Introduction
Peripheral nerve injury is a common clinical
problem, and severe nerve injury has a devastating impact on the
quality of life of patients. Extraneural scarring and adhesion are
detrimental side effects of nerve injury, which can prevent axonal
regeneration and recovery of nerve function and can even cause
additional nerve damage (1).
Therefore, preventing extraneural scarring and adhesion is a key
research focus in the field of peripheral nerve injury recovery.
Previous studies on the structure and function of the nerve
regeneration chamber have suggested that therapeutic interventions
on the microenvironment of nerve regeneration may effectively
prevent scar and adhesion formation (1,2).
Hyaluronic acid (HA) gel is a type of natural and
transparent polysaccharide composed of straight-chain polymers,
which exists widely in the body as an important component of
extracellular matrix. Considering that HA does not exhibit species
or tissue specificity, and exogenous HA is biodegradable in
vivo, HA is often applied to the study of peripheral nerve
injury recovery as an ideal biomaterial. HA has been reported to
effectively reduce scar formation following neurolysis (2). Smit et al (3) revealed that HA gel significantly
reduces nerve adhesions following different types of peripheral
nerve damage. However, no further studies have investigated the
effect of HA on nerve regeneration.
Chitosan, a macromolecular polysaccharide and a type
of artificial extracellular matrix material, has attracted
increasing attention because of its availability and non-toxic
biodegradability in vivo. Rosales-Cortes et al
(4) reported that no obvious
immune rejection response was observed for chitosan in female dogs.
Chitosan has good biocompatibility, and it has been demonstrated to
support the growth of nerve cells and Schwann cells, to promote
axonal extension of nerve cells and to inhibit the growth of
fibroblasts (5,6). Patel et al (7), using a novel evaluation method for
function, reported that chitosan conduit not only benefits the
morphology recovery of regenerated nerves, but also promotes the
recovery of nerve function. Several studies have reported that
chitosan, as a vector combined with supplements, such as
brain-derived neurotropic factor and nerve growth factor, is
important in bridging peripheral nerve defects and in enhancing the
regeneration and functional recovery of peripheral nerves (8–11).
As previously reported, HA has inhibitory effects on
scarring and adhesion and promotive effects on regeneration of
injured nerves, while chitosan conduit enhances regeneration and
restoration of injured peripheral nerves. Study from our group has
demonstrated that chitosan conduit can prevent scarring, and
promote the functional recovery of facial nerve in early stages
(unpublished data). The purpose of the present study was to
evaluate the effect of topical administration of HA around chitosan
conduit on the formation of extraneural scarring, adhesion and
regeneration and functional recovery of injured peripheral nerves
using a rat sciatic nerve clamp injury model.
Materials and methods
Animals and surgical procedure
A total of 60 healthy adult Sprague-Dawley (SD) rats
weighing 180–220 g and maintained under controlled lighting and
temperature conditions were supplied by the Laboratory Animal
Centre of Chinese PLA General Hospital (Beijing, China) in this
experiment. All studies on rats were performed with approval from
the Institutional Animal Care and Use Committee (IACUC) of the
Laboratory Animal Centre of Chinese PLA General Hospital. Animals
were housed in steel cages at room temperature 22–26°C under a
12/12 h light/dark cycle and were fed with pelleted standard feed
and water. The 8-week-old rats (male or female) were randomly
allocated to four groups, with 15 animals in each group. They were
all anesthetized with 10% chloral hydrate (0.3 ml/100 g). Then, the
fur of the right hind limbs was shaved off. The rats were kept in
prone position. Following local povidone-iodine disinfection and
covering with a paper towel, an oblique incision (3 cm) was
performed on the right hind leg. The sciatic nerve was exposed
through the spatium intermusculare prior to clamping the nerve (1
cm) with needle holders (J32220; Shanghai Medical Instruments Ltd.,
Shanghai, China) for 30 sec. In the present study, an identical
needle clamp was used in all the animals, which, when fully closed,
it generates the same length nerve clamp (1 cm) and during the same
working time (30 sec) results in identical force injury in each
group. The chitosan conduits were longitudinally split prior to
immersing in physiological saline. The chitosan conduit was 1 mm
long, 1 mm wide and 0.05 mm thick.
The four experimental groups were as follows:
Chitosan group, the injury sites of sciatic nerves were covered
with chitosan conduits and 6-0 sutures were used to anchor the
conduits to the fascia around the nerves; chitosan/HA group, the
animals were treated with the chitosan conduits which were fixed as
described above, plus HA gel (0.2 ml; MW ~200 million Dalton;
Shanghai Medical Instruments Ltd. (Shanghai, China) which was
injected evenly onto the surface of the injury nerve and chitosan
conduits; control group, no additional treatment was performed
following clamping the nerve; and HA group, HA gel (0.2 ml) was
injected at the site of injury. Following the appropriate treatment
establishing the animal models, the incision was sutured with 6-0
sutures one layer simultaneously and appositionally. Finally, the
skin was closed with subcuticular suture.
Sciatic functional index (SFI)
At 4, 8 and 12 weeks following surgery, evaluation
of SFI was performed based on a method described previously
(12,13). Prior to the test, the rats were
trained to walk through the channel (length × width × height:
100×10×15 cm), from one end to the other. Following laying some
white papers on the bottom of the walking channel and painting of
hind paws of rats with ink, the rats walked through the channel
once again, and at least 5 paw-prints of every rat were recorded.
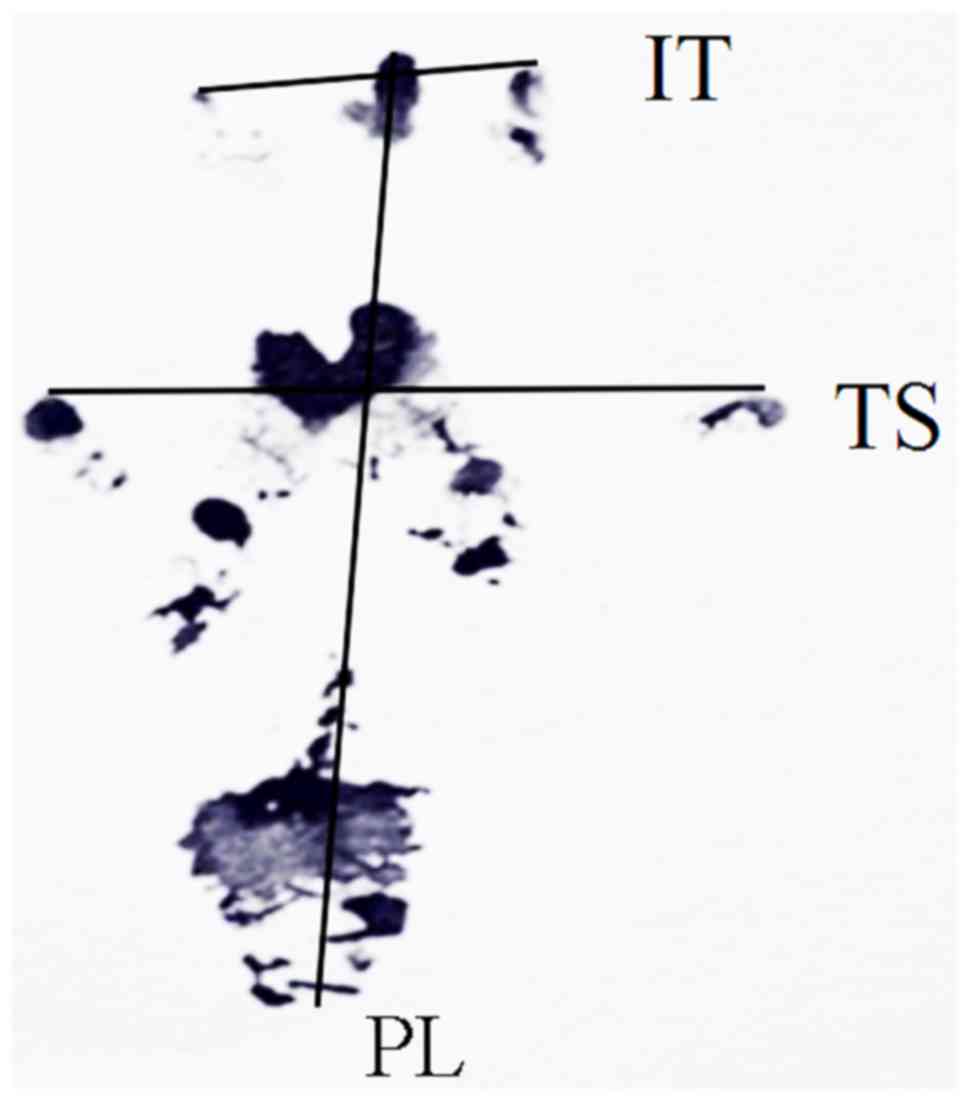
The paw-prints of every rat on the experimental operated side (E)
and the contralateral normal side (N) were measured. PL is the
length from the third toe to the heel, TS is the length from the
first to the fifth toe, and IT is the length from the second to the
fourth toe (Fig. 1). The SFI of
each rat was then calculated by the following equation: SFI = −38.3
[(EPL-NPL)/NPL] + 109.5 [(ETS-NTS)/NTS) + 13.3 [(EIT-NIT)/NIT] -
8.8.
