Introduction
Benign soft tissue tumors with aggressive features
are commonly encountered in clinical practice. When lesions are
found on the toes or digits, one possible differential diagnosis is
superficial acral fibromyxoma, a rare myxoid tumor with few cases
described (1). Among them,
superficial acral fibromyxoma is a relatively uncommon,
slow-progressing, benign tumor. Superficial acral fibromyxoma
sometimes leads to bone erosion, but a case with this
characteristic in a great toe has not yet been reported. Herein, we
describe a very rare clinical case in which such a lesion was
found.
Case report
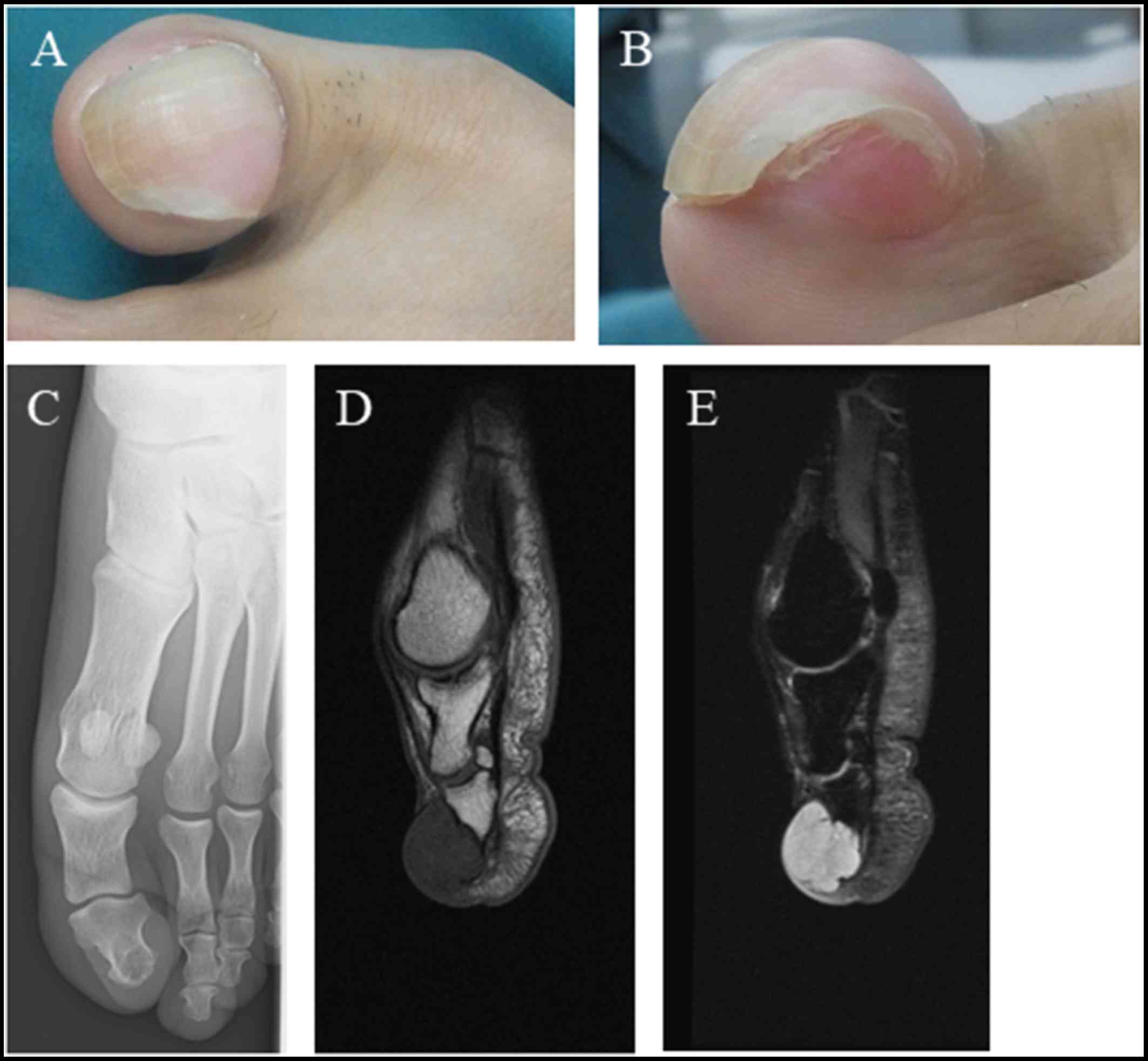
We describe the case of a 37-year-old male
kickboxer, who presented with a lump under the nail of his left
great toe. The lesion had been rapidly growing for the previous 6
months and measured about 2.4×2.7 cm at presentation (Fig. 1A and B). The patient associated the
onset of the lesion with kickboxing, but there had not been any
trauma to the region. When he first noticed the mass, the patient
did not experience any pain; however, he subsequently developed
pain and as a result visited Kindai University Hospital (Osaka,
Japan). Radiographic imaging showed an osteolytic lesion of the
distal phalanx bone (Fig. 1C).
