Introduction
Liposarcomas originate from primitive mesenchymal
cells (1). According to the World
Health Organization, they are divided into five subtypes:
Dedifferentiated, pleomorphic, myxoid, round cell and
well-differentiated (2). Primary
liposarcomas arising from the mediastinum are uncommon and
constitute <1% of all mediastinal tumors (3). According to statistics reported by Kashu
et al (3), the most common
sites of primary mediastinal liposarcomas are the lower extremities
(75%) and the retroperitoneum (20%). Mediastinal liposarcomas are
insidiously growing tumors, which extend into the pleural spaces or
compress the contiguous structures, including the esophagus, lung,
superior vena cava and pericardium (1). Due to the rarity of this tumor type,
there is currently no standard treatment regime. Complete resection
alone or in combination with chemotherapy or radiotherapy has been
performed by a number of surgeons (4). In addition, mortality and survival rates
of mediastinal liposarcoma remain uncertain, since cases of this
disease are rare. The current study describes a case of recurrent
primary liposarcoma in the mediastinum of a 63-year-old man, with
histopathological and clinical analysis, and review of previously
reported cases in the literature.
Case report
A 63-year old man was referred to Lishui Center
Hospital (Lishui, China) in July 2005 with a 6-month history of
chest pain and increasing dysphagia for 2 month. The patient had a
history of cigarette smoking, but no history of diabetes mellitus,
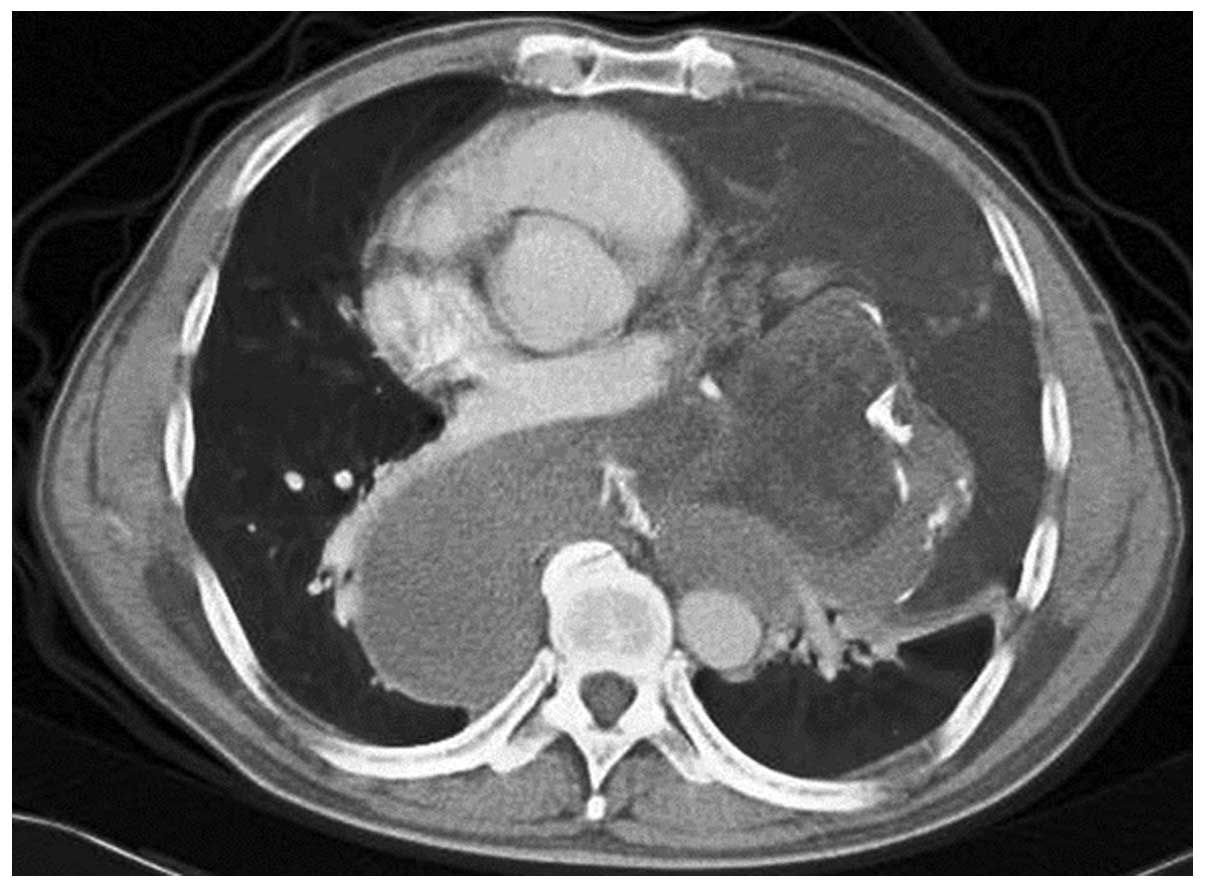
hypertensive disease or coronary disease. A chest computed
tomography (CT) scan (Brilliance iCT; Philips Healthcare,
Amsterdam, The Netherlands) revealed a large mixed solid mass
involving the posterior mediastinum and expanding to the left
pleural cavity (Fig. 1). Other
physical examinations, including electrocardiogram, lung functional
examination and transesophogeal echocardiogram, were normal.
Distant metastasis was not found by head magnetic resonance imaging
(MRI) and abdominal ultrasound. However, as the possibility of
malignancy could not be ruled out, a left posterolateral
thoracotomy was performed in the fourth intercostal space under
general anesthesia on August 3, 2005. During thoracotomy, it was
observed that the tumor tissue was multilobulated and the
pseudocapsule was intact. There was less invasion of the tumor into
the left lung and close adhesion of aortic arch, esophagus
diaphragm, pericardium or left principal bronchus. The tumor was
resected intact, weighed 2,464 g (Fig.
2) and measured 24×22×16 cm in size. Resected tumor tissue was
