Introduction
Thyroid nodules are a frequent pathology, with a
lifetime occurrence risk in the general population estimated at
5–10% and a gender predilection since their prevalence is higher in
women (1). Furthermore, due to
technological advancement and increased availability of high
resolution ultrasound and other imaging modalities (e.g. incidental
findings on carotid or heart ultrasound, or routine scans), in
combination with the increased focus on preventive medicine and
improved access to healthcare resources, their prevalence seems to
be higher than estimated, with a recent study revealing thyroid
nodules in about 19–68% of randomly selected individuals (1).
In regards to treatment strategies, beyond surgery,
several non-invasive procedures have been developed including,
radiofrequency ablation, alcohol injection, high intensity-focused
ultrasound, or laser ablation. A minimally invasive procedure was
recently shown to be a safe and effective treatment for benign
thyroid nodules: ablation with monopolar radiofrequency (2). The last treatment approach is
performed with a 16 or 18 Gauge internally cooled radiofrequency
electrode after local anesthesia, which is able to treat
autonomously functional nodules (3). This leads to better results for
smaller and cystic nodules; post-procedural complications are
present only in 17% of patients (2). Other studies have shown various
results with mean decreases of 40–75% at 6 months (4,5) and
minimal complications in treating benign thyroid nodules with
radiofrequency ablation (5,6). Of
note key success factors are technical skill and patient selection
based on clinical evaluation (7).
Even though the vast majority (around 95%) of
thyroid nodules are benign (1,8), and
5% remnant thyroid malignancies are among the most successfully
treated endocrine cancers (2,9), a
novel, medical non-invasive treatment, which results in a decrease
in the size of thyroid nodules would be beneficial.
Materials and methods
Patients
Participants in this clinical study were consecutive
patients who presented for initial evaluation or follow-up of
thyroid nodules in the outpatient department of the National
Institute of Endocrinology (Bucharest, Romania) during
May-September 2018 and fulfilled the inclusion and exclusion
criteria.
Inclusion criteria were: Adult patients >18 years
old; agreement to participate in the study by signing the informed
consent form; euthyroid status [normal thyroid stimulating hormone
(TSH) and free thyroxine (fT4) values], no active dysfunctional
thyroid disease; benign thyroid nodule confirmed by FNAB (Bethesda
2); no previous thyroid surgery, thyroid ablation treatment,
substitution treatment with thyroid hormones; no steroid or
beta-blocker treatment; presence of one or more thyroid nodules
documented by ultrasound.
Exclusion criteria were: pediatric patients (<18
years old); diagnosis or suspicion of malignancy, including
thyroid; autoimmune disease, including Hashimoto; Wilson's disease;
hypo- or hyper-thyroidism; contraception with intrauterine device;
acute infection; known allergy to spirulina, curcumin or
Boswellia.
Thirty eight patients were enrolled and a total of
34 patients, 29 women and 5 men, completed the study. After being
informed about the objective and requirements of the study (blood
samples, ultrasound evaluations, supplement administration) with
possible risks and benefits, the participants signed the informed
consent form and were enrolled in the clinical study. Ethical rules
established by the National Institute of Endocrinology CI Parhon
according to the World Health Organisation guidelines were
observed.
Study design
A double-blind, placebo-controlled, cross-over
clinical trial was performed to assess the efficacy of the
spirulina-based supplement in decreasing the size of thyroid
nodules. The study population consisted of 34 consecutive cases
randomized initially to placebo (P) or active ingredients (AI).
There were three visits for each patient, noted as
V1 - initial visit at enrollment; V2 - intermediary visit, 6 weeks
post-administration of placebo (P) or active ingredients (AI); and
V3 - final visit, after another 6 weeks of administration of P or
AI. At each visit, each patient was tested for plasma TSH, fT4 and
copper (Cu) levels, by an independent laboratory and a thyroid
ultrasound was performed by an endocrinologist (DM) using the same
ultrasound machine. The nodule images and dimensions were printed
for comparison.
At V1, patients were randomly selected to receive
either AI or P, so that half of them (n=17) received P and the
other half (n=17) received AI. Subsequently at V2, the 17 patients
previously on P received AI, and 12 of the 17 patients previously
on AI received P, while the remaining 5 randomly chosen patients
continued to receive AI. Consequently at V3, 17 patients received
the sequence P-AI, 12 patients received AI-P, and 5 patients had
AI-AI. The study was registered on clinicaltrials.gov site with protocol ID ‘TiroNod’ and
ID number NCT03535974, and titled: ‘Efficacy of a spirulina
supplement for Amelioration of benign thYroid nodules (ESSAY)’.
Outcomes
The primary outcome of the study was a change in
size of the thyroid nodules and this is usually evaluated through a
comparison of the largest diameter of the nodules between
measurements via ultrasound. However, we have observed that there
are patients in which the largest diameter decreases while the
smallest diameter increases, and this variability may lead to
significant bias in comparisons. Therefore, for more consistent
results and comparisons we calculated the product of the largest
(D) and smallest (d) diameters of the nodules in the same incident
angle (S = D × d) and compared the resulting area of the nodules
measured at visits V1, 2, 3.
