Introduction
Hepatocellular carcinoma (HCC), the most common
primary cancer of the liver, is the sixth most common type of
malignant tumor and is the second leading cause of cancer-related
mortality, worldwide (1). The
long-term prognosis of HCC remains poor due to postoperative
recurrence. Although progression in therapeutic modalities may
result in long-term survival for patients with small HCCs or
solitary encapsulated tumors, the 5-year overall survival (OS) rate
is only 34–50% (2–4). Thus, identification of prognostic
markers of HCC has long been of interest.
Methyl-CpG binding domain 2 (MBD2) has been
demonstrated to be able to specifically bind to methylated DNA,
independent of sequence context. This function involves the
presence of a highly conserved protein motif termed the methyl-CpG
binding domain (5). MBD2
overexpression induced by hepatitis B virus X protein may be
involved in transcriptional activation of the human insulin-like
factor-II promoters. However, the clinicopathological and
prognostic importance of MBD2 in HCC remains unknown. It was shown
to participate in suppressing transcription of a number of
antioncogenes, including in breast cancer, colorectal cancer, lung
cancer and endometrial carcinoma (6–9). The
CpG island encompassing the π-class glutathione S-transferase gene
(GSTP1) becomes hypermethylated during the pathogenesis of HCC. It
has been reported that MBD2 is involved in CpG island
hypermethylation to repress GSTP1 expression in HCC cells (10). Strong evidence for the multi-modal
action of MBD2 in controlling gene expression and DNA methylation
in liver cancer has been demonstrated and it was proposed that
co-occupancy with certain transcription factors determines the
effect of MBD2 at transcriptional start sites (11).
In the present study, MBD2 expression and the
correlation with the clinicopathologic characteristics of HCC were
investigated.
Materials and methods
Patients
Fresh HCC and PTL tissues used for western blotting
were obtained from 20 HCC patients. In addition, formalin-fixed,
paraffin-embedded blocks of HCC and PTL tissues were obtained from
159 patients with HCC patients. All of patients underwent hepatic
resection between January, 2003 and October, 2008 at the
Hepatopancreatobiliary Surgery Department of the Beijing Cancer
Hospital and Institute. The diagnosis of HCC was confirmed by
histology. Each patient was carefully informed with details of
treatment and risk, and written informed consent was obtained from
the patient or patient's family. The present study was approved by
the ethics committee of Beijing Cancer Hospital and Institute and
Peking University (Beijing, China).
Western blotting
Total protein was extracted from 20 pairs of fresh
tissue samples and solubilized in tissue lysis buffer (500
µl of 1 M Tris-HCl, pH 8.0; 300 µl of 5 M sodium
chloride; 5 µl of 1 M DTT and 100 µl of 1X protease
inhibitor). The protein concentration was measured using a Bradford
assay. For immunoblotting, 50 µg of protein was separated on
8% sodium dodecyl sulfate-polyacrylamide gel and transferred onto
polyvinylidene fluoride membranes (Amersham Pharmacia Biotech, GE
Healthcare Life Sciences, Pittsburgh, PA, USA). The membranes were
blocked with 0.5% skimmed milk, then probed with anti-MBD2 primary
antibody (cat. no. NB100-93352; Novus Biologicals, Ltd., Cambridge,
UK) against MBD2 at a dilution of 1:500 for 1 h at room
temperature. After washing with phosphate-buffered saline 0.5%
Tween, the membranes were incubated with horseradish
peroxidase-conjugated goat anti-rabbit antibody (cat. no. ZD-2301;
Zhongshan Golden Bridge Biotechnology, Beijing, China) at a
dilution of 1:8,000. Blots were developed with the enhanced
chemiluminescence kit. Glyceraldehyde 3-phosphate dehydrogenase was
used as the protein loading control. The signals of the bound
antibodies were visualized by enhanced chemiluminescence (EMD
Millipore, Billerica, MA, USA). Image Pro Plus (version 6.0; Media
Cybernetics, Inc., Rockville, MD, USA) was used to quantify the
densities of the protein signals on X ray films following scanning.