Magnetic resonance imaging (MRI) revealed a T1 low, T2 high
intensity lobular, cyst-like nodule under the nail (Fig. 1D and E). The MRI also showed a tumor
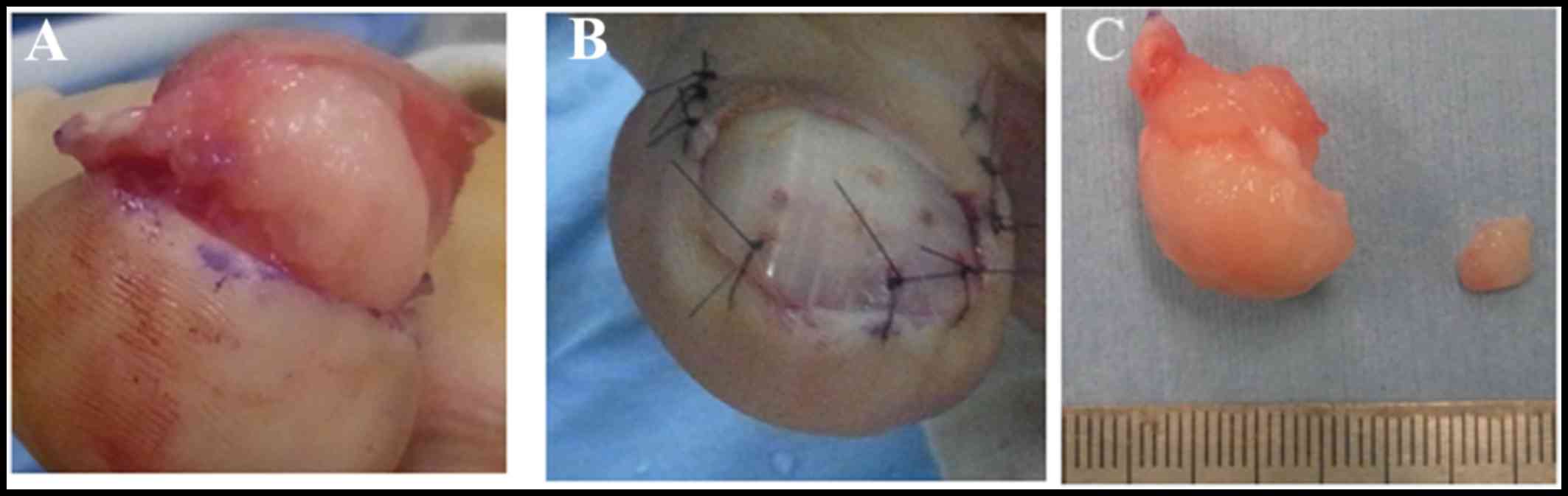
infiltrating the distal phalanx bone. Surgical excision of the
tumor with primary closure was performed, with the purpose
performing a biopsy (Fig. 2A and B).
The tumor was excised piece by piece with transverse skin incision.
