Introduction
Chronic and non-healing wounds give rise to
significant morbidity and mortality, as well as considerable health
care expenditure. Devising a therapeutic approach in order to treat
extensive deep wounds remains a major clinical challenge (1). Due to the lack of effective
treatments, a combination of conventional managements such as
surgical debridement and skin grafting with skin substitutes in
combination with growth factors have been used to treat wounds. The
potential application of mesenchymal stem cells (MSCs) in
accelerating wound healing has been an active area of investigation
(2).
MSCs were first identified in bone marrow (3), but it has since been subsequently
demonstrated that MSCs are present in nearly all tissues (4). However, MSCs isolated from bone
marrow, adult organs and fetuses exhibit several disadvantages,
including invasive methods for isolation, low yield and a variety
of ethical issues. Stem cells from other sources such as embryonic
stem cells (ESCs) and induced pluripotent stem cells (iPSCs) also
have clinical concerns, including potential immunorejection and/or
tumorigenesis (5). Therefore,
there is the need to identify additional sources for the collection
of MSCs that do not have the above mentioned technical, ethical and
clinical concerns. The umbilical cord is regarded as a promising
source of MSCs. As perinatal stem cells, human umbilical
cord-derived mesenchymal stem cells (HUMSCs) have the potential for
self-renewal, extended proliferation and immunomodulatory
properties, making them excellent candidates for stem cell-based
therapy (6). HUMSCs also possess
characteristics of stem cells, such as multipotency and the ability
to differentiate into cells of multiple lineages, such as bone,
osteoblasts, chondroblast and adipocytes, under appropriate
differentiation conditions (7,8). As
HUMSCs are obtained from discarded umbilical cord tissue during
caesarean sections, there are fewer ethical issues involved
compared with ESCs. Compared with MSCs derived from adipose and
bone marrow, HUMSCs represent a source of more primitive stromal
cells that do not undergo spontaneous malignant transformation
(9). Together with their relative
ease of accessibility, cost-effectiveness, and efficacy, it is
predicted that HUMSCs will have increasing application in tissue
engineering and cellular-based therapies (10).
MSCs contribute to wound repair through several
mechanisms including: i) structural repair of wounds via
differentiation; ii) immunomodulation; iii) paracrine release of
growth factors that promote neovascularization and
re-epithelialization; and iv) mobilization of the resident stem
cell niche (11). Among these
mechanisms, it is widely believed that MSC paracrine signaling is
the predominant mechanism accounting for enhanced wound repair and
reduced scar formation (12–14).
However, paracrine activities are influenced by many factors,
including the local microenvironment and cell culture conditions.
Traditionally, HUMSCs are commonly cultured as 2-dimensional
monolayers on tissue culture plastic. This method is widely
regarded as poorly efficient, as evidenced by the poor survival of
HUMSCs engrafted at the site of injury. In addition, in
vivo, HUMSCs support the extracellular matrix. Therefore,
HUMSCs are integrated in a 3-dimensional manner in vivo once
grafted. Optimization of culture conditions for HUMSCs to achieve
successful engraftment remains an area of active research.
The present study mimicked the 3-dimensional in
vivo environment by culturing HUMSCs with platelet poor plasma
(PPP) gel combined with amnion (PPPA) to evaluate the influence of
a new carrier, PPPA, on the healing efficacy in treatment of
full-thickness excisional skin wounds in Sprague-Dawley rats. ELISA
was also performed to assess the expression of HUMSC growth factors
in a variety of experimental conditions and timings in
vitro. The aim of the present study was to evaluate the
potential of a novel carrier for HUMSCs in wound healing in
vivo.
Materials and methods
Umbilical cords and amnion
collection
Umbilical cords and amnion from four full-term
(38–40 weeks) healthy pregnancies (excluding HIV, hepatitis and
syphilis) through cesarean section were obtained from the
Department of Obstetrics and Gynecology, the Second Affiliated
Hospital of Shantou University Medical College (Shantou, China).
Informed consent and ethical permission were obtained before
parturition in accordance with the Ethics Committee of Shantou
University Medical College.
Isolation, culture and identification
of HUMSCs from human umbilical cords
Isolation, culture and identification of HUMSCs was
performed in the translational medicine center, as previously
described (15). Briefly, within
24 h after collection of umbilical cords from the operating room,
umbilical cords were flushed with phosphate buffered solution (PBS)
to remove blood cells. Umbilical cords containing two arteries and
a vein buried within the mucous connective tissue, known as the
Wharton's jelly, were sectioned into pieces (3–4 cm long) with a
sterile scalpel. After removing intact vessels, the remaining
Wharton's jelly was transferred to a sterile container containing
high glucose Dulbecco's modified Eagle's medium (H-DMEM; Gibco;
Thermo Fisher Scientific, Inc., Waltham, MA, USA) and then
dissected into smaller pieces. Thereafter, explants were plated on
100 mm cell culture dishes (JET BIOFIL) which were inverted in a
humidified atmosphere with 5% CO2 at 37°C for 15–30 min
until the explants adhered to the bottom of the dish. Fresh growth
medium [5 ml; H-DMEM supplemented with 10% fetal bovine serum, 100
mg/ml penicillin, 100 mg/ml streptomycin and 1 mg/ml amphotericin B
(all Gibco; Thermo Fisher Scientific, Inc.)] was then added to
cover the explants. Cell culture dishes were left undisturbed at
37°C in a humidified incubator at 5% CO2. The culture
medium was replenished every 2 days until sporadic fibroblast-like
cells grew from the tissue edge, usually after 5–7 days. Cells were
passaged when cultures reached 80–90% confluence. Third passage
cells were used in experiments. HUMSCs at passage 3 were
characterized using flow cytometry to examine the expression of
pluripotent cell markers as previously detailed (15).
Chloromethylbenzamido-1,1′-dioctadecyl-3,3,3′3′-tetrameth-ylindocarbocyanine
perchlorate (CM-DiI; lipophilic carbocyanine dye) labelling
(16)
CM-DiI is a lipophilic carbocyanine fluorescent dye,
which attaches to the cell membrane and has low cytotoxicity.
CM-DiI can be well preserved after fixation, permeabilization and
paraffin embedding of cells. Therefore, CM-Dil is been widely used
for immunofluorescence staining on tissue sections (17). HUMSCs at passage 3 were cultured in
complete growth medium under aforementioned conditions. Prior to
labeling, all HUMSCs were suspended at a density of
1×106/ml in serum-free DMEM and incubated with 4
µMCM-DiI (Molecular Probes; Thermo Fisher Scientific, Inc.) for 15
min at 37°C, followed by 10 min incubation at 4°C to optimize
staining levels. Cells were then precipitated at 250 × g for 5 min
at 37°C. Cell pellets were gently re-suspended in 37°C medium and
washed twice. The efficiency of CM-DiI labeling was checked by
immunofluorescence using fluorescence microscopy (Olympus BX51,
Olympus Corporation, Tokyo, Japan). Briefly, the cells seeded onto
coverslips and fixed in 4% paraformaldehyde for 30 min and then
washed with PBS three times. Cells were counterstained with
4′,6-diamidino-2-phenylindole (DAPI) for 5 min as a nuclear stain.
