Introduction
Intertrochanteric fractures encountered by
orthopedic surgeons most commonly occur in the elderly population
(1). Complications of
intertrochanteric fractures, such as nonunion and delayed healing,
are not common during fracture healing due to the good blood supply
and excellent cancellous bone in the intertrochanteric area
(2). However, complications
resulting in pain, functional disability, psychological barriers
and an economic burden may occur in patients with intertrochanteric
fractures. To date, there have been few studies concerning primary
intertrochanteric nonunions and their prevention (1,3,4).
Although a number of methods for predicting the progress of
fracture healing exist, diagnostic methods at a molecular level are
lacking. Bone biochemical markers are likely to be of particular
interest, since they reflect the metabolic states of osteoblasts
and osteoclasts (5). Changes in
these markers may reflect the molecular basis of fracture
healing.
Receptor activator NF-κB (RANK), receptor activator
NF-κB ligand (RANKL) and the osteoprotegerin (OPG) molecular system
play important roles in the biology of osteoblasts and osteoclasts
(6). RANK, a member of the tumor
necrosis factor receptor superfamily, is a main activator of the
transcription factor NF-κB, and acts as a receptor for RANKL in a
signal transduction pathway. RANKL is secreted by osteoblasts;
following binding to RANK on the surface of preosteoclasts, RANKL
stimulates the activation and development of osteoclasts. The
soluble protein OPG is also a member of the tumor necrosis factor
receptor superfamily, and is secreted by many cell types, such as
the liver, heart, spleen, kidney cells and osteoblasts. OPG
inhibits bone resorption by inhibiting the interaction between
RANKL and RANK (7–10).
The RANKL/OPG system is a major signaling pathway
that regulates the differentiation and function of osteoblasts and
osteoclasts (11). RANKL, which is
a cytokine, is synthesized and secreted by osteoblasts and promotes
bone resorption. Following binding to RANKL, OPG inhibits bone
resorption caused by osteoclasts and increases bone formation
(12,13). Therefore, a number of studies have
suggested that the balance between RANKL and OPG regulates bone
resorption and formation (14–18).
However, the changes in RANKL and OPG that occur during fracture
healing in elderly patients with intertrochanteric fractures, as
well as the importance of the RANKL/OPG ratio, have not yet been
elucidated.
In the present study, the changes of serum RANKL and
OPG levels in elderly patients with intertrochanteric fractures
were investigated over time, and were compared with the respective
levels in healthy control subjects. These measurements were
analyzed to investigate the roles of RANKL, OPG and the RANKL/OPG
ratio in elderly patients with normal intertrochanteric fracture
healing, and to determine the significance of the RANKL/OPG ratio
in elderly patients with intertrochanteric fractures.
Patients and methods
Study subjects
The study group included 36 patients with
intertrochanteric fractures, with a mean age of 69.0 years (range,
65–79 years). All patients were treated between January 1, 1998 and
January 1, 2005 in the Department of Orthopedics, The Luhe Teaching
Hospital of the Capital Medical University. All patients had no
systemic diseases and were admitted to the hospital immediately
after injury. Surgery was performed on all patients with
intertrochanteric fractures by the same group of surgeons. After
surgery, all the patients underwent serial radiography to evaluate
bone formation. All the fractures were healed 16–26 weeks following
surgery. The control group consisted of 30 healthy subjects with a
mean age of 71.0 years (range, 65–81 years). The study was approved
by the Research Ethics Committees of our hospital, and informed
consent was obtained from all study subjects.
Measurement of serum RANKL and OPG
levels
Peripheral blood samples (20 ml) were obtained from
the 36 patients with intertrochanteric fractures within the first
few hours of admission to hospital (at baseline), as well as at 4,
8, and 12 weeks following injury. Additionally, 20 ml peripheral
blood were obtained from normal control subjects at baseline and
after 4, 8 and 12 weeks. Serum was extracted from the blood samples
in the morning and was immediately centrifuged. All the specimens
were stored at −80°C until analyzed.
