Introduction
Recent estimates indicate that esophageal cancer
(EC) affects approximately half a million people worldwide, and its
incidence continues to increase (1,2).
Currently, EC is the eighth most common incident cancer in the
world and has been characterized by its poor survival rate
(3,4). Although esophageal carcinogenesis has
not been fully elucidated, EC is thought to result from complex
interactions between host and environmental elements (5).
While some risk factors for EC have already been
recognized, they may have some peculiarities depending on the major
subtype: Squamous cell carcinoma (ESCC) or adenocarcinoma (EAC).
More common in males than in females and among blacks than among
whites in the United States, ESCC has been consistently associated
with smoking and alcohol consumption. In contrast, EAC is 8-fold
more common among males and 5-fold more common in whites than in
blacks in the United States (6).
Although tobacco is also a known risk factor for EAC (7), chronic gastroesophageal reflux disease
(GERD) is believed to represent the most important underlying
mechanism, either directly or through the induction of a
preneoplastic lesion, which is known as Barrett's esophagus.
Notably, the increased incidence of GERD and Barrett's esophagus in
the last few decades has been correlated with an increased
incidence of EAC in the Western population (8,9). Obesity
has also been implicated in the increased risk for EAC (10,11),
either through the association with GERD or through inflammatory
mediators produced by adipocytes (6).
Although ESCC predominates worldwide, recent data
from Western European countries, the United States and Australia
point to a marked increase in the EAC subtype (2). In contrast, ESCC continues to represent
the most common type of EC in South America and in the ‘Asian
esophageal cancer belt’ (12).
Indeed, in some areas in China, the ESCC incidence reached more
than 100 cases per 100,000 person-years (13,14).
Further investigating the etiopathogenesis,
including the epigenetic modifications involved in esophageal
carcinogenesis (15,16), will be fundamental for explaining the
increase in EC (17) and for
unveiling underlying mechanisms that may impact future therapies
for EC. Meanwhile, understanding the epidemiology of EC will
hopefully be the key to elucidating risk factors and potential
causes and may become the cornerstone of preventive strategies.
Therefore, the aim of this study was to analyze the geographic
distributions and time trends of the EC incidence and lethality in
Brazil to identify areas with differential risks and outcomes of
EC.
Materials and methods
Data source
The study methods have been described in similar
previous studies from our group elsewhere (18,19).
Data from the Health Informatics Department of the Brazilian
Ministry of Health (DATASUS) (http://www2.datasus.gov.br/DATASUS) were
retrospectively searched for patients with the International
Statistical Classification of Diseases and Related Health Problems,
Tenth Revision code of EC (ICD-10 code: C15.0 to C15.9). This
population-based health and disease registry includes information
such as medical procedures, hospital admission and discharge,
mortality, and demographic data, covering approximately the entire
population. Hospital discharge records were used to estimate the EC
incidence. All data is anonymous archival data that does not allow
for the identification of individual subjects; therefore, the
requirement for ethical approval was waived. We assumed that
hospital-based procedures for either EC diagnosis or treatment
would reflect the actual disease numbers.
Study design, population, and
variables
We performed an ecological study using the DATASUS
registry and searched for the most recent and consistent
information containing complete data entries of hospitalizations
due to EC. Ecological studies allow geographic and temporal
analyses of risk factors potentially involved in the development of
diseases in a given population. We analyzed all cases from January
2005 to December 2015 for which a diagnosis of EC was assigned. The
period of study was defined according to the most consistent data
available in recent years. The data included the town of residence
during hospital admission and death, and patients were categorized
by gender and age; for the latter category, individuals were
stratified as <20 years, 20–49 years, 50–69 years, and >70
years of age. Standardized rates regarding the incidence (the rate
of new hospital admissions for EC) and lethality (the capacity of
EC to cause intra-hospital death) were estimated from
hospitalizations. For the geographic distribution analysis, EC
hospitalization rates were obtained per 100,000 inhabitants in the
individual municipalities.
Statistical analysis
Exploratory procedures with a quantitative approach
were applied to the data using IBM SPSS software for Windows
(Version 20, SPSS Inc.). Summary descriptive statistics and
graphical displays were generated by Tabwin 3.2 (Tab for Windows
3.2, free software that allows organization of multiple
applications into grouped tabs, available at http://www2.datasus.gov.br/DATASUS). EC
hospitalization rates were adjusted by the available hospital beds
in Brazil in the study period. Estimates of resident populations
were obtained from Instituto Brasileiro de Geografia e Estatística
(IBGE; Brazilian Institute of Geography and Statistics)
projections. Linear regression was applied to evaluate temporal
trends in the EC incidence and lethality by sex using Microsoft
Excel Software (Microsoft Excel for Mac 2011, Version 14.4.9, 2010;
Microsoft Corporation).