In general, SFI equal to 0 represents normal nerve
function, whereas an SFI oscillating around-100 indicates total
dysfunction.
Scar adhesion analysis
After anesthetizing the rats with 10% chloral
hydrate at 4, 8, 12 weeks following surgery, the nerves sections
were exposed by incising the scar along the original incisions.
According to the classification standard by Petersen et al
(14), the force size of
separating the skin and muscles, fascia and nerves was graded: 1,
no need of or just in need of blunt dissection slightly; 2, need of
blunt separation using a lot of force; and 3, need of point-sharp
dissection.
Electrophysiological evaluation
At 12 weeks following surgery, all rats were
subjected to electrophysiological measurement. The sciatic nerve
sections clamped were re-exposed by surgical incision at the
previous surgical site under general anesthesia. The stimulating
electrodes were placed at the proximal and distal segments of the
sciatic nerve section of clamping, while the recording electrodes
were inserted into the gastrocnemius muscle. Then,
electrophysiological instrument was used to test and record
nerve-muscle action potential. The amplitude and latency period of
sciatic nerves was recorded for the rats in each group, the
distance between two electrodes was measured and the conduction
velocity of the nerves separately was calculated.
Histological staining
At 4, 8, 12 weeks following surgery, the conduits
and nerves of the anesthetized rats were exposed by incision of the
skin and excision of both. Each group had 15 rats, with 5 rats for
each time-point (4, 8 and 12 weeks), then tissues samples from each
rat were divided into four blocks on average: Two middle parts were
used in epoxy resin embedding [for toluidine blue staining and
transmission electron microscopy (TEM)] and paraffin embedding [for
hematoxylin and eosin (H&E) staining and Masson staining]. The
epoxy resin-embedded samples were first fixed in glutaraldehyde
(2.5%; 24 h at 4°C) and osmium (2%; 2 h at 4°C) and dehydrated
through a gradient of propyl alcohol. Toluidine blue staining and
TEM investigations for each specimen were performed as described
below. The paraffin-embedded samples were first fixed in 4%
formaldehyde solution for 8 h at room temperature prior to 4 µm
sectioning for H&E staining and Masson staining.
Masson's trichrome stain was performed as previously
described (15), and the resulting
images were used for semi-quantitative analysis. Extraneural scars
are composed primarily of collagen fibers. In the present research,
the average thickness of collagen in the epineurium was determined
in four random optical fields from 1 randomly selected section of
each rat, using Image-Pro 6.0 Plus software (Media Cybernetics,
Inc., Rockville, MD, USA).
Toluidine blue staining
The experimental samples were embedded in Epon resin
prior to 1.5 µm sectioning. Then, the sections were treated with
toluidine blue stain to label the myelin sheath. The mean number of
myelinated axons was calculated in six randomly selected fields
from 1 randomly selected section of each rat using Image-Pro 6.0
Plus software following observation using a light microscope.
TEM
The experimental samples were embedded in Epon resin
prior to 70 nm ultrathin sections, saturated in uranyl acetate for
30 min at room temperature and stained with citric acid for 15 min
at room temperature. The myelin sheath morphology, the cellular
construction and the regeneration situation of cell organelles was
evaluated in six randomly selected fields from 1 randomly selected
section of each rat, observed using a transmission electron
microscope (JEM-2000ex; JEOL, Ltd., Tokyo, Japan). The average
diameter of myelinated fibers and myelin sheath thickness was
calculated using Image-Pro 6.0 Plus.
Statistical analysis
Statistical analysis was performed using SPSS 19.0
(IBM Corp., Armonk, NY, USA). The data were presented as the mean ±
standard deviation. One-way analysis of variance was used to
compare differences among groups. P<0.05 was considered to
indicate a statistically significant difference.
Results
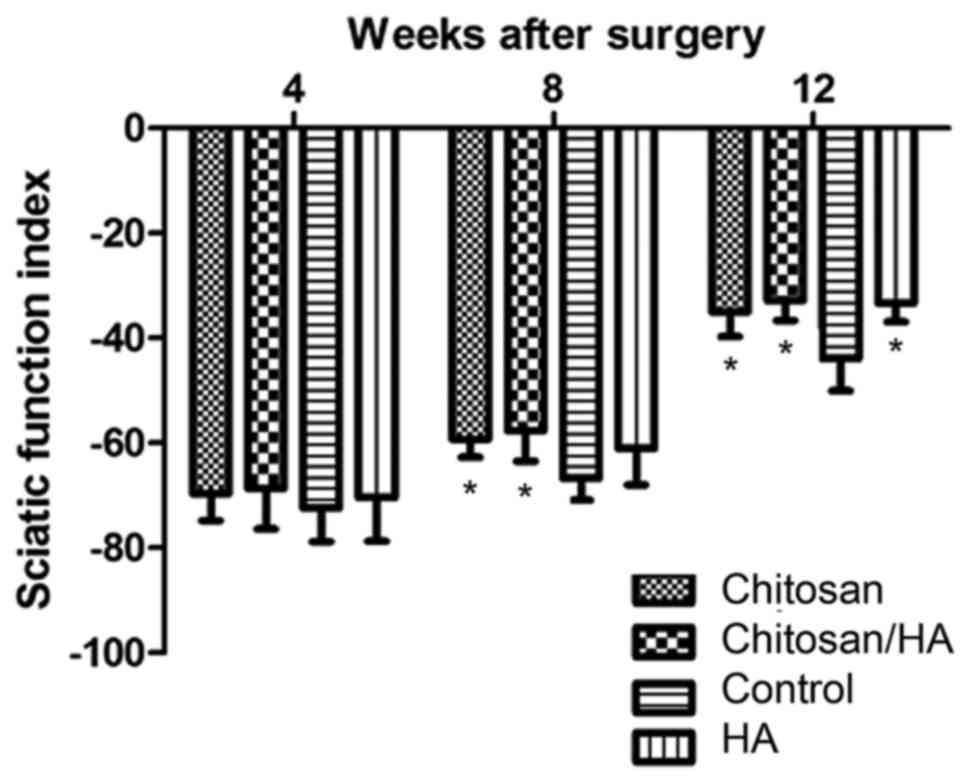
SFI outcome
At 4 weeks following surgery, the SFI of each group
exhibited no statistically significant difference (P>0.05;
Fig. 2). At 8 weeks following
surgery, the SFI of the chitosan group and the chitosan/HA group
was significantly higher compared with the control group
(P<0.05; Fig. 2). However, no
significant difference was observed between the SFI of the chitosan
and the chitosan/HA groups, suggesting that the chitosan alone
treatment was equally beneficial to nerve recovery as the combined
treatment. In addition, HA treatment alone exhibited no significant
difference in SFI outcome compared with control at 8 weeks
(Fig. 2). At 12 weeks following
surgery, the results demonstrated that the recovery of the clamped
nerves function in the control group was the worst in all four
groups (P<0.05; Fig. 2).