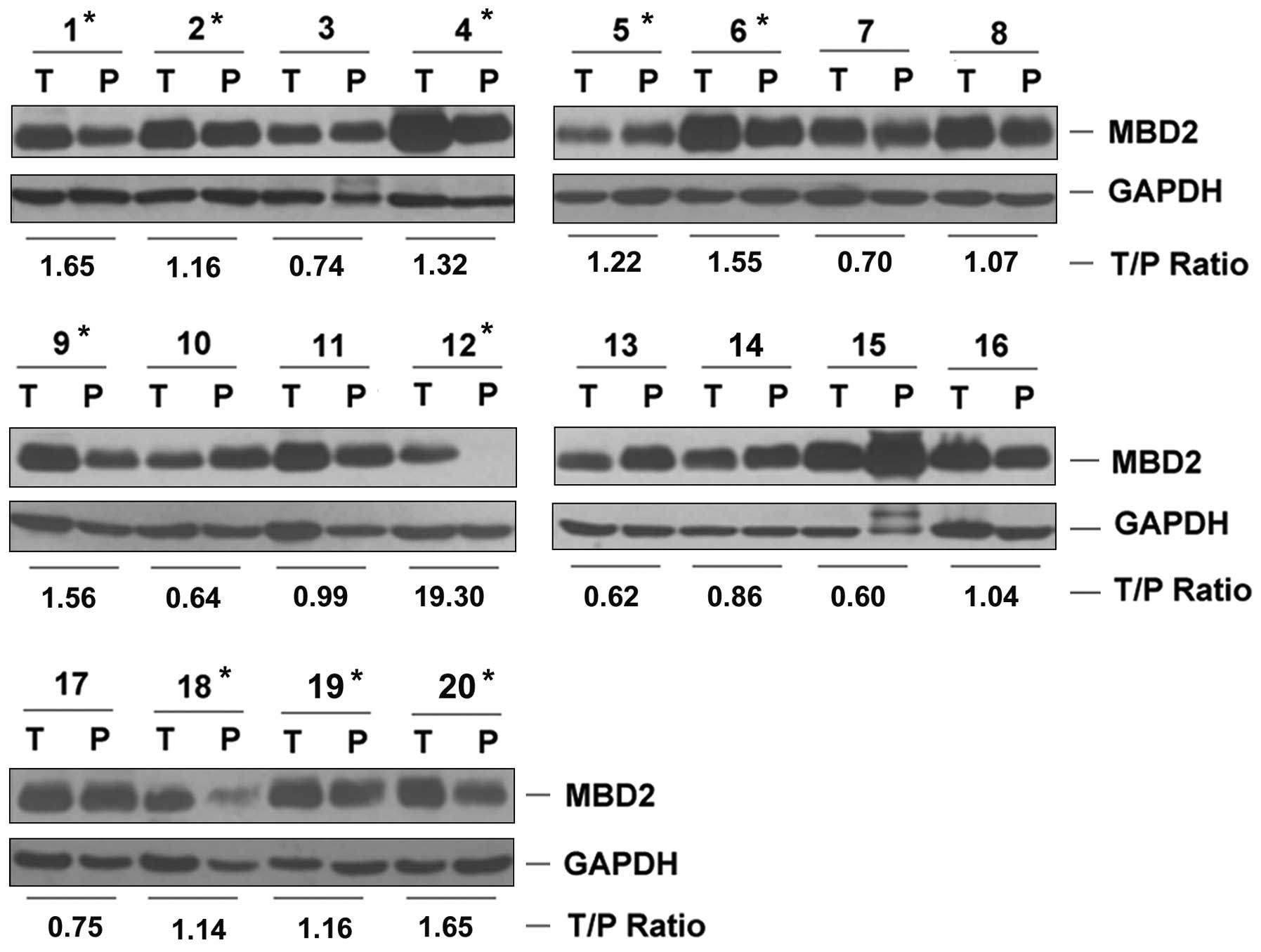
A tumor tissue/paratumoral liver tissue ratio of ≥1.1 was defined
as upregulation.
Immunohistochemistry
After dewaxing in xylene and rehydrating through a
graded series of ethanol, the 4-µm sections were subjected
to heat antigen retrieval in citrate buffer solution and heated for
3 min at 37°C. Hydrogen peroxide (3%) was applied to block
endogenous peroxidases for 30 min. The sections were then incubated
at room temperature for 30 min and blocked with normal goat serum
for nonspecific binding. Sections were incubated with rabbit
anti-human MBD2 polyclonal antibody (Santa Cruz Biotechnology Inc.)
