Introduction
Endometrial cancer is the most frequent malignancy
of the female reproductive system. Approximately 70% of cases with
endometrial cancer belong to stage I, and only 8% present distant
metastases to other organs including the lung, liver and bones
(1). The main treatment for stage I
endometrial cancer is surgery, occasionally followed by
radiotherapy, chemotherapy and/or hormonal therapy if high risk
factors exist. However, 75% of endometrial cancer recurrence occurs
within two or three years of the surgery (2). The three most common recurrent patterns
of endometrial cancer are local invasion, lymphatic spread and
hematogenous spread (3). Vaginal
implantation is extremely rare. Here we present the case of a
77-year-old female with recurrent endometrial carcinoma as a
possible pattern of vaginal implantation metastasis differing from
any of the patterns mentioned above. Written informed consent was
obtained from the patient.
Case report
Patient presentation
A 77-year-old Chinese female, gravid 4, Para 2, who
had experienced the menopause 27 years earlier, was admitted to the
First Affiliated Hospital of Xi'an Jiaotong University (Xi'an
China) with a 5-day history of vaginal bleeding. The patient had a
history of hormone replacement therapy following her menopause.
Speculum examination revealed that the cervix was enlarged and
smooth, and the vagina was smooth. On bimanual examination, the
uterus was observed to be of normal size and the bilateral adnexa
were free. Ultrasound examination of the pelvis revealed an
endometrial thickness of ~6 mm with a 2-cm mass in the uterine
