Introduction
Malignant digestive tumors are a growing concern in
human health. In China, the incidence and mortality rates
associated with malignant digestive tumors appear to be steadily
increasing. Among the different types of digestive malignant
tumors, liver and pancreatic cancers remain the most difficult to
diagnosis and treat. New treatments are continuously developed,
however, the overall survival rate has only modestly improved over
the past decade. Liver cancer is the fifth most common cancer in
the world and the third leading cause of cancer-associated
mortality worldwide (1,2). Pancreatic cancer is the fourth
leading cause of cancer-associated mortality globally (3). The World Health Organization
classifies primary liver cancers into hepatocellular carcinoma
(HCC), intrahepatic cholangiocarcinoma (ICC) and combined
hepatocellular-cholangiocarcinoma (4). HCC represents the major histological
subtype of primary liver cancer, however the incidence of ICC, the
second most frequent type of liver cancer, has increased
dramatically over the past two decades (5).
Sex determining region Y-box 7 (SOX7), SOX17 and
SOX18, belong to the SOX group F subfamily (6). SOX7 encodes a high mobility group box
transcription factor and has been implicated in a number of
developmental processes (7),
including hematopoiesis (8),
cardiogenesis (9), vasculogenesis
(10), endoderm differentiation
(11) and myogenesis (12). As a transcription factor, SOX7
activates target genes and regulates the Wnt/β-catenin signaling
pathway (13). SOX7 may compete
with T-cell factor (TCF)/lymphoid enhancing factor (LEF) activity
by interacting with β-catenin and inhibiting the expression of
target genes. Previous studies have observed that SOX7 expression
is deregulated in different human cancer types compared with SOX7
in normal tissues (14–16). Katoh (17) revealed that SOX7 expression levels
were increased in a number of pancreatic, gastric and esophageal
cancer cell lines, and also in 4 cases of primary gastric cancer.
The majority of other studies investigating SOX7 expression in
cancer have demonstrated a downregulation of SOX7 expression levels
in a variety of human cancer types, including breast (18), lung (15), colon (14) and prostate (19). A decrease in SOX7 expression levels
has been associated with poor prognosis in lung adenocarcinoma
(15) and prostate cancer
(19). However, the clinical
significance of SOX7 expression in liver and pancreatic cancers
remains unclear. Thus, the aim of the present study was to
investigate the association between SOX7 expression and tumor
progression and prognosis in patients with liver and pancreatic
cancer.
Materials and methods
Patients and tissue samples
The present study was approved by the Ethics
Committee of Guangzhou First People's Hospital, Guangzhou Medical
University (Guangdong, China). All procedures performed involving
human participants were in accordance with the ethical standards of
the institutional and/or national research committee and with the
1964 Helsinki declaration and its later amendments or comparable
ethical standards. All applicable international, national, and/or
institutional guidelines for the care and use of animals were
followed. Informed consent was obtained from all individual
participants included in the study. Tissue microarrays (TMAs) were
obtained from Xi'an Ailina Biotechnology Co., Ltd. (Xi'an, China).
The HCC TMA (cat. no. LV802a) used in the present study contained
78 primary HCC and 2 adjacent non-cancerous liver tissues, with the
age of the donors ranging between 18 and 73 years (mean age, 51.78
years). The ICC TMA (cat. no. LV1004) used contained 100 primary
ICC tissues that were collected from 42 female and 58 male patients
(age range, 27 to 74 years; mean age, 54.72 years), and 5 adjacent
normal tissues were recruited from the Huadu District People's
Hospital (Guangzhou, China) in September 2015 as the ICC TMA did
not contain any normal tissues. Of the HCC and ICC TMA samples, 1
sample from each TMA was removed, and 3 samples were interstitial
samples, which were also not analyzed. Therefore, the total number
of cancer samples analyzed in HCC and ICC TMAs was 173. The
pancreatic microarray (cat. no. PA961b) contained 91 pancreatic
cancer tissues and 5 normal pancreatic tissues that were collected
from patients aged 21 to 78 years old (mean age, 51.87 years). As 3
pancreatic cancer samples could not be evaluated and scored for the
percentage of staining, a total of 88 pancreatic cancer samples
were analyzed for SOX7 protein expression.
To investigate the expression of SOX7 at the mRNA
level, the Cancer Genome Atlas (TCGA) dataset, a large cancer
dataset with high-throughput sequencing data for protein coding
genes (mRNA), which includes 134 HCC tissues, was used (https://tcga-data.nci.nih.gov, liver hepatocellular
carcinoma). Detailed information regarding the clinical features of
the patients is presented in Table
I.
 | Table I.Clinical features of the patients
recruited in the present study. |
Table I.
