Introduction
As the survival times of non-small cell lung cancer
(NSCLC) patients have been significantly prolonged in recent years,
leptomeningeal metastasis (LM) has exhibited a tendency for
increasing in these patients (1–3). The
median survival time of NSCLC patients with LM is ≤2 months if the
patients do not receive any treatment (1,4).
For the treatment of LM in NSCLC patients, numerous
different interventions and regimens [such as radiotherapy,
epidermal growth factor receptor tyrosine kinase inhibitors (EGFR
TKIs), systemic chemotherapy, intrathecal chemotherapy (ITC)] have
been attempted. Although each intervention has been reported to be
effective, no intervention has been confirmed to be the most
effective (5–14). In fact, the most effective
intervention has not been established for LM from many other types
of tumor (15–18). This is predominantly due to the lack
of randomized clinical trials (RCTs). Despite its rapidly
increasing incidence, LM remains a rare complication of NSCLC. The
very limited number of patients significantly restricts the
implementation of RCTs.
Recently, it was noted that WBRT may have no
contribution to the survival time of patients with LM from NSCLC
(3,10). It has been proposed that ITC may offer
more benefits, according to the results of two retrospective
studies analyzing the connection between treatment and clinical
outcome in NSCLC patients with LM (2). Thus, in order to better evaluate ITC as
a treatment for these particular patients, a pooled analysis of
eligible clinical studies was conducted in the present study.
Patients and methods
Studies
A systematic search of the (http://www.ncbi.nlm.nih.gov/pubmed), OVID (http://ovidsp.ovid.com/autologin.html),
EBSCO (http://search.ebscohost.com), and
Cochrane Library databases (http://www.thecochranelibrary.com) was performed to
identify all clinical studies that contained NSCLC patients with LM
that were treated by ITC. The search strategy included articles
indexed under the subject headings ‘cancer’, ‘tumor’, ‘carcinoma’,
‘neoplasm’, ‘carcinomatosis’, ‘malignancy’, ‘meningitis’,
‘meningeal’, ‘leptomeningeal’, ‘metastasis’ and ‘metastases’. The
latest search was conducted on July 31, 2014. The language was
limited to English. Reviews and case reports were excluded.
Different types of studies were included via different
criteria.
Prospective studies were included according to the
following criteria: i) diagnosis of LM complies with the National
Comprehensive Cancer Network (NCCN) guidelines (19); ii) ITC was administered in prospective
manner, even if few patients received concurrent systemic
chemotherapy; and iii) contains individually assessable information
regarding the therapeutic response or survival of NSCLC patients
with LM. Finally, 4 prospective studies investigating ITC were
included (7,20–22). No
control group was set in all 4 studies.
Retrospective studies were included according to the
following criteria: i) Diagnosis of LM complies with the NCCN
guidelines (19); ii) only analyzed
NSCLC patients with LM; and iii) contains comparable information
regarding response rate or survival related to ITC. There were 5
retrospective studies analyzing LM from NSCLC that were included
(1,10,12,23,24).
Patients
In each prospective study, only the patients
diagnosed with LM from NSCLC were pooled for analysis. As the
prospective studies did not mention which patients were treated by
concurrent systemic chemotherapy, these patients could not be
analyzed separately. All patients in the included retrospective
studies were analyzed. However, all retrospective studies did not
provide the individual information of each patient. Hence, the data
of prospective and retrospective studies could not be
reorganized.
Reevaluation of therapeutic
response
As no standardized criteria for the evaluation of
therapeutic response had been defined or universally agreed at the
time that the included prospective studies were conducted (16), there were some differences in criteria
among these studies. For the feasibility of reevaluating data from
different studies, therapeutic responses of each reevaluable
patient were graded again via the unified criteria defined in the
present study (as follows).
Clinical criteria were defined as follows: Complete
response (CR), resolution of all neurological signs; partial
response (PR), incomplete resolution of neurological signs; stable
disease (SD), no change in clinical signs; progressive disease
(PD), worsening of preexisting or new neurological signs.
