Introduction
Gastric cancer remains the most common cancer and
the third most frequent cause of cancer death in Japan, although
its incidence and mortality have declined over the years. Early
discovery and subsequent treatment are important for survival in
the case of cancer. Resection of pulmonary metastases for selected
patients with malignancies, such as colorectal cancer and renal
cancer, has been demonstrated as effective (1,2).
However, gastric cancer mainly recurs by spreading
intra-abdominally or as liver metastasis, and solitary pulmonary
metastasis of gastric cancer is rare. As such, the outcome of
metastasectomy is unknown. We therefore aimed to confirm the
effectiveness of pulmonary metastasectomy for gastric cancer.
Gastric cancer remains the most common cancer and
the third most frequent cause of cancer death in Japan, although
its incidence and mortality have declined over the years.
Demographic trends differ by tumor location and histology. While
there has been a marked decline in distal, intestinal type gastric
cancers, the incidence of proximal, diffuse type adenocarcinomas of
the gastric cardia has been increasing, particularly in Japan.
Prognosis of unresectable, metastatic gastric cancer is still low
and five-year survival rate for unresectable, metastatic gastric
cancer is about 5–20%, with median overall survival being less than
1 year (1). Early discovery and
subsequent treatment are important for survival in the case of
gastric cancer.
Pulmonary metastasis usually occurs at advanced
stages of malignancies, however resection of pulmonary metastases
for selected patients with malignancies, such as colorectal cancer
and renal cancer, has been demonstrated as effective (2,3).
However, gastric cancer mainly recurs by spreading
intra-abdominally or as liver metastasis, and pulmonary metastasis
of gastric cancer is very rare. Koga et al (4) reported 7 (0.5%) pulmonary metastases in
1,314 gastric cancer patients and Kong et al (5), reported 193 (0.96%) pulmonary
metastasis in 20,187 gastric cancer patients. Moreover,
approximately 80% of patients with lung metastasis had concomitant
metastasis to other organs such as peritoneum, liver and bone
(5). As such, the outcome of
resection of pulmonary metastasis have not been extensively
studied. We therefore aimed to confirm the effectiveness of
pulmonary metastasectomy for gastric cancer.
Patients and methods
We retrospectively reviewed the preoperative data
and clinical courses of patients who underwent pulmonary resection
for metastasis from gastric cancer at our institution between July
1986 and December 2017. Ten patients underwent pulmonary resection
and a total of 1,714 patients underwent gastrectomy for gastric
cancer during the period. The study protocol was examined and
approved by the Ethics Committee of Tokyo Metropolitan Cancer and
Infectious Diseases Center Komagome Hospital. The pulmonary lesions
were detected on chest computed tomography (CT) or plain chest
X-ray. In general, we used Thomford's criteria for resection of
pulmonary metastases (6). Positron
emission tomography/computed tomography (PET/CT) was used to detect
extrapulmonary metastases, thereby preventing needless surgery. We
reviewed the medical records and collected the following data:
Operative record, pathological data, induction and/or adjuvant
therapy record, and concomitant sites other than the lung. The TNM
classification for stomach tumors was based on the 3rd edition of
the Japanese Classification of Gastric Carcinoma (JCGC) (7).
The median follow-up period of the patients after
the pulmonary metastasectomy was 59 months (range, 3–156 months).
Overall survival (OS) was defined as the interval between the date
of pulmonary resection of lung metastases and the date of death
from any cause or the date of the last follow-up visit. The
disease-free survival (DFS) time was defined as the interval
between the date of gastric surgery and the date of recurrence. OS
was estimated using the Kaplan-Meier product method. The
statistical analyses were performed with EZR (Saitama Medical
Center, Jichi Medical University, Saitama, Japan), which is a
graphical user interface for R (The R Foundation for Statistical
Computing, Vienna, Austria) (8).
