Introduction
Gastric adenocarcinoma is a common malignant tumor,
and surgical resection is considered to be the most effective
treatment (1,2). The incidence of gastric adenocarcinoma
has declined over time, due to improving living standards,
improvements in early diagnosis, advanced surgical techniques and
combined therapy (surgery, chemotherapy and radiotherapy). However,
distant metastasis and local recurrence are unavoidable in the
majority of cases, and the survival rate and prognosis of gastric
adenocarcinoma patients remains far from satisfactory (1). Despite advances in the elucidation of
the molecular basis of this disease, the spectrum of genes that
have altered expression in gastric adenocarcinoma and the roles
these genes play remain unclear (2).
Therefore, sensitive gastric adenocarcinoma biomarkers that predict
the prognosis and guide effective targeted therapy of patients are
required.
The DEK proto-oncogene (DEK) protein was identified
in a subset of patients with acute myeloid leukemia as a fusion
gene with nucleoporin 214 (3,4). In the majority of aggressive human
tumors, including neuroblastoma, malignant glioma, melanoma, acute
adult leukemia, and bladder and cervical cancer, the DEK gene
frequently exhibits an increased expression level (5–9). In
addition, autoantibodies to DEK have been identified in juvenile
rheumatoid arthritis, systemic lupus erythematosus and sarcoidosis.
Previous studies have suggested that the DEK protein is closely
associated with the apoptosis of cells, since it inhibits
p53-mediated apoptosis, it works in combination with the viral
oncogenes, E6 and E7, to overcome senescence in cells, and it also
promotes Harvey Rat Sarcoma Viral Oncogene Homolog-driven
keratinocyte transformation (4,10–12).
A study by Han et al (13) demonstrated that the DEK protein was
closely associated with the proliferation of serous ovarian tumor
cells, and that the overexpression of DEK was significantly
associated with the increased proliferating index of Ki-67. In the
study, the demonstration that DEK expression is associated with the
proliferative index of cells and cervical cancer is important for
the diagnosis of precancerous lesions. Furthermore, according to
the results from tumor tissue analysis, previous studies reported
that DEK expression was associated with the development of human
colorectal cancer, and was proposed as a novel molecular target for
cancer treatment (14). However, to
the best of our knowledge, there have been no studies to support
the increase in DEK protein expression in patients with gastric
adenocarcinoma. The present study used tissue microarrays (TMAs) to
compare the expression of DEK in gastric adenocarcinoma samples and
adjacent non-cancerous mucosa. In addition, the association between
DEK protein expression, clinicopathological characteristics and
patient survival rates was analyzed.
Materials and methods
Patient samples
A total of 192 cases of gastric adenocarcinoma were
paired with adjacent noncancerous tissues from patients who
underwent surgery between May 2004 and May 2007 at Dandong Central
Hospital (Dandong, Liaoning, China). The patient cohort consisted
of 148 men and 44 women, with a mean age of 49.7 years (range,
29–72 years). All the patients were diagnosed with gastric
adenocarcinoma by pathological examination. Tumor stage was
determined according to the 2010 American Joint Committee on Cancer
Staging Manual (15), and as
previously described (16), was
demonstrated to be closely associated with the prognosis of the
patients: Stage I–II, 122 patients and stage III–IV, 70 patients;
well-differentiated tumor, 60 patients and poorly-differentiated
tumor, 132 patients. The adjacent non-cancerous gastric mucosa
tissues surrounding the tumor were also used in the present study.
None of the patients received chemotherapy prior to surgery.
The study was approved by the Institutional Review
Board and informed written consent was obtained from all the
patients prior to sample collection.
TMAs
The TMAs were produced by Shanghai Xinchao
Biological Technology Co., Ltd., (Shanghai, China) and were
prepared as follows: Tissue cores (diameter of 1.5 mm) were
extracted from paraffin-embedded tissues using a tissue array
instrument (TMArrayer™, Organization Microarrayer; Pathology
Devices Inc., Westminster, MD, USA) and the tissues were arranged
regularly on a paraffin block. The tissue array blocks were heated
at 52°C to fuse the tissue cores to the paraffin. The tissue array
blocks were subsequently processed using a Leica RM2235 Manual
Rotary Microtome (Leica Microsystems GmbH, Wetzlar, Germany; speed,
20 µm/rpm). Up to 80% of the tissue cores were fully exposed. The
tissue array blocks were cut into 4-µm thick sections using the
Leica RM2235 Microtome at a speed of 240 rpm. The cut tissue array
blocks were attached to glass slides, which were heated to 60°C in
an oven for 16 h and subsequently placed in a 5°C refrigerator
until required.