at a dilution of 1:100 at 4°C overnight. Sections were then
incubated at 37°C for 30 min with horseradish peroxidase-conjugated
goat anti-rabbit IgG (Beijing Zhongshan Golden Bridge Biotechnology
Co., Ltd., Beijing, China). Immunocomplexes were visualized using
3,3-diaminobezidine. Sections were counterstained with hematoxylin,
dehydrated and mounted with coverslips. The immunostaining results
were evaluated independently by two pathologists who were blinded
to the patient clinical data. For assessment of MBD2, 5 high power
fields in each specimen were selected randomly, and nuclear
staining was examined by light microscopy. Cells (>500) were
counted to determine the labeling index, which represented the
percentage of immunostained cells relative to the total number of
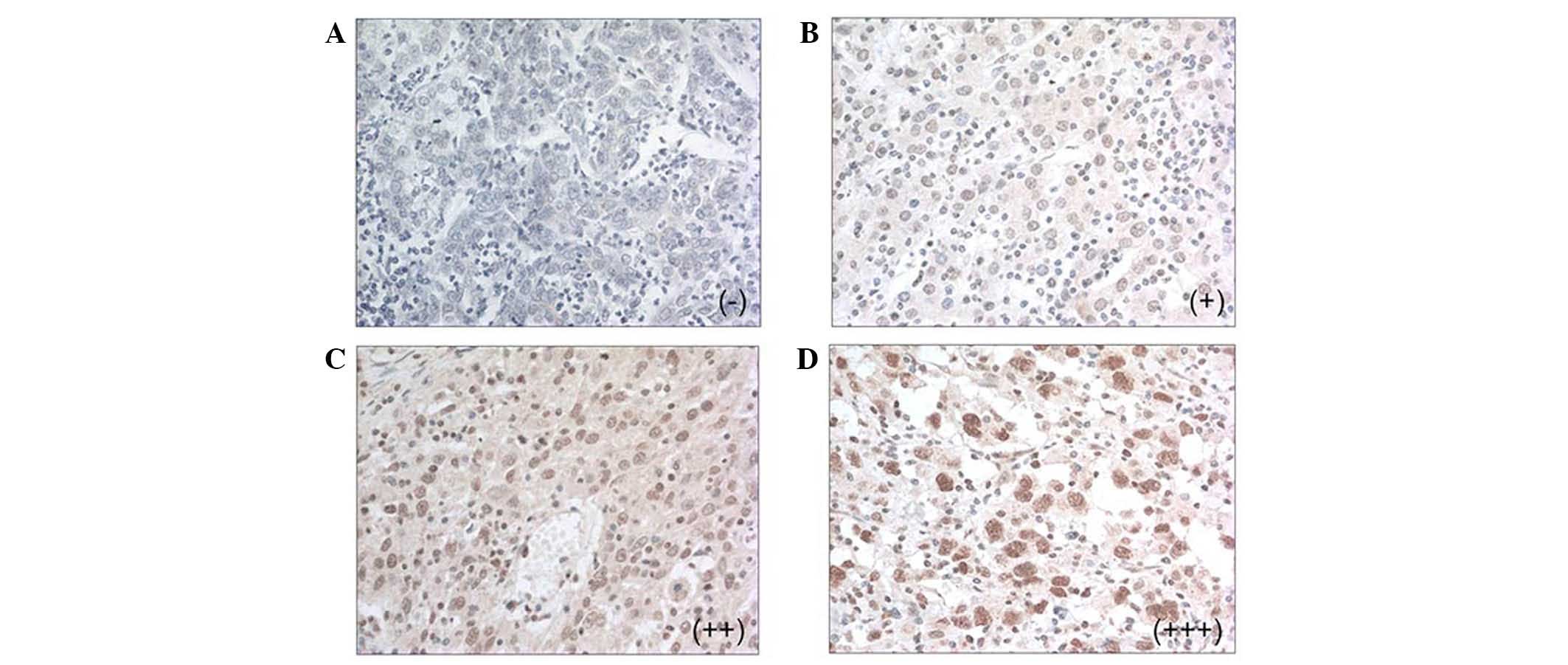
cells. In brief, MBD2 staining was categorized into four different
levels: Negative (−) nuclear labeling in no cells; faintly positive
(+), nuclear labeling in ≤1/3 of the cells; moderately positive
(++), strong nuclear labeling in 1/3 to 2/3 of the cells; and
highly positive (+++), intense nuclear labeling in ≥2/3 of the
cells.
Follow up
The median follow up was 31 months (range, 1–110
months). In total, 132 (83.02%) patients experienced recurrence
following hepatic resection. This resulted in the mortality of 129
(81.13%) of these patients.
Statistical analysis
MBD2 expression in the HCC and PTL tissues was
compared using the McNemar test. The correlation between MBD2
immunohistochemical staining and clinico-pathologic variables was
analyzed by the χ2 test. Disease-free survival (DFS) and
OS rates were calculated from the date of hepatic resection using
the Kaplan-Meier method and significant differences between the
groups were determined with the log-rank test. The multivariate Cox
proportional hazard model was adopted to analyze significance of
various variables for survival. Statistical analysis was conducted
using SPSS 19.0 for Windows (IBM, Armonk, NY, USA). P<0.05 was
considered to indicate a statistically significant difference.
Results
Clinical profiles of the patients
Of the 159 patients included, 134 were male and 25
were female. The median age was 51 years (range, 28–79). All
clinicopathologic and pathological data, including age, gender,
number of tumor nodules, tumor size, microscopic vascular invasion,
serum α-fetoprotein level, Edmondson-Steiner grade, BCLC stage and
capsule formation, were recorded. Hepatitis B was present in 124
patients (77.99%), hepatitis C was present in 12 patients (7.55%),
and both hepatitis B and hepatitis C were presented in 4 patients
(2.52%). Preoperative evaluation showed that all the patients was
rated as Child-Pugh class A, or grade B but could recover to grade
A after short-term treatment to protect liver function, and thus
were eligible for hepatic resection. Informed consent from the
patients and approval of the Institutional Ethics Committee were
obtained.
