Introduction
Keratocystic odontogenic tumors (KCOTs) are locally
aggressive benign tumors which occur in the bones of both jaws with
a high recurrence rate (1). They may
occur at any age with a peak in the second and third decades of
life (2). The most important clinical
features of KCOTs are their potential for locally destructive
behavior, recurrence rate, and their tendency to multiplicity,
particularly when associated with naevoid basal cell carcinoma
syndrome.
Ameloblastoma is a rare, benign, slow-growing but
locally invasive neoplasm of the odontogenic origin involving the
mandible (80%) and maxilla; conservative treatment results in a
high recurrence rate (3).
Ameloblastoma may be characterized as solid/multicystic,
extraosseous/peripheral, desmoplastic or unicystic types. Unicystic
type ameloblastomas account for 5–15% of all cases, as is in the
present case. The mean age of presentation for cases associated
with an unerupted tooth is 16 years, as opposed to 35 years in the
absence of an unerupted tooth (2). It
is uncommon for these tumors to simultaneously occur in a patient's
jaw. To the best of our knowledge, no previous studies have
reported the co-occurrence of these tumors.
Previous reports that observed the occurrence of
simultaneous odontogenic lesions or simultaneous odontogenic and
non-odontogenic lesions, described combined lesions, sometimes
called hybrid lesions (4,5). By contrast the present study describes
the case of the challenging diagnostic process of the simultaneous
presentation of KCOT and ameloblastoma in the mandible of a
45-year-old male.
Case report
A 45-year-old asymptomatic male patient was referred
to the outpatient clinic of the Osaka Dental University (Osaka,
Japan) for further investigation of radiolucency observed on the
apex of the lower-right first molar. The lesions were first
detected at the local doctor whom the patient had visited for the