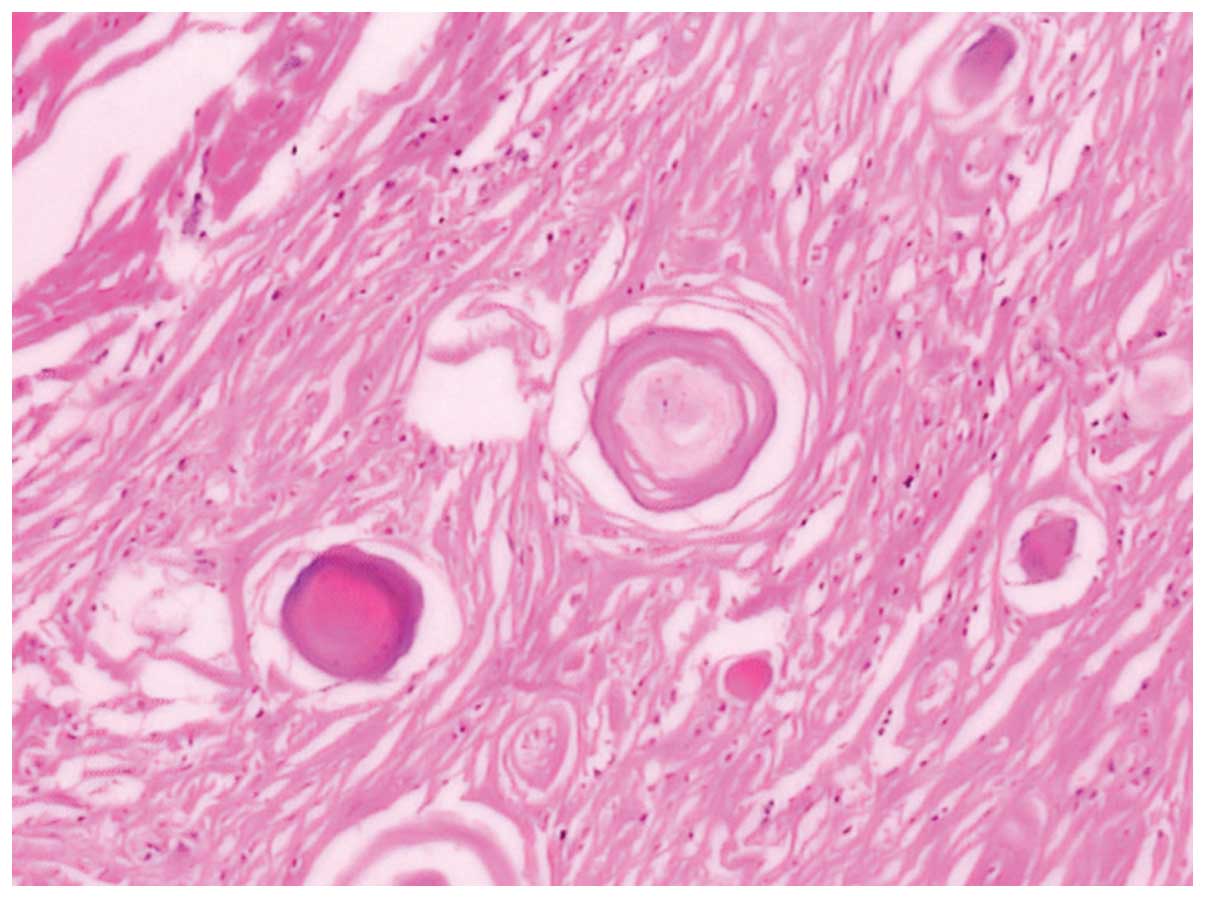
formalin-fixed, paraffin-embedded and cut into 4-µm sections.
Histopathological examination using hematoxylin and eosin staining
(Sinopharm Chemical Reagent Co., Ltd., Shanghai, China) revealed
the tumor to have common histological findings of liposarcomas with
scattered atypical and hyperchromatic stromal cells (Fig. 3) (3).
The patient was discharged on the tenth postoperative day after an
uneventful course. The patient was followed up 6 months later.
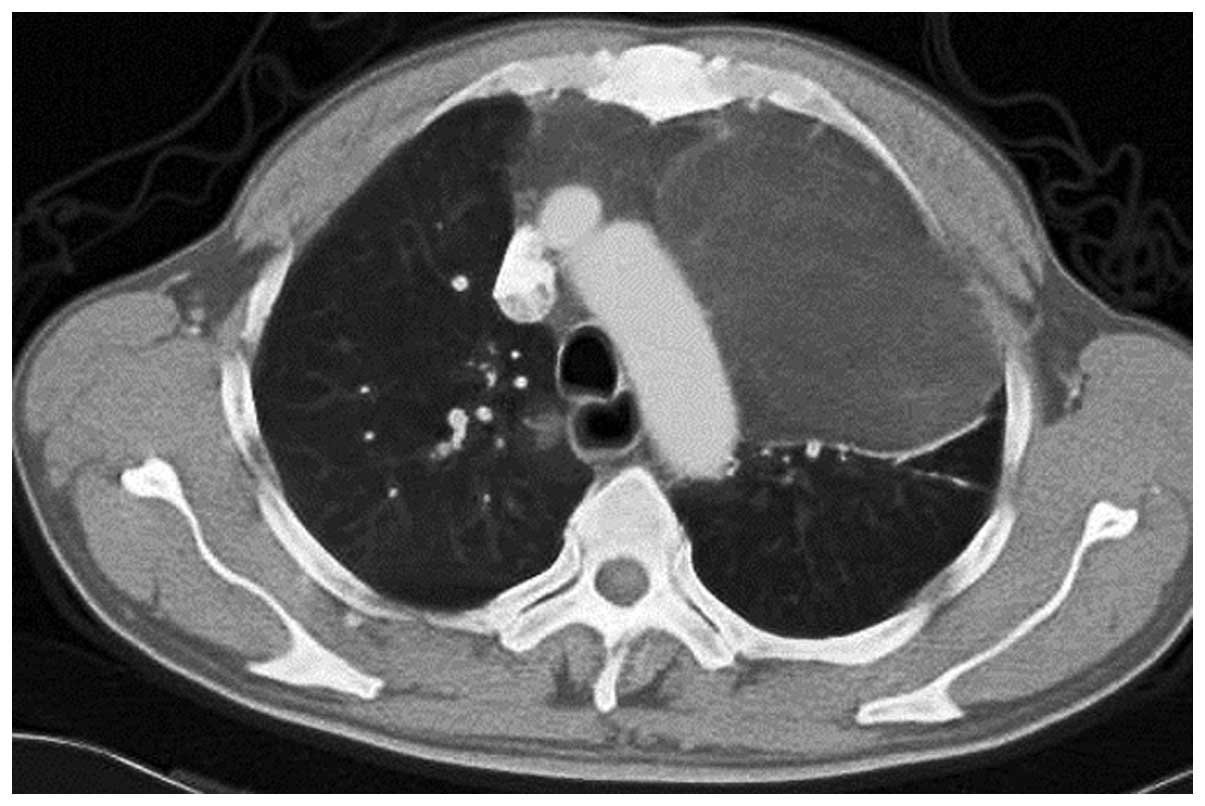
The patient again presented to Lishui Center
Hospital for dysphagia 1 year later in July 2006. A preoperative
chest CT scan revealed a massive anterior mediastinal tumor
expanding to the left pleural cavities (Fig. 4). The tumor was consider to be
recurrent liposarcoma, thus, resective surgery was proposed. A left
anterolateral thoracotomy was performed in the fourth intercostal
space and the tumor was complete resection. The massive tumor
weighed 980 g with dimensions of 16×12×8 cm (Fig. 5). Follow-up CT examinations were
performed every 6 months following surgery, and the patient was
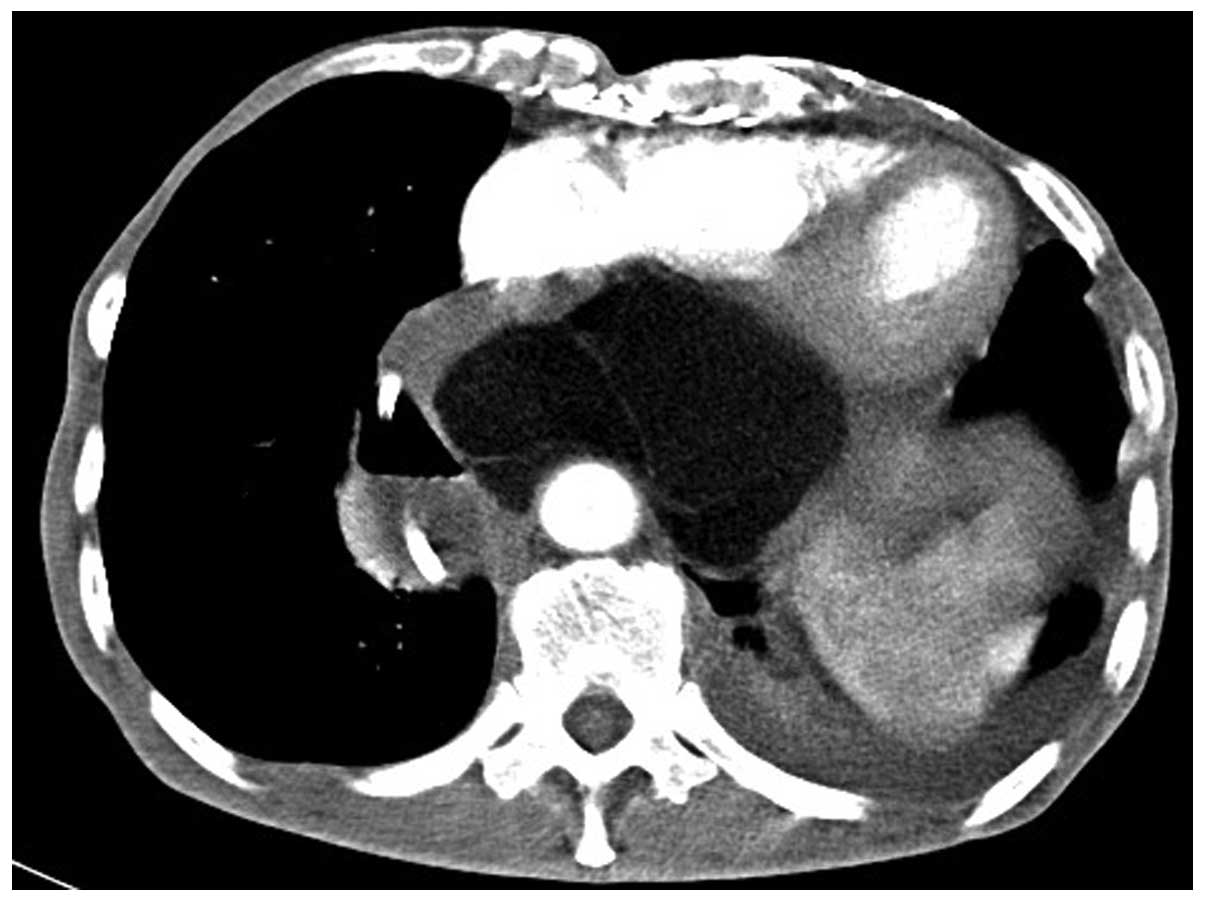
alive 2 years after the second surgery. In August 2008, the patient
again presented with symptoms of dysphagia and a giant tumor was
