Introduction
Urachal cancer (UrC) is a very rare but highly
malignant tumor with an incidence of <1% of all bladder cancers
(1–3). Because of the silent nature of early
lesions, their propensity for local growth and the tendency to
metastasize late in the clinical course, a large proportion of
patients with UrC present with disease at the pT3 stage: Local
extension to the (a) bladder, (b) abdominal wall, (c) viscera other
than the bladder, or higher (1).
UrC consisted of well differentiated tumors, and
non-involvement of adjacent organs and the peritoneum indicates
better prognosis when treated operatively (3), however, there have been lack of
evidence for advanced UrC. Furthermore, a recurrent rate is very
high in patient with advanced UrC even if treated operatively.
Patients with metastatic or recurrent UrC have
extreme poor prognosis because there is currently no established
standard regimen in chemotherapy or radiation protocol for these
patients. A median survival time of patients with metastatic UrC is
reported as up to 1.3 years at best (4). Here, we report a patient with
metastatic UrC who achieved a comparatively long-term survival with
gemcitabine (GEM)/cisplatin (CDDP) combination chemotherapy and
radiotherapy.
Case report
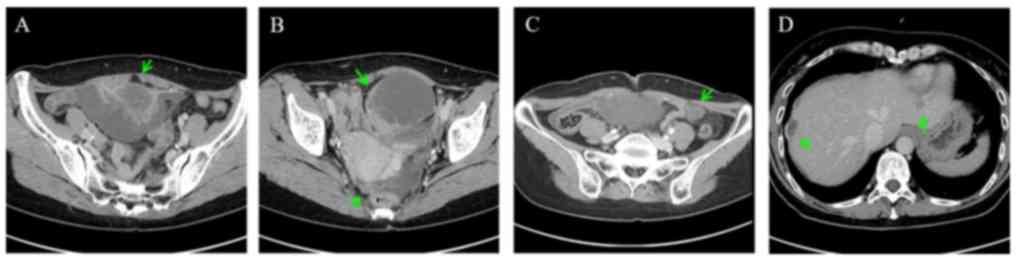
A 55-year-old female reported to our department with
right lower abdominal pain in March 2013. The patient did not
present with any other diseases and urinary symptoms. A
contrast-enhanced computed tomography (CT) examination at the first
visit showed a tumor extended along the course of the urachus
(Fig 1A-C). Peritoneal dissemination
spread to the surface of the liver (Fig.
1D). Both serum carcinoembryonic antigen (CEA) and carbohydrate
antigen (CA) 125 were present in high levels, with values of 294
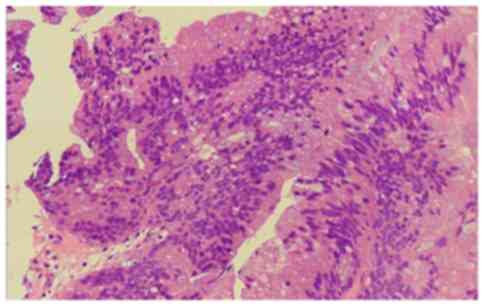
ng/ml and 92 U/ml, respectively. The patient immediately underwent
transurethral biopsy of the urachal tumor, which revealed urachal
adenocarcinoma (Fig. 2). She was
accordingly diagnosed with Sheldon's stage IVB. As she did not
previously have a history of urachal cancer, the disease was not
recurrent and was considered primary.
Because surgical resection for primary site is not
curative for this stage, she was eventually administered systemic
chemotherapy since April 2013 (repeated every 4 weeks) with GEM
(1,000 mg/m2/day) on day 1, 8, 15, and CDDP (70
mg/m2/day) on day 2. The CT examination after first
course of chemotherapy showed exacerbation of her right
hydronephrosis and renal function declined at the end of the first
course, we inserted an indwelling right ureteral stent for right
hydronephrosis.