purpose of having treated for dislocated crown in the left molar.
An electric pulp test was performed and demonstrated vitality of
the adjacent premolars. Clinical examination revealed no extra-oral
asymmetry or swelling.
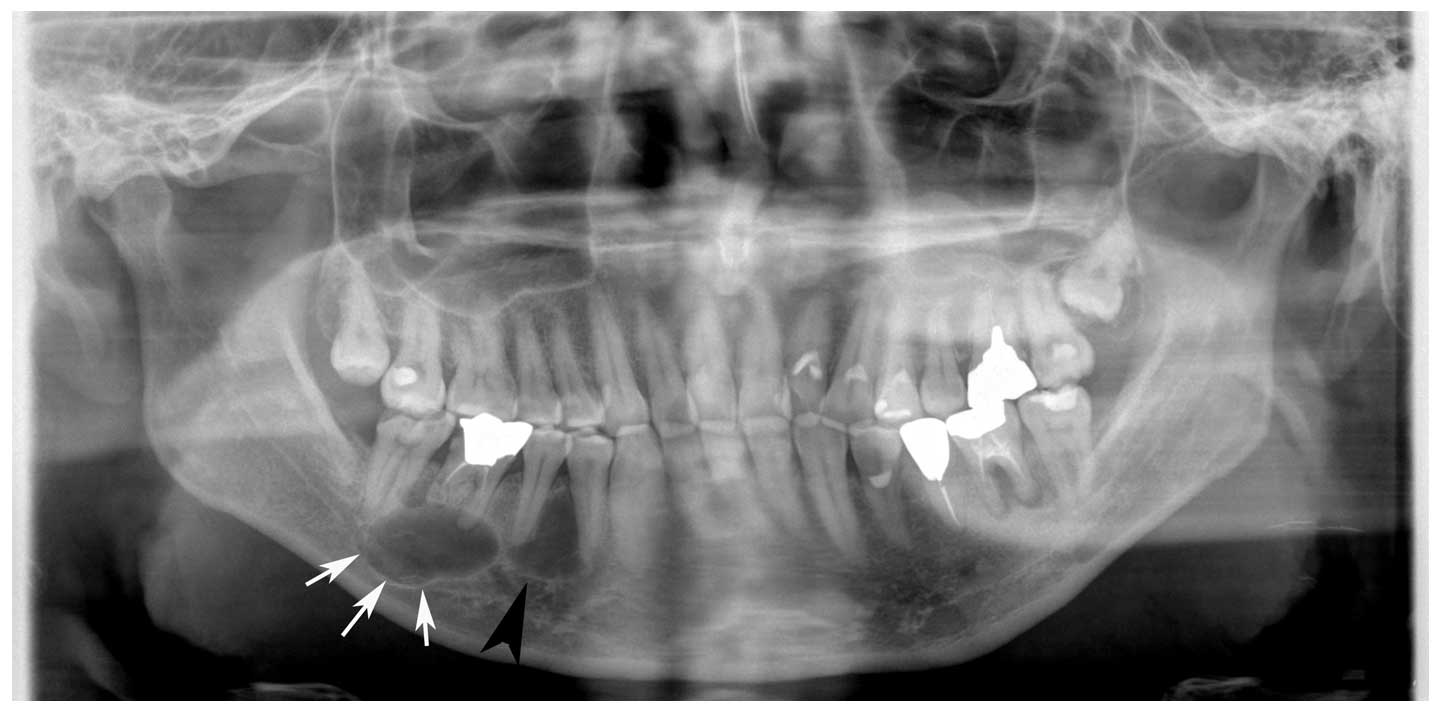
A panoramic image was obtained using conventional
equipment (Super Veraview X500 AE; J Morita MFG. Corp., Kyoto,
Japan) at 78 kV, 9 mA. Initial panoramic images obtained revealed
the presence of a cystic lesion around the root apex of the lower
right first molar whose root canal was filled. The mandibular canal
was shifted downward due to the pressure from a cystic lesion.
Overall, the imaging diagnosis was of a radicular cyst (Fig. 1). Radiolucency with pencil sketch-like
rim was also evident in the inter-alveolar septum of the
lower-right premolars; however, no resorption or adverse findings
were observed and this was diagnosed as a simple bone cyst
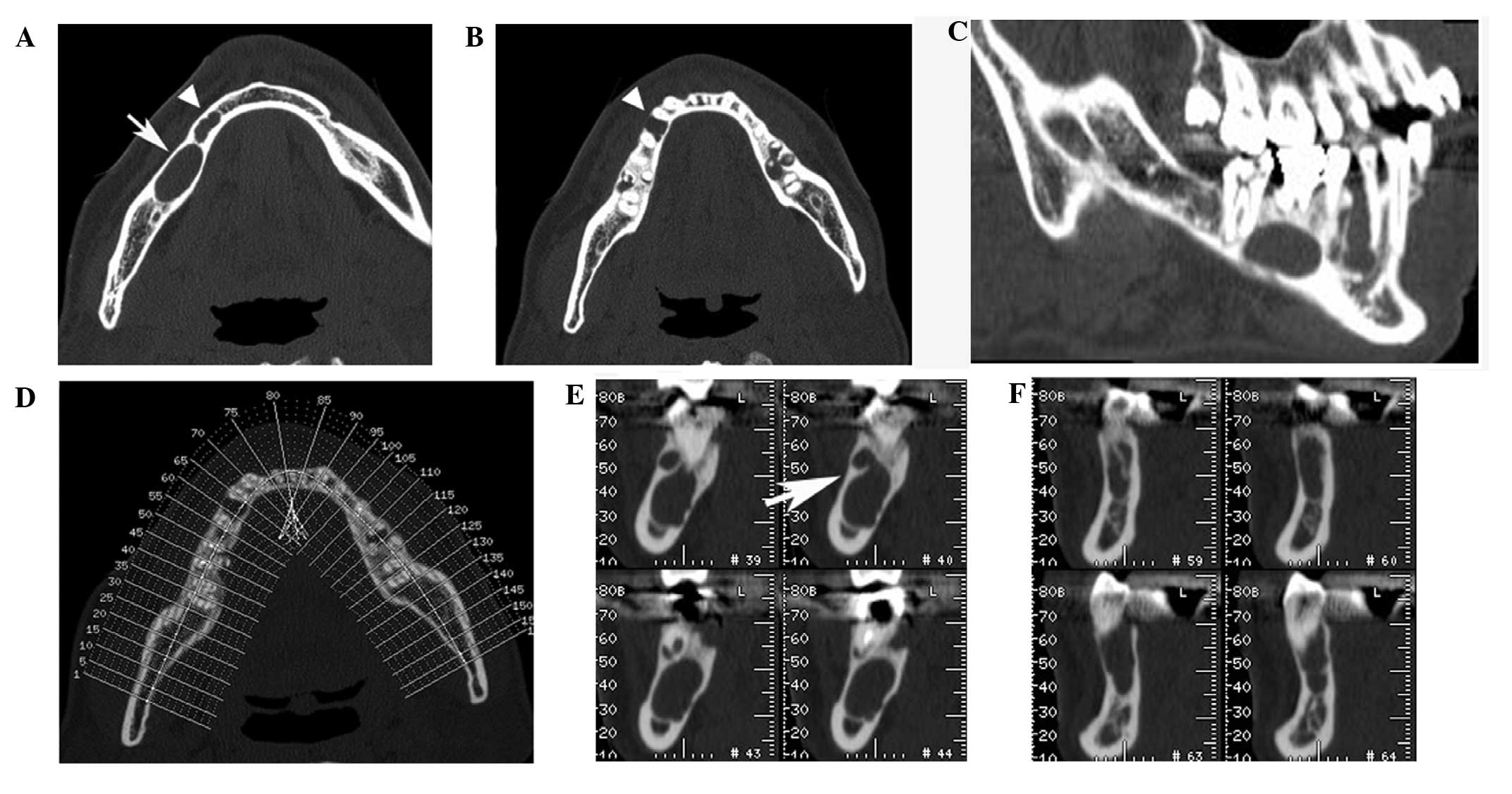
(Fig. 1). Computed tomography (CT)
images were obtained using CT scanners (BrightSpeed Elite; GE
Healthcare, Milwaukee, WI, USA) at 120 kV. The electrical current
was automatically optimized for the object thickness (maximum, 120
mA). In addition, the CT was performed according to the following
parameters: Slice thickness, 0.65 mm; pitch and tube voltage,
0.625:1; and field of view, 16.8 cm2. Para-sagittal and
orthogonal views (thickness, 1 mm) were reformatted and
reconstructed in the right molar and premolar region. These images
revealed two independent abnormal lesions, comprising a 15-mm
sized, round-style, well-defined cystic lesion on the root apex of
the lower-right first molar and a 12-mm sized, radiolucent lesion
with pencil sketch-like rim in the inter-alveolar septum of the
lower-premolars (Fig. 2). These
lesions induced the slight divergency of lower-right premolars.
Neither of the lesions demonstrated evidence of root resorption.