MBD2 expression in HCC and PTL
tissues
Compared with the PTL tissues, western blotting
demonstrated that MBD2 expression was upregulated in 10 of the 20
patients with HCC (50%, Fig. 1).
Immunohistochemistry showed that MBD2 was expressed in 81 of the
159 HCC tissues (50.94%), being faintly positive in 43 patients
(27.04%), moderately positive in 31 patients (19.50%) and highly
positive in 7 patients (4.40%, Fig.
2). No expression of MBD2 was observed in any of the PTL
tissues. Compared with the PTL tissue, the MBD2 expression rate in
HCC tissues was significant increased (50.94% vs. 0%, P<0.001,
McNemar test).
Correlation between MBD2 expression and
clinicopathologic variables in HCC
Using the χ2 test, tumor size,
microscopic vascular invasion and BCLC B stage were shown to have a
significant association with MBD2 expression (P<0.05; Table I).
 | Table ICorrelation between MBD2 expression
and clinicopathological features in hepatocellular carcinoma. |
Table I
Correlation between MBD2 expression
and clinicopathological features in hepatocellular carcinoma.
| Variable | Patient number | MBD2 expression
| P-value |
|---|
| (−) | (+) | (++) | (+++) |
|---|
| Tumor size (cm) | 159 | | | | | 0.004 |
| ≤5 | | 51 | 17 | 10 | 3 | |
| >5 | | 27 | 26 | 21 | 4 | |
| Tumor nodules | 159 | | | | | 0.401 |
| Solitary | | 64 | 38 | 23 | 5 | |
| Multiple | | 14 | 5 | 8 | 2 | |
| Capsular
formation | 154 | | | | | 0.403 |
| Absence | | 43 | 19 | 20 | 4 | |
| Presence | | 33 | 22 | 10 | 3 | |
| Microscopic vascular
invasion | 157 | | | | | 0.039 |
| Absence | | 59 | 28 | 16 | 3 | |
| Presence | | 18 | 14 | 15 | 4 | |
| Serum α-fetoprotein
level (ng/ml) | 149 | | | | | 0.690 |
| ≤400 | | 45 | 26 | 21 | 4 | |
| >400 | | 29 | 13 | 8 | 3 | |
| Edmondson-steiner
grade | 158 | | | | | 0.215 |
| 1,2 | | 60 | 33 | 19 | 4 | |
| 3,4 | | 17 | 10 | 12 | 3 | |
| BCLC stage | 159 | | | | | 0.003 |
| A | | 48 | 17 | 8 | 2 | |
| B | | 30 | 26 | 23 | 5 | |
MBD2 expression is an independent
prognostic factor in HCC
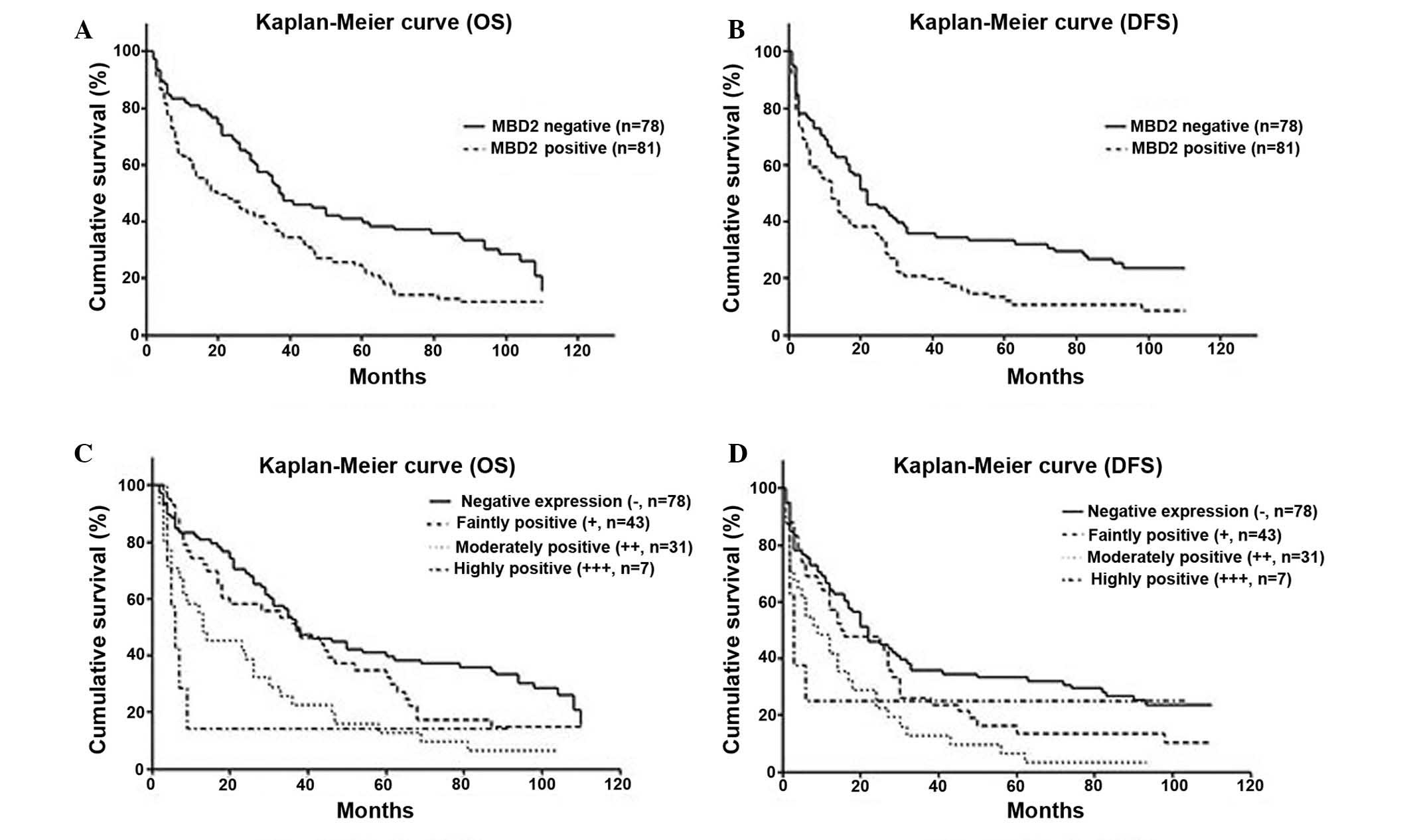
Based on MDB2 immunohistochemical staining, 78
patients were negative for staining of MBD2 and 81 patients showed
positive staining. The OS and DFS of MBD2-positive patients were
less than those negative for MBD2 (P=0.002 for OS, P=0.006 for DFS,
Fig. 3A and B). Moreover, based on
the immunohistochemical staining, the OS and DFS for different
levels of MBD2 expression significant different (P<0.01;
