Introduction
Prostate cancer is the most commonly diagnosed solid
malignancy that occurs in the Western male population, with an
incidence rate that is continually increasing (1). Prostate cancer is the sixth leading
cause of cancer related mortality in males, worldwide (2); annual global mortality rates increased
from 156,000 to 256,000 mortalities between 1990 and 2010 (3). Patients diagnosed with prostate cancer
usually exhibit one or more symptoms, including frequent urination,
nocturia, difficulty starting and maintaining a steady stream of
urine, hematuria and dysuria. Prostate cancer is diagnosed by
biopsy. Medical imaging may then be performed to determine if the
cancer has spread to other parts of the body (4). Approximately 8% of all prostate cancers
are diagnosed at an advanced stage (5). Bone and lung metastases from prostate
cancer are common, but metastases to both the testis and epididymis
are rare, with a usually poor prognosis (6). The treatments for prostate cancer
include a combination of surgery, radiation therapy, hormone
therapy and chemotherapy. Patient outcome depends on the patient's
age and general medical condition, as well as how aggressive and
extensive the cancer is (7). The
current study presents the case of a 69-year-old male who was
diagnosed with synchronous testicular and epididymal metastases
from a high-grade prostate carcinoma, without distant metastasis.
To the best of our knowledge, such a case has seldom been described
in the literature. Written informed consent was obtained from the
patient.
Case report
In July 2012, a 69-year-old male was admitted to The
First Hospital of Shijiazhuang (Shijiazhuang, China) with a 2-year
history of lower urinary tract symptoms, including increased
frequency of urination, noturia and a weak urinary stream, without
dysuria or hematuria. In a routine examination 1 month prior to
admittance, it was found that the patient's serum prostate-specific
antigen (PSA) level was >100 ng/ml (normal range, <4.0