Clinical features of the patients
recruited in the present study.
|
| Immunohistochemistry
results |
|
|---|
|
|
|
|
|---|
| Clinical feature | Liver | Pancreatic | Liver TCGA
dataset |
|---|
| Total no. of cancer
cases | 178 | 91 | 134 |
| Gender (n) |
|
|
|
| Male | 120 | 56 | 80 |
|
Female | 58 | 35 | 54 |
| Age (n) |
|
|
|
|
<60 | 124 | 71 | 67 |
| ≥60 | 54 | 20 | 67 |
| Mean age (years) | 53.41±11.11 | 52.70±9.96 | 62.10±13.34 |
| Pathological grade
(n) |
|
|
|
| ≤2 | 77 | 51 | – |
|
>2 | 89 | 15 | – |
| Clinical stage
(n) |
|
|
|
| I/II | 80 | 84 | – |
|
III/IV | 98 | 6 | – |
| I | – | – | 50 |
|
II–IV | – | – | 75 |
| pT stage (n) |
|
|
|
|
T1-T2 | 91 | 34 | 53 |
|
T3-T4 | 86 | 56 | 81 |
| pN stage (n) |
|
|
|
| N0 | 144 | 78 | 83 |
|
N1/N2 | 33 | 12 | 3 |
| Metastasis (n) | 3 | 2 | 3 |
| Benign (n) | 7 | 5 | 0 |
Immunohistochemistry
The TMA slides were deparaffinized with xylene and
then serially rehydrated with ethanol (100, 100, 95, 95, 90, 80 and
70%). Following brief proteolytic digestion using the IHC enzyme
antigen retrieval agent (Wuhan Boster Biological Technology, Ltd.,
Wuhan, China) and peroxidase blocking with 3%
H2O2, the slides were incubated at 4°C
overnight with a rabbit polyclonal primary antibody against SOX7
(dilution, 1:200; cat. no. sc-20,093; Santa Cruz Biotechnology,
Inc., Dallas, TX, USA). Following washing with PBS to remove any
unbound primary antibodies, the slides were incubated for 30 min
with peroxidase-conjugated secondary antibody (HRP-labeled Goat
Anti-Rabbit IgG; dilution, 1:1,000; cat. no. A0208; Beyotime
Institute of Biotechnology Co., Ltd., Haimen, China) at room
temperature. The specifically bound secondary antibody was detected
using a DAKO EnVision detection system (Dako Diagnostics; Agilent
Technologies, Inc., Santa Clara, CA, USA).
Evaluation of staining
Following counterstaining with hematoxylin, stained
TMAs were scanned by Xi'an Ailina Biotechnology Co., Ltd. using a
digital high resolution microscope scanner (Aperio ScanScope;
Aperio Technologies, Inc., Vista, CA, USA) and viewed using
ImageScope v.11 software (Aperio Technologies, Inc.). Protein
expression was scored by two independent, experienced pathologists
who were unaware of the clinical data and patient outcomes. The two
sets of scores produced were compared and the discrepant scores
were re-examined by the two pathologists to achieve a consensus
score. The number of positively stained cells was counted in 10
representative microscopic fields, and the percentage of positively
stained cells was calculated. Given the homogeneity of the target
protein staining, the tumor specimens were scored in a
semi-quantitative manner. The percentage scoring of immunoreactive
tumor cells was as follows: 0, no staining; 1, weak; 2, moderate;
and 3, strong. The specimens were also evaluated and scored for the
percentage of staining as follows: 1, 0–25%; 2, 25–50%; 3, 50–75%;
and 4, 75–100%. A final immunoreactivity score (IRS) was obtained
for each case by summing the percentage and the intensity scores.
Protein expression levels were further analyzed by classifying the
IRS values as low or high, based on the median IRS value.
Statistical analysis
SPSS 21.0 software (IBM SPSS, Armonk, NY, USA) was
used for statistical analysis. Pearson's Chi-squared tests and
Fisher's exact test were used to analyze the association between
SOX7 protein expression and clinicopathological characteristics.
Student's t-test was used to analyze the association between SOX7
mRNA expression and clinicopathological characteristics. Overall
survival was analyzed using the Kaplan-Meier method, and the
differences were assessed using a log-rank test. Univariate
analysis comparisons [comparisons between gender, age, the clinical
stage, the pathological tumor node metastasis (pTNM) stage and SOX7
mRNA expression] and multivariate survival comparisons were
performed using Cox proportional hazard regression models. The
relative risks of mortality were expressed as adjusted hazard
ratios (HRs) with corresponding 95% confidence intervals (CIs).
P<0.05 was considered to indicate a statistically significant
difference.
