14.6% of cancer
patients had pathological evidence of CVD and approximately half of
them were symptomatic (11). More
recent studies, such as that among Hodgkin lymphoma 5-year
survivors, demonstrated that 7% of patients developed an ischemic
stroke in the 17.5-year follow-up period (12).
The underlying causes for the development of a
stroke in cancer patients differ from those of non-cancer patients,
and are associated with the cancer itself, as well as with the type
of treatment (1,9,13-19).
In general, hypercoagulopathy or other coagulation disorders are
most often related to the development of ischemic/embolic stroke
(9,15,19).
Cardio-embolism, large-vessel atherosclerosis and small-vessel
occlusion have been reported as the major causes of ischemic
stroke, while non-bacterial thrombotic endocarditis (NBTE) is
rarely noted (9,17). In the pathogenesis and prognosis of
acute ischemic stroke, active cancer (recurrent malignant tumor,
metastases, or ongoing chemo-/radiotherapy) plays an active role
(1). In survivors of childhood
Hodgkin's disease, who are at an increased risk for stroke, mantle
radiation exposure is strongly associated with subsequent stroke
and the potential mechanisms may include carotid artery disease or
cardiac valvular disease (14).
Nevertheless, brain tumors always remain the main etiology for
stroke or other neurological pathologies, while cases where the
diagnostic misinterpretation of a brain tumor as a stroke or the
diagnostic misinterpretation of an underlying malignancy as an
incident of CVD, are not rare (13).
Stroke in cancer patients may be hemorrhagic or
ischemic (16,20), while embolisms have been reported
to be the most common cause of stroke (9). In a wide, population-based Swedish
study, the risk [expressed as standardized incidence ratio (SIR)]
of hemorrhagic and ischemic stroke in the first 6 months following
cancer diagnosis was 2.2 and 1.6, respectively. While the overall
stroke risk decreased rapidly with time, it remained elevated even
after a decade following the cancer diagnosis (16). In that same study, metastasis was
also associated with a greater risk of hemorrhagic and ischemic
stroke (SIR=2.2 and SIR=1.5, respectively) (16). In a similar vein, intracranial
hemorrhages (ICHs) have been reported in 20 to 50% of patients with
metastatic brain tumors (21). In
cancer patients, cerebral infarctions have been found to be more
frequent than hemorrhage (11,22),
whereas in patients with leukemia, hemorrhages have been found to
be much more common than infarcts caused by coagulopathy or CNS
infiltration (11,16,23).
The present review focuses on the possible
pathophysiological mechanisms and causes of stroke in cancer
patients, and aims to identify the most common and specific types
of stroke. Moreover, clinical manifestations are discussed, and
useful modalities to diagnose the cause of stroke in cancer
patients are presented, while providing valuable information on
treatment and prevention measures.
2. Cancer types associated with stroke
To date, several studies have attempted to elucidate
which cancer types present a stronger association with the
occurrence of stroke. A concise presentation is presented in
Table I. In a previous study,
among 1,274 patients with stroke admitted to a stroke unit, 12% had
an additional diagnosis of cancer, with urogenital, breast and
gastrointestinal being the most frequent cancer types (15). In addition, in patients diagnosed
with lung, pancreatic, colorectal, breast and prostate cancers, a
higher stroke incidence was reported (24). The stroke risk also seemed to be
associated with the aggressiveness of the cancer; lung, pancreatic
and colorectal cancers, which presented the highest stroke risks,
are usually diagnosed at a later stage than breast and prostate
cancer (24). The aforementioned
cancer types were also identified as the most common among patients
diagnosed with cancer post-stroke (7). Lung/respiratory tract cancer had one
of the strongest independent associations with death during a
follow-up of patients under 49 years of age with ischemic stroke
(25). Among 820,491 Swedish
patients with cancer, cancers of the small intestine, pancreas,
lung, nervous system and endocrine glands, and leukemia, presented
a >2-fold higher risk of ischemic stroke in the first 6 months
post-diagnosis, and this risk remained increased even after a
decade after hospitalization in cancer types, such as upper
respiratory/digestive tract cancer, salivary gland, colon, rectum,
nose, breast, prostate, urinary bladder, skin (squamous cell),
nervous system cancers and non-Hodgkin lymphoma. For hemorrhagic
stroke, the cancer type pattern changed and a highly elevated risk
was reported for cancers of the small intestine, liver, kidneys,
nervous system, thyroid gland, endocrine glands, connective tissue,
non-Hodgkin lymphoma, myeloma and leukemia (16). Similarly, patients with melanoma or
renal cell carcinoma and brain metastasis were characterized by a
4-fold higher risk of ICH compared to patients with lung cancer
with brain metastasis (21,25).
In general, melanoma, renal cell carcinoma, and choriocarcinoma are
the cancer types considered to have a higher tendency for
hemorrhaging (26).
 | Table IAssociation of cancer types with
ischemic (Is.S.) and hemorrhagic stroke (H.S.). |
Table I
Association of cancer types with
ischemic (Is.S.) and hemorrhagic stroke (H.S.).
| Cancer type | Is.S. | H.S. | Authors/(Refs.),
year |
|---|
| Lung | ✓ | - | Navi et al
(24), 2015a; Selvik et al (7), 2015; Aarnio et al (25), 2015; Zoller et al (16), 2012 |
| Colorectal-GI | - | ✓ | Stefan et al
(15), 2009; Navi et al
(24), 2015; Selvik et al
(7), 2015; Zoller et al
(16), 2012 |
| Breast | ✓ | - | Stefan et al
(15), 2009; Navi et al
(24), 2015 |
| Prostate | ✓ | - | Navi et al
(24), 2015; Selvik et al
(7), 2015 |
| Pancreatic | ✓ | - | Navi et al
(24), 2015; Zoller et al
(16), 2012 |
| Urogenital | ✓ | - | Stefan et al
(15), 2009 |
| Nervous system | ✓ | ✓ | Zoller et al
(16), 2012 |
| Skin/melanoma | ✓ | ✓ | Zoller et al
(16), 2012; Donato et al
(21), 2015b; Dearborn et al (26), 2014 |
| Leukemia | ✓ | ✓ | Zoller et al
(16), 2012 |
| Non-Hodgkin
lymphoma | ✓ | ✓ | Zoller et al
(16), 2012 |
| Myeloma | - | ✓ | Zoller et al
(16), 2012 |
|
Choriocarcinoma | - | ✓ | Dearborn et
al (26), 2014 |
| Endocrine
gland/thyroid | ✓ | ✓ | Zoller et al
(16), 2012 |
| Liver | - | ✓ | Zoller et al
(16), 2012 |
| Renal
cell/kidney | - | ✓ | Zoller et al
(16), 2012; Donato et al
(21), 2015b; Dearborn et al (26), 2014 |
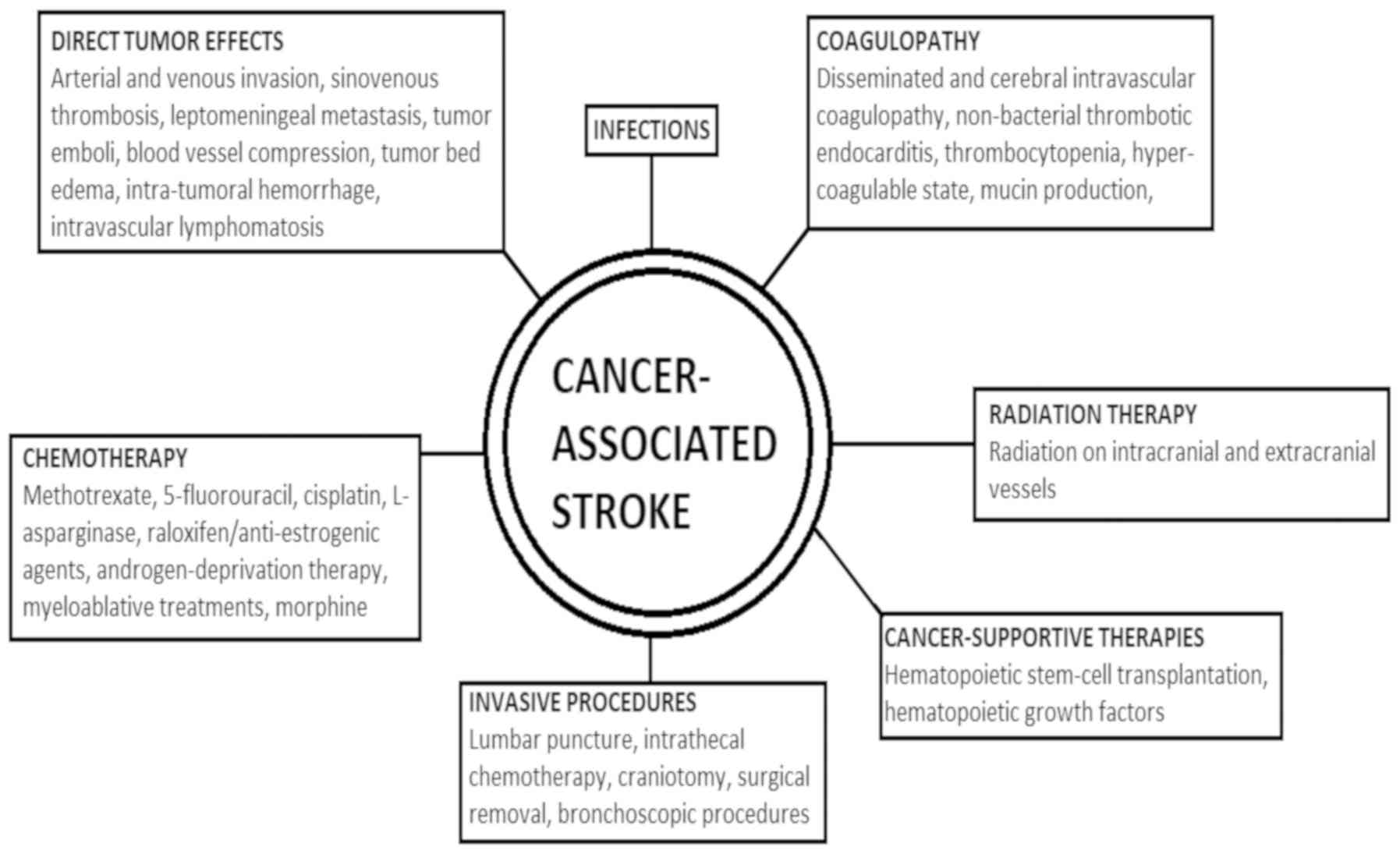
3. Pathophysiology
Several major pathophysiological mechanisms of
stroke exist in cancer patients, which can be directly related to
cancer, and are caused by cancer complications, such as coagulation
disorders and infections, or by therapeutic and diagnostic
interventions (4,25). Complications of chemotherapy,
radiation therapy (RT) and hematopoietic stem cell transplantation
(HSCT) for cancer can occur during the course, or even years after
treatment (20). A short depiction
of the various factors pertaining to a cancer-associated stroke is
presented in Fig. 1.
In many cases, the establishment of whether the
stroke is caused by the cancer itself and its complications or by
the treatment of cancer remains a challenge. In several occasions,
a combination of processes operate, and both hemorrhagic and
ischemic stroke can simultaneously occur (20). Consequently, in patients with
active malignancy, strokes are more frequently classified as 'of
undetermined etiology' or as 'other determined etiology' by TOAST
(https://radiopaedia.org/articles/toast-classification-in-acute-ischemic-stroke)
classification, whereas in non-malignancy patients, the majority of
strokes derives from small vessel occlusion (19,27,28).
Direct tumor effects
In clinical practice, direct tumor-related stroke is
rare and also difficult to identify (4). Direct tumor effects vary
considerably, and include arterial and venous sinus invasion by
tumor mass or leptomeningeal infiltrates, tumor emboli, blood
vessel compression by tumor growth or tumor bed edema, and
intratumoral hemorrhage (ITH) (20,26).
Leptomeningeal metastasis, also known as meningeal
carcinomatosis or neoplastic meningitis, is most commonly caused by
breast cancer, lung cancer and malignant melanoma, when cancer
cells spread into the cerebrospinal fluid (CSF) of the subarachnoid
space (2). It is estimated to
occur in approximately 5% of all cancer patients and is the third
most common metastatic complication of the CNS (29). Multiple lesions and venous sinus
occlusion from leptomeningeal carcinomatosis most commonly occur in
patients with neuroblastoma, lymphoma and lung cancer (30,31).
These can lead to cerebral infarctions due to tumor growth in the
Virchow-Robin perivascular spaces, leading to vessel thrombosis or
spasm and the infiltration of vessel walls (4,32).
Sinovenous thrombosis (SVT) is most widely reported
in pediatric patients. Occlusion in the cerebral venous system
obstructs venous outflow, leading to intracranial hypertension,
which in turn may lead to cerebral ischemia (33). Risk factors for its appearance
include cancer treatment, otitis media, sinusitis, trauma,
dehydration, heart failure or inherited thrombophilia (34), and the superior sagittal sinus is
the one most often affected (31,35).
In a multicenter retrospective study on patients with acute
lymphoblastic leukemia (ALL), the stroke prevalence was low (at
0.47%), but all cases were due to SVT (36). Similarly, a Nordic multicenter
study reported a SVT prevalence of 2% in pediatric patients with
ALL (34).
Intravascular lymphomatosis (IVL) (or
malignant/neoplastic angioendotheliosis, or Tappeiner syndrome) is
a rare lymphoproliferative disorder, a form of extranodal B-cell
non-Hodgkin's lymphoma, within the lumen of medium and small
vessels (4,37,38).
Only few are of T-cell or natural killer (NK)-cell origin (4,38).
IVL can affect any organ, but most frequently involves the CNS,
which also presents the highest rate of postmortem diagnosis and
exhibits a poor survival rate, particularly in the elderly, as
patients exhibit stroke-like symptoms. However, IVL is rarely
included in the differential diagnosis of CNS malignancy (37,38).
Patients often present with diffuse encephalopathy or multifocal
cerebral infarcts (4).
Arterial embolic infarction, although rare, can be
the result of tumor embolization, which can be large enough to
induce a transient ischemic attack (TIA) or infarction (23,39).
Myxoma or other heart and lung tumors can be the source of tumor
emboli in the brain (4). In the
literature, embolic cerebral infarcts are the most commonly
observed events in left atrial myxoma patients; in 10 to 30% of
whom, neurologic symptoms have been reported; these can also be the
initial and sole manifestations (40). As case reports have suggested, a
tumor embolus may also lead to a cerebral aneurysm via the invasion
of the vessel and its subsequent dilatation, which may rupture into
the parenchyma or the subarachnoid space (4,41).
Cancer is also associated with hemorrhage in each
brain compartment, with intraparenchymal hemorrhage (IPH) being the
most frequent, followed by subdural (SDH), subarachnoid (SAH) and
epidural hemorrhage (EDH), respectively (42). ITH is the most common cause of ICH
in cancer patients (42,43). The hemorrhage mechanism is
multifactorial and includes the increased creation of dilated,
thin-walled, intra-tumoral vessels, the rupture of these
newly-formed vessels, the tumor invasion of pre-existent vessels
and tumor necrosis (44).