As secondary outcomes the serum levels of TSH, fT4
and Cu were assessed. The first two are considered standard
evaluations of the thyroid function, while the latter was chosen
for multiple reasons: i) spirulina is a significant source of Cu
along with other minerals and vitamins; ii) most serum Cu is bound
and transported by ceruloplasmin (10), and iii) while there is an excellent
correlation between serum Cu and ceruloplasmin, changes of Cu
plasma levels are faster than plasma ceruloplasmin levels, thus
serum Cu would provide more accurate information.
Statistical analysis
NCSS 16 software was used for data analysis.
Quantitative data were expressed as mean ± standard deviation (SD).
Paired sample t-test was used for comparisons of two groups (AI and
P). Pearson's correlation was used to assess correlations between
specific variables. Wald Z test for proportions was used for
comparing differences in outcomes between two groups. One-way ANOVA
test with the Tukey and Bonferroni post-hoc was used to compare
values of TSH, fT4 and Cu. α=0.05, and P<0.05 indicated
statistical significance.
Treatment
The active treatment administered was a combination
of spirulina, curcumin and Boswellia extracts, 400-50-50 mg
per capsule, which were prepared alongside matching placebo
capsules by DVR Pharm and BioNovative SRL. Patients were instructed
to take two capsules twice daily, about 30 min before breakfast and
lunch. Any adverse reactions were to be reported to the
investigator.
Spirulina is the common generic name of about 15
species from two types of monocellular microalgae (Spirulina and
Arthrospira), the most common being Arthrospira
platensis (11), which grows
naturally in freshwater and saltwater on all continents and in most
climates, optimally in an alkaline milieu (pH 9.5–12.0). It was
used as the only source of nutrition in some areas in Africa for
more than 1 month at a time and its first documented use was in
China around 2,000 years ago even during periods of famine
(12). It has a very high protein
content: 40–65% of dry mass depending on species and conditions of
growth/cultivation (13), and
contains all essential amino acids, minerals (Fe, K, Na, Ca, P, I,
Mg, Zn, Cu, Se, Mn, Cr) and vitamins (carotenoids 5 mg/g vitamins
B1, B2, B3, B6, B12, folate, biotin, pantothenic acid, vit K1, K2),
gamma linolenic acid, chlorophyll and phycocyanin, making it a
complete food source. Alongside this remarkable composition it has
important quantities of antioxidants, such as superoxide dysmutase
(360 UI/g), zeaxanthin (3 mg/g), and vitamin E (14).
Curcumin, a natural extract from the roots of
Curcuma longa, has also been in use for centuries in Asia
for various ailments. It is a potent anti-inflammatory substance
with pleiotropic actions, including antioxidant and metabolic
modulation. Its effects are well studied, with multiple clinical
trials showing benefits in arthritis, inflammatory bowel disease,
prediabetes, and even in early stages of neoplastic disease
(15). A recent meta-analysis on
15 randomized clinical trials shows that curcumin downregulates
inflammation and oxidation products by reducing levels of IL-6,
hs-CRP, and MDA (16).
Boswellia is also a potent anti-inflammatory
molecule, which blocks the NFkB pathway and modulates the activity
of regulatory and effector T cells (17). Together with curcumin it was shown
to inhibit production of inflammatory cytokines Il-6, IL-8, TNF-α
and reactive oxygen species (18,19).
Results
Patients
A total of 38 patients were enrolled of whom 34
patients, 29 women and 5 men, aged 53.44±12.63 years, completed the
study and were evaluated for the primary outcome - the size of the
thyroid nodules evaluated by ultrasound at 1st (initial), 2nd
(intermediate) and 3rd (final) patient visits. These 34 patients
were also tested for serum TSH, fT4 and Cu.
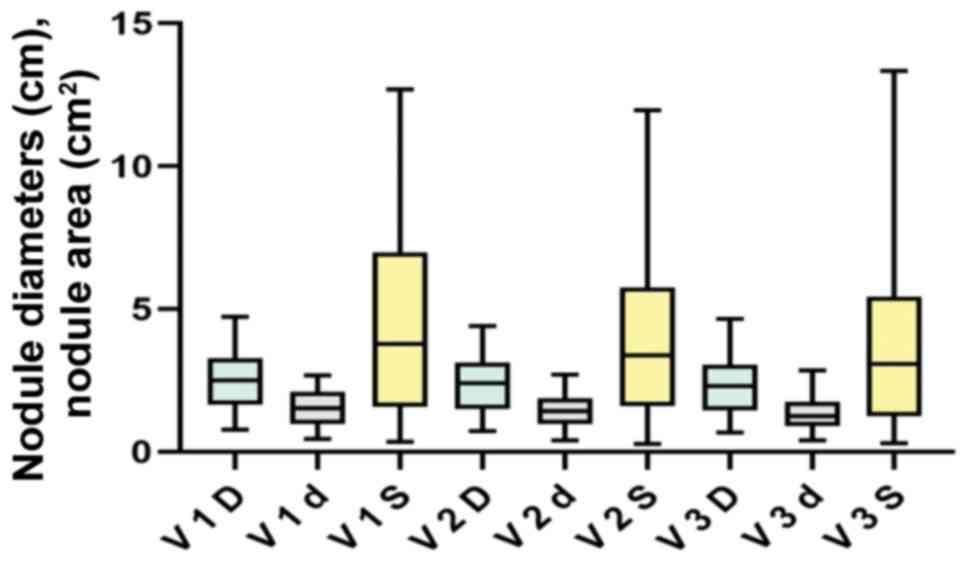
The overall reduction in the measured surface of the
thyroid nodules for all the 34 study participants, calculated as
the mean percentage decrease in the surface of nodules, was
20.3%±19.18% (SD). For all 34 patients, mean initial nodule area at
initial visit (V1 S) was 4.38±3.14 cm2; at 2nd visit (V2
S) mean nodule area and SD was: 3.87±2.79 cm2; and at
3rd visit (V3 S) mean nodule area and SD was 3.53±2.84
cm2.