Immunohistochemistry
For the immunohistochemical analysis, a
streptavidin-alkaline phosphatase-labeling method was performed
according to the following protocol: The paraffin biopsy slides
were de-waxed and hydrated in a citrate antigen solution (Beijing
Zhongshan Technology Co., Ltd., Beijing, China). The slides were
subsequently rinsed in phosphate-buffered saline (PBS; Beijing
Zhongshan Technology Co., Ltd.), placed in 30 ml/l hydrogen
peroxide (Beijing Zhongshan Technology Co., Ltd.) for 10 min and
normal serum was added to the slides at 37°C for 15 min. The
following primary antibodies were added to the slides overnight at
4°C: Monoclonal mouse anti-DEK antibody (dilution, 1:50; catalog
no. 610948; BD Biosciences, Franklin Lakes, NJ, USA) and monoclonal
anti-Ki-67 antibody (dilution, 1:50; catalog no. MAB-0672; Fuzhou
Maixin Biotech. Co., Ltd., Fuzhou, China). For the negative
control, the antibody was replaced by PBS. The secondary antibody
was goat anti-mouse immunoglobulin (Ig)G horseradish
peroxidase-conjugated antibody (dilution, 1:500; catalog. no
ZB-2305; Beijing Zhongshan Technology Co., Ltd.), which were
incubated with the slides for 60 min at 37°C. Hematoxylin and eosin
and 3,3′-diaminobenzidine were then added to the slides. DEK and
Ki-67 exhibit nuclear staining. The expression index was determined
by staining intensity and percentage of cells, according to the
following criteria (17): Cells were
scored as ‘−’ (negative, no or <5% positive cells), ‘+’ (0–50%
positive cells), and ‘++’ (>50% positive cells). The positive
descriptor (DEK overexpression) was assigned to ‘++’ scored cells.
For survival analysis, DEK expression level was denoted as high
expression or overexpression (‘++’) and low expression (‘−’ and
‘+’).
Follow-up observation
The 192 cancer patients were followed-up for
survival. On the data of final follow-up (October 30, 2013), 70
patients had died while 122 patients remained alive. The median
survival time was 63 months. The long interval between the final
treatment date and conclusion of follow-up is responsible for the
delay in manuscript submission.
Statistical analysis
Analysis was performed using SPSS version 17.0
(SPSS, Inc., Chicago, IL, USA). The association between DEK
expression and the clinicopathological characteristics of the
patients was evaluated using the χ2 test and Fisher's
exact test. The survival rates of patients following tumor
resection were calculated using the Kaplan-Meier method, and the
difference between survival curves was analyzed using the log-rank
test. Multivariant survival analysis was performed on all the
characteristics using Cox proportional hazard regression model.
P<0.05 was considered to indicate a statistically significant
difference.