Of the primary brain tumors, glioblastoma
multiforme, being the most common primary brain tumor, with highly
invasive cells, is most frequently linked to ICH.
Oligodendrogliomas are also predisposed to hemorrhage and even
benign tumors, mainly meningiomas, can be the cause of ITH
(42). Solid tumors most commonly
associated with ICH are lung, breast, melanoma and renal cell
cancers, due to their high population incidence, brain metastases
and histological components of neoangiogenesis, necrosis and blood
vessel invasion. Thyroid cancer, hepatocellular carcinoma and
choriocarcinoma also present an abnormally high tendency towards
hemorrhage (42,44). Choriocarcinoma has also been
associated with the occurrence of neoplastic aneurysms (4). Granulocytic sarcomas, rare tumors
that occur primarily in patients with acute myeloid leukaemia (AML)
or other myeloproliferative disorders, may also cause ICH (45). Hematological malignancies,
particularly leukemia, are also a frequent cause of ICH, although
their mechanism mainly involves disorders in coagulation (42), analyzed further below.
SDH in cancer patients is usually the result of
coagulopathy or trauma, alongside dural metastases (23,42,46).
The occurrence of SDH is speculated to be the result of the rupture
of vessels within the metastatic tumor, the erosion of adjacent
vessels by the tumor, or the rupture of the inner dural vessels due
to congestion of the outer vessels (23). However, only 15-40% of patients
with dural metastases have a coexistent SDH (42). SDH has been most commonly reported
in leukemia, prostate, lung and breast cancer and lymphoma
(46). SAH and intraventricular
hemorrhage are also usually due to coagulopathy, trauma or ITH, and
very rarely from arteriovenous malformations. When aneurysmal SAHs
occur in cancer patients, they should be investigated for atypical
etiologies, such as mycotic or neoplastic. These aneurysms are
fusiform, typically develop in distal middle cerebral artery
branches and are commonly tied to atrial myxoma, choriocarcinoma
and lung carcinoma (42). Finally,
EDH in association with a skull metastasis is a rare incident
(47).
Hyperleukocytosis, defined as a white blood cell
(WBC) count of >100,000 per mm3, has been commonly reported in
acute leukemia, causing CNS leukostasis (48,49).
The accumulation of leukemic blast cells within the capillary
vascular lumen can result in ICH (49) and mainly medium-sized vessels are
involved (50). It occurs in
approximately 7% of pediatric patients with acute leukemia,
worsening its prognosis as it is associated with a higher mortality
rate (49). Finally, in multiple
myeloma patients, ischemic stroke can be the result of
hyperviscosity syndrome due to elevated protein levels (4).
Coagulopathy
Coagulopathy is one of the main causes of stroke in
cancer patients. Coagulation disorders are the most common cause of
CVD in cancer patients and involve disseminated intravascular
coagulopathy (DIC), NBTE and thrombocytopenia (10,20).
The first post-mortem characteristics of cerebral intravascular
coagulation were described in 1975, in patients with breast cancer,
leukemia and lymphoma, in the setting of widespread metastasis and
sepsis (51).
In patients with cancer, the most common cause of
cerebrovascular thrombosis (CVT), identified in several clinical
series, is a hypercoagulable state that accompanies cancer,
resulting in systemic and cerebral arterial or venous thrombosis
(19,52). In intravascular coagulation, tumor
procoagulant activity, host inflammatory responses and extrinsic
factors are involved. Tumor cells express the procoagulants, tissue
factor (binds to factor VII) and cancer procoagulant, and release
inflammatory cytokines and vascular endothelial growth factor,
mediators that enhance procoagulant activity and angiogenesis
(6,26,53).
They also overexpress cytokines that attract leucocytes, possibly
triggering an inflammatory response, with prothrombotic effects
(16). Lung and pancreatic cancers
are the most common cancer types causing this coagulopathy
(24,52).
In 2015, an analysis by Karlińska et al
stated that stroke patients with an active cancer tend to
demonstrate lower hematocrit levels, higher serum C-reactive
protein (CRP) levels, and a higher erythrocyte sedimentation rate
when compared to cancer-free stroke patients. Since it is known
that the aforementioned inflammatory markers are associated with
coagulation, these findings indicate that, indeed, in active
malignancy, the cancer-specific prothrombotic mechanisms may play
an important role in stroke pathophysiology (27).
Specifically concerning adenocarcinomas, Dearborn
et al (2014) reported that they are considered to potentiate
thrombi via the production of mucin, a high molecular weight
molecule that is glycosylated and secreted normally by endothelial
cells. Adenocarcinomas, particularly those of the pancreas, colon,
breast, lung, prostate and ovarian system, can secrete this
molecule directly into the bloodstream, assisting in the appearance
of a viscous and hypercoagulable state. Mucin can also interact
with certain cell adhesion molecules on endothelial cells,
platelets, and lymphocytes to induce the formation of platelet-rich
microthrombi (26).
A broad small arterial and venous thrombotic
vasculopathy can also manifest in cancer patients (13). It is termed 'cerebral intravascular
coagulopathy' when the predominant signs are neurological, and is
considered as the CNS equivalent of cancer patients' systemic
thrombotic microangiopathy (35).
This condition is not often reported (35), and it is speculated to be more
common than originally estimated, as it can be mistaken with other
encephalopathy causes in cancer patients, and its diagnosis can
only be confirmed at autopsy (23). In the first autopsy study by Graus
et al in 1985, it was only reported in 8% out of 500
patients (11).
Depending on the type, cancer can also be linked to
acute or chronic DIC. In DIC, a disruption in the balance between
thrombus formation and thrombolysis can either lead to the
thrombotic occlusion of vessels, due to the excess activation of
the coagulation process, or to diffuse hemorrhage, due to the
subsequent depletion of platelets and coagulation factors.
Therefore, in cancer patients, it can manifest as thrombotic stroke
and intracerebral hemorrhage (4).
A variety of thrombohemorrhagic entities, such as low-grade DIC,
are associated with solid tumors, whereas leukemia, myelocytic and
lymphocytic, usually present acute DIC, which manifest as marked
bleeding (4,54). Patients with pancreatic cancer and
adenocarcinoma have particularly been reported to be at a very high
risk of DIC (55). Acute
promyelocytic leukemia is strongly associated with severe
hemorrhage in the setting of DIC and other hemostatic disorders
(54). These bleeding
manifestations usually occur in the parenchyma or the subdural
compartment, and rarely in the subarachnoid space (4,56,57).
NBTE, also known as marantic endocarditis, is
defined as non-infectious, sterile cardiac valvular vegetations
with negative blood cultures, and it is most commonly caused by an
underlying malignancy (58). The
cancer in this case is more often widespread and cerebral
infarction is a late complication; however, in rare instances, NBTE
with cerebral infarction is the presenting sign of cancer (59). In NBTE, sterile platelet-thrombin
vegetations develop on cardiac valves (almost exclusively the left
heart valves; mitral and aortic) in association with widespread
systemic and cerebral thrombosis (60,61).
It usually presents with systemic and pulmonary embolization, with
the most common neurological complication being ischemic stroke
(58).
The exact NBTE prevalence in cancer patients has not
been accurately estimated, as tissue diagnosis is often
inaccessible and echocardiographic studies are not widely used to
screen cancer patients for NBTE (62). Some original autopsy studies have
reported NBTE in 9.3% of cancer patients, and cancer in 59% of
patients with NBTE (63,64). In a study by Edoute et al
(1997), valvular vegetations consistent with NBTE were found in 19%
out of 200 cancer patients (65);
Liu and Frishman (2016), several years later, also reported NBTE in
19% of disseminated adenocarcinomas (61). Of note, Taccone et al (2008)
reported NBTE as the most common cause of stroke in their cancer
patients, followed by intravascular coagulation and atherosclerosis
(5). As an entity, NBTE is most
commonly reported in adenocarcinomas, particularly mucin-producing
carcinomas of the lung or the gastrointestinal tract, lymphoma, and
also in carcinomas of the ovarian, the pancreas and biliary system
(35,61,62).
Adenocarcinomas, as previously mentioned, are considered to
potentiate thrombi via the production of mucin (26).
Thrombocytopenia may be the result of hematological
cancers or, most frequently, the result of chemotherapy (54,57).
Additional causes of significant thrombocytopenia include tumor
involvement of bone marrow and spleen, microangiopathic disorders
such as DIC, thrombotic thrombopenic purpura (TTP) or hemolytic
uremic syndrome (HUS). Lymphoproliferative malignancies can also be
associated with secondary immune thrombocytopenia (54). In a study by Correale et al
(1990) on 989 patients with lymphoma, 2% had ICH, in clear
association with platelet alterations (66) and in a 2013 study on pediatric
cancer patients, all those suffering with ICH had platelet counts
of <100,000/mm3 (67).
Infections
Infections rank among the first causes of morbidity
in cancer patients, particularly in those with hematological
malignancies, where autopsy studies have demonstrate that
approximately 60% of deaths are infection-related (68). Cancer patients are frequently
immunocompromised, and thus are automatically at risk of infection,
relevant to the type of cancer (4,68,69),
and the association between stroke and systemic infection has been
well established. The organisms most frequently linked to an
increased risk of stroke include Helicobacter pylori,
Chlamydia pneumoniae, Mycoplasma pneumoniae,
Haemophilus influenzae, Epstein-Barr virus, herpes simplex
virus (HSV)-1 and HSV-2, and cytomegalovirus (CMV) (70).
The systemic inflammatory response induced by the
pathogen can damage the vascular endothelium and predispose
patients to ICH (70). Infectious
endocarditis is a predominant cause of stroke, via embolism to the
brain. The degradation of the arterial wall by bacteria or septic
emboli results in abnormal dilatation or mycotic aneurysms
(70). These aneurysms usually
occur at distal branches of the middle cerebral artery and can
rupture, leading to ICH (56,70).
Staphylococcus aureus, β-hemolytic streptococci and
Streptococcus viridans are the bacteria which most commonly
complicate an infective endocarditis with ICH (70).
Moving on to more specific mechanisms, HSV-1
meningoenchephalitis can lead to petechial cerebral hemorrhages and
ICH in its severe forms. Syphilis causes an obliterative
endarteritis, which may in turn lead to ischemic stroke through
progressive luminal stenosis. Tuberculosis (TB) can present
infarcts in tuberculous meningitis, which accompanies pulmonary TB
in 1% of the patients (70). In
cancer patients, opportunistic infections with pathogens, such as
the JC40 virus can cause a progressive multifocal
leukoencephalopathy, which maybe be mistakenly characterized as a
cerebrovascular lesion (4).
Fungal infections are the second most common in
cancer patients, following bacterial ones (68). Fungal meningitis can be caused by
yeasts (such as Cryptococcus spp. and Candida spp.)
and moulds (such as Aspergillus spp.) (70). Yeasts can cause stroke, ischemic or
hemorrhagic, via a vasculopathy of the large vessels traversing the
subarachnoid space, venous outflow obstruction, endarteritis and
the formation of abscesses linked to hemorrhage. They do not
usually invade cerebral vessels; moulds on the contrary, produce
enzymes that allow vessel-wall invasion, causing mycotic arteritis
or aneurysms (70). The
hematogenous spread of septic emboli to the brain can trigger an
ischemic or hemorrhagic stroke, with or without the presence of
arteritis and aneurysms (20,70).
Cerebral Aspergillus infections are mostly secondary to lung
infection, whereas Candida ones usually originate from the
gastrointestinal or genitourinary tract (4). Fungal septic emboli can also occur in
leukemic patients who have undergone bone marrow transplantation
(23).
Viral infections are not a rare instance either, in
cancer patients, and are usually the result of reactivation of a
latent disease, primarily in hematological malignancies. Parasitic
and unusual infections should also be considered in patients with a
history of exposure (68).
Susceptibility to infections in cancer patients is
due to host-associated and treatment-related factors (68,69).
The former include underlying immune deficiencies, comorbidities,
ulcerating lesions in mucosal surfaces, past infections, poor
nutritional status, catatonic state and psychological stress, while
the latter consist of surgery and invasive procedures, radiation,
immunosuppressant regimens and antimicrobial use (68,69).
However, the identification of a sole immunodeficiency factor in
cancer patients is utopic in common clinical practice, as multiple
deficiencies usually co-exist (68).
Hematological malignancies heavily burden patients
in terms of immunodeficiency. Patients with acute leukemia and
lymphoma manifest neutropenia, due to the disease itself or the
cytotoxic chemotherapy, and present different types of infections
(68). Typically, Gram-negative
bacilli, such as Escherichia coli, Klebsiella spp.
and Pseudomonas aeruginosa, are the causes of the earliest
infections. However, an increase in infections caused by
Gram-positive aerobic bacteria, mainly staphylococci and
streptococci, has recently been reported (68,69).
Fungal and viral infections occur later in the course of
neutropenia (68), and patients
with neutropenia are particularly prone to developing bloodstream
infections (BSIs), particularly following bone marrow
transplantation (69). On the
other hand, chronic lymphocytic leukemia (CLL) usually leads to
deficits in humoral immunity, while additional defects in
cell-mediated immunity, complement activity, and neutrophil and
other phagocytic cell activity manifest following the treatment.
Hypogammaglobulinemia predisposes patients to infections by
Streptococcus pneumoniae, Haemophilus influenzae,
Neisseria meningitidis and Escherichia coli, whereas
treatment modalities, such as alkylating agents predispose to
streptococcal, staphylococcal, and enteric Gram-negative bacterial
infections. Additionally, purine analogs or alemtuzumab treatments
predispose to opportunistic infections with Listeria spp.,
Mycobacterium tuberculosis, Nocardia spp.,
Candida spp., Aspergillus spp., Pneumocystis
jiroveci and herpesviruses. Finally, multiple myeloma increases
the susceptibility to infections with encapsulated bacteria such as
Streptococcus pneumoniae, Haemophilus influenzae and
Neisseria meningitidis (68).
Solid organ tumors do not lead to the same degree
of immunodeficiency as hematological malignancies, mainly as
chemotherapy in these cases does not cause long-term or profound
neutropenia; a few exceptions exist, such as metastatic breast
carcinoma, prostate, lung, adrenal, thyroid and kidney cancers,
that tend to infiltrate the bone marrow and actually cause
neutropenia in advanced stages (68). Any tumor that disrupts anatomical
barriers can give way to infections, and specifically skin cancers
are usually associated with staphylococci and streptococci, oral
cavity and nasopharynx with anaerobic bacteria, streptococci and
Haemophilus influenzae, gastrointestinal tract with
enterobacteriaceae and fungi, and the female genital tract with
Enterobacteriaceae, anaerobic Gram-negative bacteria, Enterococci
and Clostridium spp. (68).