Results
Hospitalizations for EC
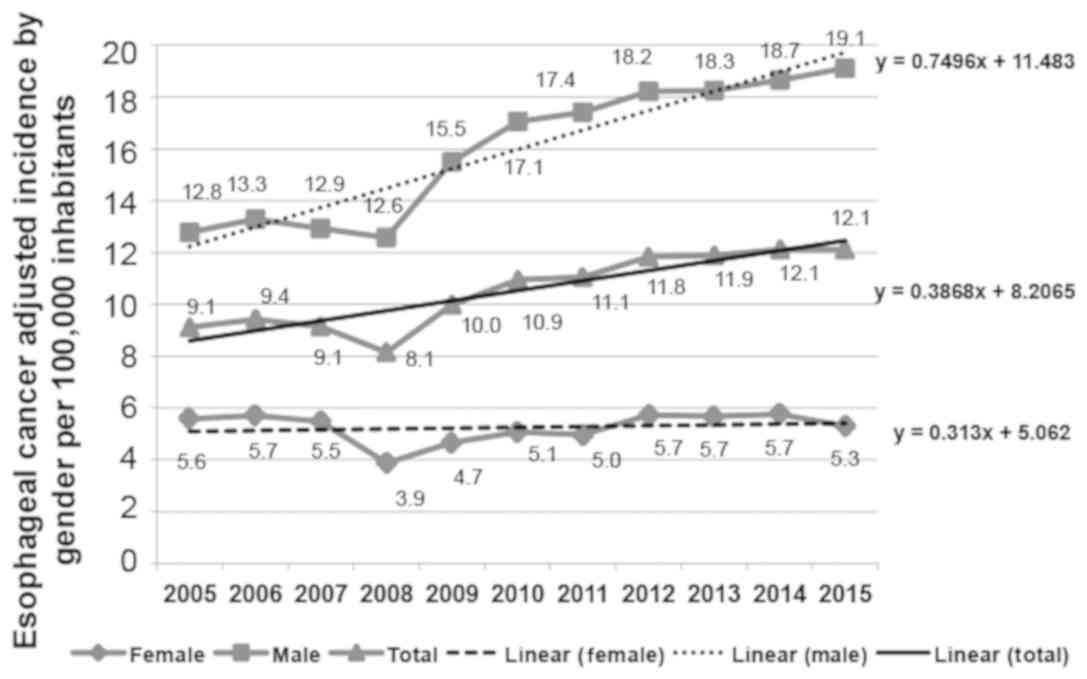
The total numbers of hospitalizations for EC were
12,641 in 2005 and 17,792 in 2015, 1935 and 2966 of which ended in
death, respectively. Adjusted rates according to available hospital
beds (Fig. S1) increased from 9.1
in 2005 to 12.1 in 2015 per 100,000 inhabitants. Regarding gender,
EC rates were consistent with the world trend for male
predominance, which were 69% in 2005 and 78% in 2015. In fact, in
males, hospitalization rates for EC per 100,000 inhabitants
increased from 12.8 to 19.1, while female rates remained stable
during the period (Fig. 1).
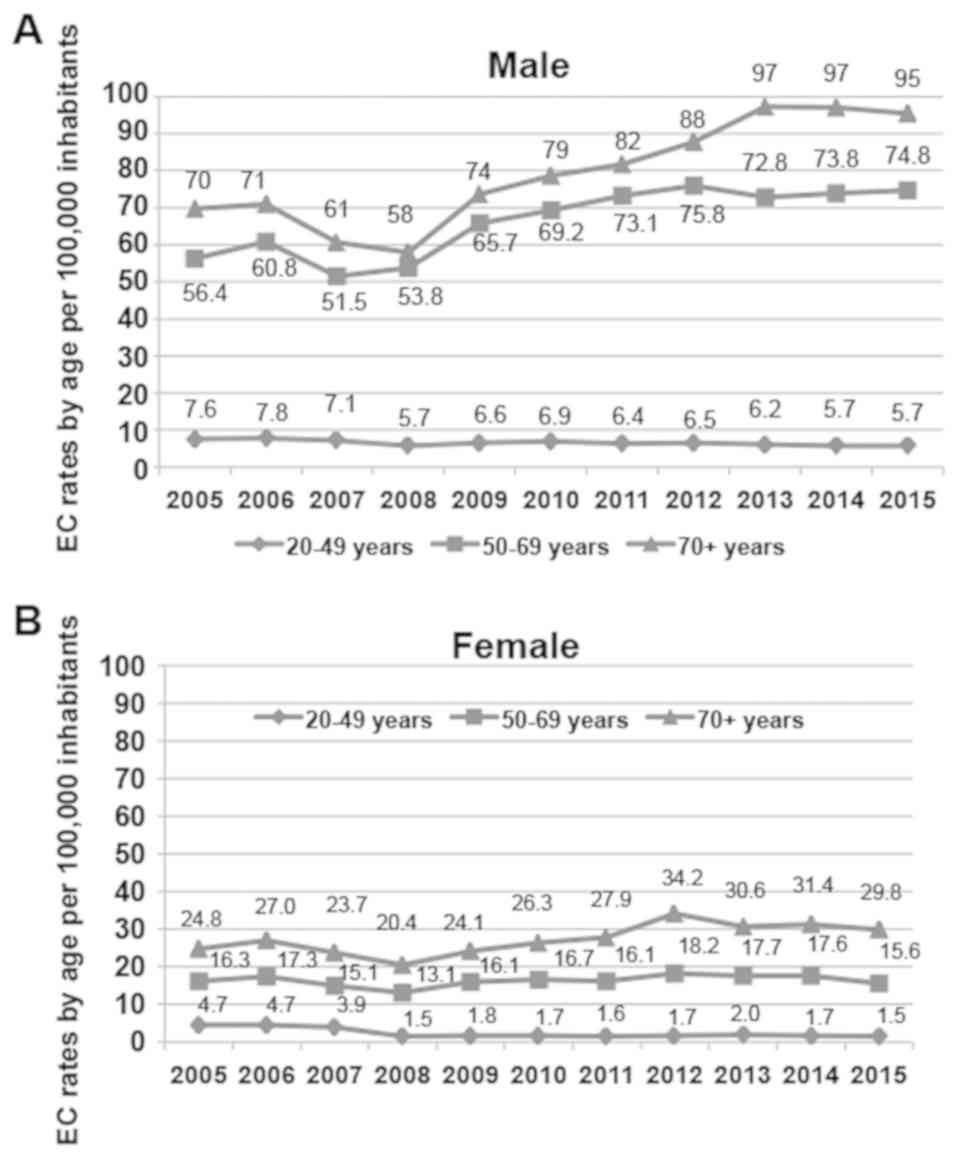
Next, we analyzed the distribution of EC according
to the age at diagnosis using age-standardized rates of
hospitalizations. Very few cases were observed below the age of 20
years; therefore, the data are not shown (Fig. 2). Relatively low rates of EC were
detected within the population below 50 years of age. In this age
group, both male and female hospitalization rates fell from 2005 to
2015, especially among females for whom rates decreased more than
3-fold. In the age range of 50–69 years, we observed an increase of
approximately 32% among males in contrast to a decrease of almost
5% among females. Above the age of 70, we detected an increase of
approximately 20% among females (Fig.
2A) and an increase of more than 35% among males (Fig. 2B) in the same period.