Results
SOX7 protein expression is increased
in human liver and pancreatic cancers
The present study investigated whether SOX7
expression is altered with clinical cancer specimens by analyzing
liver and pancreatic TMAs (Table
I). In these TMAs, the expression profile and localization of
SOX7 in the 173 liver cancer tissues and 7 adjacent non-cancerous
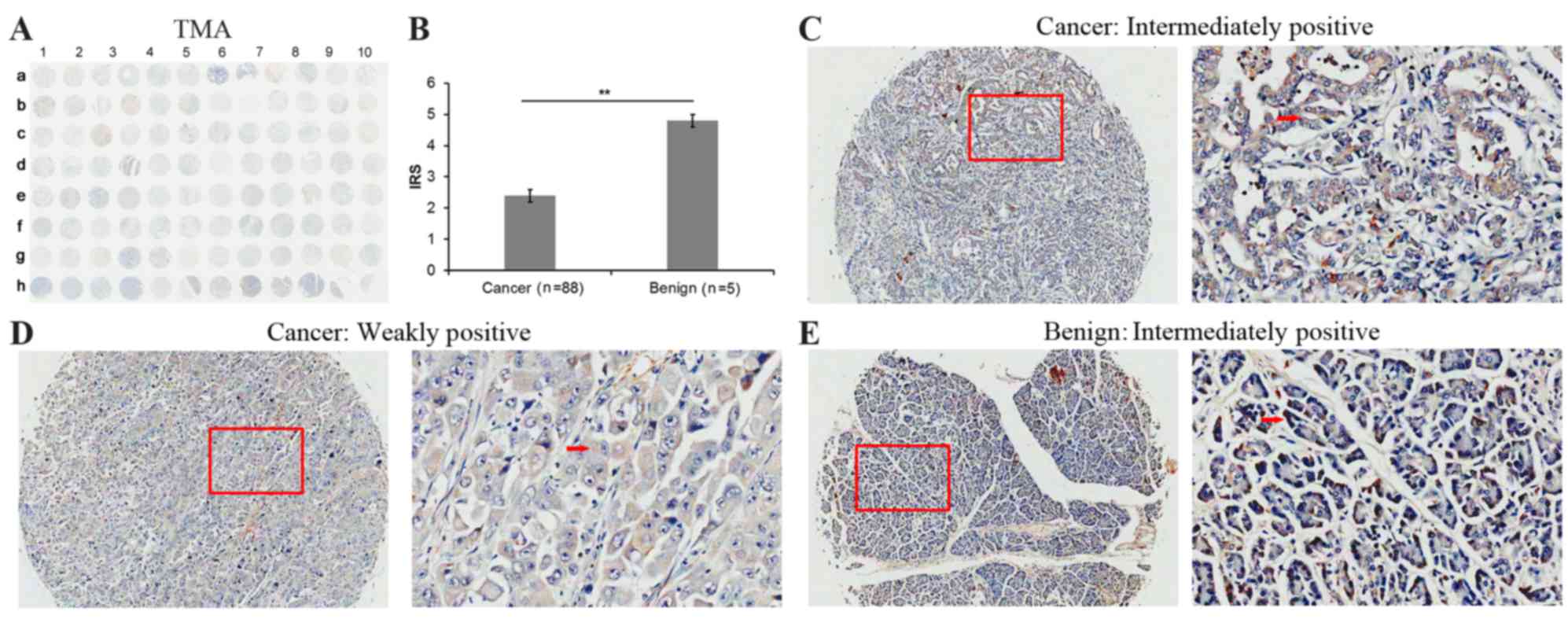
liver tissues (Fig. 1), and 88
pancreatic cancer tissues and 5 adjacent non-cancerous pancreatic
tissues (Fig. 2) were examined by
immunohistochemical analyses.
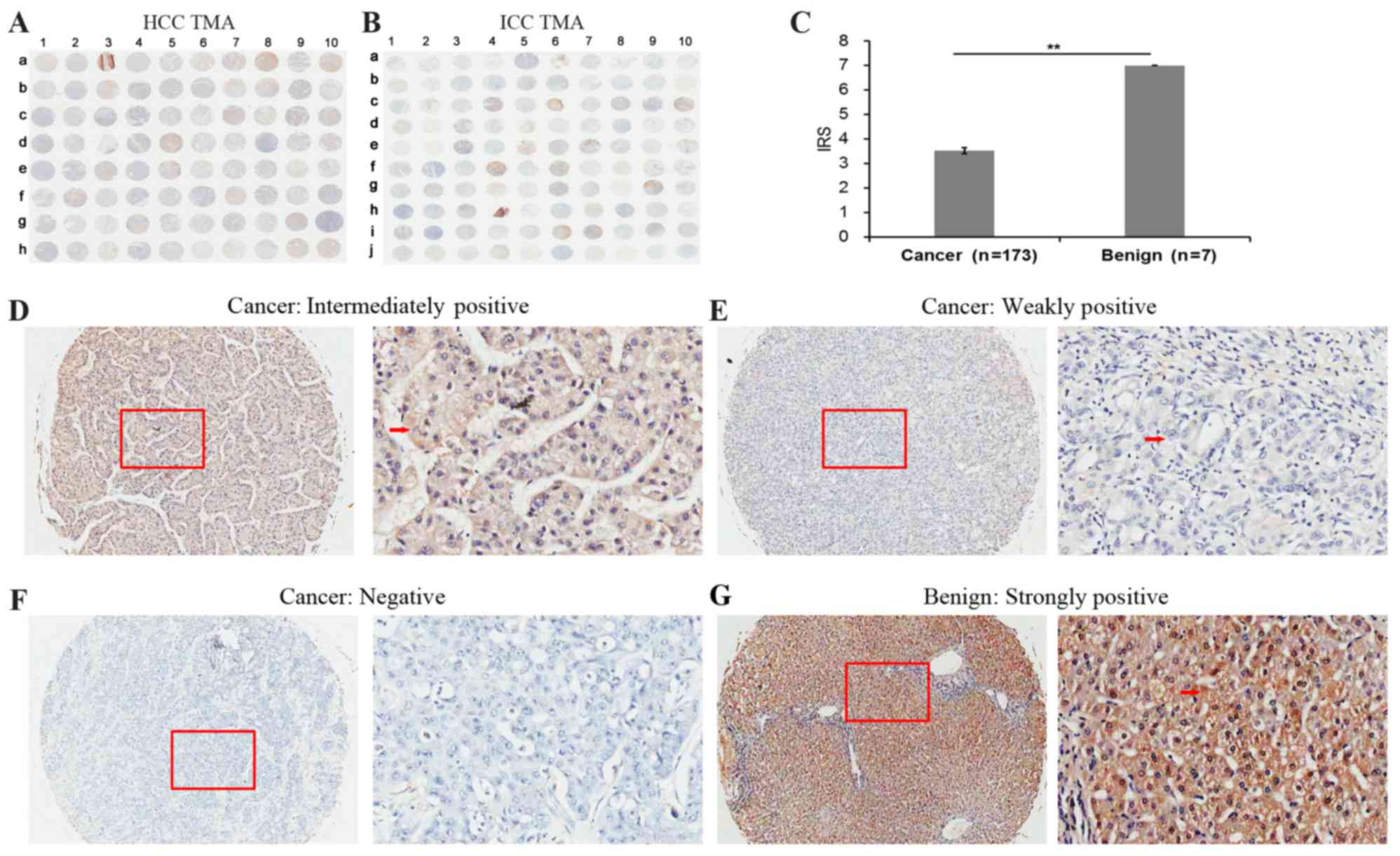 | Figure 1.Immunohistochemical staining for SOX7
in liver cancer and adjacent non-cancerous liver tissues in a TMA.