The nails, including the nail bed, were preserved. The tumor had
partially invaded to the distal phalanx bone. The lesion had a firm
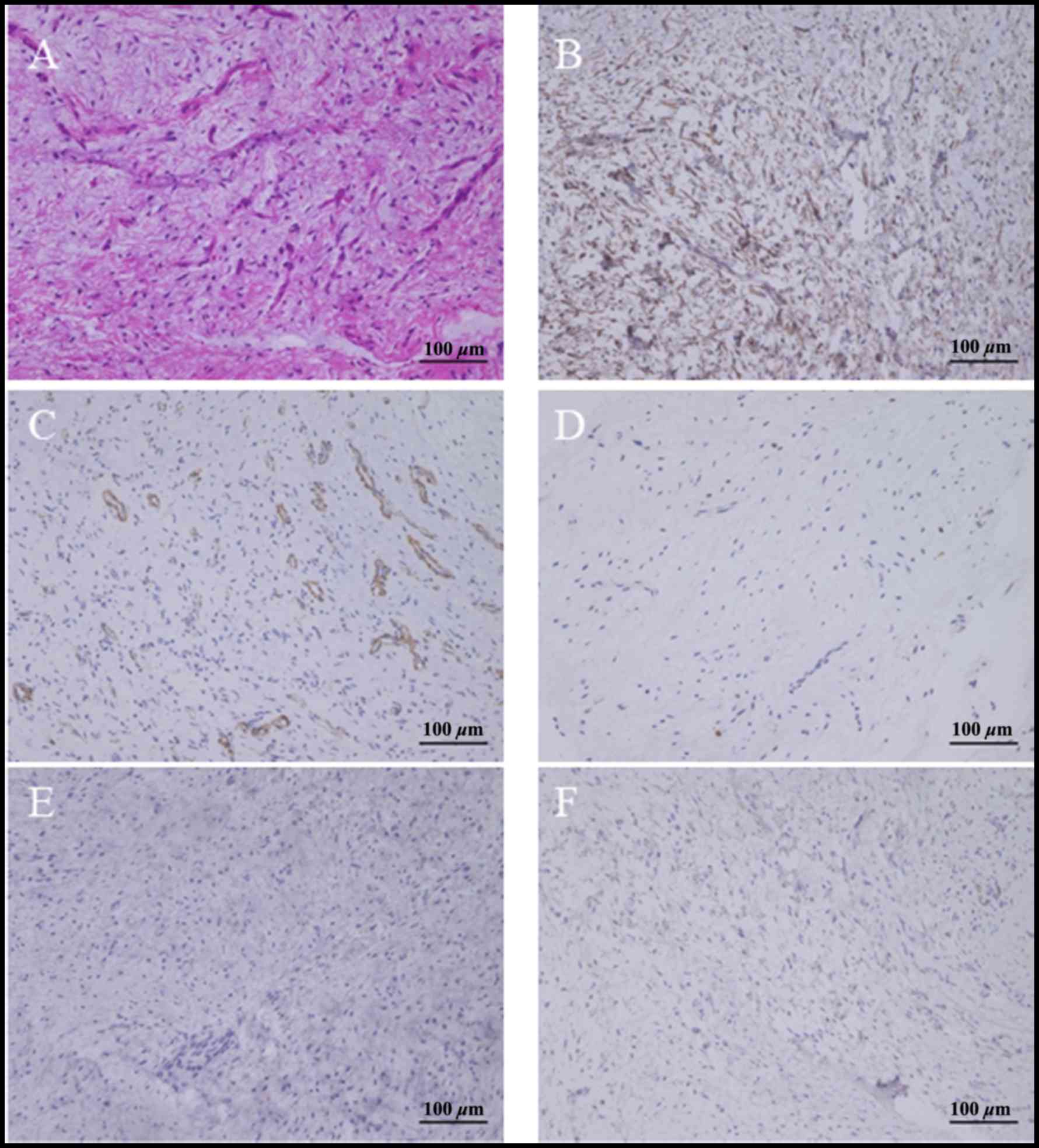
consistency and was a light pink color (Fig. 2C). Histologically, spindle-shaped
cells had proliferated in the myxocollagenous interstitium
(Fig. 3A). No evidence of cellular
atypia or mitotic figures was found. The immunohistochemical study
revealed positivity for CD34 (sc-74499; dilution, 1:100) and
negativity for S100 protein (sc-53438; dilution, 1:200), α-smooth
muscle actin (sc-53142; dilution, 1:200) (all from Santa Cruz
Biotechnology, Dallas, TX, USA), epithelial membrane antigen
(M0613; dilution, 1:400; Dako Corporation, Carpinteria, CA, USA),
and desmin (60226-1-Ig; dilution, 1:50; Cosmo Bio, Tokyo, Japan) in
the neoplastic cells (Fig. 3B-F).
The diagnosis was superficial acral fibromyxoma. At 24 months of
follow-up, the patient had no symptoms or signs of recurrence.
Radiography of the bone after treatment showed no erosive
lesion.
Discussion
Superficial acral fibromyxoma is a very rare soft
tissue tumor that was first described in 2001 by Fetsch et
al (1). It is a slow-growing
tumor (median duration of ~3 years) with a preponderance in men
(male/female ratio of 2:1) and a mean age at presentation of 43
(range, 4–86) years (1,2). The most frequently affected sites are
the subungual and periungual regions of the toes or digits
(2). Previously, superficial acral
fibromyxoma of the great toe had been described in 8 cases
(Table I) (3–8).