Neuroradiographic criteria were defined as follows: CR, resolution
of all neuroradiographic signs; PR, incomplete resolution of
neuroradiographic signs; SD, no change in neuroradiographic signs;
PD, worsening of preexisting or new neuroradiographic signs. For
cytological response, the definitions of CR, PR, SD and PD were
difficult to determine because of the variety of original criteria
in the included studies. Thus, cytological response was graded only
into two levels: With response [improved cerebrospinal fluid (CSF)
cytology]; and without response (worsening CSF cytology or no
change). Although this grading is simple, it was the optimal option
available for the present analysis.
The present clinical and neuroradiographic criteria
are the same as the criteria defined by Chamberlain et al
(7). As the retrospective studies did
not provide individual information, the response rates of these
reports were combined only when necessary.
Reevaluation of survival
The time of survival of reevaluable patients was
calculated on the basis of the records of each original study. The
start point of survival was the onset of LM-directed therapy in
prospective studies, and the diagnosis of LM in retrospective
studies. The end point of survival was mortality of the patient. If
the patient was alive at the end of study, the recorded time was
considered to be their overall survival. Survival curves were
constructed using the Kaplan-Meier method and SPSS 19.0 software
(IBM, Armonk, NY, USA).
Comparison among different studies
(groups)
As the data of prospective and retrospective studies
could not be reorganized, a simple comparison among the included
studies was conducted. To do this, these studies were first
renumbered via a suitable index: Response rate was used as the
numbering index for the comparison of therapeutic response; and
median survival was used as the numbering index for the comparison
of survival. Then, studies were ranked by this number to compare
relevant information.
Results
Studies
The basic information of the included studies is
summarized in Table I. The original
eligibility criteria of patients, criteria of diagnosis and
evaluation of the included studies are summarized in Tables II, III and IV,
respectively.
 | Table I.Design information of the included
studies. |
Table I.
Design information of the included
studies.
| Author, year | Type | Region | Time of
enrolling | N | Objective | Regimen of ITC | Ref. |
|---|
| Chamberlain et
al, 1998 | P | USA |
1986/07-1996/06 | 32 | To evaluate
survival, cause of mortality, and treatment-related toxic effects
in patients undergoing combined modality therapy | MTX, first-line;
Ara-C, second-line; ThioTEPA, third-line | (7) |
| Gwak et al,
2013 | P | Korea |
2009/01-2010/04 | 22 | To define the
maximum tolerated dose, toxicities and pharmacokinetics of VLP
chemotherapy, according to different modes of administration,
perfusion rate and daily MTX dose | MTX, 24–60 mg
daily, bolus or continuous injection, VLP | (20) |
| Nakagawa et
al, 1999 | P | Japan |
1996/01-1998/09 | 23 | To determine the
suited dose of intrathecal 5-FdUrd | 5-FdUrd, dose and
schedule are variable | (21) |
| Nakagawa et
al, 1996 | P | Japan | N/A | 13 | To evaluate the
efficacy and side effects of VLP therapy with MTX and Ara-C | MTX, 10–30 mg/8–12
h; Ara-C, 40 mg/8–12 h, VLP | (22) |
| Lee et al,
2013 | R | Korea | 2001–2009 | 149 | To identify the
clinical features and prognostic factors of NSCLC patients with
LM | MTX | (1) |
| Morris et
al, 2012 | R | USA |
2002/01-2009/12 | 125 | To assess the
impact of WBRT, ITC and EGFR TKIs on outcomes | MTX or liposomal
Ara-C | (10) |
| Umemura et
al, 2012 | R | Japan |
2001/07-2010/09 | 91 | To examine the
prognosis of patients with LM from NSCLC, and that stratified by
EGFR mutation status in LM patients receiving EGFR TKIs | MTX or Ara-C or PSL
or MTX/Ara-C or MTX/PSL or MTX/Ara-C/PSL | (12) |
| Gwak et al,
2013 | R | Korea |
2002/09-2010/12 | 105 | To report clinical
outcomes of ITC for LM from NSCLC | MTX or
MTX/Ara-C/hydrocortisone | (23) |
| Park et al,
2012 | R | Korea | 2003–2009 | 50 | To analyze the
patterns of treatment and clinical outcomes of LM in patients with
NSCLC in the modern chemotherapy era | MTX or ThioTEPA or
MTX/Ara-C/hydrocortisone | (24) |
| Table II.Original eligibility criteria of
patients in the included studies. |
Table II.