Immunohistochemistry staining for SOX7 in the (A) HCC and (B) ICC
TMA cohorts. (C) IRS of SOX7 in liver cancer were lower than those
observed in the adjacent normal liver tissues. IRS: **P<0.001,
liver cancer (3.53±1.57) vs. benign (7.00±0.00). Data are presented
as the mean ± standard deviation. Immunohistochemistry staining
indicated that SOX7 immunostaining primarily occurred in the
cytoplasm and cellular membrane of liver cancer tissues cells. The
intensities of SOX7 immunostaining were (D) intermediate, (E) weak
and (F) negative, no strong staining was observed in cancer
samples. Left image, magnification ×100; right image, magnification
×400; the red squares indicate the area shown at higher
magnification. (G) Strongly positive immunohistochemistry staining
in the adjacent non-cancerous liver tissue cells. Red arrows
indicate positively-stained cells. SOX7, sex determining region
Y-box 7; HCC, hepatocellular carcinoma; TMA, tissue microarrays;
ICC, intrahepatic cholangiocarcinoma; IRS, immunoreactivity
scores. |
The SOX7 expression level in liver cancer tissues
(Fig. 1A and B) was significantly
lower than that observed in non-cancerous liver tissues [IRS: Liver
cancer (3.53±1.57) vs. benign (7.00±0.00), P<0.001; Fig. 1C). Immunohistochemistry revealed
weak or moderate SOX7 staining in the cytoplasm of liver cancer
cells (Fig. 1D-F) however, strong
SOX7 staining was observed in the adjacent non-cancerous liver
tissues (Fig. 1G). As observed in
the cancerous liver tissues, SOX7 protein was expressed in the
cytoplasm of pancreatic cancer cells and adjacent non-cancerous
pancreatic tissue cells (Fig. 2A).
However, the level of SOX7 expression was different between the two
cancer types (Fig. 2B-E). In
pancreatic cancer tissues the level of SOX7 expression was
significantly lower than that observed in non-cancerous pancreatic
tissues [IRS: Pancreatic cancer (2.39±1.88) vs. benign (4.80±0.45),
P=0.005; Fig. 2B).
The immunostaining results were analyzed further
using the limited quantity of clinical information regarding the
liver and pancreatic TMAs of the donors (Tables II and III). The liver TMA results indicated
that a low level of SOX7 expression is significantly associated
with higher clinical stage (P<0.001), high primary pathological
tumor (pT) stage (P=0.006) and a high regional lymph node (pN)
stage (P=0.002) however, it was not associated with age (P=0.313),
gender (P=0.328) or pathological grade (P=0.448). The pancreatic
TMA results (Table III)
indicated that a low level of SOX7 expression is significantly
associated with a high pathological grade (P=0.026), however, it is
not associated with age (P=0.378), gender (P=0.132), clinical stage
(P=0.305), pT stage (P=0.718), pN stage (P=0.097) or pathological
metastasis (pM) stage (P=0.411).
| Table II.Associations between SOX7 expression
and clinicopathological characteristics in patients with liver
cancer. |
Table II.
Associations between SOX7 expression
and clinicopathological characteristics in patients with liver
cancer.
|
| IRS of SOX7 protein
expression in the cohort | SOX7 mRNA
expression in TCGA database |
|---|
|
|
|
|
|---|
| Clinical
feature | No. of total
cases | No. of low (% of
total no.) | No. of high (% of
total no.) | P-value | No. of total
cases | x±s | P-value |
|---|
| Tissue |
|
|
| 0.022a |
|
| – |
|
Cancer | 173 | 118 (68.2) | 55 (31.8) |
| 134 | 144.81±166.64 |
|
|
Benign | 7 | 3 (42.9) | 4 (57.1) |
| – | – |
|
| Age |
|
|
| 0.313 |
|
| 0.978 |
|
<60 | 120 | 79 (65.8) | 41 (34.2) |
| 67 | 144.41±164.23 |
|
|
≥60 | 53 | 39 (73.6) | 14 (26.4) |
| 67 | 145.21±170.26 |
|
| Gender |
|
|
| 0.328 |
|
| 0.340 |
|
Male | 117 | 77 (65.8) | 40 (34.2) |
| 80 | 156.13±187.80 |
|
|
Female | 56 | 41 (73.2) | 15 (26.8) |
| 54 | 128.03±128.98 |
|
| Pathological
grade |
|
|
| 0.448 |
|
| – |
| ≤2 | 77 | 55 (71.4) | 22 (28.6) |
| – | – |
|
|
>2 | 85 | 56 (65.9) | 29 (34.1) |
| – | – |
|
| Clinical stage |
|
|
| <0.001b |
|
| 0.012a |
|
I/II | 75 | 27 (36.0) | 48 (64.0) |
| – | – |
|
|
III/IV | 98 | 91 (92.9) | 7 (7.1) |
| – | – |
|
| I | – | – | – | – | 50 | 187.66±227.94 |
|
|
II–IV | – | – | – | – | 75 | 111.95±96.99 |
|
| pT stage |
|
|
| 0.006b |
|
| 0.010a |
| T1 | 54 | 29 (53.7) | 25 (46.3) |
| 53 | 190.64±230.06 |
|
|
T2-T4 | 119 | 89 (74.8) | 30 (25.2) |
| 81 | 114.82±97.27 |
|
| pN stage |
|
|
| 0.002b |
|
| 0.004b |
| N0 | 139 | 87 (62.6) | 52 (37.4) |
| 83 | 156.05±178.34 |
|
| N1 | 33 | 30 (90.9) | 3 (9.1) |
| 3 | 50.42±32.27 |
|
| pM stage |
|
|
| 0.231 |
|
| 0.037a |
| M0 | 169 | 114 (67.5) | 55 (32.5) |
| 98 | 143.94±168.04 |
|
| M1 | 3 | 3 (100.0) | 0 (0.0) |
| 3 | 100.87±16.91 |
|
| Table III.Association between SOX7 protein
expression and clinicopathological characteristics in patients with
pancreatic carcinoma. |
Table III.
