Introduction
Epidermal growth factor receptor-tyrosine kinase
inhibitors (EGFR-TKIs), including gefitinib, erlotinib, and
afatinib, have a dramatic effect on non-small cell lung cancer
(NSCLC) with major EGFR mutations consisting of exon 19 deletion
and exon 21 L858R point mutation (1,2). More
recently, some clinical and radiological characteristics of NSCLC
with major EGFR mutations were revealed: Miliary lung metastases
are frequently observed in NSCLC with EGFR mutation (3,4). In
addition, miliary brain metastases have been reported to be
correlated with exon 19 deletion (5,6).
However, it remains undetermined whether NSCLC with
minor EGFR mutations possesses characteristics similar to those
with major EGFR mutations. Exon 20 insertion is reportedly rare and
accounts for only 4% of EGFR mutations (7–9). Between
January 2014 and September 2017, we observed four cases of NSCLC
with exon 20 insertion. Among them, two patients presented with
miliary lung metastases at the time of NSCLC diagnosis. In the
present study, we describe notable clinical courses in these two
patients.
Case report
Case 1
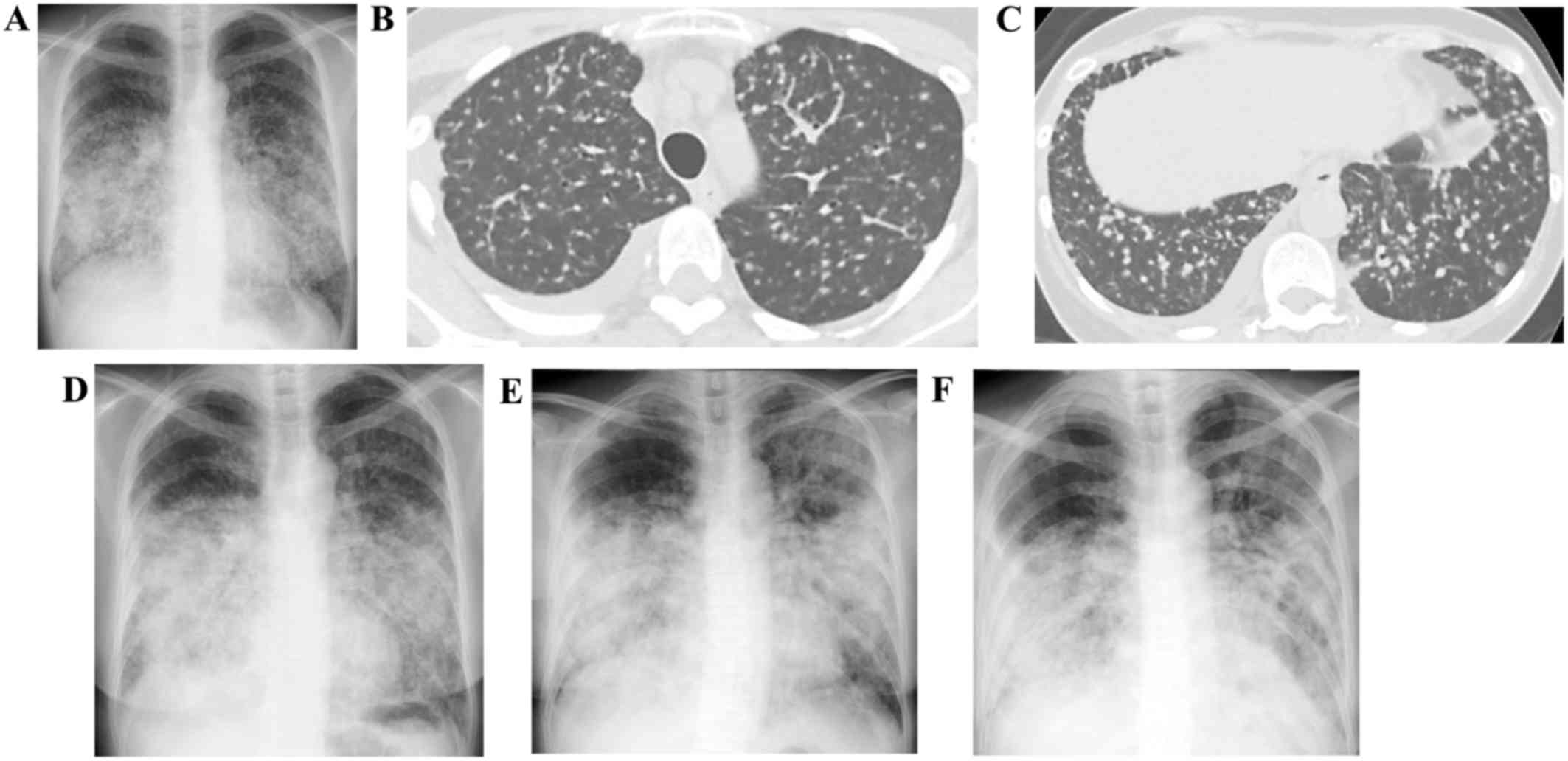
A 53-year old non-smoking woman developed cough and
visited a hospital on July 12, 2016. A chest radiograph
demonstrated multiple pulmonary nodules (Fig. 1A), which suggested miliary
tuberculosis. The patient was referred to our hospital on July 13.
Chest CT showed numerous miliary nodules throughout bilateral lungs
(Fig. 1B and C); however, a sputum
smear stain for mycobacteria was negative. Transbronchial lung