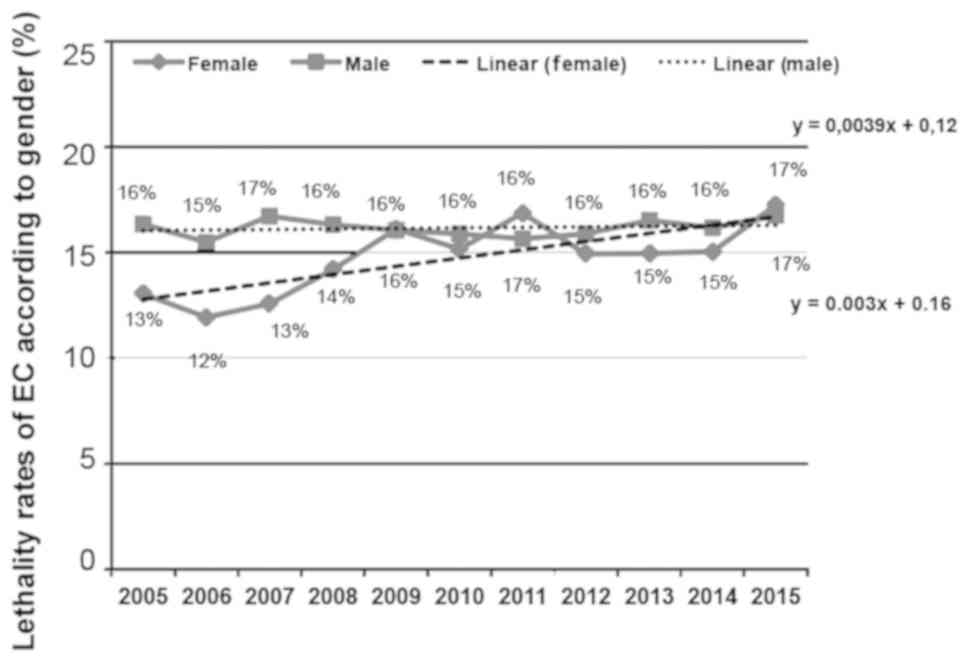
Lethality rates from EC
Regarding EC-associated lethality, considering
gender, rates remained relatively stable during the period analyzed
(Fig. 3).
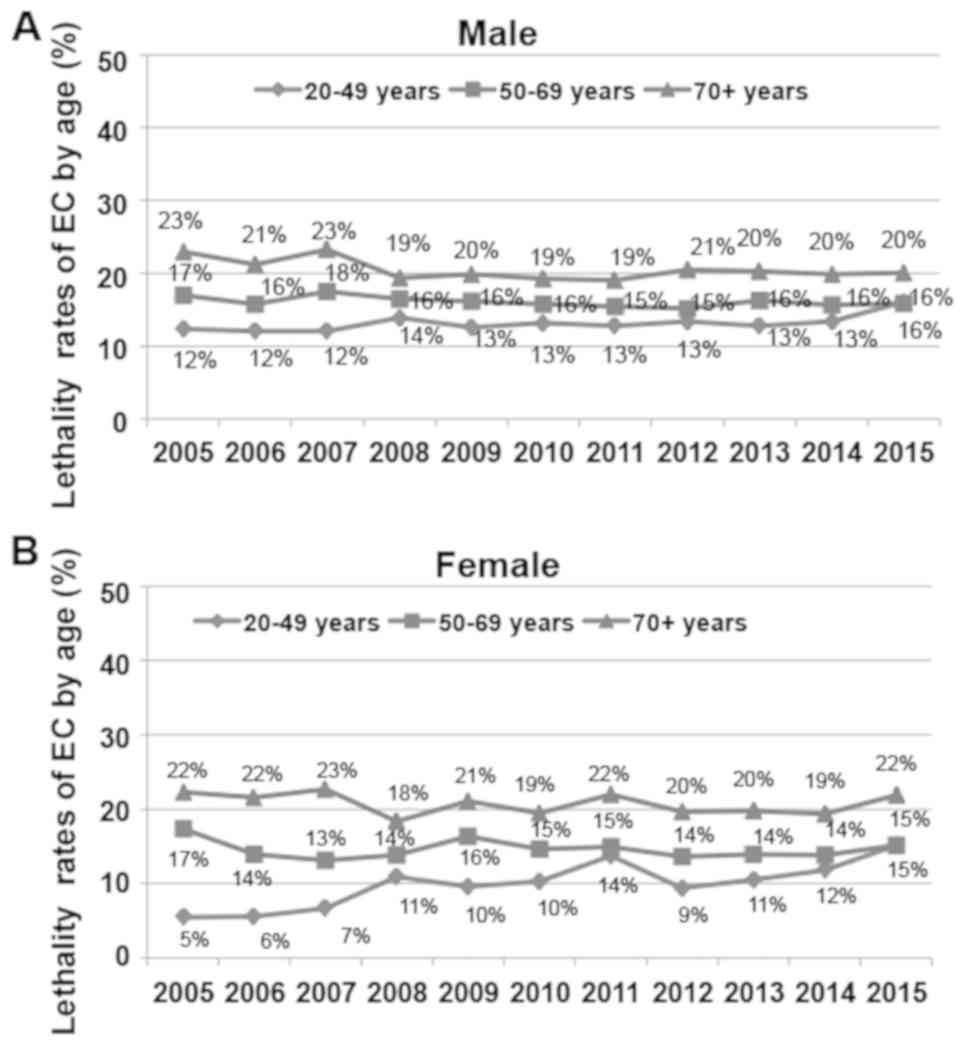
The age-standardized analysis revealed that
lethality among males also remained stable over the 11-year period,
with only a slight increase in cases below 50 years of age (12% in
2005 and 16% in 2015) (Fig. 4A).
Among females under 50 years of age, the rate increased from 5% in
2005 to 15% in 2015 (Fig. 4B). In
both genders, a slightly increased lethality rate was observed
among people over 70 years old.
Geographic distribution of EC
During the study period, an overall 33% increase in
estimated EC rates in Brazil was noted, which was mainly driven by
men aged 50 to 69 years (+32%) and both men and women aged 70 years
or older (+36 and +20%, respectively). Marked increases in EC rates
were observed in all five major regions of the country,
particularly in the Central-West region with an increase of 61% in
the period. The Southeast, Northeast and North regions also showed
notable increases (51, 51 and 48%, respectively), while the South
region had the lowest increase (35%).