The wall of mandibular canal proximal to the lesion was intact and
there was a slight bucco-lingual bony expansion on the lesions'
medial-distal size. Therefore, the diagnoses made based on CT
images were also of a radicular cyst and simple bone cyst (Fig. 2).
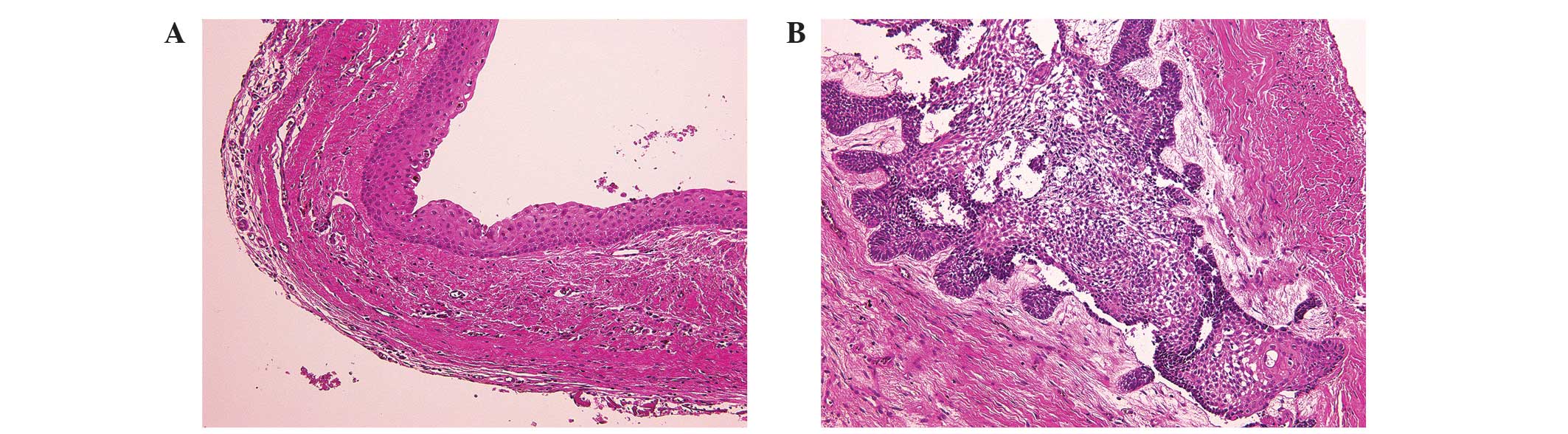
Following the incisional biopsy, histopathological
examinations were performed, which demonstrated that each lesion
had two principal features. One of the specimens revealed a thin
layer of parakeratinized stratified squamous epithelium (5–8 cell
layers thick) and fibrous connective tissue (Fig. 3A). The other specimen revealed an
odontogenic epithelium, structured stellate reticulum and
peripheral palisading within a fibrous stroma (Fig. 3B). These histopathological results
indicated the diagnoses of KCOT and ameloblastoma,
respectively.
Under general anesthesia, the patient underwent
conservative tumor resection with extensive bone curettage
associated with extractions of the lower-right molars and
premolars. The diagnoses were confirmed based on excisional biopsy
specimens. No recurrences or post-operative complications were
observed during the 6 months follow-up period.
Discussion
The present study reported a case of simultaneous
occurrence of KCOT and ameloblastoma in the mandible of a patient.
To the best of our knowledge, the synchronous occurrence of KCOT
and ameloblastoma as distinct lesions has not been previously
reported.
In the present case, the diagnoses that were
concluded from imaging and histopathological studies were entirely
different. The presence of two mandibular radiolucent lesions led
to the suspicion of a radicular cyst and a simple bone cyst.
However, the incisional and excisional biopsies allowed for the
definitive diagnosis of two pathologically distinct lesions: KCOT
and ameloblastoma. Due to the high recurrence rate of these types
of lesions (6,7), close post-surgical follow-up is
