Introduction
Exposure to asbestos is known to increase the
incidence of mesothelioma as well as that of lung cancer; however,
reports of cases of double cancers comprising these two cancer
types are rare (1).
The efficacy of radiotherapy for multimodal
treatment of mesothelioma and lung cancer has been reported
previously (2). However, only few
reports have described the use of radiotherapy for two different
tumors in the same patient.
In the present study, we report the case of a
patient with double cancer comprising malignant pleural
mesothelioma and squamous cell lung cancer, in whom radiotherapy
used to treat the lung cancer may have helped control the
progression of the malignant pleural mesothelioma. This case is
reported together with a discussion of the literature, as it
provides valuable insight into the future positioning of
radiotherapy in multimodal therapy for malignant pleural
mesothelioma.
Case report
The patient was a 75-year-old man with a history of
early gastric cancer who was employed at a cement factory, with a
history of exposure to asbestos from the age of 25 to 40 years.
The patient was first seen at the asbestos center of
our hospital in November 2005 for a Hyogo Labor Bureau Asbestos
Examination in accordance with the patient's Asbestos Health
Monitoring Handbook; thereafter, he underwent periodic examinations
for pulmonary asbestosis and bilateral pleural thickening.
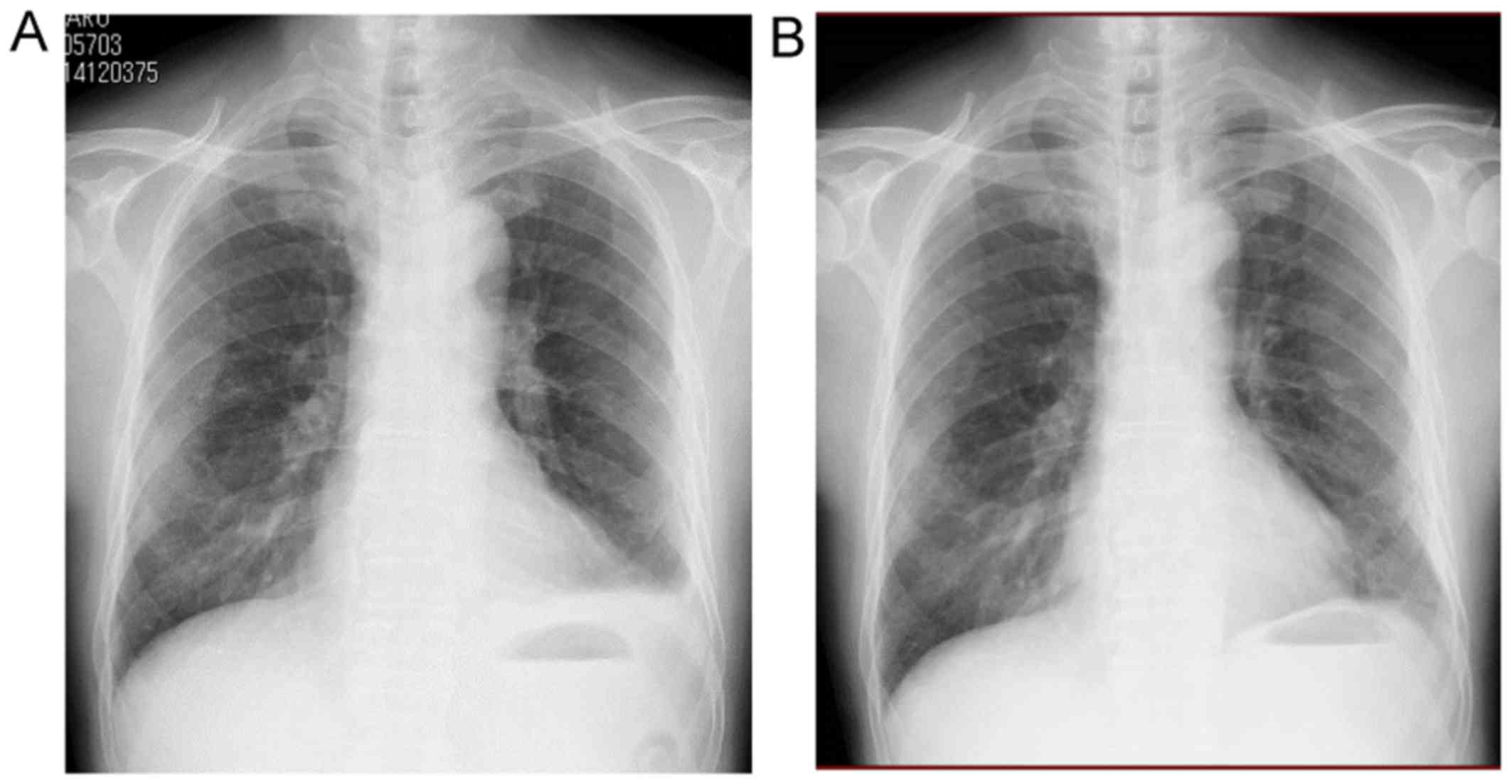
In October 2009, chest radiography (Fig. 1A) revealed left pleural effusion that
had not been present on the previous (March 2009) chest radiography