Thyroid nodule size and
modifications
From the total of 34 patients who completed the 3
ultrasound evaluations, 29 patients (85.29%) had decreases in the
areas of thyroid nodules of 5% or more at the end of the study, and
22 patients (64.7%) had decreases of 10% or more of the thyroid
nodule area after 3 months.
One patient had insignificant decrease in nodule
area (0.21%), and 4 patients had increases in the size of the
nodules of 1.66, 2.36, 5.13 and 23.81%, respectively, at the final
ultrasound assessment (Table
I).
 | Table I.Percentage change from initial vs.
final area of thyroid nodules. |
Table I.
Percentage change from initial vs.
final area of thyroid nodules.
| Initial vs. final
area decrease % | <0
(increase) | ~0 (unchanged) | 5–9.9%
(decrease) | 10–19.9%
(decrease) | 20–49.9%
(decrease) | 50-99%
(decrease) |
|---|
| No. of
patients | 4 | 1 | 7 | 7 | 12 | 3 |
Patients were also grouped according to the initial
area of the nodules and their modifications at V2 and V3.
Table II
summarizes the modifications in nodule areas and shows an increase
in the number of patients with nodule areas of <6 cm2
at study visits 2 and 3 compared to V1 due to a gradual decrease in
nodule areas. Patients with larger thyroid nodules (>6
cm2) were the most dynamic group, their number
decreasing from V1-V2-V3 to 11-7-5, respectively.
| Table II.Number of patients at V1, V2, V3,
grouped by nodule area. |
Table II.
Number of patients at V1, V2, V3,
grouped by nodule area.
| Initial nodule
surface / no. of patients | 0.1–0.99
cm2 | 1–2.99
cm2 | 3–5.99
cm2 | 6–8.99
cm2 | >9
cm2 |
|---|
| Visit 1 | 4 | 10 | 9 | 8 | 3 |
| Visit 2 | 5 | 10 | 12 | 5 | 2 |
| Visit 3 | 6 | 9 | 14 | 3 | 2 |
Nodule size and visits
A graphic comparison of the effects of all patients
at the three study visits is given in Fig. 1, which shows that the decrease of
the mean areas of the nodules between the three visits were
statistically significant: for V1 S vs. V2 S the paired sample
t-test has P=0.00006; for V2 S vs. V3 S the paired sample t-test
has P=0.04182; and for V1 S vs. V3 S paired sample t-test has
P=0.00008.
A comparison of the effects of the active substance
vs. placebo on decreasing the surface of thyroid nodules showed
that after the initial administration of the placebo and active
substances, the mean decrease with AI was 19.88±15.55%, while with
the placebo the decrease was less, 9.31%±14.29%. The two-sided
t-test for the two groups had a t value of 2.03, and the difference
between placebo and active substances was marginally statistically
significant (P=0.047).
Consequently, we used two additional statistical
tests: the Wald Z test to compare the proportion of patients with
modifications in nodule areas, grouped in AI vs. P and also tested
both the equal variance and Aspin-Welch variants for the difference
of means ± SD between the AI and P groups.
Decrease in thyroid nodules area after
active substances and placebo
The difference in the proportion of patients with
decreased thyroid nodule areas on active substances vs. placebo
groups was directly increased with each visit and the number of
patients on AI vs. P; it achieved statistical significance at V3
vs. V1 (P=0.033); statistically significant results were obtained
by comparing the mean ± SD of nodule areas in AI and P groups at
V3-V1 (P=0.027) and V2-V1 (P=0.017), but not V3-V2 (P=0.16),
probably because the AI effect was still present in patients taking
P in the sequence AI-P (Table
III).
| Table III.Decrease in thyroid nodules area
after active substances and placebo. |
Table III.
Decrease in thyroid nodules area
after active substances and placebo.
| Mean ± SD
decrease | Active
substance | Placebo | Statistical
significance | Total active +
placebo |
|---|
| V2 - V1,
cm2 | 0.784±0.708 | 0.238±0.444 |
P=0.017a | 0.511±0.645 |
| V3 - V2,
cm2 | 0.499±1.069 | 0.094±0.612 | P=0.16a | 0.343±0.944 |
| V3 - V1,
cm2 | 0.611±0.933 | 0.178±0.515 |
P=0.027a | 0.854±1.108 |
| Patients nb V2 vs.
