Introduction
Chronic pain inadequately treated is a major public
health issue (1). This is
particularly relevant, when we are talking of supportive care in
cancer patients. Opioids are the most used analgesics for cancer
pain, but the clinical benefits of opioid analgesics are dependent
of substantial individual variations in the responses to opioids,
insufficient drug dosing and/or a high rate of adverse events. The
wide interindividual variability in sensitivity to opioids leads to
unpredictable clinical responses to opioid treatment and adverse
events, along with narrow therapeutic window and are still nowadays
an important problem (1,2).
To date, only a limited number of studies have
addressed the relationship between human genetic variations and
sensitivity to opioids; however there is growing evidence that
pharmacogenetic differences may impact in interindividual
variability in opioid response. Human genetic variation may
directly modulate opioids pharmacokinetic and pharmacodynamic
effects; candidate genes are sought in polymorphisms of drug
transporters, metabolizing enzymes or opioid receptors (1,2).
Cytochrome P450 (CYP) are enzymes located on the
smooth endoplasmic reticulum membranes of liver hepatocytes and
along the mucosal surface of the intestinal tract. The CYP system
can inactivate or activate a given drug (type I reactions) and is
responsible for glucuronidation and sulfation, connected with drug
excretion (type II). Along with CYP iso-enzyme 3A4 (CYP3A4), the
most important enzyme is CYP 2D6 (CYP2D6). She is involved in the
metabolism many drugs used in pain and palliative medicine (e.g.,
opioids, neuroleptics, antidepressants). More than 80 distinct
allelic variants for CYP2D6 are known, which leads to a wide
spectrum of metabolic capacity and phenotype diversity within
populations for several drugs like tramadol, dihydrocodeine,
codeine (3). Fentanyl is thought
to be predominantly metabolized in the liver by CYP3A4-mediated
N-dealkylation (less than 1% is metabolized by alkyl hydroxylation,
N-dealkylation or amide hydrolysis) (4). Ketamine is mainly metabolized by
CYP2B6 and CYP3A4 (5). Morphine is
metabolized to morphine-3-glucuronide (M3G) and
morphine-6-glucuronide (M6G) via glucuronidation by phase II
metabolism of UDP-glucuronosyl transferase 2B7 (UGT2B7). About 60%
of morphine is converted to M3G and 6–10% is converted to M6G. Both
metabolites are excreted in the urine. M6G is a very potent opioid
analgesic, which activates µ-opioid receptors, while M3G has no
opioid properties and has been proposed to be responsible for
neuroexcitatory effects, including allodynia, myoclonus and
seizures. Two variants of the UGT2B7 gene have been described, with
inconsistent results on their influence on morphine glucuronidation
and pain relief (6).
The opioid pharmacogenetic studies in cancer
patients have primarily focused on three genes: µ-opioid receptor
(OPRM), catechol-O-methyl transferase (COMT) and multidrug
resistance 1 gene (MDR-1) (7).
Mu-opioid receptors (MOR) receptors are the main
site of action of opioids. Recent genetic research shows that
genetic variations in µ-opioid receptor 1 (OPRM1) gene locus play
an essential role in inter-individual responses. This may explain
why some patients do need higher doses of opioid for pain relief,
translating into decreased morphine potency in pupil constriction
and experimental analgesia, or poor receptor signaling in
vitro (8). Numerous single
nucleotide polymorphisms (SNPs) in the mu opioid receptor have been
identified, but the majority of genetic association studies have
focused on the A118G polymorphism (A>G functional substitution
at locus 118,) which codes for a non-synonymous change in OPRM1
exon 1 (9,10).
Another line of evidence indicates that the
influence of COMT gene polymorphisms on pain has also been
investigated. It has been shown that the Val158Met polymorphism, a
common genetic variant in Caucasian populations, influences the
activity of the COMT enzyme. This enzyme, which metabolizes
dopamine, adrenaline and noradrenaline, is an important modulator
of dopaminergic and noradrenergic neurotransmission, known to play
a role in pain (11–13).
Furthermore, functional impairment of peripheral
blood morphine transporters (multi-drug resistance protein,
proteins 2 and 3; -MRP2 and MRP3 genes), and morphine transporters
through the blood-brain barrier, like ATP-binding cassette (ABC)
family of efflux transporters, may result in modification of
brain's morphine concentration (14).
There are a growing number of candidate genes for
genetic polymorphisms of potential clinical relevance (not all
referred in this paper). The aim of this study is to determine if
there is now enough evidence to make treatment recommendations
based on specific genomic profile in cancer pain patients. In the
future, a faster titration of opioid needs would be possible, with
less episodes of irruptive pain or persistent pain, fewer side
effects and thus better quality of life. We would probably have a
lower incidence of chronic pain. Identifying patients' subgroups
more susceptible to refractory pain or adverse symptoms would give
us the ability to anticipate cases of difficult pain control, with
better pain control, fewer visits and hospitalizations for
uncontrolled pain or adverse events and lower costs; pain control
could increase cost-effectiveness.
Materials and methods
A bibliographic survey was carried out in the
following databases: PubMed (NLM), Evidence Based Medicine
Guidelines and Google. Clinical guidelines, systematic reviews,
metaanalyzes and clinical trials, published until January 2018,
were searched using MeSH terms ‘cancer pain’, polymorphism,
genetic, gene polymorphism. Similar search strings were adapted for
the others databases. In Google, search was also conducted by
organization with particularly dedication to cancer pain issues.
Only guidelines in English, which were published and downloadable
from the web, were taken into consideration. Exclusion criteria in
the selection of articles were: papers without any reference to
polymorphism (or genetic variation) in the abstract, reporting drug
use in non-cancer pain or being related to nursing practice or
anti-cancer therapies or translational pain research (animal
models).
The American Family Physician's (AFP) Strength of
Recommendation Taxonomy (15) was
applied to classify levels of evidence and recommending strengths.
According to this taxonomy, the quality of the study is subdivided
into three Levels of Evidence (Level of Evidence 1: Good quality
studies, evidence-oriented decision; Level of Evidence 2: Limited
quality studies, patient-oriented evidence; Level of Evidence 3:
Other evidence) and the Strength of Recommendation in also divided
in three levels-(Strength of Recommendation A: consistent, evidence
patient-oriented; Strength of Recommendation B: Inconsistent or
limited quality, evidence oriented for the patient; Strength of
Recommendation C: consensus, evidence-oriented disease). The final
text has been reviewed and approved by all authors.