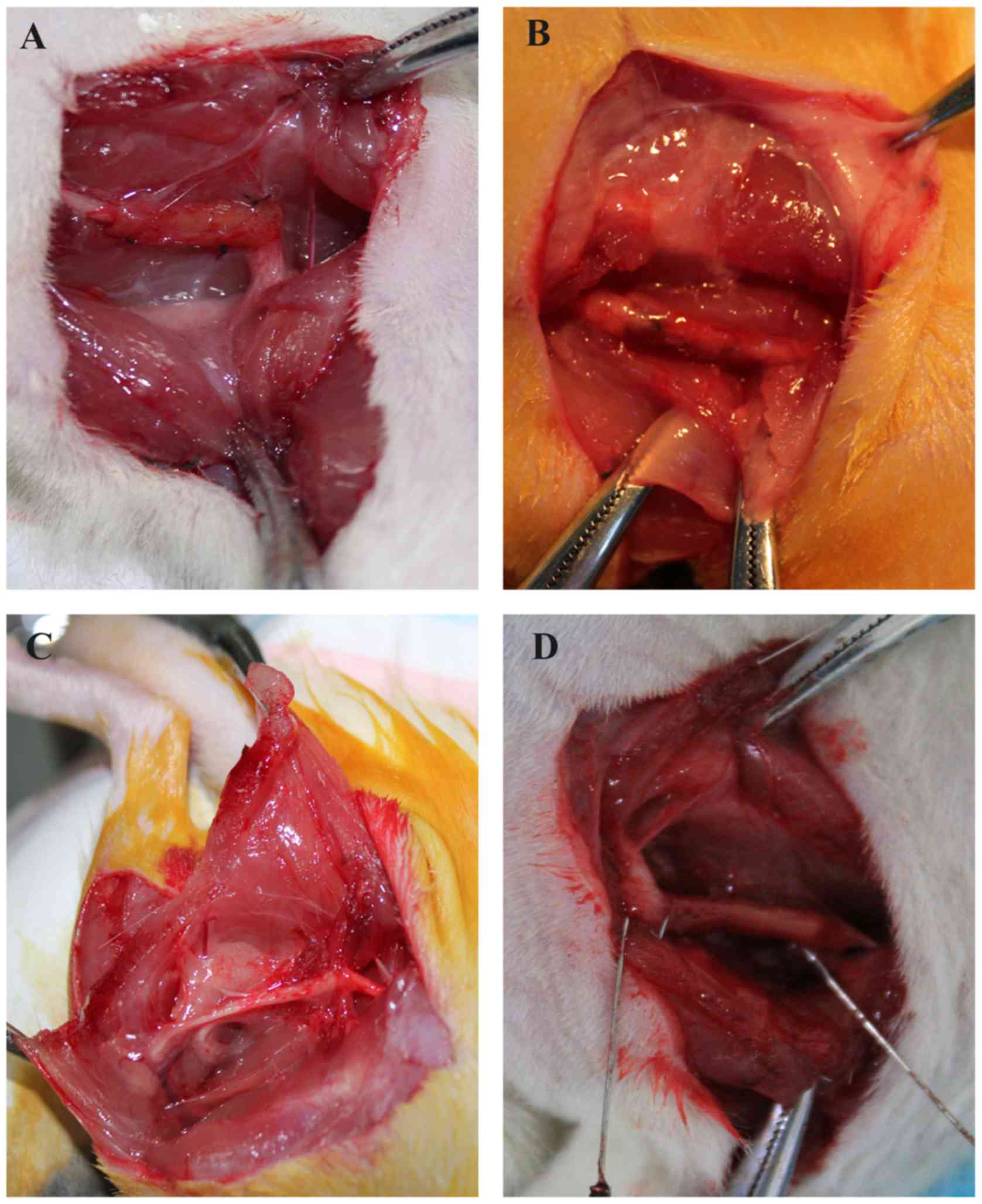
Scar adhesions
Following anesthesia, the skin was incised along the
original incision, and then the muscle, fascia and nerves were
separated layer by layer (Fig. 3).
At 4, 8 and 12 weeks following surgery, test results revealed that
the skin, muscle and fascia of all the rats healed well without
wound disruption and infection (Table
I). At 4 weeks following surgery, the nerves in all four groups
had only a mild adhesion with the surrounding muscle and fascia
tissue, and were easy to separate from them. Statistically, there
was no significant difference among the groups (P>0.05; Table I), as measured by the Petersen
classification (14). At 8 and 12
weeks following surgery, the control group had a significantly
heavier adhesion compared with the chitosan/HA group (P<0.05;
Table I). No statistically
significant differences were observed by either the chitosan alone
group or the HA alone group when compared with the control group
(P>0.05; Table I).
 | Table I.Evaluation of scar adhesion according
to the Petersen classification. |
Table I.
Evaluation of scar adhesion according
to the Petersen classification.
|
| 4 weeks | 8 weeks | 12 weeks |
|---|
|
|
|
|
|
|---|
|
| Skin | Muscle and
fascia | Neurons | Skin | Muscle and
fascia | Neurons | Skin | Muscle and
fascia | Neurons |
|---|
| Chitosan | 1 | 1 | 1.4±0.55 | 1 | 1.4±0.55 | 1.6±0.55 | 1 | 1.4±0.55 | 1.8±0.45 |
| Chitosan/HA | 1 | 1 | 1.2±0.45 | 1 |
1.2±0.45a |
1.2±0.45a | 1 |
1.2±0.45a |
1.6±0.55a |
| Control | 1 | 1 | 1.4±0.55 | 1 | 1.4±0.55 | 2.0±0.00 | 1 | 1.6±0.55 | 2.0±0.45 |
| HA | 1 | 1 | 1.2±0.45 | 1 | 1.2±0.45 | 1.6±0.55 | 1 | 1.4±0.55 | 2.0±0.00 |
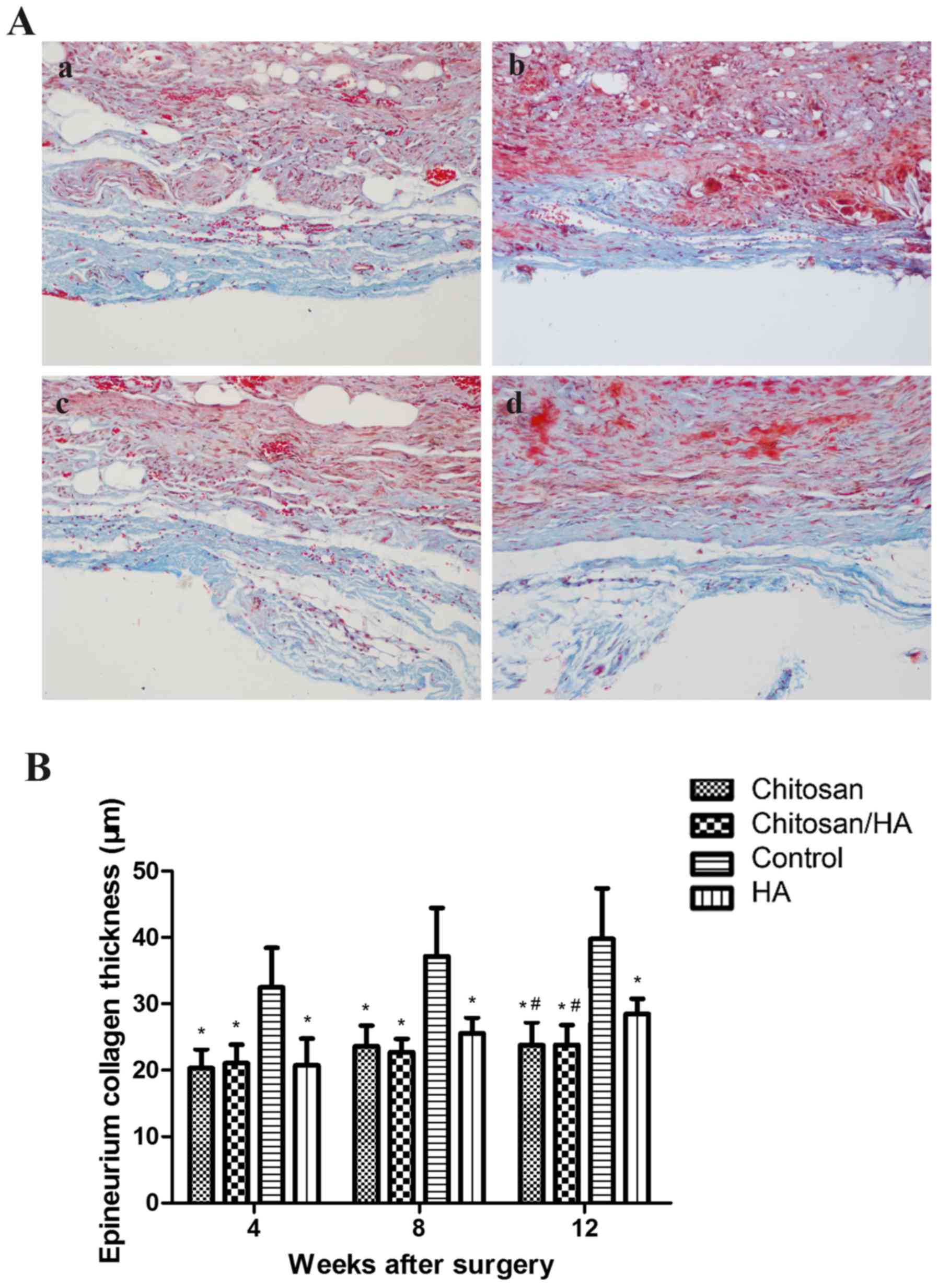
Histological findings
The status of extraneural scar hyperplasia was
observed by Masson staining (Fig.