V1 | 16/17 | 13/17 | P=0.14b |
29/34 |
| Patients nb V3 vs.
V2 | 18/22 | 6/12 |
P=0.051b | 23/34 |
| Patients nb V3 vs.
V1 | 34/39 | 19/29 |
P=0.033b | 30/34 |
Comparing the overall effects of the placebo and the
active substances on all administrations (39 active substances, 29
placebo, total 68 sequences in 34 patients, Fig. 2), we have observed that the
administration of the active substances (n=39) was followed by a
mean decrease in nodule areas of 0.611 cm2±0.933 (SD),
while placebo administration (n=29) was followed by a mean decrease
of 0.178 cm2±0.515 (SD). Testing for statistical
significance between the two groups (active and placebo) at V3
versus V1 with t-test for means and standard deviation, there was a
mean difference of 0.433 cm2, which is statistically
significant both when calculated with the equal variance t-test
(standard error of the difference of 0.192, P=0.027) and the
unequal variance Aspin-Welch test (standard error of the difference
of 0.177, P=0.017) (Table
III).
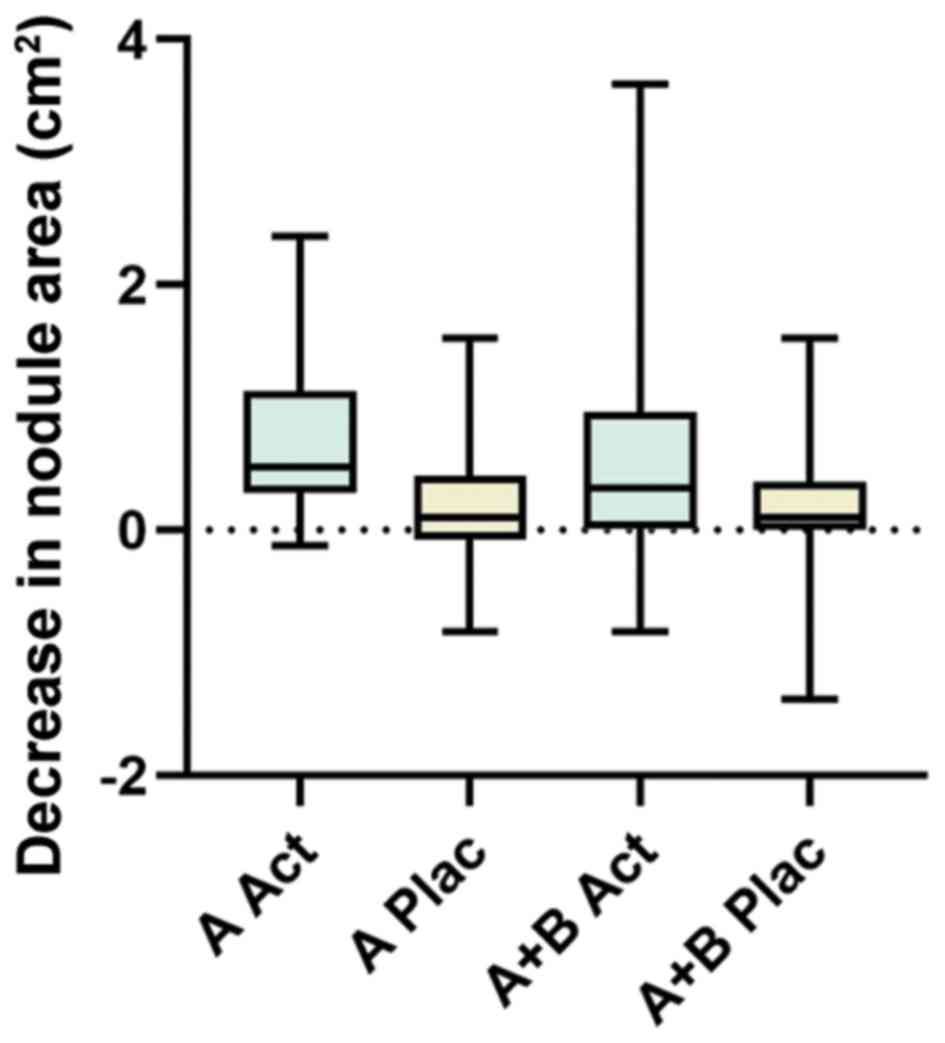 | Figure 2.The figure graphically represents the
significant data from Table III,
comparing the means, min and max values nodule areas in the AI
(Act) and P (Plac) groups after the initial 6 week administration
of AI or P (V2-V1, noted ‘A’) and after 12 weeks of AI or P (V3-V1,
noted ‘A+B’, A being the initial 6 weeks, B the final 6 weeks of
study). As noted in Table III,
in the ‘B’ period of the study (V3-V2) the mean nodule areas in the
AI vs. P groups were not statistically significant. A Act, A Plac
(n=17), A+B Act (n=39), A+B Plac (n=29). |
Based on these data it is evident that the active
combination is effective in reducing the size of the thyroid
nodules, even though it was administered for only 6 weeks out of
the total of 3 months.