Results
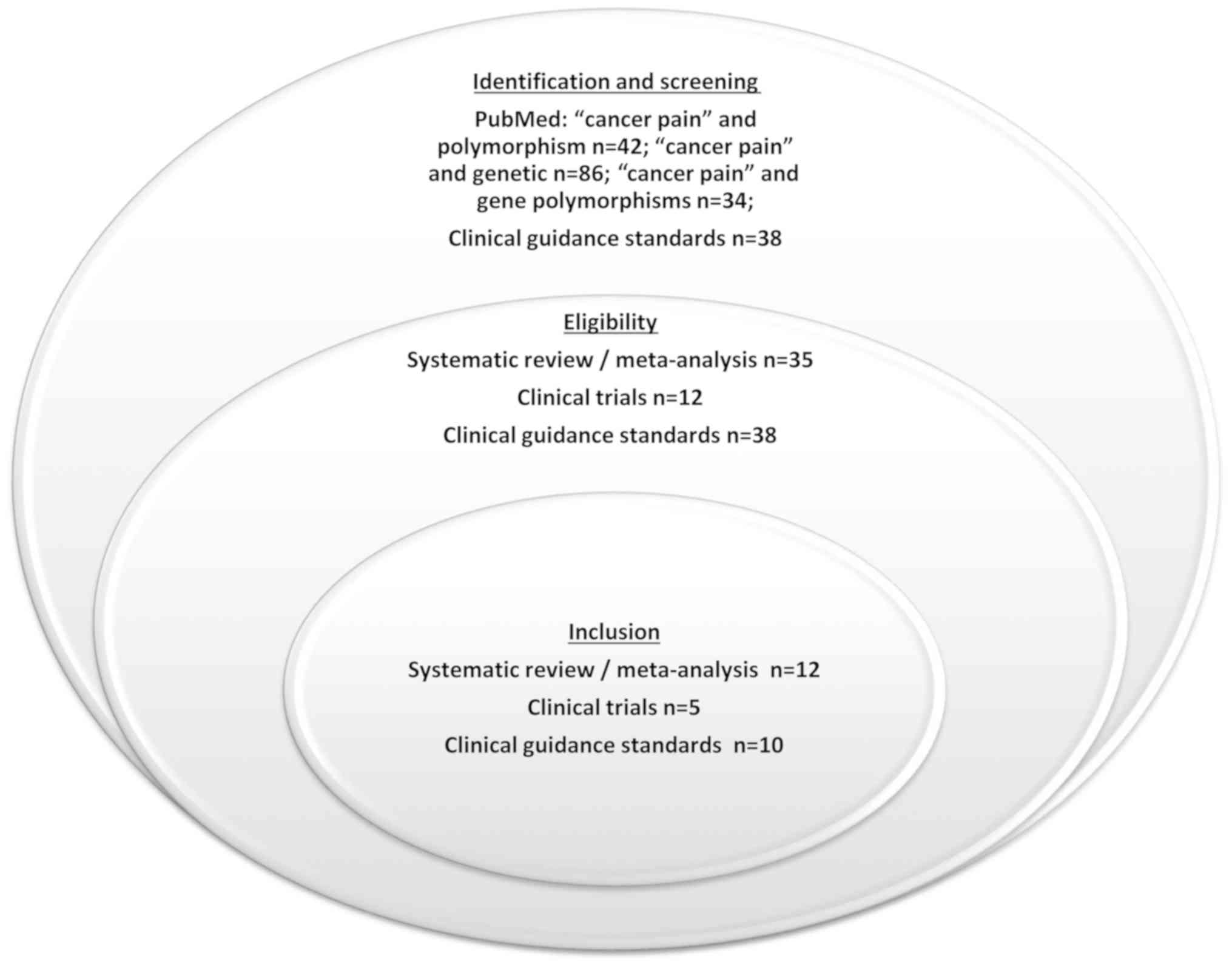
The search for polymorphism (42 papers) or genetic
(86 papers) or gene polymorphisms (34 papers) in patients with
‘cancer pain’ identified 35 systematic review and/or meta-analysis
and 12 clinical trials. More than half of the articles were
excluded because they did not concern systematic review and/or
meta-analysis and clinical trials or they did not meet the
inclusion/exclusion criteria (Fig.
1). For these analyses 12 systematic review and/or
meta-analysis and 5 clinical trials were selected. The search for
Clinical Guidance Standards found 10 guidelines with reference to
pain polymorphism or genetics of pain (from a total of 38 found in
our search).
Clinical guidance standards
We found at least 38 guidelines on supportive care
and pain but reference to pain polymorphism, or the need to search
for any particular polymorphism at the individual at level, was
absent in the great majority; some have a generic reference to this
subject.
The genetics associated with pain arises, as in the
position paper promoted by the European Pain Federation in January
2017 (2), as an explanation for
the marked inter-individual variability in responsiveness to
different opioids, both in terms of analgesic benefit and toxicity
(2,16). This paper refers to genetic
variability in µ-opioid receptors (central and peripheral), with
different binding affinities of the opioids, and additional k- and
δ-opioid receptors to explain the need for individualization of
pain treatment, both in terms of response to treatment and adverse
events. However, authors cite, without further specification, that
other molecular, pharmacological, genetic and phenotypic factors
may explain the variation in observed clinical responses (2).
The National Comprehensive Cancer Network (NCCN)
guidelines (January 2018) recognizes that different polymorphisms
in CYP2D6, as in some ethnic group, may justify the existence of
either slow or fast metabolizers of codeine (17). Codeine is a weak µ and δ-opioid
receptor agonist with little direct analgesic effect. The action of
the cytochrome P450 enzyme-CYP2D6-is necessary to convert the
prodrug into active metabolites (codeine-6-glucuronide, norcodeine,
morphine, morphine-3-glucuronide, morphine-6-glucuronide and
normorphine). The poor/slow metabolizers (five to ten per cent of
the population) will obtain reduced or no analgesic effects and the
hyper-metabolisers metabolizers (five to ten percent) may
experience more rapid morphine production with increased risk of
toxicity. There is considerable inter-ethnic variability in gene
encoding for CYP2D6 (17,18).
The European Palliative Care Research Collaborative
opioid guidelines project endorsed by MASCC (Multinational
Association of Supportive Care in Cancer, also refers that
approximately 8% of the European population are poor metabolizers
of codeine to morphine, with resulting diminished analgesic
efficacy. Also genetic polymorphisms, with impact in
O-demethylation (via CYP2D6) can lead to alterations in response to
tramadol in a similar way to codeine. The active metabolite,
O-desmethyltramadol, has a higher affinity to the µ-opioid
receptor, than the parent drug, however in vivo; production
seems to be slow with minimal clinically relevant accumulation
(19–21). Searching for this profile is not
done routinely, despite the reference in the NCCN and WHO
guidelines (17,22–24).
In addition to the analgesic effect, codeine is probably used more
often as antitussive than analgesic, in cancer patients (17,20–25).
These authors suggest that the great interindividual variation in
the amount and ratios of metabolite production may not be all
accounted for by known polymorphisms. For instance the CNS adverse
effects have been shown to occur even in the absence of significant
CYP2D6 activity, suggesting a potential role for metabolites other
than morphine in toxicity (17,20,21,25).
The World Health Organization (WHO) guideline
explains that both codeine and tramadol may be less analgesic in
poor metabolizers (22–24). Tramadol is also extensively
metabolized in the liver by demethylation, oxidation and
conjugation (2–4). The main active metabolite,
O-demethyl-tramadol (M1), is the result of the catalytic action of
CYP 2D6 and is two to four times more potent than the parent
compound. The poor metabolizers have 14-fold lower concentrations
of the active metabolite and may have less analgesic efficacy
(22–25). Schug et al (26) based on WHO guideline proposed in
Expert opinion-Pain management of the cancer patient-that
polymorphisms in CYP2D6 result in a range of metabolic patterns,
from ultrarapid to ultra-slow metabolizers of codeine, with some
patients showing no analgesic effect at all. This paper also refers
that genetic variability in morphine metabolism may have a role in
neurotoxic and hyperalgesic effects of M3G, but also with the
influence of genetic variants of the OPRM1 gene, encoding the
µ-opioid receptor (26).
The Centers for Disease Control and Prevention (CDC)
published the CDC Guideline for Prescribing Opioids for Chronic
Pain clarifying that equianalgesic dose conversions are only
estimates and do not account for individual variability in genetics
and pharmacokinetics. This fact is particularly relevant to
patients' members of racial and ethnic minority groups that can be
at risk for inadequate pain treatment (27).