Original eligibility criteria of
patients in the included studies.
|
| Inclusion
criteria |
|
|
|---|
|
|
|
|
|
|---|
| Author, year | Diagnosis | Other | Exclusion
criteria | Ref. |
|---|
| Chamberlain et
al, 1998 | LM | Karnofsky
performance status ≥70; expected survival ≥3 months; no prior ITC
patients; desire for further therapy | Patients not
matching the inclusion criteria | (7) |
| Gwak et al,
2013 | LM | Symptoms of
hydrocephalus; increased intracranial pressure (>15 cm
H2O) measured at the subgaleal reservoir; either cauda
equina symptoms or signs of cranial neuropathy | Mass effects | (20) |
| Nakagawa et
al, 1999 | LM | – | – | (21) |
| Nakagawa et
al, 1996 | LM | – | An apparent spinal
mass and spinal block on magnetic resonance imaging | (22) |
| Lee et al,
2013 | LM from NSCLC | – | – | (1) |
| Morris et
al, 2012 | LM from NSCLC | – | – | (10) |
| Umemura et
al, 2012 | LM from NSCLC | – | – | (12) |
| Gwak et al,
2013 | LM from NSCLC | Patients who had
undergone installation of a subgaleal intraventricular reservoir
after informed consent, and received intraventricular chemotherapy
for LM | Patients refused
ITC, or received ITC through lumbar puncture | (23) |
| Park et al,
2012 | LM from NSCLC | – | Patients with
radiological evidence of LM not confirmed by positive cerebrospinal
fluid cytology | (24) |
| Table III.Original diagnosis criteria of LM in
included studies. |
Table III.
Original diagnosis criteria of LM in
included studies.
| Author, year | Original diagnostic
criteria | Ref. |
|---|
| Chamberlain et
al, 1998 | Positive CSF
cytological finding, or CSF abnormalities and clinical syndrome or
neuroradiographic findings consistent with LM | (7) |
| Gwak et al,
2013 | Positive CSF
cytology result | (20) |
| Nakagawa et
al, 1999 | Positive CSF
cytology result | (21) |
| Nakagawa et
al, 1996 | Positive CSF
cytology result | (22) |
| Lee et al,
2013 | Positive CSF
cytology result; CSF exploration was only performed in patients who
developed neurological problems or had abnormal brain imaging | (1) |
| Morris et
al, 2012 | Cytological
evidence of malignant cells on CSF; or neuroimaging (gadolinium
enhanced T1-weighted MRI) consistent with LM, as defined by the
presence of multifocal enhancing subarachnoid nodules | (10) |
| Umemura et
al, 2012 | Diagnosis of LM was
based on the detection of malignant cells in CSF, the typical
findings of subarachnoid tumor cell deposits on MRI, or both | (12) |
| Gwak et al,
2013 | Diagnosis of LM was
based on either the presence of malignant cells in the CSF or on
typical neuroimaging findings (clear leptomeningeal enhancement in
cerebral sulci, cerebellar foliae, spinal cord, cauda equina, or
subependymal lining on the MRI) in patients with an established
diagnosis of systemic malignancy | (23) |
| Park et al,
2012 | Cytological
identification of malignant cells within CSF | (24) |
| Table IV.Original criteria of response
evaluation in studies available for comparison of therapeutic
response. |
Table IV.