Values of TSH, fT4 and Cu at the three
visits
Beyond efficacy, we have also monitored the
influence of treatment on thyroid function and the correlation with
Cu levels. To determine whether the active substances or the
placebo had a significant effect on thyroid function, we compared
the respective values of TSH and fT4 for all 3 visits (visit 1 vs.
2, visit 1 vs. 3 and 2 vs. 3) with the one-way ANOVA test and the
Tukey and Bonferroni post-hoc tests. There was no statistically
significant difference between the respective values of TSH or fT4
in the initial, intermediary or final visits. A similar result was
obtained when comparing the levels of serum Cu between the 3
visits; there were no significant differences between the
respective values (Table IV).
| Table IV.Values of TSH, fT4 and Cu at the
three visits, and ANOVA test values. |
Table IV.
Values of TSH, fT4 and Cu at the
three visits, and ANOVA test values.
| Visit and test
type | V1 TSH | V2 TSH | V3 TSH | V1 fT4 | V2 fT4 | V3 fT4 | V1 Cu | V2 Cu | V3Cu |
|---|
| Number tested | 34 | 34 | 32 | 33 | 34 | 32 | 33 | 33 | 31 |
| Mean | 1.50 | 1.37 | 1.30 | 1.18 | 1.18 | 1.196 | 127.65 | 127.13 | 128.38 |
| SD | 1.27 | 1.11 | 0.96 | 0.17 | 0.17 | 0.16 | 21.55 | 21.34 | 16.26 |
| ANOVA V1-V2-V3 | F-ratio =0.28472,
P=0.75 | F-ratio =0.06792,
P=0.93 | F-ratio =0.03162,
P=0.96 |
To verify the interdependence of the four variables
measured in this study: nodule surface, TSH, fT4 and Cu levels, we
calculated the Pearson's correlation indices and found that the
strongest correlation was between the decrease in nodules surface
and TSH levels at visits 2 and 3: Δ S2-S3 and Δ TSH2 - TSH3,
Pearson's correlation =0.52, P=0.002. There was also a significant
inverse correlation of serum Cu and TSH modifications between the
initial and final visits: Pearson's correlation of Δ Cu V1-V3 and Δ
TSH V1-V3 was r=−0.3885; with P=0.033 (data not shown).
Adverse effects
Four patients withdrew from the study before
completion. Three of them reconsidered participation due to
personal reasons, while one patient stopped one week
post-administration of the study substances, because of development
of a rash on the trunk and upper portions of limbs, while on
multiple medications. Following investigation, it was revealed that
the type of substance administered to the patient was the
placebo.
No other adverse effects were recorded on the study
participants for either the active substances or the placebo.
Discussion
The link between thyroid function and ceruloplasmin,
the most important Cu-based enzyme, was observed a few decades ago,
with a significant elevation of serum ceruloplasmin being observed
in patients on oral contraceptives together with an increase in
thyroxine binding index, while free thyroxine levels were unchanged
(20). Similarly, in male rats
estradiol elevated ceruloplasmin levels, while testosterone and
thyroid hormones inhibited this action (21). Furthermore, it was shown that
administration of L-thyroxine suppresses the stimulation of
ceruloplasmin by estrogen administration (22). Opposite modifications of
ceruloplasmin levels in hypo- and hyper-thyroid patients, in tandem
with thyroid function, as well as oxidation status
(malonyldialdehyde) and uric acid levels were observed by a
Romanian team (23). New direct
links between ceruloplasmin, oxidative stress and inflammation were
recently shown with TNF-related apoptosis-inducing ligand (TRAIL)
down-regulating ceruloplasmin expression in inflammation (24), and modulation of TNF-α-induced
neutrophil apoptosis by ceruloplasmin (25). Low levels of ceruloplasmin were
shown in a hypothyroid patient with Hashimoto thyroiditis (26).
Recent findings have shown that thyroid hormones
increase serum Cu levels by stimulating the synthesis of
ceruloplasmin in the liver as reflected in the mRNA levels, and
this action is abolished in cases of hyperthyroidism associated
with receptor resistance to thyroid hormones (27). In addition, the ratio of serum Cu
and selenium was proposed as an indirect marker for receptor
resistance to thyroid hormones. Stimulation of hepatic
ceruloplasmin mRNA by thyroxine and dexamethasone was previously
shown in rats (28). It was also
found that a Cu-deficient diet increases the levels of serum free
triiodothyronine but not fT4 in rats (29); similarly a strong link between
serum T3 and Cu was demonstrated in rat pups (30). Cu and Zn levels in serum and tissue
are modulated by thyroid hormones as shown by
thyro-parathyroidectomy and T4 replacement in rat. Interestingly,
it was seen that ceruloplasmin is present in follicular carcinoma
and absent in adenomas (31–33).