ng/ml). The patient's medical history included 24 years of diabetes
treated with insulin (fasting glucose level of 6.55 mmol/l; normal
range, 3.89–6.1 mmol/l) and a 20-year history of hypertension that
was treated with benazepril and metoprolol. The patient had
undergone a prostate transurethral resection five years previously
due to prostate bleeding. The current prostate pathology showed
prostatic hyperplasia. The patient also had a history of smoking 10
cigarettes per day for 40 years.
Physical examination showed that the right testicle
was slightly enlarged and tough, without tenderness. No
abnormalities were found in the spermatic cord and left testicle.
B-mode ultrasound showed prostatic hyperplasia with calcification
(51×63×58 mm). An increased post-void residual urine volume of 110
ml (normal range, 5–12 ml) was noted. The kidneys, ureters,
bladder, liver and spleen were normal. Magnetic resonance imaging
revealed prostate carcinoma with seminal vesicle involvement. A
prostate biopsy revealed prostate gland adenocarcinoma, with a
Gleason score of 3+3 (8).
Immunohistochemical staining showed strong positive staining for
prostatic acid phosphatase (PAP) (+++), PSA (+++) and P504s (+++),
but not for p63 (−)or CK34βE12 (−) (9). The Ki-67 was ~5%. A metastatic
evaluation of the chest, abdomen, pelvis, bones, kidneys, ureters,
bladder, liver and spleen were negative. The patient was treated
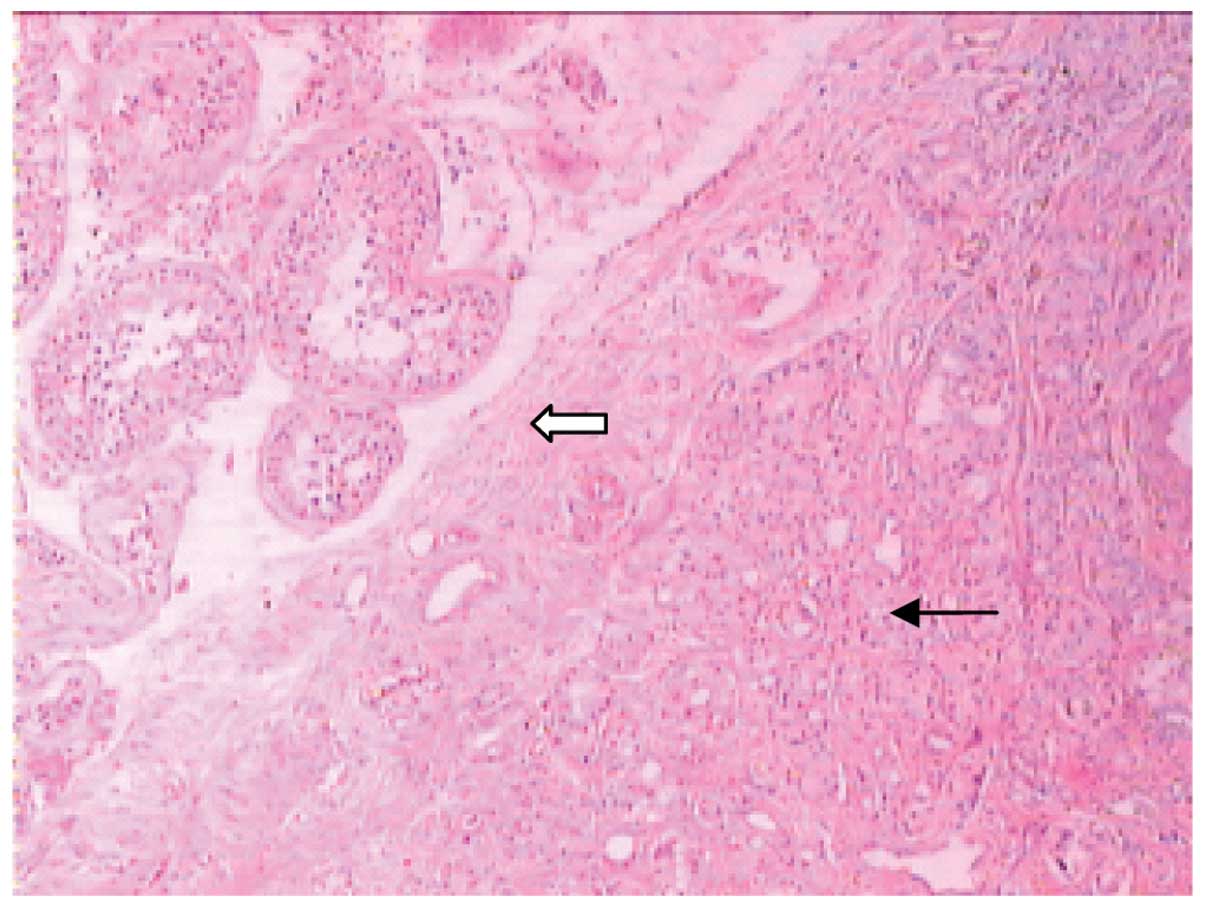
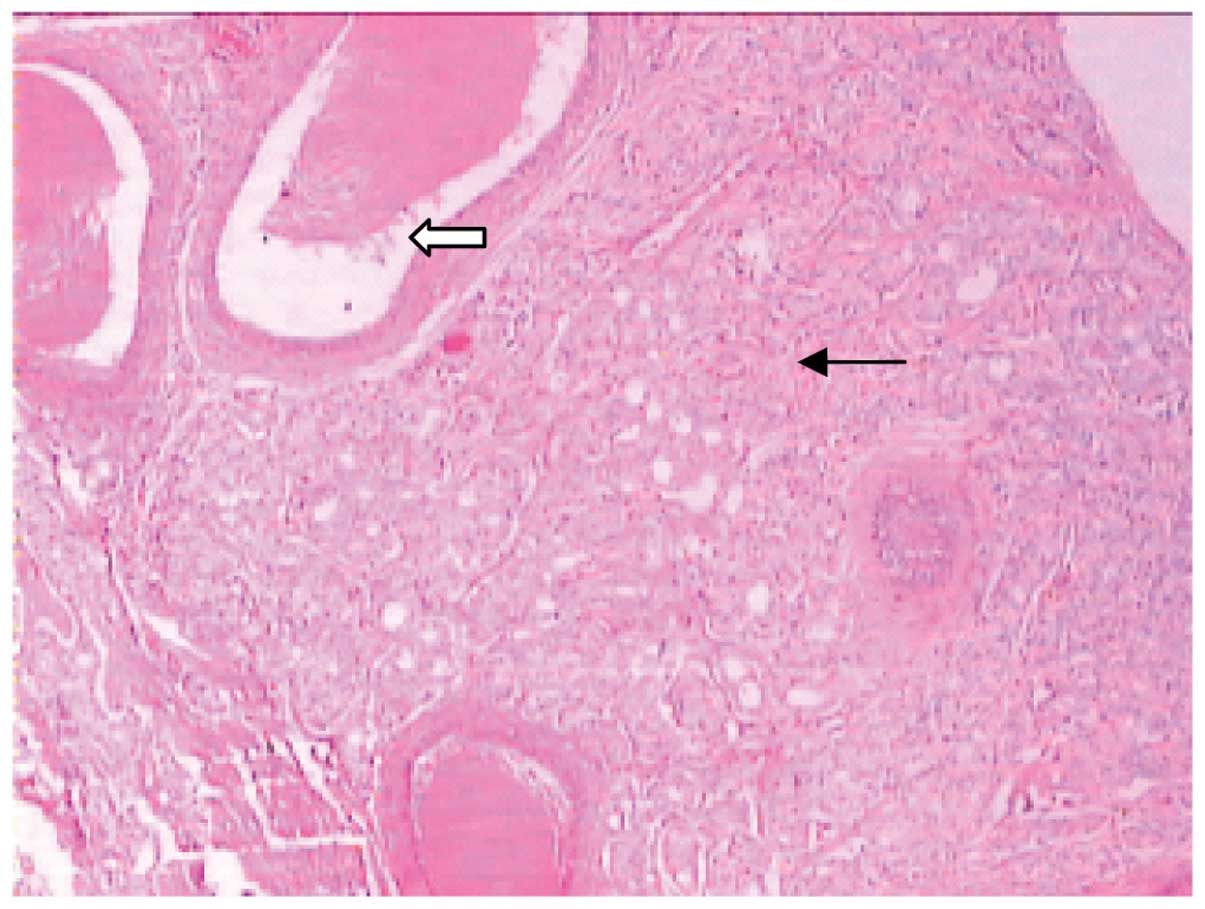
with a bilateral orchiectomy. The testicular pathology showed that
the right testicle, the tunica albuginea and the epididymis were
infiltrated by metastatic adenocarcinoma (Figs. 1 and 2);
microscopically, malignant round tumor cells were observed within
the interstitium of the testicular parenchyma beneath the capsule.
The cells had infiltrated the seminiferous tubules and exhibited a
discohesive growth pattern. Immunohistochemical staining once again
showed strong positive staining for PAP (+++), PSA (+++) and P504s
(+++). The left testis and epididymis were normal.