Positive cells were scored from four randomly selected fields per
specimen, and the efficiency of CM-DiI labeling was represented as
incorporation into the positive rate. Viability of CM-DiI labeled
HUMSCs was assessed by Trypan blue staining.
Preparation of acellular amnion
The preparation of acellular amnion was performed as
detailed previously (18).
Briefly, human amnion collected at cesarean section was washed with
PBS under sterile conditions and stored at −80°C in PBS containing
12% dimethyl sulfoxide. The amnion was frozen and thawed 3 times
and cut into pieces (2.5×2.5 cm), followed by the removal of
epithelial cells by incubation in 0.02% EDTA at 37°C for 2 h using
gentle scraping under a microscope. The spongy layer was also
removed. The complete removal of the epithelial cells was confirmed
by hematoxylin and eosin (H&E) staining.
Extraction of PPP
PPP was the residual material of platelet rich
plasma (PRP) therapy collected following cosmetic surgery
procedures on outpatients of the Second Affiliated Hospital,
Shantou University Medical College. Informed consent was obtained
from the patients who provided PPP before the collection procedure.
The specific extraction method was performed as previously
described (19). Blood samples
were centrifuged twice to obtain PPP and PRP. A 30 ml venous blood
sample was collected under aseptic conditions at room temperature,
and was aspirated with a 21 G needle into a 50 ml sterile
centrifuge tube preloaded with 6.5 ml anticoagulant citrate
dextrose solution. The blood sample was centrifuged for 15 min at
320 × g, at 4°C, resulting in the following three layers: An
inferior layer composed of red cells, an intermediate layer
composed of white cells, and a superior layer made up of plasma.
The 20 ml plasma layer was centrifuged for a further 5 min at 1,000
× g in order to obtain a two-part plasma sample: The upper part,
consisting of 18 ml PPP; and the lower part, consisting of 2 ml
PRP. The PPP was gently aspirated with a pipette and placed in a
sterile centrifuge tube, without being mixed with PRP. Allergic
reactions were not observed when administering PPP in these
experiments.
Preparation of PPPA and generation of
wound animal model
When passage 3 CM-DiI labeled HUMSCs reached 80%
confluence, HUMSCs were detached with trypsin solution, washed with
PBS (37°C) and precipitated. Cell pellets were re-suspended in PPP
at a density of 1×106/ml, and 1 ml PPP was transferred
to each well of a 12-well tissue culture plate (Corning
Incorporated, Corning, NY, USA), followed by addition of 10%
calcium gluconate at a volume ratio of 1:7. Preliminary experiments
revealed that this ratio was the most conducive to forming PPP gels
(data not shown). Plates were left undisturbed for 15 min at 37°C
in a humidified incubator with 5% CO2 to allow PPP gel
formation. Following gel formation, fresh growth medium was added
to cover the gel to maintain HUMSC growth. Gels containing HUMSCs
were used in wound healing in animals the following day. Blank gels
were made in the same way, without the inclusion of HUMSCs, and
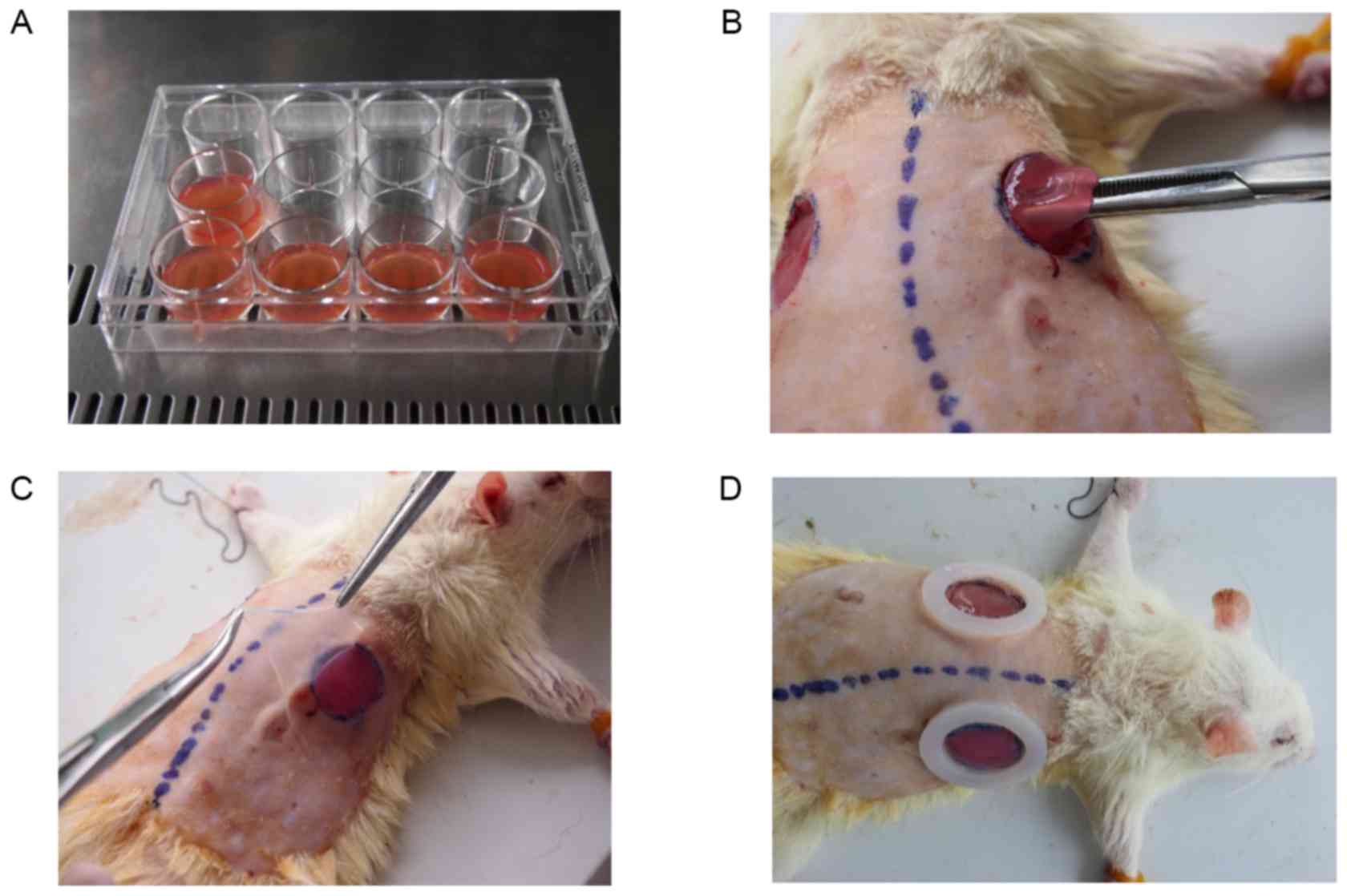
were used as a control. At the time of surgery, all gels were
detached from the 12-well plates with forceps (Fig. 1A).