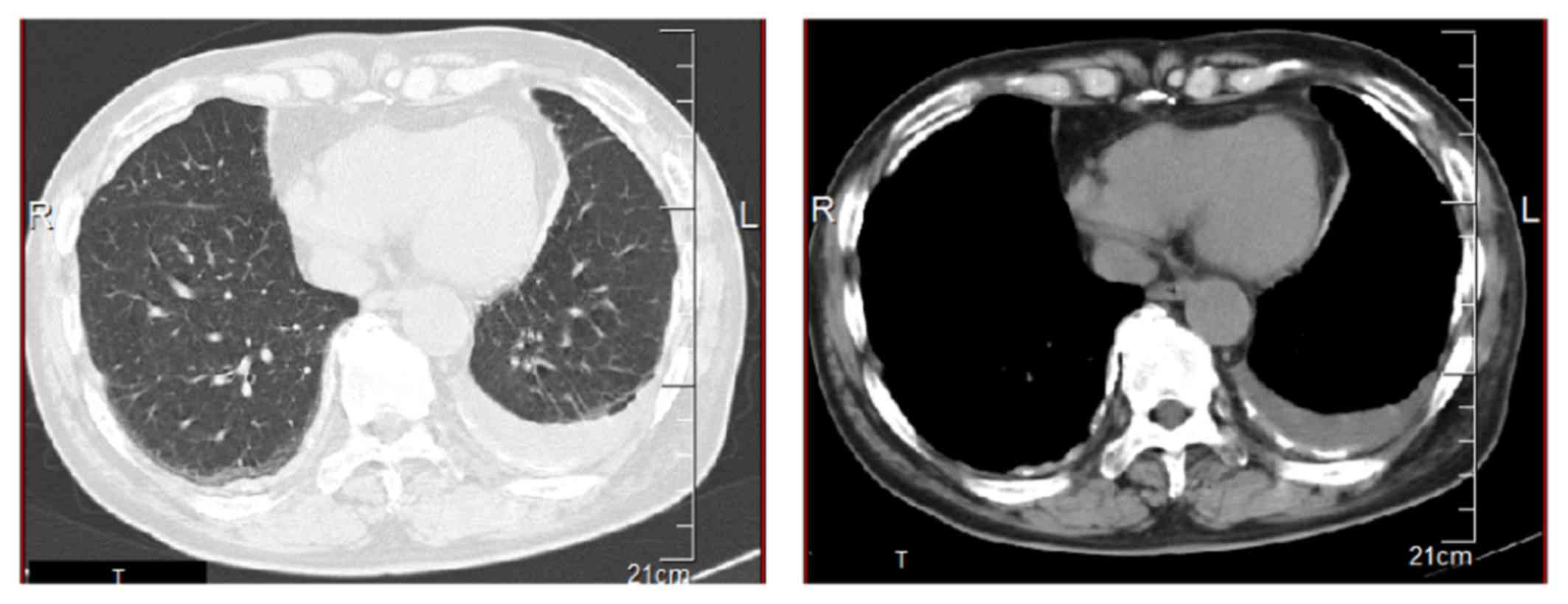
images (Fig. 1B). However, chest
computed tomography (CT) revealed no worsening of the pleural
lesions; thus, a strategy of follow-up observation was selected
(Fig. 2). Approximately 3 months
later, the patient developed exertional dyspnea, and the left
pleural effusion worsened over time; therefore, the pleural
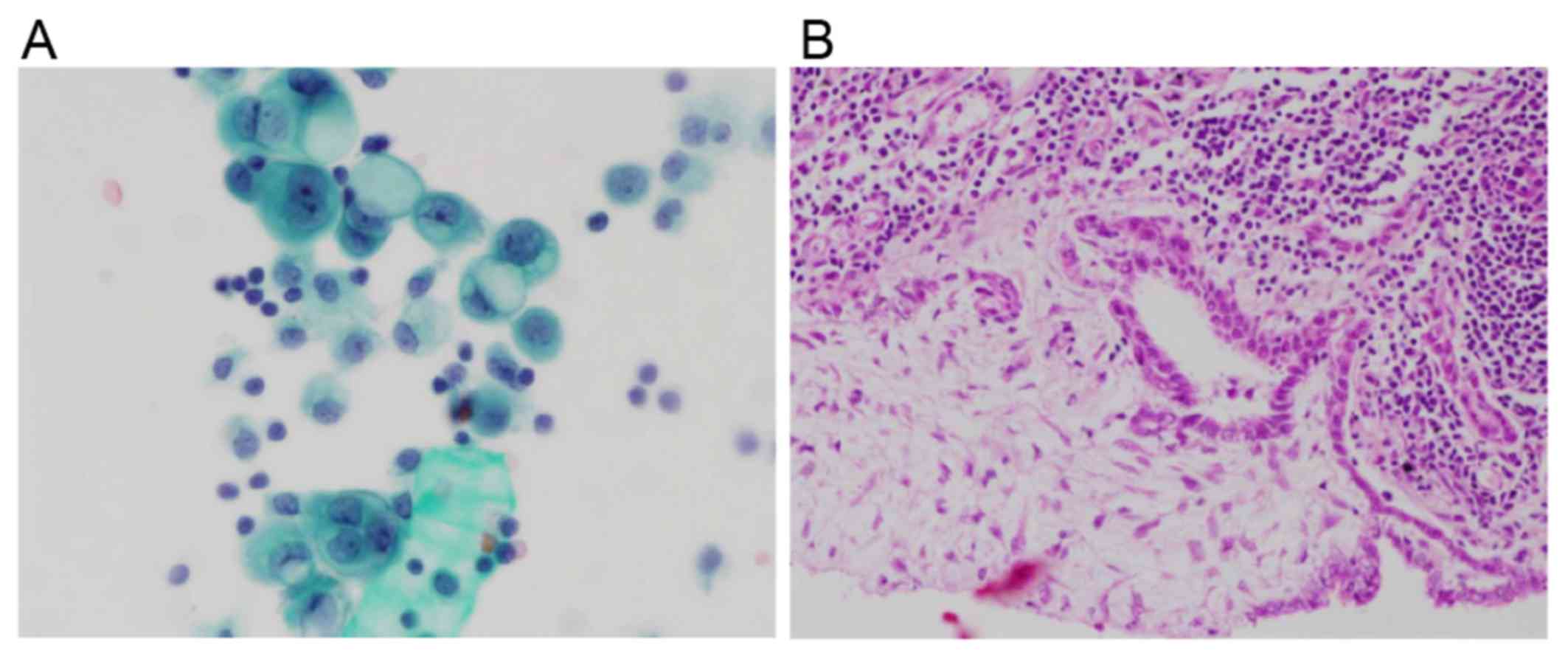
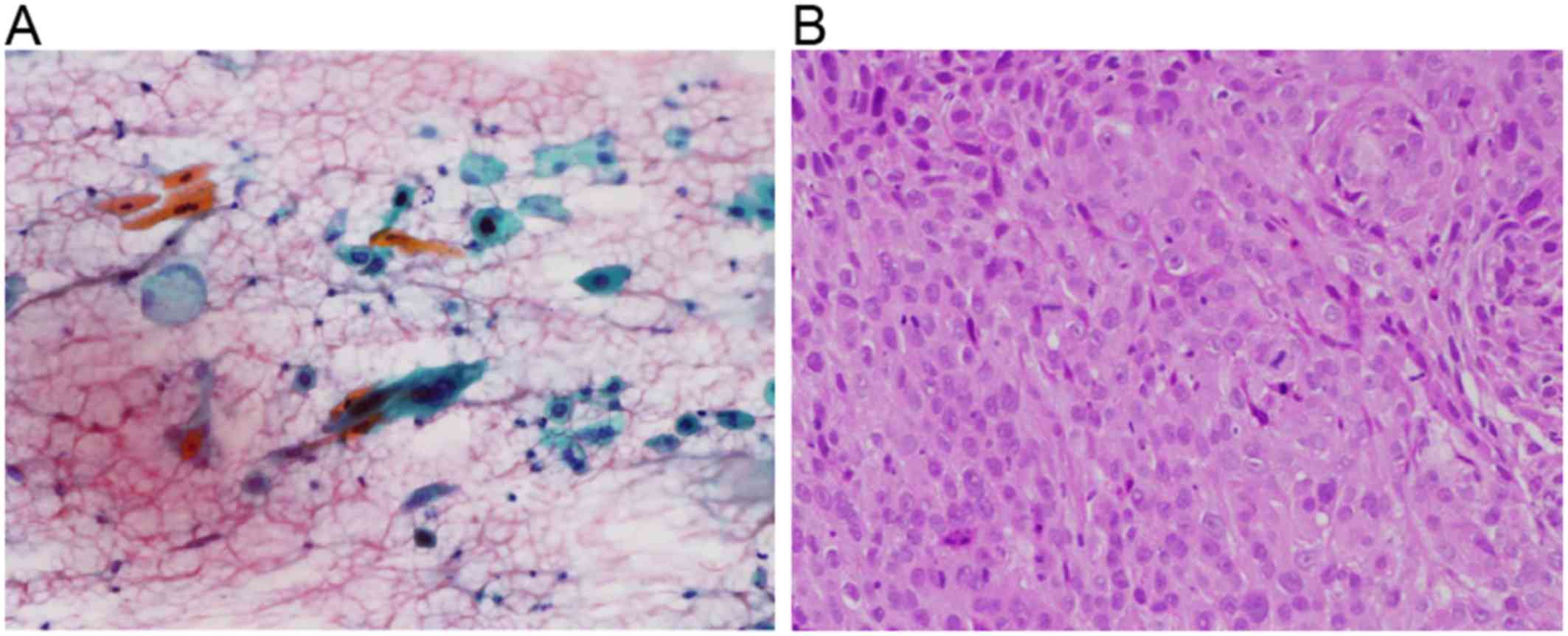
effusion was aspirated and subjected to cytological examination.
Cytological examination detected class V malignant mesothelioma
(Fig. 3A). In February 2010, the
patient underwent a pleural surgical biopsy under general
anesthesia and was diagnosed with malignant pleural mesothelioma,
International Mesothelioma Interest Group classification cT1aN0M0,