preferred.
In regards to the present study, it was also
important to consider possible explanations for the difficult
nature of the diagnosis based on radiographic images. In general,
KCOT is a pathological entity with aggressive behavior and a high
rate of recurrence (1). In 2005, the
World Health Organization revised and updated the classification of
odontogenic tumors as well as certain associated terminologies
(8). Although odontogenic keratocysts
were previously classified as cysts, they have been reclassified as
KCOTs due to their neoplastic nature (2,9).
Radiologically, KCOTs appear as unilocular or multilocular
radiolucencies, which commonly have a thin, reactive, sclerotic
bony rim and smooth or scalloped margins; in addition, these tumors
may be destructive and invade into adjacent bone (10). By contrast, ameloblastomas are slowly
growing solid and cystic tumors, which are characterized as
multiloculated, honeycombed, lytic lesions that are devoid of
mineralization in radiographs (10).
In the panoramic images of the present case, the two
lesions appeared to be unilocular radiolucent lesions without root
resorption. The cystic lesion surrounding the root apex of the
lower-right first molar was initially diagnosed as a radicular
cyst; however, the associated lesion was ultimately revealed to be
a KCOT. In addition, the radiolucency identified in the
inter-alveolar septum of the lower-right premolars resembled a
simple bone cyst; however, this lesion was determined to be an
ameloblastoma. The CT results appeared to be concurrent with the
panoramic image impression; however, this was due to a lack of
reliable evidence for root resorption. As these lesions were
immature, the radiographic examinations did not provide any typical
characteristics that would have been suggestive of odontogenic
tumors, including root resorption, divergence or multilocular
radiolucency.