As HUMSCs possess immunosuppressive properties,
Sprague-Dawley (SD) rats were used rather than severe immune
deficient mice. SD rats (age, 16 weeks; weight, 240–260g; n=36)
were purchased from Shantou University Medical College Laboratory
Animal Center (SUMC; Shantou, China) and maintained under specific
pathogen free conditions in the Laboratory Animal Center of SUMC.
All animals were allowed to acclimate for 1 week in the facility
before experiments were performed. Animal protocols were approved
by the Institutional Animal Care and Use Committee at SUMC.
SD rats were randomly assigned into four groups (n=9
rats/group): Group 1, grafted with PPPA+HUMSCs (PPPA+cells; PPPAC);
group 2, grafted with PPPA (PPPA); group 3, injected with HUMSCs
(Injection); and group 4, injected with PBS as blank control
(Blank). An excisional wound splinting mouse model was generated as
previously described (20) with
slight modifications. In brief, after hair removal from the dorsal
surface under anesthesia (10% chloral hydrate solution; 0.1 ml/20g;
Sigma-Aldrich; Merck KGaA, Darmstadt, Germany), two 14 mm (area
1.5386 cm2) full thickness excisional skin wounds were
created on each side of the midline. A donut-shaped silicone splint
was placed so that the wound was centered within the splint, which
was fixed to the skin by an immediate-bonding adhesive. Interrupted
sutures were utilized to stabilize its position. The same shaped
hoops were attached to the silicone splint to prevent rats from
gnawing it. Acellular amnion was placed over the wounds. After the
surgical procedure, the animals were housed individually. Our
preliminary studies suggested that the adhesive on the skin in rats
prior to the experiment did not cause any skin irritation or
allergic reaction. Each wound in the PPPAC group was grafted with
PPP gel with 1×06 CM-DiI labeled HUMSCs (Fig. 1B-D). In the PPPA group, the same
procedure was employed for the PPPAC group, except for the use of
the blank gels. Each wound in the Injection Group received 1,000 µl
HUMSC suspension containing 1×106 CM-DiI-labeled HUMSCs,
among which 800 µl was used for subcutaneous injection around the
wound and 200 µl for topical application on the wound bed. Blank
Group animals were injected with PBS as a blank control.
Wound healing assessment
Following surgery, wound dressings were changed
every day and the behavioral activity and wound healing progression
of the SD rats was monitored. On days 0, 2, 4, 6, 8, 10, 12 and 14
post-surgery, the open wounds on both sides of midline of each
animal from the four groups were imaged and wound healing was
assessed by comparison of images captured at different time points
with the initial images using an image analyzer (Image Pro Plus 6,
Media Cybernetics, Inc., Rockville, MD, USA). The healing index
included re-epithelialization and contraction. The healing rate was
calculated as (area of original wound-area of left exposing
wound)/area of original wound ×100%.
In addition, 2 SD rats randomly selected from each
group were sacrificed at 3, 7 or 14 days, and the skin samples
containing the wound and 3 mm of the surrounding skin were
harvested (21), fixed in 10%
buffered formalin and embedded in paraffin. H&E staining was
performed on 3-µm thick tissue sections.
Determination of the HUMSC
distribution in the wound
Sequential slides were used for detecting the
distribution of CM-DiI- labeled HUMSCs by immunofluorescence.
Briefly, the sections were rehydrated and the antigens were
retrieved via microwaving in 10 mM sodium citrate (pH 6.0) for 10
min, followed by counterstaining with DAPI. Following this, slides
were washed 3 times with PBS, covered with anti-fade solution, and
positive cells were scored on the wound region under fluorescence
microscopy to evaluate the distribution of HUMSCs.
Determination of expression levels of
growth factors in HUMSCs in PPPA
The same procedure described above was used to
generate PPPA. In the experimental group (PPPAC group), passage 3
PPPA HUMSCs (a total of 1×106 CM-DiI labeled HUMSCs in 1
ml PPP) grown in a 12-well plate, were cultured in vitro,
and the supernatant of each well in experimental group was
collected on days 1, 3, 7 and 14. In the control group (PPPA
group), PPPA without HUMSCs formed in a 12-well plate were cultured
in vitro, and the supernatant was collected on day 1 as an
initial reference. A monolayer group (a total of 1×106
CM-DiI labeled HUMSCs in 2D culture conditions in 1 well of a
12-well plate) were used as a 2D reference (2D group). The culture
medium was changed 24 h prior to supernatant collection, and the
expression levels of growth factors including insulin-like growth
factor (IGF-1), hepatocyte growth factor (HGF), transformation
growth factor (TGF)-β1, vascular endothelial growth factor (VEGF)
and keratinocyte growth factor (KGF) in the collected supernatant
was detected using ELISA kits (Human VEGF Quantikine ELISA kit;
cat. no. SVE00; Human HGF Quantikine ELISA kit; cat. no. SHG00;
Human KGF Quantikine ELISA kit; cat. no. DKG00; Human TGF-β1
Quantikine ELISA kit; cat. no. SB100B; and Human IGF-1 Quantikine
ELISA kit; cat. no. SG100) from R&D Systems, Inc. (Minneapolis,
MN, USA) according to the manufacturer's protocol. The data were
compiled from three independent assays per sample with each
performed in duplicate.
Statistical analysis
Data were analyzed using SPSS version 20.0 (IBM
Corp., Armonk, NY, USA) and are presented as the mean ± standard
deviation. Student's paired t-test was performed for comparison of
data of paired samples. One-way analysis of variance was used for
multiple group comparisons followed by the least significant
differences t-test. P<0.05 was considered to indicate a
statistically significant difference.
Results
Isolation of HUMSCs from human
umbilical cords
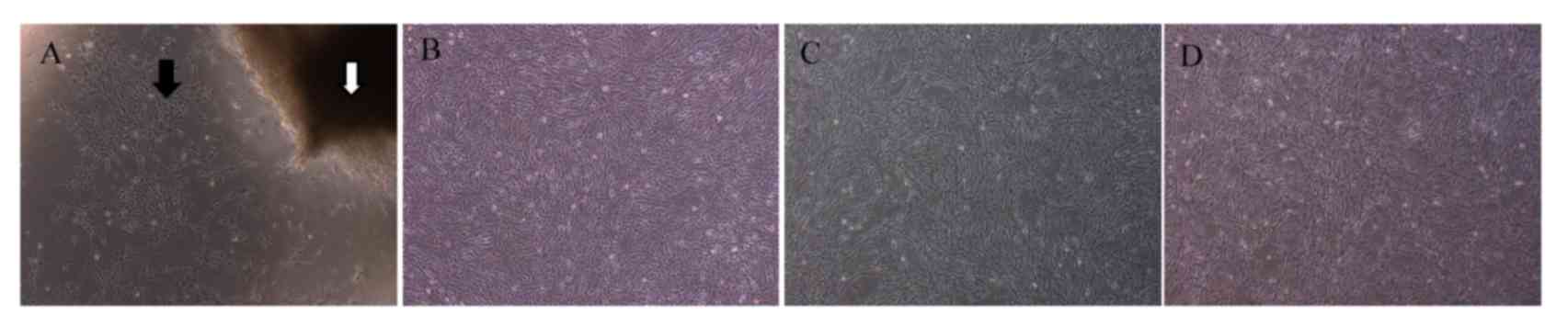
Fig. 2 presents the
primary culture of isolated HUMSCs. At day 5–7 in culture,
spindle-shape cells (Fig. 2A,
black arrow) began to migrate out from Wharton's jelly fragments
(Fig. 2A, white arrow). Half of
the volume of culture medium was replaced with new fresh medium
every 3–4 days until cells completely covered the culture area,
which was reached by ~day 10–14. HUMSCs exhibited fibroblast-like
morphology, with most demonstrating a flat, wide and polygonal
appearance after passaging. The above-mentioned morphology did not
alter significantly up to passage 9 (Fig. 2B-D). Cells at passage 3 expressed
cluster of differentiation (CD)29, CD59 and CD44, but not CD34 and
human leukocyte antigen D related (data not shown), and were used
in the subsequent experiments.