Superficial acral fibromyxoma rarely occurs on the volar surface of
the digits (1). In the current case,
the tumor occurred on the volar side of the great toe under the
nail. It presented as a single, relatively rapid-growing, and
generally painless mass. Previous trauma of the affected site has
only been reported in a very small number of cases (1,9).
Previous superficial acral fibromyxoma of the great toe has also
been reported to be slow-growing (3–8). Only
two cases have been described in which the patients experienced
pain, and only one case involved a patient with a traumatic history
(Table I). In the current case, the
patient showed a painful rapid-growing tumor without a traumatic
history. Despite the absence of trauma, it was suggested that
chronic stimulation may have promoted tumor growth and lead to the
rapid growth rate. In ~36% of superficial acral fibromyxoma cases,
bone involvement may be present in the form of erosion (2), like in our case. Cases involving the
great toe have shown no features of erosion or lytic bone lesions
(Table I). We hypothesized that
chronic stimulation may have promoted the invasion of the bone.
 | Table I.Superficial acral fibromyxoma
originating from a great toe. |
Table I.
Superficial acral fibromyxoma
originating from a great toe.
| Authors, year | Demographic data | Erosion or lytic
lesion of bone | Reactivity | Management | Recurrence | (Refs.) |
|---|
| Wakabayashi et
al, 2012 | 51 years, female | – |
CD10+,CD34+, | 2-mm | NR | (3) |
|
| 14 months
history |
| VIM+,
CD99+, | wide margin |
|
|
|
| No trauma |
| HMB45−,
EMA−, |
|
|
|
|
| painless |
| S-100−,
α-SMA− |
|
|
|
| Schwager et
al, 2015 | N=3 | – |
| Marginal
excision | NR | (4) |
|
| 35 years, male |
| CD34+,
S-100−, |
|
|
|
|
| 12 months
history |
| XIII− |
|
|
|
|
| No trauma |
|
|
|
|
|
|
| Pain+ |
|
|
|
|
|
|
| 47 years, male |
|
CD34+,
S-100− |
|
|
|
|
| 12 months
history |
|
|
|
|
|
|
| No trauma |
|
|
|
|
|
|
| Painless |
|
|
|
|
|
|
| 45 years, female |
| CD34+,
S-100− |
|
|
|
|
| 12 months
history |
|
|
|
|
|
|
| No trauma |
|
|
|
|
|
|
| Painless |
|
|
|
|
|
| Raghupathi et
al, 2015 | 27 years, female |
| N/A | Marginal
excision | NR | (5) |
|
| 2 years history |
|
|
|
|
|
|
| No trauma |
|
|
|
|
|
|
| painless | – |
|
|
|
|
| Moon et al,
2015 | 46 years, female | – | CD68+,
CD99+, | Surgical
excision | NR | (6) |
|
| 2 years history |
|
CD34−,
S-100− | of the distal
phalanx |
|
|
|
| No trauma |
|
|
|
|
|
|
| painless |
|
|
|
|
|
| Braga et al,
2017 | 88 years, male | – | CD34+,
CD99+, | Marginal
excision | NR | (7) |
|
| 10 years history |
|
EMA−,
S-100+ |
|
|
|
|
| Trauma |
|
|
|
|
|
|
| Painless |
|
|
|
|
|
| Robati et al,
2017 | 18 years, female | – | CD99+,
CD34−, | Marginal
excision | NR | (8) |
|
| 2 years history |
|
SMA+,
VIM+ |
|
|
|
|
| No trauma |
|
|
|
|
|
|
| Painless |
|
|
|
|
|
| Current case | 37 years, male | + | CD34+, S-100-, | Marginal
excision | NR |
|
|
| 6 months history |
| EMA-, α-SMA-, |
|
|
|
|
| No trauma |
| desmin- |
|
|
|
|
| Painless |
|
|
|
|
|
Simple resection is the basic treatment of
superficial acral fibromyxoma (1,2).
Although the recurrence rate is ~20%, no malignant transformation
has been documented (1,2,9). All
cases of superficial acral fibromyxoma of the toe that were treated
with marginal resection showed no recurrence (Table I).
Macroscopically, superficial acral fibromyxoma is a
non-capsulated, gelatinous or solid lesion with a size range of 0.6
to 5.0 cm. It is located in the dermis and can extend to the
subcutaneous tissue. On histologic examination, it consists of a
proliferation of fibroblast-like cells with a myxocollagenous
matrix. Mild nuclear atypia and mitotic figures are infrequently
seen. Most reported cases are immunohistochemically positive for
CD34 and CD99 and negative for epithelial membrane antigen,
although the staining for these markers is variable. No reactivity
is observed for S100 (1,2,10).