Fig. 3C and D).
Univariate analysis showed that tumor size >5 cm
[hazard ratio (HR), 2.375; P<0.001], multiple tumor nodules (HR,
2.234; P<0.001), absence of capsule formation (HR, 0.673;
P=0.035), microscopic vascular invasion (HR, 3.297; P<0.001),
BCLC stage B (HR, 2.785; P<0.001) and positive MBD2 expression
(HR, 2.570; P<0.001) were all associated with poor OS.
Multivariate Cox regression analysis revealed that multiple tumor
nodules (HR, 1.979; P=0.012), microscopic vascular invasion (HR,
2.134; P=0.001), and positive MBD2 expression (HR, 2.089; P=0.001)
were found to be independent prognostic factors for OS (Table II).
| Table IIUnivariate and multivariate cox
regression analyses of prognostic factors for OS in HCC. |
Table II
Univariate and multivariate cox
regression analyses of prognostic factors for OS in HCC.
| Variable | Patient number | Univariate analysis
| Multivariate
analysis
|
|---|
| HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Tumor size
(cm) | 159 | | | | 0.886 |
| ≤5 | | 1 | | 1 | |
| >5 | | 2.375
(1.647–3.426) | 0.000 | 0.939
(0.399–2.212) | |
| Tumor nodules | 159 | | | | 0.886 |
| Solitary | | 1 | | 1 | |
| Multiple | | 2.234
(1.432–3.485) | 0.000 | 1.979
(1.159–3.378) | |
| Capsular
formation | 154 | | | | 0.886 |
| Absence | | 1 | | 1 | |
| Presence | | 0.673
(0.465–0.973) | 0.035 | 0.628
(0.322–1.147) | |
| Microscopic
vascular invasion | 157 | | | | 0.001 |
| Absence | | 1 | | 1 | |
| Presence | | 3.297
(2.255–4.819) | 0.000 | 2.134
(1.392–3.272) | |
| Serum α-fetoprotein
level (ng/ml) | 149 | | | | 0.133 |
| ≤400 | | 1 | | 1 | |
| >400 | | 0.063
(0.980–2.121) | 0.063 | 1.370
(0.909–2.066) | |
| Edmondson-steiner
grade | 158 | | | | 1.027 |
| 1,2 | | 1 | | 1 | |
| 3,4 | | 1.026
(0.966–1.090) | 0.399 | 1.027
(0.953–1.107) | |
| BCLC stage | 159 | | | | 0.134 |
| A | | 1 | | 1 | |
| B | | 2.785
(1.912–4.056) | 0.000 | 1.985
(0.810–4.868) | |
| MBD2
expression | 159 | | | | 0.001 |
| Negative | | 1 | | 1 | |
| Positive | | 2.570
(1.761–3.749) | 0.000 | 2.089
(1.369–3.185) | |
Similarly, univariate analysis indicated that tumor
size >5 cm (HR, 2.078; P<0.001), multiple tumor nodules (HR,
2.371; P<0.001), microscopic vascular invasion (HR, 2.737;
P<0.001), greater serum α-fetoprotein level (>400 ng/ml; HR
1.495; P=0.031), BCLC stage B (HR, 2.355; P<0.001) and positive
MBD2 expression (HR, 2.128; P<0.001) were correlated with DFS.
