Introduction
Annually, >275,000 novel cases of oral cancer
worldwide are reported and two-thirds of these cases occur in
developing regions, including Southeast Asia (1). Tongue squamous cell carcinoma (SCC)
is the most common subtype of oral cancer, which accounts for
40–50% of all cases (2). In recent
years, the incidence rate of tongue SCC has significantly
increased, particularly among young adults (3). Furthermore, a number of patients with
tongue SCC present with local lymph node metastasis at the time of
diagnosis. Despite the development of comprehensive therapies,
including extensive resection, and chemo- and radiotherapy
committed to tongue SCC, the prognosis remains poor due to tumor
recurrence and metastasis. For prognostic prediction to improve the
survival rate of patients with fewer therapy-associated
complications, it has become urgent to seek potential biomarkers
for tongue SCC (4).
The runt-related transcription factor (RUNX) family
has three members: RUNX1, RUNX2 and RUNX3 (5). The RUNX family encodes proteins that
contain a well-conserved 128 amino acid region (Runt domain), which
form a stable complex with core-binding factor subunit β to exert
their transactivation ability. RUNX proteins may regulate target
genes by binding to the promoters or enhancers of these genes,
which become disrupted in cancer cells (6). Among these three RUNX family members,
RUNX3 has been identified to be closely associated with
tumorigenesis and/or tumor progression (7). Absence of RUNX3 expression has been
detected in various types of human cancer, including esophageal,
gastric, colorectal, lung and breast cancer (8–12).
Inactivation of RUNX3 is additionally significantly correlated with
lymph node metastasis and worse prognosis. Conversely, the
restoration of RUNX3 may suppress the migration and invasion of
cancer cells in vitro (13–16).
These previous studies suggested that RUNX3 exerts tumor
suppressive effects and may serve a critical role in the
development of tumor metastasis. However, the function of RUNX3 in
tongue SCC has yet to be fully elucidated.
The present study aimed to detect RUNX3 expression
in patients with tongue SCC using tissue microarray (TMA)
technology and to analyze its association with clinicopathological
parameters. In addition, the present study aimed to analyze the
characteristics of RUNX3 in clinical samples and tongue SCC cell
lines.
Patients and methods
Ethics statement
The present study was performed under a protocol
approved by the Institutional Review Boards of the Affiliated
Hospital of Stomatology, Nanjing Medical University (Nanjing,
China). All patients provided written informed consent prior to the
study.
Patient samples
In total, three cancerous and paired non-cancerous
tissues were obtained from patients with tongue SCC without a
history of smoking or alcohol consumption. All three patients were
admitted to the Department of Oral and Maxillofacial Surgery,
Stomatological Hospital Affiliated to Nanjing Medical University in
2015. The patients comprised two men: i) Age, 46 years; admitted in
December, 2015; ii) age, 56 years; admitted in May, 2015, and one
woman (age, 68 years; admitted in December, 2015). All patients
were pathologically diagnosed with moderate SCC and T1N0M0. The
fresh samples were washed three times with sterilized PBS and lysed
in ice-cold lysis buffer (Becton, Dickinson and Company, Franklin
Lakes, NJ, USA) for 2 h at 4°C. The samples were subsequently
centrifuged at 12,000 × g for 30 min at 4°C, the supernatants were
collected and total protein concentration was measured by a
bicinchoninic acid protein assay (Invitrogen; Thermo Fisher
Scientific, Inc., Waltham, MA, USA) for RUNX3 protein
detection.
Western blot analysis
Tissue proteins (10 µg) were separated by 12%
SDS-PAGE, blocked with 5% bovine serum albumin (cat. no. 36101ES25;
Yeasen Biological Technology, Ltd., Shanghai, China) room
temperature for 2 h, and subsequently transferred onto a
nitrocellulose membrane. The member was incubated overnight at 4°C
with monoclonal anti-RUNX3 (cat. no. ab135248; 1:2,000; Abcam,
Cambridge, UK) and mouse anti-β-actin (1:1,000; cat. no. BA5180;
Wuhan Boster Biological Technology, Ltd., Wuhan, China). Membranes
were washed with PBS, incubated with secondary antibodies [goat
anti-rabbit (1:3,000; cat. no. BA1056; Wuhan Boster Biological
Technology, Ltd.) and goat anti-mouse immunoglobulin G (IgG;
1:3,000; cat. no. BA1050; Wuhan Boster Biological Technology,
Ltd.)] for 2 h at room temperature and washed with PBS containing
0.05% Tween-20 at room temperature. Subsequently, visualization
fluid (containing 10 ml alkaline phosphatase buffer, 33 µl
5-bromo-4-chloro-3-indolyl phosphate and 66 µl nitro-blue
tetrazolium chloride) was added to the membrane and the protein
bands were detected using Super Signal West Pico Chemiluminescent
Substrate (Thermo Fisher Scientific, Inc.). In total, three
independent blots of each protein were semi-quantified using Image
J software (1.48 version; National Institutes of Health, Bethesda,
MD, USA).
Tongue SCC cell culture
Human tongue SCC cell lines SCC25 and Cal27 were
purchased from the Shanghai Institute of Biochemistry and Cell
Biology, Chinese Academy of Sciences (Shanghai, China). SCC25 and
Cal27 cells were cultured in RPMI 1640 medium supplemented with 10%
fetal calf serum (both Gibco; Thermo Fisher Scientific, Inc.) at
37°C in a humidified incubator containing 95% air and 5%
CO2.
Immunofluorescence
SCC25 and Cal27 cells (0.5×105) were
seeded on coverslips and cultured for 24 h at 37°C; subsequently,
the coverslips were washed with PBS, fixed with 4% paraformaldehyde
for 30 min at room temperature, permeabilized in PBS containing
0.25% Triton X-100 for 30 min at room temperature and incubated
with 10% normal rabbit serum (cat. no. BSD0009; Yuduo Bio.,
Shanghai, China) for 30 min at room temperature, in order to block
nonspecific staining. Cells were then incubated overnight at 4°C
with mouse anti-RUNX3 antibody (1:500) and were incubated with
fluorescein isothiocyanate-conjugated secondary IgG (1:50; cat. no.
