Introduction
Osteomas are benign neoplasms characterized by the
proliferation of compact, lamellar, mature, normal osseous tissue.
The disease presents as an exophytic mass usually arising from the
paranasal sinuses, facial bones, skull or mandible. Subsural
osteomas attached to the meninges unrelated to bone are extremely
rare (1–9). They are most likely located in the
frontal region, according to the literature (1–9). The
initiating factor that triggers the formation of subdural osteoma
remains unclear; however, Choudhury et al (2), Aoki et al (3) and Sugimoto et al (4) have reported that head trauma may trigger
the activation of dural ectopic osteoblasts. Symptomatic subdural
osteomas may present as pressure symptoms or epilepsy, and simple
excision is the treatment of choice for symptomatic lesions. In
this case report, we discuss the radiological and
clinicopathological findings of a subdural osteoma in a 54-year-old
male, and speculate on its etiological mechanism.
Case report
A 54-year-old male presented at Beijing Tiantan
Hospital, Capital Medical University (Beijing, China) in June 2014,
with a 5-month history of intermittent dizziness. He had a history
of right zygomatic fracture 10 years prior without brain injury.
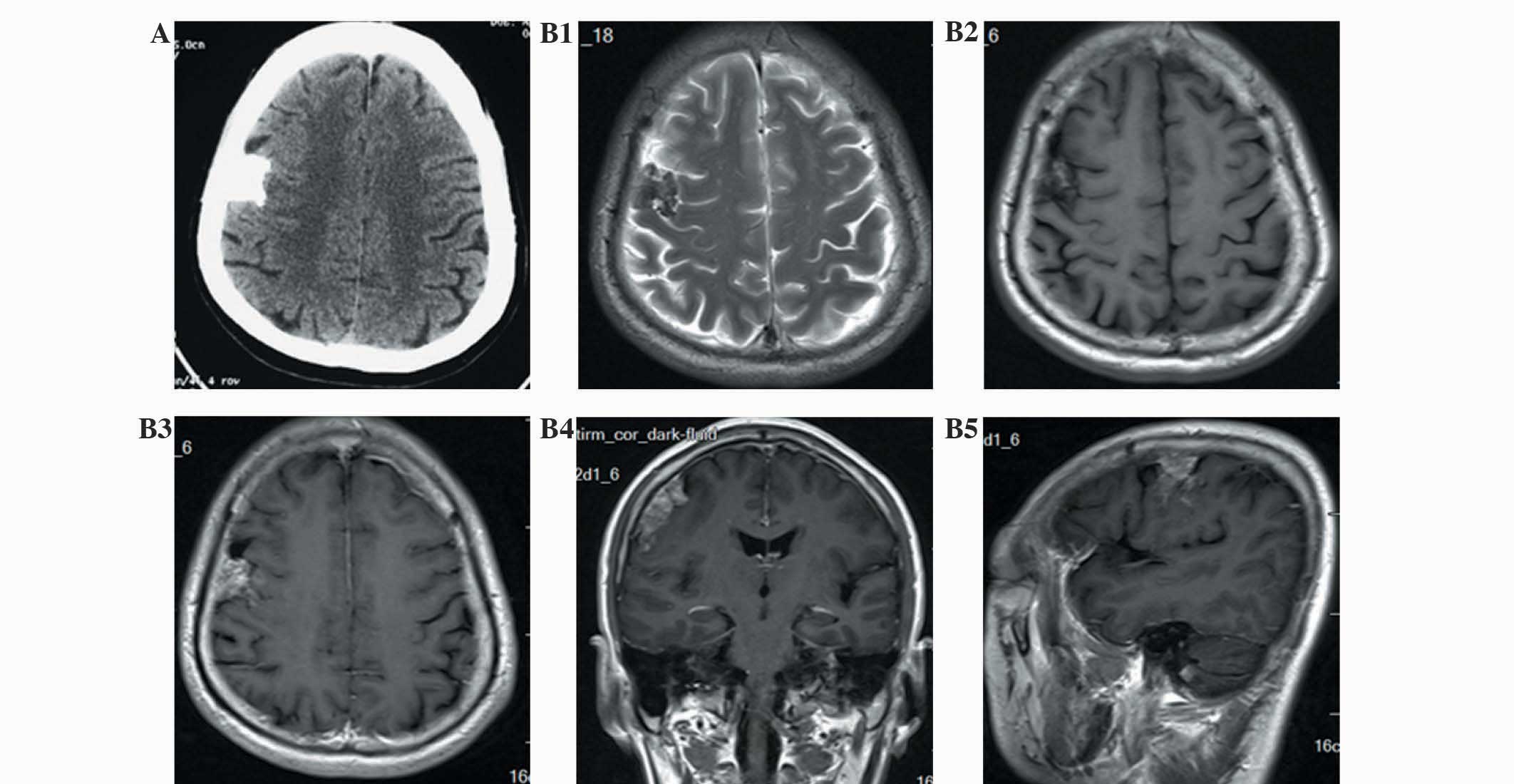
Physical examination revealed no neurological abnormality. A
non-contrast computerized tomography (CT) scan demonstrated a
densely calcified mass beneath the right parietal bone, which
exhibited a mild mass effect upon the right frontal lobe. Magnetic
resonance imaging (MRI) revealed that the mass was iso- and
hyperintense on T1-weighted imaging and iso- and hypointense on
T2-weighted imaging. The mass and the attached dura mater could be
enhanced by gadolinium-diethylenetriamine pentaacetic acid
(Fig. 1). The tumor was misdiagnosed
as calcified meningioma preoperatively, and a right frontal
craniotomy was performed to remove it. The dura mater was observed
to be intact intra-operatively, while the calcified mass attached
to the inner layer of the meninges exhibited no association with