Further differences in the oxidative and inflammatory processes
involved in benign and malignant thyroid nodules versus normal
thyroid tissue (hypoxia-inducible factor-1, complement factor D,
matrix metalloprotease 1, Von Willebrand Factor - were shown in
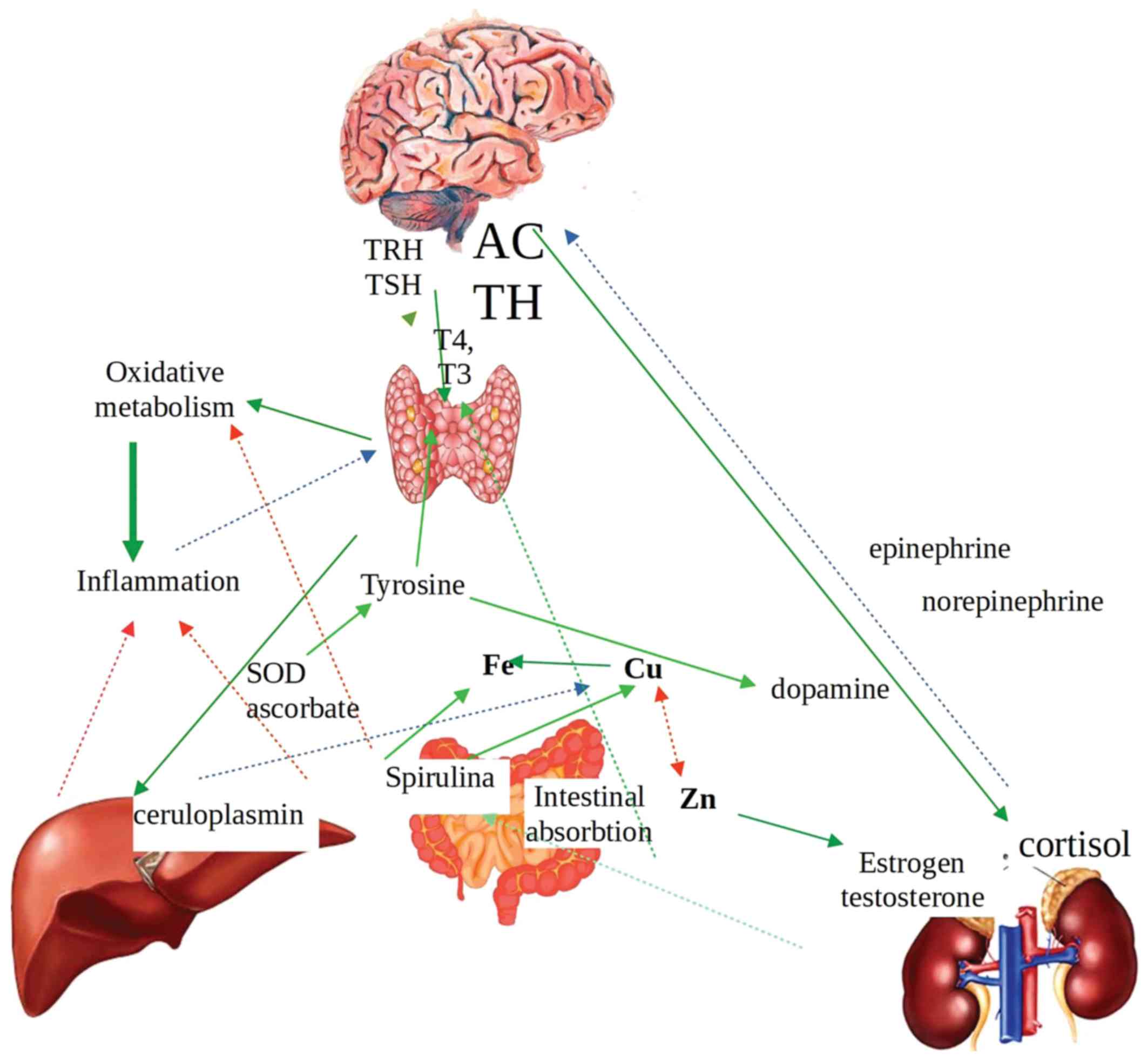
different studies (34) The
interrelations between thyroid hormones, ceruloplasmin, adrenal
hormones and important metabolic processes are presented in
Fig. 3.
Before administration of the indicated
spirulina-curcumin-Boswellia combination, a thorough
evaluation by an DM (with or without a thyroid ultrasound) should
be performed, in order to establish euthyroid status, exclude
patients with suspicion of malignancy, acute infection, autoimmune
disease, Wilson's disease, and monitor possible associations with
contraceptives or other simultaneous medical treatments.
In summary, the combination of
spirulina-curcumin-Boswellia is effective in reducing the
size of benign thyroid nodules and can be safely administered in
the doses used in the presented clinical study. The mechanism by
which the decrease of the nodule size is facilitated, is probably
linked to the anti-inflammatory effects, the improvement of the
antioxidant status and the ceruloplasmin actions. However,
additional studies are needed in order to elucidate these
associations, which may also provide important insights into the
pathogenesis of thyroid nodules.
Acknowledgements
Not applicable.
Funding
This study was financed by a grant received by The
Bio-Forum Foundation from DVR Pharm SRL and BioNovativ SRL which
intend to manufacture and bring to market the
spirulina-curcumin-boswellia combination under the name
“TiroDren”.