Also the Canadian or Scottish guidelines support
that conversion ratios for opioids are subject to variations in
kinetics governed by genetics and other drugs. Even with the same
chronic pain syndrome, the underlying neurobiology will differ
between individuals, influencing analgesic response and side
effects (18,28). Studies into factors that contribute
to the inter-individual variation in response to different
treatments (clinical, genetic, pharmacokinetic, neurobiological)
and clinical biomarkers for predicting response to treatments are
still needed. Another factor that must be considered, when
assessing opioid responses, is that several opioids including
codeine, tramadol, oxycodone and hydrocodone are affected by
variations in metabolism, mediated by cytochrome P450 enzyme
CYP2D6, resulting in unpredictable effects in individuals (18,28).
Pharmacological Management of Cancer Pain in
Adults-National Clinical Guideline No. 9 was promoted by Ireland
experts and classified with level 5 of evidence (based on the
Centre for Evidence Based Medicine method of Oxford University) the
role of CYP2D6 enzyme inhibitors or genetic polymorphisms in
morphine sulphate production with reduced analgesic response. This
poor or absent analgesic effect of codeine can affect approximately
7% of Caucasian people, 3% of black people and 1% of Asian people
(29). Wide inter-individual
variability in opioid pharmacokinetics is influenced by genetic
variation but also by age, ethnicity and the presence of renal or
hepatic impairment (29,30). Further prospective research may
allow prediction of inter-individual response to different opioids
and better opioid prescribing (27).
Summary, we can say that the guidelines are divided
in 3 groups: One first group with reference to the route of
metabolization of cytochrome P450 enzyme CYP2D6; a second group
that's presents a generic reference to the impact of the
polymorphisms on pain treatment, without specifying any one; and a
last group (not exhaustively referred to in this work) that´s does
not present any reference to this matter.
Systematic review and/or
meta-analysis
The search identified 35 systematic review and/or
meta-analysis, but only 12 had direct reference to some specific
polymorphism (Table I). Three
reviews were excluded because they don't have any reference to
polymorphism (or genetic variation) in the abstract, five articles
was only available in Japanese, Chinese or German language and
three was reporting drug use in chronic non-cancer pain and the
others was related with nursing practice or anti-cancer therapies
or translational pain research (animal models). Data summarized in
Table I.
 | Table I.Systematic review and/or
meta-analysis. |
Table I.
Systematic review and/or
meta-analysis.
| Author, year | Title | Major
conclusions | Genotype
groups/reference SNP identification | Evidence level | (Refs.) |
|---|
| Kuip et al,
2017 | A review of factors
explaining variability in fentanyl pharmacokinetics; focus on
implications for cancer patients. | Patients with the
CYP3A5*3 gene single nucleotide polymorphism (*3*3) had a ~2-fold
higher fentanyl plasma concentration normalized by the measured
absorption rate when compared with patients with the wild-type
(*1*1) gene polymorphism and the patients with the heterozygous
(*1*3) gene polymorphism (further research is needed). | Enzymes: CYP3A4*22;
CYP3A5*3. Transporters: ABCB1 C1236T; SLCO1B1*a1 and
SLCO1B*15. | 1 | (4) |
| Andersen et
al, 2016 | Personalizing
supportive care in oncology patients using pharmacogenetic-driven
treatment pathways. | CYP2D6 metabolizes
codeine, tramadol, oxycodone and hydrocodone into their more potent
metabolites. In case of new, worsening or persisting pain the
CYP2D6 status should be determined. CYP2D6 ultra-rapid metabolizers
and poor metabolizers should avoid tramadol, codeine, hydrocodone
and oxycodone. Morphine dosing may require adjustment based on the
COMT and OPRM1 genotype, as patients with GG genotypes are less
sensitive to morphine's analgesic effect. | CYP2D6 genotype:
Ultrarapid metabolizer *1/*1×N; *1/*2×N; *2/*2×N; Extensive
metabolizer: *1/*1; *1/*2; *2/*2; *1/*9; *1/*10; *1/*41; *10/*10;
*41/*41; *1/*3; *1/*4; *1/*5; *1/*6; Intermediate metabolizer:
*4/*41; *5/*9; *4/*10; Poor metabolizer *3/*4; *4/*4; *5/*5; *5/*6.
COMT (rs4680)-also identified as G472A, G586A, Val108Met and
Val158Met. OPRM1 rs1799971. | 2 | (38) |
| Nielsen et
al, 2015 | Association Between
Human Pain-Related Analgesia: An Updated Review. | Genetic variation
can influence pharmacokinetics (such as drug transporters and
drug-metabolizing enzymes) and/or pharmacodynamics (such as opioid
receptor and catechol-O-methyltransferase enzymes). The methadone
dose was increased in carriers of the 2 copies of the AGCGC (wild
type) haplotype and of CGT, TTC, and TGT haplotypes composed of
ABCB1 C1236T, G2677T/A, and C3435T. Methadone doses are affected by
CYP2D6 phenotypes. Patients homozygous for the 118G allele (GG)
required more morphine than patients homozygous for the 118Aallele
(AA). | Morphine: ABCB1
C3435T; OPRM1 rs6912029, rs17999711 (A118G), rs589046, rs563649,
rs9479757, rs2075572 rs533586; OPRD1 rs10504151, rs7836120,
rs6473799, rs1365098, rs7016778, rs7824175, rs16918875, rs963549;
OPRK1 rs1042114, rs533123, rs419335, rs2236857, rs2234918; COMT
Val158Met, 11 SNPs. Tramadol/acetaminophen OPRM1 A118G. Methadone:
ABCB1 12 haplotypes; C3435T, 7 haplotypes; CYP2D6, CYP3A5, CYP2B6,
CYP2C9, CYP2C19. Various: ABCB1 C3435T. | 1 | (31) |
| De Gregori et
al, 2015 | OPRM1 receptor as
new biomarker to help the prediction of post mastectomy pain and
recurrence in breast cancer. | OPRM1 may be used
in near future to customize the opioid therapies, avoiding not only
opioid side effects but also the disease progression. | OPRM1 SNP rs1799971
and rs563649. | 3 | (44) |
| Hwang et al,
2014 | OPRM1 A118G gene
variant and postoperative opioid requirement: A systematic review
and meta-analysis. | The OPRM1 A118G
polymorphism was associated with interindividual variability in
postoperative responses to opioids. Carriers of the G-allele were
observed to exhibit higher opioid analgesic requirements. | Genotypes AA AG GG
(AA homozygotes and G-allele carriers). | 1 | (33) |
| Tammimäki et
al, 2012 |
Catechol-O-methyltransferase gene
polymorphism and chronic human pain: A systematic review and
meta-analysis. | Low COMT activity
has been associated with increased pain sensitivity in human pain
studies and may enhance opioid analgesia and exacerbate adverse
effects, at least in some cancer pains. | COMT single
nucleotide polymorphism rs4680-Val158Met | 1 | (36) |
| Leppert et
al, 2011 | CYP2D6 in the
metabolism of opioids for mild to moderate pain. | Experimental and
clinical studies demonstrated that. tramadol analgesia depends on
CYP2D6 activity and is not recommend in patients with the
ultra-rapid metabolizer genotype (duplication or multi-duplication
of gene-mostly CYP2D6*1/CYP2D6*2 alleles) and renal impairment | >80 distinct
allelic variants for CYP2D6 are known, including CYP2D6* 4,
CYP2D6*3, CYP2D6*6, CYP2D6*5, CYP2D6*1, CYP2D6*2, CYP2D6*10,
CYP2D6*17. | 3 | (3) |
| Droney et
al, 2011 | Evolving knowledge
of opioid genetics in cancer pain. | A number of
different variations in the gene coding for CYP2D6 have been
identified, with subsequent differential response to the codeine