4A). At 4, 8, 12 weeks following surgery, the collagen of
epineurium in the control group was noticeably thicker compared
with the treatment groups. Quantification of the epineurium
collagen thickness demonstrated that this was significantly higher
in the control group compared with the treatment groups (P<0.05;
Fig. 4B). At 12 weeks following
surgery, the collagen of the epineurium in the HA group was
significantly thicker compared with the chitosan group and the
chitosan/HA group (P<0.05; Fig.
4B).
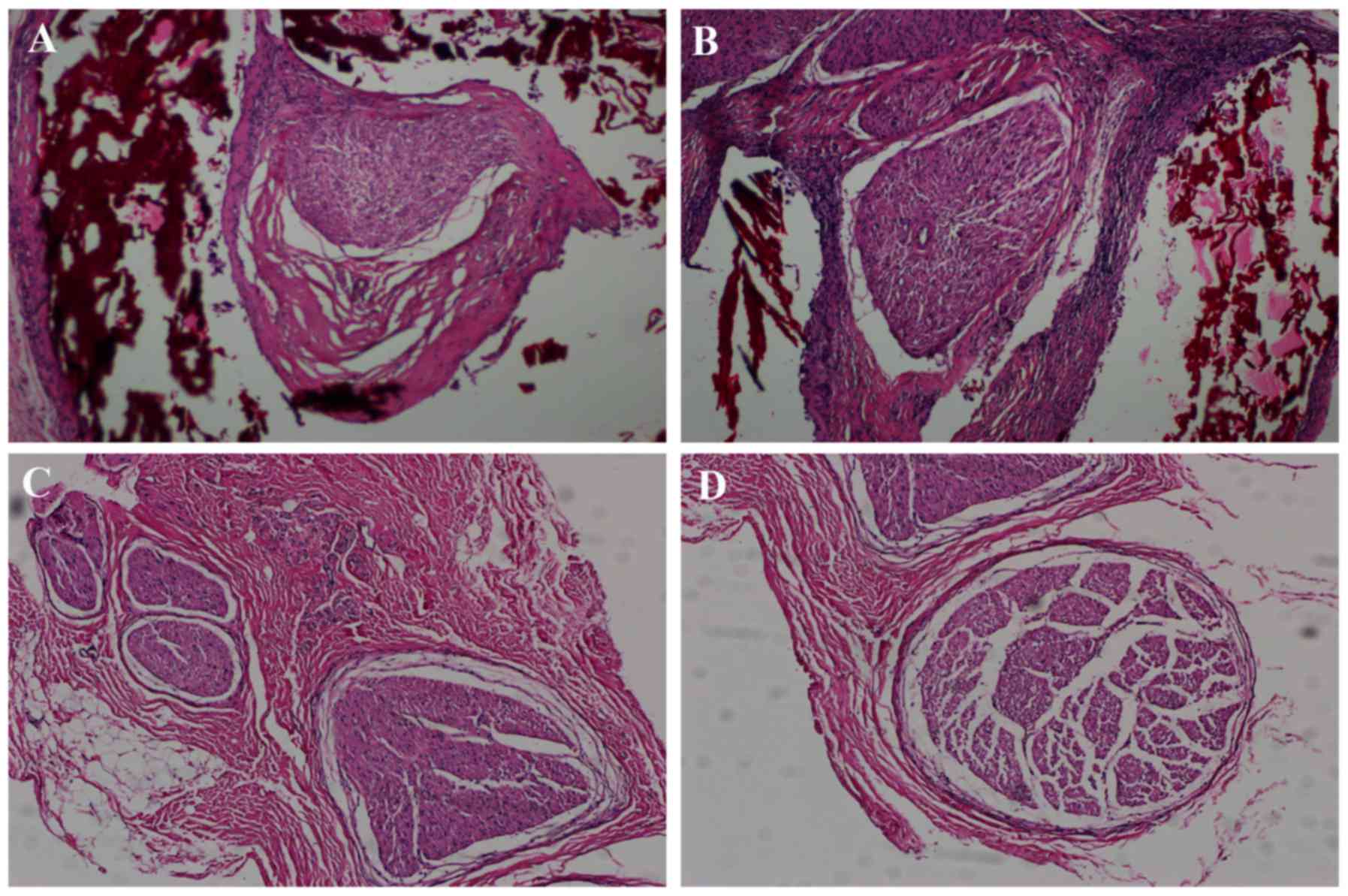
At 12 weeks following surgery, there were no
significant inflammatory changes observed among the experimental
groups (Fig. 5). H&E staining
demonstrated that there were a large number of nerve fibers in each
group, which grew in closely packed bundles, with the nerve fibers
in the chitosan/HA group being the most compact (Fig. 5).
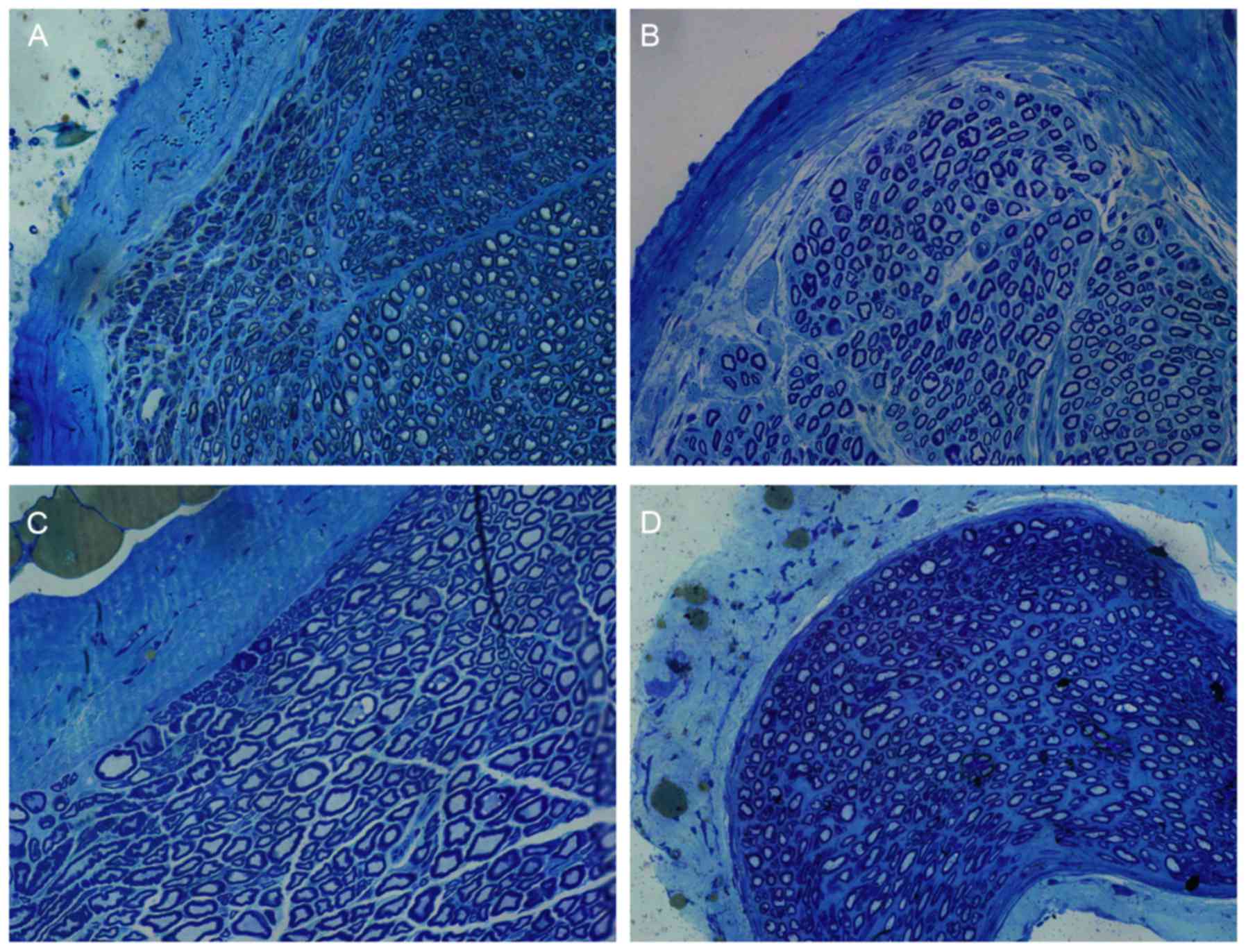
Toluidine blue staining results revealed that a
number of myelinated nerve fibers in each group existed in the
trauma area (Fig. 6). The
myelinated nerve fibers in the chitosan/HA group displayed the most
orderly arrangement (Fig. 6). The
myelinated nerve fibers of the control group were arranged in an
organized way but relatively sparse, and the morphology of the
axons was the most irregular compared with the treatment groups
(Fig. 6).