After confirming improved renal function, we adopted
the strategy of GEM plus split-dose CDDP method (GEM: 1,000
mg/m2/day, day 1, 8, 15, CDDP: 35 mg/m2/day,
day 2, day 9, repeated every 4 weeks). She completed the
chemotherapy without any change to her renal function through
course 6. Serum levels of CEA and CA 125 declined to 37 ng/ml and
29 U/ml, respectively, and radiological examination showed disease
stability. Chemotherapy was discontinued once, owing to the
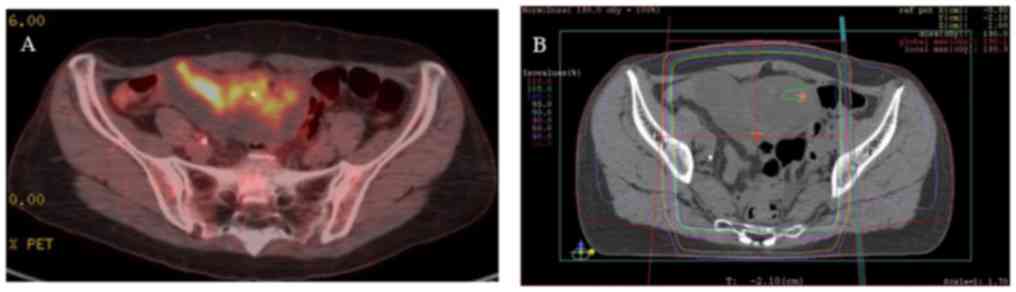
patient's limited physical strength. Though CT examination at 10
months after initial diagnosis revealed disease stability,
examination using 18F-FDG positron emission tomography at 11 months
after initial diagnosis led us to suspect viable cells at a primary
site; therefore, we conducted external beam radiation therapy
(EBRT, 50.4 Gy, 28 fractions, Fig. 3A
and B).
Because serum CEA and CA 125 gradually increased and
we observed progression of multiple peritoneal metastases after
EBRT at 19 months after initial diagnosis, we administered
additional chemotherapy with GEM plus split-dose CDDP method.
However, she did not complete chemotherapy due to hematological
toxicity and exhibited a decline in her status. Her general
condition gradually deteriorated, and she died of urachal
adenocarcinoma 23 months after initial diagnosis.
Discussion
The therapeutic strategy for metastatic UrC has not
yet been established because of its rare occurrence. A review with
meta-analysis conducted on 1,010 cases of urachal cancer suggested
the superiority of 5-FU-containing chemotherapy regimens to
cisplatin-based chemotherapy regimens. However, the authors
indicated that their combination seemed to provide the strongest
anti-tumor effect (5). Furthermore,
some reports have confirmed the efficacy of combination
chemotherapy for metastatic UrC.
Incidentally, gemcitabine, which is an analog of
deoxycytidine, is also an inhibitor of DNA synthesis (6). The combination chemotherapy with this
drug is still considered to be standard induction chemotherapy for
many types of advanced cancer such as pancreatic cancer (7), biliary tract cancer (8), and urothelial carcinoma of the bladder
(9). Regarding metastatic UrC, some
reports have detailed the efficacy of combination chemotherapy with
GEM, and some cases achieved complete or partial response in
several case reports or series (10–12).
Urologists have an expertise in this treatment method because
GEM/CDDP combination chemotherapy is now considered the gold
standard for both advanced upper tract urothelial cancer and
bladder cancer.
In terms of histological similarity of UrC to colon
cancer, reports of FOLFOX (oxaliplatin, 5-FU, and leukovolin)
regimen for metastatic UrC have been found on occasion.
Nevertheless, they are all in the case series (13,14).
Similarly, although CPT-11/TS-1 combination chemotherapy is
considered as a salvage or adjuvant therapy (15), and TS-1/CDDP combination chemotherapy
for UrC with multiple lung metastases (16) has been reported; they are only
limited cases.
With respect to radiotherapy, the effectiveness of
EBRT for bone metastases in a metastatic UrC case to relieve pain
has been reported (10). Although
EBRT for primary site has been reported and has showed a certain
therapeutic efficacy (17), it
remains in the case series.
Regarding therapeutic effect, Hasegawa et al
(18) recommended measurements of
serum CEA and CA 19-9 because their value appears to reflect the
progression of UrC. Zong and Chen (19) also indicated efficacy of serum tumor
markers such as CA 724, CA 125, CA 19-9, and CEA for a case report
of urachal cancer with repeated relapses.