Association between SOX7 protein
expression and clinicopathological characteristics in patients with
pancreatic carcinoma.
| Clinical
feature | No. of total
cases | SOX7 protein
expression (x±s) | P-value |
|---|
| Tissue |
|
| 0.002a |
|
Cancer | 88 | 1.89±1.87 |
|
|
Normal | 5 | 4.80±0.45 |
|
| Age (years) |
|
| 0.378 |
|
<50 | 29 | 2.14±2.22 |
|
|
≥50 | 59 | 1.76±1.68 |
|
| Gender |
|
| 0.132 |
|
Males | 54 | 2.26±2.39 |
|
|
Female | 34 | 1.65±1.42 |
|
| Pathological
grade |
|
| 0.026b |
|
<2 | 21 | 2.38±1.47 |
|
| ≥2 | 44 | 1.36±1.78 |
|
| Clinical stage |
|
| 0.305 |
|
I/II | 81 | 1.85±1.78 |
|
|
III/IV | 6 | 2.67±2.94 |
|
| pT stage |
|
| 0.718 |
|
T1/T2 | 32 | 1.81±1.58 |
|
| T3 | 55 | 1.96±2.03 |
|
| pN stage |
|
| 0.097 |
| N0 | 75 | 2.28±1.86 |
|
| N1 | 12 | 3.25±1.82 |
|
| pM stage |
|
|
|
| M0 | 85 | 2.39±1.89 | 0.411 |
| M1 | 2 | 3.50±0.71 |
|
Decreased SOX7 expression is
associated with the aggressive progression and poor prognosis of
human liver cancer in the TCGA dataset
To validate the results of the TMA cohort, a
publicly available dataset was used. The TCGA dataset (https://tcga-data.nci.nih.gov), consists of
high-throughput sequencing data for protein coding gene expression
(mRNA) data from 134 liver cancer tissues. The data presented in
Table II revealed that SOX7
downregulation is frequently identified in liver cancer tissues
with an advanced clinical stage (P=0.045), pT stage (P=0.010), pN
stage (P=0.004) or pM stage (P=0.037). However, SOX7 expression was
not significantly different when comparing patient gender (female
vs. male, P=0.340) or age (<60 vs. ≥60 years, P=0.978).
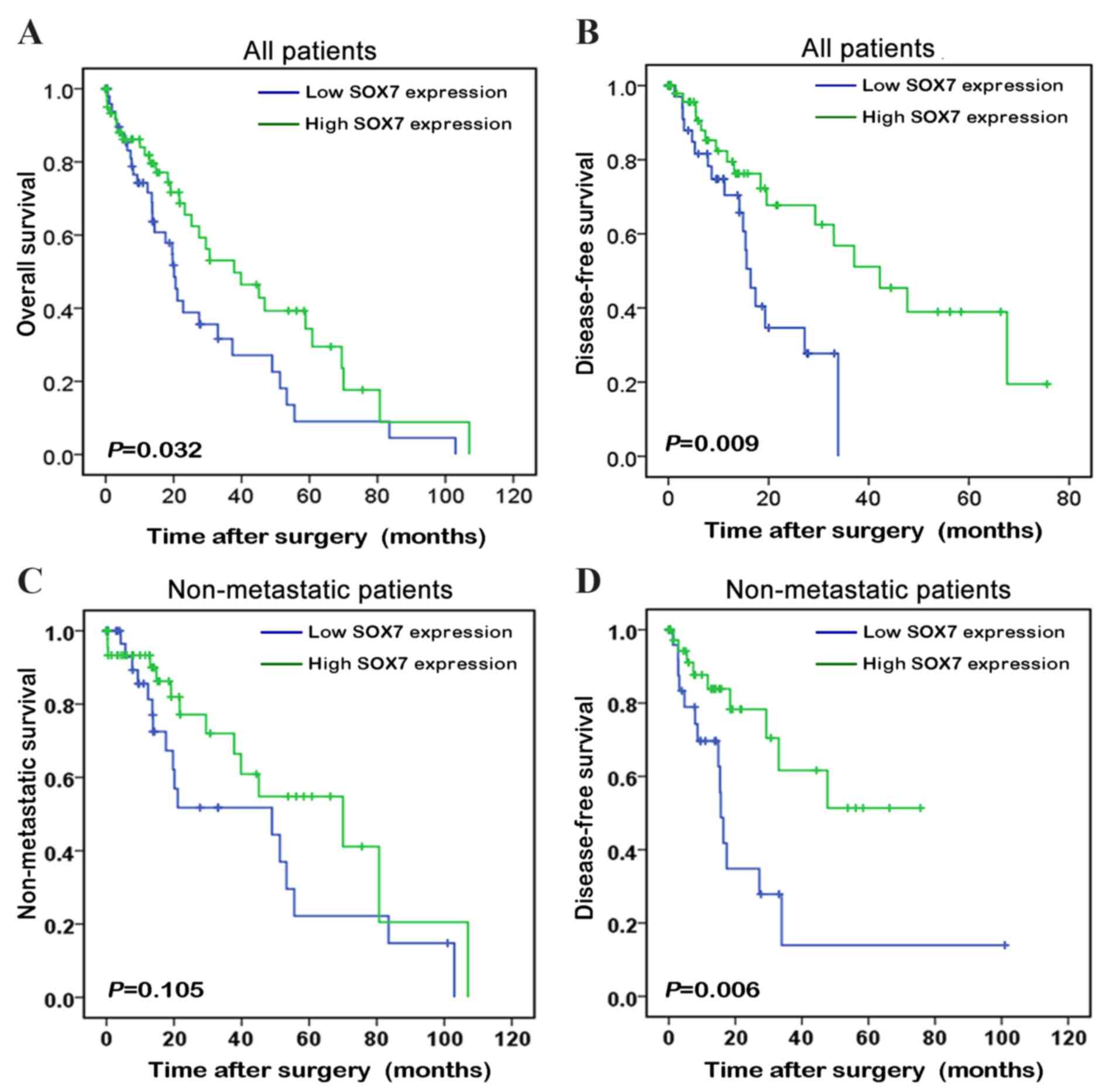
To demonstrate the prognostic value of detecting
SOX7 expression levels in patients with liver cancer, the
Kaplan-Meier method was performed to compare the prognosis among
patients with high and low SOX7 expression levels (Fig. 3). The mean level of SOX7 mRNA
expression in the TCGA dataset was used as the cut-off to divide
patients with liver cancer into the high and low SOX7 expression
groups. The patients with liver cancer and low SOX7 expression
levels had a poorer prognosis than those with high SOX7 expression
levels (P=0.032; Fig. 3A), and
their length of biochemical recurrence (BCR)-free survival time was