TEM findings
Using TEM, plenty of nerve fibers, myelinated nerve
fibers and Schwann cells were observed in each group (Fig. 7). Microtubules, microfilaments and
mitochondria were also abundant in the nerve axons. However, more
nerve fibers were observed in the chitosan and the chitosan/HA
groups compared with the other groups. Compared with the other
three groups, the chitosan/HA group had the least connective
tissue, the most myelinated nerve fibers and the most distinct
morphology (Fig. 7). The control
and HA groups exhibited less dense nerve fibers, irregular axon
morphology, and a more dissolved myelin. The number of nerve fibers
was calculated by counting the number of axons of slices stained
with toluidine blue. The nerve fiber diameter and myelin sheath
thickness were quantified using the images from the TEM
analysis.
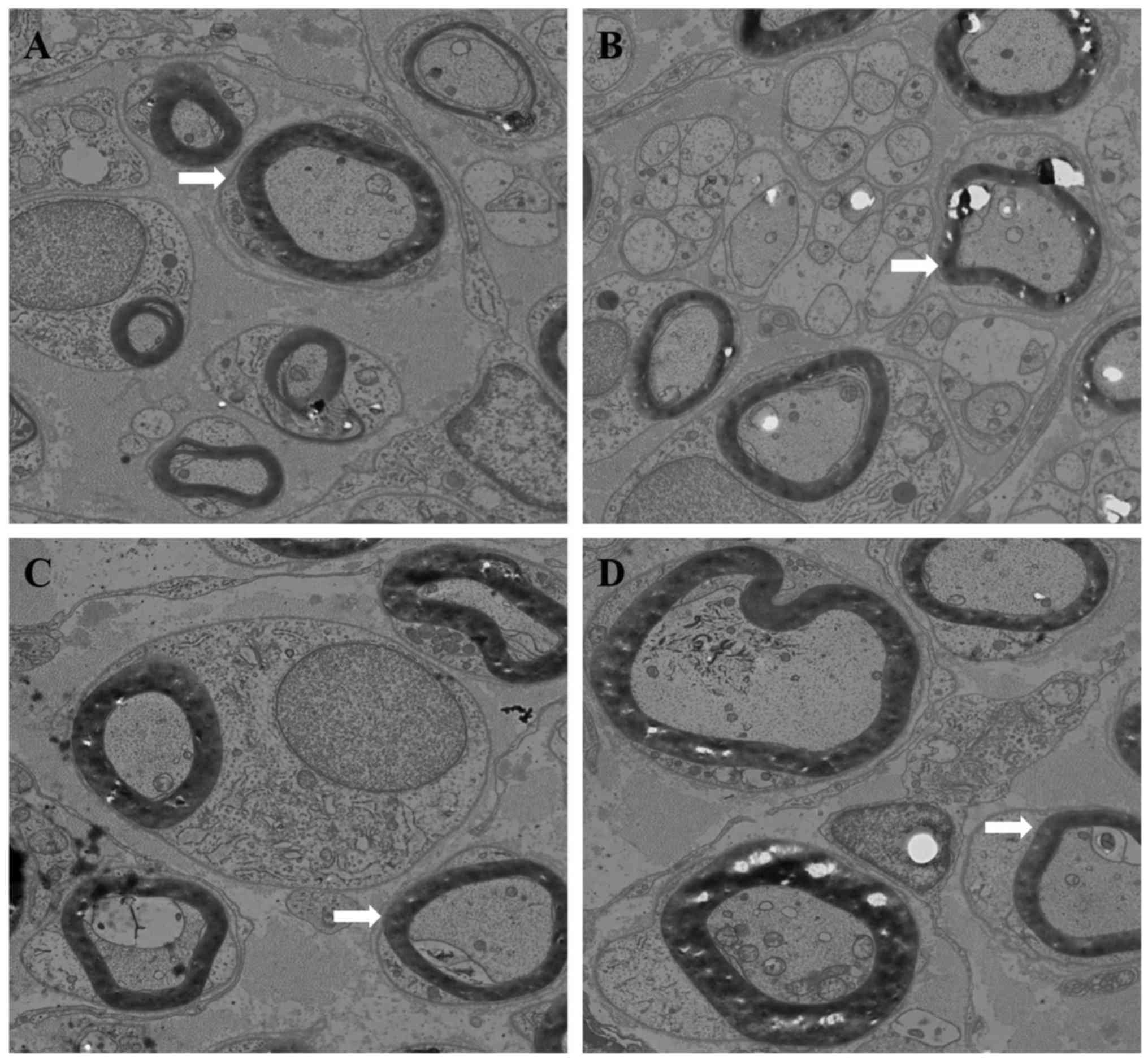 | Figure 7.Transmission electron microscopy
analysis of tissue samples from the four experimental groups.
Representative images of (A) chitosan group, (B) chitosan/HA group,
(C) control group and (D) HA group (magnification, ×4,000). Arrow
heads indicate the representative axons in each group. The diameter
of axons and the thickness of myelin sheath in the control group
appeared decreased compared with the treatment groups. Plenty of
myelinated nerve fibers and Schwann cells were observed in each
group. Axons contained a large number of neuronal microtubules,
microfilaments, mitochondria. Compared with the other groups, the
chitosan/HA group exhibited less connective tissue, the myelinated
nerve fibers were arranged more tightly, the myelinated nerve
fibers were more regular and uniform in diameter, and the shapes of
axons were more equal and regular. HA, hyaluronic acid. |
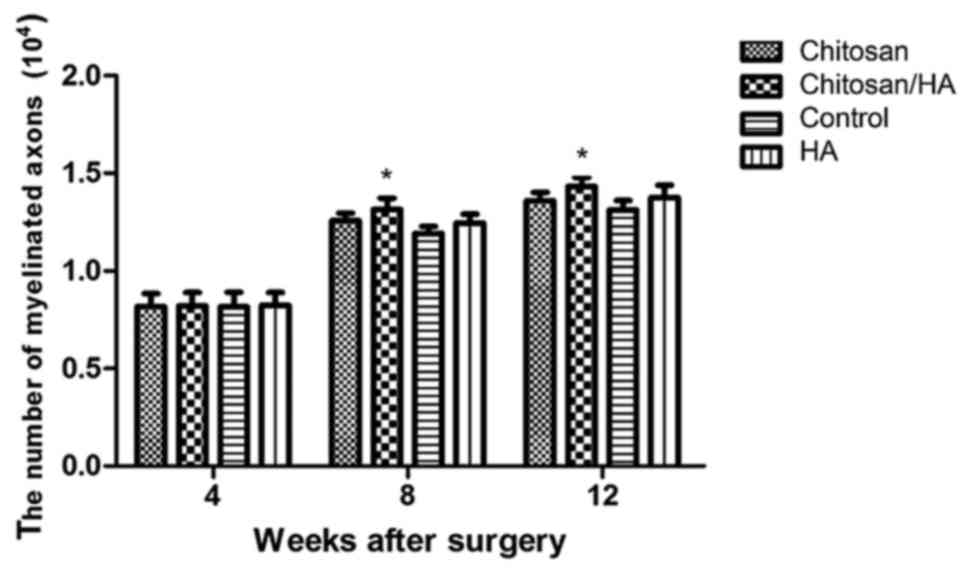
Nerve fiber number
At 4 weeks following surgery, the number of nerve
fibers per section in either group had no obvious difference
(P>0.05; Fig. 8). At 8 and 12
weeks following surgery, the nerve fiber number in the chitosan/HA
group was significantly larger compared with the control group
(P<0.05; Fig. 8).