Results
Clinicopathological characteristics in
primary gastric cancer
The clinicopathological features of patients with
primary gastric cancer are summarized in Table I. There were 7 males and 3 females,
and the mean age was 70.5 years (range, 53–82 years). Macroscopic
features of gastric cancer were type 2 for 7 patients, type 3 for 2
patients and 0-IIc for 1 patient. Macroscopic features of type 2
tumors represent ulcerated tumors with raised margins surrounded by
a thickened gastric wall with clear margins and type 3 tumors
represent ulcerated tumors without clear margins. Type 0-IIa tumors
represent slightly elevated tumors (7). Among these patients, 40% had N1
disease, 30% had N0, 20% had N3 and 10% had N2. Five patients
underwent total gastrectomy and the others underwent distal
gastrectomy. Lymphatic permeation was observed in 9 and vascular
invasion in 7. Five patients received adjuvant chemotherapy (S-1
for 2, 5-fluorouracil/cisplatin for 1 and 5-fluorouracil/leucovorin
for 1; the other was not described specifically). The patient #2
had a synchronous lung metastasis of gastric cancer and the median
DFS was 34.5 months (range, 0–59 months).
 | Table I.Clinicopathological features of
patients with primary gastric cancer. |
Table I.
Clinicopathological features of
patients with primary gastric cancer.
| No. | Sex | Age (years) | Types of
gastrectomy | Macroscopic type | Histological
type | pT | pN | ly | v | Chemotherapy after
gastrectomy | Disease-free interval
(months) |
|---|
| 1 | Male | 82 | Total | 2 | Tub1 | SS (T3) | 0 | 1 | 2 | – | 19 |
| 2 | Female | 76 | Total | 2 | Tub1 | SS (T3) | 1 | 1 | 1 | – | 0 |
| 3 | Female | 63 | Total | 2 | Pap | SI (T4b) | 1 | 3 | 1 | 5-FU+CDDP | 49 |
| 4 | Male | 70 | Distal | 2 | Pap | MP (T2) | 0 | 0 | 3 | – | 59 |
| 5 | Male | 53 | Distal | 3 | Tub1 | SS (T3) | 1 | 3 | 0 | 5-FU+l-LV | 48 |
| 6 | Female | 55 | Total | 2 | Tub2 | SS (T3) | 1 | 2 | 0 | + (unspecified) | 24 |
| 7 | Male | 71 | Total | 0-IIc | Tub2 | SM (T1b) | 0 | 1 | 0 | – | 45 |
| 8 | Male | 81 | Distal | 2 | Pap | SS (T3) | 2 | 1 | 1 | – | 7 |
| 9 | Male | 72 | Distal | 2 | Tub2 | SE (T4a) | 3 | 1 | 3 | S-1 | 14 |
| 10 | Male | 63 | Distal | 3 | Tub2 | SI (T4b) | 3 | 1 | 2 | S-1 | 51 |
Surgical outcomes for pulmonary
metastases of gastric cancer
Surgical outcomes for pulmonary metastases from
gastric cancer are summarized in Table
II. All patients had solitary pulmonary lesions and the median
tumor size was 1.9 cm (range, 0.8–5.2 cm). Of the 10 thoracotomies,
5 were lobectomy, 3 were wedge resection and 2 were segmentectomy.
Tumor recurrence occurred in several organs in 3 patients after
pulmonary metastasectomy. One patient had lung recurrence, 1 had
liver metastasis and 1 had left ilium metastasis.
| Table II.Surgical outcomes of patients with
pulmonary metastases from gastric cancer. |
Table II.
Surgical outcomes of patients with
pulmonary metastases from gastric cancer.