Superficial acral fibromyxomas of the great toe show varied
immunohistochemical features (Table
I). We finally reached a diagnosis with histological findings
of hematoxylin and eosin staining and immunopositive findings of
CD34.
The differential diagnosis of superficial acral
fibromyxoma includes fibroma of the tendon sheath, myxoid
neurofibroma, glomus tumor, giant cell tumor of the tendon sheath,
sclerosing perineuroma, acral fibrokeratoma, cutaneous myxoma,
myxoinflammatory acral fibroblastic sarcoma, fibrous histiocytoma,
and dermatofibrosarcoma protuberans. In particular, superficial
acral fibromyxoma should be considered in the differential
diagnosis of glomus tumors when they develop under the nail. The
histologic features seen on immunohistochemical analysis are used
to distinguish superficial acral fibromyxoma from these other
lesions (1,2,10).
There are some limitations in the current study.
First, we could not detect CD99 in the specimen by
immunohistochemistry. However, we reached a diagnosis with other
histological observations including hematoxylin and eosin staining
and immunopositive findings. Second, we did not conduct a biopsy
before resecting the tumor. We should have treated the tumor
carefully because the radiological findings were doubtful for
malignancy.
In conclusion, we described a rapid-growing
superficial acral fibromyxoma of a great toe with bone erosion. If
a soft tissue tumor occurs under the nail, we should suspect
superficial acral fibromyxoma and we also should keep in mind that
such tumors can grow aggressively.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
KH, SN, HT, NO and RK were involved in the
acquisition of data. KH, SN and NO analyzed the data. MA made
substantial contributions to conception and design and analysis and
interpretation of data. KH and MA prepared the manuscript.
Ethics approval and consent to
participate
The Ethics Committee of the Kindai University
Faculty of Medicine approved the present study, and the patient
provided informed consent to participate.
Patient consent for publication
The patient provided written informed consent.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
MRI
|
magnetic resonance imaging
|
|
N/A
|
not applicable
|
|
VIM
|
vimentin
|
|
EMA
|
epithelial membrane antigen
|
|
SMA
|
α-smooth muscle actin;
|
References
|
1
|
Fetsch JF, Laskin WB and Miettinen M:
Superficial acral fibromyxoma: A clinicopathologic and
immunohistochemical analysis of 37 cases of a distinctive soft
tissue tumor with a predilection for the fingers and toes. Hum
Pathol. 32:704–714. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sawaya JL and Khachemoune A: Superficial
acral fibromyxoma. Int J Dermatol. 54:499–508. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wakabayashi Y, Nakai N, Takenaka H and
Katoh N: Superficial acral fibromyxoma of the great toe: Case
report and mini-review of the literature. Acta Dermatovenerol
Croat. 20:263–266. 2012.PubMed/NCBI
|
|
4
|
Schwager ZA, Mannava KA, Mannava S, Telang
GH, Robinson-Bostom L and Jellinek NJ: Superficial acral
fibromyxoma and other slow-growing tumors in acral areas. Cutis.
95:E15–E19. 2015.PubMed/NCBI
|
|
5
|
Raghupathi DS, Krishnamurthy J and Kakoti
LM: Cytological diagnosis of superficial acral fibromyxoma: A case
report. J Cytol. 32:39–41. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Moon A, Yoon N and Kim HS: Myxoid
dermatofibroma on a great toe: A case report. Int J Clin Exp
Pathol. 8:7605–7609. 2015.PubMed/NCBI
|
|
7
|
Braga JM, Bartosch I, Baldaia H, Oliveira
I, Canelhas A and Silva Á: Superficial acral fibromyxoma: A rare
soft tissue tumor. J Foot Ankle Surg. 56:653–655. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Robati RM, Dadkhahfar S and Rakhshan A:
CD34 negative superficial acral fibromyxoma: A rare case report.
Indian Dermatol Online J. 8:45–47. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hollmann TJ, Bovée JV and Fletcher CD:
Digital fibromyxoma (superficial acral fibromyxoma): A detailed
characterization of 124 cases. Am J Surg Pathol. 36:789–798. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kazakov DV, Mentzel T, Burg G and Kempf W:
Superficial acral fibromyxoma: Report of two cases. Dermatology.
205:285–288. 2002. View Article : Google Scholar : PubMed/NCBI
|