cavity. Fractional endometrial curettage revealed
well-differentiated endometrial adenocarcinoma. The patient's human
papillomavirus infection status was unknown. Positron emission
tomography-computed tomography (PET-CT) of the chest and whole
abdomen revealed no metastatic lesions.
Treatment and findings
The patient's general health was extremely good, and
her routine laboratory examinations were considered normal for her
age. The patient underwent a total abdominal hysterectomy with
bilateral salpingo-oophorectomy. Frozen-section pathological
examination during the surgery revealed well-differentiated
endometrial adenocarcinoma, with the lesion located only in the
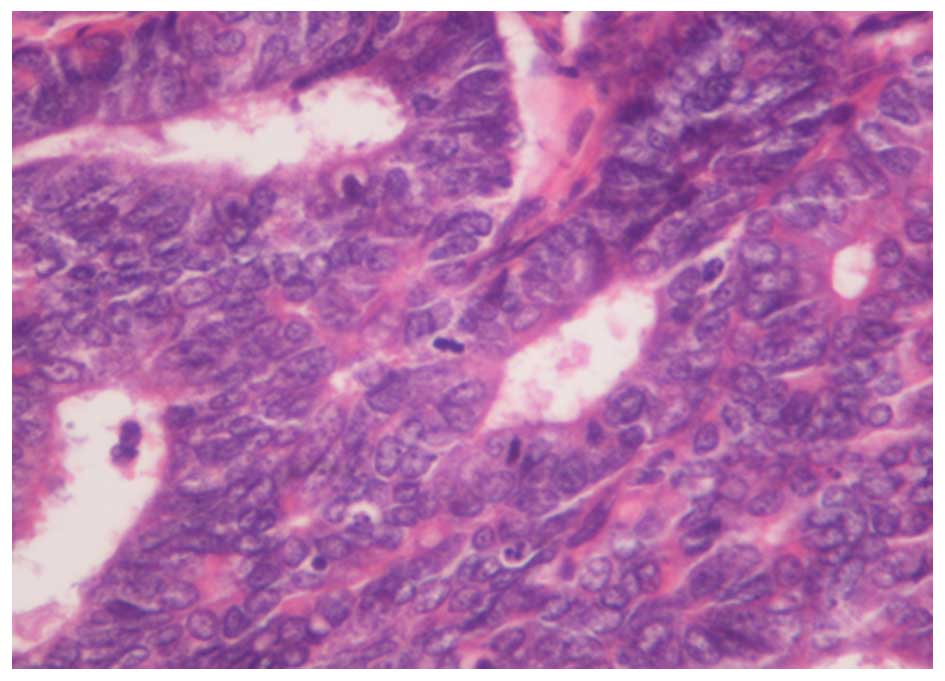
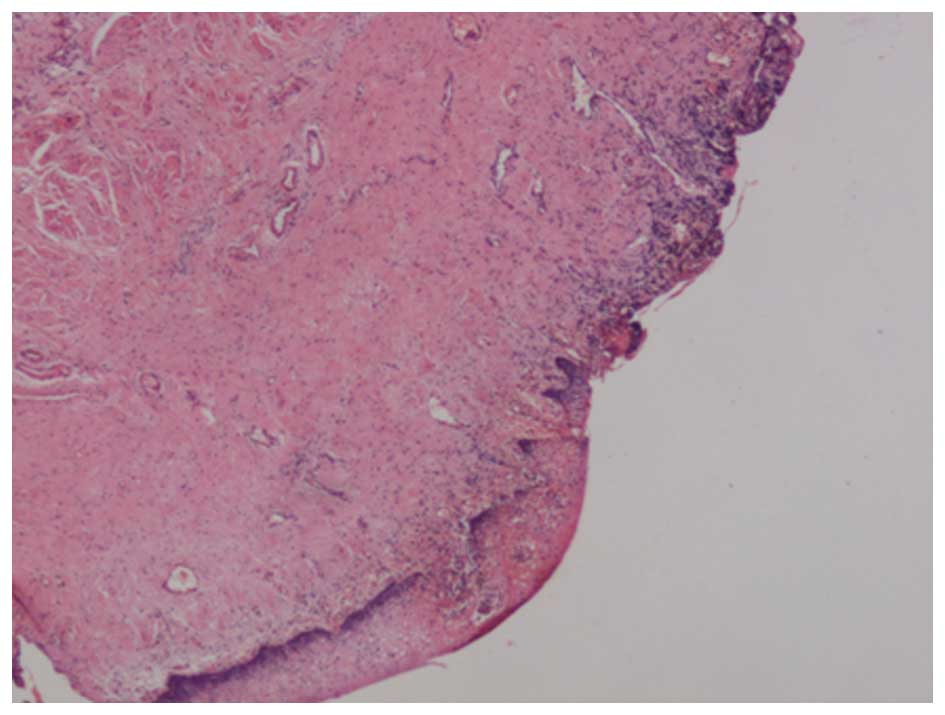