In a study using predominantly solid-organ-cancer patients to
examine the microorganisms that cause BSIs, Escherichia coli
was the most common Gram-negative bacterium cultivated in the
cancer patient group. Cancer patients also presented twice as many
BSIs by Enterococcus faecalis, Enterococcus faecium,
Pseudomonas aeruginosa and Enterobacter cloacae.
Doubled was also the percentage of positive yeast blood cultures
from cancer patients compared with non-cancer patients (69).
Chemotherapy
Chemotherapy has often been blamed as the cause of
cerebral arterial or venous thrombosis, although this can occur in
the setting of advanced malignancy as well (56). Chemotherapy can lead to stroke via
endothelial toxicity and abnormalities in coagulation and
hemostasis factors (71). It can
also trigger the manifestation of a stroke by transferring
susceptibility via immunosuppression and the increase in
opportunistic infections (68). In
general, the risk of a chemotherapy-induced stroke is rather low
and the risk is higher for some specific regimens, such as
methotrexate (MTX), 5-fluorouracil, cisplatin and L-asparaginase
(4,71). However, even neoadjuvant
chemotherapy (NC) has been linked to an increased risk of stroke;
Abt et al (2014) reported that NC was linked to a higher
risk of short-term stroke and mortality in patients undergoing
brain tumor resection (72).
L-asparaginase has one of the best known
associations with thrombosis and stroke (56,71,73).
It is typically used in combination regimens for breast cancer and
in the induction therapy of ALL (4,56).
It has repeatedly been associated with CVT in children treated for
leukemia (4,26), as asparaginase and steroids are
deemed strong prothrombotic agents (34). The cerebrovascular effects can
manifest as cerebral thrombosis or hemorrhage, and the patients
that receive such treatments should be closely monitored and the
treatment should be interrupted in the case of a cerebrovascular
event (CVE) (4).
All agents with anti-estrogenic effects may
increase the risk of CVD (74,75).
More specifically, raloxifene, a selective estrogen receptor
modulator, has been linked to a higher incidence of stroke and
thromboembolic events (76). For
tamoxifen, historically the standard endocrine therapy for breast
cancer, the reported findings vary among studies. It was the only
factor associated with an increased risk of stroke in 4,414 10-year
survivors of early breast cancer (77) and was associated with a
significantly increased risk of venous thromboembolic events,
pulmonary embolism and stroke, as reviewed by Esteva and Hortobagyi
(74). In other analyses however,
tamoxifen alone was not associated with an increased risk of CVD
(78), but only when combined with
hypertension (79). Using data
from the Swedish National Hospital Discharge Registry and the
Swedish Cause of Death Registry, the incidence of CVD was increased
during the active treatment phase and decreased in the
post-treatment period (80).
Contrary to the above, a Taiwanese study including 3,690
breast-cancer women revealed a significant reduction in
cardiovascular events, including hemorrhagic and ischemic stroke
(81). Hence, the literature data
on tamoxifen have yielded conflicting results (4).
In three large-scale studies, patients with
prostate cancer treated with endocrine hormonal therapy [androgen
deprivation therapy (ADT)] were found to be at an increased risk of
stroke (75,82,83).
In a smaller prospective study from Taiwan, no significant
difference was found in the risk of stroke between ethnic Chinese
patients with prostate cancer who did or did not receive ADT, after
adjusting for potential confounders (84). A review of the literature by Meng
et al (2016) concluded that ADT does indeed present an
increased risk of stroke. Significance was reached when ADT
monotherapy was examined after removing prostatectomy and
radiotherapy patients, and in gonadotropin-releasing hormone
(GnRH), GnRH plus oral antiandrogen and orchiectomy treatments
(85).
Platinum compounds, clinically, seem to present the
highest risk of stroke (4).
Cisplatin has repeatedly been reported to be associated with CVEs
(4,71,86).
However, the mechanisms involved remain largely unknown.
Circulating endothelial- and platelet-derived particles can
contribute to cisplatin-induced stroke (4). Kuan et al (2014) reported an
elevated relative risk (RR) of stroke in patients with ovarian
cancer that were treated with cisplatin-based or carboplatin-based
chemotherapy agents, as opposed to non-platinum-based regimens
(87).
Stroke-like events and stroke have been reported in
MTX treatment (4,88). In pediatric patients, they have
been linked with acute treatment, but not with subsequent
administration (88). However,
long-term survivors from pediatric cancer groups were found to be
40-fold more prone to developing stroke than their sibling controls
(4).
Brain hemorrhages can also manifest in the setting
of chemotherapy treatment. The chemotherapy of AML with a
monoblastic component has been associated with a high incidence of
SDH (89); an associated
hemorrhagic vasculitis or cerebritis has occasionally been reported
as well (56) and hemolysis from
chemotherapy administration is a rare cause of brain hemorrhage
(23). Chemotherapy, particularly
the myeloablative treatment of hematological malignancies, remains
the most common cause of thrombocytopenia in cancer patients.
However, several non-myeloablative chemotherapeutic agents have
also been connected to its appearance, even though most of the
classic chemotherapeutic treatment plans in cancers, such as of the
colon, lung, breast and prostate, have a low incidence of National
Cancer Institute (NCI) Grade 3 (platelet count of 25 to
49.9×109/l) and 4 (<25×109/l)
thrombocytopenia. Moreover, thrombocytopenia development has also
been related to newer therapeutic agents. When examining patients
treated with sunitinib, a multi-targeted tyrosine kinase FDA
approved for the treatment of renal cell carcinoma, pancreatic
neuroendocrine tumors and gastrointestinal stromal tumors, 7.6% of
them presented high-grade (NCI Grade 3 or 4) thrombocytopenia
(54).
Finally, a recent study based on a large malignancy
cohort of cancer patients, demonstrated that symptomatic therapy in
cancer patients may be related to stroke as well; intense morphine
treatment is associated with an increased stroke incidence in
cancer patients, and the association is particularly significant
for prostate cancer patients (90).
Radiation therapy
RT has been shown to be an independent risk factor
for cardiovascular disease and CVD in cancer patients (91-93).
Post-radiation vasculopathy occurs in intra-cranial and
extracranial vessels, with medium and large-sized vessels being
most frequently affected (4). The
subsequent stenosis or occlusion is typically more extensive within
the radiation portal, than the atherosclerosis which develops in
its absence as well (56).
Radiation to the neck has been related to
subsequent vascular wall thickening, atherosclerotic plaque
formation and vascular damage (26,91,94).
Studies have also confirmed that RT predisposes to the formation of
inflammatory plaques, which are more likely to rupture and cause a
stroke, or a heart attack (91).
Patients that have received RT to the head and neck area have also
been shown to have significant internal carotid artery/common
carotid artery stenosis (95), and
notably, patients can develop a radiological image that closely
resembles Moyamoya syndrome; stenosis of the carotid vessel with
abnormal netlike vessels and transdural anastomosis distal to the
stenosis (26). The frequency of
secondary-to-RT internal carotid stenosis ranges from 12 to 60%,
depending on the study (4). Thus,
several studies using different methods and patients with varied
disease processes have reported an increased risk of CVEs following
RT for head and neck cancers or lymphoma (12,92,94,96,97).
The first large study was conducted in 1981 and demonstrated a
post-cervical-RT stroke incidence of 6.3% (96). Subsequent studies further reported
a 15-year cumulative stroke risk of 12% following RT, and RT to the
neck and mediastinum to be an independent risk factor for CVD
(12,97). Scott et al (2009) reported a
crude stroke risk of 2.6% following neck RT, compared to 0.29% of
non-RT patients (94), whereas
Smith et al (2008) associated an excess CVD risk to
definitive RT for head and neck cancers, but not to post-operative
RT in older patients (98).
Concerning the effects of RT on operated patients, a 2014 study
compared patients with lung cancer, and found a higher stroke
incidence (almost double) compared to post-operative RT and with
surgery alone and a lower two-year-stroke-free survival rate
(99). However, finally, radiation
fields that included the carotid artery did not seem to increase
the risk of stroke in breast cancer survivors in three large-scale
studies (6,79,100).
Pediatric cancer patients are not excluded from
this side-effect; their cerebral vessels can also be the subject of
stenosis or occlusion following RT. Morris et al (2009)
described the manifestations of RT-induced CVD in pediatric
patients having received RT to the brain and/or the neck, and they
include steno-occlusive disease, aneurysm, mineralizing
microangiopathy, vascular malformations and stroke-like migraines
(101). A 2005 study found a RR
for late-occurring stroke in patients who received mantle RT of
5.62 (14). Mueller et al
(2013) confirmed that cranial irradiation placed childhood cancer
survivors at a risk of both, first and recurrent, and stroke
(102). Finally, a large cohort
study revealed that the risk of stroke in childhood cancer
survivors was associated with cranial RT in a dose-dependent manner
(103).
Cancer supportive therapies: HSCT and
hematopoietic growth factors (HGFs)
HSCT and HGFs are increasingly used in cancer care
in support of standard anticancer therapies in order to limit bone
marrow toxicity due to chemotherapeutic agents and to ameliorate
the quality of life of patients, reducing asthenia,
thrombocytopenia and neutropenia. Both HSCT and HGFs are considered
cancer-supporting therapies; however, there are still concerns
about the safety of these treatments, particularly regarding
peripheral and cerebral cardiovascular complications (20). To date, several mechanisms have
been described for HSCT-related hemorrhagic stroke, including
graft-versus-host disease (GVHD) (only for allogenic
transplantation), alterations in coagulation profiles and
infections (35,104,105). Syed et al, in 2016
(105), reported that cerebral
IPH occurred after a median time of 122 days after HSCT in 1.1 to
2.4% of the patients with a higher mortality rate compared to
subarachnoid hemorrhage or subdural hematoma (105,106). Furthermore, another
cerebrovascular complication related to HSCT is that of vasculitis,
which rarely occurs due to chronic GVHD, leading to cerebral
infarction, hemorrhage, or leukoencephalopathy (106-108).
Cerebrovascular complications following HSCT are
potentially fatal events. Generally, cerebrovascular hemorrhagic
events are related to recalcitrance to platelet transfusions, to
arterial hypertensions, low fibrinogen serum levels and, as
previously described, to high-grade GVHD (109). Usually, the onset of
cerebrovascular complications is characterized by worsening
sensorium and headache without lateralizing signs. However, in some
cases, the onset of CVDs is asymptomatic, making a firm diagnosis
difficult (110). The diagnosis
of stroke and other CVDs is often performed by a computer-assisted
tomography (CT) scan, as this technique allows for the highlighting
of the hemorrhagic regions as hyper-intense areas assisting the
diagnosis of intracranial bleeding. The CT scan is preferred as
this reveals possible lesions at least 12 h earlier than what can
be done with magnetic resonance imaging (MRI), which is therefore
not widely used. However, sometimes patients are asymptomatic with
negative CT scans in 20-25% of patients (109,111,112).
Overall, conflicting data have been generated as
regards the frequency of CVDs and hemorrhagic stroke following
HSCT. Katz and Segal (2005) reported a hemorrhagic stroke rate of
>32% established following the autopsy examination of patients
who died as a result of HSCT (20). Liu et al (2017) recently
presented the results of an observational study conducted on 459
adult patients undergoing allogeneic HSCT at an Asian tertiary
medical center between January, 2003 and December, 2015. Those
authors reported that the percentage of both ischemic and
hemorrhagic stroke occurred only in 5.2% of HSCT-treated patients
(24 out of 459) (113). Zhang
et al (2016) studied the risk of ICH in a cohort of 2,169
patients treated with HSCT for both malignant and non-malignant
hematopoietic disorders. These investigators reported that only
1.5% of these patients (32 patients) developed an ICH complication
in a median onset time of 147.5 days (114). These data underline that the risk
assessment of HSCT-related stroke is not yet completely defined,
probably due to different pathological manifestations that
characterize CVDs, among which the most common are IPH, SDH, SAH
and multiple hemorrhage lesions in the brain parenchyma. Hence,
there is a need for a better understanding of the prodromal
symptoms of ICH after HSCT in cancer patients with hematological
and non-hematological malignancies.
As described above, numerous studies have
associated the onset of stroke with the use of hematopoietic stem
cells for the treatment of oncohematological diseases, while
regarding the existing association between stroke and
colony-stimulating factors, current data is still limited and
conflicting.
Over the past decades, patients diagnosed with
cancer have begun to be treated with HGFs, which consist of
colony-stimulating factors (CSFs) and erythropoiesis-stimulating
agents (ESAs). Both CSFs and ESAs are commonly used to prevent
infection and neutropenia in patients receiving chemotherapy and
for the treatment of asthenia by stimulating the growth of red
blood cells, respectively (115-117). The use of CSFs and ESAs results
in better cancer patient adherence to chemotherapy without a
reduction in dose administration, thus improving the clinical
outcomes of the therapy (118,119).
The use of CSFs and ESAs has definitely improved
the effectiveness of chemotherapy treatments, although several
observational and randomized studies have indicated that these HGFs
had some short- and long-term side effects in several cancer
pathologies (120,121). Among these side-effects are
venous thromboembolism (VTE), stroke, ischemic heart disease and
AML or myelodysplastic syndrome (MDS) in patients with various
types of cancer, including breast cancer (120-122).
Several studies have assessed the risk of AML or
MDS following the administration of CSFs and ESAs in cancer
patients. However, there are still doubts concerning the safety of
these treatments and their potential increased risk of developing
vascular and cardiovascular diseases (e.g., stroke and VTE)
(123,124). In particular, the use of CSFs and
ESAs has been related to the development of blood clots and
vascular dysfunctions, including stroke (125). For these reasons, in 2007, the
Food and Drug Administration (FDA) stated that the use of HGFs can
be dangerous and therefore, the safety of these compounds still
needs to be verified (126).
Du and Zhang (2015) and Du et al (2016)
evaluated the association between the use of CSFs and ESAs and the
increased risk of VTE, stroke, ischemic heart disease and AML/MDS
onset in patients with breast and colorectal cancers (120,121). These authors demonstrated that
patients with colorectal cancer treated with chemotherapy combined
with CSFs and ESAs had an increased risk of MDS, VTE and to a
lesser extent, an increased risk of ischemic heart disease
(120). With regards to breast
cancer patients, the retrospective cohort study by Du et al
demonstrated that the combination of chemotherapy, CSFs and ESAs
was associated with a 2-fold increased risk of developing VTE (2.01
hazard ratio) and AML/MDS (4.55 hazard ratio) and a weak increased
risk of ischemic heart disease (1.08 hazard ratio), while the use
of both CSFs and ESAs was not associated with an increased risk of
stroke (121). These two studies
demonstrated that the use of HGFs was not associated with the risk
of stroke in cancer patients. Other studies have also tried to
define the risk associated with stroke following the administration
of CSFs and ESAs; however, studies are limited in this regard with
inconsistent data, preventing the proper estimation of the real
risk of stroke events following the administration of HGFs as
supportive therapies in cancer patients (127-130).