biopsy on July 19 revealed papillary adenocarcinoma staged cT4N3M1b
(PUL, BRA) and cobas version 2 method detected exon 20 insertion.
Because the performance status (PS) score was zero, cisplatin plus
pemetrexed were administered as first-line therapy on August 16.
However, pleural effusion and multiple lung nodules deteriorated
after two-courses of this regimen. On September 9, docetaxel plus
ramucirumab were administered as second-line treatment. However,
the patient developed lymphangitis with deterioration of her
respiratory condition. After methylprednisolone was administered to
treat the lymphangitis on September 17 (Fig. 1D), afatinib was administered as
third-line chemotherapy on September 19th. Although the patient
exhibited temporary improvement in her respiratory condition on
30th September from required oxygen of 15 to 1 l/min (Fig. 1E), the lesions in the right lower
lung deteriorated and progression of disease was confirmed on
October 24 (Fig. 1F). Subsequently,
nivolumab was administered on October 25, but it failed to produce
the desired outcome. Finally, she died of lung cancer on November
2.
Case 2
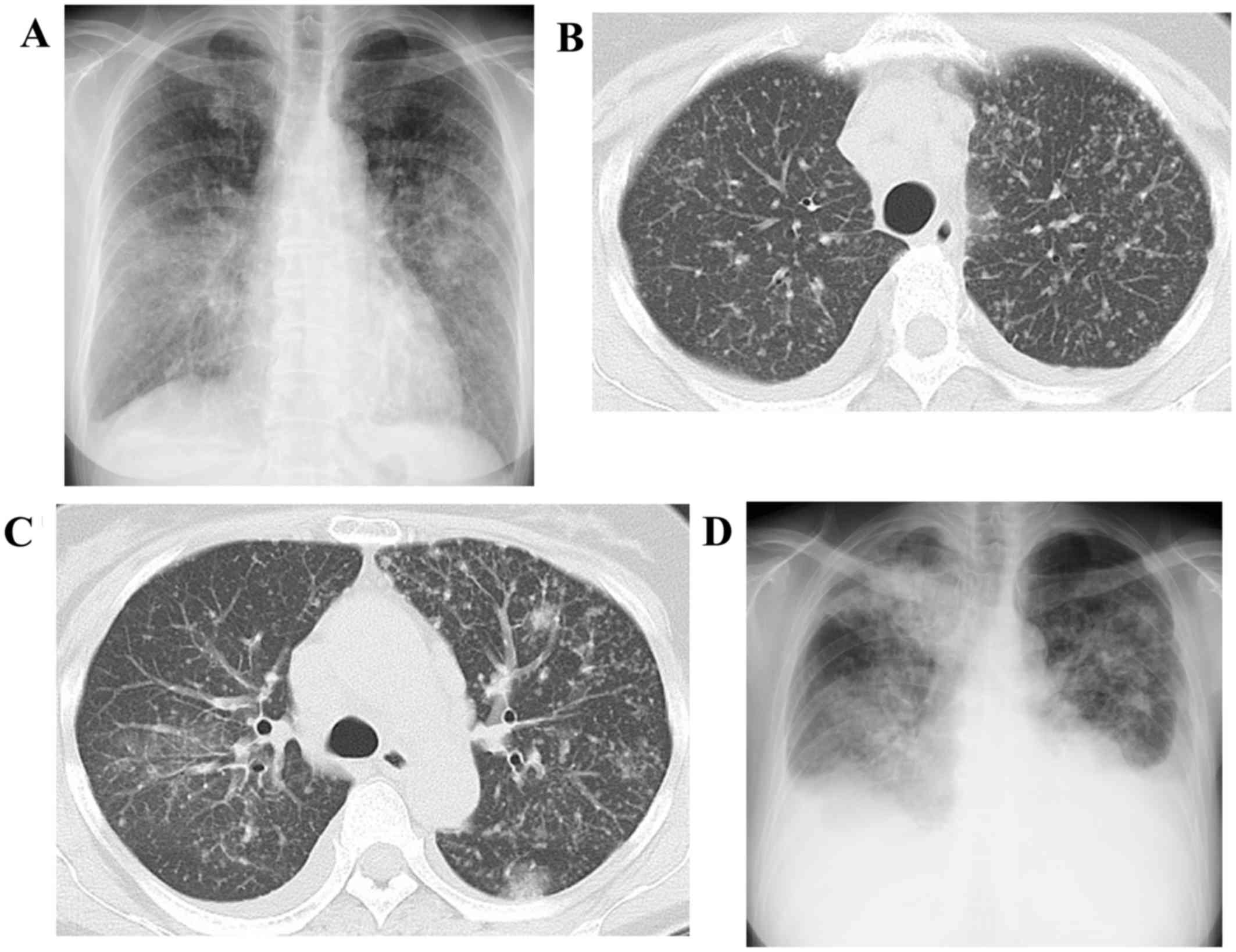
A 61-year-old non-smoking woman developed cough and
dyspnea during exercise in December 2016. Consequently, she visited
a hospital on January 14 2017. Because both chest radiograph and CT
revealed miliary lung nodules (Fig.
2A-C) and miliary tuberculosis was suspected, she was
transferred to our hospital on the same day. Because a sputum smear