superficial muscle layer of the corpus. Histopathological
examination following surgery revealed grade 1 endometrial
adenocarcinoma (Fig. 1) with the
tumor measuring 10 mm in diameter and myometrial invasion of 4 mm
in depth. No cervical invasion and adnexal metastasis were
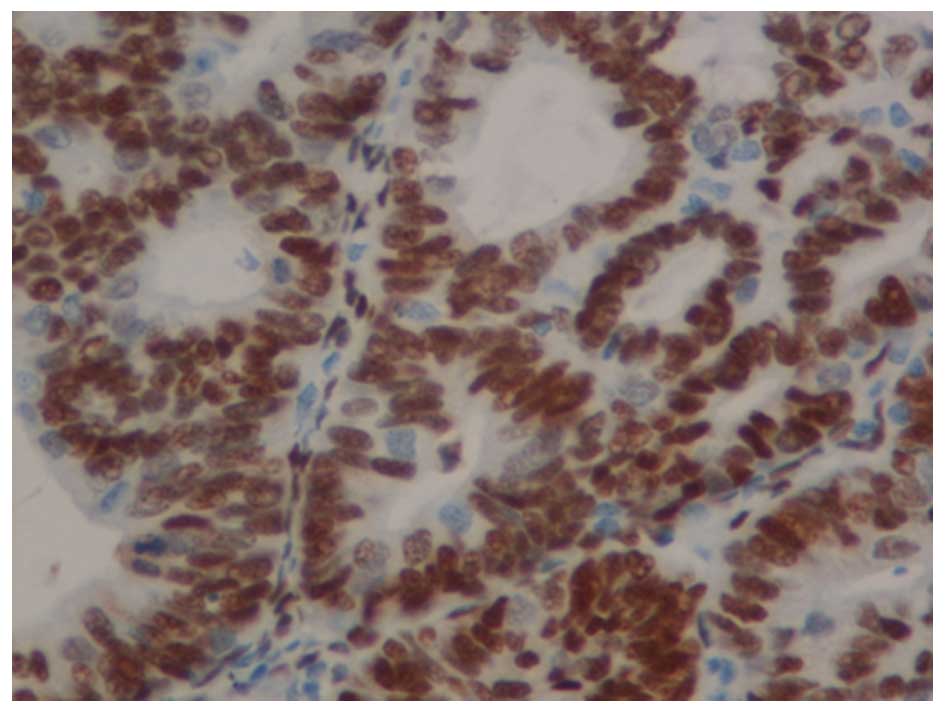
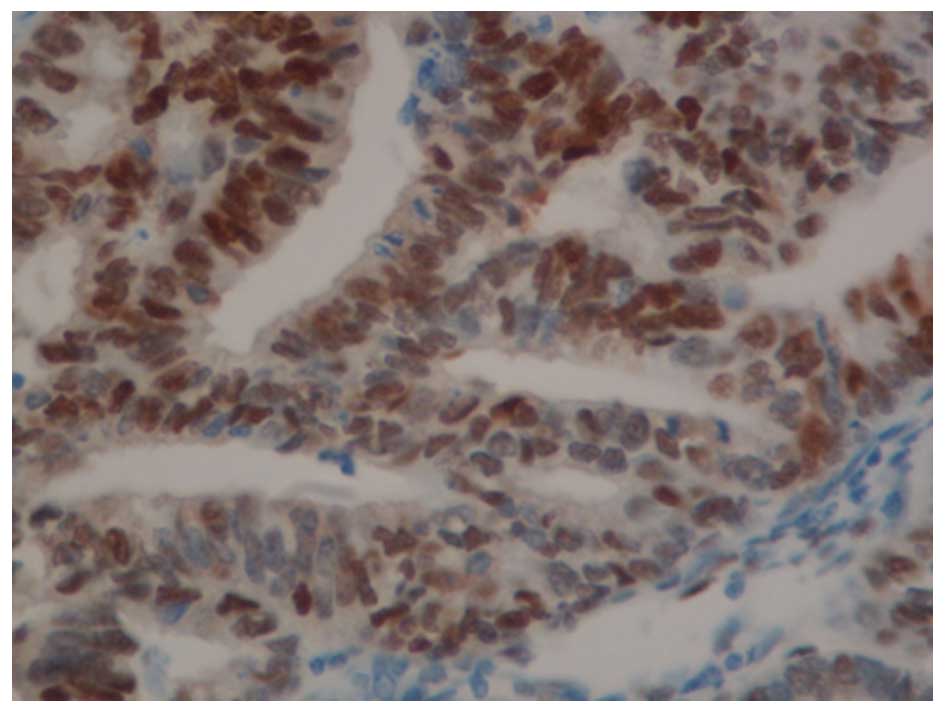
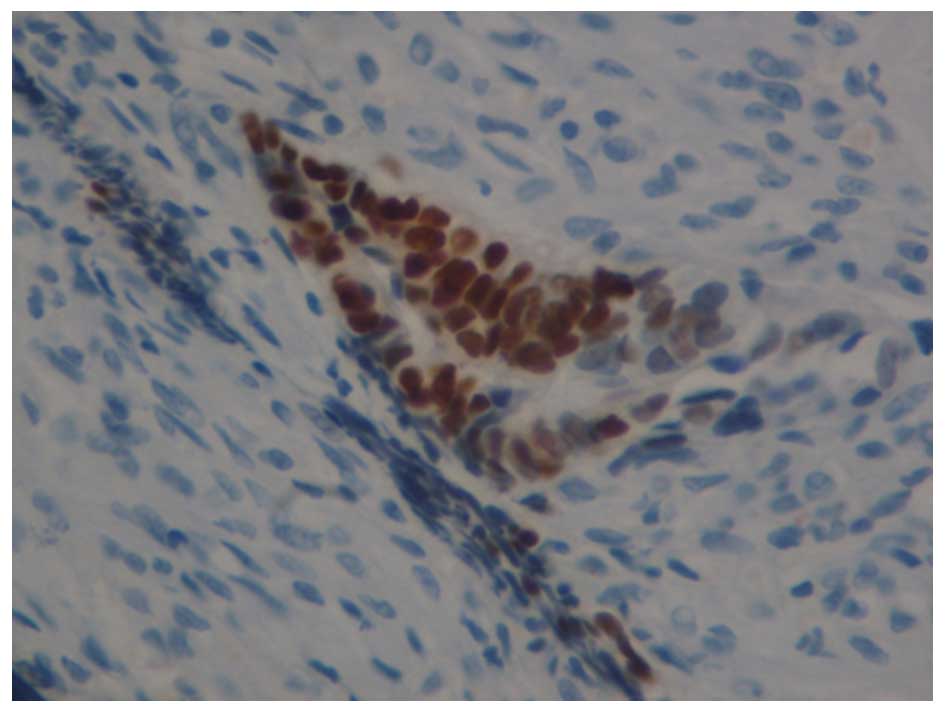
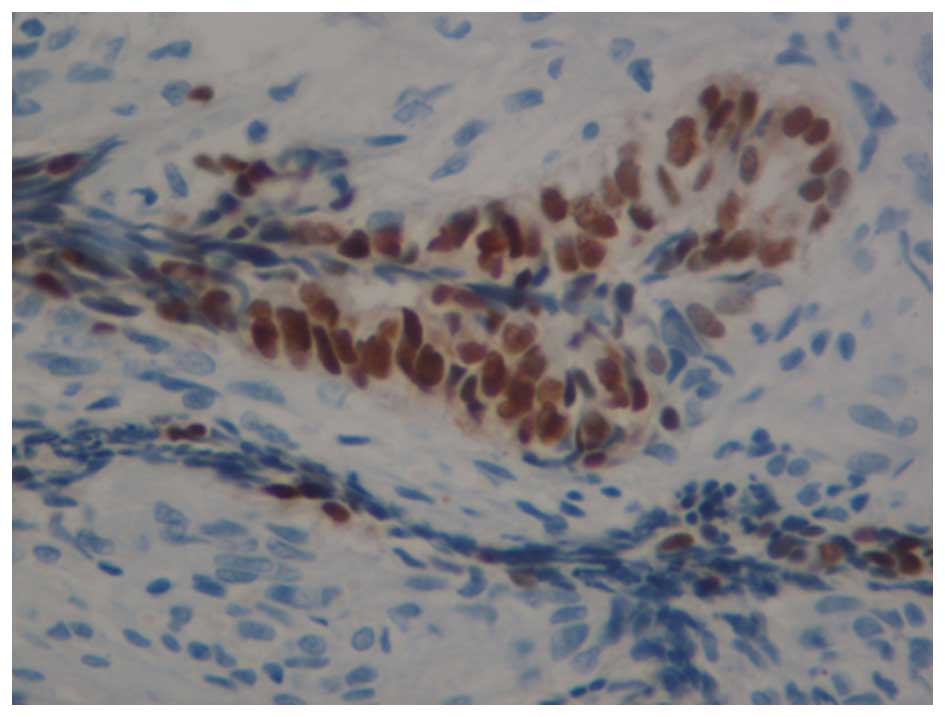
observed. Immunohistochemical staining revealed positivity for
estrogen receptor (ER) and progesterone receptor (PR) (Figs. 2 and 3).
According to the International Federation of Gynecology and
Obstetrics (FIGO) staging system of 2009, the endometrial neoplasm
was assessed as stage IA. The patient did not undergo any adjuvant
treatment following surgery.