A sandwich enzyme-linked immunosorbent assay (ELISA;
Immundiagnostik, Bensheim, Germany) was used to assess RANKL levels
in the serum samples. Firstly, the biotin anti-RANKL detection
antibody (sc-377079; Santa Cruz Biotechnology, Inc., Santa Cruz,
CA, USA) and the serum sample were pipetted into the wells of the
ELISA plate. When human RANKL is present in the serum sample, it
binds the recombinant OPG (sc-358754, Santa Cruz Biotechnology)
precoated onto the wells and constitutes a sandwich with the
detection antibody. In order to remove nonspecifically bound
material, a streptavidin-horseradish peroxidase conjugate was added
to the wells following washing. After removing the unbound
conjugate by washing, the substrate tetramethylbenzidine was added
to the wells. RANKL levels were measured by reading the substrate
on a standard ELISA plate reader at 450 nm. The detection limit was
1.63 pg/ml. The intra-assay coefficient of variation (CV) was 2–4%
for the serum RANKL measurements, and the inter-assay CV was
5–8%.
A sandwich ELISA method was also used to assess OPG
levels in the serum samples. This assay contained two antibodies
against OPG; the biological activity of recombinant human OPG was
neutralized by the antibodies. The detection antibody was a goat
polyclonal anti-human OPG antibody labeled with biotin (sc-8468;
Santa Cruz Biotechnology, Inc.), where during manufacture the goat
was immunized with human recombinant OPG (sc-361910Rx; Santa Cruz
Biotechnology, Inc.). The serum levels of OPG were determined on
the basis of the protein concentration, according to the
manufacturer’s instructions (sc-363390; Santa Cruz Biotechnology,
Inc.). The detection limit was 2.53 pg/ml. The intra-assay CV for
OPG measurements was 7–9%, and the inter-assay CV was <8%.
Statistical analysis
Statistical analyses were performed using SPSS 13.0
(SPSS, Inc., Chicago, IL, USA). Data were expressed as the mean ±
standard deviation (SD) and evaluated using Student’s t-test.
P<0.05 was considered to indicate a statistically significant
difference.
Results
Serum RANKL and OPG levels
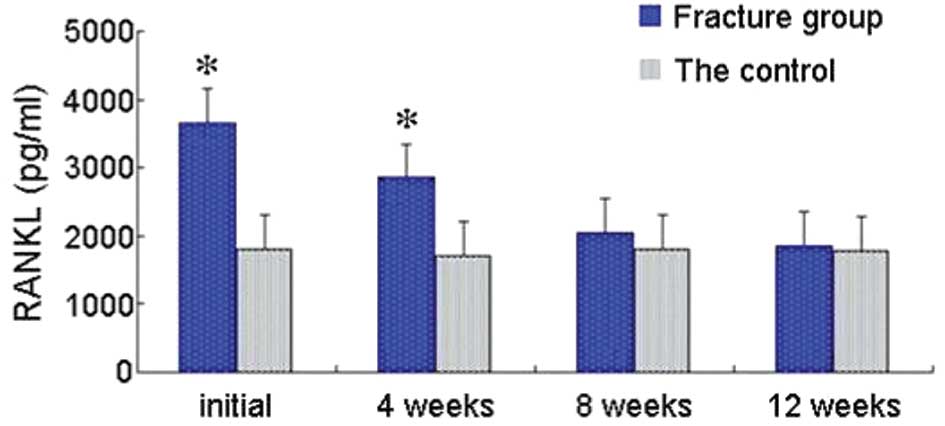
RANKL levels were significantly higher in the
intertrochanteric fracture group than in the controls at baseline
and 4 weeks following injury (P<0.05). However, RANKL serum
levels were not significantly different between the two groups 8
and 12 weeks following injury (P>0.05 at both time intervals).
Serum RANKL levels were higher in the injury group than in the
control group at all four time intervals (Fig. 1).