SA1064; Wuhan Boster Biological Technology, Ltd. Wuhan, China) for
2 h at room temperature. Cells were stained with DAPI (1:1,000;
cat. no. c1002; Beyotime Institute of Biotechnology, Haimen, China)
for 1 min to label the nuclei and were subsequently washed with
PBS. PBS was used instead of a primary antibody as a negative
control. Fluorescence images were captured under a fluorescence
microscope (Leica Microsystems GmbH, Wetzlar, Germany;
magnification, ×200).
Immunocytochemistry
SCC25 and Cal27 cells (0.5×105 cells)
were seeded on coverslips and were processed using the same
protocol as for immunofluorescence. Following an overnight
incubation at 4°C with the RUNX3 (1:500) antibody, cells were
subjected to the streptavidin-peroxidase (Sp) method using a
standard Sp kit (cat. no. PV-9000; Zhongshan Bio-Tech Co., Ltd.,
Beijing, China) according to the manufacturer's protocol.
Immunoreactivity was assessed and representative images were
captured using a light microscope with AxioCam MRc5 camera (Carl
Zeiss AG, Oberkochen, Germany; magnification, ×200).
TMA immunohistochemistry
Between January 2009 and January 2014, tissues were
collected during surgery from 79 patients with tongue SCC
hospitalized in the Department of Oral and Maxillofacial Surgery,
Affiliated Hospital of Stomatology, Nanjing Medical University, in
order to manufacture a tongue SCC TMA. Patients who had received
preoperative radiotherapy or chemotherapy were excluded from the
study and two pathologists confirmed all cases. All patients were
staged according to the classification of oral cancer by the
National Comprehensive Cancer Network (17) (2015) and were followed up at least
24 months post-operation for prognostic analysis. The array dot
diameter was 1.5 mm, and each dot represented a tissue spot from
one individual specimen that had been selected and pathologically
confirmed (18).
Immunohistochemistry was performed according to the
Sp method using a standard Sp kit (OriGene Technologies, Inc.). The
tongue SCC TMA slide was incubated with the monoclonal RUNX3
antibody (1:250) overnight at 4°C. Cells were subjected to the Sp
method (cat. no. PV-9000; Zhongshan Bio-Tech Co., Ltd.) according
to the manufacturer's protocol Diaminobenzidine (OriGene
Technologies, Inc. Beijing, China) was used as a chromogen for the
immunoperoxidase reaction. The slides were counterstained with
hematoxylin for 5 min at room temperature. Non-immune serum (cat.
no. BSD0009; Yuduo Bio.) instead of first antibody was used as a
negative control.
Immunoreactivity in carcinoma nests and stroma was
blindly assessed by two independent observers using a Zeiss Imager
Z1 light microscope (magnification, ×100), and the representative
images were obtained using an AxioCam MRc5 camera (both Carl Zeiss
AG). Carcinoma nests were defined as a cluster of cancer cells and
the connective tissues around the nests were considered as tumor
stroma. RUNX3 immunoreactivity in nuclei or cytoplasm was graded as
follows: Positive expression (positive cells ≥5%) and negative
expression (positive cells <5%) (19).
Statistical analysis
Statistical analysis was performed using SPSS
software version 20 (IBM Corp., Armonk, NY, USA). The western
blotting data were analyzed using a paired Student's t-test. The
associations between RUNX3 staining and clinicopathological
parameters were evaluated by Fisher's exact test and χ2
test. The association between RUNX3 expression in carcinoma
nests/stroma and patient survival was analyzed by Kaplan-Meier
survival analysis and a log-rank test. Univariate and multivariate
Cox regression analyses were used to investigate whether RUNX3
expression in carcinoma nests may be a predictor of overall
survival in patients with tongue SCC. P<0.05 was considered to
indicate a statistically significant difference.
Results
Reduced expression of RUNX3 protein in
tongue SCC
RUNX3 expression was significantly reduced in tongue
SCC tissues compared with paired non-cancerous tissues, indicating
that RUNX3 may be inactivated in patients with tongue SCC (Fig. 1A and B; P<0.01). To confirm this
observation, immunofluorescence and immunocytochemistry were used
to detect RUNX3 expression in the human tongue SCC cell lines,
SCC25 and Cal27. Immunofluorescence demonstrated that there was low
RUNX3 expression in the cytoplasm (Fig. 1C), thus confirming that RUNX3 was
localized to the cytoplasm in SCC25 and Cal27 cells.
Immunocytochemical analysis demonstrated similar results (Fig. 1D); however, nuclear staining of
RUNX3 was detected in a number of tongue SCC cells (Fig. 1D).