Follow-up treatment and final
diagnosis
Half a year after the initial surgery, the patient
experienced occasional bloody vaginal discharge and had vaginal
bleeding for two weeks before her admission. Gynecological
examination revealed a cauliflower-like tumor mass of 15×15×10 mm
at the eight o'clock position on the upper third of the vaginal
wall. PET-CT of the pelvic examination revealed an isolated vaginal
mass. There was some loose tissue detaching during the examination,
and histopathological study of the loose section revealed
well-differentiated endometrial adenocarcinoma. The vaginal mass
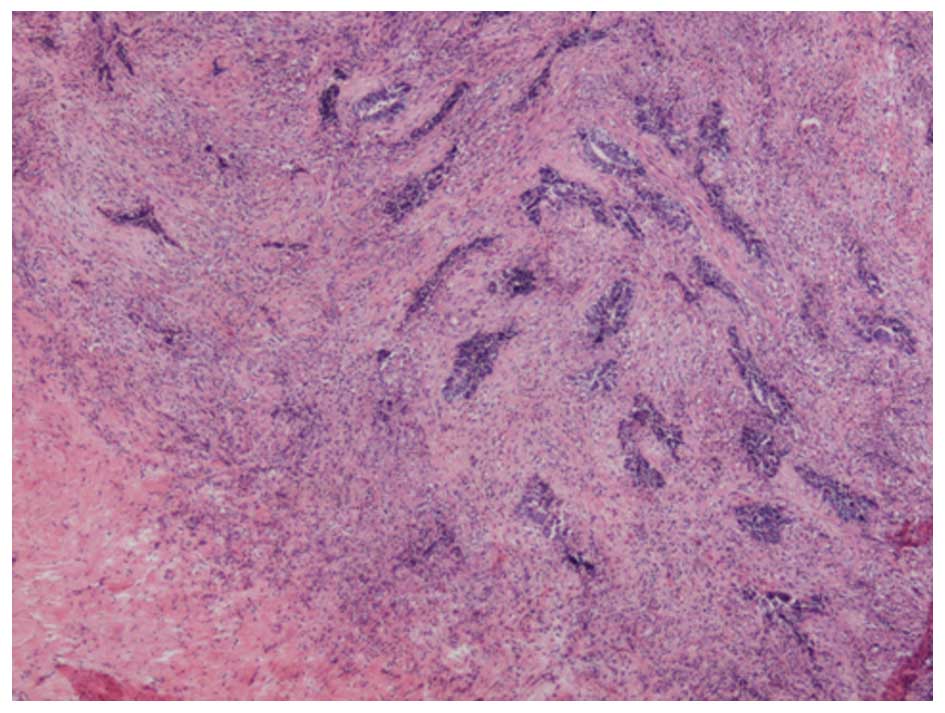
was removed under general anesthesia. Under a microscope following
hematoxylin and eosin staining, the vaginal mucosa was observed to
be damaged, and the superficial squamous epithelium had
disappeared. The carcinoma cells appeared funicular and glandular
in the vaginal mucosa lamina propria infiltration (Fig. 4), and carcinoma tissue fibrosis with
inflammatory cell infiltration was observed (Fig. 5). From this microscopic examination,
we were able to confirm that the tumor was superficial and
localized implantation metastasis. Immunohistochemical staining
revealed that ER and PR were positive in the vaginal tumor tissue
(Figs. 6 and 7). Following treatment, the patient's
vaginal bleeding subsided. The patient had regular follow-ups in
the next year. On the recurrence of endometrial carcinoma, the
patient received an external pelvic radiotherapy (2 Gray/day, days
1–5) and chemotherapy with liposome (135 mg/m2) and
carboplatin (300 mg/m2) following the surgery. Following
that, the patient received vaginal brachytherapy with four
applications of 500 centigray (cGy) (total dose of 2000 cGy).
During the two-year follow-up after treatment, there was no any
sign of recurrence.
Discussion
We deduce that the recurrence of vaginal tumors may
be considered as a type of implantation metastasis. This conclusion
is mainly deduced from pathological examination. It is known that
90% of endometrial cancers are adenocarcinomas, and that most
vaginal cancers are squamous cell carcinomas (4). In the present case, the vaginal tumor
was histologically identical to primary endometrial adenocarcinoma.
The expression of ER and PR was positive in the vaginal tumor as
well as in the endometrial carcinoma. The vaginal mucosa was
damaged and the vaginal squamous epithelium had dissolved. The
carcinoma cells are a funicular and glandular inside the vaginal
mucosa lamina propria infiltration, and carcinoma tissue fibrosis
with inflammatory cell infiltration. Histopathological study
revealed a superficial and localized implantation metastasis tumor.