detected in the posterior mediastinum by chest CT (Fig. 6). However, the patient refused any
treatment and succumbed after 3 months.
Written informed consent was obtained from the
family of the patient for the publication of the present study.
Discussion
Liposarcoma is a mesenchymal tumor that is commonly
derived from adipocytes (5). It is
one of the most frequent malignant soft tissue tumors in adults
(5). However, primary liposarcomas of
the mediastinum are extremely rare. Thus far, <130 cases have
been reported in the published literature (3). According to statistics reported by Kashu
et al (3), the most common
sites of these tumors are the lower extremities (75%) and the
retroperitoneum (20%). In the early stage primary mediastinal
liposarcomas, patients do not typically exhibit any obvious
clinical symptoms. However, as in the present case, patients
present with various different symptoms as the tumor grows,
depending on its location and on the compression of neighboring
structures, such as progressive dysphagia, dyspnea, chest pain,
shortness of breath or hoarseness.
Over several years, the common characteristics of
mediastinal liposarcoma have been increasingly recognized. It is
impossible to be certain whether the mass is benign or malignant by
performing imaging examinations alone, such as chest X-ray, CT and
MRI, and histopathology is used for a definitive diagnosis.
However, they do assist in diagnosing mediastinal liposarcoma; on
MRI, T1-weighted images reveal the fatty tissue with high signal
intensity, whereas in T2-weighted images, the signal intensity
diminishes (6).
Due to of the great variety of histological
presentations, primary mediastinal liposarcoma may be easily
misdiagnosed. Therefore, the differential diagnosis of mediastinal
liposarcomas should include lipoma, teratoma, mesothelioma,
fibrosarcoma, leiomyosarcoma and neurogenic tumor.
The most effective treatment for primary mediastinal
liposarcoma is surgery. The efficacy of this therapeutic method
depends on the extent of resection, with total resection performed
when possible. According to the published literature, aggressive
surgical intervention appears to prolong survival and favor good
quality of life (7). For example,
Kashu et al (3) reported a
case of large mediastinal liposarcoma that was successfully treated
with radical resection. The patient remained alive with no evidence
of disease recurrence at 22 months after the surgery. Furthermore,
Decker et al (4) reported a
case of large mediastinal liposarcoma occupying the majority of the
right chest, and abutting the great vessels and pericardium.