and morphine. The opioid pharmacogenetic studies in cancer patients
that have shown some positive results have primarily focused
attention on three genes; OPRM, COMT and multidrug resistance 1
gene (MDR-1). | OPRM rs1799971
(A118G), rs563649; COMT rs4680 (Val158Met), rs7290221, rs5746849;
MDR-1 C3435T (rs1045642), GT2677A (rs2032582), C1236T (rs1128503);
SNPs in gene coding β-arrestin; SNPs in stat6 (MOR
transcription); SNPs in UGT2B7. | 2 | (7) |
| Shi et al,
2010 | Biological pathways
and genetic variables involved in pain. | Four categories
were identified for analgesic efficacy: Genes associated with
receptor interaction, modulation of opioid effects, metabolism, and
transport. Personalized analgesic treatment will require a more
complete understanding of the effects of genetic variants and
gene-gene interaction in response to pain and analgesics. | COMT: rs4680,
haplotype of SNPs in intron 1, haplotype of 11 SNPs; OPRM1:
rs17999711; IL-6 rs1800795; IL-8 rs4073; TNF-a rs1800629; ABCB1
rs1045642, rs2032582; CYP2B6 rs34830389, rs2279343; CYP2D6
rs35742686, rs3892097, rs5030655, rs5030867, rs1065852; UGT2B7 −840
G/A. | 2 | (32) |
| Andersen et
al, 2009 | Variation in the
COMT gene: implications for pain perception and pain
treatment. | A remarkable,
complex relationship between COMT genotypes or haplotypes and pain
phenotypes has been revealed. Met-allele (rs4680) was associated
with a reduced need for morphine; rs740603 was associated with
central side effects to morphine. | COMT gene: rs4680
(Val/Met), rs2075507, rs737866, rs7287550, rs174680, rs7290221,
rs5746849, rs740603,rs6269, rs6270A, rs4633, rs2239393, rs4680,
rs165631, rs174699, rs165728. | 2 | (45) |
| Slatkin et
al, 2009 | Opioid switching
and rotation in primary care: Implementation and clinical
utility. | The pharmacogenetic
factors influencing the opioid response and the mechanisms
underlying incomplete cross-tolerance are not yet fully understood.
Consequently, opioid switching and rotation remain largely
trial-and-error procedures, both in terms of patient selection and
with respect to implementation. | Opioid receptor
heterogeneity (eg. OPRM1) and other genetic variations: COMT,
CYP450 (CYP3A4, CYP3A5, CYP2D6), UGT, ABC1, solute carrier uptake
transporters (1A2, 1B3), melanocortin-1 (M1R) alleles,
β-arrestin-2 alleles. | 3 | (39) |
| Nagashima et
al, 2007 | Is there genetic
polymorphism evidence for individual human sensitivity to
opiates? | There are >100
polymorphisms identified in the human MOP (OPRM1) gene. These
polymorphisms may be associated with OPRM1 mRNA stability and
opiate sensitivity, including opiate analgesia, tolerance, and
dependence. | Referred to several
reference SNP identification numbers of polymorphisms of the OPR1
gene. | 2 | (35) |
These papers try to summarize and value the
functional impact of several genotype groups/reference SNP
identification. Principals polymorphism referred in this literature
review and the strength of recommendation for pain polymorphisms
are discussed below.
Clinical trials
The search identified 12 clinical trials, but only
five had direct reference to some specific polymorphism in cancer
patients (Table II). Clinical
trials were related with polymorphisms in CYP2B6 (metabolism of
ketamine), CYP2D6 (analgesia of tramadol) and UGT2B7 (morphine).
One trial was related with single nucleotide polymorphism at
nucleotide position 118 in the µ-opioid receptor gene. Another
reported pain outcomes and genetic variation was analyzed for 112
single nucleotide polymorphisms (SNPs) in 25 candidate genes
relevant for opioid efficacy. The choice of the candidate SNPs was
based on the expected clinical relevance of the variant alleles
(allele frequency >0.10), previously described associations or
putative functional effects related to pain and opioid
pharmacology. The relevance of this papers and main findings are
discussed below.
| Table II.Clinical trials. |
Table II.
Clinical trials.
| Author, year | Type of study and
the population | Intervention
(reference SNP identification) | Results | Evidence level | (Refs.) |
|---|
| Li et al,
2015 | Prospective cohort
study. n=49 chronic pain patients. | Impact of the
CYP2B6*6 allele (c.516G>T, rs3745274 and c.785A>G) on
ketamine plasma clearance and on adverse effects. | CYP2B6*6 allele is
associated with a substantial decrease in steady-state ketamine
plasma clearance with higher plasma concentrations and incidence of
adverse effects. | 2 | (5) |
| Fladvad et
al, 2012 | Prospective study,
case-control (patients randomly divided). n=2201 cancer pain
patients. | Pain outcomes and
genetic variation was analyzed for 112 single nucleotide
polymorphisms (SNPs) in 25 candidate genes relevant for opioid
efficacy. HTR3A rs2276302; HTR3C rs6807670; HTR3E rs7627615; HTR3C
rs6807362; HTR3D rs939334; COMT rs4646312; HTR4 rs4264931; ABCB1
rs1045642; TACR1 rs12713837; ARRB2 rs2036657; ARRB2 rs3786047;
ARRB2 rs7208257; HINT1 rs3852209; STAT6 rs167769; HTR3D rs6443930;
HRH1 rs346076; HTR3C rs6766410; HRH1 rs2606731; ADRA2A rs1800545;
OPRM1 rs9479757; ADRA2A rs11195419; DRD3 rs963468; DRD3 rs3773679;
DRD3 rs3732790; STAT6 rs3024971; GNAZ rs3788339; HTR3B rs1176744;
HTR3A rs1062613; DRD2 rs1125394. | None of the
examined SNPs exceeded P-values corrected for multiple testing for
any of the outcomes in the EPOS study, as previously shown for
opioid dose. A consensus is required if the information on genetic
variation is to be used in clinical decision making, for example,
as has been done previously for estimating warfarin dose, which is
based on clinical and genetic data. | 1 | (46) |
| Wang et al,
2006 | Prospective cohort
study. n=70 gastric cancer Chinese patients. | Impact of CYP2D6*10
C188T polymorphism/CYP2D6* 10 (100C>T) genotype on postoperative
analgesic effect of tramadol. | CYP2D6*10 allele
had a significant impact on analgesia with tramadol in the
immediate postoperative period of gastrectomy. | 2 | (47) |
| Chou et al,
2006 | Prospective cohort
study. n=80 female patients (hysterectomy). | Contributes to the
variability of morphine efficacy of the polymorphism (single
nucleotide polymorphism at nucleotide position 118 in the µ-opioid
receptor gene). | Cancer patients
homozygous for the 118G allele require higher doses of morphine to
relieve pain in postoperative period (no statistically significant
difference). | 2 | (34) |
| Holthe et
al, 2002 | Prospective cohort
study. n=70 cancer patients. | Investigated
whether the UGT2B7 H268Y and UGT1A1*28 polymorphisms contributed to
the variability in morphine glucuronide-to-morphine plasma ratios
among cancer patients undergoing analgesic therapy with
morphine. | UGT2B7 H268Y
polymorphism cannot account for the considerable variation in
glucuronide-to-morphine ratios. Contribution of UGT1A1 to the
formation of M3G appears to be of minor biological
significance | 2 | (48) |
Discussion
Revealing the relationship between genetic
variations and individual differences in sensitivity to opioids
will provide valuable information, for appropriate
individualization of opioid doses required for adequate pain
control. This evidence based review identifies the most promising
polymorphism in the cancer pain treatment. However, application of
this knowledge to clinical practice, creating easier to use
diagnostic tools is more difficult to achieve (31).