Because of the economic and demographic disparities
of Brazil, we utilized a model that classifies municipalities
according to population and demographic density as rural small
(<50,000 or <80 inhabitants/km), rural medium (≥50,000 or ≥80
inhabitants/km, even if the population is <50,000 inhabitants),
and true urban centers (>100,000 inhabitants) (20). To analyze the trend of the Brazilian
population to congregate in large urban centers, EC incidence and
lethality rate data were collected considering municipality size
and relations to metropolitan regions. Large municipalities
comprise 86% of the metropolitan-integrated population.
Municipalities integrated or not integrated into metropolitan
regions had increases in the EC incidence of 24 and 39%,
respectively, between 2005 and 2015. In this period, we observed
increases in EC in small municipalities integrated (127%) and in
large municipalities not integrated (131%) into metropolitan
regions. Regarding the lethality rate, the most notable increases
were observed in medium and large municipalities not integrated
into metropolitan regions (14 and 17%, respectively; Table I).
 | Table I.Distribution of esophageal cancer
hospitalization and lethality rates in 2005 and 2015 according to
urban and rural demographic data. |
Table I.
Distribution of esophageal cancer
hospitalization and lethality rates in 2005 and 2015 according to
urban and rural demographic data.
|
| 2005 | 2015 |
|
|
|---|
|
|
|
|
|
|
|---|
| Municipalities | Admission rate (per
105) | Population | Adjusted admission
rate (per 105) | Lethality (%) | Admission rate (per
105) | Population | Adjusted admission
rate (per 105) | Lethality (%) | Changes in adjusted
admission rate (per 105), % | Changes in
lethality (%) |
|---|
| Integrated into
MR | 6.5 | 91,248,203 | 8.7 | 14 | 7.7 | 98,192,651 | 10.8 | 16 | 24 | 14 |
| Small | 6.4 | 4,542,857 | 8.5 | 13 | 13.7 | 3,919,865 | 19.3 | 13 | 127 | 0 |
| Medium | 5.8 | 9,013,588 | 7.8 | 17 | 9.0 | 9,429,076 | 12.7 | 16 | 63 | −6 |
| Large | 6.6 | 77,691,758 | 8.8 | 17 | 7.2 | 84,843,710 | 10.2 | 19 | 16 | 12 |
| Not integrated into
MR | 7.2 | 92,934,991 | 9.6 | 17 | 9.5 | 106,257,729 | 13.3 | 18 | 39 | 6 |
| Small | 6.4 | 46,661,002 | 8.6 | 12 | 9.9 | 49,253,779 | 13.9 | 14 | 62 | 17 |
| Medium | 6.6 | 22,965,072 | 8.8 | 14 | 8.5 | 26,762,001 | 11.9 | 16 | 35 | 14 |
| Large | 9.3 | 23,308,917 | 12.4 | 17 | 20.3 | 30,241,949 | 28.6 | 19 | 131 | 12 |
Municipal rates of hospitalization and in-hospital
death for EC were calculated per 100,000 inhabitants and were
plotted on maps per major region in the years 2005 and 2015 and are
shown in Figs. S2 and S3 in the appendices.
Discussion
The results of the present study indicate that the
EC incidence has increased, while the lethality rate has remained
stable from 2005 to 2015 in Brazil. In addition to the male
predominance in EC, we observed an increase among individuals older
than fifty years in contrast to a decrease among individuals under
fifty years of age. The geographic distribution of EC demonstrated
a higher concentration in the South region but also revealed a
greater relative increase across the other regions of the
country.
The considerable discrepancies in the worldwide EC
incidence (1) are probably because
ESCC and EAC are associated with different risk factors. EC is
estimated to occur 3–4-times more often in males (1,5), and the
difference is more marked for EAC for which sex ratios (M:F) range,
for example, from 5:1 in France to 10:1 in the United Kingdom
(21,22). A rapid increase in EAC among males
was also observed in the United States in the last four decades
(23). Here, we found an average
ratio of 3.6:1 (M:F), which is more compatible with the
predominance of the ESCC subtype. The male propensity may be
attributed to the greater concomitant exposure to the main risk
factors for EC, including tobacco and alcohol (24). In contrast, gastroesophageal reflux
disease and obesity, which are important risk factors for EAC, do
not justify the disproportionate gender bias towards men (25). Currently, almost one in five
Brazilians are considered obese (26). However, similar to data from European
countries and the United States, trends for the EC incidence,
including EAC, do not match corresponding trends in obesity
(27). While the reasons for male
predominance in EC remain incompletely understood, a role of
androgens and androgen receptors has been recently suggested
(28,29).
The gradual increase in EC should be further
analyzed considering the sociodemographic changes and inequalities
among the municipalities and regions of the country. Large
metropolitan municipalities and the highest development indices are
usually associated with the South and Southeast regions. In this
sense, in addition to smoking and alcohol, other factors, including
obesity, high consumption of processed foods, low fiber intake, the
aging population, improvement in the human development index (HDI),
and the Human Inequality Coefficient (30–33), may
be operating in concert to cause changes in EC epidemiology.
Interestingly, other studies had already identified South and
Southeast Brazil as regions with higher frequencies of cancer cases
(34,35). Similar to recent ecological studies
from our group pertaining to gastric cancer (18) and pancreatic cancer (19), the hospitalization rates were higher
in the South and Southeast regions, whereas in the North and
Northeast regions, the rates were the lowest in the country. Here,
the highest rates of EC were observed in areas of greater economic
development, which also have a higher HDI and lower social
vulnerability indices (SVIs). Although the highest EC rates in
Brazil were found in the South and Southeast regions, the greatest
increase occurred in the Central-West region, followed by the North
and Northeast regions. Although indices of social development
usually identify multiple deprivations in North and Northeast
Brazil, these regions exhibited the greatest advances in the last
two decades as the HDI increased 36.4% and the SVI decreased 27%
between 2000 and 2010 (32,33). Moreover, the gross product of the
Northeast increased 3% in 2012, which is greater than three-fold
compared to the national average (36). Socioeconomic development may have
allowed better access to health services and improvements in
facilities, affecting the quality of diagnosis, documentation, and
treatment in general. This development may also justify the largest
increases in EC rates within small metropolitan cities and large
cities in nonmetropolitan regions.