the overlying cranial bone. The lesion was noted to be firm and it
could be easily removed from the arachnoid membrane, so it was
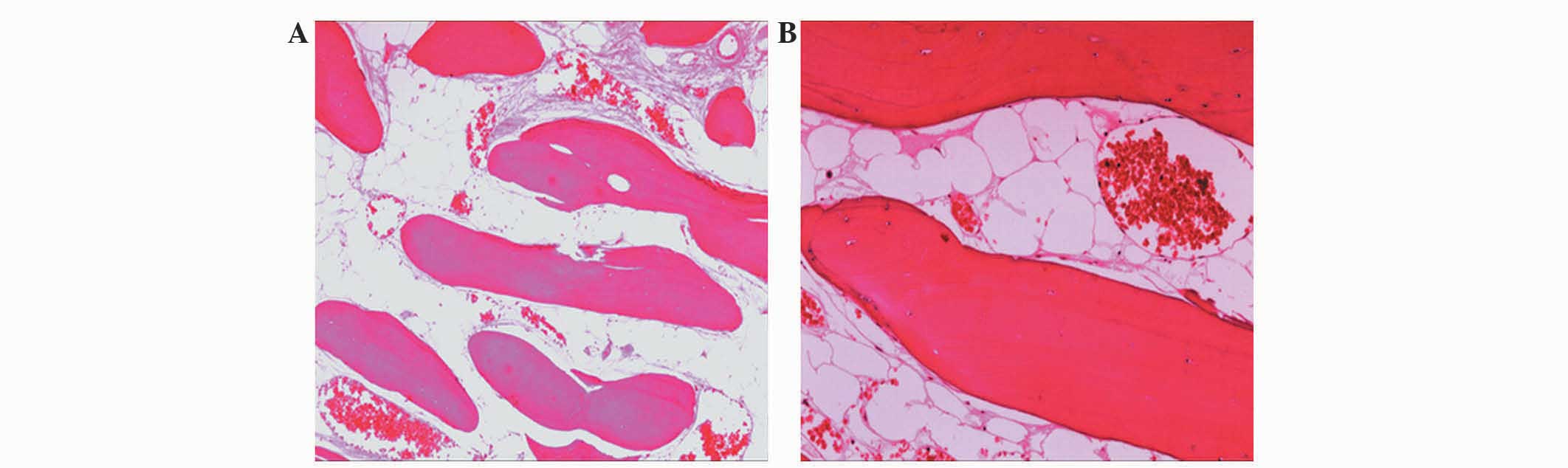
extracted en bloc without cortical injury. Pathological
examination revealed lamellated bony trabeculae lined with
osteoblasts, and the intertrabecular marrow spaces were occupied by
adipose tissue having no active osteoblastic or osteoclastic
activity (Fig. 2). The patient
recovered uneventfully and was discharged without neurological
deficits. The tumor did not recur during the 6-month follow-up
period and the dizziness subsided.
Written informed consent was obtained from the
patient prior to the publication of the present study.
Discussion
Subdural osteoma is recognized as a rare variant of
intracranial osteoma and has an unclear etiology. A reactive
mechanism may have been triggered by trauma in the present case, as
certain authors have suggested previously (2–4). In the
head, the most common anatomic sites are the frontal sinus, the
ethmoidal sinuses and the mandible. However, subdural osteomas
arising from the inner layer of the dura mater with no association
with the covered bone are rarer. We reviewed the literature and
noted that almost all previous cases of subdural osteomas were
attached to the frontal dura or falx (Table I). It was located far more commonly on
the right side than the left side (8:1 ratio). Fallon et al
(9) also observed that intracranial
meningeal osteomas were usually located at the convexity dura and
falx junction around the superior sagittal sinus. The periosteum of
the frontal bones and cells from the nasal septum, which are of
neural crest origin, contribute to the falx cerebri and the
adjacent dura (10). All of these
predilection sites, including the frontal and ethmoidal sinuses and
the mandible, are derived from the embryological neural crest
cells. We speculated that the new bones arise from ectopic
osteoblasts; this hypothesis requires further study.
 | Table I.Cases of solitary subdural osteomas
attached to dura mater without association with bone in the
literature. |
Table I.