| No. | Diagnosis before
pulmonary resection | Size of resected
nodule (cm) | Mode of pulmonary
resection | Chemotherapy after
resection | Prognosis after
pulmonary resection | Cause of death |
|---|
| 1 | Primary lung
cancer | 5.2 | Lobectomy | – | Died at 3 months | Pneumonia |
| 2 | Primary lung
cancer | 3.2 | Lobectomy | – | Died at 59
months | Unknown |
| 3 | Metastasis of gastric
cancer | 1.6 | Segmentectomy | – | Alive at 76
months |
|
| 4 | Metastasis of gastric
cancer | 2.5 | Segmentectomy | – | Alive at 156
months |
|
| 5 | Primary lung
cancer | 1.8 | Partial
resection | S-1 | Alive at 143
months |
|
| 6 | Primary lung
cancer | 2.4 | Lobectomy | S-1 | Alive at 5
months |
|
| 7 | Primary lung
cancer | 1.8 | Lobectomy | – | Died at 56
months | Pneumonia |
| 8 | Primary lung
cancer | 2 | Partial
resection | – | Died at 7
months | Pulmonary
metastasis |
| 9 | Primary lung
cancer | 0.8 | Lobectomy | – | Died at 8
months | Liver
metastasis |
| 10 | Primary lung
cancer | 1.2 | Partial
resection | S-1 | Alive at 42
months |
|
Prognosis of pulmonary metastasectomy
of gastric cancer
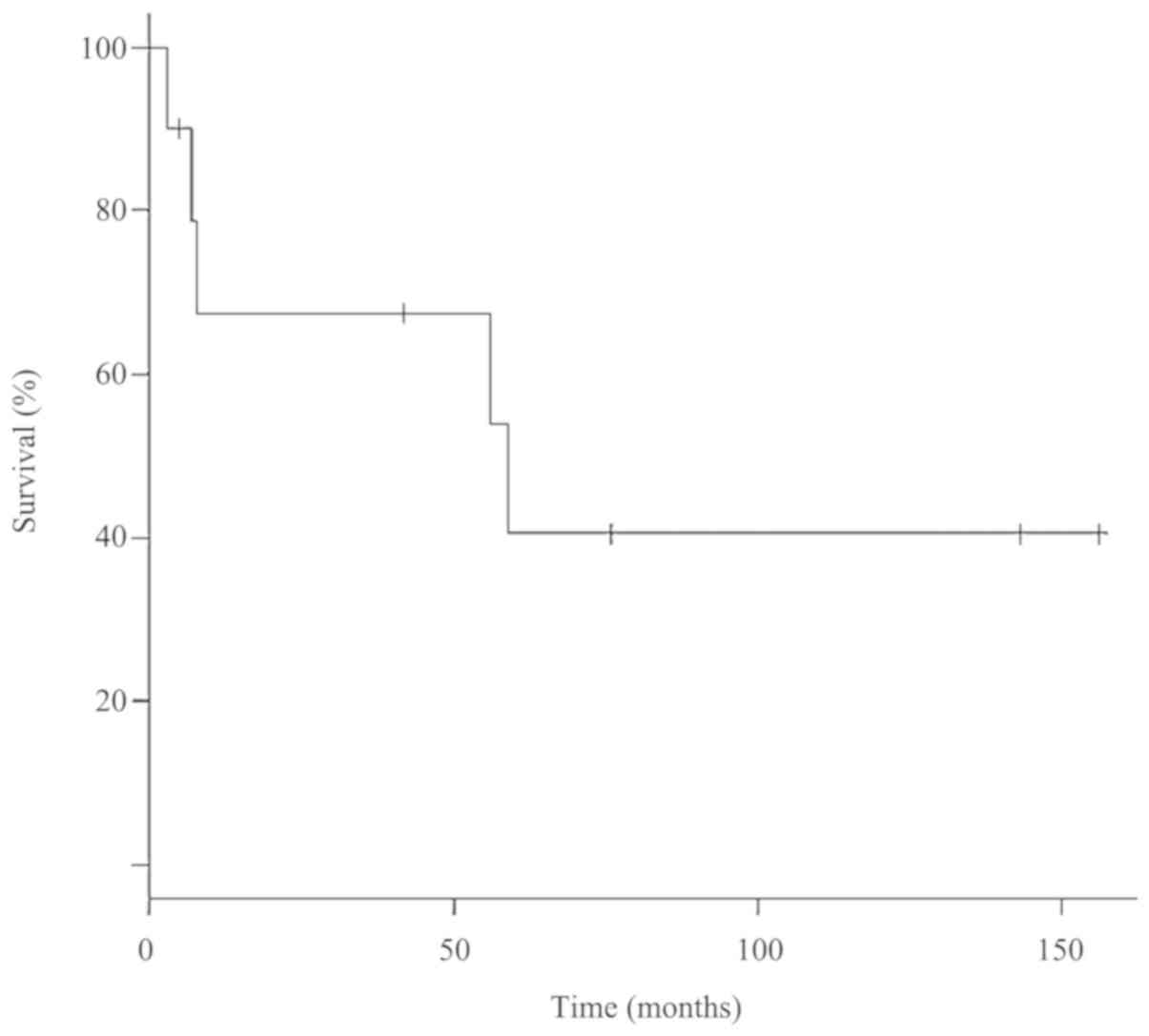
The OS after pulmonary metastasectomy is shown in
Fig. 1. The median OS of the 10
patients was 59 months and the 5-year survival rate was 40.5%. The
median OS was 42 months in patients with chemotherapy after
pulmonary resection and 56 months in those without
chemotherapy.