CM-DiI efficiently labels isolated
HUMSCs
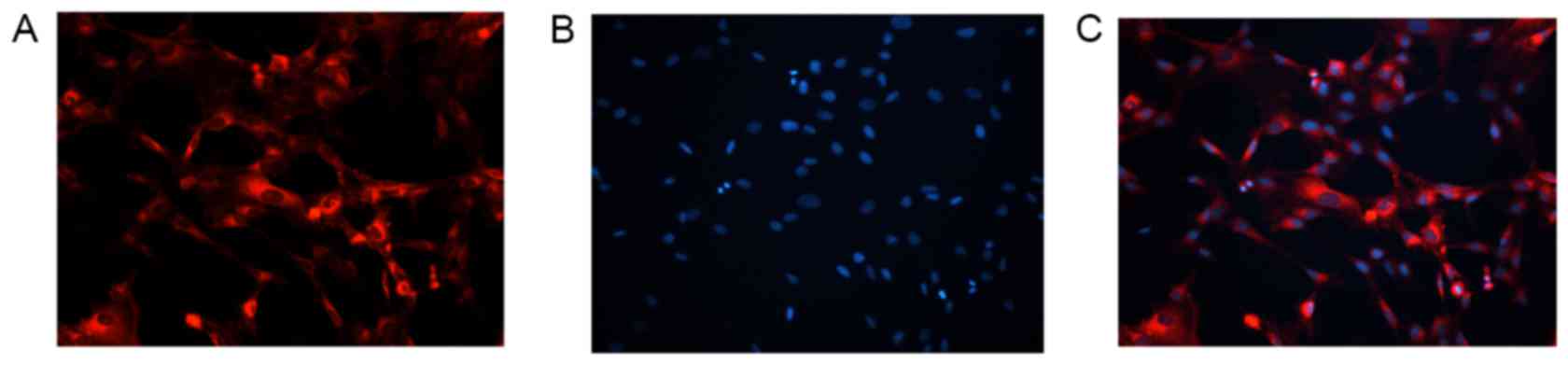
CM-DiI labeled 98.4% HUMSCs isolated from human
umbilical cord as determined by immunofluorescence (Fig. 3), while only <5% CM-DiI-positive
HUMSCs were trypan blue positive (17) (data not shown). Further culture
revealed that CM-DiI labeling, present in the cytoplasm and not the
nucleus, did not significantly affect the proliferation of HUMSCs
(data not shown). CM-DiI-labeled fluorescence was clearly visible
at 14 day after culture.
PPPA improves HUMSC-mediated wound
healing in rats with full thickness excisional skin wounds
In the animal wound model used in this study, it was
demonstrated that PPPA significantly enhanced HUMSC-mediated wound
healing in SD rats (Table I). From
day 4 post-surgery, the healing rate of the PPPAC group was
significantly higher compared with the other three experimental
groups (Table I; P<0.05 and
P<0.01). However, at days 2, 6, 8 and 14, the difference in the
healing rate between the PPPA group and the Injection group was not
statistically significant (Table
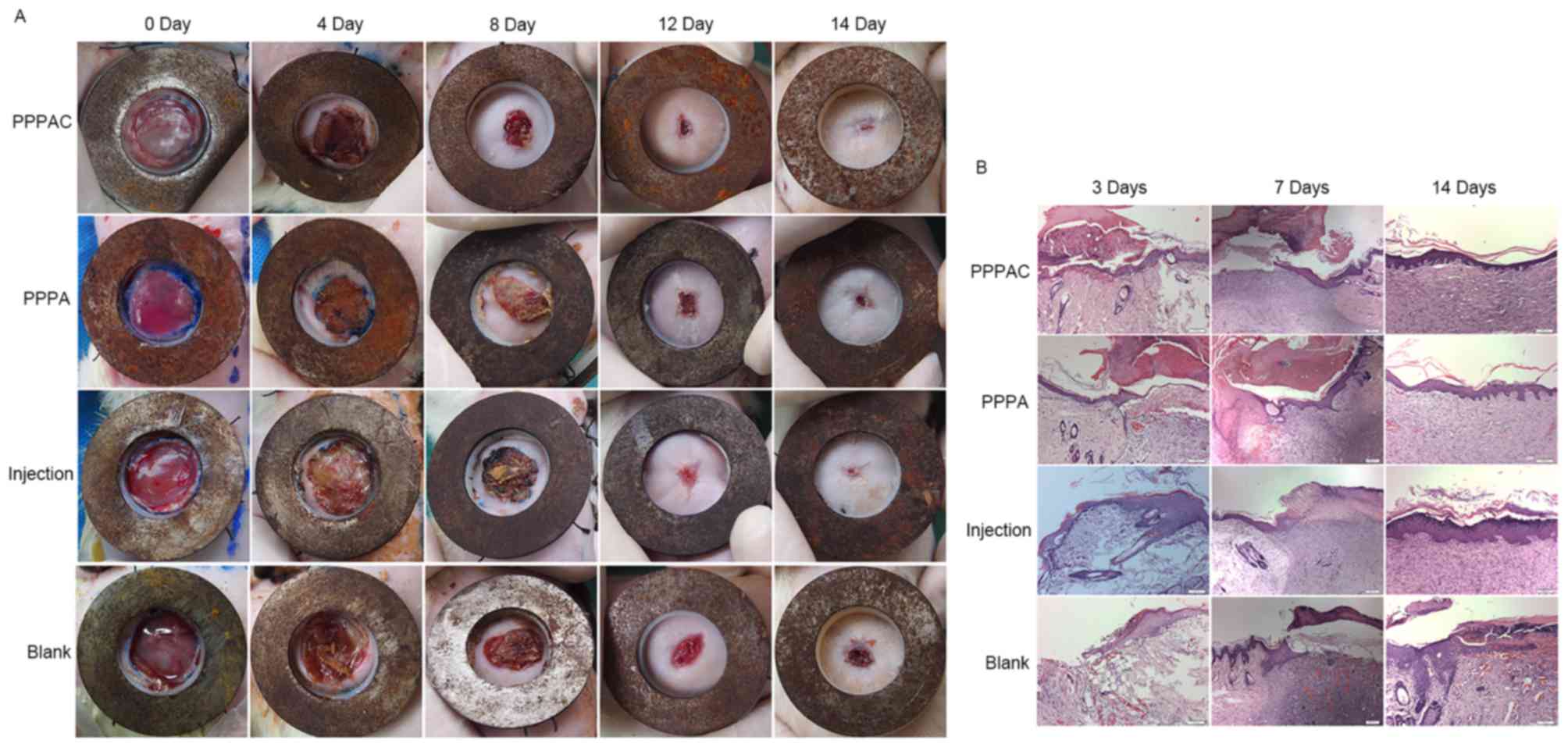
I). Wound contraction was markedly reduced in the PPPAC and
PPPA groups compared with the injection and blank groups (Fig. 4A). Furthermore, the thickness of
the newly formed epidermis layer of the PPPAC group grew faster to
cover the wounded skin tissue compared with the other groups either
on the 7th or the 14th day, as examined by histology. In addition,
the dermal papillae and the amount of CM-DiI-labeled HUMSCs in the
regenerated skin tissue were significantly increased in the PPPAC
group. The alignment of fibers in the healing skin tissue appeared
more regular in the PPPAC group than the other groups (Fig. 4B). Therefore, it was concluded that
the PPPAC group demonstrates superior wound healing compared with
the other three groups.