Original criteria of response
evaluation in studies available for comparison of therapeutic
response.
| Author, year | Original criteria
of response evaluation | Ref. |
|---|
| Chamberlain et
al, 1998 | Cytological
criteria: CR, 2 consecutive negative CSF (ventricular and lumbar
sampling) cytological examinations at least 1 week apart and
sustained for at least 1 month on a regimen of stable or decreasing
steroid dosage; PR, conversion from positive to suspicious on 2
consecutive CSF (ventricular and lumbar sampling) cytological
examinations at least 1 week apart and sustained for at least 1
month on a regimen of stable or decreasing steroid dosage; PD,
conversion from negative 2 consecutive examinations to positive, or
2 consecutive positive or suspicious cytological findings. Clinical
criteria: CR, resolution of all neurologic signs; PR, incomplete
resolution of neurologic signs; SD, no change in clinical signs;
PD, worsening of preexisting or new neurologic signs.
Neuroradiographic criteria: CR, resolution of all neuroradiographic
signs; PR, incomplete resolution of neuroradiographic signs; SD, no
change in neuroradiographic signs; PD, worsening of preexisting or
new neuroradiographic signs. | (7) |
| Gwak et al,
2013 | Post-treatment ICPs
were measured 3 days after cessation of the VLP (i.e. day 7), to
avoid the immediate effect of VLP (drainage) on the CSF flow. The
other pretreatment symptoms and signs were checked 10 days after
completion of the therapy (day 14). | (20) |
| Nakagawa et
al, 1999 | Cytological
criteria: CR, negative cytology and normal cell counts and tumor
marker levels (cell count ≤10/mm3 and 50 mg/dl protein)
in both ventricular and spinal CSF; PR, ≥50% reduction in either
ventricular or spinal CSF malignant cell count; SD, failure to
fulfill criteria for either a response or progressive disease; PD,
positive cytology in either ventricular or spinal CSF. | (21) |
| Nakagawa et
al, 1996 | Once a week, before
and after perfusion therapy, routine and cytological examination of
the CSF was performed. Clinical criteria: Good, CSF findings were