Discussion
Pulmonary metastasectomy has become a therapeutic
option for metastases of gastrointestinal tumors. In colon and
rectal cancers, indications for pulmonary metastasectomy include:
i) feasible R0 resection; ii) the patient can tolerate pulmonary
resection; iii) control of the primary tumor is warranted; and iv)
absence of extrathoracic lesions (9). However pulmonary metastasis of gastric
cancer is often unresectable because of metastatic forms such as
lymphagitic carcinomatosis and carcinomatous pleuritis (10). The incidence of pulmonary metastases
from gastric cancer ranges from 19.4 to 52.4% based on autopsy
cases (11,12). On the other hand, resectable solitary
pulmonary metastases have only been identified in 0.1% of patients
who have undergone curative resection of gastric cancer (13).
Thus far, it has been reported that lymphatic
permeation is more important than vascular invasion in pulmonary
metastases from gastric cancer (13). In our patients, the most common
histopathological feature of gastric wall invasion was that the
tumor invaded deeper than the serosa with lymphatic permeation.
Although the median survival after diagnosis of
pulmonary metastasis is 4 months, and even in patients treated by
chemotherapy alone, the reported 5-year survival rate is only 2–4%
(5,14,15),
pulmonary resection for selected patients with solitary metastasis
was reported to provide a relatively favorable outcome (16,17). The
median OS differed between the groups with and without
chemotherapy. Chemotherapy following surgery may be able to prolong
the OS; however, our study included only a small number of patients
and one patient who received chemotherapy after pulmonary resection
(patient no. 6) was referred back to their family doctor. Thus, it
is unclear whether chemotherapy after resection can improve the
prognosis.
Solitary pulmonary metastases from gastric cancer
after complete resection are difficult to diagnose before pulmonary
resection. Kobayashi et al (18), reported that a short tumor doubling
time and a low tumor disappearance rate are useful for
preoperatively distinguishing metastatic gastric cancer from
primary adenocarcinoma of the lung. Regardless of radiological
findings, solitary pulmonary lesions detected after curative
resection of gastric cancer are occasionally difficult to diagnose.
Surgical resection is the most reliable way to differentiate
metastases from primary lung cancer. These two entities differ
greatly in their prognosis and an exact histological diagnosis is
essential.
Some limitations exist in this study. First, the
study was retrospective small cases and we should collect more
datas. Second, we selected patients who had only solitary lung
metastasis, causing a selection bias. If patients have multiple
metastases, it becomes difficult to choose surgical treatment
instead of systematic therapy. Third, some patients did not receive
adjuvant chemotherapy even though they had advanced cancer. If they
had all received the same regimen, the DFS, mode of pulmonary
resection and prognosis may have improved.
We conclude that pulmonary resection for metastasis
of gastric cancer may be an effective therapeutic option when there
is a solitary metastatic lesion.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets obtained and/or analyzed during the
present study are available from the corresponding author on
reasonable request.
Authors' contributions
YO, MO and HH analyzed patient data and wrote the
manuscript. TY, AA and MH collected the data and critically revised
the manuscript.
Ethics approval and consent to
participate
This original article was approved by the
institutional review board, and written informed consent was
obtained from all the patients.
Patient consent for publication
Written consent for publication was obtained from
all the patients.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
CT
|
computed tomography
|
|
PET/CT
|
positron emission tomography/computed
tomography
|
|
JCGC
|
the Japanese Classification of Gastric
Carcinoma
|
|
OS
|
overall survival
|
|
DFS
|
disease-free survival
|
References
|
1
|
Kamangar F, Dores GM and Anderson WF:
Patterns of cancer incidence, mortality, and prevalence across five
continents: Defining priorities to reduce cancer disparities in
different geographic regions of the world. J Clin Oncol.