Multivariate Cox regression analysis showed that microscopic
vascular invasion (HR, 1.884; P=0.003) and positive MBD2 expression
(HR, 1.601; P=0.022) were independent risk factors for poor DFS
(Table III).
| Table IIIUnivariate and multivariate cox
regression analyses of prognostic factors for DFS in HCC. |
Table III
Univariate and multivariate cox
regression analyses of prognostic factors for DFS in HCC.
| Variable | Patient number | Univariate analysis
| Multivariate
analysis
|
|---|
| HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Tumor size
(cm) | 159 | | | | 0.600 |
| ≤5 | | 1 | | 1 | |
| >5 | | 2.078
(1.467–2.942) | 0.000 | 1.348
(0.607–2.995) | |
| Tumor nodules | 159 | | | | 0.092 |
| Solitary | | 1 | | 1 | |
| Multiple | | 2.371
(1.542–3.647) | 0.000 | 1.206
(0.836–3.641) | |
| Capsular
formation | 154 | | | | 0.104 |
| Absence | | 1 | | | |
| Presence | | 0.753
(0.532–1.065) | 0.109 | 0.732
(0.503–1.066) | |
| Microscopic
vascular invasion | 157 | | | | 0.003 |
| Absence | | 1 | | 1 | |
| Presence | | 2.737
(1.900–3.943) | 0.000 | 2.033
(1.357–3.046) | |
| Serum α-fetoprotein
level (ng/ml) | 149 | | | | 0.090 |
| ≤400 | | 1 | | 1 | |
| >400 | | 1.495
(1.037–2.154) | 0.031 | 1.306
(0.893–1.909) | |
| Edmondson-steiner
grade | 158 | | | | 0.527 |
| 1,2 | | 1 | | 1 | |
| 3,4 | | 1.027
(0.969–1.089) | 0.374 | 1.024
(0.952–1.101) | |
| BCLC stage | 159 | | | | 0.451 |
| A | | 1 | | 1 | |
| B | | 2.355
(1.654–3.354) | 0.000 | 1.329
(0.581–3.040) | |
| MBD2
expression | 159 | | | | 0.022 |
| Negative | | 1 | | 1 | |
| Positive | | 2.128
(1.485–3.049) | 0.000 | 1.513
(1.018–2.248) | |
Discussion
MBD1, MBD2, MBD3, MBD4 and MeCP2 constitute a family
of vertebrate proteins that share the MBD domain. The MBD is
consisted of ~70 residues, and possesses a unique a/b-sandwich
structure with characteristic loops, which is able to bind single
methylated CpG pairs as a monomer (12). It has been suggested the molecular
mechanism of the functional properties of methylated DNA is
mediated via histone deacetylases (13).
Depending on recruitment of chromatin modifying
proteins, MBD2 is a well-established 'reader' of the methylation
signal that leads to the silencing of methylated genes (14,15).
It was also shown previously that MBD2 was implicated in the
activation of several prometastatic genes (16–18).
MBD2 specifically binds to methylated hMLH1 promoters and silences
this gene, which leads to histone modification (6). While, the lack of MBD2 at the
BRCA1-NBR2 CpG island leads to an elevated level of NBR2
transcripts (7). It was also
reported that MBD2 was a tumor suppressor gene in transcriptional
repression of the methylated p14ARF and suggested
that repression by MBD2 selectively affects a subset of methylated
promoters (19). A number of
specific antisense inhibitors of MBD2 inhibited
anchorage-independent growth of human lung and colorectal cancer
cell lines in vitro and tumorigenic growth of human cancer
cell xenografts in vivo (9). It suggested that MBD2 was critical in
tumorigenesis and was a potential anticancer target (20). Thus, Ivanov et al (21) proposed that MBD2-antisense
electrotransfer gene therapy and chemotherapy with bleomycin was a
novel candidate approach to anticancer therapy. Recently, it was
reported that MBD2 overexpression induced by Hepatitis B virus X
protein may be involved in the hypomethylation and transcriptional
activation of the human insulin-like factor-II promoters (22).