significantly shorter than that of patients with high SOX7
expression levels (P=0.009; Fig.
3B). When the liver patients with metastases were removed from
the analysis, pairwise comparisons revealed no significant
differences in the lengths of BCR-free survival time between the
two groups (P=0.105; Fig. 3C);
however, SOX7 expression was able to stratify the non-metastatic
patients into those with a high risk and a low risk of BCR
(P=0.006; Fig. 3D).
SOX7 expression serves as an
independent predictor of disease-free survival in patients with
liver cancer
The present study also investigated whether SOX7
expression levels were an effective independent predictor of
disease-free survival in the patients with liver cancer from the
TCGA dataset by performing univariate and multivariate analyses.
Patients with liver cancer and low tumor levels of SOX7 expression
had significantly lower disease-free survival rates than those with
high tumor levels of SOX7 expression (Table IV). The SOX7 expression level (HR:
0.314; 95% CI: 0.130–0.760; P=0.010) and the pM stage (HR: 10.922;
95% CI: 1.897–62.883; P=0.007) were able to serve as independent
predictors for disease-free survival (Table IV). This suggests that the SOX7
expression level may be an independent predictor for disease-free
survival in patients with liver cancer.
| Table IV.Prognostic value of SOX7 mRNA
expression for biochemical recurrence-free survival evaluated by
the Cox proportional hazards model. |
Table IV.
Prognostic value of SOX7 mRNA
expression for biochemical recurrence-free survival evaluated by
the Cox proportional hazards model.
| A, BCR free
survival univariate analysis |
|---|
|
|---|
| Variable | HR (95% CI) | P-value |
|---|
| Age (<60 vs. ≥60
years) | 0.750
(0.349–1.614) | 0.462 |
| Gender (male vs.
female) | 0.615
(0.314–1.202) | 0.155 |
| Clinical stage (I
vs. II–IV) | 1.754
(0.804–3.789) | 0.159 |
| pT stage (T1 vs.
T2-T4) | 1.889
(0.919–3.884) | 0.084 |
| pN stage (N0 vs.
N1) | 0.893
(0.119–6.682) | 0.912 |
| pM stage (M0 vs.
M1) | 5.454
(1.204–24.709) | 0.028a |
| SOX7 (low vs. high
expression) | 0.499
(0.251–0.991) | 0.047a |
|
| B, BCR free
survival multivariate analysis |
|
| Age (<60 vs. ≥60
years) | 0.597
(0.221–1.610) | 0.308 |
| Gender (male vs.
female) | 0.895
(0.336–2.185) | 0.807 |
| pM stage (M0 vs.