Moreover, there was no sign of lymphatic or hematogenous spread of
the primary endometrial carcinoma. Therefore, the vaginal mass
could be considered as an implantation metastasis tumor of the
primary endometrial carcinoma.
There is no clear cause of vaginal implantation
metastasis, and how to minimize this implantation remains unclear.
Here, we present several possible mechanisms of vaginal
implantation metastases of endometrial cancer. First of all, the
possible spread pattern may be attributed to iatrogenic transtubal
spill (3). Endometrial adenocarcinoma
cell dissemination during hysteroscopy and saline infusion
sonography may increase the risk of spill. The second possibility
is that high-grade endometrial cancers have implantation capacity,
and as a result, peritoneal invasion (5) or vaginal implantation occurs. The shed
tissue during the examination or surgery of patients with
endometrial cancer may cause endometrial cancer cells to implant in
a suitable location. These cells could survive and be capable of
invasion and metastasis (6).
To avoid implantation metastasis of endometrial
carcinoma in these patients, certain changes may be made in the
surgical procedure. First of all, when surgery for endometrial
cancers is performed, the initial surgical site should be examined
carefully (7), and the surrounding
tissue should be carefully protected to avoid implantation of the
tumor cells. Secondly, cervical cerclage, ligation of the fallopian
tubes and vaginal douching should be performed during surgery to
prevent carcinoma cells from implanting in other organs. Thirdly,
reducing unnecessary gynecological examinations is expected to
lower the possibility of cancer cell dissemination. Further
research should be carried out to establish the actual mechanisms
of vaginal implantation metastases of endometrial carcinoma.
Glossary
Abbreviations
Abbreviations:
|
FIGO
|
International Federation of Gynecology
and Obstetrics
|
|
ER
|
estrogen receptor
|
|
PR
|
progesterone receptor
|
|
PET-CT
|
positron emission tomography-computed
tomography
|
|
cGy
|
centigray
|
References
|
1
|
Ma XG, Wang YM, Sheng HN, Qi Z, Tian WY,
Liu GY and Xue FX: Endometrial cancer metastasize to the skin of
lower leg and vagina: Case report and literature review. Eur J
Gynaecol Oncol. 34:350–352. 2013.PubMed/NCBI
|
|
2
|
Tejerizo-Garcia A, Álvarez-Conejo C,
Muñoz-Hernando L, Guillñn-Gámez C, Seoane-Ruiz JM, Pñrez-Sagaseta C
and Jimñnez-López JS: Tumor recurrence and tumor-related mortality
in endometrial cancer: Analysis in 276 patients. Indian J Cancer.
52:682–684. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Guralp O and Kushner DM: Iatrogenic
transtubal spill of endometrial cancer: risk or myth. Arch Gynecol
Obstet. 284:1209–1221. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Woelber L1, Kock L, Gieseking F, Petersen
C, Trillsch F, Choschzick M, Jaenicke F and Mahner S: Clinical
management of primary vulvar cancer. Eur J Cancer. 47:2315–2321.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Stewart CJ, Doherty DA, Havlat M, Koay MH,
Leung YC, Naran A, O'Brien D, Ruba S, Salfinger S and Tan J:
Transtubal spread of endometrial carcinoma: Correlation of
intra-luminal tumour cells with tumour grade, peritoneal fluid
cytology, and extra-uterine metastasis. Pathology. 45:382–387.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Atallah D, el Kassis N, Lutfallah F, Safi
J, Salameh C, Nadiri S and Bejjani L: Cutaneous metastasis in
endometrial cancer: once in a blue moon - case report. World J Surg
Oncol. 12:862014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nguyen ML, Friedman J, Pradhan TS, Pua TL
and Tedjarati SS: Abdominal wall port site metastasis after
robotically staged endometrial carcinoma: A case report. Int J Surg
Case Rep. 4:613–615. 2013. View Article : Google Scholar : PubMed/NCBI
|