negative, in association with a moderate to marked improvement of
neurological deficits and the ability to walk unassisted; moderate,
improvement of both CSF parameters and neurological deficits,
regardless of the degree of change; minor, improvement of either
the CSF parameters or the neurological deficits; none, no
improvement of either their neurological deficits or CSF
parameters. | (22) |
| Lee et al,
2013 | No specific
evaluation, just mentioned ‘ITC was administered to 109 patients
(73.2%), and the median number of ITC administrations was 9 (range,
1–27); only 15 patients achieved cytologically negative conversion’
in the text. | (1) |
| Gwak et al,
2013 | Changes of ICP;
other LM-related symptoms were evaluated tentatively as normalized,
improved, stationary, and worsen based on patients' subjective
statements and a physician's description retrieved from the medical
records; cytological criteria are the same as Chamberlain et
al in Ref. 6. | (23) |
| Park et al,
2012 | The response of LM
to ITC was evaluated by cytological findings of the CSF. An
objective systemic response to systemic chemotherapy was assessed
by the Response Evaluation Criteria In Solid Tumors. | (24) |
Patients
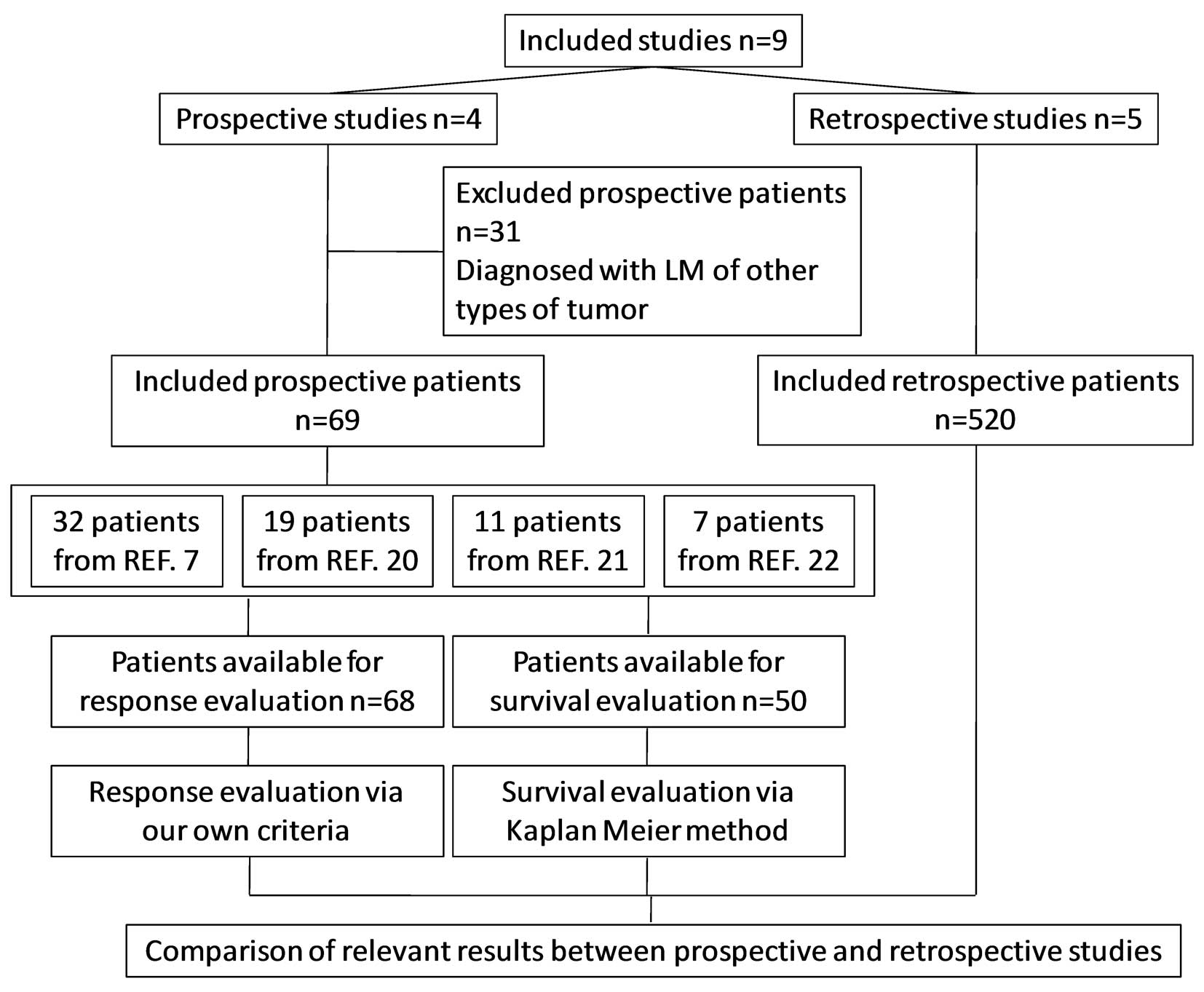
According to the eligibility criteria defined in the
present study, 69 patients in prospective studies and 520 patients
in retrospective studies were pooled for analysis. In detail, 68
patients were reevaluable for analysis of response rate, 50
patients were reevaluable for analysis of survival and 589 patients
were available for comparison (Fig.
1). In total, 37 patients received ITC only, and 552 patients
received multiple interventions (ITC, whole-brain radiotherapy,
EGFR TKI, systemic chemotherapy, and/or support care). The basic
information of pooled patients is summarized in Table V, and the individual information of
reevaluable patients is listed in Table
VI.
| Table V.Patient characteristics (only
patients enrolled in the current study) of included studies. |
Table V.
Patient characteristics (only
patients enrolled in the current study) of included studies.