stage 1A (Fig. 3B). The patient was
not a candidate for extrapleural pneumonectomy (EPP) due to the
impaired pulmonary function caused by pulmonary asbestosis and
chronic obstructive pulmonary disease; therefore, a strategy of
chemotherapy alone was selected, and the patient was administered
cisplatin (75 mg/m2 on day 1 then every 21 days) plus
pemetrexed (500 mg/m2 on day 1 then every 21 days) from
April 2010 onwards. After completing four courses of chemotherapy,
the left pleural effusion improved and stable disease was
achieved.
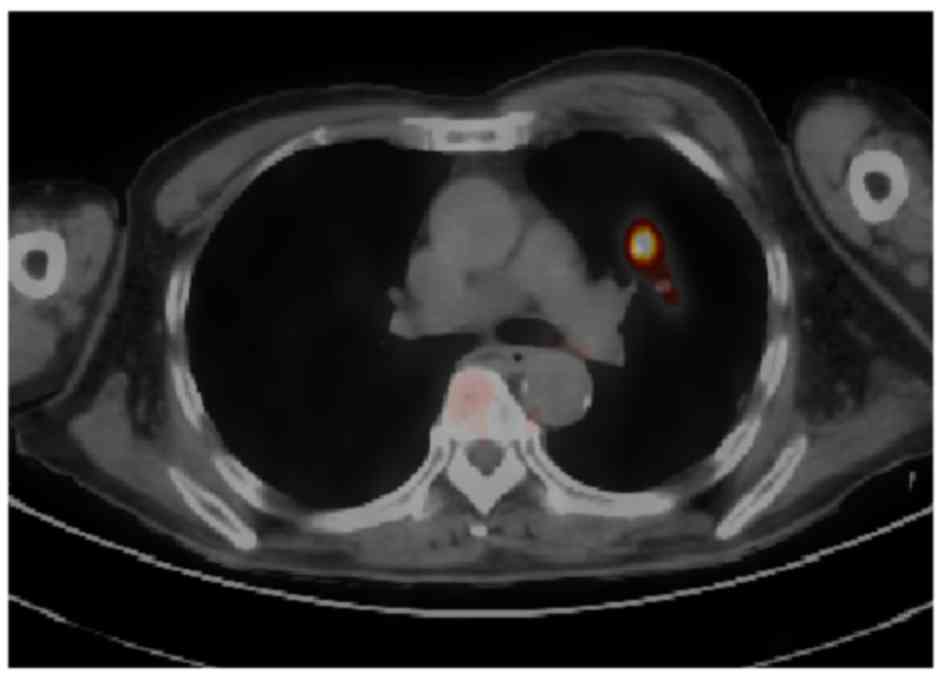
In February 2011, fluorodeoxyglucose (FDG) positron
emission tomography (PET)/CT revealed the emergence of 20-mm
nodular shadows with irregular margins in two locations, with FDG
uptake in the S3 of the left lung (Fig.