Finally, a growing body of evidence has indicated
how the use of granulocyte colony-stimulating factor (G-CSF) and
granulocyte macrophage colony-stimulating factor (GM-CSF) may
induce the recovery of a stroke-related cerebral damage via
neuroprotective and neurorepairing mechanisms involving the
activation of bone marrow-derived CD34(+) stem cells and the
reduction of the lesion volume (131-133). In particular, the administration
of G-CSF appears to be safe and well tolerated by patients,
although further studies are required to verify the efficacy and
tolerability of these factors for the treatment of stroke.
Invasive procedures
Cancer patients are subjected to a wide variety of
aggressive treatments and tests, including invasive procedures,
many of which can induce stroke. Cancer can heavily impact the
surgical outcome as well. As Jacob and Kostev (2016) have
previously suggested, cancer has a negative effect on the
occurrence of intraoperative and post-procedural complications,
with colorectal and breast cancers presenting the strongest
association (134). Specifically,
lumbar puncture, intrathecal chemotherapy and craniotomy have been
linked to an increased risk of SDH (42,46).
In surgery, the risk of an embolic stroke is generally elevated, as
it may promote the release of emboli. Pulmonary interventions in
particular, such as bronchoscopic biopsies and lung surgery, have
presented stroke peri- and post-operatively (4).
In a study carried out on patients with glioma with
ischemic stroke, Kamiya-Matsuoka et al (2015) (135), reported that 53% of the patients
had post-operative stroke and 33% had a CVE after 2 weeks of
surgery; the episodes were, therefore, quite frequent in the
post-operative period. The majority of the stroke cases were close
to the resection cavity, possibly suggesting iatrogenic causes.
However, surgery in general remains a main stroke risk factor in
these patients. Further adding to the aforementioned data, the
events were frequent, particularly in patients treated with prior
chemotherapy and radiation (135).
4. From stroke to cancer
Despite a plethora of evidence in the literature
linking the occurrence of stroke to malignancy, the retrograde
association between cancer and stroke has yet to be proven. It
remains to be determined as to whether stroke causes cancer or
whether it is likely an early manifestation of cancer (136,137). A 2017 survey of Taiwanese
patients found out that although patients with stroke presented a
lower risk of developing any type of cancer compared to the
controls, patients with brain cancer presented a higher risk
(adjusted RR of 3.09). In the same survey, 40-60 years old females
had a higher risk of developing brain cancer, while overall, the
mean time for developing any type of cancer, including brain
cancer, was significantly shorter in the stroke group. The
researchers also reported that upon examining their own cases of
malignant gliomas, only the ones with stroke previous to cancer
were strongly histologically stained for HIF-1α, a key hypoxic
regulator, possibly signifying the connection between stroke and
the malignancy (136).
Similarly, but possibly showing somewhat
conflicting results by gender stratification, a study on menopausal
women found an overall lower incidence of cancer in women with a
history of stroke compared to women without stroke and adjusted for
covariate factors (137).
However, it is speculated that the observed lower incidence of
cancer in women that suffered a stroke and survived long enough to
develop a cancer, could have been associated with lifestyle changes
occurring following the survival of the stroke (137).
5. Clinical presentation and diagnosis
As stroke greatly affects the prognosis of a cancer
patient, its early discovery remains critical. The interval time
from cancer diagnosis to stroke manifestation varies considerably
and depends on the cancer type as well; solid tumors usually take
longer periods of time than hematological malignancies (31). When a stroke occurs in a cancer
patient, the clinician can/must pinpoint its cause by carefully
examining the clinical setting, taking into consideration the
cancer type and its treatment (11). However, caution is advised, as an
increase in brain tumors has been noted within the first year after
stroke, insinuating that brain tumors can be misinterpreted as
strokes (13). The original
autopsy study by Graus et al (1985) described the main
clinical presentation of CVD in cancer patients to resemble that of
a diffuse encephalopathy more than the typical image of acute onset
with a focal deficit (11).
ICH commonly presents with focal neurological
deficits, headaches and encephalopathy; the presentation in cancer
patients largely follows the general population. Other common
symptoms include hemiparesis, nausea or vomiting, seizure and maybe
even coma. Occasionally, symptoms may be gradual and non-specific,
largely characterized by confusion and lethargy, particularly in
SDH (42). Primary or metastatic
hemorrhage in the brain or dura may also produce the initial
clinical signs of a brain tumor or a change in chronic signs
induced by the tumor (56). In
gliomas, hemorrhages appear within the tumor, while in the majority
of metastatic brain tumors, they are located around the tumor
borders (44). The initial
diagnostic evaluation of these hemorrhages does not differentiate
from the standard guidelines (42). In the case of a suspected ICH,
patients should first be evaluated with a non-contrast head CT and
if there are no contraindications, post-contrast sequences and CT
angiography can further assist in locating an underlying tumor or
vascular malformations (42).
Cerebral metastasis can occasionally be the initial
cancer manifestation and patients may develop intracerebral
hemorrhage with a stroke-like image (138). Brain metastases can present with
a wide variety of neurological symptoms, with the most common ones
being headaches, an impaired mental status and focal weakness, with
usually a hemiparetic pattern. Sensory loss and gait deficits
typically involve one side of the body, as the tumor affects its
respective hemisphere (29).
Metastatic brain tumors can be confirmed by a CT scan or MRI, where
they typically appear rounded, well-circumscribed,
non-infiltrative, with an excessive amount of edema and almost
always enhanced by contrast mediums. In some cases, a biopsy is
needed to reach a firm diagnosis (29).
Leptomeningeal metastases should be considered in
cancer patients with signs and symptoms involving more than one
anatomic site within the nervous system. The spine is affected in
the majority of leptomeningeal carcinomatosis patients; the most
common manifestations include neck or back pain, asymmetric
reflexes, extremity weakness (usually affects both legs), pain,
spinal tenderness and cranial nerve palsies, that appear in more
than half of the patients (29).
Rarely, as case reports have suggested, it can present with signs
of meningitis and focal cerebral infarction (32). The staging of leptomeningeal
metastasis includes contrast-enhanced brain and spine MRI, along
with a radionuclide CSF flow study (29). Leptomeningeal dissemination has
also been shown, in a case report, to resemble cerebral
vasculopathy (30).
Cerebral venous occlusion often presents with
headaches in cancer patients (31,51).
In children, symptoms and signs are age-related, as seizures and an
altered mental status are the most frequent manifestations in
newborns, as opposed to headaches, vomiting, lethargy and sixth
cranial nerve palsy in children and adolescents. The findings of a
physical examination may only include the altered mental status, or
even signs of intracranial hypertension, such as papilledema
(33). Tumor-related CVT usually
develops gradually and can also produce signs of elevated
intracranial pressure (ICP) (56).
Combining the results of two studies on patients with pediatric ALL
and SVT (2005 and 2015), the most common manifestations are diffuse
neurological signs, seizures, headache, fatigue, cerebral nerve
palsies and hemiparesis (34,36).
CT, MRI and the respective venographies can be used to diagnose
venous occlusion (31,34). The 'empty delta' sign in a CT scan
represents a lack of enhancement in the thrombosed sinus and is
considered characteristic (4,30).
Simultaneously, a tumor or associated occurrences such as
infarction, hemorrhage and infiltrates can also be detected
(20,30).
Intravascular lymphomatosis (IVL) can also occur
with stroke-like symptoms (38)
and in general, the signs and symptoms are related to the involved
organs (139). MRI has limited
use in its diagnosis, as it does not present enhancement and the
majority of diagnoses are still made post-mortem; an unfortunate
realisation, since IVL is sensitive to chemotherapy when diagnosed
(38). Specifically, it is
accompanied by many false negative results as it typically arises
without tumor masses or lymphadenopathy (139). Patients usually display a
pathological hemogram, with anemia in more than half of the
patients, and increased lactate dehydrogenase (LDH) and
β2-microglobulin levels in the vast majority. Organ-specific
symptoms require specific laboratory or imaging exams, and
eventually biopic assessment (139).
The course of intravascular coagulopathy is
progressive and can result in coma and death (51). These progressive and extensive
vessel occlusions can lead to diffuse microinfarctions and
encephalopathy, with superimposed transient focal signs, such as
partial focal seizures (23). In
leukemia and lymphoma, the coagulopathy is typically that of acute
DIC and can lead to systemic and brain hemorrhages (4,54),
mostly located in the brain parenchyma or the subdural compartment
(4). Laboratory results should be
interpreted with caution; evidence of coagulopathy is challenging
to distinguish. The main points of interest are the peripheral
smear, low platelet counts, affected coagulation function tests,
high D-dimer levels, low fibrinogen levels and increased partial
thromboplastin time, which, alongside prothrombin, may at times
only be slightly altered or even appear within normal range
(4,140). Finally, limb venous duplex scans,
echocardiograms and pulmonary ventilation perfusion scans are also
useful modalities in the investigation of systemic coagulopathy
(60).
NBTE is usually silent until severe complications
occur, such as embolization; the incidence of cerebral ischemia is
significantly higher than in infective endocarditis (61). The valvular lesions can lead to
new-onset cardiac murmurs, arrhythmias and heart failure, with
dyspnea, orthopnea and peripheral edemas (61). NBTE-induced stroke usually presents
with focal or multifocal symptoms (23) and aphasia is considered to be the
commonest neurological feature (59). The widespread infarctions may cause
confusion and lethargy, and the encephalopathy may also fluctuate
(23,141).
The diagnosis of NBTE requires, first and foremost,
the exclusion of infection (61).
Transthoracic or transesophageal echocardiography can serve as the
initial imaging processes for the assessment of the valvular
lesions, which are usually rounded, sessile, heterogeneous in
shape, and >3 mm in size, and are located mainly on the mitral
and aortic valves (60,61,142). An MRI typically shows numerous
infarctions of varying size in several territories (61,143) and a CT scan/MRI is also useful in
detecting neurovascular embolization (61). Angiography can also detect the
occlusions with sensitivity, which are commonly located in the
middle cerebral artery (59), and
diffusion-weighted MRI can also assist in characterizing the stroke
patterns (61). Ultimately, the
most definite diagnosis can only occur postmortem (61).
Concerning infections, septic emboli may result in
focal cerebral signs, seizures or encephalopathy and distinct
manifestations depending on the microorganism (56,68).
In order to diagnose fungal infections in particular, a high index
of clinical suspicion is crucial, since the isolation of the
microorganism is difficult (56,144). The diagnosis may require cultures
and histopathology of tissue samples, fungal antigen assays or
molecular tests for fungal DNA (144).
Leukostasis as a result of hyperleukocytosis
usually affects the lungs and the CNS (145). In the CNS, it is dynamic and
reversible, fluctuating according to the leukocyte count (50). The CNS symptoms range from nausea,
tinnitus, visual impairment, ataxia, psychiatric manifestations
such as agitation or delirium, to mental status disorders, with
somnolence, stupor and even coma. The respiratory involvement
varies and can lead to acute respiratory failure. Often, fever, leg
or intestinal pain and priapism can occur (145). There is a lack of objective and
definitive diagnostic criteria for leukostasis. The absolute number
of WBC alone is not a criterion; it must be interpreted in the
context of the underlying malignancy. Chest X-rays or CT are not of
much help; they correlate poorly to the clinical status. Cranial CT
should be performed when CNS symptoms arise to exclude hemorrhage
and evaluated alongside echocardiography, as this condition also
heavily affects the right ventricle function (145).
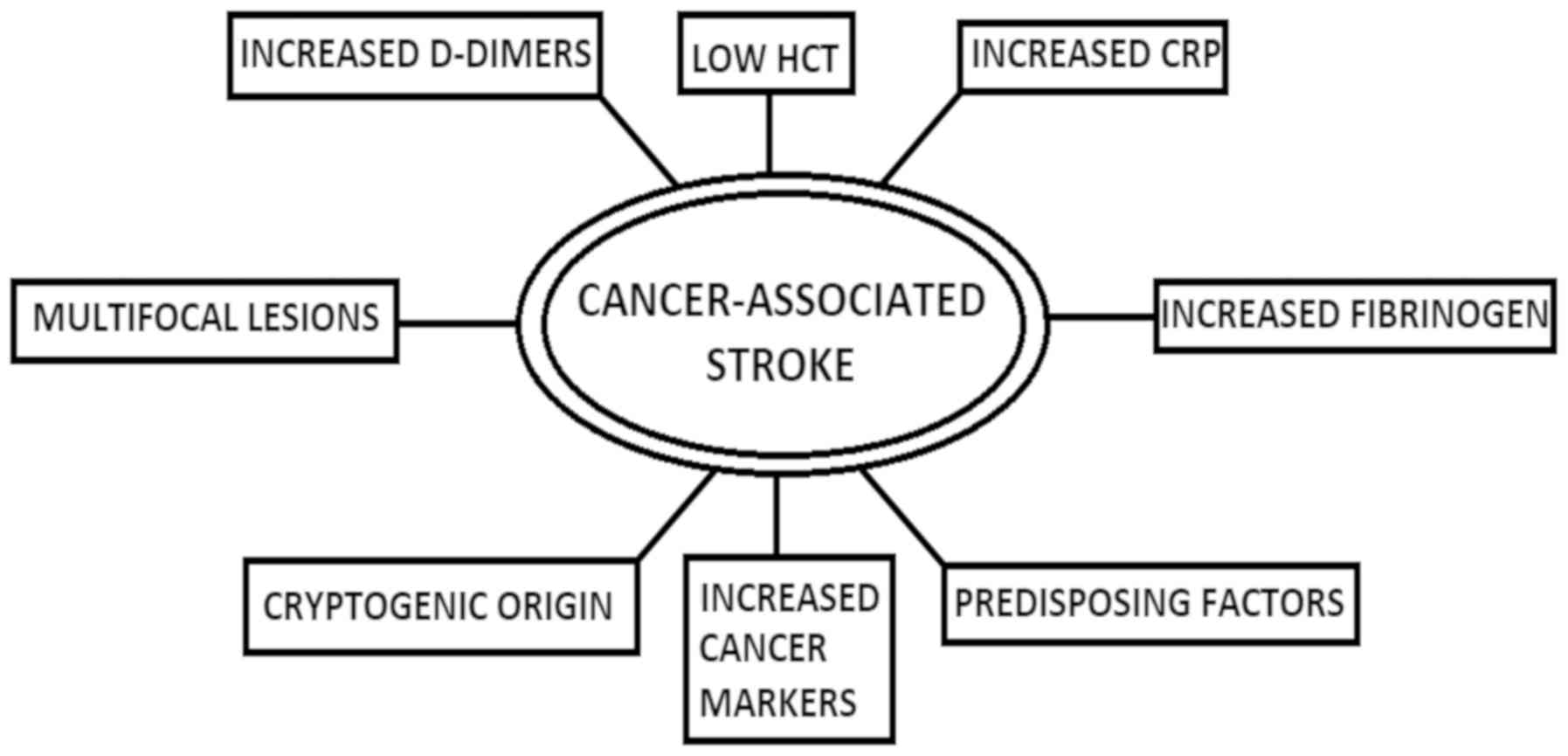
6. Detection of a cancer-associated
stroke
A concise presentation of the elements that hint
towards the presence of a cancer-associated stroke is shown in
Fig. 2. D-Dimers have gained
significant ground in publications over the detection of a
cancer-related stroke. In a 2014 study, patients with active cancer
and ischemic stroke tended to demonstrate higher CRP and D-dimers,
more frequent cryptogenic strokes and patterns of multiple lesions,
and among those patients, higher CRP and D-dimer levels were
associated with a cryptogenic mechanism and multiple lesion
patterns (17). In agreement with
that study, Xie et al analyzed data from patients with lung
cancer and came to the conclusion that high D-Dimers, alongside
CA125 and CA199, were independent risk factors for
lung-cancer-associated stroke (146). In a different study, lung cancer
was also associated with high CRP levels (7). High CRP and high fibrinogen have also
been found in patients with occult malignancy that presented with a
stroke. More specifically, Cocho et al (2015) reported that
levels of CRP >20 mg/l had a sensitivity of 75% and a
specificity of 96%, whereas fibrinogen levels >600 mg/dl had a
sensitivity of 67% and a specificity of 91% for occult malignancy
presenting with a stroke. Therefore, it was suggested that
screening be carried out in cancer patients exhibiting elevated
levels of these two markers, particularly when the etiology of the
stroke is unknown (28).