 | Table I.Wound healing rate of Sprague-Dawley
rats (n=9/group). |
Table I.
Wound healing rate of Sprague-Dawley
rats (n=9/group).
| Wound healing rate
(%) |
|---|
|
|---|
| Group | Day 2 | Day 4 | Day 6 | Day 8 | Day 10 | Day 12 | Day 14 |
|---|
| Blank |
9.01±2.17 |
17.15±2.84 |
26.14±3.75 |
45.52±4.02 |
64.26±4.41 |
83.27±2.99 |
90.10±2.86 |
| Injection |
9.73±2.45 |
19.06±2.98 |
32.48±4.89 |
55.68±7.61 |
73.55±4.86 |
86.05±3.68 |
94.67±2.63 |
| PPPA |
11.46±1.86a |
22.81±2.92b.c |
36.50±4.68b |
57.53±3.15b |
80.12±3.83b,c |
91.50±2.09b,c |
96.53±1.41b |
| PPPAC |
11.11±3.06 |
25.45±4.69b–d |
46.35±6.51b–d |
65.02±6.12b–d |
85.10±3.56b–d |
95.50±2.10b–d |
99.51±0.69b–d |
Distribution of CM-DiI-labeled HUMSCs
in the newly formed healing skin tissue
Next, the present study determined the distribution
of CM-DiI labeled HUMSCs in the wounded area of skin of rats from
the different experimental groups. Immunofluorescence was observed
in the basal layer of epidermis, dermis, spinous layer and
superficial fascia in newly regenerated skin tissue in the PPPAC
and Injection groups (Fig. 5 and
data not shown). Fluorescent-positive cells were polygonal or
spherical in shape and were located in the newly regenerated skin
tissue or in the nearby healthy skin tissue. The distribution of
HUMSCs in PPPAC group was more homogeneous compared with that in
PPPA group. Taken together, these results indicated that the PPPAC
group demonstrates a better survival rate of HUMSCs after
engrafting.
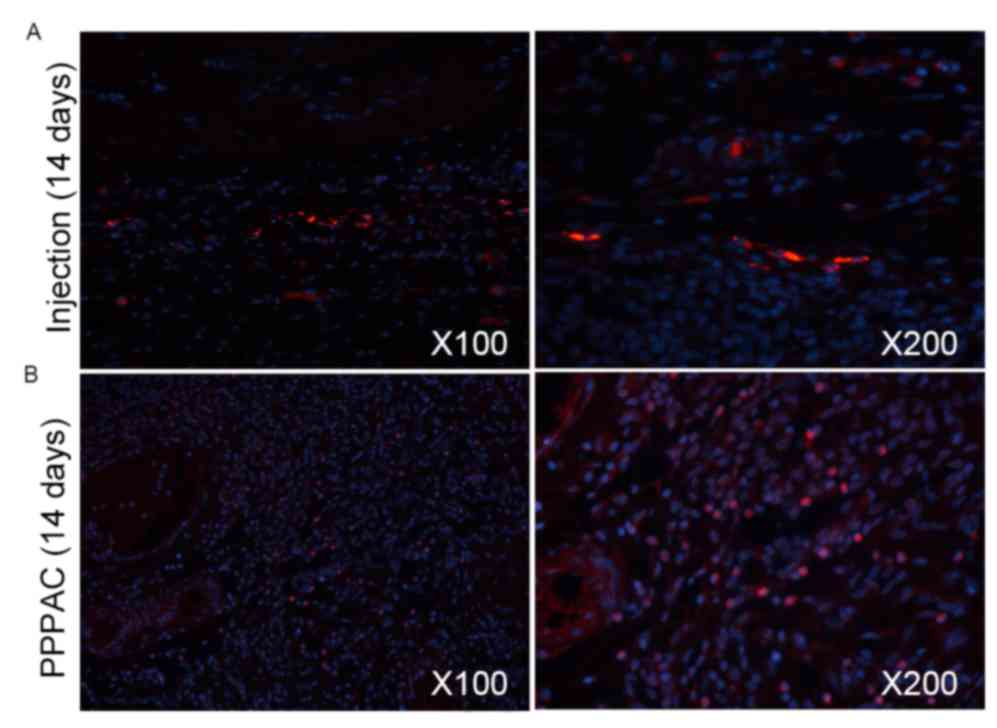 | Figure 5.Examination of distribution of
CM-DiI-labeled HUMSCs in the healed wound. At days 7 and 14, a
biopsy was performed to obtain the healed wound tissues, which were
fixed and sectioned, followed by immunofluorescence examination for
distribution of CM-DiI-labeled HUMSCs. Red fluorescence indicates
positive cells, blue fluorescence is nuclear staining with
4′,6-diamidino-2-phenylindole. The positive cells were emitting red
fluorescence as indicated in the images. Representative images at
day 14 from the (A) Injection and (B) PPPA groups. CM-DiI,
chloromethylbenzamido-1,1′-dioctadecyl-3,3,3′3′-tetramethylindocarbocyanine
perchlorate; HUMSCs, human umbilical cord-derived mesenchymal stem
cells; PPPA, platelet poor plasma gel combined with amnion. |
Increased levels of HUMSC-secreted
growth factors at different time points in the PPPAC group
ELISAs were subsequently performed to evaluate the
protein expression levels of secreted growth factors (including
HGF, TGF-β1, VEGF, IGF-1 and KGF) in HUMSCs at different culture
stages and times in the PPPA group (Fig. 6). As PPPA contained certain
baseline levels of growth factors, the culture medium was collected
at day 1 from the PPPA group as an initial reference value. The
findings suggested that the secretion levels of HGF, TGF-β1, VEGF,
IGF-1 and KGF released by HUMSCs in the PPPAC group were
significantly increased compared with those from the 2D group.
Therefore, it was concluded that PPPAC promotes the release of
growth factors from HUMSCs after engrafting into the wounded area
of skin.