4).
The patient was admitted to our department for
detailed examination and treatment. Upon admission, right-sided
hemiparesis caused by the after-effects of a left cerebral
infarction was observed; the superficial lymph nodes were not
palpable. On auscultation, a fine crackle was heard in the
posterior portion of both lower lung fields. There was no digital
clubbing, and the SpO2 was 95% (room air).
The laboratory findings upon admission are listed in
Table I. All blood cell counts and
biochemical tests were normal. The KL-6 levels were mildly elevated
to 638 U/ml (normal, <500 U/ml). The tumor markers
carcinoembryonic antigen, squamous cell carcinoma (SCC) antigen,
cytokeratin-19 fragments and pro-gastrin-releasing peptide were all
within the normal ranges.
 | Table I.Laboratory findings upon
admission. |
Table I.
Laboratory findings upon
admission.
| Tests | Values | Units |
|---|
| Total protein | 6.9 | g/dl |
| Albumin | 4.0 | g/dl |
| Total bilirubin | 0.4 | mg/dl |
| AST | 24 | U/l |
| ALT | 37 | U/l |
| LDH | 163 | U/l |
| ALP | 321 | U/l |
| γGTP | 46 | U/l |
| BUN | 10 | mg/dl |
| Creatinine | 0.64 | mg/dl |
| Na | 139 | mmol/l |
| K | 3.6 | mmol/l |
| Cl | 101 | mmol/l |
| Ca | 8.9 | mg/dl |
| CRP | 5.8 | mg/dl |
| WBC count | 5,910 | /µl |
| RBC count | 476 |
x104/µg |
| Hb | 13.4 | g/dl |
| HCT | 37.9 | % |
| MCV | 79.6 | fl |
| MCHC | 35.4 | pg |
| PLT count | 27.1 |
x104/µg |
| KL-6 | 638 | U/ml |
| CEA | 1.4 | ng/ml |
| SCC | 1.1 | ng/ml |
| CYFRA | <1.0 | ng/ml |
| ProGRP | 31.8 | pg/ml |
Chest radiography revealed two 15-mm nodular shadows
with irregular margins in the left central lung field. The images
showed circumferential pleural thickening and partial coverage by
pleural plaques. Chest contrast-enhanced CT revealed a reticulate
shadow in both lung fields; scattered nodular shadows with a
centrilobular distribution were observed. Two 20-mm nodular shadows
with irregular margins were detected in S3 of the left lung
(Fig. 5A). Pleural plaques and
pleural thickening were observed bilaterally, along with thickening
of the left interlobular pleura. Contrast enhancement was evident,
and exacerbation of the mesothelioma lesions was suspected
(Fig. 5B).
Following admission, the left S3 nodular shadows
were examined by bronchoscopy, and a diagnosis of SCC (cT3N0M0
stage IIA) was confirmed (Fig. 6).
Thus, the patient was diagnosed with a double cancer comprising
malignant pleural mesothelioma and SCC. He was not considered to be
a candidate for surgery due to the impaired pulmonary function;
therefore, chemoradiotherapy with vinorelbine (10 mg/m2
on day 1 then every 7 days) and radiotherapy (60 Gy in 20 fractions
at 3 Gy per fraction) were administered. The patient was discharged
without complications on day 59 after admission. Although the
patient later developed a treatment-related complication (grade II
radiation pneumonitis), the primary tumor was well-controlled.
In September 2011, FDG PET/CT revealed the emergence
of a new 20-mm nodular shadow with irregular margins and FDG uptake
in the left S8. Since the left S3 primary tumor was
well-controlled, this was not considered a recurrence, but a second
primary cancer was suspected. On November 2011, bronchoscopy was
performed, and the diagnosis of SCC (cT1bN0M0 stage IA) was
confirmed.
As the patient still suffered from grade II
radiation pneumonitis, radiotherapy for the S8 lesion was deemed
high-risk, and it was decided that chemotherapy would be
implemented after the radiation pneumonitis had subsided.
While waiting for the radiation pneumonitis to
subside, in March 2012, docetaxel chemotherapy was started (60
mg/m2 on day 1 then every 21 days), but the disease
activity of the S8 lesion was worse after four courses. In October
2012, chemotherapy was changed to four courses of gemcitabine
(1,000 mg/m2 on days 1, 8 and 15 then every 28 days).
However, the pathological status of the patient worsened, and he
eventually succumbed to lung cancer in November 2013.