Several candidate genes have been used to provide
evidence for the genetic modulation of pain perception and response
to analgesics. However due to the limited number of patients in
prospective trials, the several number of genes and genetic
variants investigated and the lack of clinical randomized trials,
the level of evidence is in general low. Precision medicine and
personalized analgesic treatments will require a more complete
understanding of the effects of genetic variants and gene-gene
interactions in response to analgesics (32).
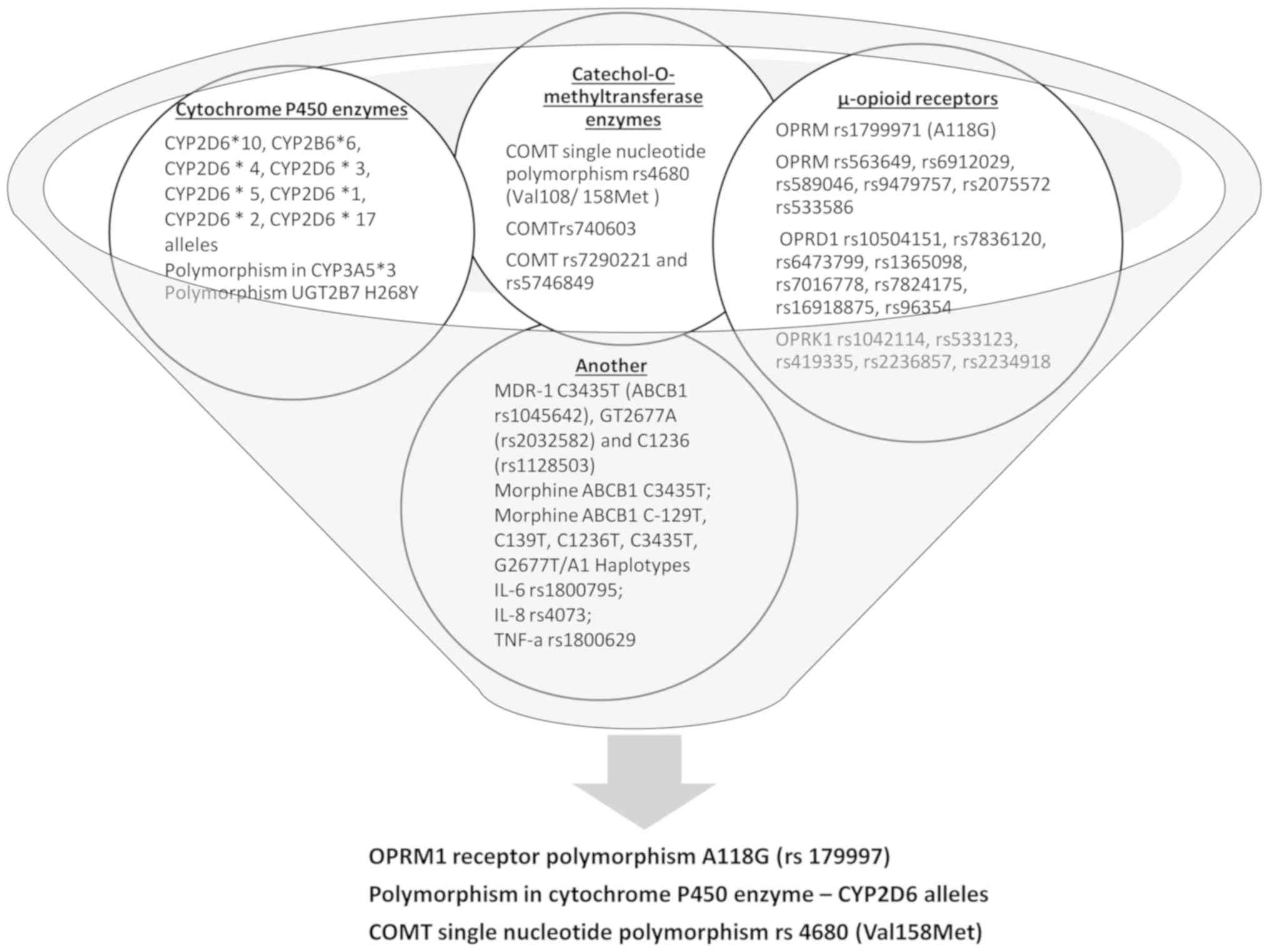
According to our evaluation, three groups of
polymorphism were highlighted in this research (Fig. 2; Table III). Firstly, the genetic
variation of the µ-opioid receptor may contribute to
interindividual differences in morphine consumption. In the future,
identifying single nucleotide polymorphisms of patients may provide
information to modulate the analgesic dosage of opioid for faster
achievement of satisfactory pain control (33,34).
The mu opioid peptide receptor (MOP) is the principal site of
pharmacologic actions for most clinically important opiate drugs,
but there are more than 100 polymorphisms identified in the human µ
opioid peptide receptor (OPRM1) gene. These polymorphisms
correlated with OPRM1 mRNA stability and opiate sensitivity,
including opiate analgesia, tolerance and dependence. Particularly
relevant is OPRM1 A118G polymorphism rs17999711 (33,34).
In addition to the A118G polymorphism, another functional SNP
(rs563649), which is located within an alternatively-spliced OPRM1
isoform (MOR-1K), has also has been the subject of several work
(7,8). More precise studies are need to
better understanding the relationship between gene polymorphisms
and opiate sensitivity, that will allowed personalized pain
treatment, by predicting opiate sensitivity and requirements for
each patient (35).
| Table III.Strength of recommendation for pain
polymorphisms. |
Table III.
Strength of recommendation for pain
polymorphisms.
| Polymorphism | Impact | Recommendation
level |
|---|
| µ-opioid receptors
(central and peripheral): OPRM1 polymorphism A118G (rs1799971) | Individualization
of pain treatment in terms of response to treatment and adverse
events. If OPRM1 G/G genotype consider initiating morphine at a
higher dose and/or more aggressive dose titration. May also
influence tramadol/acetaminophen analgesic response. | A |
| Polymorphism in
cytochrome P450 enzyme: CYP2D6 genotype (particularly CYP2D6*10
allele/C188T) | Several opioids
metabolisms are affected (codeine, tramadol, oxycodone,
hydrocodone, methadone). Poor metabolizers may be at risk of
treatment failure due to the inability to convert the parent drug
into its more active metabolite. Ultra-rapid metabolizers may be at
risk of treatment-related toxicities to supratherapeutic
concentrations of the more active metabolites. | A |
| Polymorphism in
catechol-O-methyltransferase (COMT) enzyme: Single nucleotide
polymorphism rs4680) (Val158Met) | Low COMT activity
(Val158Met) can increase opioid receptors and enhance opioid
analgesia and adverse effects. If COMT G/G genotype, consider
initiating morphine at a higher dose and/or more aggressive dose
titration. | B |
| Polymorphism in
cytochrome P450 enzyme: CYP2B6*6 allele (c.516G>T, rs3745274 and
c.785A>G) | Variations in
metabolism of ketamine. | C |
| Polymorphism in
cytochrome P450 enzyme: CYP3A5*3 gene single nucleotide
polymorphism | May influence
fentanyl pharmacokinetics. | C |
| Polymorphism in
ABCB1 (MDR1): C1236T, G2677T/A and C3435T | Methadone doses are
subject to ABCB1 genetic modulations. C3435T polymorphism (variant
T allele) may influence dose requirements for others opioids (e.g.