Karlińska et al (2015) also noted that
patients with stroke with an active cancer tended to present lower
hematocrit levels, higher serum CRP levels, and a higher
erythrocyte sedimentation rate when compared to cancer-free stroke
patients (27). Several other
studies have also reported elevated D-Dimers levels in cancer
patients (7,19,146,147). Taking into consideration the
significance D-Dimers seem to have in the diagnosis of
cancer-related stroke, Guo et al (2014) used D-Dimers of
≥0.55 mg/l, and multiple territory infarctions, as criteria for the
development of a clinically meaningful test for cancer-associated
stroke. The specificity and positive predictive value (PPV) for
cancer-related stroke were 99.7 and 92.9%, respectively. When the
cut-off D-Dimers value was set at ≥5.5 mg/l, the test had a high
specificity and PPV regardless of the imaging results (148).
Nonetheless, the question of when a stroke patient
should be screened for cancer remains. Selvik et al (2015)
claimed that routine investigation for cancer was not justified in
acute ischemic stroke (7).
However, a number of studies have corroborate that systemic cancer
workup should be considered in patients in whom stroke origin is
unclear, who have an early vascular recurrence, predisposing
factors for cancer, such as smoking, high D-Dimers, fibrinogen and
CRP levels (7,28,146). Xie et al suggested that
patients with cryptogenic stroke and high plasma levels of CA125
and CA199 should also be investigated to rule out lung cancer
(146). Regardless, stroke as the
first manifestation of an underlying malignancy is mostly secondary
to specific cancer-related causes (5). In a recent publication, Selvik et
al (2018) developed a predictive score for clinical use, in
order to uncover an underlying malignancy. The score consists of
three elements, and when a patient fulfills one, it counts as one
point. Specifically, D-dimers ≥3 mg/l, Hb ≤12.0 g/dl and an active
smoking or history of smoking give one point each. When a patient
fulfills all 3 score points, the probability of active cancer is
53%, and the overall test gave an area under the curve (AUC) of 73%
for patients younger than 75 years of age (149).
As regards neuroimaging findings, cancer patients
with stroke mostly have multiple lesions in multiple vascular
territories (1,61,150), a finding that has been used in
developing clinical tests, as previously mentioned. Summarizing,
neuroimaging studies, measurement of coagulation function, and
echocardiography are the most useful modalities to identify the
stroke (23,31). In general, cancer-associated
ischemic stroke is widely associated with lesions in multiple
vascular territories (1,61,150), elevated D-dimers and fibrin
degradation products (7,17,19,27,146,147,149,150), cancer markers (146) and proinflammatory components such
as low hematocrit and high CRP levels (7,27,28,149). It is up to the experience of the
doctor to assess the patient using the aforementioned tools, when a
high level of clinical suspicion is present; consequently,
vigilance is essential. Several methods are currently being
investigated to help the clinician to diagnose such a case, and
they may be applied to every-day clinical practice in the near
future.
7. Management
The clinical management and care of cancer patients
with stroke differs from that of patients with stroke alone
(3). The stroke extent depends on
the activity and the severity of the cancer (17), and cancer patients have an inferior
neurological condition at discharge and a tendency towards a longer
stay in the stroke unit (15). The
survival rate of patients hospitalized with cerebral infarction is
worse in cancer patients than in those without cancer, and the
outcome is poorer, and associated with both the severity of
neurological disability and the tumor stage (1,10,25,73).
CVD in cancer patients is often aggressive, with a tendency to
provoke recurrent events and rapid neurological devastation
(62). Thus, adequate therapy in
cancer patients with stroke may ameliorate the symptoms or prevent
further episodes (56,151). The management of specific
occurrences in cancer patients is presented in Table II.
| Table IIManagement of specific occurrences in
patients with cancer-associated stroke. |
Table II
Management of specific occurrences in
patients with cancer-associated stroke.
| Occurrence | Indicated
treatment |
|---|
| Ischemic
strokea | rTPA/IV
thrombolysis |
| Brain
hemorrhage | Evacuation,
antineoplastic treatment |
| Vasogenic
edema | Corticosteroids,
tumor resection |
| Cerebral vein
thrombosis | Observation,
anticoagulation, mechanical clot thrombectomy, fibrinolytic or
endovascular therapy |
| Acute venous
thromboembolism | LMWH |
| Tumor-related
venous occlusion | Brain radiation,
chemotherapy, tumor resection |
| Leptomeningeal
metastases | Irradiation,
surgical extirpation, chemotherapy |
| Intravascular
lymphomatosis | Chemotherapy |
| NBTE | Heparin, valvular
repair or replacement |
| DIC |
Categorizationb, platelet transfusion, fresh-frozen
plasma, cryoprecipitate or fibrinogen concentrate
administrationc, heparin or
LMWHd |
Acute stroke in patients with cancer can be treated
with recombinant tissue plasminogen activator (rTPA), and the
active cancer should not be seen as an absolute contraindication to
rTPA use (27,151,152). Clinical experience and
small-scale trials, such as the one published by Cappellari et
al (2013) have revealed that intravenous thrombolysis is not
associated with a higher risk of hemorrhage in cancer patients, but
rather improves the neurological state of such patients (151). The same findings were reported in
an analysis by Sobolewski et al (2015) on intravenous
thrombolysis, showing no impact of neoplastic disease on
unfavorable outcomes (153).
Murthy et al (2013) reported that of the
32,576 stroke cases treated with thrombolysis, the
cancer-associated stroke cases had significantly higher comorbidity
indices, although there was no difference in the rates of home
discharge and in-hospital mortality, after adjusting for
confounders. Additionally, subgroup analysis revealed that compared
with liquid cancers, patients with solid tumors had lower home
discharge rates and higher in-hospital mortality. Metastatic
cancers had the poorest outcomes, but the intracerebral hemorrhage
rates were similar, implying that even in patients with metastatic
cancer, thrombolysis remains the main therapeutic option (77). Thrombolysis is also considered safe
for patients with primary brain tumors. Analysis did show that
malignant brain tumors were tied to higher in-hospital mortality
rate, lower home discharge and an overall increased risk of ICH,
particularly when they had an intraparenchymal location, but
thrombolysis did not present an additional risk for of ICH
(154).
As for brain hemorrhage, the hemorrhage may require
evacuation alongside with the additional antineoplastic treatment
(56). The management of acute ICH
in patients with cancer should conform to established guidelines
for IPH, SAH, SDH, and EDH and in ITH, steroids could also be used
to decrease mass effect from vasogenic edema, while the underlying
tumor should further be considered for resection if surgically
feasible (42).
For CVT, in some cases, observation alone may be
adequate. Treatment with anticoagulation agents has been shown to
be safe and may be beneficial in reducing mortality and long-term
morbidity (33). As regards
safety, anticoagulation agents could be administered even in the
presence of a hematoma (33,155). Mechanical clot thrombectomy has
also been proven safe and effective (156); fibrinolytic or endovascular
therapy may even prove life-saving in critically ill patients
(33). Low-molecular-weight
heparins (LMWHs) constitute the current treatment of choice for
cancer-associated acute venous thromboembolism (157,158), although the evidence to support
the superiority of heparin or LMWHs is still insufficient (33). The addition of aspirin or steroids
is not recommended (33).
The treatment of tumor-related venous occlusion is
typically brain radiation or chemotherapy, depending on the tumor
type. Venous flow can be restored if therapy effectively treats the
underlying tumor, and tumor resection, chemotherapy or radiation
may be indicated for some large skull or dural tumors obstructing
the sinus (4,159).
Concerning leptomeningeal metastases, preferred
treatments for select patients encompass irradiation, alongside
surgical extirpation and chemotherapy. The radiotherapy is
administered to the involved disease sites, while chemotherapy can
be intra-CSF and systematic (29).
The prognosis of intravascular lymphomatosis (IVL)
is poor (37,38); CNS IVL in particular has a very
poor survival rate when compared to non-CNS or skin IVL and the
highest postmortem diagnosis rate (38); however, IVL is sensitive to
systematic chemotherapy (38).
The current therapy for NBTE focuses on treating
the underlying disease while managing the risk for systemic
embolization (23,61). Anticoagulation is crucial for
preventing recurrent embolization and the American College of Chest
Physician Guidelines recommend long-term anticoagulation,
regardless of the evidence of emboli (61). Unfractionated heparin decreases the
occurrence of thromboembolic events, particularly in patients with
malignancy, and consequently, the rates of ischemic stroke,
something that cannot be said about warfarin, which is not
recommended (23,61). Valvular repair or replacement has
an indication in patients with severe dysfunction, large
vegetations, recurrent embolism and no response to anticoagulation
treatment, which should be explored prior to reaching a surgical
decision. In any case, the clinician should weigh the benefits and
risks, as the surgical mortality rate for these patients is high
(61).
The management of DIC is a complex matter and
should be individualized according to the clinical setting
(55,56). Recent guidance for cancer patients
suggests, as a first step, the categorization of DIC into
procoagulant, hyperfibrinolytic and subclinical. In general,
appropriate management of the underlying malignancy remains key in
its treatment. Specifically for DIC, platelet transfusions are
recommended for a high risk of bleeding or active bleeding, which
may also be further treated with the administration of fresh-frozen
plasma, cryoprecipitate or fibrinogen concentrate. For the
inhibition of the excess thrombin effects, heparin or LMWHs can be
used as prophylactic therapy when no contraindications, such as low
platelet count or active bleeding, are present. Subclinical types
may also benefit from this prophylaxis, but it is not recommended
for hyperfibrinolytic DIC (55).
The new oral anticoagulants (NOAGs) are nowadays
considered an attractive option for coagulation prophylaxis and
treatment; thus, discussing the efficiency of NOAGs in a cancer
setting is appropriate. In a recent meta-analysis for the use of
NOAGs in treating acute venous thromboembolism, NOAGs have been
shown to have the same efficacy as Vitamin K antagonists in cancer
patients and share many of the advantages of LMWHs, such as the
short half-life (157).
Accordingly, the safety of these drugs may also be considered in
cancer patients with stroke. Furthermore, anticoagulants
(enoxaparin) did not seem to aggravate the risk of ICH in patients
with metastatic brain cancer, and did not pose an additional risk
to patients with cancers that inherently present a higher risk for
ICH, such as melanoma (21).
In conclusion, the clinician should carefully
evaluate the risks and benefits of prescribing an oral
anticoagulant to a patient with active malignancy. Further studies
on their safety and efficacy on cancer patients are still required
(160). Since they have not been
compared directly to LMWHs, van Es and Büller (2015) suggested
refraining from administering oral anticoagulants to cancer
patients, though it may indeed be a good solution for patients not
willing to endure constant injections (161). However, it must be said, that
atrial fibrillation should still be considered over the
cancer-induced hypercoagulability in patients with embolic
appearing strokes, and, if discovered, anticoagulation should be
initiated (26).
Finally, for carotid stenosis following RT,
although there is a lack of large-scale studies, available
literature to date estimates that revascularization surgery does
not present a larger peri-operative risk than in regular
angioplasty procedures (56,162).
8. Prevention
Stroke is a serious condition that majorly impacts
the prognosis in every patient, and particularly that of cancer
patients. Therefore, measures to prevent it should be seriously
considered. Furthermore, protective measures can also be taken in
several conditions that are involved in a cancer-associated stroke.
Firstly, cancer patients still present the same predisposing
factors (high blood pressure, hyperlipidemia, diabetes mellitus,
atrial fibrillation, carotid disease, smoking) with the rest of the
population, so regulating those first and foremost is crucial
(26). Secondly, cancer is
generally accompanied by various complications that derive from the
hypercoagulable state it creates. Thus, clinicians may need to
administer anticoagulant treatment and the NOAGs are, as previously
mentioned, an attractive option; per os consumption
facilitates patient compliance and they offer a wide therapeutic
window, requiring no laboratory monitoring (160,161). However, some concern is raised
due to their possible interaction with several chemotherapeutic
agents and drugs used for supportive care through the CYP3A4 enzyme
and/or P-glycoprotein transporter, and their possibly-impaired
absorption in vomiting patients and patients with
chemotherapy-induced intestinal mucosal defects (157,160,161). Further caution is advised in
cases of renal insufficiency that can occur in cancer patients, as
serious and fatal bleeding complications can emerge in that setting
(160). Another considerable
drawback remains the lack of efficient measures to promptly reverse
their anticoagulant activity in cases of overdose, bleeding, or
other urgent indication for reversal (160).
Young adult pediatric cancer survivors have an
increased stroke risk that is associated with cervical RT in a
dose-dependent manner (103),
implying that the lower the RT dose is, the lower the stroke risk
becomes. Limiting neck radiation, wherever possible, in lymphoma
patients, should consequently be considered (94). Routine duplex ultrasound screening
is indicated for patients who had received RT to the head and neck
(95). Fludeoxyglucose
(18F) (18-FDG) positron emission tomography (PET)/CT
successfully identified patients at risk for future vascular events
in an otherwise asymptomatic cohort with neoplastic disease
(163), so it could also be used
to pinpoint the patients more prone towards stroke.
Concerning chemotherapy, agents that have
anti-estrogenic effects, such as most endocrine therapies for
breast cancer, may also increase the risk of CVD. Long-term
adjuvant anastrozole treatment may result in significantly fewer
thromboembolic cases and CVE when compared to tamoxifen (74). For chemotherapy-induced
thrombocytopenia, which may predispose to hemorrhage, a delay in
administration or a dose reduction of the chemotherapeutic drugs is
usually the method of choice (54). With the exception of myeloablative
therapy in hematologic malignancies, chemotherapy for
non-hematologic ones rarely requires platelet transfusion support
(54). An additional interesting
finding to be mentioned is that paclitaxel presented a
platelet-sparing effect in ovarian cancer patients that were
treated with platinum regimens. In these patients, dose-dense
carboplatin regimens were given as to overcome platinum resistance,
but it led to high-grade thrombocytopenia (54).