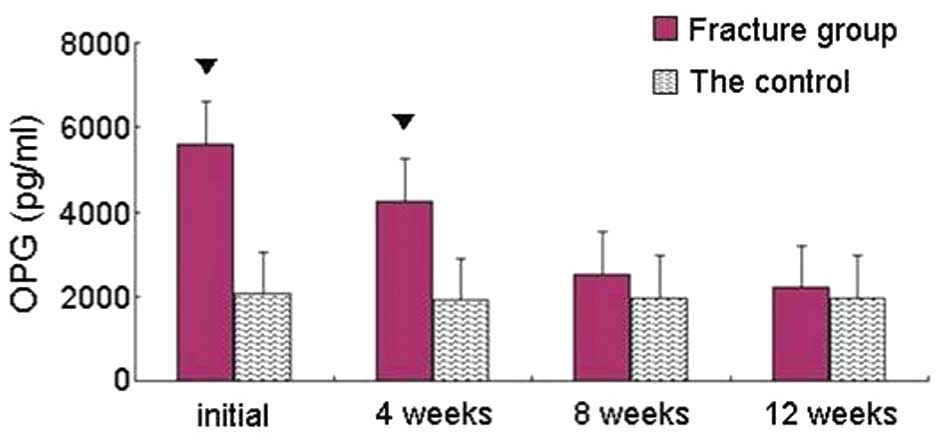
Serum OPG levels were higher in the fracture group
than in the control group at all four time points (Fig. 2). Although the OPG levels were
significantly higher in the intertrochanteric fracture group than
in the controls immediately after and 4 weeks after injury
(P<0.05 at both time intervals), there was no significant
difference between the two groups 8 and 12 weeks following injury
(P>0.05 at both time intervals; Fig. 2).
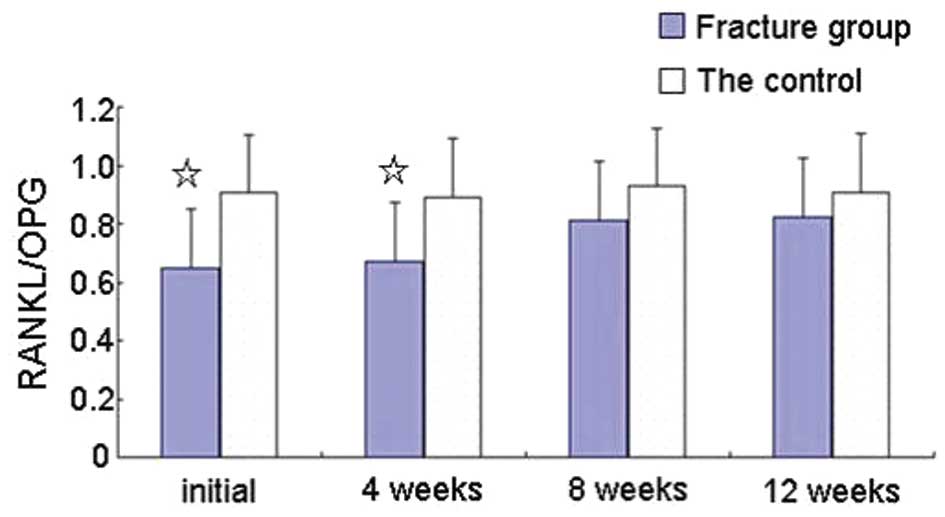
RANKL/OPG ratios
The RANKL/OPG ratio was lower in the
intertrochanteric fracture group than in the controls at all four
time intervals. The ratios were significantly lower immediately
after and 4 weeks after injury (P<0.05 at both time intervals),
while there was no significant difference between the two groups 8
and 12 weeks after injury (Fig.
3).
Discussion
In the present study, the serum levels of RANKL and
OPG in elderly patients with intertrochanteric fractures and in
healthy controls were assessed. To the best of our knowledge, this
is the first study to demonstrate a role of the serum levels of
RANKL and OPG in elderly patients with intertrochanteric
fractures.
The levels of RANKL (Fig. 1) and OPG (Fig. 2) were significantly higher in the
fracture group than in the controls immediately after and 4 weeks
following injury, while there were no significant differences
between the groups 8 and 12 weeks after injury. A previous study
has shown that the secretion of RANKL by osteoblasts stimulates
osteoclast differentiation (19).
Schett et al(20) suggested
that serum RANKL levels may be used as a predictor of fracture.
Abdallah et al reported an association between high OPG
levels and low risk of fracture (21). It has also been suggested that OPG
in combination with RANKL may inhibit osteoclast differentiation
(22).
In the present study, it was observed that RANKL
levels were higher in the intertrochanteric fracture group than in
the healthy controls immediately after and 4 weeks after injury
(Fig. 1), while the RANKL levels
were lower than the OPG levels in the intertrochanteric fracture
group at baseline and 4 weeks after injury. These data suggest that
the number of osteoblasts increases during healing, particularly
immediately after and 4 weeks after injury. As a result, bone
formation is likely to dominate the healing process at these two
time intervals. Therefore, our results indicate that serum RANKL
and OPG may be involved in the healing of intertrochanteric
fractures in elderly patients.