stain for mycobacteria was negative, transbronchial lung biopsy was
performed on January 17 and micropapillary adenocarcinoma staged
cT4N3M1b (PLE, PUL, OSS) was diagnosed. Furthermore, exon 20
insertion was detected by cobas version 2 method. Because the PS
score was 1, carboplatin plus nab-paclitaxel were administered as
first-line treatment on February 1. However, this therapeutic
regimen did not produce a satisfactory outcome (Fig. 2D). Therefore, we administered
docetaxel as second-line therapy on February 23 but the outcome was
the same as that produced by first-line treatment, and the patient
rapidly developed respiratory failure. Finally, she died of lung
cancer on March 17.
Discussion
The results of our two cases would provide the
following two important clinical issues.
First, NSCLC with exon 20 insertion can present
miliary type of lung metastases. In fact, two in four NSCLC
patients (with exon 20 insertion) (50%) had miliary lung
metastases. To the best of our knowledge, there is no report
regarding the radiological characteristics of patients with NSCLC
with exon 20 insertion. Furthermore, it is widely accepted that
NSCLC with major EGFR mutations, especially exon 19 deletion,
occasionally presents a miliary metastatic pattern in lungs. Laack
et al reported five cases of miliary lung metastases from
NSCLC with exon 19 deletion, which dramatically responded to
EGFR-TKIs (10). In addition, two
recent studies by Togashi et al and Wu et al revealed
that NSCLC patients with miliary lung metastases had a high EGFR
mutation rate in the range of 70–87.5% (3,4).