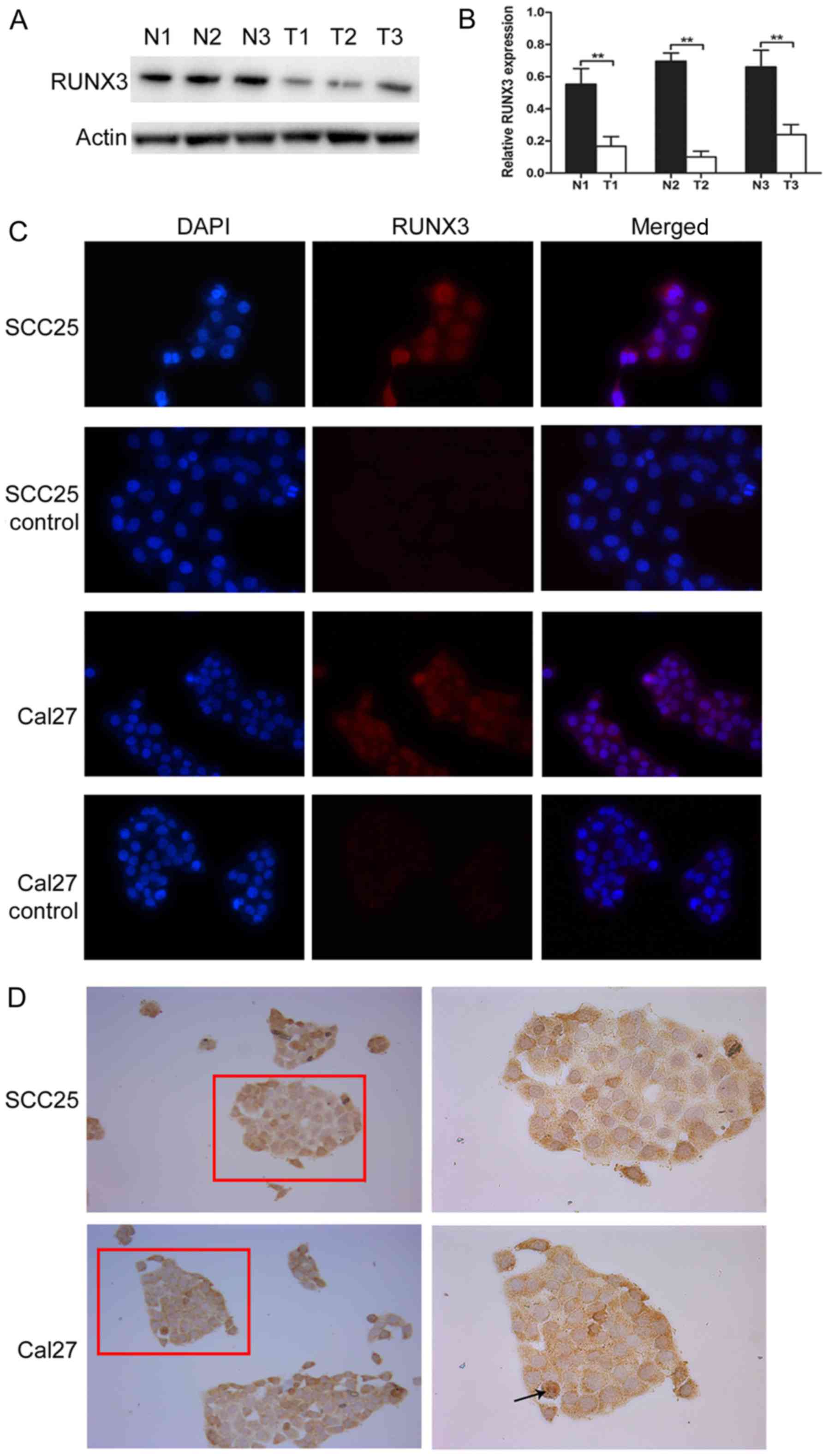 | Figure 1.Expression and localization of RUNX3
in tongue SCC. (A and B) Western blot analysis of the relative
protein expression levels of RUNX3 in three tongue SCC tissues and
paired non-cancerous tissues. **P<0.01. (C) Immunofluorescence
of RUNX3 in tongue SCC cell lines SCC25 and Cal27; low expression
was detected in the cytoplasm (magnification, ×200). Control groups
were incubated with PBS instead of first antibody. (D)
Immunochemistry of RUNX3 in tongue SCC cell lines SCC25 and Cal27
(left panel, magnification, ×100; right panel, magnification,
×200). The majority of staining was detected in the cytoplasm, but
a number of individual cells presented with nuclear staining (black
arrow). N, non-cancerous tissue; RUNX3, runt-related transcription
factor 3; SCC, squamous cell carcinoma; T, tumor tissue. |
Distinct expression of RUNX3 in tongue
SCC nests and stroma
Immunohistochemistry of 79 patients with tongue SCC
was performed using TMA technology to detect RUNX3 expression. The
distribution of RUNX3-positive cells revealed that RUNX3 was
expressed in different manners in carcinoma nests and stroma; to
the best of our knowledge, this has not been reported in previous
studies. RUNX3 in carcinoma nests (nRUNX3) exhibited nuclear
staining in 24 cases (30.4%). Cytoplasmic and undetectable staining
were considered negative expression of RUNX3, with a total of 55
cases (Table I). RUNX3-positive
staining in the nucleus and cytoplasm was not observed in any
carcinoma nest. RUNX3 in stroma (sRUNX3) was nuclear positive in 40
cases (50.6%) and nuclear negative in 39 cases (49.4%; Table II).
 | Table I.nRUNX3 and its clinicopathological
characteristics in 79 patients with tongue squamous cell
carcinoma. |
Table I.
nRUNX3 and its clinicopathological
characteristics in 79 patients with tongue squamous cell
carcinoma.
|
| nRUNX3 staining |
|
|
|---|
|
|
|
|
|
|---|
| Variable | Negative (%) | Positive (%) | Total |
P-valuea |
|---|
| Age, years |
|
|
|
|
|
≥60 | 23 (74.2) | 8 (25.8) | 31 | 0.618 |
|
<60 | 32 (66.7) | 16 (33.3) | 48 |
|
| Sex |
|
|
|
|
|
Male | 30 (69.8) | 13 (30.2) | 43 | 0.975 |
|
Female | 25 (69.4) | 11 (30.6) | 36 |
|
| Tumor size, cm |
|
|
|
|
| ≤2 | 25 (71.0) | 16 (29.0) | 41 | 0.093 |
|
>2 | 30 (78.9) | 8 (21.1) | 38 |
|
| Lymph node
status |
|
|
|
|
| N0 | 21 (55.3) | 17 (44.7) | 38 | 0.014 |
| N1, 2
and 3 | 34 (82.9) | 7 (17.1) | 41 |
|
| Histological
grade |
|
|
|
|
| I | 30 (68.2) | 14 (31.8) | 44 | 0.809 |
| II and
III | 25 (71.4) | 10 (28.6) | 35 |
|
| Clinical stage |
|
|
|
|
| I | 23 (57.5) | 17 (42.5) | 40 | 0.027 |
| II,
III, and IV | 32 (82.1) | 7 (17.9) | 39 |
|
| Total | 55 | 24 | 79 |
|
| Table II.sRUNX3 and its clinicopathological
characteristics in 79 patients with tongue squamous cell
carcinoma. |
Table II.