Results
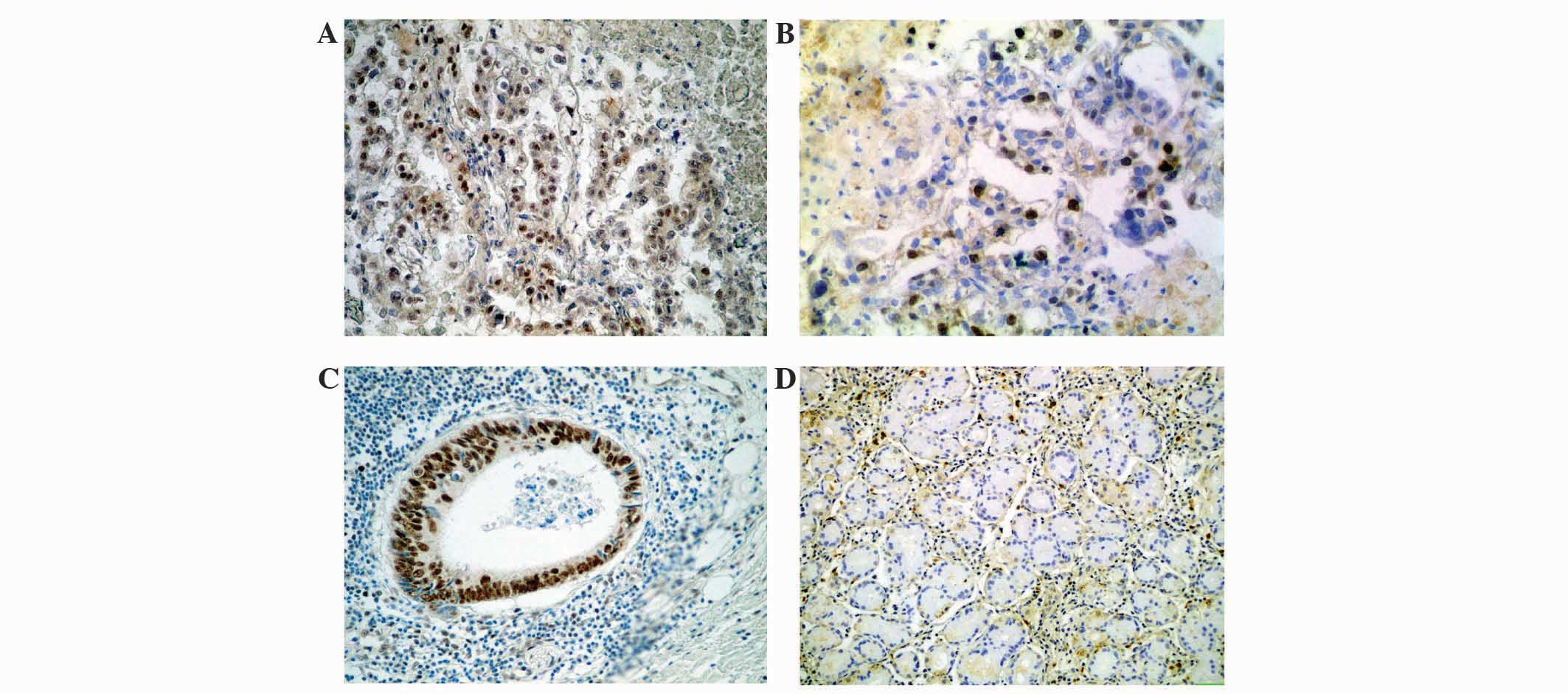
Expression of DEK protein in gastric
adenocarcinoma
The DEK protein was identified as highly expressed
in the cell nuclei of 84 gastric adenocarcinoma (43.8%) and 22
adjacent non-cancerous tissues (11.5%) using immunohistochemistry.
There was consequently a significant difference between cells
classified as overexpressing DEK in the gastric adenocarcinoma
tissues and the adjacent non-cancerous gastric mucosa tissues
(P<0.0001; Fig. 1).
Clinicopathological and prognostic
significance of DEK expression
To elucidate the role of DEK in gastric
adenocarcinoma progression, the present study investigated the
association between DEK protein overexpression and the
clinicopathological characteristics of the patients. Table I reveals that DEK overexpression was
associated with tumor size, tumor grade, lymph node metastasis,
serosal invasion, tumor stage and expression of Ki-67 (P=0.006,
P=0.023, P=0.018, P=0.026, P=0.001 and P=0.003, respectively), but
not with the age and gender of the patients. Furthermore, the
patients with gastric adenocarcinoma with DEK overexpression had a
lower overall survival rate compared with patients with no DEK
overexpression (P<0.0001; Fig
2).
 | Table I.Univariant analysis of the expression
of DEK and various risk factors in 192 patients presenting with
gastric adenocarcinoma. |
Table I.