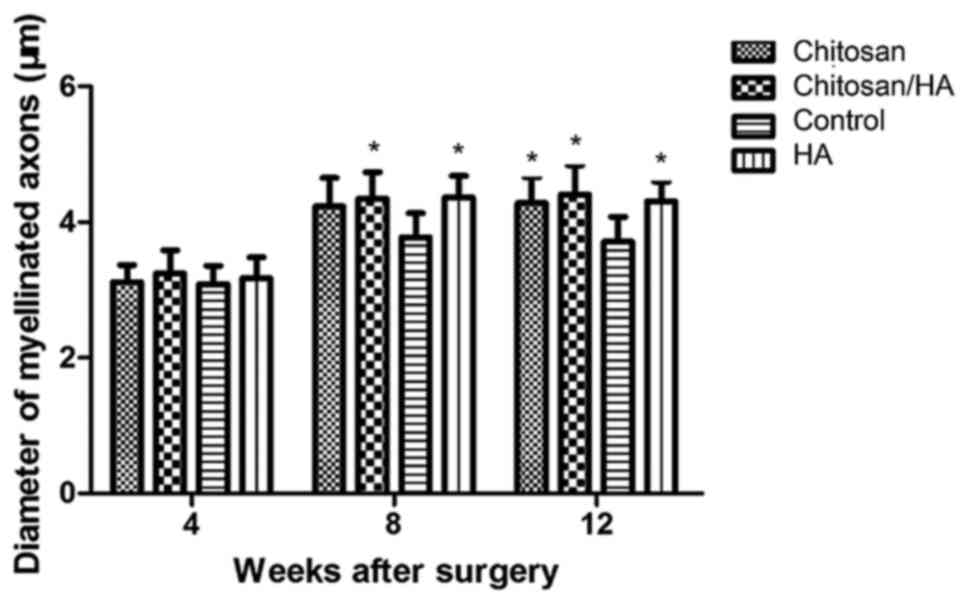
Myelinated nerve fiber diameter
At 4 weeks following surgery, the average diameter
of myelinated nerve fibers in each group had no significant
difference (P>0.05; Fig. 9).
However, at 8 and 12 weeks following surgery, the average diameter
of myelinated nerve fibers in the control group was significantly
smaller compared with the three treatment groups (Fig. 9). No significant difference was
observed among the treatment groups (P>0.05; Fig. 9).
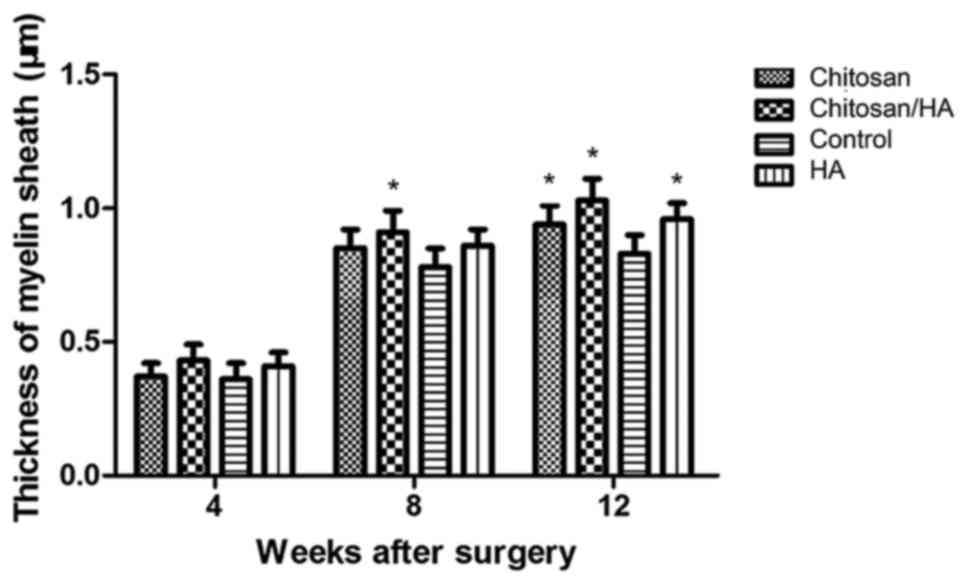
Myelin sheath thickness
At 4 weeks following surgery, the average myelin
sheath thickness was similar in the four experimental groups
(Fig. 10). At 8 weeks following
surgery, the myelin sheath thickness in the chitosan/HA group was
slightly but significantly larger compared with the control group
(Fig. 10). Finally, at 12 weeks
following surgery, the thickness of the myelin sheath was
significantly larger in all three treatment groups compared with
the control (Fig. 10).
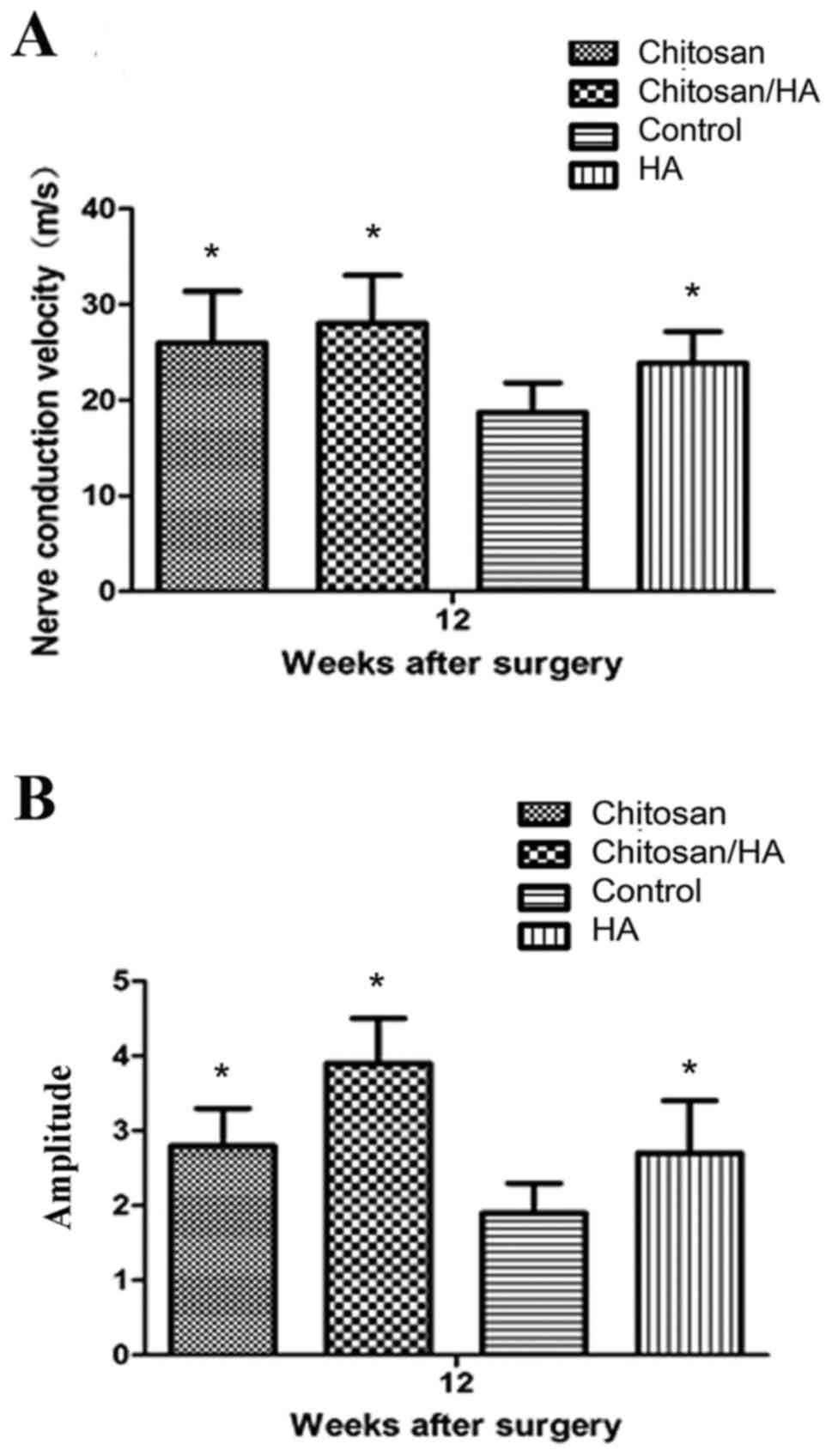
Electrophysiological measurement
At 12 weeks following surgery, nerve conduction
velocity (NCV) and amplitude was measured in the experimental rats
by electrophysiological assessment. As presented in Fig. 11, the results revealed that NCV in
the control group was significantly slower compared with the
treatment groups (P<0.05; Fig.