Retrospectively, certain imaging findings were
indicative of significant pathological characteristics, including
the occurrence of a septum inside the ameloblastoma on the
para-sagittal CT scan (Fig. 2C) as
well as a minute septum in the KCOT on the orthogonal reconstructed
CT images (Fig. 2E, arrow).
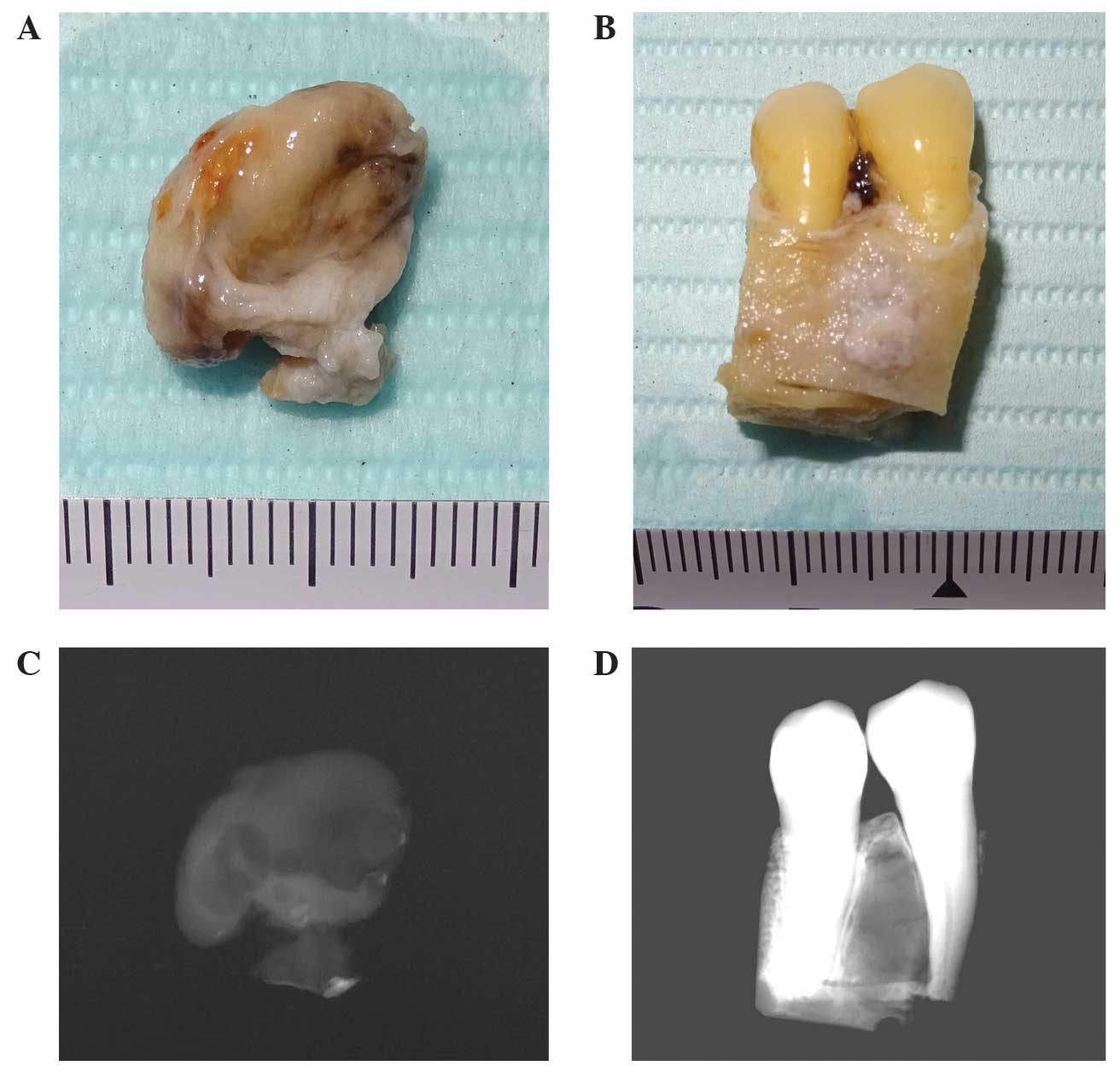
Soft X-ray is a form of X-ray with low permeability,
which has a wavelength of between 10 and 102 Å. Soft X-ray is
generally used to visualize the detailed internal structures of
specimens with more precision than conventional diagnostic X-rays.