Univariant analysis of the expression
of DEK and various risk factors in 192 patients presenting with
gastric adenocarcinoma.
|
|
| DEK expression |
|
|
|---|
|
|
|
|
|
|
|---|
| Characteristics | Total, n | ++, n | −/+, n | HR (95% CI) | P-value |
|---|
| Total | 192 | 84 | 108 |
|
|
| Gender |
|
|
|
| 0.078 |
| Male | 148 | 72 | 76 |
|
|
|
Female | 44 | 12 | 32 | 2.526
(0.890–7.170) |
|
| Age, years |
|
|
|
| 0.645 |
| ≥50 | 113 | 51 | 62 |
|
|
|
<50 | 79 | 33 | 46 | 1.147
(0.642–2.049) |
|
| Tumor size, cm |
|
|
|
| 0.006a |
| ≤5 | 108 | 34 | 74 |
|
|
|
>5 | 84 | 50 | 34 | 0.312
(0.135–0.725) |
|
| Tumor grade |
|
|
|
| 0.023b |
| Good | 60 | 19 | 41 |
|
|
| Poor | 132 | 65 | 67 | 0.478
(0.251–0.908) |
|
| LN metastasis |
|
|
|
| 0.018b |
|
Negative | 123 | 46 | 77 |
|
|
|
Positive | 69 | 38 | 31 | 0.487
(0.268–0.887) |
|
| Serosal invasion |
|
|
|
| 0.026b |
|
Negative | 127 | 48 | 77 |
|
|
|
Positive | 65 | 36 | 29 | 0.502
(0.274–0.922) |
|
| TNM stage |
|
|
|
| 0.001a |
|
I–II | 122 | 38 | 84 |
|
|
|
III–IV | 70 | 46 | 24 | 0.236
(0.098–0.571) |
|
| Ki-67 |
|
|
|
| 0.003a |
|
Negative | 74 | 18 | 56 |
|
|
|
Positive | 118 | 66 | 52 | 0.253
(0.102–0.629) |
|
DEK expression is associated with the
survival rate of patients with gastric adenocarcinoma
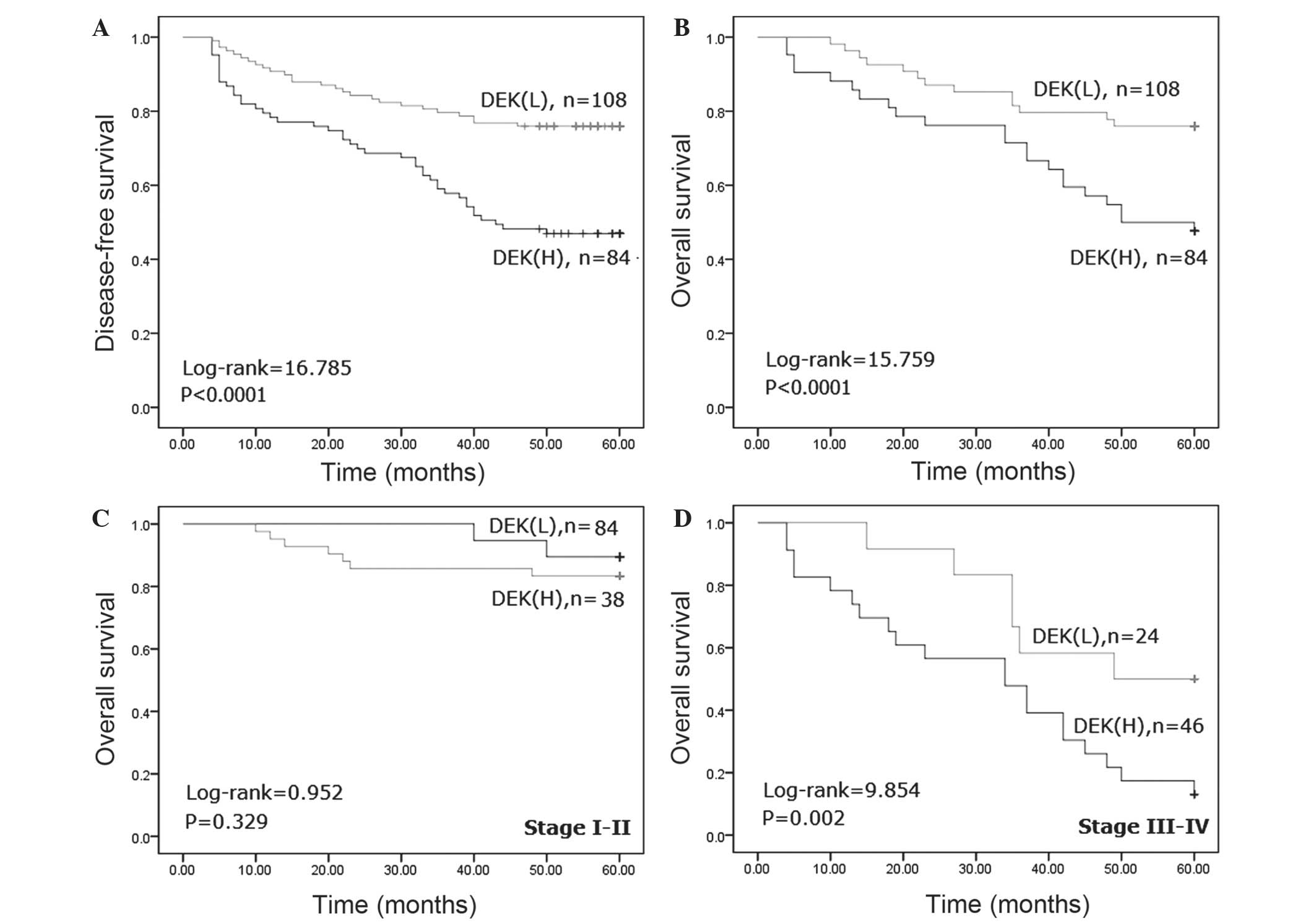
To additionally confirm the role of DEK
overexpression in gastric adenocarcinoma progression, the present
study analyzed the disease-free and overall survival rates for the
192 patients with gastric adenocarcinoma using Kaplan-Meier
survival curves and demonstrated that patients with gastric
adenocarcinoma that overexpressed DEK had lower disease-free
(log-rank, 16.785; P<0.0001) and overall (log-rank, 15.759;
P<0.0001) survival rates compared with patients without DEK