morphine). | C |
Secondly, polymorphism associated to the
metabolization process of morphine and other opioid drugs, manly
polymorphism of CYP enzymes, are nowadays very relevant in opioid
titration and rotation. Also referenced in the literature are
genetic polymorphisms in genes of uridine diphosphate
glucuronosyltransferase (UGT) enzymes. Ethnical and population
subgroups differences have to be taken in account. Prospective
trials of cancer patients and healthy controls are need, at a
national or regional level, to identify these subgroups (31). Catechol-O-methyltransferase (COMT)
is one of several enzymes that metabolize catecholamines. In human
studies, COMT genotype affects the efficacy of opioids in acute and
chronic pain in different settings (e.g. migraines, fibromyalgia,
musculoskeletal pain and cancer pain). Low COMT activity increases
opioid receptors and enhances opioid analgesia and adverse effects
in cancer pains. Pain animal models had elucidated the mechanism
behind these findings: COMT inhibitors are pronociceptive, except
for neuropathic pain. The complex network between adrenergic and
dopaminergic activity in different parts of the nociceptive system
may have a role in the action of low COMT activity (36).
Finally, ATP-binding cassette (ABC) family of efflux
transporters consists of around 50 human members. However ABCB1
(MDR1) is the most well characterized, coding for the
P-glycoprotein (P-gp) efflux transporter (31).
Among all, only two of them satisfied the proposed
criteria as A level of recommendation: OPRM1 polymorphism A118G
(rs1799971) and polymorphisms in cytochrome P450 enzyme-CYP2D6
(Table III). These polymorphisms
were studied in randomized trials and are extensively referred in
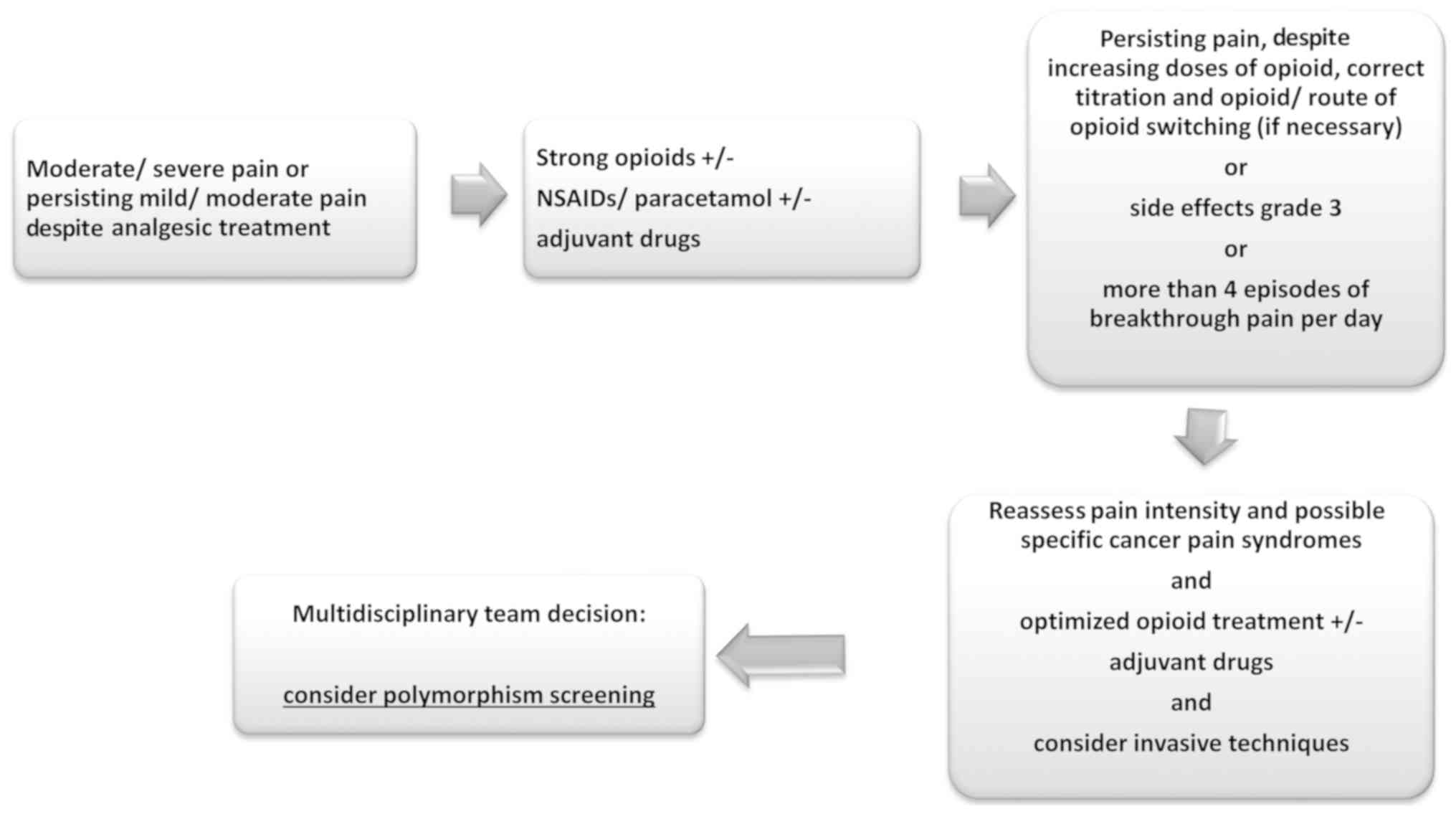
the systematic reviews and meta-analyzes. An algorithm of
management of pain and polymorphism screening is proposed in the
Fig. 3 (17,19,37).
Actual guidelines make some appointments about these genetic
variations, as responsively for interindividual differences in the
response to opioids, yet almost all without, without proposed a
real clinical setting to use them (17,38,39).
It is important to remind, that a combined effect of
SNPs in multiple genes is possible and its investigation, at the
same time, should remain a concern for prospective studies in this
field. And also take in consideration, the role of environmental
factor in interpatient variability in responses to opioids.
Information on type of SNPs (intronic, exonic, or intergenic) was
not present in the majority of these papers. Only two papers
refered to intronic SNPS in COMT (rs7290221, rs5746849, rs4646312,
rs6269 and rs740603). Usually intronic SNPs are not drivers, but
could be functional by changing the conformation of RNA and DNA
neighboring the SNPs (7,40–42).
The clinical utilization in daily practice is also
much dependent of the cost of time and laboratory resources of
these analyses (38). Pain is an
oncology emergence and pain drugs titration may be incompatible
with delayed laboratory tests and very expensive polymorphism
determinations. Frequently the allocation of technical and economic
resources to anti-cancer treatment limits the evolution of these
strategies for better individualized supportive and palliative care
treatment. Resources are currently limited and a global balance is
needed for fairer and more equitable treatment worldwide. The
identification of population or ethnic subgroups more prone to poor
pain control may lead to a strategy of lowering the costs of the
treatments. However, an investment in the development of laboratory
tests for the rapid identification of these polymorphisms and an
exhaustive training for health professionals is still an unmet
need.