In the present study, soft X-ray images were obtained using a
SOFTEX CSMW-2 system (Softex Co., Ltd, Kanagawa, Japan) in order to
investigate the details of the internal structures of the lesions.
As a novel trial, imaging plates were used as soft X-ray sensors,
with the tube voltage set at 40 kV and an electrical current of 2
mA. In order to capture images of the KCOT and ameloblastoma
specimens (Fig. 4A and B), the timer
was set to 10 and 20 seconds, respectively. The resultant images
revealed the detailed structure of the internal septum inside the
lesion (Fig. 4C and D). These
characteristics were concurrent with the histopathological features
observed.
The occurrence of two distinct and simultaneous
odontogenic lesions in one patient is extremely uncommon (6). Ameloblastomas have been previously
reported to co-occur with an orthokeratinized odontogenic cyst and
a glandular odontogenic cyst (10)
and Fregnani et al (6)
reported a case of synchronous ameloblastoma and orthokeratinized
odontogenic cyst located on bilateral posterior regions of the
mandible (6). In addition, Hisatomi
et al (11) described a case
of a glandular odontogenic cyst that was associated with an
ameloblastoma; in particular, this study referred to the
correlation between diagnostic imaging results and
histopathological features (11).
Shimamoto et al (12)
presented a case of ossifying fibroma and KCOT. Another study
reported a unique case of multiple ossifying fibromas in the
mandible (13). Case reports of the
simultaneous occurrence of odontogenic cysts and/or tumors are
summarized in Table I.
 | Table I.Case reports of simultaneous
odontogenic lesions of the jaw. |
Table I.
Case reports of simultaneous
odontogenic lesions of the jaw.
| Case (reference) | Year | Age | Gender | Histopathological
diagnosis | Imaging modality | Location |
|---|
| Hisatomi et al
(11) | 2000 | 45 | F | Glandular odontogenic
cyst and ameloblastoma | IO, CT, MR | Mandible |
| Fregnani et al
(6) | 2006 | 21 | M | Ameloblastoma and
orthokeratinized odontogenic cyst | PI, CT | Mandible |
| Shimamoto et
al (12) | 2011 | 48 | F | OF and KCOT | PI, CT | Mandible |
| Gamoh et al
(13) | 2011 | 32 | F | OF and OF | IO, PI, CT | Mandible |
| Present case | – | 45 | M | KCOT and
ameloblastoma | PI, CT, SI | Mandible |
KCOT is one of the consistent features of
Gorlin-Goltz syndrome, which is also known as nevoid basal cell
carcinoma syndrome (14).
Gorlin-Goltz syndrome demonstrates an autosomal dominant
inheritance pattern with variable phenotypic expression, which may
result in skin, jaw and other skeletal lesions. In addition, the
involvement of the central nervous system and vision in this
syndrome coincide with typical facial features, including frontal
bossing and hypertelorism (7). In
1965, Gorlin had already noted striking analogies between the
cutaneous and jaw lesions, stating that jaw cysts correspond to the
cutaneous milia and the mural proliferations observed in certain
jaw cysts were analogous with adnexal skin tumors. Furthermore, the
ameloblastoma may be compared with cutaneous basal-cell carcinoma
(15). These previous studies
therefore supported the co-occurrence of KCOT and ameloblastoma in
the present case, although there does not appear to be any
association with Gorlin-Goltz syndrome due to the lack of cutaneous
milia and solitariness of the KCOT. Therefore, the lesions observed
in the present study may have generated fully independently;
however, the present case may offer a proof-of-principal for
Gorlin's insightful theory.
The present case proved the possibility of the
simultaneous occurrence of KCOT and ameloblastoma in a jaw. This
knowledge should be a valuable warning as both tumors have high
recurrence rate if improperly treated.