The patient was treated with ongoing conventional
flutamide (250 mg, 3 times/day) endocrine therapy and radiotherapy
(60 Gy/30 fractions 5 times/week) for 6 weeks, and currently
remains in a stable condition after follow-up for 24 months.
Discussion
Prostate cancer is a common cancer in older men
(10). With changes in life style,
diet and environment, as well as the improved detection level, the
incidence of prostate cancer has recently increased (11). The majority of prostate cancer is
adenocarcinoma, usually occurring in the peripheral zone of the
prostate (12). Prostate cancer may
spread through the lymph and blood vessels, or through direct
invasion to adjacent organs. Blood transfer accounts for 35% of
this spread. The most common sites of metastases are the bones,
lungs, liver, pleura and adrenal glands (13), while the occurrence rates of
metastases in the testes and epididymis are low. Johansson and
Lannes showed that ~4% of metastases to the testes are found
incidentally during orchiectomy for advanced prostate carcinoma
(14). Following the examination of
24,000 autopsy results, Pienkos and Jablokow reported a testicular
metastasis rate of 0.06% (15).
However, asymptomatic metastases of prostate carcinoma to both the
testis and the epididymis are extremely rare occurrences; only a
small number of cases have been reported previously (1,2). Thon
et al (16) reported a case of
carcinoma of the prostate in a German patient who exhibited
metastases to the testis and epididymis. However, to the best of
our knowledge, to date no cases of such have been reported in Asia.
Prostate cancer metastasis to the testes usually lacks symptoms and
signs, and can only can be incidentally detected during autopsies,
or following a bilateral orchiectomy for hormonal management in
cases of advanced prostate carcinoma. Prostate carcinoma may spread
to the testes or epididymis by retrograde venous diffusion,
arterial embolism, retrograde lymphatic spread or direct extension
via the vas deferens (14,15).