The time trends of the age-stratified groups show an
increased EC incidence among males aged 50 years or more, a
phenomenon usually attributed to accumulated environmental exposure
(37,38). This finding suggests that exposure to
risk factors for EC probably differed between male and female
patients. Here, we noted a marked increase in EC among males in the
age groups above 50 years, while among females, we noted only a
small increase in the age group over 70 years. The overall tendency
for increases apparently accompanies the increased longevity
observed in the country. Recent data indicate that Brazil has the
sixth oldest population in the world, with an increase of
approximately 500% in the last four decades (39,40). In
addition, the relative decrease in EC rates among people under 50
years may reflect a more recent reduction in environmental
exposure, such as smoking. Although the country's population is
progressively growing older, changes were not relevant in the
relatively short period analyzed in this study. Moreover, the
subgroup analyses including age-standardized and gender incidences
used rates considering relative differences within each
municipality unit. Thus, changes in the EC incidence have been
considered to be probably related to the different municipalities
characterized by specific environments and individual
particularities.
Smoking, one of the most important factors related
to EC, has dropped almost 30% in the last decade in Brazil, and
rates are higher among men (14.4%) than among women (8.6%)
(41,42). Moreover, smoking is more prevalent in
the South and Southeast regions where the highest rates of EC are
also observed (41). Actually, the
highest smoking frequencies in the country are located in two large
metropolises in South Brazil: Porto Alegre, 25.2% and Curitiba,
21.5% (41,43). Notably, Brazil is currently one of
the largest tobacco producers in the world, and the South region
accounts for 98% of the country's tobacco farms (44,45). In
particular, Brazilian tobacco farmers show a higher frequency of
smoking (31%) than the rural male population as a whole (46). Some other lifestyle factors, however,
may also act directly on the esophagus and be implicated in EC. For
instance, ethanol consumption, especially together with smoking, is
also a well-recognized factor related to EC. For example, recently,
the abusive consumption of alcoholic beverages in Brazil was
determined to be 19.1% on average and was greater among males
(47). Interestingly, the
traditional habit of drinking mate, a kind of hot tea, has been
proposed as an additional explanation for the concentration of EC
in the South region of the country (48–50). Hot
mate tea has been associated with different patterns of TP53
mutations, probably due to epigenetic modifications driven by
chronic hyperthermic irritation (51). However, concomitant exposure to other
various lifestyle risk factors, including ethanol, tobacco,
charcoal-grilled red meat and animal fat, and the low consumption
of fruits and vegetables (52), may
render the influence of mate difficult to interpret. Moreover, the
potential roles of other elements associated with low living
standards still present in several Brazilian municipalities should
be considered, such as poor oral hygiene and nutrition, which are
also linked to oral and pharyngeal cancer (53).
The highest EC rates observed in the South region
should also be analyzed in the context of specific population
features. The Brazilian population is regarded as one of the most
heterogeneous in the world due to five centuries of crossings among
distinct ethnic origins (54). The
genetic background of the population shows a wide range and
variable patterns of admixture, with a major contribution of
European ancestry, followed by African and Amerindian contributions
(55). In a recent study,
investigators demonstrated the prevalence of the European ancestry
among urban populations, which reached almost 80% in the South
region versus less than 60% in the North, Northeast, and
Central-West regions, increasing along a north-to-south gradient
(56) and corroborating the notion
that the genetic heterogeneity in Brazil is mostly detected among
regions rather than within regions (57). While the incidence of ESCC is
reported to be three-times higher in blacks (58), EAC is markedly more common in whites
(58,59). In a recent study on EC in Sao Paulo,
Southeast Brazil, with more than five hundred cases, investigators
found marked predominance rates of both ESCC and EAC among white
patients (60). These findings are
in agreement with other international studies showing increased
incidence rates among whites and may reflect the local predominance
of European ancestry as observed throughout South Brazil. Although
the methodology of this study does not allow distinction between
the major subtypes of EC, the disproportionately high
concentrations observed in the Southeast region and particularly in
the South region may reflect local ongoing increases in EAC.
Notably, Brazil is a continental country with substantial
demographic and developmental inequalities throughout its more than
five thousand municipalities. In fact, the country is extremely
heterogeneous in several aspects, including urbanization,
population densities, climate, economy, and industrialization, in
addition to cultural, dietary, and even genetic particularities.
Thus, the increase in EC rates in Brazil may have been fueled by
the acquisition of risk factors typical of modern societies in the
last few decades (such as dietary changes and smoking patterns)
along with other elements, including industrialization, improvement
in the HDI, and the Human Inequality Coefficient.
EC represents a serious malignancy since its
incidence continues to increase while its prognosis and mortality
rate remain practically unchanged (61,62). EC
is usually associated with a very poor survival rate, and the
geographic distribution of mortality is similar to that of its
incidence, with the highest rates per 100,000 inhabitants occurring
in East Asia (14.1) and Southern Africa (12.8) in men and in
Eastern (7.3) and Southern Africa (6.2) in women. In this study, we
observed a small increase in lethality in females and a relatively
stable trend among males. These trends were maintained fairly well
in the analysis by age-standardized groups and are also consistent
with previous reports (1,63). Despite improvements in diagnosis,
including the availability of endoscopy, the mortality rate remains
unacceptably high in most countries (64). Nonetheless, reports showing
reductions in mortality rates in some countries have been
attributed to better surgical results. As surgical treatment
represents the best potentially curative option for EC, improved
outcomes reflect an increasing number of surgeries in high-volume
centers and the implementation of multimodal therapy (65,66).