sRUNX3 and its clinicopathological
characteristics in 79 patients with tongue squamous cell
carcinoma.
|
| sRUNX3
staining |
|
|
|---|
|
|
|
|
|
|---|
| Variable | Negative (%) | Positive (%) | Total |
P-valuea |
|---|
| Age, years |
|
|
|
|
|
≥60 | 14 (45.2) | 17 (54.8) | 31 | 0.647 |
|
<60 | 25 (52.1) | 23 (47.9) | 48 |
|
| Sex |
|
|
|
|
|
Male | 24 (55.8) | 19 (44.2) | 43 | 0.261 |
|
Female | 15 (41.7) | 21 (58.3) | 36 |
|
| Tumor size, cm |
|
|
|
|
| ≤2 | 19 (46.3) | 22 (53.7) | 41 | 0.655 |
|
>2 | 20 (52.6) | 18 (47.4) | 38 |
|
| Lymph node
status |
|
|
|
|
| N0 | 12 (31.6) | 26 (68.4) | 38 | 0.003 |
| N1, 2
and 3 | 27 (65.9) | 14 (34.1) | 41 |
|
| Histological
grade |
|
|
|
|
| I | 18 (40.9) | 26 (59.1) | 44 | 0.069 |
| II and
III | 21 (60.0) | 14 (40.0) | 35 |
|
| Clinical stage |
|
|
|
|
| I | 13 (32.5) | 27 (67.5) | 40 | 0.003 |
| II,
III, and IV | 26 (66.7) | 13 (33.3) | 39 |
|
| Total | 39 | 40 | 79 |
|
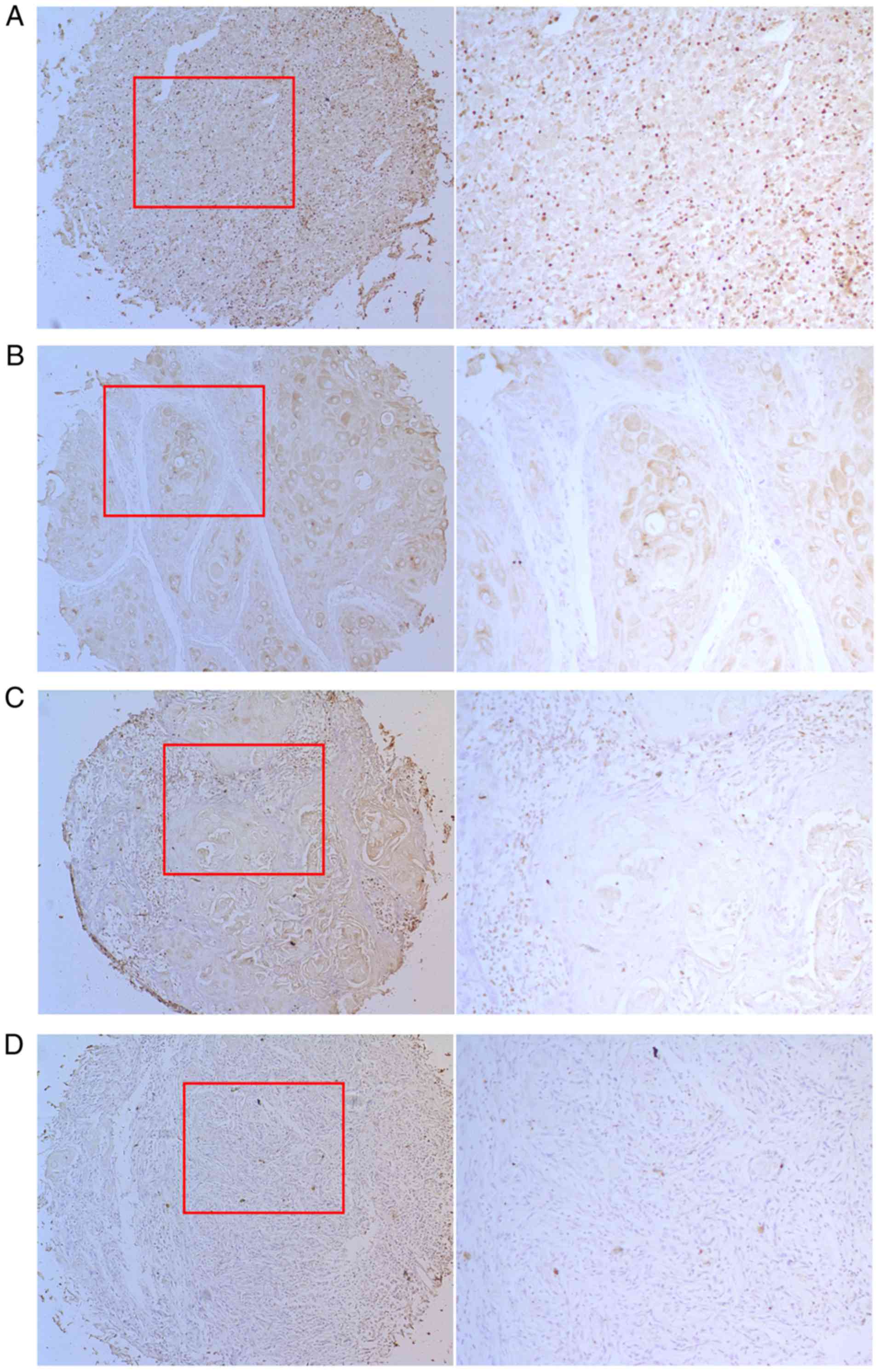
As presented in Fig. 2A
and B, positive nRUNX3 immunoreactivity was detected in the
nuclei and cytoplasm of cancer cells. Cytoplasmic staining was
distributed in the keratin pearl, and was the most common type of
staining among the 79 cases. This ‘RUNX3 mislocalization’ suggested
that RUNX3 protein was restricted to the cytoplasm and was not able
to function as a tumor suppressor as reported in previous studies
(9,12). The reduced expression and
mislocalization of RUNX3 protein were aberrant, thus indicating
RUNX3 gene impairment in cancer cells; therefore, these two types
of aberration were analyzed together as negative expression
(Table I). As presented in
Fig. 2C, the majority of positive
sRUNX3 cells were detected in clumps in the connecting zone
surrounding the carcinoma tissue. In addition, negative nRUNX3 and
sRUNX3 staining appeared in certain cases (Fig. 2D).