Similar to the present study, a thoracoscopic approach was used for
exploration and surgical excision of this large mediastinal mass.
The patient remained disease-free for almost 3 years after the
resection (8). A few cases also
report the use of radiotherapy, chemotherapy or other methods for
the treatment of primary mediastinal liposarcomas (7); for example, Shoji et al (9) reported the case of a patient with
mediastinal liposarcoma treated by radiofrequency ablation (RFA).
The patient was followed up for an additional 12 months without any
other treatment, and CT revealed that the lesion had not progressed
in size. Therefore, RFA has been demonstrated to be an effective
option for patients who are not well suited to undergo a further
surgical resection (9). A number of
authors consider radiotherapy to be useful in the adjuvant
treatment of unresectable tumors; however, the role of adjuvant
chemotherapy remains controversial (10).
In conclusion, the current study presents a rare
case of liposarcoma arising from the mediastinum in a 63-year-old
man. Tumor resection was successfully performed, however, at a
follow-up examination 12 mouths after surgery, recurrence was
identified in the posterior mediastinum. Subsequently, the tumor
was successfully removed. However, recurrence again occurred in the
posterior mediastinum 2 years later. The patient refused further
treatment and succumbed after 3 months. A diagnosis of mediastinal
liposarcoma was made based on the clinical features, imaging
findings and pathological findings. The current case and previous
studies indicate that careful long-term follow-up with radiological
imaging is necessary to rule out recurrence or metastasis.
References
|
1
|
Punpale A, Pramesh CS, Jambhekar N and
Mistry RC: Giant mediastinal liposarcoma: A case report. Ann Thorac
Cardiovasc Surg. 12:425–427. 2006.PubMed/NCBI
|
|
2
|
Wick MR: The mediastinum. Diagnostic
Surgical Pathology. Sternberg SS and Antonioli DA: (3rd). 1 and
2:Lippincott Williams and Wilkins. (Philadelphia, PA). 1147–1208.
1999.
|
|
3
|
Kashu Y, Yukumi S, Tsunooka N, Tanigawa K,
Arakane M, Nakagawa H and Kawachi K: Successful resection of a
massive mediastinal liposarcoma that rapidly extended into the
entire left thoracic cavity: Report of a case. Surg Today.
42:68–71. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Decker JR, de Hoyos AL and Decamp MM:
Successful thoracoscopic resection of a large mediastinal
liposarcoma. Ann Thorac Surg. 92:1499–1501. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Teschner M and Lüllig H: Diagnosis and
treatment of primary mediastinal liposarcoma. Pneumologie.
57:22–26. 2003.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Munk PL, Lee MJ, Janzen DL, Connell DG,
Logan PM, Poon PY and Bainbridge TC: Lipoma and liposarcoma:
Evaluation using CT and MR imaging. AJR Am J Roentgenol.
169:589–594. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Gasiorowski L, Dyszkiewicz W and Piwkowski
CT: An unusual case of giant primary mediastinal liposarcoma.
Thorac Cardiovasc Surg. 57:247–248. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Meyer M, Holzhausen HJ, Neef H and
Zerkowski HR: Primary liposarcomas of the mediastinum. Langenbecks
Arch Chir Suppl Kongressbd. 115:369–373. 1998.(In German).
PubMed/NCBI
|
|
9
|
Shoji F, Taketomi A, Yano T and Maehara Y:
Intraoperative radiofrequency ablation in an open thoracotomy
setting for the new treatment of mediastinal liposarcoma: Report of
a case. Surg Today. 41:992–994. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Saad R Jr, Dorgan Neto V, Gonçalves R,
Botter M and Siqueira LC: Mediastinal liposarcoma: a case report. J
Bras Pneumol. 34:55–58. 2008.(In Portuguese). View Article : Google Scholar : PubMed/NCBI
|