Availability of data and materials
The data sets used and/or analyzed during the
current study are available from the corresponding author on
reasonable request.
Authors' contributions
FS, DM and CB participated in data collection and
analysis. FS, GZP, AT and DAS participated in the design of the
study. FS, DM and GZP participated in the writing of the
manuscript. FS, AT and CB participated in data interpretation. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
All participants provided written informed consent
for the whole study. The study observed the ethical rules on
clinical studies established by the National Institute of
Endocrinology CI Parhon (Bucharest, Romania) according to the World
Health Organisation guidelines.
Patient consent for publication
Not applicable.
Competing interest
DAS is the Editor-in -Chief for the journal, but had
no personal involvement in the reviewing process, or any influence
in terms of adjudicating on the final decision, for this article.
The other authors declare that they have no competing interests.
Bio-Forum Foundation from DVR Pharm SRL and BioNovativ SRL intend
to manufacture and bring to market the spirulina-curcumin-boswellia
combination under the name ‘TiroDren’.
References
|
1
|
Haugen BR, Alexander EK, Bible KC, Doherty
GM, Mandel SJ, Nikiforov YE, Pacini F, Randolph GW, Sawka AM,
Schlumberger M, et al: 2015 American thyroid association management
guidelines for adult patients with thyroid nodules and
differentiated thyroid cancer: The American thyroid association
guidelines task force on thyroid nodules and differentiated thyroid
cancer. Thyroid. 26:1–133. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Burman KD and Wartofsky L: CLINICAL
PRACTICE. Thyroid Nodules. N Engl J Med. 373:2347–2356. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bernardi S, Stacul F, Michelli A, Giudici
F, Zuolo G, de Manzini N, Dobrinja C, Zanconati F and Fabris B:
12-month efficacy of a single radiofrequency ablation on
autonomously functioning thyroid nodules. Endocrine. 57:402–408.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cesareo R, Palermo A, Pasqualini V,
Simeoni C, Casini A, Pelle G, Manfrini S, Campagna G and Cianni R:
Efficacy and safety of a single radiofrequency ablation of solid
benign non-functioning thyroid nodules. Arch Endocrinol Metab.
61:173–179. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wu W, Gong X, Zhou Q and Chen X and Chen
X: Ultrasound-guided percutaneous microwave ablation for solid
benign thyroid nodules: Comparison of MWA versus control group. Int
J Endocrinol. 2017:97240902017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yue W, Wang S, Wang B, Xu Q, Yu S, Yonglin
Z and Wang X: Ultrasound guided percutaneous microwave ablation of
benign thyroid nodules: Safety and imaging follow-up in 222
patients. Eur J Radiol. 82:e11–e16. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Dobnig H and Amrein K: Monopolar
radiofrequency ablation of thyroid nodules: A prospective Austrian
single-center study. Thyroid. 28:472–480. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Durante C, Costante G, Lucisano G, Bruno
R, Meringolo D, Paciaroni A, Puxeddu E, Torlontano M, Tumino S,
Attard M, et al: The natural history of benign thyroid nodules.
JAMA. 313:926–935. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Hay ID, Thompson GB, Grant CS, Bergstralh
EJ, Dvorak CE, Gorman CA, Maurer MS, McIver B, Mullan BP, Oberg AL,
et al: Papillary thyroid carcinoma managed at the Mayo Clinic
during six decades (1940–1999): Temporal trends in initial therapy
and long-term outcome in 2444 consecutively treated patients. World
J Surg. 26:879–885. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Twomey PJ, Viljoen A, House IM, Reynolds
TM and Wierzbicki AS: Relationship between serum copper,
ceruloplasmin, and non-ceruloplasmin-bound copper in routine
clinical practice. Clin Chem. 51:1558–1559. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Habi b, M Ahsan B, Huntington T and Hasan
MA: A review on culture, production and use of Spirulina as food
for humans and feeds for domestic animals and fish. In: FAO
Fisheries and Aquaculture Circular No.1034. Food and Agriculture
Organization of the United Nations; Rome, Italy: 2008, PubMed/NCBI
|
|
12
|
Spolaore P, Joannis-Cassan C, Duran E and
Isambert A: Commercial applications of microalgae. J Biosci Bioeng.