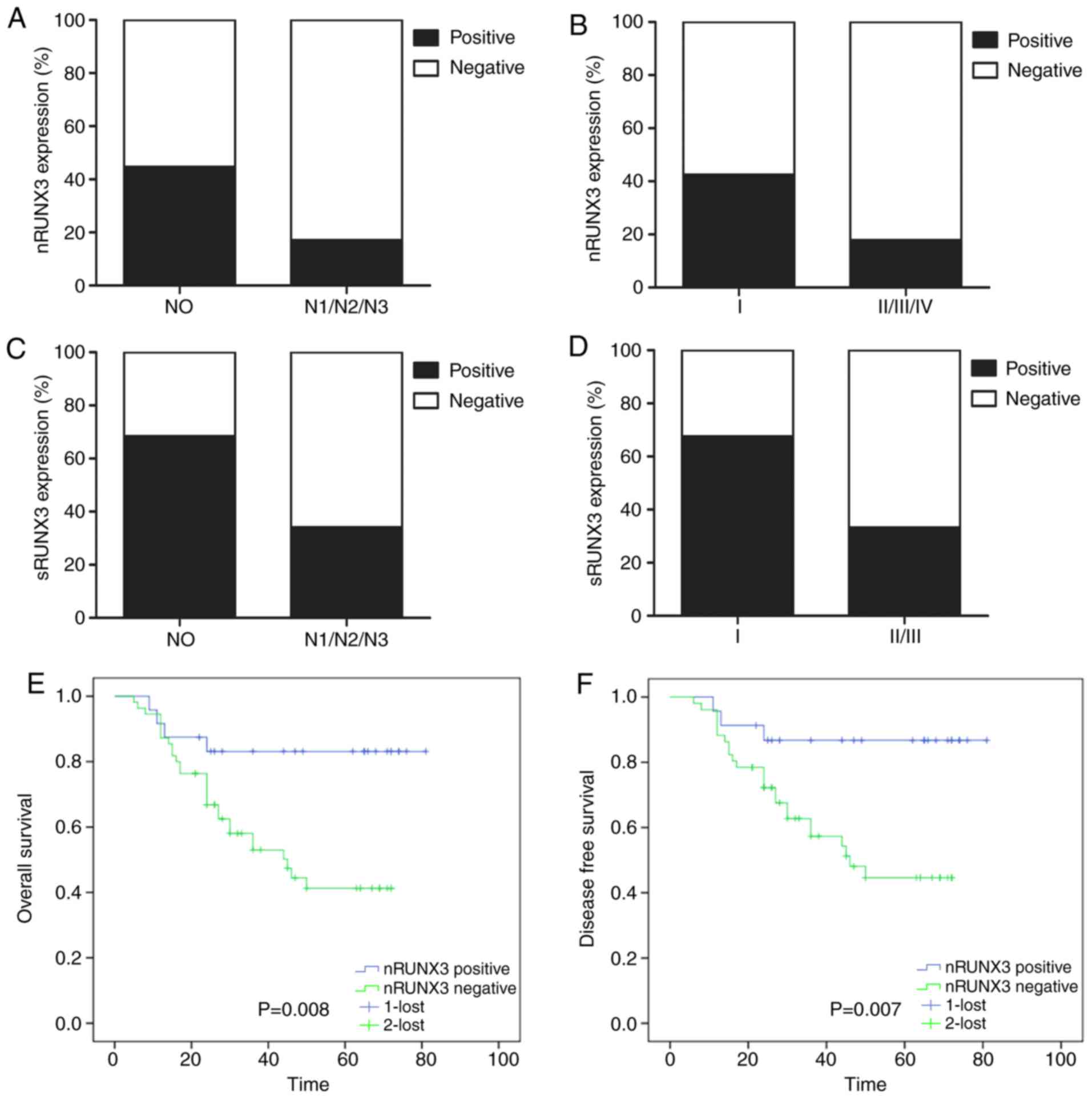
Association of nRUNX3 and sRUNX3 with
clinicopathological parameters
The association between RUNX3 expression and
clinicopathological variables was further investigated. It was
demonstrated that positive nRUNX3 expression was more frequent in
N0 cases and in clinical stage I cases (Fig. 3A and B). Positive sRUNX3 expression
was also higher in N0 cases and clinical stage cases (Fig. 3C and D). Through statistical
analysis, it was demonstrated that nRUNX3 expression was
significantly associated with lymph node status and clinical stage
(P=0.014 and P=0.027, respectively; Table I). In addition, sRUNX3 expression
was significantly associated with lymph node status and clinical
stage (P=0.003 and P=0.003, respectively; Table II). No significant associations
were observed between the expression of nRUNX3 and sRUNX3 and other
clinicopathological variables, including patient age, sex and tumor
size.
Negative expression of nRUNX3 is
associated with poor patient survival
To determine whether RUNX3 expression was associated
with the survival of patients with tongue SCC a Kaplan-Meier
survival analysis was conducted. The data revealed that nRUNX3
expression was associated with overall patient survival and
disease-free patient survival (P=0.008 and P=0.007, respectively,
log-rank test; Fig. 3E and F);
however, this was not the case for sRUNX3 (data not shown).