M1) | 10.922
(1.897–62.883) | 0.007b |
| SOX7 (low vs. high
expression) | 0.314
(0.130–0.760) | 0.010a |
Discussion
The majority of digestive malignant tumors,
including liver and pancreatic cancers, are diagnosed at an
advanced stage, when clinical deterioration has occurred and
curative therapies are no longer effective (20,21).
Therefore, the early detection of HCC and pancreatic cancers,
particularly at a time when curative surgery can still be
performed, is potentially the best method to improve patient
prognosis (21,22). Thus, screening novel tumor
biomarkers is important for the prevention, diagnosis and targeted
therapy of liver and pancreatic cancers. The present study
demonstrated that there are reduced levels of SOX7 expression in
liver and pancreatic cancer tissues, which may serve a suppressive
role in the progression of these cancer types. To the best of our
knowledge, this is the first study in which the association between
the level of SOX7 expression and the clinicopathological features
of liver and pancreatic cancers, particularly its prognostic
significance, has been extensively investigated.
A previous study suggested that SOX genes are widely
expressed and serve a role in the regulation of the Wnt/β-catenin
signaling pathway during development (23). A motif in the SOX7 protein enables
it to bind to β-catenin, permitting their interaction (24), and so SOX7 is a key regulator in
embryonic development. In addition, the Wnt/β-catenin signaling
pathway is known to have important roles in a number of
malignancies, including lung, breast, colorectal, ovarian and liver
cancer. A number of studies have revealed that SOX7 has an
important role in tumorigenesis (10). In 2002, Katoh (17) demonstrated that SOX7 mRNA was
significantly upregulated in esophageal cancer cell lines and in a
primary gastric cancer cell line, however, it was downregulated in
primary colorectal tumors, prostate cancer, lung cancer and breast
cancer, indicating that the role of SOX7 in tumorigenesis may
depend on the tumor type. To the best of our knowledge, the role of
SOX7 in liver and pancreatic cancer has not been previously
investigated, therefore the present study analyzed SOX7 protein
levels in a human liver TMA (including 78 HCC tissues and 100 ICC
tissues) and a pancreatic cancer TMA (containing 91 pancreatic
cancer tissues and 5 adjacent non-cancerous pancreatic tissues).
The results demonstrate that SOX7 expression levels decrease in
liver and pancreatic cancers.
SOX7 expression was previously reported to be
negatively correlated with the depth of invasion, lymph node
metastasis, distant metastasis and pTNM stage in gastric cancer
patients (25). Li et al
(15) demonstrated that reduced
SOX7 expression was significantly associated with poor
differentiation (P=0.002), lymph node metastasis (P=0.011) and
advanced TNM stage (P=0.006). Similarly, the present study
investigated the association between the level of SOX7 protein and
the clinicopathological features of the donors who were included in
the TMAs. The results indicate that the downregulation of SOX7
expression levels in liver cancer was markedly associated with
advanced clinical stage, pT stage and pN stage. Notably, these
findings were further validated using the TCGA dataset. However, in
the pancreatic cancer TMA dataset, SOX7 expression levels were not
associated with advanced clinical stage or pTNM stage; it was only
significant associated with the pathological grade of pancreatic
cancer. These results support the hypothesis that the loss of SOX7
activity may critically contribute to cancer severity.
Previous studies have demonstrated that SOX7
expression in lung, prostate and gastric cancers is associated with
the prognosis or survival of patients (14,15,19,25).
In the present study, due to the limited number of clinical
specimens and follow-ups available for patients with liver cancer,
the prognostic value of SOX7 was assessed based only on the TCGA
dataset, which consisted of 134 liver cancer tissues with
high-throughput sequencing data for mRNA expression. The results
suggest that decreased expression of SOX7 is associated with poor
prognosis in patients with liver cancer. The overall survival and
the disease-free survival were shorter in patients with low SOX7
expression cancer types than in those with high SOX7 expression
cancer types. These results are consistent with previous work
(19), suggesting that the reduced
expression of SOX7 may be a potential biomarker for poor prognosis
in patients with liver cancer.
Previous evidence suggests that SOX7 may have tumor
suppressive functions in a number of cancer types (14–16).
Multiple reports have indicated that SOX7 inhibits proliferative
β-catenin signaling via direct protein interactions, suggesting
that it antagonizes tumor growth, at least in part, through
activities that are independent of DNA binding (25). Takash et al (24) demonstrated that SOX7 inhibits
TCF/LEF-β-catenin activation of the TCF/LEF-dependent TOPFLASH
reporter in HEK293 cells, an observation that was later
recapitulated in colon and prostate cancer cell lines (14,26).
In addition, SOX7 co-localizes and physically interacts with
β-catenin in endometrial cancer cells (16).
In conclusion, the results suggest that the
decreased expression of SOX7 is an important feature of liver
cancer. The expression levels of the SOX7 protein may be a
potential indicator for predicting the clinical outcome of patients
with liver cancer. The results of the present study may
significantly contribute to the understanding of the molecular
mechanisms underlying carcinogenesis and disease progression in
liver cancer.
Acknowledgements
The present study was supported by the Science and
Technology Project of Huadu District of Guangzhou (grant no.
15-HDWS-012).