9. Conclusions
Vigilance for stroke and CVD is always required in
patients with cancer. CVD in cancer patients is often aggressive,
with a tendency to provoke recurrent events and rapid neurological
devastation; therefore, a prompt and accurate diagnosis is crucial.
The vascular events in cancer patients can derive from a plethora
of mechanisms that differ from non-cancer ones and include, among
others, direct tumor effects, hypercoagulability, infections and
the effects of the cancer-treatment, chemo- and radiotherapy.
Cancers with the highest incidences of stroke are
lung, pancreatic, colorectal, breast and prostate. Though not as
frequent but dangerous when it comes to strokes, are renal-cell
carcinomas and melanomas, especially concerning hemorrhages.
The diagnosis of stroke and stroke-related
situations entails several laboratory and imaging tests, following
the clinician's suspicion based on the clinical presentation and
patient history. Thus, when it comes to detecting a
cancer-associated stroke, it is crucial that suspicion first
arises. Cancer-associated ischemic strokes tend to be more
multifocal and have consistently been tied to high D-Dimer plasma
levels, and various other markers, such as CRP and fibrin
degradation products. They are also associated with multifocal
lesions in neuroimaging. As new data become available, more
clinical tests and criteria for detecting these particular strokes
are being developed.
The management of acute ischemic stroke has not
been shown to differ largely in cancer and non-cancer patients;
cancer should not be considered an absolute contraindication for
intravenous thrombolysis. When it comes to prevention, the
clinician should weigh the benefits and risks of an anticoagulation
treatment plan and proceed with caution in administering it. So
far, LMWHs remain the first choice.
In conclusion, cancer-associated stroke should be
seriously evaluated. Clinicians should be aware of the risk, and
upon development, able to face it efficiently, particularly when it
complicates or occurs in the course of a malignancy, as these
patients have been shown to have the worst clinical outcomes.
Funding
MA was supported by the National Institute of
Health (NIH) R01 ES10563, R01 ES07331 and R01 ES020852. This study
was also supported by the Special Research Account of University of
Crete (ELKE nos. 4602, 4920 and 3963) and ToxPlus S.A.
Availability of data and materials
Not applicable.
Authors' contributions
ED, AMA, SM, VS, DAS, PDM and AT were involved in
the conception of the study. ED, AMA, SM, VS, KT, GT, ML, APK, AGB,
MA, IL, DPB, DAS, PDM and AT were involved in the acquisition of
the data and the study design, and were involved in the writing of
the article and critically revised the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
DAS is the Editor-in-Chief for the journal, but had
no personal involvement in the reviewing process, or any influence
in terms of adjudicating on the final decision, for this
article.
Acknowledgments
Not applicable.
Abbreviations:
|
ADT
|
androgen deprivation therapy
|
|
ALL
|
acute lymphoblastic leukemia
|
|
AML
|
acute myeloid leukaemia
|
|
AUC
|
area under the curve
|
|
BSI
|
bloodstream infection
|
|
CLL
|
chronic lymphoblastic leukemia
|
|
CMV
|
cytomegalovirus
|
|
CNS
|
central nervous system
|
|
CRP
|
C-reactive protein
|
|
CSF
|
cerebrospinal fluid
|
|
CSFs
|
colony-stimulating factors
|
|
CT
|
computer-assisted tomography
|
|
CVD
|
cerebrovascular disease
|
|
CVE
|
cerebrovascular event
|
|
CVT
|
cerebrovascular thrombosis
|
|
DIC
|
disseminated intravascular
coagulation
|
|
EDH
|
epidural hemorrhage
|
|
ESAs
|
erythropoiesis-stimulating agents
|
|
18-FDG
|
fludeoxyglucose (18F)
|
|
GVHD
|
graft-versus-host disease
|
|
HGFs
|
hematopoietic growth factors
|
|
HSCT
|
hematopoietic stem cell
transplantation
|
|
HSV
|
herpes simplex virus
|
|
HUS
|
hemolytic uremic syndrome
|
|
ICH
|
intracranial hemorrhage
|
|
ICP
|
intracranial pressure
|
|
IPH
|
intraparenchymal hemorrhage
|
|
ITH
|
intratumoral hemorrhage
|
|
IVL
|
intravascular lymphomatosis
|
|
LDH
|
lactate dehydrogenase
|
|
LMWHs
|
low-molecular-weight heparins
|
|
MDS
|
myelodysplastic syndrome
|
|
MRI
|
magnetic resonance imaging
|
|
MTX
|
methotrexate
|
|
NBTE
|
non-bacterial thrombotic
endocarditis
|
|
NC
|
neoadjuvant chemotherapy
|
|
NCI
|
National Cancer Institute
|
|
NK
|
natural killer
|
|
NOAGs
|
new oral anticoagulants
|
|
PET
|
positron emission tomography
|
|
PPV
|
positive predictive value
|
|
RR
|
relative risk
|
|
RT
|
radiation therapy
|
|
rTPA
|
recombinant tissue plasminogen
activator
|
|
SAH
|
subarachnoid hemorrhage
|
|
SDH
|
subdural hemorrhage
|
|
SVT
|
sinovenous thrombosis
|
|
TB
|
tuberculosis
|
|
TIA
|
transient ischemic attack
|
|
TTP
|
thrombotic thrombopenic purpura
|
|
VTE
|
venous thromboembolism
|
References
|
1
|
Kneihsl M, Enzinger C, Wünsch G, Khalil M,
Culea V, Urbanic-Purkart T, Payer F, Niederkorn K, Fazekas F and
Gattringer T: Poor short-term outcome in patients with ischaemic
stroke and active cancer. J Neurol. 263:150–156. 2016. View Article : Google Scholar
|
|
2
|
Newton HB: Neurologic complications of
systemic cancer. Am Fam Physician. 59:878–886. 1999.PubMed/NCBI
|
|
3
|
Arboix A: Cerebrovascular disease in the
cancer patient. Rev Neurol. 31:1250–1252. 2000.In Spanish.
|
|
4
|
Grisold W, Oberndorfer S and Struhal W:
Stroke and cancer: A review. Acta Neurol Scand. 119:1–16. 2009.
View Article : Google Scholar
|
|
5
|
Taccone FS, Jeangette SM and Blecic SA:
First-ever stroke as initial presentation of systemic cancer. J
Stroke Cerebrovasc Dis. 17:169–174. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Selvik HA, Thomassen L, Logallo N and Næss
H: Prior cancer in patients with ischemic stroke: The Bergen
NORSTROKE study. J Stroke Cerebrovasc Dis. 23:919–925. 2014.
View Article : Google Scholar
|
|
7
|
Selvik HA, Thomassen L, Bjerkreim AT and
Næss H: Cancer-Associated Stroke: The Bergen NORSTROKE Study.
Cerebrovasc Dis Extra. 5:107–113. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sanossian N, Djabiras C, Mack WJ and
Ovbiagele B: Trends in cancer diagnoses among inpatients
hospitalized with stroke. J Stroke Cerebrovasc Dis. 22:1146–1150.
2013. View Article : Google Scholar
|
|
9
|
Cestari DM, Weine DM, Panageas KS, Segal
AZ and DeAngelis LM: Stroke in patients with cancer: Incidence and
etiology. Neurology. 62:2025–2030. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zhang YY, Chan DK, Cordato D, Shen Q and
Sheng AZ: Stroke risk factor, pattern and outcome in patients with
cancer. Acta Neurol Scand. 114:378–383. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Graus F, Rogers LR and Posner JB:
Cerebrovascular complications in patients with cancer. Medicine
(Baltimore). 64:16–35. 1985. View Article : Google Scholar
|
|
12
|
De Bruin ML, Dorresteijn LD, van't Veer
MB, Krol AD, van der Pal HJ, Kappelle AC, Boogerd W, Aleman BM and
van Leeuwen FE: Increased risk of stroke and transient ischemic
attack in 5-year survivors of Hodgkin lymphoma. J Natl Cancer Inst.
101:928–937. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Lindvig K, Møller H, Mosbech J and Jensen
OM: The pattern of cancer in a large cohort of stroke patients. Int
J Epidemiol. 19:498–504. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bowers DC, McNeil DE, Liu Y, Yasui Y,
Stovall M, Gurney JG, Hudson MM, Donaldson SS, Packer RJ, Mitby PA,
et al: Stroke as a late treatment effect of Hodgkin's Disease: A
report from the Childhood Cancer Survivor Study. J Clin Oncol.
23:6508–6515. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Stefan O, Vera N, Otto B, Heinz L and
Wolfgang G: Stroke in cancer patients: A risk factor analysis. J
Neurooncol. 94:221–226. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zöller B, Ji J, Sundquist J and Sundquist
K: Risk of haemorrhagic and ischaemic stroke in patients with
cancer: A nationwide follow-up study from Sweden. Eur J Cancer.
48:1875–1883. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lee EJ, Nah HW, Kwon JY, Kang DW, Kwon SU
and Kim JS: Ischemic stroke in patients with cancer: Is it
different from usual strokes? Int J Stroke. 9:406–412. 2014.
View Article : Google Scholar
|
|
18
|
Sheng B, Fong MK, Chu YP, Cheong AP, Teng
SK, Chu JP, Yip WM and Chow DH: Stroke and cancer: Misfortunes
never come singularly. Int J Stroke. 8:E302013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Carrilho Romeiro A, Valadas A and Marques
J: Acute ischemic stroke on cancer patients, a distinct etiology? A
case-control study. Acta Med Port. 28:613–618. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Katz JM and Segal AZ: Incidence and
etiology of cerebro-vascular disease in patients with malignancy.
Curr Atheroscler Rep. 7:280–288. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Donato J, Campigotto F, Uhlmann EJ,
Coletti E, Neuberg D, Weber GM and Zwicker JI: Intracranial
hemorrhage in patients with brain metastases treated with
therapeutic enoxaparin: A matched cohort study. Blood. 126:494–499.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Rogers LR: Cerebrovascular complications
in cancer patients. Neurol Clin. 9:889–899. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Rogers LR: Cerebrovascular complications
in patients with cancer. Semin Neurol. 24:453–460. 2004. View Article : Google Scholar
|
|
24
|
Navi BB, Reiner AS, Kamel H, Iadecola C,
Elkind MS, Panageas KS and DeAngelis LM: Association between
incident cancer and subsequent stroke. Ann Neurol. 77:291–300.
2015. View Article : Google Scholar :
|
|
25
|
Aarnio K, Joensuu H, Haapaniemi E, Melkas
S, Kaste M, Tatlisumak T and Putaala J: Cancer in young adults with
ischemic stroke. Stroke. 46:1601–1606. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Dearborn JL, Urrutia VC and Zeiler SR:
Stroke and cancer: A complicated relationship. J Neurol Transl
Neurosci. 2:10392014.
|
|
27
|
Karlińska AG, Gromadzka G, Karliński MA
and Członkowska A: The activity of malignancy may determine stroke
pattern in cancer patients. J Stroke Cerebrovasc Dis. 24:778–783.
2015. View Article : Google Scholar
|
|
28
|
Cocho D, Gendre J, Boltes A, Espinosa J,
Ricciardi AC, Pons J, Jimenez M and Otermin P: Predictors of occult
cancer in acute ischemic stroke patients. J Stroke Cerebrovasc Dis.
24:1324–1328. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Chamberlain MC: Leptomeningeal metastasis.
Semin Neurol. 30:236–244. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Herman C, Kupsky WJ, Rogers L, Duman R and
Moore P: Leptomeningeal dissemination of malignant glioma
simulating cerebral vasculitis. Case report with angiographic and
pathological studies. Stroke. 26:2366–2370. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Raizer JJ and DeAngelis LM: Cerebral sinus
thrombosis diagnosed by MRI and MR venography in cancer patients.
Neurology. 54:1222–1226. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Klein P, Haley EC, Wooten GF and
VandenBerg SR: Focal cerebral infarctions associated with
perivascular tumor infiltrates in carcinomatous leptomeningeal
metastases. Arch Neurol. 46:1149–1152. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ichord R: Cerebral sinovenous thrombosis.
Front Pediatr. 5:1632017. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Ranta S, Tuckuviene R, Mäkipernaa A,
Albertsen BK, Frisk T, Tedgård U, Jónsson ÓG, Pruunsild K,
Gretenkort Andersson N, Winther Gunnes M, et al: Cerebral sinus
venous thromboses in children with acute lymphoblastic leukaemia -
a multicentre study from the Nordic Society of Paediatric
Haematology and Oncology. Br J Haematol. 168:547–552. 2015.
View Article : Google Scholar
|
|
35
|
Rogers LR: Cerebrovascular complications
in patients with cancer. Semin Neurol. 30:311–319. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Santoro N, Giordano P, Del Vecchio GC,
Guido G, Rizzari C, Varotto S, Masera G and De Mattia D: Ischemic
stroke in children treated for acute lymphoblastic leukemia: A
retrospective study. J Pediatr Hematol Oncol. 27:153–157. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Anghel G, Petrinato G, Severino A, Remotti
D, Insabato L, De Renzo A, Rotoli B and Majolino I: Intravascular
B-cell lymphoma: Report of two cases with different clinical
presentation but rapid central nervous system involvement. Leuk
Lymphoma. 44:1353–1359. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Fonkem E, Lok E, Robison D, Gautam S and
Wong ET: The natural history of intravascular lymphomatosis. Cancer
Med. 3:1010–1024. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Lefkovitz NW, Roessmann U and Kori SH:
Major cerebral infarction from tumor embolus. Stroke. 17:555–557.
1986. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Zheng Z, Guo G, Xu L, Lei L, Wei X and Pan
Y: Left atrial myxoma with versus without cerebral embolism: Length
of symptoms, morphologic characteristics, and outcomes. Tex Heart
Inst J. 41:592–595. 2014. View Article : Google Scholar
|
|
41
|
Murata J, Sawamura Y, Takahashi A, Abe H
and Saitoh H: Intracerebral hemorrhage caused by a neoplastic
aneurysm from small-cell lung carcinoma: Case report. Neurosurgery.
32:124–126. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Velander AJ, DeAngelis LM and Navi BB:
Intracranial hemorrhage in patients with cancer. Curr Atheroscler
Rep. 14:373–381. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Navi BB, Reichman JS, Berlin D, Reiner AS,
Panageas KS, Segal AZ and DeAngelis LM: Intracerebral and
subarachnoid hemorrhage in patients with cancer. Neurology.
74:494–501. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Lieu AS, Hwang SL, Howng SL and Chai CY:
Brain tumors with hemorrhage. J Formos Med Assoc. 98:365–367.