Discussion
Malignant pleural mesothelioma (3) and lung cancer (4) are typical malignancies of the chest
caused by asbestos exposure. In Japan, cases of malignant
mesothelioma and asbestos-related lung cancer have been increasing
due to the effects of asbestos that was extensively used in the
past. The prognosis of malignant pleural mesothelioma is extremely
dismal, with poor treatment outcomes. The efficacy of treatment is
low, even when the disease is diagnosed at an early clinical
stage.
A variety of multimodal treatment approaches,
combining chemotherapy, surgery and radiotherapy, have been used.
Trimodal therapy consisting of preoperative chemotherapy, EPP and
postoperative hemithoracic radiotherapy, was reported to be
effective in the treatment of malignant pleural mesothelioma,
although high rates of surgical complications and perioperative
mortality were observed (5). In
contrast to the high incidence of surgical complications and
perioperative mortality reported by Krug et al the MARS
study (6) reported that EPP added no
benefit to trimodal therapy, with other reports showing that
pleurectomy/decortication (P/D) achieves better survival outcomes
compared with EPP (7,8), and indicating the possibility that
treatment outcomes are improved by conserving the lung on the
affected side. Recently, there has been a tendency toward using P/D
reduction surgery in the treatment of early-stage cases of
mesothelioma in which gross complete resection can be obtained.
To date, trimodal therapy has been implemented with
total hemithoracic radiotherapy when EPP was the procedure used
after preoperative chemotherapy. Although thoracic irradiation
following P/D has been reported to have a high feasibility and
efficacy in multimodal treatment for mesothelioma at an early stage
(9), radiotherapy following lung
dose constraints may make radiotherapy after P/D of the affected
lung challenging, and is currently contraindicated after surgery
(10). Therefore, bimodal therapy
(chemotherapy plus surgery) is typically used when P/D is
performed.
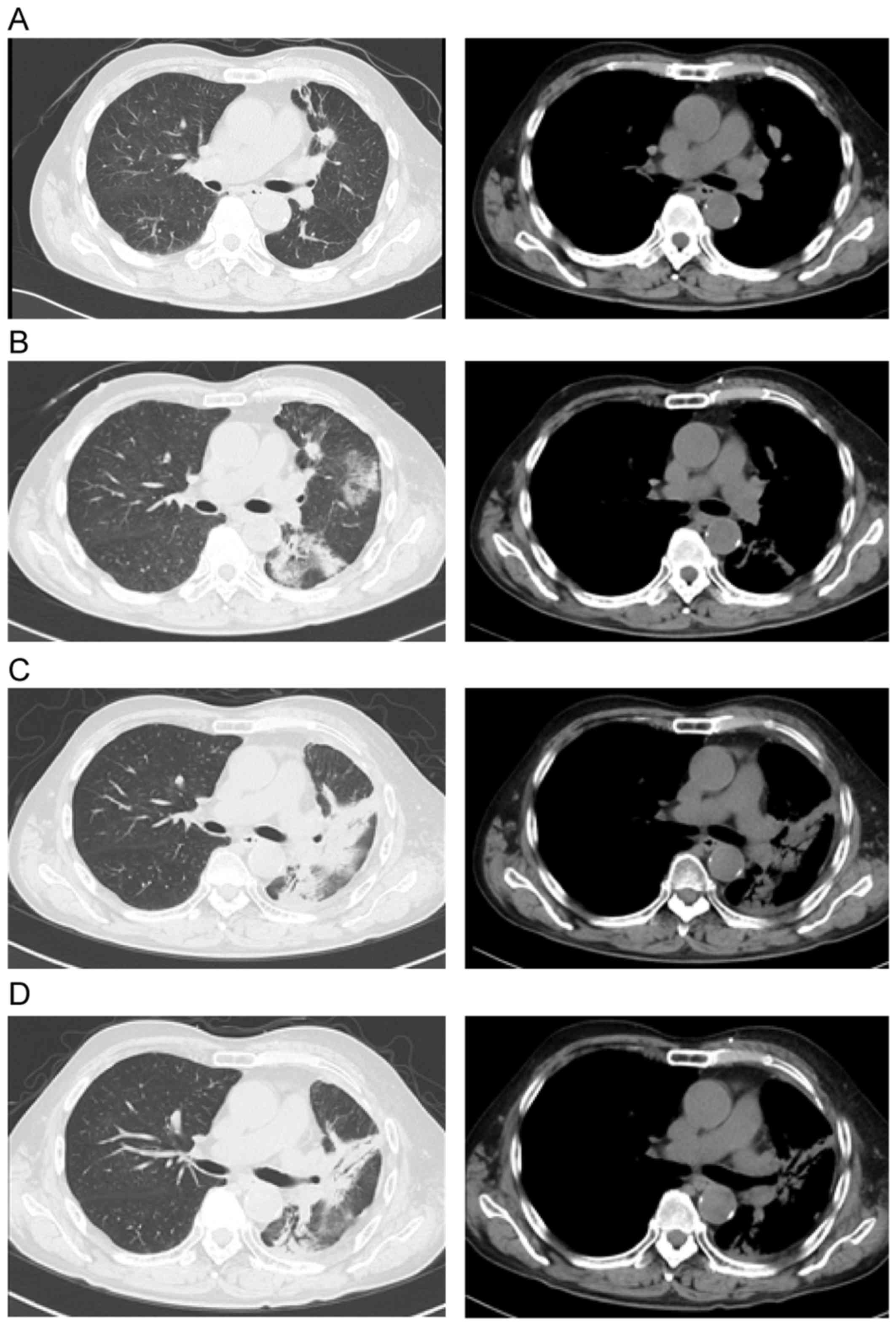
In the present case of double cancer, the patient
developed lung SCC while receiving treatment for malignant pleural
mesothelioma. Our findings suggest that the radical radiotherapy
used for the treatment of the SCC may have also resulted in local
control of the pre-existing malignant pleural mesothelioma,
although only as a side effect (Fig.