overexpression (Fig. 2A and B).
Furthermore, the present study analyzed the association between the
DEK overexpression rate and the clinical stage of gastric
adenocarcinoma to additionally substantiate the importance of DEK
overexpression in gastric adenocarcinoma progression. The present
analysis identified that patients with late-stage gastric
adenocarcinoma that overexpressed DEK had a lower overall survival
rate compared with patients with late-stage gastric adenocarcinoma
that did not express DEK (P=0.002). However, the overall survival
rate was not associated with the DEK expression status in patients
with early-stage gastric adenocarcinoma (P=0.329) (Fig. 2C and D).
DEK overexpression is an independent
prognostic factor in gastric adenocarcinoma
Univariate analysis for all significant variables
demonstrated that patients that overexpressed DEK had a
significantly lower overall survival rate compared with patients
that did not overexpress DEK (hazards ratio (HR), 0.565; 95%
confidence interval (CI), 0.369–0.866; P=0.009; Table II). Age, lymph node metastasis,
serosal invasion and tumor stage were also associated with the
overall survival rate of the patients. Additionally, multivariate
analysis was performed using the Cox proportional hazards model.
The results demonstrated that tumor stage was an independent
prognostic factor for the survival rate of patients with gastric
adenocarcinoma (HR, 0.663; 95% CI, 0.481–0.915; P=0.012; Table III). Notably, DEK overexpression was
a significant independent prognostic factor in patients with
gastric adenocarcinoma (HR, 0.556; 95% CI, 0.337–0.918; P=0.022;
Table III).
| Table II.Univariate survival analyses of
various characteristics in 192 patients with gastric adenocarcinoma
using the Cox regression model. |
Table II.