1999.PubMed/NCBI
|
|
45
|
Fukushima S, Terasaki M, Tajima Y and
Shigemori M: Granulocytic sarcoma: An unusual complication of acute
promyelocytic leukemia causing cerebellar hemorrhage. Case report J
Neurosurg. 105:912–915. 2006.
|
|
46
|
Reichman J, Singer S, Navi B, Reiner A,
Panageas K, Gutin PH and Deangelis LM: Subdural hematoma in
patients with cancer. Neurosurgery. 71:74–79. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
McIver JI, Scheithauer BW, Rydberg CH and
Atkinson JL: Metastatic hepatocellular carcinoma presenting as
epidural hematoma: Case report. Neurosurgery. 49:447–449.
2001.PubMed/NCBI
|
|
48
|
Würthner JU, Köhler G, Behringer D,
Lindemann A, Mertelsmann R and Lübbert M: Leukostasis followed by
hemorrhage complicating the initiation of chemotherapy in patients
with acute myeloid leukemia and hyperleukocytosis: A
clinicopathologic report of four cases. Cancer. 85:368–374. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Shiber JR and Fines RE: Cerebral
hemorrhage due to hyperleukocytosis. J Emerg Med. 40:674–677. 2011.
View Article : Google Scholar
|
|
50
|
Nowacki P, Fryze C, Zdziarska B, Zyluk B,
Grzelec H and Dudzik T: Central nervous system leukostasis in
patients with leukemias and lymphomas. Folia Neuropathol. 33:59–65.
1995.PubMed/NCBI
|
|
51
|
Collins RC, Al-Mondhiry H, Chernik NL and
Posner JB: Neurologic manifestations of intravascular coagulation
in patients with cancer. A clinicopathologic analysis of 12 cases.
Neurology. 25:795–806. 1975. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Schwarzbach CJ, Schaefer A, Ebert A, Held
V, Bolognese M, Kablau M, Hennerici MG and Fatar M: Stroke and
cancer: The importance of cancer-associated hypercoagulation as a
possible stroke etiology. Stroke. 43:3029–3034. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Lee AY: Cancer and thromboembolic disease:
Pathogenic mechanisms. Cancer Treat Rev. 28:137–140. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Liebman HA: Thrombocytopenia in cancer
patients. Thromb Res. 133(Suppl 2): S63–S69. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Thachil J, Falanga A, Levi M, Liebman H
and Di Nisio M: Scientific and Standardization Committee of the
International Society on Thrombosis and Hemostasis: Management of
cancer-associated disseminated intravascular coagulation: Guidance
from the SSC of the ISTH. J Thromb Haemost. 13:671–675. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Rogers LR: Cerebrovascular complications
in cancer patients. Neurol Clin. 21:167–192. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Nguyen T and DeAngelis LM: Stroke in
cancer patients. Curr Neurol Neurosci Rep. 6:187–192. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Yagi T, Takahashi K, Tanikawa M, Seki M,
Abe T and Suzuki N: Fatal intracranial hemorrhage after intravenous
thrombolytic therapy for acute ischemic stroke associated with
cancer-related nonbacterial thrombotic endocarditis. J Stroke
Cerebrovasc Dis. 23:e413–e416. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Rogers LR, Cho ES, Kempin S and Posner JB:
Cerebral infarction from non-bacterial thrombotic endocarditis.
Clinical and pathological study including the effects of
anticoagulation. Am J Med. 83:746–756. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Reisner SA, Brenner B, Haim N, Edoute Y
and Markiewicz W: Echocardiography in nonbacterial thrombotic
endocarditis: From autopsy to clinical entity. J Am Soc
Echocardiogr. 13:876–881. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Liu J and Frishman WH: Nonbacterial
Thrombotic Endocarditis: Pathogenesis, Diagnosis, and Management.
Cardiol Rev. 24:244–247. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Royter V and Cohen SN: Recurrent embolic
strokes and cardiac valvular disease in a patient with non-small
cell adenocarcinoma of lung. J Neurol Sci. 241:99–101. 2006.
View Article : Google Scholar
|
|
63
|
Lopez JA, Ross RS, Fishbein MC and Siegel
RJ: Nonbacterial thrombotic endocarditis: A review. Am Heart J.
113:773–784. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Steiner I: Nonbacterial thrombotic
endocarditis - a study of 171 case reports. Cesk Patol. 29:58–60.
1993.PubMed/NCBI
|
|
65
|
Edoute Y, Haim N, Rinkevich D, Brenner B
and Reisner SA: Cardiac valvular vegetations in cancer patients: A
prospective echocardiographic study of 200 patients. Am J Med.
102:252–258. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Correale JD, Monteverde DA, Bueri JA,
Reich EG and Lucatelli N: Craniocerebral involvement in lymphoma.
Arq Neuropsiquiatr. 48:306–314. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Noje C, Cohen K and Jordan LC: Hemorrhagic
and ischemic stroke in children with cancer. Pediatr Neurol.
49:237–242. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Zembower TR: Epidemiology of infections in
cancer patients. Cancer Treat Res. 161:43–89. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Bos MM, Smeets LS, Dumay I and de Jonge E:
Bloodstream infections in patients with or without cancer in a
large community hospital. Infection. 41:949–958. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Fugate JE, Lyons JL, Thakur KT, Smith BR,
Hedley-Whyte ET and Mateen FJ: Infectious causes of stroke. Lancet
Infect Dis. 14:869–880. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Saynak M, Cosar-Alas R, Yurut-Caloglu V,
Caloglu M, Kocak Z and Uzal C: Chemotherapy and cerebrovascular
disease. J BUON. 13:31–36. 2008.PubMed/NCBI
|
|
72
|
Abt NB, Bydon M, De la Garza-Ramos R,
McGovern K, Olivi A, Huang J and Bydon A: Concurrent neoadjuvant
chemotherapy is an independent risk factor of stroke, all-cause
morbidity, and mortality in patients undergoing brain tumor
resection. J Clin Neurosci. 21:1895–1900. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Wall JG, Weiss RB, Norton L, Perloff M,
Rice MA, Korzun AH and Wood WC: Arterial thrombosis associated with
adjuvant chemotherapy for breast carcinoma: A Cancer and Leukemia
Group B Study. Am J Med. 87:501–504. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Esteva FJ and Hortobagyi GN: Comparative
assessment of lipid effects of endocrine therapy for breast cancer:
Implications for cardiovascular disease prevention in
postmenopausal women. Breast. 15:301–312. 2006. View Article : Google Scholar
|
|
75
|
Robinson D, Garmo H, Lindahl B, Van
Hemelrijck M, Adolfsson J, Bratt O, Holmberg L and Stattin P:
Ischemic heart disease and stroke before and during endocrine
treatment for prostate cancer in PCBaSe Sweden. Int J Cancer.
130:478–487. 2012. View Article : Google Scholar
|
|
76
|
Mosca L, Grady D, Barrett-Connor E,
Collins P, Wenger N, Abramson BL, Paganini-Hill A, Geiger MJ,
Dowsett SA, Amewou-Atisso M, et al: Effect of raloxifene on stroke
and venous thromboembolism according to subgroups in postmenopausal
women at increased risk of coronary heart disease. Stroke.
40:147–155. 2009. View Article : Google Scholar
|
|
77
|
Murthy SB, Karanth S, Shah S, Shastri A,
Rao CP, Bershad EM and Suarez JI: Thrombolysis for acute ischemic
stroke in patients with cancer: A population study. Stroke.
44:3573–3576. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Ligibel JA, James O'Malley A, Fisher M,
Daniel GW, Winer EP and Keating NL: Risk of myocardial infarction,
stroke, and fracture in a cohort of community-based breast cancer
patients. Breast Cancer Res Treat. 131:589–597. 2012. View Article : Google Scholar
|
|
79
|
Jagsi R, Griffith KA, Koelling T, Roberts
R and Pierce LJ: Stroke rates and risk factors in patients treated
with radiation therapy for early-stage breast cancer. J Clin Oncol.
24:2779–2785. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Rosell J, Nordenskjöld B, Bengtsson NO,
Fornander T, Hatschek T, Lindman H, Malmström PO, Wallgren A, Stål
O, et al: Time dependent effects of adjuvant tamoxifen therapy on
cerebrovascular disease: Results from a randomised trial. Br J
Cancer. 104:899–902. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Yang TL, Wu TC, Huang CC, Huang PH, Chung
CM, Lin SJ, Chen JW, Chan WL, Chiang CH and Leu HB: Association of
tamoxifen use and reduced cardiovascular events among asian females
with breast cancer. Circ J. 78:135–140. 2014. View Article : Google Scholar
|
|
82
|
Azoulay L, Yin H, Benayoun S, Renoux C,
Boivin JF and Suissa S: Androgen-deprivation therapy and the risk
of stroke in patients with prostate cancer. Eur Urol. 60:1244–1250.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Jespersen CG, Nørgaard M and Borre M:
Androgen-deprivation therapy in treatment of prostate cancer and
risk of myocardial infarction and stroke: A nationwide Danish
population-based cohort study. Eur Urol. 65:704–709. 2014.
View Article : Google Scholar
|
|
84
|
Chung SD, Chen YK, Wu FJ and Lin HC:
Hormone therapy for prostate cancer and the risk of stroke: A
5-year follow-up study. BJU Int. 109:1001–1005. 2012. View Article : Google Scholar
|
|
85
|
Meng F, Zhu S, Zhao J, Vados L, Wang L,
Zhao Y, Zhao D and Niu Y: Stroke related to androgen deprivation
therapy for prostate cancer: A meta-analysis and systematic review.
BMC Cancer. 16:1802016. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Gerl A: Vascular toxicity associated with
chemotherapy for testicular cancer. Anticancer Drugs. 5:607–614.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Kuan AS, Teng CJ, Wu HH, Su VY, Chen YT,
Chien SH, Yeh CM, Hu LY, Chen TJ, Tzeng CH, et al: Risk of ischemic
stroke in patients with ovarian cancer: A nationwide
population-based study. BMC Med. 12:532014. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Rollins N, Winick N, Bash R and Booth T:
Acute methotrexate neurotoxicity: Findings on diffusion-weighted
imaging and correlation with clinical outcome. AJNR Am J
Neuroradiol. 25:1688–1695. 2004.PubMed/NCBI
|
|
89
|
Jourdan E, Dombret H, Glaisner S, Micléa
JM, Castaigne S and Degos L: Unexpected high incidence of
intracranial subdural haematoma during intensive chemotherapy for
acute myeloid leukaemia with a monoblastic component. Br J
Haematol. 89:527–530. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Lee CW, Muo CH, Liang JA, Sung FC and Kao
CH: Association of intensive morphine treatment and increased
stroke incidence in prostate cancer patients: A population-based
nested case– control study. Jpn J Clin Oncol. 43:776–781. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Stewart FA, Hoving S and Russell NS:
Vascular damage as an underlying mechanism of cardiac and cerebral
toxicity in irradiated cancer patients. Radiat Res. 174:865–869.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Tsai SJ, Huang YS, Tung CH, Lee CC, Lee
MS, Chiou WY, Lin HY, Hsu FC, Tsai CH, Su YC, et al: Increased risk
of ischemic stroke in cervical cancer patients: A nationwide
population-based study. Radiat Oncol. 8:412013. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Santoro F, Tarantino N, Pellegrino PL,
Caivano M, Lopizzo A, Di Biase M and Brunetti ND: Cardiovascular
sequelae of radiation therapy. Clin Res Cardiol. 103:955–967. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Scott AS, Parr LA and Johnstone PA: Risk
of cerebrovascular events after neck and supraclavicular
radiotherapy: A systematic review. Radiother Oncol. 90:163–165.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Cheng SW, Wu LL, Ting AC, Lau H, Lam LK
and Wei WI: Irradiation-induced extracranial carotid stenosis in
patients with head and neck malignancies. Am J Surg. 178:323–328.
1999. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Elerding SC, Fernandez RN, Grotta JC,
Lindberg RD, Causay LC and McMurtrey MJ: Carotid artery disease
following external cervical irradiation. Ann Surg. 194:609–615.
1981. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Dorresteijn LD, Kappelle AC, Boogerd W,
Klokman WJ, Balm AJ, Keus RB, van Leeuwen FE and Bartelink H:
Increased risk of ischemic stroke after radiotherapy on the neck in
patients younger than 60 years. J Clin Oncol. 20:282–288. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Smith GL, Smith BD, Buchholz TA, Giordano
SH, Garden AS, Woodward WA, Krumholz HM, Weber RS, Ang KK and
Rosenthal DI: Cerebrovascular disease risk in older head and neck
cancer patients after radiotherapy. J Clin Oncol. 26:5119–5125.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Hung SK, Lee MS, Chiou WY, Lee CC, Chen
YC, Lai CL, Chien NC, Hsu WL, Liu DW, Su YC, et al: High incidence
of ischemic stroke occurrence in irradiated lung cancer patients: A
population-based surgical cohort study. PLoS One. 9:e943772014.
View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Woodward WA, Giordano SH, Duan Z,
Hortobagyi GN and Buchholz TA: Supraclavicular radiation for breast
cancer does not increase the 10-year risk of stroke. Cancer.
106:2556–2562. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Morris B, Partap S, Yeom K, Gibbs IC,
Fisher PG and King AA: Cerebrovascular disease in childhood cancer
survivors: A Children's Oncology Group Report. Neurology.
73:1906–1913. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Mueller S, Sear K, Hills NK, Chettout N,
Afghani S, Gastelum E, Haas-Kogan D and Fullerton HJ: Risk of first
and recurrent stroke in childhood cancer survivors treated with
cranial and cervical radiation therapy. Int J Radiat Oncol Biol
Phys. 86:643–648. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Mueller S, Fullerton HJ, Stratton K,
Leisenring W, Weathers RE, Stovall M, Armstrong GT, Goldsby RE,
Packer RJ, Sklar CA, et al: Radiation, atherosclerotic risk
factors, and stroke risk in survivors of pediatric cancer: A report
from the Childhood Cancer Survivor Study. Int J Radiat Oncol Biol
Phys. 86:649–655. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Ruggiu M, Cuccuini W, Mokhtari K, Meignin
V, Peffault de Latour R, Robin M, Fontbrune FS, Xhaard A, Socié G,
et al: Case report: Central nervous system involvement of human
graft versus host disease: Report of 7 cases and a review of
literature. Medicine (Baltimore). 96:e83032017. View Article : Google Scholar
|
|
105
|
Najima Y, Ohashi K, Miyazawa M, Nakano M,
Kobayashi T, Yamashita T, Akiyama H and Sakamaki H: Intracranial
hemorrhage following allogeneic hematopoietic stem cell
transplantation. Am J Hematol. 84:298–301. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Syed FI, Couriel DR, Frame D and
Srinivasan A: Central nervous system complications of hematopoietic
stem cell transplant. Hematol Oncol Clin North Am. 30:887–898.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Grauer O, Wolff D, Bertz H, Greinix H,
Kühl JS, Lawitschka A, Lee SJ, Pavletic SZ, Holler E and Kleiter I:
Neurological manifestations of chronic graft-versus-host disease
after allogeneic haematopoietic stem cell transplantation: Report
from the Consensus Conference on Clinical Practice in chronic
graft-versus-host disease. Brain. 133:2852–2865. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Saad AG, Alyea EP III, Wen PY, Degirolami
U and Kesari S: Graft-versus-host disease of the CNS after
allogeneic bone marrow transplantation. J Clin Oncol. 27:e147–e149.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
109
|
Maffini E, Festuccia M, Brunello L,
Boccadoro M, Giaccone L and Bruno B: Neurologic Complications after
Allogeneic Hematopoietic Stem Cell Transplantation. Biol Blood
Marrow Transplant. 23:388–397. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
110
|
Goddeau RP and Alhazzani A: Headache in
stroke: A review. Headache. 53:1019–1022. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Yew KS and Cheng EM: Diagnosis of acute
stroke. Am Fam Physician. 91:528–536. 2015.PubMed/NCBI
|
|
112
|
Leiva-Salinas C and Wintermark M: Imaging
of acute ischemic stroke. Neuroimaging Clin N Am. 20:455–468. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
113
|
Liu YC, Lin TA, Ko PS, Wang HY, Chien SH,
Liu CJ, Chiou TJ, Hsiao LT, Gau JP and Liu JH: Cerebrovascular
disease after allogeneic hematopoietic stem cell transplantation:
Incidence, manifestations, risk and clinical outcome. Blood.