7).
The present case confirms the value of radiotherapy
in the treatment of malignant pleural mesothelioma, with only minor
side effects, despite it being a radical and localized treatment
for lung cancer. Since P/D is becoming the prevailing surgical
procedure used in the treatment of early-stage cases of malignant
pleural mesothelioma, a literature search was performed and it was
considered whether radiotherapy could be added to treat the
conserved lung after P/D.
Gupta et al implemented total hemithoracic
radiotherapy of the affected side following P/D in patients with
malignant pleural mesothelioma (median dose, 42.5 Gy; range,
7.2–67.8 Gy), but reported poor results, with a median survival of
12.5 months and a 2-year survival rate of 23% (11). They also reported being unable to
increase the radiation dose to a level sufficient to destroy the
tumor due to radiation-induced toxicity in the residual lung, and
concluded that hemithoracic radiotherapy of the affected side
following P/D was not an effective treatment option (11). However, since the emergence of
intensity-modulated radiotherapy (IMRT), it has been demonstrated
that radical irradiation is possible, even in the treatment of the
conserved lung (12). Minatel et
al performed extended P/D in 35 of 69 patients with malignant
pleural mesothelioma and partial pleurectomy in the remaining 34
patients. After implementing postoperative IMRT (50 Gy/25 fr) with
a simultaneous boost of 60 Gy in 25 fractions (2.4 Gy per fraction)
for residual disease, favorable 2-year survival rates of 65 and
58%, respectively, were achieved in the two groups (13). They also reported that complications
from IMRT did not cause treatment interruptions in any of the
patients; the scheduled irradiation was completed in all patients,
and complications were generally within a tolerable range (13).
In this report, the patient received radiotherapy of
60 Gy in 20 fractions (3 Gy per fraction). This dosing may result
in a similar to slightly greater local effect on mesothelioma in
terms of the biologically effective dose (BED), using the
linear-quadratic model with an assumed α/β ratio of 10 Gy for the
tumor (BED10), since the BED10 is 78 Gy and
74.4 Gy for 60 Gy/20 fr and 60 Gy/25 fr, respectively. Therefore,
we suggest that radiotherapy at a dose >60 Gy may be used as
local therapy in a conventional treatment schedule for mesothelioma
(14).
Favorable outcomes have recently been obtained with
IMRT following P/D. Moreover, an increasing number of reports,
mainly from the USA and Europe, have indicated that this treatment
is well-tolerated by the patients. Radiotherapy is not currently
performed on the conserved lung after P/D in Japan; however, based
on the present case and reports from outside Japan, there appears
to be sufficient grounds to consider the suitability of this
treatment modality.
In conclusion, the present case highlights the
application of radiotherapy in the treatment of malignant
mesothelioma. In addition, the potential of new multimodal
treatments for mesothelioma and a comprehensive review of the
literature are presented.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
YN, HD and NF contributed to the conception of the
work and the acquisition, analysis and interpretation of data. YN
analyzed and interpreted the patient data regarding the
hematological disease. YK, EF and TM performed the histological
examination of the lung and pleura. KK, KM and TM were responsible
for drafting the manuscript and revising it critically for
important intellectual content. TM was a major contributor to
writing the manuscript. KK, TY and TK agree to be accountable for
all aspects of the work in ensuring that questions related to the
accuracy or integrity of any part of the work are appropriately
investigated and resolved. All authors have read and approved the
final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Appropriate written informed consent was obtained
for the publication of this case report and the accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
BED
|
biologically effective dose
|
|
CT
|
computed tomography
|
|
EPP
|
extrapleural pneumonectomy
|
|
FDG
|
fluorodeoxyglucose
|
|
IMRT
|
intensity-modulated radiotherapy
|
|
P/D
|
pleurectomy/decortication
|
|
PET
|
positron emission tomography
|
References
|
1
|
Allen TC and Moran C: Synchronous
pulmonary carcinoma and pleural diffuse malignant mesothelioma.