The prognostic significance of testicular metastasis
from prostate carcinoma remains unknown. The study by Tu et
al suggested that prostate cancer with testicular metastasis is
equally sensitive to endocrine and radiation therapy (17). The mean sensitive period for endocrine
treatment is 33 months, while the mean lifetime of prostate cancer
patients following diagnosis is 78 months (14). The present patient had been treated
with endocrine therapy and radiation therapy for 1 month, and the
serum PSA level was slowly being reduced. However, after 1 year of
treatment with endocrine therapy, the patient's serum PSA level
returned to normal. The patient remains under close follow-up.
Acknowledgements
This study was supported by grants from the National
Natural Science Foundation of China (no. 31171097), the Natural
Science Foundation of Hebei Province (no. C2014206419), the Hebei
Province Overseas Returnees Start-up Fund (no. C2012003031) and the
Research Project of Science and Technology of Higher Education of
Hebei Province (nos. ZD2015007 and Z2015005).
References
|
1
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2012. CA Cancer J Clin. 62:10–29. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lozano R, Naghavi M, Foreman K, Lim S,
Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, et
al: Global and regional mortality from 235 causes of death for 20
age groups in 1990 and 2010: A systematic analysis for the Global
Burden of Disease Study 2010. Lancet. 380:2095–2128. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Miller DC, Hafez KS, Stewart A, Montie JE
and Wei JT: Prostate carcinoma presentation, diagnosis, and
staging: An update form the National Cancer Data Base. Cancer.
98:1169–1178. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jemal A, Siegel R, Xu J and Ward E: Cancer
statistics, 2010. CA Cancer J Clin. 60:277–300. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wang SQ, Mecca PS, Myskowski PL and Slovin
SF: Scrotal and penile papules and plaques as the initial
manifestation of a cutaneous metastasis of adenocarcinoma of the
prostate: Case report and review of the literature. J Cutan Pathol.
35:681–684. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kumar S, Shelley M, Harrison C, Coles B,
Wilt TJ and Mason MD: Neo-adjuvant and adjuvant hormone therapy for
localized and locally advanced prostate cancer. Cochrane Database
Syst Rev. 18:CD0060192006.
|
|
8
|
Gleason DF and Mellinger GT: Prediction of
prognosis for prostatic adenocarcinoma by combined histological
grading and clinical staging. J Urol. 111:58–64. 1974.PubMed/NCBI
|
|
9
|
Parwani AV, Marlow C, Demarzo AM,
Mikolajczyk SD, Rittenhouse HG, Veltri RW and Chan TY:
Immunohistochemical staining of precursor forms of
prostate-specific antigen (proPSA) in metastatic prostate cancer.
Am J Surg Pathol. 30:1231–1236. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kessler ER and Flaig TW: Geriatric
considerations in the treatment of advanced prostate cancer. F1000
Prime Rep. 6:332014.
|
|
11
|
Antczak A, Kluźniak W, Wokolorczyk D,
Kashyap A, Jakubowska A, Gronwald J, Huzarski T, Byrski T, Dębniak
T and Masojć B: A common nonsense mutation of the BLM gene and
prostate cancer risk and survival. Gene. 532:173–176. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Cortesi M, Fridman E, Volkov A, Shilstein
SSh, Chechik R, Breskin A, Vartsky D, Raviv G and Ramon J: New
prospective for non-invasive detection, grading, size evaluation
and tumor location of prostate cancer. Prostate. 70:1701–1708.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bubendorf L, Schöpfer A, Wagner U, Sauter
G, Moch H, Willi N, Gasser TC and Mihatsch MJ: Metastatic patterns
of prostate cancer: An autopsy study of 1,589 patients. Hum Pathol.
31:578–583. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Johansson JE and Lannes P: Metastases to
the spermatic cord, epididymis and testicles from carcinoma of the
prostate-five cases. Scand J Urol Nephrol. 17:249–251. 1983.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Pienkos EJ and Jablokow VR: Secondary
testicular tumors. Cancer. 30:481–485. 1972. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Thon W, Mohr W and Altwein JE: Testicular
and epididymal metastasis of prostate cancer. Urologe A.
24:287–290. 1985.(In German). PubMed/NCBI
|
|
17
|
Tu SM, Reyes A, Maa A, Bhowmick D, Pisters
LL, Pettaway CA, Lin SH, Troncoso P and Logothetis CJ: Prostate
carcinoma with testicular or penile metastases. Clinical,
pathologic and immunohistochemical features. Cancer. 94:2610–2617.
2002. View Article : Google Scholar : PubMed/NCBI
|