Immunohistochemistry indicated that MDB2 was only
expressed in HCC tissues, supporting the hypothesis that MBD2 was
involved in the carcinogenesis of HCC. Multivariate Cox regression
showed that MBD2 expression was significantly correlated with BCLC
stage B, tumor size >5 cm, and the presence of microscopic
vascular invasion. It suggested that MBD2 may be involved in the
progression and invasion of HCC as the parameters were all
associated with HCC staging and phenotypes (23,24).
Although there has been noteworthy improvement in surgical
techniques and perioperative management, the long-term outcome
following resection remains unsatisfactory (25,26).
Thus, it was hypothesized that conventional clinicopathologic
factors used to select suitable candidates for hepatic resection
were inadequate. Therefore, novel prognostic factors, either
clinicopathologic or molecular, are required to define the tumor
biology and determine which patients are at higher risk of tumor
recurrence (27,28). In the present study, upregulated
expression of MBD2 in HCC tissue was associated with poor OS and
DFS, along with tumor size >5 cm, BCLC stage B and microscopic
vascular invasion. These findings suggest that MBD2 may be a novel
molecular prognostic indicator in HCC. This raises the possibility
that MBD2 may be a prognostic parameter for HCC which is as or more
reliable than the clinicopathological factors currently in use.
Microvascular invasion is a histological feature of
HCC that is associated with aggressive biological behavior and poor
prognosis. A number of studies have also addressed HCC patients
with microvascular invasion that was consistently predictive of
intrahepatic metastasis (29,30).
To date, the complex interplay between different variables that can
be obtained has not led to any predictive model to recognize
microvascular invasion prior to hepatic resection. In the present
study, microscopic vascular invasion was shown to be significantly
associated with MBD2 upregulated expression, which indicated that
MBD2 protein could be a marker of MVI in HCC. However, further
investigation of the MBD2 expression level in the serum is
required.
In conclusion, the present study demonstrated that
MBD2 was upregulated in HCC. Additionally, MBD2 is a poor
prognostic factor for OS and DFS. Consequently, targeting MBD2 may
provide a promising therapeutic strategy for the treatment of HCC.
However, the prognostic significance of MBD2 in HCC still requires
further validation, particularly regarding the correlation with
tumor size, microscopic vascular invasion and BCLC stage.
Acknowledgments
This study was supported by grants from the Chinese
State Key Project for Basic Research (973; 2014CBA02001).
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Shimozawa N and Hanazaki K: Longterm
prognosis after hepatic resection for small hepatocellular
carcinoma. J Am Coll Surg. 198:356–365. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Verhoef C, de Man RA, Zondervan PE,
Eijkemans MJ, Tilanus HW and Ijzermans JN: Good outcomes after
resection of large hepatocellular carcinoma in the non-cirrhotic
liver. Dig Surg. 21:380–386. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lang H, Sotiropoulos GC, Brokalaki EI,
Schmitz KJ, Bertona C, Meyer G, Frilling A, Paul A, Malagó M and
Broelsch CE: Survival and recurrence rates after resection for
hepatocellular carcinoma in noncirrhotic livers. J Am Coll Surg.
205:27–36. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hendrich B, Abbott C, Mcqueen H, Chambers
D, Cross S and Bird A: Genomic structure and chromosomal mapping of
the murine and human Mbd1, Mbd2, Mbd3 and Mbd4 genes. Mamm Genome.
10:906–912. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Xiong Y, Dowdy SC, Eberhardt NL, Podratz
KC and Jiang SW: hMLH1 promoter methylation and silencing in
primary endometrial cancers are associated with specific
alterations in MBDs occupancy and histone modifications. Gynecol
Oncol. 103:321–328. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Auriol E, Billard LM, Magdinier F and
Dante R: Specific binding of the methyl binding domain protein 2 at
the BRCA1-NBR2 locus. Nucleic Acids Res. 33:4243–4254. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Mian OY, Wang SZ, Zhu SZ, Gnanapragasam
MN, Graham L, Bear HD and Ginder GD: Methyl-binding domain protein
2-dependent proliferation and survival of breast cancer cells. Mol
Cancer Res. 9:1152–1162. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Campbell PM, Bovenzi V and Szyf M:
Methylated DNA-binding protein 2 antisense inhibitors suppress
tumourigenesis of human cancer cell lines in vitro and in vivo.