Univariate Cox proportional hazards regression model
was used to estimate the crude hazard ratios (HRs) of nRUNX3
expression or each clinicopathological variable on patient
survival. The log-rank test and univariate Cox regression analyses
revealed that nRUNX3 expression was significantly associated with
overall survival in patients with tongue SCC [HR 3.71; 95%
confidence interval (CI) 1.30–10.60; P=0.015; Table III]. To further validate the
prognostic value of nRUNX3, multivariate analysis was performed and
the significant factors are summarized in Table IV. The Cox regression model
indicated that nRUNX3 expression was an independent prognostic
marker for overall survival in patients with tongue SCC (HR 3.15;
95% CI 1.04–9.51; P=0.042, Table
IV).
| Table III.Univariate Cox regression analysis of
nRUNX3 expression and clinicopathological variables predicting the
survival of patients with tongue squamous cell carcinoma. |
Table III.
Univariate Cox regression analysis of
nRUNX3 expression and clinicopathological variables predicting the
survival of patients with tongue squamous cell carcinoma.
|
| (n=79 cases) |
|---|
|
|
|
|---|
| Variable | HR (95% CI) | P-value |
|---|
| Age (<60 vs. ≥60
years) | 1.55
(0.77–3.11) | 0.222 |
| Sex (male vs.
female) | 0.81
(0.40–1.65) | 0.567 |
| Tumor size (≤2 cm
vs. >2 cm) | 1.56
(0.78–3.12) | 0.210 |
| Lymph node
metastasis (N0 vs. N1/N2/N3) | 1.62
(0.79–3.31) | 0.190 |
| Histological grade
(I vs. II/III) | 1.21
(0.60–2.41) | 0.596 |
| Clinical stage (I
vs. II/III/IV) | 1.11
(0.56–2.24) | 0.762 |
| nRUNX3 expression
(negative vs. positive) | 3.71
(1.30–10.60) | 0.015 |
| Table IV.Multivariate Cox regression analysis
assessing the effects of covariates on overall survival in patients
with tongue squamous cell carcinoma. |
Table IV.
Multivariate Cox regression analysis
assessing the effects of covariates on overall survival in patients
with tongue squamous cell carcinoma.
|
| (n=79 cases) |
|---|
|
|
|
|---|
| Variable | HR (95% CI) | P-value |
|---|
| Age (<60 vs. ≥60
years) | 1.57
(0.76–3.23) | 0.219 |
| Sex (male vs.
female) | 0.83
(0.40–1.69) | 0.600 |
| Tumor size (≤2 cm
vs. >2 cm) | 1.84
(0.83–4.07) | 0.132 |
| Lymph node
metastasis (N0 vs. N1/N2/N3) | 3.91
(1.16–13.10) | 0.027 |
| Histological grade
(I vs. II/III) | 1.11
(0.48–2.58) | 0.803 |
| Clinical stage (I
vs. II/III/IV) | 0.22
(0.06–0.82) | 0.023 |
| nRUNX3 expression
(negative vs. positive) | 3.15
(1.04–9.51) | 0.042 |
Discussion
While the overall incidence of oral cancer has
barely altered in the last decade, the number of novel cases of
tongue SCC significantly increases each year, particularly among
young adults (3,20). Tongue SCC exhibits a more
aggressive phenotype, with a high rate of local lymph node
metastasis and recurrence following comprehensive therapy, compared
with other subtypes of oral cancer (2). However, the molecular mechanisms
underlying these aggressive behaviors remain unclear and the
prognosis of tongue SCC requires further evaluation.
The RUNX3 gene is located on chromosome 1p36, which
has been suggested to harbor numerous tumor suppressor genes that
are frequently deleted in various types of human cancer, including
oral SCC (21). Evidence has
suggested that RUNX3 is causally associated with carcinogenesis,
and its inactivation contributes to tumor metastasis by enhancing
cell migration and invasion in human cancer (6,22).
The RUNX3 gene may be inactivated by two mechanisms: i) Promoter
hypermethylation, which leads to gene silencing and the absence of
RUNX3 expression; and ii) protein mislocalization, which refers to
the cytoplasmic retention of RUNX3 protein in a nonfunctional form,
instead of normal nuclear localization. These two mechanisms may
affect the progression of a number of types of human cancer
(9,12,19).
Hypermethylation of the RUNX3 gene promoter is a common event in
oral SCC, including tongue SCC (17,23–25),
and is significantly associated with lymph node involvement and
tumor stage in tongue SCC (23).
Downregulation of RUNX3 protein expression and protein
mislocalization are additionally correlated with histological
grades in oral SCC (19).
Furthermore, cytoplasmic mislocalization of the RUNX3 protein has
been reported to be more frequent compared with the absence of
RUNX3 protein expression in oral SCC (19); however, has not been fully
investigated in tongue SCC. In tongue SCC tissue, RUNX3 has been
reported to be hypomethylated, whereas its mRNA expression is
increased (23). These findings
suggested that the function of RUNX3 in tongue SCC may be distinct
from other subtypes of oral SCC, although this remains to be fully
elucidated. The present study detected the protein expression
levels of RUNX3 protein in tongue SCC tissues and demonstrated that
protein expression was reduced compared with in paired
non-cancerous tissues. TMA results of samples obtained from
patients with tongue SCC demonstrated that 51.9% of cases exhibited
cytoplasmic staining of RUNX3, whereas only 17.7% cases exhibited
negative staining. These findings suggested that RUNX3 inactivation
in tongue SCC may be due to protein mislocalization, rather than
absence of expression.
The exact mechanism underlying RUNX3 protein
mislocalization has not been clearly elucidated; however, it has
been confirmed that RUNX3 protein cannot elicit tumor suppressive
activity when the protein is restricted to the cytoplasm (5). Transforming growth factor-β (TGF-β)
is a tumor-suppressing factor and an upstream molecule of RUNX3,
which can initiate RUNX3 protein translocation from the cytoplasm
into the nucleus (6). In gastric
cancer, it has been reported that the cytoplasmic retention of
RUNX3 increases tumorigenicity when TGF-β-induced nuclear
translocation of RUNX3 is impaired (9). Therefore, in the present study,
immunofluorescence and immunocytochemistry were performed to locate
the distribution of RUNX3 in tongue SCC cell lines. In agreement
with TMA results, SCC25 and Cal27 cells exhibited low RUNX3 protein
expression, which was predominately localized to the cytoplasm.