Univariate survival analyses of
various characteristics in 192 patients with gastric adenocarcinoma
using the Cox regression model.
|
Characteristics | B | SE | Wald | HR (95% CI) | P-value |
|---|
| DEK | −0.571 | 0.218 |
6.862 | 0.565
(0.369–0.866) | 0.009a |
| Gender | −0.324 | 0.206 |
2.464 | 0.723
(0.483–1.084) | 0.116 |
| Age, years | −0.469 | 0.206 |
5.154 | 0.626
(0.418–0.938) | 0.023b |
| Tumor size, cm | −0.199 | 0.243 |
0.671 | 0.820
(0.509–1.319) | 0.413 |
| Tumor grade | −0.048 | 0.220 |
0.048 | 0.953
(0.619–1.467) | 0.826 |
| LN | −0.485 | 0.215 |
5.116 | 0.616
(0.404–0.937) | 0.024b |
| SI | −0.463 | 0.233 |
3.934 | 0.629
(0.398–0.995) | 0.047b |
| Tumor stage | −0.831 | 0.216 | 14.818 | 0.436
(0.285–0.665) | 0.000a |
| Ki-67 | −0.099 | 0.104 |
0.907 | 0.906
(0.739–1.111) | 0.341 |
| Table III.Multivariant survival analyses of
various characteristics in 192 patients with gastric adenocarcinoma
using Cox regression model. |
Table III.
Multivariant survival analyses of
various characteristics in 192 patients with gastric adenocarcinoma
using Cox regression model.
|
Characteristics | B | SE | Wald | HR (95% CI) | P-value |
|---|
| DEK | −0.587 | 0.256 | 5.275 | 0.556
(0.337–0.918) | 0.022a |
| Age, years | −0.388 | 0.209 | 3.445 | 0.679
(0.451–1.022) | 0.063 |
| LN | −0.331 | 0.223 | 2.193 | 0.718
(0.464–1.113) | 0.139 |
| SI | −0.257 | 0.253 | 1.028 | 0.774
(0.471–1.271) | 0.311 |
| Tumor stage | −0.411 | 0.164 | 6.244 | 0.663
(0.481–0.915) | 0.012a |
Discussion
The DEK gene is located on chromosome 6p22.3
(18); it is a highly conserved
nuclear factor and the only member of its protein class. DEK is
preferentially expressed in proliferating and malignant cells,
which may result in 4–6 million copies per nucleus (19). DEK was originally identified as the
target of a recurrent t(6;9) translocation in a subset of patients
with acute myeloid leukemia (AML). The human DEK protein has been
independently purified as a protein that modulates the topology of
SV40 mini-chromosomes (20) and
consists of 375 amino acids with 4 distinct acidic amino acids, and
has a central SAP box DNA-binding domain and an additional
carboxy-terminal DNA-binding region that partially overlaps with a
multimerization domain. DEK is widely known as a proto-oncogene due
to its involvement in the chromosomal translocation in patients
with AML and its increased expression in multiple human
malignancies (5). Kavanaugh et
al (21) demonstrated that
overexpression of DEK induces human keratinocyte transformation and
that DEK-knockout mice are partially resistant to chemically
induced papilloma formation.
Previous studies have revealed that DEK mRNA
expression is increased in invasive ductal breast cancer, and has
an increased gene expression in high-grade and late-stage breast
cancer, therefore implicating it as a potential novel target in
recurrent tumors (5,22–24). In
addition, Shibata et al (25)
identified that DEK overexpression affects the activity of global
transcriptional regulators and is associated with tumor development
and a poor prognosis of patients with high-grade neuroendocrine
carcinoma. Our previous study indicated that DEK was additionally
significantly correlated with the prognostic characteristics of
patients with colorectal cancer, and DEK depletion by RNAi in
SW-620 and HCT116 cells significantly decreased cell proliferation
and increased cell apoptosis. Upregulation of DEK was involved in
the p53/mouse double minute, B-cell lymphoma 2 family, and caspase
signaling pathways (26). Notably,
certain studies have revealed that DEK expression is associated
with resistance to chemotherapeutic drugs, such as camptothecin,
etoposide, neocarzinostatin and doxorubicin, which is often used to
treat breast cancer (21,27,28).
The present results demonstrated that DEK is
potentially important in the progression of gastric adenocarcinoma.