11A), and amplitude was significantly smaller compared with the
treatment groups (P<0.05; Fig.
11B).
Discussion
Extraneural scarring results in tissue contracture
around nerves and pressure on the nerve trunk, which may reduce the
diameter of nerves by up to 80–90% in the three months following
nerve injury (13). In addition,
extraneural scarring may mechanically compress and then interrupt
blood flow in the injury area, leading to hypoxic nerves and
inhibiting nerve functional recovery (16,17).
Nerves adhered to peripheral tissue cannot slide
normally, and this effect may disturb the recovery of nerves or
lead to stretch injury at the proximal ends of nerves. If nerves
are adhered to hard bone tissue, it can even cause new stretch
injury to the nerve segments already repaired (1). Therefore, extraneural scarring and
adhesion directly influences the functional recovery of peripheral
nerves. To date, many methods have been explored in order to
prevent extraneural scarring and adhesion, mainly involving drug
intervention and physical barriers using autologous tissue flap or
synthetic material to coat the injured nerves.
While many pharmaceutical agents have been used to
prevent nerve scarring and adhesion in experimental studies,
results have been poor. Doxorubicin (DXR), an anthracycline
anticancer agent, is mainly used in treating lymphoma and
soft-tissue sarcoma in clinical practice (18,19).
Albayrak et al (20)
reported that when DXR was placed around nerves that had complete
epineurium for 5 min, the formation of extraneural scar and
adhesion was reduced after 12 weeks. However, other experimental
studies have reported that DXR may lead to neurotoxic effects due
to anterograde axonal transport, even if it is administered by
intraneural microinjection into the nerves (21,22).
Methyl prednisolone acetate, an anti-inflammatory drug, has also
been used in the surgical site following neurolysis, in order to
reduce adhesion, however, Ikeda et al (2) reported that less intraneural and
extraneural scar tissue existed in the HA treatment group compared
with the methyl prednisolone acetate group, and the tensile
strength needed to strip the sciatic nerve from surrounding tissue
in the HA group was less compared with the other groups, suggesting
that methyl prednisolone acetate did not significantly improve
nerve scarring and adhesion.
HA-carboxymethylcellulose (HA-CMC), also known as
Seprafilm, is a type of degradable biomembrane, which is a mixture
of HA with carboxymethylcellulose (23,24).
Several clinical studies have claimed that HA-CMC can effectively
reduce adhesion following abdominal and pelvic surgeries. According
to Magill et al (25), when
Seprafilm was placed in proximity to nerves or used following nerve
injury, no obvious deleterious effect was observed, while it
markedly reduced extraneural scarring and increased the diameter of
axonal fibers. However, results from walking track analysis
revealed no improvement in nerve regeneration by seprafilm
(25). Park et al (26) have also reported that HA-CMC can
effectively reduce extraneural scarring and adhesion. Another
study, however, reported that, under bacterial peritonitis
conditions, Seprafilm may increase the inflammatory reaction and
fibrosis and lead to increased adhesion (27). Hence, further study and validation
is needed in order to fully understand whether HA-CMC is beneficial
for nerve regeneration and its potential disadvantages.
Ozgenel et al (28) applied human amniotic membrane
wrapping to the injury section of sciatic nerve and injected HA
into nerves, and they reported that this treatment method was safe
and effective in preventing extraneural scarring and adhesion
(29,30). However, limited sources of amniotic
membrane exist. Therefore, in the present study, chitosan, which is
widely available, was used in combination with HA. Previous studies
regarding application of chitosan in peripheral nerve injury
repair, chitosan was used only as a physical channel for nerve
regeneration, and other substances, such as growth factors, cells
and hydrogels, were used in order to promote the regeneration of
peripheral nerve defects (8,9). In
the present study, however, we focused on the role of chitosan and
HA gel in promoting neural regeneration during nerve repair.
Chitosan was used to cover the sciatic nerve following the sciatic
nerve clamp, and the HA gel was applied to cover the surface of the
scaffold. Then the potential preventive effects of chitosan or HA
or their combination were evaluated on extraneural scarring and
adhesion, and on the regeneration and functional recovery of nerves
following nerve injury using a rat sciatic nerve clamp injury
model.
The present results demonstrated that the
extraneural scarring was reduced by treatment with chitosan or HA
or their combination. At 12 weeks following surgery, the chitosan
group and the chitosan/HA group displayed better results compared
with the HA group and the control group. Scar adhesion analysis
revealed that chitosan combined with HA effectively reduced the
sciatic nerve adhesion with surrounding tissue. Another study has
also reported that HA can inhibit the formation of scar and reduce
adhesion by histological examination and measuring the tensile
strength that is needed to peel the sciatic nerve away from
surrounding tissue (2). Assessment
of the SFI revealed that, at 8 weeks following surgery, functional
recovery of sciatic nerves in the chitosan group and the
chitosan/HA group was obviously better compared with the control
group. At 12 weeks following surgery, SFI analysis and
electrophysiological measurement revealed that all three treatment
groups recovered sciatic nerve function and increased their nerve
conduction velocity compared with control. Due to the scar
formation, the progress of nerve regeneration was most likely
inhibited in the control group at this later stage. The present
data demonstrated that both chitosan and HA had a role in nerve
regeneration. Ishikawa et al (31) applied chitosan conduit to bridge a
sciatic nerve gap in rats, and observed an increased number of
regenerated axons using electron microscopy. The present
experimental results of the combination treatment indicated that
chitosan and HA might have a synergistic effect, including a
stronger inhibition of neural scar and adhesion formation, and
promotion of nerve regeneration. It should be noted that the
effects from the combination group were not significantly better
than the chitosan or HA alone groups in several of the functions
tested, and this may be due to the small sample sizes in the
present study. However, the chitosan/HA combination treatment
exhibited markedly decreased scar adhesion compared with the
chitosan or HA alone groups, which thus may provide a more
favorable microenvironment for nerve regeneration. Since HA and
chitosan both have roles in promoting nerve regeneration (29,30),
using a combination treatment for nerve clamp injury may
synergistically promote never regeneration.
In conclusion, both chitosan and HA inhibited
extraneural scarring, promoted nerve regeneration, increased the
nerve conduction velocity and improved the recovery of nerve
function. Chitosan exhibited a more significant effect on
inhibiting extraneural scarring compared with HA in the later phase
of neural repair. In addition, chitosan conduit combined with HA
may be more effective than either chitosan or HA alone to reduce
extraneural scarring and adhesion, and to promote neural
regeneration and repair. Further studies will be required in the
future in order to fully investigate the mechanisms and effects of
a chitosan conduit and HA combination in preventing nerve scarring
and adhesion and promoting nerve regeneration.