Notably, the RANKL/OPG ratios were observed to be
significantly lower in the intertrochanteric fracture group than in
the normal control subjects immediately after and 4 weeks after
injury; and remained lower 8 and 12 weeks following injury
(Fig. 3). The RANKL/OPG ratio was
lower in the intertrochanteric fracture group than in the normal
group, while a slight increase of the ratio with time was noted
(Fig. 3). An increasing RANKL/OPG
ratio after fracture is considered to tilt the balance of RANKL and
OPG toward bone resorptive status (17), since this balance is critically
important for bone remodeling and the preservation of bone mass
(23). The RANKL-OPG balance may
affect osteoclast activity, which is why it has been suggested that
the serum RANKL/OPG ratio is a critical factor for determining
osteoclast activation (24).
The results of the current study indicate that the
RANKL/OPG ratio may be important in the healing process of
intertrochanteric fractures in elderly patients. Coetzee and Kruger
(25) suggested that this ratio
may determine osteoclast activation and affect bone formation,
which underlies the potential value of the ratio for predicting
fracture healing. Moreover, Tsangari et al(26) demonstrated that the RANKL/OPG ratio
predicts fracture healing (26).
The present study indicates that bone formation mainly occurs
during the first 8 weeks, and particularly during the first 4 weeks
following injury; bone remodeling mainly occurs 8 and 12 weeks
following injury. Future studies are required in order to determine
why the RANKL and OPG levels are higher at the initial time
intervals after intertrochanteric fracture than their levels in
healthy subjects. Since fracture healing is a complex process, the
changes in RANKL and OPG levels may also be influenced by other
factors, which will be investigated in future studies.
In conclusion, high serum levels of RANKL and OPG
were detected in patients with intertrochanteric fractures compared
with healthy controls. The present study demonstrated that the
RANKL/OPG ratio was lower in the intertrochanteric fracture group
than in the healthy controls. These observations provide important
information regarding the healing process of intertrochanteric
fractures in the elderly at a molecular level. In the present
study, the serum RANKL/OPG ratio has been suggested to contribute
to the modulation of fracture repair. Consequently, these findings
may lead to novel therapeutic interventions for nonunion of
intertrochanteric fractures.
Acknowledgements
The authors would like to thank Dr Li-Juan Guo from
the Molecular Laboratory of Peking University (Beijing, China) for
advice regarding the setup of the ELISA experiment, and Dr Guo-Xing
Li from the Department of Public Health (Peking University) for
assistance in statistical analysis.
References
|
1
|
Kesmezacar H, Oğüt T, Bilgili MG, Gökay S
and Tenekecioğlu Y: Treatment of intertrochanteric femur fractures
in elderly patients: internal fixation or hemiarthroplasty. Acta
Orthop Traumatol Turc. 39:287–294. 2005.(In Turkish).
|
|
2
|
Angelini M, McKee MD, Waddell JP,
Haidukewych G and Schemitsch EH: Salvage of failed hip fracture
fixation. J Orthop Trauma. 23:471–478. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Talmo CT and Bono JV: Treatment of
intertrochanteric nonunion of the proximal femur using the S-ROM
prosthesis. Orthopedics. 31:1252008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Dhammi I, Jain A, Singh A, Rehan-Ul-Haq,
Mishra P and Jain S: Primary nonunion of intertrochanteric
fractures of femur: an analysis of results of valgization and bone
grafting. Indian J Orthop. 45:514–519. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Looker AC, Bauer DC, Chesnut CH 3rd,
Gundberg CM, Hochberg MC, Klee G, Kleerekoper M, Watts NB and Bell
NH: Clinical use of biochemical markers of bone remodeling: current
status and future directions. Osteoporos Int. 11:467–480. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kurban S and Mehmetoglu I:
Osteoprotegerin, RANK and RANK ligand. Turk J Biochem. 34:178–184.
2007.
|
|
7
|
Stejskal D, Bartek J, Pastorková R,
Růzicka V, Oral I and Horalík D: Osteoprotegerin, RANK, RANKL.
Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub. 145:61–64.