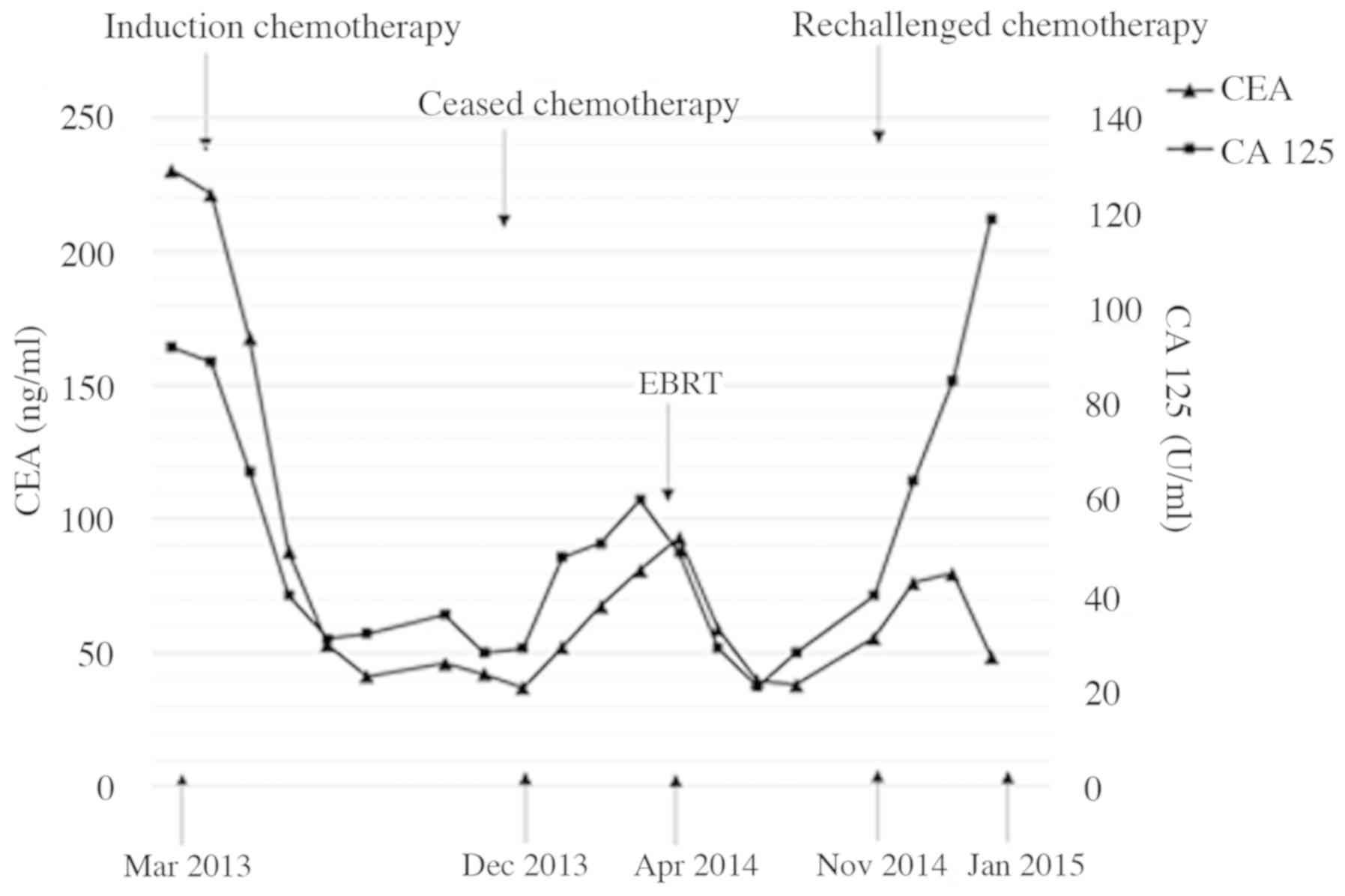
Based on these facts, we measured serum CEA, CA 19-9
and CA 125 at initial diagnosis as well and found an increase in
CEA and CA 125. Because serum CEA and CA 125 reflected some
improved therapeutic effect in our present case (Fig. 4), the measurement and follow-up of
such tumor markers should be necessary and standard during
treatment.
In conclusion, we observed a case of metastatic UrC
treated with combination chemotherapy and EBRT. The evaluation of
tumor markers such as CEA and CA 125 appear to be effective in
predicting therapeutic response. Further investigation is warranted
to improve survival rates in metastatic UrC.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
HY, KI and AM designed the study and drafted the
manuscript. TN, KS and YK made substantial contributions to the
study conception and design. HY also retrieved the pathology
images. HY, SK, RN, TM, HI and KI reviewed the patient's history,
and clinical and imaging data. AM supervised the entire project. HY
and KI critically revised the manuscript. All the authors have read
and approved the final version of this manuscript.
Ethics approval and consent to
participate
The Ethics Committee of Kanazawa University waived
the requirement for ethical approval and patient consent due to the
retrospective nature of the report and as the patients' relatives
were unable to be reached.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Gopalan A, Sharp DS, Fine SW, Tickoo SK,
Herr HW, Reuter VE and Olgac S: Urachal carcinoma: A
clinicopathologic analysis of 24 cases with outcome correlation. Am
J Surg Pathol. 33:659–668. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Johnson DE, Hodge GB, Abdul-Karim FW and
Ayala AG: Urachal carcinoma. Urology. 26:218–221. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pinthus JH, Haddad R, Trachtenberg J,
Holowaty E, Bowler J, Herzenberg AM, Jewett M and Fleshner NE:
Population based survival data on urachal tumors. J Urol.