Acknowledgements
The authors would like to thank Dr Akihiro Nakajima
(Second Department of Oral and Maxillofacial Surgery, Osaka Dental
University) and Dr Kaname Tsuji (First Department of Oral and
Maxillofacial Surgery, Osaka Dental University) for their support
in the present study.
References
|
1
|
Antonoglou GN, Sándor GK, Koidou VP and
Papageorgiou SN: Non-syndromic and syndromic keratocystic
odontogenic tumors: Systematic review and meta-analysis of
recurrences. J Craniomaxillofac Surg. 42:e364–e371. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Philipsen HP: Keratocystic odontogenic
tumourPathology and Genetics of Head and Neck Tumours. Barnes L,
Eveson JW, Reichart P and Sidransky D: IARC Press; Lyon: pp.
306–307. 2005
|
|
3
|
McClary AC, West RB, McClary AC, Pollack
JR, Fischbein NJ, Holsinger CF, Sunwoo J, Colevas AD and Sirjani D:
Ameloblastoma: A clinical review and trends in managementEur Arch
Otorhinolaryngol. Apr 30–2015.(Epub ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Siar CH and Ng KH: ‘Combined ameloblastoma
and odontogenic keratocyst’ or ‘keratinising ameloblastoma’. Br J
Oral Maxillofac Surg. 31:183–186. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Nishimura T, Nagakura R, Ikeda A and Kita
S: Simultaneous occurrence of a squamous cell carcinoma and an
ameloblastoma in the maxilla. J Oral Maxillofac Surg. 58:1297–1300.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fregnani ER, DE Cruz Perez, Soares FA and
Alves FA: Synchronous ameloblastoma and orthokeratinized
odontogenic cyst of the mandible. J Oral Pathol Med. 35:573–575.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shear M and Speight PM: Odontogenic
keratocyst. Cysts of the Oral and Maxillofacial Regions. 4th.
Blackwell Munksgaard; Oxford: pp. 6–58. 2007, View Article : Google Scholar
|
|
8
|
Philipsen HP and Reichart PA:
Classification of odontogenic tumours. A historical review. J Oral
Pathol Med. 35:525–529. 2006.PubMed/NCBI
|
|
9
|
Gardner DG, Heikinheimo K, Shear M,
Philipsen HP and Coleman H: AmeloblastomasPathology and Genetics of
Head and Neck Tumours. Barnes L, Eveson JW, Reichart P and
Sidransky D: International Agency for Research on Cancer (IARC)
Press; Lyon: pp. 296–297. 2005
|
|
10
|
Som PM and Curtin HD: Tumors and
Tumor-like ConditionsHead and Neck Imaging. Som PM and Brandwein
MS: 4th. 1. Mosby; St. Louis, MO: pp. 347–352. pp. 354–356.
2003
|
|
11
|
Hisatomi M, Asaumi J, Konouchi H, Yanagi Y
and Kishi K: A case of glandular odontogenic cyst associated with
ameloblastoma: Correlation of diagnostic imaging with
histopathological features. Dentomaxillofac Radiol. 29:249–253.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Shimamoto H, Kishino M, Okura M,
Chindasombatjaroen J, Kakimoto N, Murakami S and Furukawa S:
Radiographic features of a patient with both cemento-ossifying
fibroma and keratocystic odontogenic tumor in the mandible: A case
report and review of literature. Oral Surg Oral Med Oral Pathol
Oral Radiol Endod. 112:798–802. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Gamoh S, Koseki T, Yotsui Y, Akiyama H and
Shimizutani K: Mutiple ossifying fibromas of the mandible: Report
of an unique case. Dental Radiology. 51:16–18. 2011.
|
|
14
|
Shepard M and Coleman H: Simultaneous
adenomatoid odontogenic and keratocystic odontogenic tumours in a
patient with Gorlin-Goltz syndrome. Aust Dent J. 59:121–124. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Gorlin RJ, Vickers RA, Kellen E and
Williamson JJ: Multiple basal-cell nevi syndrome. An analysis of a
syndrome consisting of multiple nevoid basal-cell carcinoma, jaw
cysts, skeletal anomalies, medulloblastoma, and hyporesponsiveness
to parathormone. Cancer. 18:89–104. 1965. View Article : Google Scholar : PubMed/NCBI
|