However, in these studies, exon 20 insertions were not observed
(4), and the details of EGFR
mutation status were not provided (3). Most of EGFR mutations were major EGFR
mutation (4). More recently, miliary
type of metastases in lung and/or brain was reported in NSCLC
harboring non-EGFR oncogene driver mutation such as echinoderm
microtubule associated protein like 4-anaplastic lymphoma kinase
(EML4-ALK) gene translocation (11)
and c-ros oncogene 1 (ROS-1) rearrangement (12). Taking together these reports and the
two cases presented in this study, miliary type of metastases can
be closely correlated not only with major EGFR mutation, but also
other oncogene driver mutation including exon 20 insertion.
Second, miliary lung metastases from NSCLC with exon
20 insertion appear to be an extremely poor prognostic entity. As
reported in this study, disease progression in the two patients was
rapid, and both the patients died within 3 months from beginning
first-line treatment. To date, the prognosis in NSCLC patients with
exon 20 insertions has been reported to vary, with a median OS of
5–26 months (7,8,13–15).
However, most studies included a high proportion of patients with
post-operation recurrence, which suggests low-tumor burden. In
contrast, a study by Noronha et al included more patients
with PS≥3 (40%) and revealed a dismal poor prognosis, with a median
OS of 5 months (8). The authors
proposed that the reasons for poor prognosis were attributable to
high tumor burden and poor response to EGFR-TKIs (8), which were observed in the prospective
randomized trial (16). In the two
cases presented in this study, despite high tumor burden, when the
first-line treatment was commenced, the PS score was low (0 for the
first and 1 for the second case). However, miliary lung metastases
easily and rapidly caused respiratory failure resulting in PS
reduction. Therefore, NSCLC patients with miliary lung metastases
and exon 20 insertions seem to have a poor prognosis with low
chances of receiving further chemotherapy.
In conclusion, we presented two cases of miliary
lung metastases from NSCLC patients with exon 20 insertion. PS
rapidly deteriorated and the efficacy of chemotherapies including
cytotoxic agents and EGFR-TKIs was limited. Chest physician should
be aware that NSCLC with exon 20 insertion could present as miliary
type of lung metastases and rapid disease progression. The
accumulation of additional case series is necessary to confirm our
results.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
AS and HS participated in the conception and design
of the case report, analyzed and interpreted the data and wrote the
manuscript. AS, TaK, TsO, SI and TaO evaluated the patient and
participated in the therapy. SI, HS and TaO revised the manuscript
for intellectual content. TI, ToK, and KO evaluated radiological
images or pathological specimens. All authors have read and
approved the final draft.
Ethics approval and consent to
participate
The patient provided written informed consent for
participation in the present study.
Patient consent for publication
The patient provided written informed consent for
the publication of any associated data and images in this case
report.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Lynch TJ, Bell DW, Sordella R,
Gurubhagavatula S, Okimoto RA, Brannigan BW, Harris PL, Haserlat
SM, Supko JG, Haluska FG, et al: Activating mutations in the
epidermal growth factor receptor underlying responsiveness of
non-small-cell lung cancer to gefitinib. N Engl J Med.