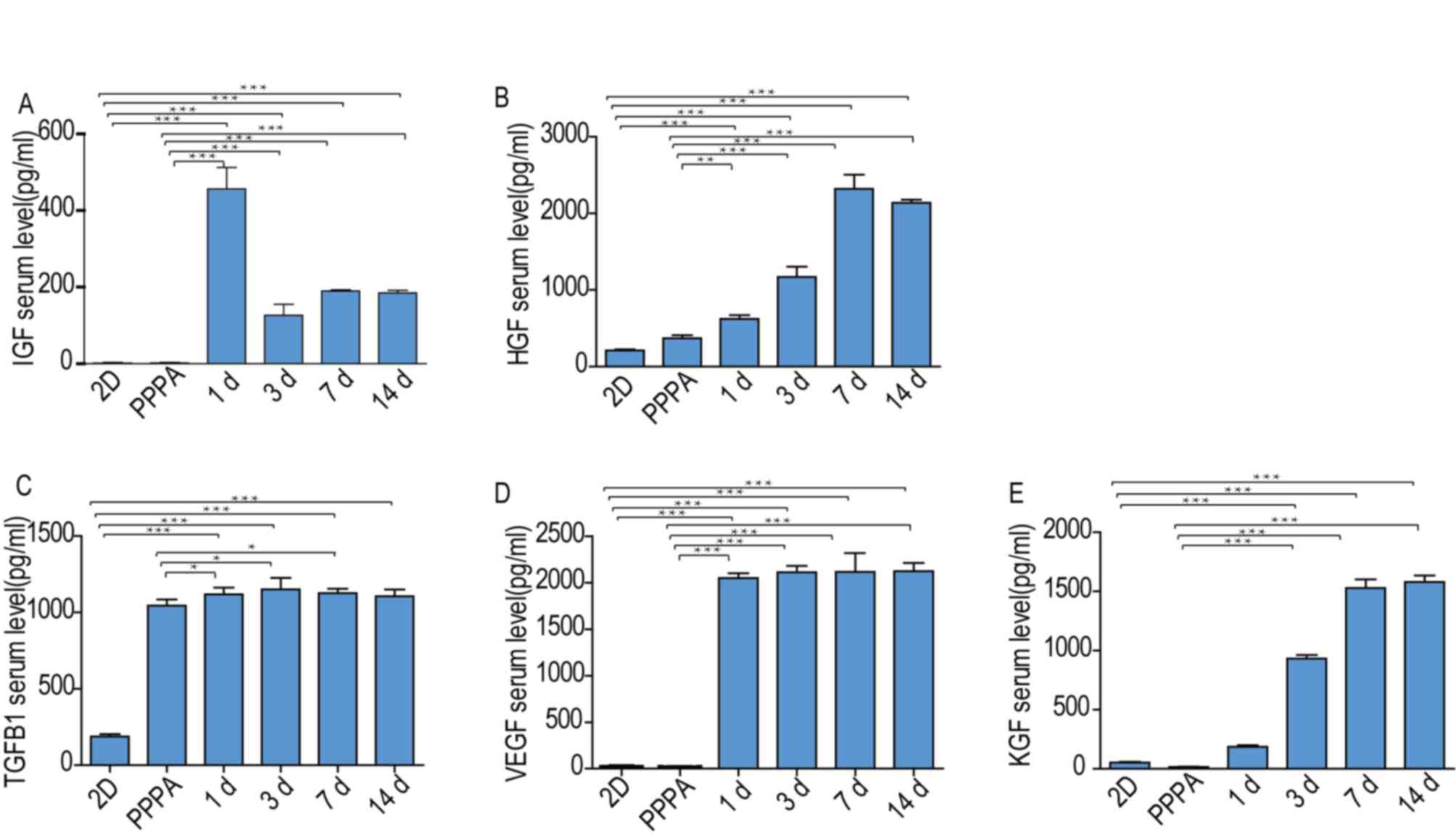 | Figure 6.Measurement of levels of growth
factors released by human umbilical cord-derived mesenchymal stem
cells at different time points. (A) IGF-1, (B) HGF, (C) TGF-β1, (D)
VEGF and (E) KGF serum levels were measured at days 1, 3, 7 and 14
following gel formation. The culture medium in the PPPA group was
collected at day 1 as an initial reference. The culture medium from
the 2D group (monolayers group) was collected as the 2D reference.
*P<0.05, **P<0.01, ***P<0.001. IGF-1, including
insulin-like growth factor; HGF, hepatocyte growth factor; TGF-β1,
transformation growth factor-β1; VEGF, vascular endothelial growth
factor; KGF, keratinocyte growth factor; PPPA, platelet poor plasma
gel combined with amnion. |
Discussion
Previously, several studies have isolated MSCs from
umbilical cord blood (22–24). However, Secco et al
(25) reported that more MSCs were
present in the cord itself than in the blood, and that different
experimental conditions used to isolate/culture MSCs accounted for
the differences in experimental outcomes and efficacy of MSCs. The
present study followed a previously published protocol and isolated
and cultured stem cells from human umbilical cord Wharton's jelly
(26), and successfully purified
HUMSCs from five samples. HUMSCs were isolated and characterized,
and it was demonstrated that i) isolated HUMSCs highly express
CD29, CD44 and CD59, and ii) isolated HUMSCs are able to
differentiate into multiple cell types including adipocytes and
osteoblasts under appropriate conditions, as previously reported
(27,28). Furthermore, the HUMSCs displayed
fibroblast-like morphology, and most were flat, wide and polygonal
following passaging. These properties did not alter significantly
up to passage 9. Therefore, a sufficient number of cells were
obtained to perform experiments.
Compared with stem cells from other sources such as
ESCs, HUMSCs may prove a more suitable choice for clinical
applications with respect to ethical and practical issues. Clinical
trials have used MSCs to treat human diseases, including
Parkinson's disease and myocardial infarction (29). However, their use regarding their
application in wound healing remains unknown. Several barriers to
their clinical use exist, including poor integration of MSCs
grafted into the wound. One of the primary mechanisms by which MSCs
exert their therapeutic effects is through paracrine activity,
which is affected by many factors including local microenvironment,
inflammatory cytokines and cell phenotypes. A growing body of
evidence suggests that when differentiated cells reach confluence,
they cease to proliferate due to contact inhibition. These
contact-inhibited cells exhibit lower protein synthesis and
metabolic rate (30,31). In previous studies, MSCs were
expanded on tissue culture plastic as monolayers in vitro,
and lost their cell-specific properties with several rounds of
passages and prolonged cultured time in vitro (32). In contrast, MSCs developed in 3D
conditions using AggreWell expressed genes associated with
angiogenesis and wound healing, and exhibited better multipotent
differentiation capacity in vitro (33).
The findings of the present study suggested that
HUMSCs cultured in PPPAC upregulated the secretion of paracrine
molecules such as HGF, TGF-β1, VEGF, IGF-1 and KGF,
involved in cellular proliferation and wound re-epithelialization,
compared to the monolayer culture of HUMSCs. These findings were in
line with those previously reported for MSCs cultured in 3D
conditions using AggreWell (5).