Although the results of this study may allow initial
insight into EC behavior and time trends in Brazil due to the
collection of information from all 5565 municipalities and the time
trend analysis of EC in the country for the first time, some
limitations need to be addressed. First, using the available
DATASUS database, distinguishing between ESCC and EAC, the two
major types of tumors, is impossible given their epidemiological
peculiarities. Second, the system does not allow evaluation of
information regarding co-morbidities and therapy. Third,
differences in the availability and quality of health care in less
developed areas of the country may result in potential
discrepancies in the available data. Fourth, the analysis based on
hospitalization records does not consider outpatients who had not
been subjected to medical procedures or hospital admissions. Fifth,
the concept of a municipality is probably different in Brazil from
that in most countries. In this regard, in addition to geographic
heterogeneities, Brazilian cities may show discrepancies in terms
of population, with huge differences in densities. Nevertheless,
such differences would be regarded as municipal units of the same
level in our database. Therefore, considering all these limitations
together, the results of this study must be interpreted with
caution. Despite the potential limitations of this study, all
procedures were rigorously carried out to produce a database
containing nationwide information gathered in a single electronic
system.
The recent increase in the EC incidence in Brazil
follows a global tendency and is concentrated in the population
above seventy years of age. Although the current higher rates in
the South and Southeast regions may reflect the presence of major
environmental factors in association with a possible genetic
predisposition, shifts in the incidence from the south towards the
north and from urbanized to rural areas have been observed. Such
geographic shifts in addition to the relative decrease in EC among
individuals under the age of fifty years support the notion of
ongoing dynamic changes within the socioeconomic environment.
However, the unchanging high mortality associated with EC, along
with the rapidly aging population, suggests that EC will remain a
critical health issue in Brazil in the near future, potentially
imposing significant social and economic burdens.
Supplementary Material
Supporting Data
Acknowledgements
The authors would like to thank the Brazilian
Research Foundations CNPq and FAPERJ for their financial
support.
Funding
This work was supported by grants from the Brazilian
Research Council (CNPq; grant no. 302401/2016-4) and the Fundação
Carlos Chagas Filho de Amparo à Pesquisa do Estado do Rio de
Janeiro (grant no. E26/202.781/2017).
Availability of data and materials
The datasets analyzed during the current study are
available in the Health Informatics Department of the Brazilian
Ministry of Health (DATASUS) repository (www2.datasus.gov.br/DATASUS). DATASUS registries
include hospital admission and discharge information, medical
procedures and mortality, reference tables and demographic data
(age, sex, municipality) collected by the Instituto Brasileiro de
Geografia e Estatística (Brazilian Institute of Geography and
Statistics).
Authors' contributions
CAA and LPdS participated in the conception and
design of the study, the acquisition, analysis and interpretation
of data, and the drafting of the manuscript. JPM and RRL
participated in the acquisition, analysis and interpretation of the
data, and the drafting of parts of the manuscript. AJC and HSPdS
participated in the conception and design of the study, obtained
funding, analyzed and interpreted the data, and critically revised
the manuscript for important intellectual content. All authors gave
final approval of the submitted version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Pennathur A, Gibson MK, Jobe BA and
Luketich JD: Oesophageal carcinoma. Lancet. 381:400–412. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Mao WM, Zheng WH and Ling ZQ:
Epidemiologic risk factors for esophageal cancer development. Asian
Pac J Cancer Prev. 12:2461–2466. 2011.PubMed/NCBI
|
|
4
|
Enzinger PC and Mayer RJ: Esophageal
cancer. N Engl J Med. 349:2241–2252. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Domper Arnal MJ, Ferrandez Arenas A and
Lanas Arbeloa A: Esophageal cancer: Risk factors, screening and
endoscopic treatment in western and eastern countries. World J
Gastroenterol. 21:7933–7943. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wheeler JB and Reed CE: Epidemiology of
esophageal cancer. Surg Clin North Am. 92:1077–1087. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Oze I, Matsuo K, Ito H, Wakai K, Nagata C,
Mizoue T, Tanaka K, Tsuji I, Tamakoshi A, Sasazuki S, et al:
Cigarette smoking and esophageal cancer risk: An evaluation based
on a systematic review of epidemiologic evidence among the Japanese
population. Jpn J Clin Oncol. 42:63–73. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yousef F, Cardwell C, Cantwell MM, Galway
K, Johnston BT and Murray L: The incidence of esophageal cancer and
high-grade dysplasia in Barrett's esophagus: A systematic review
and meta-analysis. Am J Epidemiol. 168:237–249. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bhat S, Coleman HG, Yousef F, Johnston BT,
McManus DT, Gavin AT and Murray LJ: Risk of malignant progression
in Barrett's esophagus patients: Results from a large
population-based study. J Natl Cancer Inst. 103:1049–1057. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Renehan AG, Tyson M, Egger M, Heller RF
and Zwahlen M: Body-mass index and incidence of cancer: A
systematic review and meta-analysis of prospective observational
studies. Lancet. 371:569–578. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hoyo C, Cook MB, Kamangar F, Freedman ND,
Whiteman DC, Bernstein L, Brown LM, Risch HA, Ye W, Sharp L, et al:
Body mass index in relation to oesophageal and oesophagogastric
junction adenocarcinomas: A pooled analysis from the International
BEACON Consortium. Int J Epidemiol. 41:1706–1718. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Reed PI and Johnston BJ: The changing
incidence of oesophageal cancer. Endoscopy. 25:606–608. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tran GD, Sun XD, Abnet CC, Fan JH, Dawsey
SM, Dong ZW, Mark SD, Qiao YL and Taylor PR: Prospective study of
risk factors for esophageal and gastric cancers in the linxian
general population trial cohort in China. Int J Cancer.
113:456–463. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Munoz N, Crespi M, Grassi A, Qing WG,
Qiong S and Cai LZ: Precursor lesions of oesophageal cancer in
high-risk populations in Iran and china. Lancet. 1:876–879. 1982.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kaz AM and Grady WM: Epigenetic biomarkers
in esophageal cancer. Cancer Lett. 342:193–199. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Das M, Saikia BJ, Sharma SK, Sekhon GS,
Mahanta J and Phukan RK: p16 hypermethylation: A biomarker for
increased esophageal cancer susceptibility in high incidence region
of North East India. Tumour Biol. 36:1627–1642. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lepage C, Rachet B, Jooste V, Faivre J and
Coleman MP: Continuing rapid increase in esophageal adenocarcinoma
in England and Wales. Am J Gastroenterol. 103:2694–2699. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Amorim CA, Moreira JP, Rial L, Carneiro
AJ, Fogaça HS, Elia C, Luiz RR and de Souza HS: Ecological study of
gastric cancer in Brazil: Geographic and time trend analysis. World
J Gastroenterol. 20:5036–5044. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Perrotta de Souza LM, Moreira JPL, Fogaca
HS, Luiz RR and de Souza HS: Pancreatic cancer incidence and
lethality rates in Brazil: An ecological study. Pancreas.