101:87–96. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Becker EW: Micro-algae as a source of
protein. Biotechnol Adv. 25:207–210. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kent M, Welladsen HM, Mangott A and Li Y:
Nutritional evaluation of Australian microalgae as potential human
health supplements. PLoS One. 10:e01189852015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Perrone D, Ardito F, Giannatempo G,
Dioguardi M, Troiano G, Lo Russo L, DE Lillo A, Laino L and Lo
Muzio L: Biological and therapeutic activities, and anticancer
properties of curcumin. Exp Ther Med. 10:1615–1623. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tabrizi R, Vakili S, Akbari M, Mirhosseini
N, Lankarani KB, Rahimi M, Mobini M, Jafarnejad S, Vahedpoor Z and
Asemi Z: The effects of curcumin-containing supplements on
biomarkers of inflammation and oxidative stress: A systematic
review and meta-analysis of randomized controlled trials. Phytother
Res. 33:252–262. 2019. View
Article : Google Scholar
|
|
17
|
Beghelli D, Isani G, Roncada P, Andreani
G, Bistoni O, Bertocchi M, Lupidi G and Alunno A: Antioxidant and
ex vivo immune system regulatory properties of Boswellia
serrata extracts. Oxid Med Cell Longev. 2017:74680642017.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Governa P, Marchi M, Cocetta V, De Leo B,
Saunders PTK, Catanzaro D, Miraldi E, Montopoli M and Biagi M:
Effects of Boswellia Serrata Roxb. and Curcuma longa
L. in an in vitro intestinal inflammation model using immune cells
and Caco-2. Pharmaceuticals (Basel). 11:E1262018. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kizhakkedath R: Clinical evaluation of a
formulation containing Curcuma longa and Boswellia
serrata extracts in the management of knee osteoarthritis. Mol
Med Rep. 8:1542–1548. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Schenk H, Haralambus I, Leb G, Pickel H
and Goebel R: The effect of oral contraceptives on levels of
thyroid hormone, blood coagulation and ceruloplasmin. MMW Munch Med
Wochenschr. 119:941–944. 1977.(In German). PubMed/NCBI
|
|
21
|
Schreiber V and Pribyl T: Effect of
interaction of oestrogen, testosterone and thyroid hormones on the
serum ceruloplasmin level in rats. Physiol Bohemoslov (2). 129–137.
1977.
|
|
22
|
Schreiber V, Pribyl T and Jahodová J:
Reactions of hypothalamic ascorbic acid, serum ceruloplasmin and
the adenohypophysis to oestradiol: Inhibition by L-thyroxine.
Physiol Bohemoslov. 29:11–20. 1980.PubMed/NCBI
|
|
23
|
Dumitriu L, Bartoc R, Ursu H, Purice M and
Ionescu V: Significance of high levels of serum malonyl dialdehyde
(MDA) and ceruloplasmin (CP) in hyper- and hypothyroidism.
Endocrinologie. 26:35–38. 1988.PubMed/NCBI
|
|
24
|
Tisato V, Gallo S, Melloni E, Celeghini C,
Passaro A, Zauli G, Secchiero P, Bergamini C, Trentini A,
Bonaccorsi G, et al: TRAIL and ceruloplasmin inverse correlation as
a representative crosstalk between inflammation and oxidative
stress. Mediators Inflamm. 2018:96295372018. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Golenkina EA, Viryasova GM, Galkina SI,
Gaponova TV, Sud'ina GF and Sokolov AV: Fine regulation of
neutrophil oxidative status and apoptosis by ceruloplasmin and its
derivatives. Cells. 7:E82018. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Valenzise M, Porcaro F, Zirilli G, De Luca
F, Cinquegrani M and Aversa T: Hypoceruloplasminemia: An unusual
biochemical finding in a girl with Hashimoto's thyroiditis and
severe hypothyroidism. Pediatr Med Chir. 40:2018, https://doi.org/10.4081/pmc.2018.179 View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Mittag J, Behrends T, Nordström K, Anselmo
J, Vennström B and Schomburg L: Serum copper as a novel biomarker
for resistance to thyroid hormone. Biochem J. 443:103–109. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Fitch CA, Song Y and Levenson CW:
Developmental regulation of hepatic ceruloplasmin mRNA and serum
activity by exogenous thyroxine and dexamethasone. Proc Soc Exp
Biol Med. 221:27–31. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kralik A, Kirchgessner M and Eder K:
Concentrations of thyroid hormones in serum and activity of hepatic
5′ monodeiodinase in copper-deficient rats. Z Ernahrungswiss.
35:288–291. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Bastian TW, Lassi KC, Anderson GW and
Prohaska JR: Maternal iron supplementation attenuates the impact of
perinatal copper deficiency but does not eliminate
hypotriiodothyroninemia nor impaired sensorimotor development. J
Nutr Biochem. 22:1084–1090. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Song B: Immunohistochemical demonstration
of epidermal growth factor receptor and ceruloplasmin in thyroid
diseases. Acta Pathol Jpn. 41:336–343. 1991.PubMed/NCBI
|
|
32
|
Kondi-Pafiti A, Smyrniotis V, Frangou M,
Papayanopoulou A, Englezou M and Deligeorgi H: Immunohistochemical
study of ceruloplasmin, lactoferrin and secretory component
expression in neoplastic and non-neoplastic thyroid gland diseases.
Acta Oncol. 39:753–756. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Vaideeswar P, Pandit AA, Khilnani PH and
Powar HS: Differentiation of follicular adenoma and carcinoma of
thyroid by immunohistochemical demonstration of ceruloplasmin.
Indian J Pathol Microbiol. 37:165–169. 1994.PubMed/NCBI
|
|
34
|
Wang Q, Shen Y, Ye B, Hu H, Fan C, Wang T,
Zheng Y, Lv J, Ma Y and Xiang M: Gene expression differences
between thyroid carcinoma, thyroid adenoma and normal thyroid
tissue. Oncol Rep. 40:3359–3369. 2018.PubMed/NCBI
|