These results further suggested that protein mislocalization of
RUNX3 may serve an important role in the carcinogenesis of tongue
SCC. Notably, some tongue SCC cells exhibited nuclear staining,
whereas the majority of cells exhibited cytoplasmic staining. These
results indicated the complexity of RUNX3 function in tongue SCC,
which requires further elucidation. In previous studies, the
restoration of RUNX3 could potentially inhibit the malignant
behaviors of human cancer (9,13,14).
Therefore, it may be feasible to select RUNX3 as an antitumor
target.
Molecular abnormities caused by cancer metastasis
occur not only in tumor nests; however, additionally in the tumor
stroma. Cancer cells detach from the primary tumor, invade the
basement membrane and extracellular matrix, and transport within
the blood or lymphatic vessels in the surrounding tumor stroma,
finally arriving in the target organ to form metastasis foci.
Interactions between the tumor and surrounding tissue, which
consists of stromal cells, blood vessels and immune cells, are
vital to tumor growth and spread (26,27).
Expression of certain proteins or microRNAs in the tumor stroma may
be candidates as molecular biomarkers of prognosis (28,29).
Therefore, in the present study, nRUNX3 and sRUNX3 expression were
distinctly evaluated; to the best of our knowledge, this has not
been analyzed in previous studies. Inconsistent expression of RUNX3
was identified in tumor nests and stroma. Unlike nRUNX3,
cytoplasmic staining was not identified in sRUNX3. Positive sRUNX3
nuclear staining was observed in 50.6% of cases, which was mostly
distributed in the adjacent area between tumor nests and stroma. By
analyzing their association with clinicopathological variables, it
was revealed that nRUNX3 and sRUNX3 were significantly associated
with lymph node metastasis. In addition, negative nRUNX3
expression, but not sRUNX3, worsened the overall and disease-free
survival of patients. The univariate and multivariate Cox
regression analyses confirmed that negative nRUNX3 was associated
with poor prognosis, thus suggesting nRUNX3 may function as a
prognostic biomarker for tongue SCC.
Numerous studies have reported that RUNX3 serves as
an oncogene in head and neck SCC (HNSCC) (30,31).
However, functional mutation or protein mislocalization of RUNX3
has not been detected in HNSCC cells (31). In our previous study, it was
identified that RUNX3 serves a tumor suppressor role by inhibiting
cell migration, invasion and angiogenesis in oral SCC (18). As one subtype of oral SCC, the
protein expression levels of RUNX3 were detected in tongue SCC
tissues and cell lines. The results suggested that cytoplasmic
mislocalization of the RUNX3 protein was a common event in tongue
SCC. The findings of the present study additionally indicated that
nRUNX3 expression may be a potential prognostic biomarker for
tongue SCC. The limitations of the present study were the absence
of adjacent normal tissues paired with tongue SCC tissues for the
TMA analysis, and the limited number of fresh samples (n=3) used to
analyze the expression of RUNX3 in tumor and adjacent non-cancerous
tissues.
Acknowledgements
The authors would like to thank Professor Laikui Liu
from Jiangsu Key Laboratory of Oral Diseases, Affiliated Hospital
of Stomatology, Nanjing Medical University for his professional
suggestions for this article.
Funding
The study was funded by the Priority Academic
Program Development of Jiangsu Higher Education Institutions (grant
no. PAPD2014-37) and The Jiangsu Provincial Commission of Health
and Family Planning (grant no. Z201511).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
W-NZ and YZ collected and analyzed the oral squamous
cell carcinoma data of the patients. YD and W-NZ performed the
histological examination of the tissue microarray, and the in
vitro experiments. WZ and YZ evaluated the immunoreactions of
the tissue microarray and analyzed the results. YW, XS and JB
designed the study. W-NZ and YZ drafted the manuscript, and XS and
JB revised the manuscript. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The present study was performed under a protocol
approved by the Institutional Review Boards of the Affiliated
Hospital of Stomatology, Nanjing Medical University. All patients
provided written informed consent prior to the study.
Patient consent for publication
Written informed consent for the publication of
clinical data and accompanying images was obtained from the
patient, patient's guardian or next of kin prior to the study.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Scully C and Bagan J: Oral squamous cell
carcinoma: Overview of current understanding of aetiopathogenesis
and clinical implications. Oral Dis. 15:388–399. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Weatherspoon DJ, Chattopadhyay A,
Boroumand S and Garcia I: Oral cavity and oropharyngeal cancer
incidence trends and disparities in the United States: 2000–2010.
Cancer Epidemiol. 39:497–504. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ng JH, Iyer NG, Tan MH and Edgren G:
Changing epidemiology of oral squamous cell carcinoma of the
tongue: A global study. Head Neck. 39:297–304. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ghantous Y, Yaffi V and Abu-Elnaaj I: Oral
cavity cancer: Epidemiology and early diagnosis. Refuat Hapeh
Vehashinayim (1993). 3255–63. (71)2015.(In Hebrew). PubMed/NCBI
|
|
5
|
Hanai J, Chen LF, Kanno T, Ohtani-Fujita
N, Kim WY, Guo WH, Imamura T, Ishidou Y, Fukuchi M, Shi MJ, et al:
Interaction and functional cooperation of PEBP2/CBF with Smads.
Synergistic induction of the immunoglobulin germline Calpha
promoter. J Biol Chem. 274:31577–31582. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Subramaniam MM, Chan JY, Yeoh KG, Quek T,
Ito K and Salto-Tellez M: Molecular pathology of RUNX3 in human
carcinogenesis. Biochim Biophys Acta. 1796:315–331. 2009.PubMed/NCBI
|
|
7
|
Ito Y: Oncogenic potential of the RUNX
gene family: ‘Overview’. Oncogene. 23:4198–4208. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tonomoto Y, Tachibana M, Dhar DK, Onoda T,
Hata K, Ohnuma H, Tanaka T and Nagasue N: Differential expression
of RUNX genes in human esophageal squamous cell carcinoma:
Downregulation of RUNX3 worsens patient prognosis. Oncology.