24:2137–2150. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lin BR, Chang TC, Lee YC, Lee PH, Chang KJ
and Liang JT: Pulmonary resection for colorectal cancer metastases:
Duration between cancer onset and lung metastasis as an important
prognostic factor. Ann Surg Oncol. 16:1026–1032. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bölükbas S, Kudelin N, Eberlein M,
Fisseler-Eckhoff A and Schirren J: The influence of the primary
tumor on the long-term results of pulmonary metastasectomy for
metastatic renal cell carcinoma. Thorac Cardiovasc Surg.
60:390–397. 2012.PubMed/NCBI
|
|
4
|
Koga S, Takebayashi M, Kaibara N, Nishidoi
H, Kimura O, Kawasumi H and Makino M: Pathological characteristics
of gastric cancer that develop hematogenous recurrence, with
special reference to the site of recurrence. J Surg Oncol.
36:239–242. 1987. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kong JH, Lee J, Yi CA, Park SH, Park JO,
Park YS, Lim HY, Park KW and Kang WK: Lung metastases in metastatic
gastric cancer: Pattern of lung metastases and clinical outcome.
Gastric Cancer. 15:292–298. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Thomford NR, Woolner LB and Clagett OT:
The surgical treatment of metastatic tumor in the lung. J Thoracic
Cardiovasc Surg. 49:357–363. 1965.
|
|
7
|
Sano T and Aiko T: New Japanese
classifications and treatment guidelines for gastric cancer:
Revision concepts and major revised points. Gastric Cancer.
14:97–100. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kanda Y: Investigation of the
freely-available easy-to-use software EZR for medical statistics.
Bone Marrow Transplant. 48:452–458. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
NCCN clinical practice guidelines in
Oncology, Colon Cancer. http://www.nccn.org/professionals/physician_gls/pdf/colon.pdf13–March.
2017
|
|
10
|
Nakayama H1, Ichinose S, Kato Y, Ito H,
Masui K and Kameda Y: Long-term survival after a surgical resection
of pulmonary metastases from gastric cancer: report of a case. Surg
Today. 38:150–153. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Dupont JB Jr, Lee JR, Burton GR and Cohn I
Jr: Adenocarcinoma of the stomach: Review of 1,497 cases. Cancer.
41:941–947. 1978. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ishii T, Ikegami N, Hosoda Y, Koide O and
Kaneko M: The biological behavior of gastric cancer. J Pathol.
134:97–115. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kanemitsu Y, Kondo H, Katai H, Nakayama H,
Asamura H, Tsuchiya R and Naruke T: Surgical resection of pulmonary
metastases from gastric cancer. J Surg Oncol. 69:147–150. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ohkuwa M, Ohtsu A, Boku N, Yoshida S,
Miyata Y, Shirao K, Shimada Y and Kurihara M: Long-term results for
patients with unresectable gastric cancer who received chemotherapy
in the Japan Clinical Oncology Group (JCOG) trials. Gastric Cancer.
3:145–150. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yoshida M, Ohtsu A, Boku N, Miyata Y,
Shirao K, Shimada Y, Hyodo I, Koizumi W, Kurihara M, Yoshida S and
Yamamoto S: Long-term survival and prognostic factors in patients
with metastatic gastric cancers treated with chemotherapy in the
Japan Clinical Oncology Group (JCOG) study. Jpn J Clin Oncol.
34:654–659. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Nakayama H, Ichinose S, Kato Y, Ito H,
Masui K and Kameda Y: Long-term survival after a surgical resection
of pulmonary metastases from gastric cancer: Report of a case. Surg
Today. 38:150–153. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ogura M, Tanaka N, Furuya T, Nomura Y,
Nagai M, Takahashi M, Takayama T, Hirao H, Nakamura H and Suzuki Y:
A case of long-term survival after undergoing S-1 treatment and
splenectomy for liver, lung and splenic metastases following
curative distal gastrectomy for gastric cancer. Gan To Kagaku
Ryoho. 37:1125–1129. 2010.(In Japanese). PubMed/NCBI
|
|
18
|
Kobayashi Y, Fukui T, Ito S, Shitara K,
Ito S, Hatooka S and Mitsudomi T: Pulmonary metastasectomy for
gastric cancer: A 13-year single-institution experience. Surg
Today. 43:1382–1389. 2013. View Article : Google Scholar : PubMed/NCBI
|