350:2129–2139. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Paez JG, Janne PA, Lee JC, Tracy S,
Greulich H, Gabriel S, Herman P, Kaye FJ, Lindeman N, Boggon TJ, et
al: EGFR mutations in lung cancer: Correlation with clinical
response to gefitinib therapy. Science. 304:1497–1500. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Togashi Y, Masago K, Kubo T, Sakamori Y,
Kim YH, Hatachi Y, Fukuhara A, Mio T, Togashi K and Mishima M:
Association of diffuse, random pulmonary metastases, including
miliary metastases, with epidermal growth factor receptor mutations
in lung adenocarcinoma. Cancer. 117:819–825. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wu SG, Hu FC, Chang YL, Lee YC, Yu CJ,
Chang YC, Wu JY, Shih JY and Yang PC: Frequent EGFR mutations in
NSCLC presenting with miliary intrapulmonary carcinomatosis. Eur
Respir J. 41:417–424. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sekine A, Kato T, Hagiwara E, Shinohara T,
Komagata T, Iwasawa T, Satoh H, Tamura K, Kasamatsu T, Hayashihara
K, et al: Metastatic brain tumors from non-small cell lung cancer
with EGFR mutations: Distinguishing influence of exon 19 deletion
on radiographic features. Lung Cancer. 77:64–69. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mochizuki S, Nishimura N, Inoue A,
Murakami K, Nukiwa T and Chohnabayashi N: Miliary brain metastases
in 2 cases with advanced non-small cell lung cancer harboring EGFR
mutation during gefitinib treatment. Respir Investig. 50:117–121.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Naidoo J, Sima CS, Rodriguez K, Busby N,
Nafa K, Ladanyi M, Riely GJ, Kris MG, Arcila ME and Yu HA:
Epidermal growth factor receptor exon 20 insertions in advanced
lung adenocarcinomas: Clinical outcomes and response to erlotinib.
Cancer. 121:3212–3220. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Noronha V, Choughule A, Patil VM, Joshi A,
Kumar R, Susan Joy, Philip D, Banavali S, Dutt A and Prabhash K:
Epidermal growth factor receptor exon 20 mutation in lung cancer:
Types, incidence, clinical features and impact on treatment. Onco
Targets Ther. 10:2903–2908. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Yasuda H, Kobayashi S and Costa DB: EGFR
exon 20 insertion mutations in non-small-cell lung cancer:
Preclinical data and clinical implications. Lancet Oncol.
13:e23–e31. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Laack E, Simon R, Regier M, Andritzky B,
Tennstedt P, Habermann C, Verth CZ, Thöm I, Grob T, Sauter G and
Bokemeyer C: Miliary never-smoking adenocarcinoma of the lung:
Strong association with epidermal growth factor receptor exon 19
deletion. J Thorac Oncol. 6:199–202. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Falk AT, Poudenx M, Otto J, Ghalloussi H
and Barrière J: Adenocarcinoma of the lung with miliary brain and
pulmonary metastases with echinoderm microtubule-associated protein
like 4-anaplastic lymphoma kinase translocation treated with
crizotinib: A case report. Lung Cancer. 78:282–284. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Dziadziuszko K, Szurowska E, Pienkowska J,
Jassem J and Dziadziuszko R: Miliary brain metastases in a patient
with ROS1-rearranged lung adenocarcin-oma: A case report. J Thorac
Oncol. 9:e34–e36. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Oxnard GR, Lo PC, Nishino M, Dahlberg SE,
Lindeman NI, Butaney M, Jackman DM, Johnson BE and Jänne PA:
Natural history and molecular characteristics of lung cancers
harboring EGFR exon 20 insertions. J Thorac Oncol. 8:179–184. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lund-Iversen M, Kleinberg L,
Fjellbirkeland L, Helland Å and Brustugun OT: Clinicopathological
characteristics of 11 NSCLC patients with EGFR-exon 20 mutations. J
Thorac Oncol. 7:1471–1473. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Beau-Faller M, Prim N, Ruppert AM,
Nanni-Metéllus I, Lacave R, Lacroix L, Escande F, Lizard S, Pretet
JL, Rouquette I, et al: Rare EGFR exon 18 and exon 20 mutations in
non-small-cell lung cancer on 10 117 patients: A multicentre
observational study by the French ERMETIC-IFCT network. Ann Oncol.
25:126–131. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yang JC, Sequist LV, Geater SL, Tsai CM,
Mok TS, Schuler M, Yamamoto N, Yu CJ, Ou SH, Zhou C, et al:
Clinical activity of afatinib in patients with advanced
non-small-cell lung cancer harbouring uncommon EGFR mutations: A
combined post-hoc analysis of LUX-Lung 2, LUX-Lung 3 and LUX-Lung
6. Lancet Oncol. 16:830–838. 2015. View Article : Google Scholar : PubMed/NCBI
|