175:2042–2047; discussion 2047. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yanagihara Y, Tanji N, Miura N, Shirato A,
Nishimura K, Fukumoto T, Azuma K, Miyauchi Y, Kikugawa T and
Yokoyama M: Modified FOLFOX6 chemotherapy in patients with
metastatic urachal cancer. Chemotherapy. 59:402–406. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Szarvas T, Módos O, Niedworok C, Reis H,
Szendröi A, Szász MA and Nyirády P: Clinical, prognostic, and
therapeutic aspects of urachal carcinoma-A comprehensive review
with meta-analysis of 1,010 cases. Urol Oncol. 34:388–398. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Plunkett W, Huang P, Xu YZ, Heinemann V,
Grunewald R and Gandhi V: Gemcitabine: Metabolism, mechanisms of
action, and self-potentiation. Semin Oncol. 22:3–10.
1995.PubMed/NCBI
|
|
7
|
Kamisawa T, Wood LD, Itoi T and Takaori K:
Pancreatic cancer. Lancet. 388:73–85. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Woo SM, Lee WJ, Kim JH, Kim DH, Han SS,
Park SJ, Kim TH, Lee JH, Koh YH and Hong EK: Gemcitabine plus
cisplatin versus capecitabine plus cisplatin as first-line
chemotherapy for advanced biliary tract cancer: A retrospective
cohort study. Chemotherapy. 59:232–238. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
El Karak F and Flechon A: Gemcitabine in
bladder cancer. Expert Opin Pharmacother. 8:3251–3256. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ebara S, Kobayashi Y, Sasaki K, Araki M,
Sugimoto M, Wada K, Fujio K, Takamoto A, Watanabe T, Yanai H and
Nasu Y: A case of metastatic urachal cancer including a
neuroendocrine component treated with gemcitabine, cisplatin and
paclitaxel combination chemotherapy. Acta Med Okayama. 70:223–227.
2016.PubMed/NCBI
|
|
11
|
Yu B, Zhou J, Cai H, Xu T, Xu Z, Zou Q and
Gu M: Neoadjuvant chemotherapy for primary adenocarcinomas of the
urinary bladder: A single-site experience. BMC Urol. 15:32015.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Miyata Y, Sagara Y, Matsuo T, Ohba K,
Takahashi H, Sakai H and Kanetake H: Response of recurrent urachal
cancer to gemcitabine and cisplatin therapy: A case report and
literature review. Anticancer Res. 31:2335–2338. 2011.PubMed/NCBI
|
|
13
|
Tran B and McKendrick J: Metastatic
urachal cancer responding to FOLFOX chemotherapy. Can J Urol.
17:5120–5123. 2010.PubMed/NCBI
|
|
14
|
Kikuchi M, Kamei S, Morirama Y, Tuchiya T,
Miwa K, Yokoi S, Nakano M, Ehara H, Deguchi T and Hirose Y: Case of
urachal cancer treated by neoadjuvant chemotherapy with FOLFOX4
(oxaliplatin, 5-FU and leukovolin). Hinyokika Kiyo. 54:557–559.
2008.(In Japanese). PubMed/NCBI
|
|
15
|
Yazawa S, Kikuchi E, Takeda T, Matsumoto
K, Miyajima A, Nakagawa K and Oya M: Surgical and chemotherapeutic
options for urachal carcinoma: Report of ten cases and literature
review. Urol Int. 88:209–214. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yoshida Y, Yamanaka K, Ueda N, Hirai T,
Kishikawa H, Nishimura K and Ichikawa Y: A case of urachal
carcinoma with multiple lung metastases treated by TS-1/CDDP
chemotherapy. Hinyokika Kiyo. 60:147–150. 2014.(In Japanese).
PubMed/NCBI
|
|
17
|
Tian J, Ma JH, Li CL and Xiao ZD: Urachal
mass in adults: Clinical analysis of 33 cases. Zhonghua Yi Xue Za
Zhi. 88:820–822. 2008.(In Chinese). PubMed/NCBI
|
|
18
|
Hasegawa Y, Kato Y, Wakita T, Hayashi N
and Tsukamoto K: Carcinoma of the urachus: A case report. Hinyokika
Kiyo. 51:191–194. 2005.(In Japanese). PubMed/NCBI
|
|
19
|
Zong L and Chen P: Surgical and
chemotherapeutic experience regarding a urachal carcinoma with
repeated relapse: Case report and literature review. World J Surg
Oncol. 11:1702013. View Article : Google Scholar : PubMed/NCBI
|