46:699–706. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Veiga JE: The rural dimension of Brasil.
Estud Soc Agric. 12:71–94. 2004.
|
|
21
|
Lepage C, Drouillard A, Jouve JL and
Faivre J: Epidemiology and risk factors for oesophageal
adenocarcinoma. Dig Liver Dis. 45:625–629. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Thrift AP and Whiteman DC: The incidence
of esophageal adenocarcinoma continues to rise: Analysis of period
and birth cohort effects on recent trends. Ann Oncol. 23:3155–3162.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Mathieu LN, Kanarek NF, Tsai HL, Rudin CM
and Brock MV: Age and sex differences in the incidence of
esophageal adenocarcinoma: Results from the surveillance,
epidemiology, and end results (SEER) registry (1973–2008). Dis
Esophagus. 27:757–763. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Lindblad M, Ye W, Lindgren A and Lagergren
J: Disparities in the classification of esophageal and cardia
adenocarcinomas and their influence on reported incidence rates.
Ann Surg. 243:479–485. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Whiteman DC, Sadeghi S, Pandeya N,
Smithers BM, Gotley DC, Bain CJ, Webb PM and Green AC; Australian
Cancer Study, : Combined effects of obesity, acid reflux and
smoking on the risk of adenocarcinomas of the oesophagus. Gut.
57:173–180. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Souza L, Brunken GS, Segri NJ and Malta
DC: Trends of self-rated health in relation to overweight in the
adult population in Brazilian midwest capitals. Rev Bras Epidemiol.
20:299–309. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kroep S, Lansdorp-Vogelaar I, Rubenstein
JH, Lemmens VE, van Heijningen EB, Aragonés N, van Ballegooijen M
and Inadomi JM: Comparing trends in esophageal adenocarcinoma
incidence and lifestyle factors between the united states, Spain,
and the Netherlands. Am J Gastroenterol. 109:336–343; quiz 335,
344. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Sukocheva OA, Li B, Due SL, Hussey DJ and
Watson DI: Androgens and esophageal cancer: What do we know? World
J Gastroenterol. 21:6146–6156. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Lagergren K, Lagergren J and Brusselaers
N: Hormone replacement therapy and oral contraceptives and risk of
oesophageal adenocarcinoma: A systematic review and meta-analysis.
Int J Cancer. 135:2183–2190. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Szwarcwald CL, Bastos FI, Barcellos C,
Pina MF and Esteves MA: Health conditions and residential
concentration of poverty: A study in Rio de Janeiro, Brazil. J
Epidemiol Community Health. 54:530–536. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Bortz M, Kano M, Ramroth H, Barcellos C,
Weaver SR, Rothenberg R and Magalhães M: Disaggregating health
inequalities within Rio de Janeiro, Brazil, 2002–2010, by applying
an urban health inequality index. Cad Saude Publica. 31 (Suppl
1):S107–S119. 2015. View Article : Google Scholar
|
|
32
|
United Nations Development Programme, .
Human development indices and indicators: 2018 statistical update.
http://hdr.undp.org/en/content/human-development-indices-indicators-2018-statistical-updateNovember
5–2018
|
|
33
|
United Nations Educational, Scientific,
Cultural Organization, . United Nations Educational SaCO: Institute
for statistics. http://www.unesco.org/new/en/santiago/resources/statistics/November
5–2018
|
|
34
|
Lin CC, Chiang JH, Li CI, Liu CS, Lin WY,
Hsieh TF and Li TC: Cancer risks among patients with type 2
diabetes: A 10-year follow-up study of a nationwide
population-based cohort in Taiwan. BMC cancer. 14:3812014.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Pinto FG and Curi PR: Mortality due to
neoplasms in Brazil (1980/1983/1985): Grouping by states, behavior
and trends. Rev Saude Publica. 25:276–281. 1991.(In Portuguese).
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Instituto Brasileiro de Geografia e
Estatistica (IBGE), . Health statistics: Survey of medical-sanitary
assistance 2009. https://ww2.ibge.gov.br/english/estatistica/populacao/condicaodevida/ams/2009/default.shtmNovember
5–2018
|
|
37
|
Zhang Y: Epidemiology of esophageal
cancer. World J Gastroenterol. 19:5598–5606. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Muwonge R, Ramadas K, Sankila R, Thara S,
Thomas G, Vinoda J and Sankaranarayanan R: Role of tobacco smoking,
chewing and alcohol drinking in the risk of oral cancer in
Trivandrum, India: A nested case-control design using incident
cancer cases. Oral Oncol. 44:446–454. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Paim J, Travassos C, Almeida C, Bahia L
and Macinko J: The Brazilian health system: History, advances, and
challenges. Lancet. 377:1778–1797. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Beard JR and Bloom DE: Towards a
comprehensive public health response to population ageing. Lancet.
385:658–661. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Malta DC, Stopa SR, Santos MAS, Andrade
SSCA, Oliveira TP, Cristo EB and Silva MMAD: Evolution of tobacco
use indicators according to telephone surveys, 2006–2014. Cad Saude
Publica. 33 (Suppl 3):e001349152017.(In English, Portuguese).
|
|
42
|
Azevedo e Silva G, Valente JG and Malta
DC: Trends in smoking among the adult population in Brazilian
capitals: A data analysis of telephone surveys from 2006 to 2009.
Rev Bras Epidemiol. 14 (Suppl 1):S103–S114. 2011.(In English,
Portuguese).
|
|
43
|
Moura MA, Bergmann A, Aguiar SS and Thuler
LC: The magnitude of the association between smoking and the risk
of developing cancer in Brazil: A multicenter study. BMJ open.