In total, 43.8% (84/192) of patients with gastric adenocarcinoma
clearly overexpressed the DEK protein. The present study revealed
that DEK overexpression in patients with gastric adenocarcinoma was
associated with the presence of large tumors, a poorer tumor grade,
serosal invasion, lymph node metastasis, increased stage tumors and
Ki-67 expression. Additional analysis demonstrated that DEK
overexpression in gastric adenocarcinoma was associated with the
survival rate of patients and was a significant independent
predictor for the survival of patients with gastric adenocarcinoma
and a high-stage tumor. Therefore, the present study identified DEK
as a potential biomarker for gastric adenocarcinoma in tumor
progression and prognosis. DEK may serve as a useful novel
therapeutic biomarker, particularly for high-stage gastric
adenocarcinoma. However, additional studies are required to confirm
this conclusion.
Acknowledgements
The present study was supported by the Natural
Science Foundation (grant no. 20140082) and the Doctoral Research
Foundation of Eastern Liaoning University. (grant nos. 2014BZ0801
and 2014BZ0802).
References
|
1
|
Wang D, Wang L, Zhou J, Pan J, Qian W, Fu
J, Zhang G, Zhu Y, Liu C, Wang C, Jin Z, He Z, Wu J and Shi B:
Reduced expression of PTPRD correlates with poor prognosis in
gastric adenocarcinoma. PLoS One. 11:e1137542014. View Article : Google Scholar
|
|
2
|
Yang X, Takano Y and Zheng HC: The
pathobiological features of gastrointestinal cancers (Review).
Oncol Lett. 3:961–969. 2012.PubMed/NCBI
|
|
3
|
von Lindern M, Fornerod M, van Baal S,
Jaegle M, de Wit T, Buijs A and Grosveld G: The translocation
(6;9), associated with a specific subtype of acute myeloid
leukemia, results in the fusion of two genes, dek and can and the
expression of a chimeric, leukemia-specific dek-can mRNA. Mol Cell
Biol. 12:1687–1697. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wise-Draper TM, Allen HV, Jones EE, Habash
KB, Matsuo H and Wells SI: Apoptosis inhibition by the human DEK
oncoprotein involves interference with p53 functions. Mol Cell
Biol. 26:7506–7519. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wise-Draper TM, Mintz-Cole RA, Morris TA,
Simpson DS, Wikenheiser-Brokamp KA, Currier MA, Cripe TP, Grosveld
GC and Wells SI: Overexpression of the cellular DEK protein
promotes epithelial transformation in vitro and in vivo. Cancer
Res. 69:1792–1799. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wu Q, Li Z, Lin H, Han L, Liu S and Lin Z:
DEK overexpression in uterine cervical cancers. Pathol Int.
58:378–382. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Orlic M, Spencer CE, Wang L and Gallie BL:
Expression analysis of 6p22 genomic gain in retinoblastoma. Genes
Chromosomes Cancer. 45:72–82. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Carro MS, Spiga FM, Quarto M, Di Ninni V,
Volorio S, Alcalay M and Müller H: DEK expression is controlled by
E2F and deregulated in diverse tumor types. Cell Cycle.
5:1202–1207. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Datta A, Adelson ME, Mogilevkin Y,
Mordechai E, Sidi AA and Trama JP: Oncoprotein DEK as a tissue and
urinary biomarker for bladder cancer. BMC Cancer. 11:2342011.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Mohan S, Abdelwahab SI, Kamalidehghan B,
Syam S, May KS, Harmal NS, Shafifiyaz N, Hadi AH, Hashim NM,
Rahmani M, et al: Involvement of NF-κB and Bcl2/Bax signaling
pathways in the apoptosis of MCF7 cells induced by a xanthone
compound pyranocycloartobiloxanthone A. Phytomedicine.
19:1007–1015. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Khaw AK, Yong JW, Kalthur G and Hande MP:
Genistein induces growth arrest and suppresses telomerase activity
in brain tumor cells. Genes Chromosomes Cancer. 51:961–974. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lupescu A, Jilani K, Zbidah M and Lang F:
Induction of apoptotic erythrocyte death by rotenone. Toxicology.