Carcinogenesis. 25:499–507. 2004. View Article : Google Scholar
|
|
10
|
Bakker J, Lin X and Nelson WG: Methyl-CpG
binding domain protein 2 represses transcription from
hypermethylated pi-class glutathione S-transferase gene promoters
in hepatocellular carcinoma cells. J Biol Chem. 277:22573–22580.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Stefanska B, Suderman M, Machnes Z,
Bhattacharyya B, Hallett M and Szyf M: Transcription onset of genes
critical in liver carcinogenesis is epigenetically regulated by
methylated DNA-binding protein MBD2. Carcinogenesis. 34:2738–2749.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ballestar E, Yusufzai TM and Wolffe AP:
Effects of Rett syndrome mutations of the methyl-CpG binding domain
of the transcriptional repressor MeCP2 on selectivity for
association with methylated DNA. Biochemistry. 39:7100–7106. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wade PA: Methyl CpG-binding proteins and
transcriptional repression. Bioessays. 23:1131–1137. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Barr H, Hermann A, Berger J, Tsai HH, Adie
K, Prokhortchouk A, Hendrich B and Bird A: Mbd2 contributes to DNA
methylation-directed repression of the Xist gene. Mol Cell Biol.
27:3750–3757. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hendrich B and Bird A: Identification and
characterization of a family of mammalian methyl-CpG binding
proteins. Mol Cell Biol. 18:6538–6547. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Shukeir N, Pakneshan P, Chen G, Szyf M and
Rabbani SA: Alteration of the methylation status of tumor-promoting
genes decreases prostate cancer cell invasiveness and tumorigenesis
in vitro and in vivo. Cancer Res. 66:9202–9210. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Stefanska B, Huang J, Bhattacharyya B,
Suderman M, Hallett M, Han ZG and Szyf M: Definition of the
landscape of promoter DNA hypomethylation in liver cancer. Cancer
Res. 71:5891–5903. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Pakneshan P, Szyf M, Farias-Eisner R and
Rabbani SA: Reversal of the hypomethylation status of urokinase
(uPA) promoter blocks breast cancer growth and metastasis. J Biol
Chem. 279:31735–31744. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Martin V, Jørgensen HF, Chaubert AS,
Berger J, Barr H, Shaw P, Bird A and Chaubert P: MBD2-mediated
transcriptional repression of the p14ARF tumor suppressor gene in
human colon cancer cells. Pathobiology. 75:281–287. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Slack A, Bovenzi V, Bigey P, Ivanov MA,
Ramchandani S, Bhattacharya S, tenOever B, Lamrihi B, Scherman D
and Szyf M: Antisense MBD2 gene therapy inhibits tumorigenesis. J
Gene Med. 4:381–389. 2002. View
Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ivanov MA, Lamrihi B, Szyf M, Scherman D
and Bigey P: Enhanced antitumor activity of a combination of
MBD2-antisense electrotransfer gene therapy and bleomycin
electrochemotherapy. J Gene Med. 5:893–899. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Liu XY, Tang SH, Wu SL, Luo YH, Cao MR,
Zhou HK, Jiang XW, Shu JC, Bie CQ, Huang SM, et al: Epigenetic
modulation of insulin-like growth factor-II overexpression by
hepatitis B virus X protein in hepatocellular carcinoma. Am J
Cancer Res. 5:956–978. 2015.PubMed/NCBI
|
|
23
|
Ataide EC, Boin IF, Almeida JR,
Sevá-Pereira T, Stucchi RS, Cardoso AR, Caruy CA and Escanhoela CA:
Prognostic factors for hepatocellular carcinoma recurrence:
Experience with 83 liver transplantation patients. Transplant Proc.
43:1362–1364. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Nobuoka D, Kato Y, Gotohda N, Takahashi S,
Nakagohri T, Konishi M, Kinoshita T and Nakatsura T: Postoperative
serum alpha-fetoprotein level is a useful predictor of recurrence
after hepatectomy for hepatocellular carcinoma. Oncol Rep.
24:521–528. 2010.PubMed/NCBI
|
|
25
|
Llovet JM, Burroughs A and Bruix J:
Hepatocellular carcinoma. Lancet. 362:1907–1917. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Bruix J and Sherman M; Practice Guidelines
Committee American Association for the Study of Liver Diseases:
Management of hepatocellular carcinoma. Hepatology. 42:1208–1236.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Tandon P and Garcia-Tsao G: Prognostic
indicators in hepatocellular carcinoma: A systematic review of 72
studies. Liver Int. 29:502–510. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
van Malenstein H, van Pelt J and Verslype
C: Molecular classification of hepatocellular carcinoma anno 2011.
Eur J Cancer. 47:1789–1797. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sumie S, Kuromatsu R, Okuda K, Ando E,
Takata A, Fukushima N, Watanabe Y, Kojiro M and Sata M:
Microvascular invasion in patients with hepatocellular carcinoma
and its predictable clini-copathological factors. Ann Surg Oncol.
15:1375–1382. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Eguchi S, Takatsuki M, Hidaka M, Soyama A,
Tomonaga T, Muraoka I and Kanematsu T: Predictor for histological
micro-vascular invasion of hepatocellular carcinoma: A lesson from
229 consecutive cases of curative liver resection. World J Surg.
34:1034–1038. 2010. View Article : Google Scholar : PubMed/NCBI
|