2001. View Article : Google Scholar
|
|
8
|
Khosla S: Minireview: the OPG/RANKL/RANK
system. Endocrinology. 142:5050–5055. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kostenuik PJ and Shalhoub V:
Osteoprotegerin: a physiological and pharmacological inhibitor of
bone resorption. Curr Pharm Des. 7:613–635. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bucay N, Sarosi I, Dunstan CR, Morony S,
Tarpley J, Capparelli C, Scully S, Tan HL, Xu W, Lacey DL, Boyle WJ
and Simonet WS: Osteoprotegerin-deficient mice develop early onset
osteporosis and arterial calcification. Genes Dev. 12:1260–1268.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gravallese EM, Manning C, Tsay A, Naito A,
Pan C, Amento E and Goldring SR: Synovial tissue in rheumatoid
arthritis is a source of osteoclast differentiation factor.
Arthritis Rheum. 43:250–258. 2004.PubMed/NCBI
|
|
12
|
Hafbauer LC and Schoppet M: Clinical
implications of the osteoprotegerin/RANKL/RANK system for bone and
vascular diseases. JAMA. 292:490–495. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Masi L, Simonini G, Giani T, Del Monte F,
Giani T, Cimaz R, Vierucci S, Brandi ML and Falcini F:
Osteoprotegerin (OPG)/RANKL system in juvenile idiopathic arthitis:
is there a potential modulating role for OPG/RANKL in bone injury?
J Rheumatol. 31:986–991. 2004.PubMed/NCBI
|
|
14
|
Blaır JM, Zheng Y and Dunstan CR: RANK
ligand. Int J Biochem Cell Biol. 39:1077–1081. 2007.
|
|
15
|
Chamoux E, Houde N, L’Eriger K and Roux S:
Osteoprotegerin decreases human osteoclast apoptosis by inhibiting
the TRAIL pathway. J Cell Physiol. 216:536–542. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Boyce BF and Xing L: Function of
RANKL/RANK/OPG in bone modeling end remodeling. Arch Biochem
Biophys. 473:139–146. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lacey DL, Timms E, Tan HL, et al:
Osteoprotegerin ligand is a cytokine that regulates osteoclast
differentiation and activation. Cell. 93:165–176. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Simonet WS, Lacey DL, Dunstan CR, et al:
Osteoprotegerin: a novel secreted protein involved in the
regulation of bone density. Cell. 89:309–319. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Son A, Kim MS, Jo H, Byun HM and Shin DM:
Effects of inositol 1,4,5-triphosphate on osteoclast
differentiation in RANKL-induced osteoclastogenesis. Korean J
Physiol Pharmacol. 16:31–36. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Schett G, Kiechl S, Redlich K,
Oberhollenzer F, Weger S, Egger G, Mayr A, Jocher J, Xu Q,
Pietschmann P, Teitelbaum S, Smolen J and Willeit J: Soluble RANKL
and risk of non-traumatic fracture. JAMA. 291:1108–1113. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Abdallah BM, Stilgren LS, Nissen N, Kassem
M, Jørgensen HR and Abrahamsen B: Increased RANKL/OPG mRNA ratio in
iliac bone biopsies from women with hip fractures. Calcif Tissue
Int. 76:90–97. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Yasuda H, Shima N, Nakagawa N, Yamaguchi
K, Kinosaki M, Goto M, Mochizuki SI, Tsuda E, Morinaga T, Udagawa
N, Takahashi N, Suda T and Higashio K: A novel molecular mechanism
modulating osteoclast differentiation and function. Bone.
25:109–113. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wasilewska A, Rybi-Szuminska A and
Zoch-Zwierz W: Serum RANKL, osteoprotegerin (OPG), and RANKL/OPG
ratio in nephrotic children. Pediatr Nephrol. 25:2067–2075. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hofbauer LC, Khosla S, Dunstan CR, Lacey
DL, Boyle WJ and Riggs BL: The roles of osteoprotegerin and
osteoprotegerin ligand in the paracrine regulation of bone
resorption. J Bone Miner Res. 15:2–12. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Coetzee M and Kruger MC:
Osteoprotegerin-receptor activator of nuclear factor-kappaB ligand
ratio: a new approach to osteoporosis treatment? South Med J.
97:506–511. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Tsangari H, Findlay DM, Kuliwaba JS,
Atkins GJ and Fazzalari NL: Increased expression of IL-6 and RANK
mRNA in human trabecular bone from fragility fracture of the
femoral neck. Bone. 35:334–342. 2004. View Article : Google Scholar : PubMed/NCBI
|