One limitation of this work is the criteria for the
literature search, particularly the limitation to clinical
guidelines, systematic reviews, meta-analyzes and randomized
clinical trials in English. This evidence-based review is not a
systematic review, in the strict sense of the term, because they do
not include reviews and systematic reviews and they need a
different frame of search terms and analyses. Furthermore our goal
was to apply the levels of evidence and recommending strengths of
The American Family Physician's (AFP) Strength of Recommendation
Taxonomy (15).
There is considerable inter-ethnic variability in
gene encoding for CYP2D6. The differences between countries and the
ethnic variations may result in loss of date not published in
English or published in some national journals. Data from
retrospectives series or no randomized trials can have some
importance in this field and should be addressed in a future paper.
A statistical meta-analysis, with the strength of the associations
of the SNPs with pain score, is also a future project. Other aspect
to take in account, is the bias frequent found on this kind of
research. The papers summarized in the systems reviews and
meta-analyzes try to highlight differences in pain prevalence and
treatment conditioned by the polymorphism or other genetic
alterations, however it's difficult to eliminated the effect of
numerous others factors, with influence on human pain, and
specially cancer pain.
An algorithm of management of pain and polymorphism
screening is proposed and three groups of polymorphism are
considered of relevance for present utilization on clinical
practice. Genetic variation of the µ-opioid receptor may contribute
to interindividual differences in morphine consumption (with
recommendation grade A for OPRM A118G rs1799971) but there are more
than 100 polymorphisms identified in the human µ opioid peptide
receptor (OPRM1) gene. Polymorphism associated to the
metabolization process of morphine and other opioid drugs are
nowadays very relevant in opioid titration and rotation. Ethnical
and population subgroups difference have to be taken in account. A
recommendation grade A was awarded for polymorphism in cytochrome
P450 enzyme-CYP2D6). In human studies, COMT genotype affects the
efficacy of opioids in acute and chronic pain in different
settings, with recommendation grade B to COMT single nucleotide
polymorphism rs4680 (Val158Met).
Consistent data on pain polymorphism is nowadays
available, however with very little impact on clinical guidelines
and daily oncologist practice. Persisting pain, side effects grade
3 (NCI-CTCAE version 4.0) and breakthrough pain more than 4
episodes/day are point as criteria's to pain multidisciplinary team
discussion and consider polymorphism screening (43). Resources are currently limited and
a global balance is needed for fairer and more equitable treatment
worldwide. An investment in the development of laboratory tests for
the rapid identification of these polymorphisms is still an unmet
need.
Acknowledgements
The authors would like to thank Miss Luísa Ribeiro
from the library services of Francisco Gentil Portuguese Institute
of Oncology (Porto, Portugal).
Funding
The present study was supported as a part of a
project selected as an Internal Clinical Research Project of
Francisco Gentil Portuguese Institute of Oncology, Porto, Portugal
(grant nos. Bulletin 8/2017 and CI-IPOP 70/2017).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
CV obtained and assessed the data for this review,
proposed the levels of evidence and recommended strengths. RF, DP
and RM interpreted the results of the study, the levels of evidence
and the recommended strengths, and wrote the article. The final
manuscript was reviewed and approved by all authors.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
De Gregori S, Minella CE, De Gregori M,
Tinelli C, Ranzani GN, Govoni S, Allegri M and Regazzi M: Clinical
pharmacokinetics of morphine and its metabolites during morphine
dose titration for chronic cancer pain. Ther Drug Monit.
36:335–344. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
O'Brien T, Christrup LL, Drewes AM, Fallon
MT, Kress HG, McQuay HJ, Mikus G, Morlion BJ, Perez-Cajaraville J,
Pogatzki-Zahn E, et al: European pain federation position paper on
appropriate opioid use in chronic pain management. Eur J Pain.
21:3–19. 2017. View
Article : Google Scholar : PubMed/NCBI
|
|
3
|
Leppert W: CYP2D6 in the metabolism of
opioids for mild to moderate pain. Pharmacology. 87:274–285. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kuip EJ, Zandvliet ML, Koolen SL,
Mathijssen RH and van der Rijt CC: A review of factors explaining
variability in fentanyl pharmacokinetics; focus on implications for
cancer patients. Br J Clin Pharmacol. 83:294–313. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Li Y, Jackson KA, Slon B, Hardy JR, Franco
M, William L, Poon P, Coller JK, Hutchinson MR, Currow DC and
Somogyi AA: CYP2B6*6 allele and age substantially reduce
steady-state ketamine clearance in chronic pain patients: Impact on
adverse effects. Br J Clin Pharmacol. 80:276–284. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Smith HS: Opioid metabolism. Mayo Clin
Proc. 84:613–624. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Droney J, Riley J and Ross JR: Evolving
knowledge of opioid genetics in cancer pain. Clin Oncol (R Coll
Radiol). 23:418–428. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ross JR, Rutter D, Welsh K, Joel SP,
Goller K, Wells AU, Du Bois R and Riley J: Clinical response to
morphine in cancer patients and genetic variation in candidate
genes. Pharmacogenomics J. 5:324–336. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Diatchenko L, Robinson JE and Maixner W:
Elucidation of mu-Opioid Gene Structure: How genetics can help
predict responses to opioids. Eur J Pain Suppl. 5:433–438. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Klepstad P, Rakvåg TT, Kaasa S, Holthe M,
Dale O, Borchgrevink PC, Baar C, Vikan T, Krokan HE and Skorpen F:
The 118 A >G polymorphism in the human mu-opioid receptor gene
may increase morphine requirements in patients with pain caused by
malignant disease. Acta Anaesthesiol Scand. 48:1232–1239. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
De Gregori M, Garbin G, De Gregori S,
Minella CE, Bugada D, Lisa A, Govoni S, Regazzi M, Allegri M and
Ranzani GN: Genetic variability at COMT but not at OPRM1 and UGT2B7
loci modulates morphine analgesic response in acute postoperative
pain. Eur J Clin Pharmacol. 69:1651–1658. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Reyes-Gibby CC, Shete S, Rakvåg T, Bhat
SV, Skorpen F, Bruera E, Kaasa S and Klepstad P: Exploring joint
effects of genes and the clinical efficacy of morphine for cancer
pain: OPRM1 and COMT gene. Pain. 130:25–30. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Rakvag TT, Ross JR, Sato H, Skorpen F,
Kaasa S and Klepstad P: Genetic variation in the
catechol-O-methyltransferase (COMT) gene and morphine requirements
in cancer patients with pain. Mol Pain. 4:642008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ross JR, Riley J, Taegetmeyer AB, Sato H,
Gretton S, du Bois RM and Welsh KI: Genetic variation and response
to morphine in cancer patients: Catechol-O-methyltransferase and
multidrug resistance-1 gene polymorphisms are associated with
central side effects. Cancer. 112:1390–1403. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
SORT: The strength-of-recommendation
taxonomy. Am Fam Physician. 71:19–20. 2005.PubMed/NCBI
|
|
16
|
de Stoutz ND, Bruera E and Suarez-Almazo
M: Opioid rotation for toxicity reduction in terminal cancer
patients. J Pain Symptom Manage. 10:378–384. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Benedetti C, Brock C, Cleeland C, Coyle N,
Dubé JE, Ferrell B, Hassenbusch S III, Janjan NA, Lema MJ, Levy MH,
et al: NCCN practice guidelines for cancer pain. Oncology
(Williston Park). 14:135–150. 2000.PubMed/NCBI
|
|
18
|
Scottish Intercollegiate Guidelines
Network (SIGN). Management of chronic pain. Edinburgh: SIGN; 2013.