73:346–356. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ito K, Liu Q, Salto-Tellez M, Yano T, Tada
K, Ida H, Huang C, Shah N, Inoue M, Rajnakova A, et al: RUNX3, a
novel tumor suppressor, is frequently inactivated in gastric cancer
by protein mislocalization. Cancer Res. 65:7743–7750. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Soong R, Shah N, Peh BK, Chong PY, Ng SS,
Zeps N, Joseph D, Salto-Tellez M, Iacopetta B and Ito Y: The
expression of RUNX3 in colorectal cancer is associated with disease
stage and patient outcome. Br J Cancer. 100:676–679. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yu GP, Ji Y, Chen GQ, Huang B, Shen K, Wu
S and Shen ZY: Application of RUNX3 gene promoter methylation in
the diagnosis of non-small cell lung cancer. Oncol Lett. 3:159–162.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lau QC, Raja E, Salto-Tellez M, Liu Q, Ito
K, Inoue M, Putti TC, Loh M, Ko TK, Huang C, et al: RUNX3 is
frequently inactivated by dual mechanisms of protein
mislocalization and promoter hypermethylation in breast cancer.
Cancer Res. 66:6512–6520. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bai J, Yong HM, Chen FF, Song WB, Li C,
Liu H and Zheng JN: RUNX3 is a prognostic marker and potential
therapeutic target in human breast cancer. J Cancer Res Clin Oncol.
139:1813–1823. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kim BR, Kang MH, Kim JL, Na YJ, Park SH,
Lee SI, Kang S, Joung SY, Lee SY, Lee DH, et al: RUNX3 inhibits the
metastasis and angiogenesis of colorectal cancer. Oncol Rep.
36:2601–2608. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chen H, Wang Z, Wang S, Zhang Z and Shi S:
Effect and mechanism of RUNX3 gene on biological characteristics of
human esophageal squamous cell carcinoma (ESCC). Med Oncol.
32:3572015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Mei PJ, Bai J, Liu H, Li C, Wu YP, Yu ZQ
and Zheng JN: RUNX3 expression is lost in glioma and its
restoration causes drastic suppression of tumor invasion and
migration. J Cancer Res Clin Oncol. 137:1823–1830. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Adelstein D, Gillison ML, Pfister DG,
Spencer S, Adkins D, Brizel DM, Burtness B, Busse PM, Caudell JJ,
Cmelak AJ, et al: NCCN guidelines insights: Head and neck cancers,
version 2.2017. J Natl Compr Canc Netw. 15:761–770. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zhou WN, Du YF, Bai J, Song XM, Zheng Y,
Yuan H, Zhang W, Zhang ZD and Wu YN: RUNX3 plays a tumor suppressor
role by inhibiting cell migration, invasion and angiogenesis in
oral squamous cell carcinoma. Oncol Rep. 38:2378–2386. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Gao F, Huang C, Lin M, Wang Z, Shen J,
Zhang H, Jiang L and Chen Q: Frequent inactivation of RUNX3 by
promoter hypermethylation and protein mislocalization in oral
squamous cell carcinomas. J Cancer Res Clin Oncol. 135:739–747.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Myers JN, Elkins T, Roberts D and Byers
RM: Squamous cell carcinoma of the tongue in young adults:
Increasing incidence and factors that predict treatment outcomes.
Otolaryngol Head Neck Surg. 122:44–51. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lefeuvre M, Gunduz M, Nagatsuka H, Gunduz
E, Al Sheikh Ali M, Beder L, Fukushima K, Yamanaka N, Shimizu K and
Nagai N: Fine deletion analysis of 1p36 chromosomal region in oral
squamous cell carcinomas. J Oral Pathol Med. 38:94–98. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Chen F, Liu X, Bai J, Pei D and Zheng J:
The emerging role of RUNX3 in cancer metastasis (Review). Oncol
Rep. 35:1227–1236. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Supic G, Kozomara R, Jovic N, Zeljic K and
Magic Z: Hypermethylation of RUNX3 but not WIF1 gene and its
association with stage and nodal status of tongue cancers. Oral
Dis. 17:794–800. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
de Freitas Cordeiro-Silva M, Stur E,
Agostini LP, de Podestá JR, de Oliveira JC, Soares MS, Mendonça EF,
Gouvea SA, Von Zeidler SV and Louro ID: Promoter hypermethylation
in primary squamous cell carcinoma of the oral cavity and
oropharynx: A study of a Brazilian cohort. Mol Biol Rep.
39:10111–10119. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zhang S, Feng XL, Shi L, Gong CJ, He ZJ,
Wu HJ and Ling TY: Genome-wide analysis of DNA methylation in
tongue squamous cell carcinoma. Oncol Rep. 29:1819–1826. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hynes RO: Metastatic potential: Generic
predisposition of the primary tumor or rare, metastatic variants-or
both? Cell. 113:821–823. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Lambert AW, Pattabiraman DR and Weinberg
RA: Emerging biological principles of metastasis. Cell.
168:670–691. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Hedbäck N, Jensen DH, Specht L, Fiehn AM,
Therkildsen MH, Friis-Hansen L, Dabelsteen E and von Buchwald C:
MiR-21 expression in the tumor stroma of oral squamous cell
carcinoma: An independent biomarker of disease free survival. PLoS
One. 9:e951932014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Shinriki S, Jono H, Ueda M, Obayashi K,
Nakamura T, Ota K, Ota T, Sueyoshi T, Guo J, Hayashi M, et al:
Stromal expression of neutrophil gelatinase-associated lipocalin
correlates with poor differentiation and adverse prognosis in oral
squamous cell carcinoma. Histopathology. 64:356–364. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kudo Y, Tsunematsu T and Takata T:
Oncogenic role of RUNX3 in head and neck cancer. J Cell Biochem.
112:387–393. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Tsunematsu T, Kudo Y, Iizuka S, Ogawa I,
Fujita T, Kurihara H, Abiko Y and Takata T: RUNX3 has an oncogenic
role in head and neck cancer. PLoS One. 4:e58922009. View Article : Google Scholar : PubMed/NCBI
|