Acknowledgements
This study was supported by grants from the National
Natural Science Foundation of China (grant no. 81371116) and the
Natural Science Foundation of Beijing (grant no. 13G30867).
References
|
1
|
Ip WY, Shibata T, Tang FH, Mak AF and Chow
SP: Adhesion formation after nerve repair: An experimental study of
early protected mobilization in the rabbit. J Hand Surg Br.
25:582–584. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ikeda K, Yamauchi D, Osamura N, Hagiwara N
and Tomita K: Hyaluronic acid prevents peripheral nerve adhesion.
Br J Plast Surg. 56:342–347. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Smit X, van Neck JW, Afoke A and Hovius
SE: Reduction of neural adhesions by biodegradable autocrosslinked
hyaluronic acid gel after injury of peripheral nerves: An
experimental study. J Neurosurg. 101:648–652. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rosales-Cortes M, Rosales-Cortés M,
Peregrina-Sandoval J, Bañuelos-Pineda J, Sarabia-Estrada R,
Gómez-Rodiles CC, Albarrán-Rodríguez E, Zaitseva GP and Pita-López
ML: Immunological study of a chitosan prosthesis in the sciatic
nerve regeneration of the axotomized dog. J Biomater Appl.
18:15–23. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Yuan Y, Zhang P, Yang Y, Wang X and Gu X:
The interaction of Schwann cells with chitosan membranes and fibers
in vitro. Biomaterials. 25:4273–4278. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Freier T, Koh HS, Kazazian K and Shoichet
MS: Controlling cell adhesion and degradation of chitosan films by
N-acetylation. Biomaterials. 26:5872–5878. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Patel M, Vandevord PJ, Matthew H, Wu B,
DeSilva S and Wooley PH: Video-gait analysis of functional recovery
of nerve repaired with chitosan nerve guides. Tissue Eng.
12:3189–3199. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Meyer C, Wrobel S, Raimondo S, Rochkind S,
Heimann C, Shahar A, Ziv-Polat O, Geuna S, Grothe C and
Haastert-Talini K: Peripheral nerve regeneration through
hydrogel-enriched chitosan conduits containing engineered schwann
cells for drug delivery. Cell Transplant. 25:159–182. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nawrotek K, Tylman M, Rudnicka K,
Gatkowska J and Wieczorek M: Epineurium-mimicking chitosan conduits
for peripheral nervous tissue engineering. Carbohydr. Polym.
152:119–128. 2016.
|
|
10
|
Hsueh YY, Chang YJ, Huang TC, Fan SC, Wang
DH, Chen JJ, Wu CC and Lin SC: Functional recoveries of sciatic
nerve regeneration by combining chitosan-coated conduit and
neurosphere cells induced from adipose-derived stem cells.
Biomaterials. 35:2234–2244. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ao Q, Fung CK, Tsui AY, Cai S, Zuo HC,
Chan YS and Shum DK: The regeneration of transected sciatic nerves
of adult rats using chitosan nerve conduits seeded with bone marrow
stromal cell-derived Schwann cells. Biomaterials. 32:787–796. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kabiri M, Oraee-Yazdani S, Shafiee A,
Hanaee-Ahvaz H, Dodel M, Vaseei M and Soleimani M:
Neuroregenerative effects of olfactory ensheathing cells
transplanted in a multi-layered conductive nanofibrous conduit in
peripheral nerve repair in rats. J Biomed Sci. 22:352015.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Farjah GH and Fazli F: The effect of chick
embryo amniotic fluid on sciatic nerve regeneration of rats. Iran J
Vet Res. 16:167–171. 2015.PubMed/NCBI
|
|
14
|
Petersen J, Russell L, Andrus K, MacKinnon
M, Silver J and Kliot M: Reduction of extraneural scarring by
ADCON-T/N after surgical intervention. Neurosurgery. 38:976–984.
1996. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sunderland S and Bradley KC: Endoneurial
tube shrinkage in the distal segment of a severed nerve. J Comp
Neurol. 93:411–420. 1950. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Rydevik B, Lundborg G and Nordborg C:
Intraneural tissue reactions induced by internal neurolysis. An
experimental study on the blood-nerve barrier, connective tissues
and nerve fibres of rabbit tibial nerve. Scand J Plast Reconstr
Surg. 10:3–8. 1976. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wilgis EF and Murphy R: The significance
of longitudinal excursion in peripheral nerves. Hand Clin.
2:761–766. 1986.PubMed/NCBI
|
|
18
|
Younes A: New treatment strategies for
aggressive lymphoma. Semin Oncol. 31 6 Suppl 15:S10–S13. 2004.
View Article : Google Scholar
|
|
19
|
Pervaiz N, Colterjohn N, Farrokhyar F,
Tozer R, Figueredo A and Ghert M: A systematic meta-analysis of
randomized controlled trials of adjuvant chemotherapy for localized
resectable soft-tissue sarcoma. Cancer. 113:573–581. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Albayrak BS, Ismailoglu O, Ilbay K, Yaka
U, Tanriover G, Gorgulu A and Demir N: Doxorubicin for prevention
of epineurial fibrosis in a rat sciatic nerve model: Outcome based
on gross postsurgical, histopathological and ultrastructural
findings. J Neurosurg Spine. 12:327–333. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
England JD, Rhee EK, Said G and Sumner AJ:
Schwann cell degeneration induced by doxorubicin (adriamycin).
Brain. 111:901–913. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
England JD, Asbury AK, Rhee EK and Sumner
AJ: Lethal retrograde axoplasmic transport of doxorubicin
(adriamycin) to motor neurons. A toxic motor neuronopathy. Brain.
111:915–926. 1988. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Becker JM, Dayton MT, Fazio VW, Beck DE,
Stryker SJ, Wexner SD, Wolff BG, Roberts PL, Smith LE, Sweeney SA
and Moore M: Prevention of postoperative abdominal adhesions by a
sodium hyaluronate-based bioresorbable membrane: A prospective,
randomized, double-blind multicenter study. J Am Coll Surg.
183:297–306. 1996.PubMed/NCBI
|
|
24
|
Fazio VW, Cohen Z, Fleshman JW, van Goor
H, Bauer JJ, Wolff BG, Corman M, Beart RW Jr, Wexner SD, Becker JM,
et al: Reduction in adhesive small-bowel obstruction by Seprafilm
adhesion barrier after intestinal resection. Dis Colon Rectum.
49:1–11. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Magill CK, Tuffaha SH, Yee A, Luciano JP,
Hunter DA, Mackinnon SE and Borschel GH: The short- and long-term
effects of Seprafilm on peripheral nerves: A histological and
functional study. J Reconstr Microsurg. 25:345–354. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Park JS, Lee JH, Han CS, Chung DW and Kim
GY: Effect of hyaluronic acid-carboxymethylcellulose solution on
perineural scar formation after sciatic nerve repair in rats. Clin
Orthop Surg. 3:315–324. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kayaoglu HA, Ozkan N, Hazinedaroglu SM,
Ersoy OF and Koseoglu RD: An assessment of the effects of two types
of bioresorbable barriers to prevent postoperative intra-abdominal
adhesions in rats. Surg Today. 35:946–950. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ozgenel GY and Filiz G: Combined
application of human amniotic membrane wrapping and hyaluronic acid
injection in epineurectomized rat sciatic nerve. J Reconstr
Microsurg. 20:153–157. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Zor f, Deveci M, Kilic A, Ozdag MF, Kurt
B, Sengezer M and Sönmez TT: Effect of VEGF gene therapy and
hyaluronic acid film sheath on peripheral nerve regeneration.
Microsurgery. 34:209–216. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Chen Q, Lu H and Yang H: Chitosan prevents
adhesion during rabbit flexor tendon repair via the sirtuin 1
signaling pathway. Mol Med Rep. 12:4598–4603. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ishikawa N, Suzuki Y, Ohta M, Cho H,
Suzuki S, Dezawa M and Ide C: Peripheral nerve regeneration through
the space formed by a chitosan gel sponge. J Biomed Mater Res A.
83:33–40. 2007. View Article : Google Scholar : PubMed/NCBI
|