Cases of solitary subdural osteomas
attached to dura mater without association with bone in the
literature.
|
Case/author/year/ref. | Age/gender | Location | Symptoms | MRI | Treatment | Surgical
findings | Pathological
findings | Outcome |
|---|
| 1. Dukes et
al, 1965 (1) | 60/M | Right frontal
convexity | Headache | Not available | Right frontal
craniotomy | Attached to dura
mater | Not available | No postoperative
problems |
| 2. Choudhury et
al, 1995 (2) | 20/F | Right frontal
convexity | Headache | Enhanced | Right fronto-temporal
craniotomy | Attached to dura
mater | Contains bone
marrow | Improved |
| 3. Aoki et al,
1998 (3) | 51/F | Right frontal
convexity | Headache | Enhanced | Right frontal
craniotomy | Partially attached to
dura mater | Contains bone
marrow | No postoperative
problems |
| 4. Sugimoto et
al, 2001 (4) | 35/M | Right frontal
convexity | Vertigo | Non-enhanced | Right frontal
craniotomy | Attached to dura
mater | Not available | Not available |
| 5. Cheon et
al, 2002 (5) | 43/F | Left frontal
convexity | Headache | Not available | Left frontal
craniotomy | Attached to dura
mater | No bone marrow | Asymptomatic |
| 6. Jung et al,
2007 (6) | 60/M | Right frontal
convexity | Headache | Not available | Right frontal
craniotomy | Attached to dura
mater | Contains bone
marrow | Improved |
| 7. Barajas et
al, 2012 (7) | 63/F | Right temporal
convexity | Progressively altered
mental status | Non-enhanced | Right
fronto-temperoal craniotomy | Attached to dura
mater | No bone marrow | Improved |
| 8. Chen et al,
2013 (8) | 64/M | Right mesial frontal
lobe extra-axially | Tinnitus with
dizziness | Not available | Right frontal
craniotomy | Attached to falx | Contains bone
marrow | Improved |
| 9. Present case | 54/M | Right frontal
convexity | Dizziness | Enhanced | Right frontal
craniotomy | Attached to dura
mater | Contains bone
marrow | Improved |
This tumor type is mosts commonly associated with
the symptoms of headache or dizziness, which may be due to the
pressure on the underlying cerebral tissue. All patients in the
cases studied presented with headache or dizziness, except one, who
had a progressive, altered mental state (Table I).
On MRI, the appearance of the subdural osteomas was
consistent with that of tumors. Table
I reveals that three of the five subdural osteomas (cases 2, 3
and 9), containing intertrabecular bone marrow, were enhanced by
contrast on MRI, while the enhanced MRI examination was not
available for the other two cases (cases 6 and 8). Case 7,
containing no bone marrow, was not enhanced. Therefore, the context
of intertrabecular bone marrow contributed to the enhancement on
MRI. Calcified meningioma often destroys surrounding bone as a
consequence of extracranial extension (7), although it may also be enhanced on MRI.
Subdural osteomas should be differentially diagnosed from meningeal
ossifications, which are commonly multicentric and located on the
dural-falx junction along both sides of the superior sagittal sinus
(9).
Simple excision is the treatment of choice for
symptomatic lesions. These seldom recur following excision and they
are not associated with malignant change.
References
|
1
|
Dukes HT and Odom GL: Discrete intradural
osteoma. Report of a case. J Neurosurg. 19:251–253. 1962.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Choudhury AR, Haleem A and Tjan GT:
Solitary intradural intracranial osteoma. Br J Neurosurg.
9:557–559. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Aoki H, Nakase H and Sakaki T: Subdural
osteoma. Acta Neurochir (Wien). 140:727–728. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Sugimoto K, Nakahara I, Nishikawa M,
Tanaka M, Terashima T, Yanagihara H and Hayashi J: Osteoma
originating in the dura: a case report. No Shinkei Geka.
29:993–996. 2001.(In Japanese). PubMed/NCBI
|
|
5
|
Cheon JE, Kim JE and Yang HJ: CT and
pathologic findings of a case of subdural osteoma. Korean J Radiol.
3:211–213. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jung TY, Jung S, Jin SG, Jin YH, Kim IY
and Kang SS: Solitary intracranial subdural osteoma: intraoperative
findings and primary anastomosis of an involved cortical vein. J
Clin Neurosci. 14:468–470. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Barajas RF Jr, Perry A, Sughrue M, Aghi M
and Cha S: Intracranial subdural osteoma: a rare benign tumor that
can be differentiated from other calcified intracranial lesions
utilizing MR imaging. J Neuroradiol. 39:263–266. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Chen SM, Chuang CC, Toh CH, Jung SM and
Lui TN: Solitary intracranial osteoma with attachment to the falx:
a case report. World J Surg Oncol. 11:2212013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fallon MD, Ellerbrake D and Teitelbaum SL:
Meningeal osteomas and chronic renal failure. Hum Pathol.
13:449–453. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
O'Rahilly R and Müller F: The meninges in
human development. J Neuropathol Exp Neurol. 45:588–608. 1986.
View Article : Google Scholar : PubMed/NCBI
|