300:132–137. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Han S, Xuan Y, Liu S, Zhang M, Jin D, Jin
R and Lin Z: Clinicopathological significance of DEK overexpression
in serous ovarian tumors. Pathol Int. 59:443–447. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lin L, Piao J, Gao W, Piao Y, Jin G, Ma Y,
Li J and Lin Z: DEK overexpression as an independent biomarker for
poor prognosis in colorectal cancer. BMC Cancer. 13:366–345. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Edge S, Byrd DR, Compton CC, Fritz AG,
Greene FL and Trotti A: AJCC Cancer Staging Manual (7th). New York,
NY: Springer-Verlag New York. 2010.
|
|
16
|
Marchet A, Mocellin S, Ambrosi A, Morgagni
P, Vittimberga G, Roviello F, Marrelli D, de Manzoni G, Minicozzi
A, Coniglio A, et al: Validation of the new AJCC TNM staging system
for gastric cancer in a large cohort of patients (n=2,155): Focus
on the T category. Eur J Surg Oncol. 37:779–785. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Köbel M, Weichert W, Crüwell K, Schmitt
WD, Lautenschläger C and Hauptmann S: Epithelial hyaluronic acid
and CD44v6 are mutually involved in invasion of colorectal
adenocarcinomas and linked to patient prognosis. Virchows Arch.
445:456–464. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lazăr D, Tăban S, Raica M, Sporea I,
Cornianu M, Goldiş A and Vernic C: Immunohistochemical evaluation
of the tumor neoangiogenesis as a prognostic factor for gastric
cancers. Rom J Morphol Embryol. 49:137–148. 2008.PubMed/NCBI
|
|
19
|
Kappes F, Burger K, Baack M, Fackelmayer
FO and Gruss C: Subcellular localization of the human
proto-oncogene protein DEK. J Biol Chem. 276:26317–26323. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Killeen MR: Integrating a neurobiological
systems approach into child neglect and abuse theory and practice.
J Child Fam Nurs. 2:406–407. 1999.PubMed/NCBI
|
|
21
|
Kavanaugh GM, Wise-Draper TM, Morreale RJ,
Morrison MA, Gole B, Schwemberger S, Tichy ED, Lu L, Babcock GF,
Wells JM, et al: The human DEK oncogene regulates DNA damage
response signaling and repair. Nucleic Acids Res. 39:7465–7476.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Vinnedge Privette LM, McClaine R, Wagh PK,
Wikenheiser-Brokamp KA, Waltz SE and Wells SI: The human DEK
oncogene stimulates β-catenin signaling, invasion and mammosphere
formation in breast cancer. Oncogene. 30:2741–2752. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Abba MC, Sun H, Hawkins KA, Drake JA, Hu
Y, Nunez MI, Gaddis S, Shi T, Horvath S, Sahin A and Aldaz CM:
Breast cancer molecular signatures as determined by SAGE:
Correlation with lymph node status. Mol Cancer Res. 5:881–890.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Rhodes DR, Yu J, Shanker K, Deshpande N,
Varambally R, Ghosh D, Barrette T, Pandey A and Chinnaiyan AM:
ONCOMINE: A cancer microarray database and integrated data-mining
platform. Neoplasia. 6:1–6. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Shibata T, Kokubu A, Miyamoto M, Hosoda F,
Gotoh M, Tsuta K, Asamura H, Matsuno Y, Kondo T, Imoto I, et al:
DEK oncoprotein regulates transcriptional modifiers and sustains
tumor initiation activity in high-grade neuroendocrine carcinoma of
the lung. Oncogene. 29:4671–4681. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lin L, Piao J, Ma Y, Jin T, Quan C, Kong
J, Li Y and Lin Z: Mechanisms underlying cancer growth and
apoptosis by DEK overexpression in colorectal cancer. PLoS One.
9:e1112602014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kappes F, Fahrer J, Khodadoust MS, Tabbert
A, Strasser C, Mor-Vaknin N, Moreno-Villanueva M, Bürkle A,
Markovitz DM and Ferrando-May E: DEK is a poly(ADP-ribose) acceptor
in apoptosis and mediates resistance to genotoxic stress. Mol Cell
Biol. 28:3245–3257. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Khodadoust MS, Verhaegen M, Kappes F, et
al: Melanoma proliferation and chemoresistance controlled by the
DEK oncogene. Cancer Res. 69:6405–6413. 2009. View Article : Google Scholar : PubMed/NCBI
|