References
|
1
|
McGlynn KA, Tsao L, Hsing AW, Devesa SS
and Fraumeni JF Jr: International trends and patterns of primary
liver cancer. Int J Cancer. 94:290–296. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Mittal S and El-Serag HB: Epidemiology of
hepatocellular carcinoma: Consider the population. J Clin
Gastroenterol. 47:(Suppl). S2–S6. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wolfgang CL, Herman JM, Laheru DA, Klein
AP, Erdek MA, Fishman EK and Hruban RH: Recent progress in
pancreatic cancer. CA Cancer J Clin. 63:318–348. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Bosman FT, Carneiro F, Hruban RH and
Theise ND: WHO classification of tumours of the digestive system.
Geneva: World Health Organization; 2010
|
|
5
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wegner M: From head to toes: The multiple
facets of Sox proteins. Nucleic Acids Res. 27:1409–1420. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Stovall DB, Cao P and Sui G: SOX7: From a
developmental regulator to an emerging tumor suppressor. Histol
Histopathol. 29:439–445. 2014.PubMed/NCBI
|
|
8
|
Gandillet A, Serrano AG, Pearson S,
Lie-A-Ling M, Lacaud G and Kouskoff V: Sox7-sustained expression
alters the balance between proliferation and differentiation of
hematopoietic progenitors at the onset of blood specification.
Blood. 114:4813–4822. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nelson TJ, Chiriac A, Faustino RS,
Crespo-Diaz RJ, Behfar A and Terzic A: Lineage specification of
Flk-1+ progenitors is associated with divergent Sox7 expression in
cardiopoiesis. Differentiation. 77:248–255. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cermenati S, Moleri S, Cimbro S, Corti P,
Del Giacco L, Amodeo R, Dejana E, Koopman P, Cotelli F and Beltrame
M: Sox18 and Sox7 play redundant roles in vascular development.
Blood. 111:2657–2666. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Séguin CA, Draper JS, Nagy A and Rossant
J: Establishment of endoderm progenitors by SOX transcription
factor expression in human embryonic stem cells. Cell Stem Cell.
3:182–195. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Savage J, Conley AJ, Blais A and Skerjanc
IS: SOX15 and SOX7 differentially regulate the myogenic program in
P19 cells. Stem Cells. 27:1231–1243. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Wang C, Guo Y, Wang J and Min Z: The
suppressive role of SOX7 in hepatocarcinogenesis. PLoS One.
9:e974332014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhang Y, Huang S, Dong W, Li L, Feng Y,
Pan L, Han Z, Wang X, Ren G, Su D, et al: SOX7, down-regulated in
colorectal cancer, induces apoptosis and inhibits proliferation of
colorectal cancer cells. Cancer Lett. 277:29–37. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Li B, Ge Z, Song S, Zhang S, Yan H, Huang
B and Zhang Y: Decreased expression of SOX7 is correlated with poor
prognosis in lung adenocarcinoma patients. Pathol Oncol Res.
18:1039–1045. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chan DW, Mak CS, Leung TH, Chan KK and
Ngan HY: Down-regulation of sox7 is associated with aberrant
activation of wnt/b-catenin signaling in endometrial cancer.
Oncotarget. 3:1546–1556. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Katoh M: Expression of human SOX7 in
normal tissues and tumors. Int J Mol Med. 9:363–368.
2002.PubMed/NCBI
|
|
18
|
Stovall DB, Wan M, Miller LD, Cao P,
Maglic D, Zhang Q, Stampfer MR, Liu W, Xu J and Sui G: The
regulation of SOX7 and its tumor suppressive role in breast cancer.
Am J Pathol. 183:1645–1653. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zhong WD, Qin GQ, Dai QS, Han ZD, Chen SM,
Ling XH, Fu X, Cai C, Chen JH, Chen XB, et al: SOXs in human
prostate cancer: Implication as progression and prognosis factors.
BMC Cancer. 12:2482012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Qi J, Wang J, Katayama H, Sen S and Liu
SM: Circulating microRNAs (cmiRNAs) as novel potential biomarkers
for hepatocellular carcinoma. Neoplasma. 60:135–142. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zhang Y, Jiang H, Qin M, Su X, Cao Z and
Wang J: TNIK serves as a novel biomarker associated with poor
prognosis in patients with pancreatic cancer. Tumour Biol.
37:1035–1040. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wong R and Frenette C: Updates in the
management of hepatocellular carcinoma. Gastroenterol Hepatol (N
Y). 7:16–24. 2011.PubMed/NCBI
|
|
23
|
Kormish JD, Sinner D and Zorn AM:
Interactions between SOX factors and Wnt/beta-catenin signaling in
development and disease. Dev Dyn. 239:56–68. 2010.PubMed/NCBI
|
|
24
|
Takash W, Cañizares J, Bonneaud N, Poulat
F, Mattéi MG, Jay P and Berta P: SOX7 transcription factor:
Sequence, chromosomal localisation, expression, transactivation and
interference with Wnt signalling. Nucleic Acids Res. 29:4274–4283.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Cui J, Xi H, Cai A, Bian S, Wei B and Chen
L: Decreased expression of Sox7 correlates with the upregulation of
the Wnt/β-catenin signaling pathway and the poor survival of
gastric cancer patients. Int J Mol Med. 34:197–204. 2014.PubMed/NCBI
|
|
26
|
Guo L, Zhong D, Lau S, Liu X, Dong XY, Sun
X, Yang VW, Vertino PM, Moreno CS, Varma V, et al: Sox7 is an
independent checkpoint for beta-catenin function in prostate and
colon epithelial cells. Mol Cancer Res. 6:1421–1430. 2008.
View Article : Google Scholar : PubMed/NCBI
|