130:4527. 2017.
|
|
114
|
Zhang XH, Wang QM, Chen H, Chen YH, Han W,
Wang FR, Wang JZ, Zhang YY, Mo XD, Chen Y, et al: Clinical
characteristics and risk factors of Intracranial hemorrhage in
patients following allogeneic hematopoietic stem cell
transplantation. Ann Hematol. 95:1637–1643. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Bennett CL, Djulbegovic B, Norris LB and
Armitage JO: Colony-stimulating factors for febrile neutropenia
during cancer therapy. N Engl J Med. 368:1131–1139. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
116
|
McCune JS, Sullivan SD, Blough DK, Clarke
L, McDermott C, Malin J and Ramsey S: Colony-stimulating factor use
and impact on febrile neutropenia among patients with newly
diagnosed breast, colorectal, or non-small cell lung cancer who
were receiving chemotherapy. Pharmacotherapy. 32:7–19. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Rizzo JD, Brouwers M, Hurley P, Seidenfeld
J, Somerfield MR and Temin S: American society of clinical
oncology/american society of hematology clinical practice guideline
update on the use of epoetin and darbepoetin in adult patients with
cancer. J Oncol Pract. 6:317–320. 2010. View Article : Google Scholar :
|
|
118
|
Kreys ED, Kim TY, Delgado A and Koeller
JM: Impact of cancer supportive care pathways compliance on
emergency department visits and hospitalizations. J Oncol Pract.
10:168–173. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
119
|
Poonawalla IB, Piller LB, Lairson DR, Chan
W and Du XL: Impact of hematopoietic growth factors on blood
transfusion needs, incidence of neutropenia, and overall survival
among elderly advanced ovarian cancer patients treated with
chemotherapy. Int J Gynecol Cancer. 26:95–103. 2016. View Article : Google Scholar
|
|
120
|
Du XL and Zhang Y: Risks of venous
thromboembolism, stroke, heart disease, and myelodysplastic
syndrome associated with hematopoietic growth factors in a large
population-based cohort of patients with colorectal cancer. Clin
Colorectal Cancer. 14:e21–e31. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
121
|
Du XL, Zhang Y and Hardy D: Associations
between hematopoietic growth factors and risks of venous
thromboembolism, stroke, ischemic heart disease and myelodysplastic
syndrome: Findings from a large population-based cohort of women
with breast cancer. Cancer Causes Control. 27:695–707. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
122
|
Puhalla S, Bhattacharya S and Davidson NE:
Hematopoietic growth factors: Personalization of risks and
benefits. Mol Oncol. 6:237–241. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
123
|
Calip GS, Malmgren JA, Lee WJ, Schwartz SM
and Kaplan HG: Myelodysplastic syndrome and acute myeloid leukemia
following adjuvant chemotherapy with and without granulocyte
colony-stimulating factors for breast cancer. Breast Cancer Res
Treat. 154:133–143. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
124
|
Rosenstock AS, Niu J, Giordano SH, Zhao H,
Wolff AC and Chavez-MacGregor M: Acute myeloid leukemia and
myelodysplastic syndrome after adjuvant chemotherapy: A
population-based study among older breast cancer patients. Cancer.
124:899–906. 2018. View Article : Google Scholar
|
|
125
|
Salamin O, Kuuranne T, Saugy M and
Leuenberger N: Erythropoietin as a performance-enhancing drug: Its
mechanistic basis, detection, and potential adverse effects. Mol
Cell Endocrinol. 464:75–87. 2018. View Article : Google Scholar
|
|
126
|
Bian J, Chen B, Hershman DL, Marks N,
Norris L, Schulz R and Bennett CL: Effects of the US food and drug
administration boxed warning of erythropoietin-stimulating agents
on utilization and adverse outcome. J Clin Oncol. 35:1945–1951.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
127
|
Hollingsworth K, Romney MC, Crawford A and
McAna J: The impact of the risk evaluation mitigation strategy for
erythropoiesis-stimulating agents on their use and the incidence of
stroke in medicare subjects with chemotherapy-induced anemia with
lung and/or breast cancers. Popul Health Manag. 19:63–69. 2016.
View Article : Google Scholar
|
|
128
|
Palmer SC, Saglimbene V, Mavridis D,
Salanti G, Craig JC, Tonelli M, Wiebe N and Strippoli GF:
Erythropoiesis-stimulating agents for anaemia in adults with
chronic kidney disease: A network meta-analysis. Cochrane Database
Syst Rev. CD0105902014.PubMed/NCBI
|
|
129
|
Seliger SL, Zhang AD, Weir MR, Walker L,
Hsu VD, Parsa A, Diamantidis CJ and Fink JC:
Erythropoiesis-stimulating agents increase the risk of acute stroke
in patients with chronic kidney disease. Kidney Int. 80:288–294.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
130
|
Szczech L: Chronic kidney disease:
Association between ESA use and stroke in patients with CKD. Nat
Rev Nephrol. 7:365–366. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
131
|
England TJ, Sprigg N, Alasheev AM, Belkin
AA, Kumar A, Prasad K and Bath PM: Granulocyte-Colony Stimulating
Factor (G-CSF) for stroke: An individual patient data
meta-analysis. Sci Rep. 6:365672016. View Article : Google Scholar : PubMed/NCBI
|
|
132
|
Fan ZZ, Cai HB, Ge ZM, Wang LQ, Zhang XD,
Li L and Zhai XB: The efficacy and safety of granulocyte
colony-Stimulating factor for patients with stroke. J Stroke
Cerebrovasc Dis. 24:1701–1708. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
133
|
Huang X, Liu Y, Bai S, Peng L, Zhang B and
Lu H: Granulocyte colony stimulating factor therapy for stroke: A
pairwise meta-analysis of randomized controlled trial. PLoS One.
12:e01757742017. View Article : Google Scholar : PubMed/NCBI
|
|
134
|
Jacob L and Kostev K: Cancer is associated
with intraoperative and postprocedural complications and disorders.
J Cancer Res Clin Oncol. 142:777–781. 2016. View Article : Google Scholar
|
|
135
|
Kamiya-Matsuoka C, Cachia D, Yust-Katz S,
Rodriguez YA, Garciarena P, Rodarte EM and Tremont-Lukats IW:
Anderson Cancer Center Ischemic stroke in patients with gliomas at
The University of Texas-M.D. J Neurooncol. 125:143–148. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
136
|
Chen CW, Cheng TJ, Ho CH, Wang JJ, Weng
SF, Hou YC, Cheng HC, Chio CC, Shan YS and Chang WT: Increased risk
of brain cancer incidence in stroke patients: A clinical case
series, population-based and longitudinal follow-up study.
Oncotarget. 8:108989–108999. 2017. View Article : Google Scholar
|
|
137
|
Sealy-Jefferson S, Cote ML, Chlebowski RT,
Rexrode KM and Simon MS: Post-stroke cancer risk among
postmenopausal women: The Women's Health Initiative. Womens Health
Issues. 28:29–34. 2018. View Article : Google Scholar
|
|
138
|
Del Ben M, Caporale A, Feole K, Alessandri
C and Angelico F: Intracranial hemorrage due to brain metastases in
an Italian HCV patient with hepatocellular carcinoma. J Exp Clin
Cancer Res. 22:641–644. 2003.
|
|
139
|
Ponzoni M, Ferreri AJ, Campo E, Facchetti
F, Mazzucchelli L, Yoshino T, Murase T, Pileri SA, Doglioni C,
Zucca E, et al: Definition, diagnosis, and management of
intravascular large B-cell lymphoma: Proposals and perspectives
from an international consensus meeting. J Clin Oncol.
25:3168–3173. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
140
|
Bal S, Menon B and Demchuk A: Relationship
of endocarditis, disseminated intravascular coagulation, and
embolic signals in cancer with stroke. Ann Neurol. 71:1462012.
View Article : Google Scholar : PubMed/NCBI
|
|
141
|
Reagan TJ and Okazaki H: The thrombotic
syndrome associated with carcinoma. A clinical and neuropathologic
study. Arch Neurol. 31:390–395. 1974. View Article : Google Scholar : PubMed/NCBI
|
|
142
|
el-Shami K, Griffiths E and Streiff M:
Nonbacterial thrombotic endocarditis in cancer patients:
Pathogenesis, diagnosis, and treatment. Oncologist. 12:518–523.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
143
|
Singhal AB, Topcuoglu MA and Buonanno FS:
Acute ischemic stroke patterns in infective and nonbacterial
thrombotic endocarditis: A diffusion-weighted magnetic resonance
imaging study. Stroke. 33:1267–1273. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
144
|
Angarone M: Fungal infections in cancer
patients. Cancer Treat Res. 161:129–155. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
145
|
Schellongowski P and Staudinger T:
Leukostasis and tumor lysis: Important complications of
hyperleukocytosis. Internist (Berl). 54:1051–1060. 2013.In German.
View Article : Google Scholar
|
|
146
|
Xie X, Chen L, Zeng J, Qin C, Cheng D, Wei
X and Liang Z: Clinical features and biological markers of lung
cancer-associated stroke. J Int Med Res. 44:1483–1491. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
147
|
Kono T, Ohtsuki T, Hosomi N, Takeda I,
Aoki S, Sueda Y, Ishihara K, Nakamura T, Yamawaki T and Matsumoto
M: Cancer-associated ischemic stroke is associated with elevated
D-dimer and fibrin degradation product levels in acute ischemic
stroke with advanced cancer. Geriatr Gerontol Int. 12:468–474.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
148
|
Guo YJ, Chang MH, Chen PL, Lee YS, Chang
YC and Liao YC: Predictive value of plasma (D)-dimer levels for
cancer-related stroke: A 3-year retrospective study. J Stroke
Cerebrovasc Dis. 23:e249–e254. 2014. View Article : Google Scholar
|
|
149
|
Selvik HA, Bjerkreim AT, Thomassen L,
Waje-Andreassen U, Naess H and Kvistad CE: When to Screen Ischaemic
Stroke Patients for Cancer. Cerebrovasc Dis. 45:42–47. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
150
|
Kim SJ, Park JH, Lee MJ, Park YG, Ahn MJ
and Bang OY: Clues to occult cancer in patients with ischemic
stroke. PLoS One. 7:e449592012. View Article : Google Scholar : PubMed/NCBI
|
|
151
|
Cappellari M, Carletti M, Micheletti N,
Tomelleri G, Ajena D, Moretto G and Bovi P: Intravenous alteplase
for acute ischemic stroke in patients with current malignant
neoplasm. J Neurol Sci. 325:100–102. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
152
|
Graber JJ, Nayak L and Deangelis LM: Use
of recombinant tissue plasminogen activator in cancer patients with
acute stroke. J Neurooncol. 107:571–573. 2012. View Article : Google Scholar
|
|
153
|
Sobolewski P, Brola W, Szczuchniak W,
Fudala M and Sobota A: Safety of intravenous thrombolysis for acute
ischaemic stroke including concomitant neoplastic disease sufferers
- experience from Poland. Int J Clin Pract. 69:666–673. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
154
|
Murthy SB, Moradiya Y, Shah S, Shastri A,
Bershad EM and Suarez JI: In-hospital outcomes of thrombolysis for
acute ischemic stroke in patients with primary brain tumors. J Clin
Neurosci. 22:474–478. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
155
|
Fink JN and McAuley DL: Safety of
anticoagulation for cerebral venous thrombosis associated with
intracerebral hematoma. Neurology. 57:1138–1139. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
156
|
Soleau SW, Schmidt R, Stevens S, Osborn A
and MacDonald JD: Extensive experience with dural sinus thrombosis.
Neurosurgery. 52:534–544. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
157
|
van der Hulle T, den Exter PL, Kooiman J,
van der Hoeven JJ, Huisman MV and Klok FA: Meta-analysis of the
efficacy and safety of new oral anticoagulants in patients with
cancer-associated acute venous thromboembolism. J Thromb Haemost.
12:1116–1120. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
158
|
Raskob GE, van Es N, Verhamme P, Carrier
M, Di Nisio M, Garcia D, Grosso MA, Kakkar AK, Kovacs MJ, Mercuri
MF, et al: Hokusai VTE Cancer Investigators: Edoxaban for the
Treatment of Cancer-Associated Venous Thromboembolism. N Engl J
Med. 378:615–624. 2018. View Article : Google Scholar
|
|
159
|
Matsumoto K, Ohta M and Takeshita I:
Reversible non-thrombotic occlusion of the superior sagittal sinus
caused by metastatic malignant lymphoma - case report. Neurol Med
Chir (Tokyo). 43:349–351. 2003. View Article : Google Scholar
|
|
160
|
Short NJ and Connors JM: New oral
anticoagulants and the cancer patient. Oncologist. 19:82–93. 2014.
View Article : Google Scholar :
|
|
161
|
van Es N and Büller HR: Using direct oral
anticoagulants (DOACs) in cancer and other high-risk populations.
Hematology Am Soc Hematol Educ Program. 2015:125–131. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
162
|
Magne JL, Pirvu A, Sessa C, Cochet E,
Blaise H and Ducos C: Carotid artery revascularisation following
neck irradiation: Immediate and long-term results. Eur J Vasc
Endovasc Surg. 43:4–7. 2012. View Article : Google Scholar
|
|
163
|
Rominger A, Saam T, Wolpers S, Cyran CC,
Schmidt M, Foerster S, Nikolaou K, Reiser MF, Bartenstein P and
Hacker M: 18F-FDG PET/CT identifies patients at risk for
future vascular events in an otherwise asymptomatic cohort with
neoplastic disease. J Nucl Med. 50:1611–1620. 2009. View Article : Google Scholar : PubMed/NCBI
|