(SIGN publication no. 136). [December, 2013]. http://www.sign.ac.uk
|
|
19
|
Ripamonti CI, Santini D, Maranzano E,
Berti M and Roila F; ESMO Guidelines Working Group, : Management of
cancer pain: ESMO clinical practice guidelines. Ann Oncol. 23 Suppl
7:vii139–vii154. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Pigni A, Brunelli C, Gibbins J, Hanks G,
Deconno F, Kaasa S, Klepstad P, Radbruch L and Caraceni A: Content
development for EUROPEAN GUIDELINES on the use of opioids for
cancer pain: A systematic review and expert consensus study.
Minerva Anestesiol. 76:833–843. 2010.PubMed/NCBI
|
|
21
|
King S, Forbes K, Hanks GW, Ferro CJ and
Chambers EJ: A systematic review of the use of opioid medication
for those with moderate to severe cancer pain and renal impairment:
A European Palliative Care Research Collaborative opioid guidelines
project. Palliat Med. 25:525–552. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Burton AW and Cleeland CS: Cancer pain:
Progress since the WHO guidelines. Pain Pract. 1:236–242. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ventafridda V, Saita L, Ripamonti C and De
Conno F: WHO guidelines for the use of analgesics in cancer pain.
Int J Tissue React. 7:93–96. 1985.PubMed/NCBI
|
|
24
|
Schug SA, Zech D and Dörr U: Cancer pain
management according to WHO analgesic guidelines. J Pain Symptom
Manage. 5:27–32. 1990. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Ripamonti C and Giusti R: 21st expert
committee on the selection and use of essential medicines: Opioid
analgesics for cancer pain: fentanyl, methadone, tramadol-EML (EML
Opioids for cancer pain: A comparative overview). OMS. Available
from URL. Jan. 2018
|
|
26
|
Schug SA and Chandrasena C: Pain
management of the cancer patient. Expert Opin Pharmacother.
16:5–15. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Dowell D, Haegerich TM and Chou R: CDC
guideline for prescribing opioids for chronic pain-united states,
2016. JAMA. 315:1624–1645. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Busse JW, Craigie S, Juurlink DN, Buckley
DN, Wang L, Couban RJ, Agoritsas T, Akl EA, Carrasco-Labra A,
Cooper L, et al: Guideline for opioid therapy and chronic noncancer
pain. CMAJ. 189:E659–E666. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Lucey M; Guideline Development Group, :
Pharmacological Management of Cancer Pain in Adults-National
Clinical Guideline No. 9. Ireland. 2015.
|
|
30
|
Jara C, Del Barco S, Grávalos C, Hoyos S,
Hernández B, Muñoz M, Quintanar T, Meana JA, Rodriguez C and de Las
Peñas R: SEOM clinical guideline for treatment of cancer pain
(2017). Clin Transl Oncol. 20:97–107. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Nielsen LM, Olesen AE, Branford R,
Christrup LL, Sato H and Drewes AM: Association between human
pain-related genotypes and variability in opioid analgesia: An
updated review. Pain Pract. 15:580–594. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Shi Q, Cleeland CS, Klepstad P, Miaskowski
C and Pedersen NL; GeneQOL Consortium, : Biological pathways and
genetic variables involved in pain. Qual Life Res. 19:1407–1417.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Hwang IC, Park JY, Myung SK, Ahn HY,
Fukuda K and Liao Q: OPRM1 A118G gene variant and postoperative
opioid requirement: A systematic review and meta-analysis.
Anesthesiology. 121:825–834. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Chou WY, Wang CH, Liu PH, Liu CC, Tseng CC
and Jawan B: Human opioid receptor A118G polymorphism affects
intravenous patient-controlled analgesia morphine consumption after
total abdominal hysterectomy. Anesthesiology. 105:334–337. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Nagashima M, Katoh R, Sato Y, Tagami M,
Kasai S and Ikeda K: Is there genetic polymorphism evidence for
individual human sensitivity to opiates? Curr Pain Headache Rep.
11:115–123. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Tammimäki A and Männistö PT:
Catechol-O-methyltransferase gene polymorphism and chronic human
pain: A systematic review and meta-analysis. Pharmacogenet
Genomics. 22:673–691. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Kluetz PG, Chingos DT, Basch EM and
Mitchell SA: Patient-reported outcomes in cancer clinical trials:
Measuring symptomatic adverse events with the national cancer
institute's patient-reported outcomes version of the common
terminology criteria for adverse events (PRO-CTCAE). Am Soc Clin
Oncol Educ Book. 35:67–73. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Andersen RL, Johnson DJ and Patel JN:
Personalizing supportive care in oncology patients using
pharmacogenetic-driven treatment pathways. Pharmacogenomics.
17:417–434. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Slatkin NE: Opioid switching and rotation
in primary care: Implementation and clinical utility. Curr Med Res
Opin. 25:2133–2150. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Zhu G, Wang L, Guo H, Lu L, Yang S, Wang
T, Guo H, Wang H, Min J, Yang K, et al: DNA repair genes XRCC1 and
ERCC1 polymorphisms and the risk of sporadic breast cancer in Han
women in the Gansu Province of China. Genet Test Mol Biomarkers.
19:387–393. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Lu L, Katsaros D, Mayne ST, Risch HA,
Benedetto C, Canuto EM and Yu H: Functional study of risk loci of
stem cell-associated gene lin-28B and associations with disease
survival outcomes in epithelial ovarian cancer. Carcinogenesis.
33:2119–2125. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Lu L, Risch E, Deng Q, Biglia N, Picardo
E, Katsaros D and Yu H: An insulin-like growth factor-II intronic
variant affects local DNA conformation and ovarian cancer survival.
Carcinogenesis. 34:2024–2030. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Sloan PA, Donnelly MB, Schwartz RW and
Sloan DA: Cancer pain assessment and management by housestaff.
Pain. 67:475–481. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
De Gregori M, Diatchenko L, Belfer I and
Allegri M: OPRM1 receptor as new biomarker to help the prediction
of post mastectomy pain and recurrence in breast cancer. Minerva
Anestesiol. 81:894–900. 2015.PubMed/NCBI
|
|
45
|
Andersen S and Skorpen F: Variation in the
COMT gene: Implications for pain perception and pain treatment.
Pharmacogenomics. 10:669–684. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Fladvad T, Fayers P, Skorpen F, Kaasa S
and Klepstad P: Lack of association between genetic variability and
multiple pain-related outcomes in a large cohort of patients with
advanced cancer: The European Pharmacogenetic Opioid Study (EPOS).
BMJ Support Palliat Care. 2:351–355. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Wang G, Zhang H, He F and Fang X: Effect
of the CYP2D6*10 C188T polymorphism on postoperative tramadol
analgesia in a Chinese population. Eur J Clin Pharmacol.
62:927–931. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Holthe M, Klepstad P, Zahlsen K,
Borchgrevink PC, Hagen L, Dale O, Kaasa S, Krokan HE and Skorpen F:
Morphine glucuronide-to-morphine plasma ratios are unaffected by
the UGT2B7 H268Y and UGT1A1*28 polymorphisms in cancer patients on
chronic morphine therapy. Eur J Clin Pharmacol. 58:353–356. 2002.
View Article : Google Scholar : PubMed/NCBI
|