In recent years, PRP has been widely used in plastic
surgery (34,35). Although during the extraction
process, centrifuge parameters were adjusted to obtain better PRP,
the amount of discarded PPP remained large (36). Therefore, PPP was selected as the
cell carrier and scaffold material due to easy acquisition. In
future clinical applications, PPP is able to be obtained from the
blood of the patient, autologous material without immunogenicity,
and is available in sufficient quantities. PPP has been
demonstrated to contain a large amount of fibrinogen, and PPP
solidification occurs after calcium gluconate is added. In this
coagulation process, fibrinogen is converted into fibrin (37), which forms a mesh structure inside
the PPP gel and provides3D culture conditions for HUMSCs and
promotes wound scabbing. These conditions improved the efficiency
of HUMSCs in grafting, increasing HUMSC adhesion (38) and delivering better functional
interactions between HUMSCs (39).
The PPP gel in the present experiment was a colloidal semi-solid
gel, easy desiccate and easy to infect. Therefore, this was
combined with amnion (PPPA), using acellular amnion to seal the gel
and wound. Amnion is a tissue of interest as a biological dressing
due to its biological properties and immunologic characteristics
(40). This PPPA combination is
easy to make with moderate costs, easily adheres to wounds and can
effectively close wounds in the early trauma period, thus reducing
the bacterial infection. In the present study, 14 days after
surgery, the wound healing rate of the PPPAC group was
significantly higher than the other experimental groups. In
addition, it was demonstrated that wound contraction in the PPPAC
group was inhibited more efficiently than other groups.
Furthermore, using immunofluorescence, CM-DiI labeled HUMSCs were
identified to be scattered throughout the basal layer of the
epidermis, dermis, spinous layer, superficial fascia and connective
tissue around the wound. At particular time points examined, it was
observed that the amount of CM-DiI-labeled HUMSCs in the PPPAC
group was much higher than that of the other three experimental
groups. Taken together, these findings demonstrated that the PPPAC
group has the highest grafting survival rate and healing capacity
among all groups examined.
Skin wound repair is an intricate and highly
coordinated process that generally can be divided into three
overlapping but distinct phases: The vascular and inflammatory
phase, the granulation tissue formation, re-epithelialization and
proliferative phase, and the remodeling phase (41). Interruption of one or more phases
of this process can result in chronic wound healing, fibrosis or
scarring. Due to the lack of epidermal basal and dermal layers, it
is difficult to rebuild normal structures in full-thickness
excisional skin wounds. In H&E sections at day 3 following
grafting, wounds in each group seeped out obviously with
infiltration with neutrophils, macrophages and other inflammatory
cells, and the remaining epidermal stem cells migrated from the
wound edges to the wound center. In the Injection and Blank groups,
due to the deficiency of dermal layer and subcutaneous tissue,
sufficient granulation did not occur; therefore, epidermal stem
cells were unable to migrate to cover the surface of the wound.
Cells accumulated and proliferated at the margin surrounding the
wound, as examined at days 7 and 14 after grafting.
Re-epithelialization rates in these two groups were much slower
than that of the PPPAC group. In contrast, in the PPPAC and PPPA
groups, inflammation was mild and epidermal stem cells migrated a
longer distance. It was also demonstrated that the application of
PPPAC facilitated the formation of the epidermis layer in the
repairing skin tissue with thickness similar to the surrounding
normal skin, increasing the amount of dermal ridges, and increasing
the alignment of fibers to a more regular morphology. These
observations suggested that the administration of PPPAC was not
only able to accelerate the speed of wound healing, but also
improved the quality of the wound healing.
To further understand the molecular basis underlying
the increased rate of wound healing achieved by PPPAC, the levels
of growth factors in the culture mediums of these 3D and 2D culture
conditions were measured and compared, and the secretion levels of
HGF, TGF-β1, VEGF, IGF-1 and KGF released by HUMSCs in
the PPPAC group were significantly higher in 3D culture conditions
compared with those in the 2D group. As these cytokines were
involved in re-epithelialization, neovascularization and remodeling
of wound healing, it was hypothesized that increased secretion of
these cytokines may serve a role in facilitating wound healing
achieved by PPPAC.
In conclusion, the present study demonstrated that
PPPA modifies the paracrine activities of HUMSCs, provides a
relatively stable grafting environment and improves the efficiency
of HUMSC in wound healing in the animal model used in this study.
Further studies are required to investigate the specific mechanisms
by which PPPAC promotes wound healing, demonstrating its potential
utility for clinical therapeutic applications in skin grafts and
wound healing.
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (grant no. 81272116) and the
Scientific Research Foundation for the Returned Overseas Chinese
Scholars, Ministry of Education of China (grant no. [2013]
693).
References
|
1
|
Atiyeh BS, Gunn SW and Hayek SN: State of
the art in burn treatment. World J Surg. 29:131–148. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hocking AM and Gibran NS: Mesenchymal stem
cells: Paracrine signaling and differentiation during cutaneous
wound repair. Exp Cell Res. 316:2213–2219. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Prockop DJ: Marrow stromal cells as stem
cells for nonhematopoietic tissues. Science. 276:71–74. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
da Silva Meirelles L, Chagastelles PC and
Nardi NB: Mesenchymal stem cells reside in virtually all post-natal
organs and tissues. J Cell Sci. 119:2204–2213. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bongso A and Fong CY: The therapeutic
potential, challenges and future clinical directions of stem cells
from the Wharton's jelly of the human umbilical cord. Stem Cell
Rev. 9:226–240. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jadalannagari S and Aljitawi OS:
Ectodermal Differentiation of wharton's jelly mesenchymal stem
cells for tissue engineering and regenerative medicine
applications. Tissue Eng Part B Rev. 21:314–322. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhao G, Liu F, Lan S, Li P, Wang L, Kou J,
Qi X, Fan R, Hao D, Wu C, et al: Large-scale expansion of Wharton's
jelly-derived mesenchymal stem cells on gelatin microbeads, with
retention of self-renewal and multipotency characteristics and the
capacity for enhancing skin wound healing. Stem Cell Res Ther.
6:382015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Horwitz EM, Le Blanc K, Dominici M,
Mueller I, Slaper-Cortenbach I, Marini FC, Deans RJ, Krause DS,
Keating A, et al: International Society for Cellular Therapy:
Clarification of the nomenclature for MSC: The International
Society for Cellular Therapy position statement. Cytotherapy.
7:393–395. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tang Q, Chen Q, Lai X, Liu S, Chen Y,
Zheng Z, Xie Q, Maldonado M, Cai Z, Qin S, et al: Malignant
transformation potentials of human umbilical cord mesenchymal stem
cells both spontaneously and via 3-methycholanthrene induction.
PLoS One. 8:e818442013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hanson SE, Bentz ML and Hematti P:
Mesenchymal stem cell therapy for nonhealing cutaneous wounds.