Arch Pathol Lab Med. 130:721–724. 2006.PubMed/NCBI
|
|
2
|
Perrot M, Wu L, Wu M and Cho BCJ:
Radiotherapy for the treatment of malignant pleural mesothelioma.
Lancet Oncol. 18:e532–e542. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Whitewell F and Rawcliffe RA: Diffuse
malignant pleural mesothelioma and asbestos exposure. Thorax.
26:6–22. 1971. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Doll R: Mortality from lung cancer in
asbestos workers. Brit J Indust Med. 12:81–86. 1955.
|
|
5
|
Krug LM, Pass HI, Rusch VW, Kindler HL,
Sugarbaker DJ, Rosenzweig KE, Flores R, Friedberg JS, Pisters K,
Monberg M, et al: Multicenter phase II trial of neoadjuvant
pemetrexed plus cisplatin followed by extrapleural pneumonectomy
and radiation for malignant pleural mesothelioma. J Clin Oncol.
27:3007–3013. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Treasure T, Lang-Lazdunski L, Waller D,
Bliss JM, Tan C, Entwisle J, Snee M, O'Brien M, Thomas G, Senan S,
et al: Extra-pleural pneumonectomy versus no extra-pleural
pneumonectomy for patients with malignant pleural mesothelioma:
clinical outcomes of the Mesothelioma and Radical Surgery (MARS)
randomized feasibility study. Lancet Oncol. 12:763–772. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Flores RM, Pass HI, Seshan VE, Dycoco J,
Zakowski M, Carbone M, Bains MS and Rusch VW: Extrapleural
pneumonectomy versus pleurectomy/decortications in the surgical
management of malignant pleural mesothelioma: Results in 663
patients. J Thoracic Cardiovasc Surg. 135:620–626. 2008. View Article : Google Scholar
|
|
8
|
Lang-Lazdunski L, Bille A, Lal R, Cane P,
McLean E, Landau D, Steele J and Spicer J:
Pleurectomy/decortication is superior to extrapleural pneumonectomy
in the multimodality management of patients with malignant pleural
mesothelioma. J Thorac Oncol. 7:737–743. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Shaikh F, Zauderer MG, von Reibnitz D, Wu
AJ, Yorke ED, Foster A, Shi W, Zhang Z, Adusumilli PS, Rosenzweig
KE, et al: Improved outcomes with modern lung-sparing trimodality
therapy in patients with malignant pleural mesothelioma. J Thorac
Oncol. 12:993–1000. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Scherpereel A, Astoul P, Baas P, Berghmans
T, Clayson H, de Vuyst P, Dienemann H, Galateau-Salle F, Hennequin
C, Hillerdal G, et al: Guidelines of the european respiratory
society and the european society of thoracic surgeons for the
management of malignant pleural mesothelioma. Eur Respir J.
35:479–495. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gupta V, Mychalczak B, Krug L, Flores R,
Bains M, Rusch VW and Rosenzweig KE: Hemithoracic radiation therapy
after pleurectomy/decortication for malignant pleural mesothelioma.
Int J Radiat Oncol Biol Phys. 63:1045–1052. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Rosenzweig KE, Zauderer MG, Laser B, Krug
LM, Yorke E, Sima CS, Rimner A, Flores R and Rusch V: Pleural
intensity-modulated radiotherapy for malignant pleural
mesothelioma. Int J Radiat Oncol Biol Phys. 83:1278–1283. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Minatel E, Trovo M, Bearz A, Di Maso M,
Baresic T, Drigo A, Barresi L, Furlan C, Del Conte A, Bruschi G, et
al: Radical radiation therapy after lung sparing surgery for
malignant pleural mesothelioma: Survival, pattern of failure and
prognostic factors. Int J Radiation Oncol Biol Phys. 93:606–613.
2015. View Article : Google Scholar
|
|
14
|
Hall EJ and Giaccia AJ: Radiobiology for
the radiologist. 7th ed. Lippincott Williams & Wilkins;
Philadelphia: 2011
|