4:e0037362014. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Bartholomay P, Iser BP, de Oliveira PP,
dos Santos TE, Malta DC, Sobel J and de Moura L: Epidemiologic
investigation of an occupational illness of tobacco harvesters in
southern Brazil, a worldwide leader in tobacco production. Occup
Environ Med. 69:514–518. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Opaleye ES, Sanchez ZM, Moura YG, Galduroz
JC, Locatelli DP and Noto AR: The Brazilian smoker: A survey in the
largest cities of Brazil. Braz J Psychiatry. 34:43–51. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Fiori NS, Faria NM, Meucci RD and Fassa
AG: Smoking prevalence and associated factors among tobacco farmers
in southern Brazil. Cad Saude Publica. 32:S0102–311X2016000705012.
2016.(In Portuguese). PubMed/NCBI
|
|
47
|
Munhoz TN, Santos IS, Nunes BP, Mola CL,
Silva I and Matijasevich A: Trends in alcohol abuse in Brazilian
state capitals from 2006 to 2013: An analysis of data from the
VIGITEL survey. Cad Saude Publica. 33:e001045162017.(In
Portuguese). PubMed/NCBI
|
|
48
|
Munoz N, Victora CG, Crespi M, Saul C,
Braga NM and Correa P: Hot mate drinking and precancerous lesions
of the oesophagus: An endoscopic survey in Southern Brazil. Int J
Cancer. 39:708–709. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Szymanska K, Matos E, Hung RJ,
Wünsch-Filho V, Eluf-Neto J, Menezes A, Daudt AW, Brennan P and
Boffetta P: Drinking of mate and the risk of cancers of the upper
aerodigestive tract in Latin America: A case-control study. Cancer
Causes Control. 21:1799–1806. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Mello FW, Scotti FM, Melo G,
Warnakulasuriya S, Guerra ENS and Rivero ERC: Mate consumption
association with upper aerodigestive tract cancers: A systematic
review and meta-analysis. Oral Oncol. 82:37–47. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Putz A, Hartmann AA, Fontes PR, Alexandre
CO, Silveira DA, Klug SJ and Rabes HM: TP53 mutation pattern of
esophageal squamous cell carcinomas in a high risk area (Southern
Brazil): Role of life style factors. Int J Cancer. 98:99–105. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Castellsague X, Munoz N, De Stefani E,
Victora CG, Castelletto R and Rolon PA: Influence of mate drinking,
hot beverages and diet on esophageal cancer risk in South America.
Int J Cancer. 88:658–664. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Wunsch-Filho V: The epidemiology of oral
and pharynx cancer in Brazil. Oral Oncol. 38:737–746. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Sans M: Admixture studies in Latin
America: From the 20th to the 21st century. Hum Biol. 72:155–177.
2000.PubMed/NCBI
|
|
55
|
Lins TC, Vieira RG, Abreu BS, Grattapaglia
D and Pereira RW: Genetic composition of Brazilian population
samples based on a set of twenty-eight ancestry informative SNPs.
Am J Hum Biol. 22:187–192. 2010.PubMed/NCBI
|
|
56
|
Saloum de Neves Manta F, Pereira R, Vianna
R, Rodolfo Beuttenmüller de Araújo A, Leite Góes Gitaí D, Aparecida
da Silva D, de Vargas Wolfgramm E, da Mota Pontes I, Ivan Aguiar J,
Ozório Moraes M, et al: Revisiting the genetic ancestry of
Brazilians using autosomal AIM-Indels. PLoS One. 8:e751452013.
View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Pena SD, Di Pietro G, Fuchshuber-Moraes M,
Genro JP, Hutz MH, Kehdy Fde S, Kohlrausch F, Magno LA, Montenegro
RC, Moraes MO, et al: The genomic ancestry of individuals from
different geographical regions of Brazil is more uniform than
expected. PLoS One. 6:e170632011. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Daly JM, Fry WA, Little AG, Winchester DP,
McKee RF, Stewart AK and Fremgen AM: Esophageal cancer: Results of
an American college of surgeons patient care evaluation study. J Am
Coll Surg. 190:562–573. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Dhillon PK, Farrow DC, Vaughan TL, Chow
WH, Risch HA, Gammon MD, Mayne ST, Stanford JL, Schoenberg JB,
Ahsan H, et al: Family history of cancer and risk of esophageal and
gastric cancers in the United States. Int J Cancer. 93:148–152.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Tustumi F, Takeda FR, Kimura CM, Sallum
RA, Ribeiro UJ and Cecconello I: Esophageal carcinoma: Is squamous
cell carcinoma different disease compared to adenocarcinoma? a
transversal study in a quaternary high volume hospital in Brazil.
Arq Gastroenterol. 53:44–48. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Eslick GD: Epidemiology of esophageal
cancer. Gastroenterol Clin North Am. 3817–25. (vii)2009. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Napier KJ, Scheerer M and Misra S:
Esophageal cancer: A Review of epidemiology, pathogenesis, staging
workup and treatment modalities. World J Gastrointest Oncol.
6:112–120. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Bosetti C, Levi F, Ferlay J, Garavello W,
Lucchini F, Bertuccio P, Negri E and La Vecchia C: Trends in
oesophageal cancer incidence and mortality in Europe. Int J Cancer.
122:1118–1129. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Jemal A, Center MM, DeSantis C and Ward
EM: Global patterns of cancer incidence and mortality rates and
trends. Cancer Epidemiol Biomarkers Prev. 19:1893–1907. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Dikken JL, Dassen AE, Lemmens VE, Putter
H, Krijnen P, van der Geest L, Bosscha K, Verheij M, van de Velde
CJ and Wouters MW: Effect of hospital volume on postoperative
mortality and survival after oesophageal and gastric cancer surgery
in the Netherlands between 1989 and 2009. Eur J Cancer.
48:1004–1013. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Dikken JL, Lemmens VE, Wouters MW,
Wijnhoven BP, Siersema PD, Nieuwenhuijzen GA, van Sandick JW, Cats
A, Verheij M, Coebergh JW and van de Velde CJ: Increased incidence
and survival for oesophageal cancer but not for gastric cardia
cancer in the Netherlands. Eur J Cancer. 48:1624–1632. 2012.
View Article : Google Scholar : PubMed/NCBI
|