Plast Reconstr Surg. 125:510–516. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Balaji S, Keswani SG and Crombleholme TM:
The role of mesenchymal stem cells in the regenerative wound
healing phenotype. Adv Wound Care (New Rochelle). 1:159–165. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Sasaki M, Abe R, Fujita Y, Ando S, Inokuma
D and Shimizu H: Mesenchymal stem cells are recruited into wounded
skin and contribute to wound repair by transdifferentiation into
multiple skin cell type. J Immunol. 180:2581–2587. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Khosrotehrani K: Mesenchymal stem cell
therapy in skin: Why and what for? Exp Dermatol. 22:307–310. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Arno AI, Amini-Nik S, Blit PH, Al-Shehab
M, Belo C, Herer E, Tien CH and Jeschke MG: Human Wharton's jelly
mesenchymal stem cells promote skin wound healing through paracrine
signaling. Stem Cell Res Ther. 5:282014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Huang P, Lin LM, Wu XY, Tang QL, Feng XY,
Lin GY, Lin X, Wang HW, Huang TH and Ma L: Differentiation of human
umbilical cord Wharton's jelly-derived mesenchymal stem cells into
germ-like cells in vitro. J Cell Biochem. 109:747–754.
2010.PubMed/NCBI
|
|
16
|
Weir C, Morel-Kopp MC, Gill A, Tinworth K,
Ladd L, Hunyor SN and Ward C: Mesenchymal stem cells: Isolation,
characterisation and in vivo fluorescent dye tracking. Heart Lung
Circ. 17:395–403. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hemmrich K, Meersch M, von Heimburg D and
Pallua N: Applicability of the dyes CFSE, CM-DiI and PKH26 for
tracking of human preadipocytes to evaluate adipose tissue
engineering. Cells Tissues Organs. 184:117–127. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yang L, Shirakata Y, Shudou M, Dai X,
Tokumaru S, Hirakawa S, Sayama K, Hamuro J and Hashimoto K: New
skin-equivalent model from de-epithelialized amnion membrane. Cell
Tissue Res. 326:69–77. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Woo SH, Kim JP, Park JJ, Chung PS, Lee SH
and Jeong HS: Autologous platelet-poor plasma gel for injection
laryngoplasty. Yonsei Med J. 54:1516–1523. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Chen L, Tredget EE, Wu PY and Wu Y:
Paracrine factors of mesenchymal stem cells recruit macrophages and
endothelial lineage cells and enhance wound healing. PLoS One.
3:e18862008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Galiano RD, Michaels J 5th, Dobryansky M,
Levine JP and Gurtner GC: Quantitative and reproducible murine
model of excisional wound healing. Wound Repair Regen. 12:485–492.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hussain I, Magd SA, Eremin O and El-Sheemy
M: New approach to isolate mesenchymal stem cell (MSC) from human
umbilical cord blood. Cell Biol Int. 36:595–600. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Park SE, Jung NY, Lee NK, Lee J, Hyung B,
Myeong SH, Kim HS, Suh YL, Lee JI, Cho KR, et al: Distribution of
human umbilical cord blood-derived mesenchymal stem cells
(hUCB-MSCs) in canines after intracerebroventricular injection.
Neurobiol Aging. 47:192–200. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ding Y, Yang H, Feng JB, Qiu Y, Li DS and
Zeng Y: Human umbilical cord-derived MSC culture: The replacement
of animal sera with human cord blood plasma. In Vitro Cell Dev Biol
Anim. 49:771–777. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Secco M, Zucconi E, Vieira NM, Fogaca LL,
Cerqueira A, Carvalho MD, Jazedje T, Okamoto OK, Muotri AR and Zatz
M: Multipotent stem cells from umbilical cord: Cord is richer than
blood! Stem Cells. 26:146–150. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ma L, Feng XY, Cui BL, Law F, Jiang XW,
Yang LY, Xie QD and Huang TH: Human umbilical cord Wharton's
Jelly-derived mesenchymal stem cells differentiation into
nerve-like cells. Chin Med J (Engl). 118:1987–1993. 2005.PubMed/NCBI
|
|
27
|
Karahuseyinoglu S, Cinar O, Kilic E, Kara
F, Akay GG, Demiralp DO, Tukun A, Uckan D and Can A: Biology of
stem cells in human umbilical cord stroma: In situ and in vitro
surveys. Stem Cells. 25:319–331. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
MacKenzie TC and Flake AW: Human
mesenchymal stem cells: Insights from a surrogate in vivo assay
system. Cells Tissues Organs. 171:90–95. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Song H, Song BW, Cha MJ, Choi IG and Hwang
KC: Modification of mesenchymal stem cells for cardiac
regeneration. Expert Opin Biol Ther. 10:309–319. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Leontieva OV, Demidenko ZN and
Blagosklonny MV: Contact inhibition and high cell density
deactivate the mammalian target of rapamycin pathway, thus
suppressing the senescence program. Proc Natl Acad Sci USA.
111:8832–8837. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Hayes CS, Koskiniemi S, Ruhe ZC, Poole SJ
and Low DA: Mechanisms and biological roles of contact-dependent
growth inhibition systems. Cold Spring Harb Perspect Med. 4:pii:
a010025. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Reiser J, Zhang XY, Hemenway CS, Mondal D,
Pradhan L and La Russa VF: Potential of mesenchymal stem cells in
gene therapy approaches for inherited and acquired diseases. Expert
Opin Biol Ther. 5:1571–1584. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Michel M, L'Heureux N, Pouliot R, Xu W,
Auger FA and Germain L: Characterization of a new tissue-engineered
human skin equivalent with hair. In Vitro Cell Dev Biol Anim.
35:318–326. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Nita AC, Orzan OA, Filipescu M and Jianu
D: Fat graft, laser CO2 and platelet-rich-plasma synergy
in scars treatment. J Med Life. 6:430–433. 2013.PubMed/NCBI
|
|
35
|
Kawazoe T and Kim HH: Tissue augmentation
by white blood cell-containing platelet-rich plasma. Cell
Transplant. 21:601–607. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Amable PR, Carias RB, Teixeira MV, da Cruz
Pacheco I, do Corrêa Amaral RJ, Granjeiro JM and Borojevic R:
Platelet-rich plasma preparation for regenerative medicine:
Optimization and quantification of cytokines and growth factors.
Stem Cell Res Ther. 4:672013. View
Article : Google Scholar : PubMed/NCBI
|
|
37
|
Diamond SL: Systems biology of
coagulation. J Thromb Haemost. 11:(Suppl 1). S224–S232. 2013.
View Article : Google Scholar
|
|
38
|
Sierra DH: Fibrin sealant adhesive
systems: A review of their chemistry, material properties and
clinical applications. J Biomater Appl. 7:309–352. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Malafaya PB, Silva GA and Reis RL:
Natural-origin polymers as carriers and scaffolds for biomolecules
and cell delivery in tissue engineering applications. Adv Drug
Deliv Rev. 59:207–233. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Insausti CL, Alcaraz A, García-Vizcaíno
EM, Mrowiec A, López-Martínez MC, Blanquer M, Piñero A, Majado MJ,
Moraleda JM, Castellanos G and Nicolás FJ: Amniotic membrane
induces epithelialization in massive posttraumatic wounds. Wound
Repair Regen. 18:368–377. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Gurtner GC, Werner S, Barrandon Y and
Longaker MT: Wound repair and regeneration. Nature. 453:314–321.
2008. View Article : Google Scholar : PubMed/NCBI
|