|
|
| Histology
(NSCLC) |
|
|
|
|
|
|---|
|
|
|
|
|
|
|
|
|
|---|
|
| Enrolled Patients,
N | AD | LCC | SQ | Other | Gender
(male/female), N | Median age, years
(range) | Median KPS
(range) | Patients with a
poor PSa (%) | Ref. |
|---|
| Chamberlain et
al, 1998 | 32 | 24 | 6 | 2 | 0 | 22/10 | 57 (48–73) | 90 (70–100) | 0 | (7) |
| Gwak et al,
2013 | 19 | 18 | 1 | 0 | 0 | 7/12 | 52 (37–67) | 60 (40–90) | 47.4 | (20) |
| Nakagawa et
al, 1999 | 11 | 11 | 0 | 0 | 0 | 3/8 | 59 (48–73) | –b | –b | (21) |
| Nakagawa et
al, 1996 |
7 |
5 | 1 | 1 | 0 | 2/5 | 52 (44–57) | – | 71.4 | (22) |
| Lee et al,
2013 | 149 | 135 | – | – | 14 | 76/73 | 58 (34–80) | – | 13.4 | (1) |
| Morris et
al, 2012 | 125 | 97 | 2 | 4 | 22 | 45/80 | 59 (28–87) | 70 (30–100) | – | (10) |
| Umemura et
al, 2012 | 91 | 83 | 2 | 2 | 4 | 47/44 | 62 (35–79) | – | 42.9 | (12) |
| Gwak et al,
2013 | 105 | 101 | 2 | 2 | 0 | 44/61 | 56 (31–75) | 70 (40–90) | 47.6 | (23) |
| Park et al,
2012 | 50 | 42 | – | 3 | 5 | 25/25 | 62.5 (34–81) | – | 30.0 | (24) |
| Table VI.The individual information of
enrolled prospective patients. |
Table VI.
The individual information of
enrolled prospective patients.
|
| Patient no. |
|
| Data available
for |
|
|---|
|
|
|
|
|
|
|
|---|
|
| New | Original | Age, years | Gender | Response | Survival | Ref. |
|---|
| Chamberlain et
al, 1998 | 1 | 1 | 49 | 22 M/10 F | Y | Y | (7) |
|
| 2 | 2 | 63 |
| Y | Y |
|
|
| 3 | 3 | 61 |
| Y | Y |
|
|
| 4 | 4 | 58 |
| Y | Y |
|
|
| 5 | 5 | 60 |
| Y | Y |
|
|
| 6 | 6 | 73 |
| Y | Y |
|
|
| 7 | 7 | 59 |
| Y | Y |
|
|
| 8 | 8 | 62 |
| Y | Y |
|
|
| 9 | 9 | 56 |
| Y | Y |
|
|
| 10 | 10 | 58 |
| Y | Y |
|
|
| 11 | 11 | 60 |
| Y | Y |
|
|
| 12 | 12 | 62 |
| Y | Y |
|
|
| 13 | 13 | 61 |
| Y | Y |
|
|
| 14 | 14 | 58 |
| Y | Y |
|
|
| 15 | 15 | 54 |
| Y | Y |
|
|
| 16 | 16 | 56 |
| Y | Y |
|
|
| 17 | 17 | 62 |
| Y | Y |
|
|
| 18 | 18 | 65 |
| Y | Y |
|
|
| 19 | 19 | 52 |
| Y | Y |
|
|
| 20 | 20 | 49 |
| Y | Y |
|
|
| 21 | 21 | 61 |
| Y | Y |
|
|
| 22 | 22 | 60 |
| Y | Y |
|
|
| 23 | 23 | 58 |
| Y | Y |
|
|
| 24 | 24 | 56 |
| Y | Y |
|
|
| 25 | 25 | 54 |
| Y | Y |
|
|
| 26 | 26 | 62 |
| Y | Y |
|
|
| 27 | 27 | 48 |
| Y | Y |
|
|
| 28 | 28 | 51 |
| Y | Y |
|
|
| 29 | 29 | 62 |
| Y | Y |
|
|
| 30 | 30 | 49 |
| Y | Y |
|
|
| 31 | 31 | 51 |
| Y | Y |
|
|
| 32 | 32 | 56 |
| Y | Y |
|
| Gwak et al,
2013 | 33 | 1 | 53 | M | Y | N | (20) |
|
| 34 | 2 | 63 | M | Y | N |
|
|
| 35 | 3 | 45 | M | Y | N |
|
|
| 36 | 4 | 45 | M | Y | N |
|
|
| 37 | 5 | 45 | M | Y | N |
|
|
| 38 | 7 | 52 | M | Y | N |
|
|
| 39 | 8 | 49 | F | Y | N |
|
|
| 40 | 9 | 50 | F | Y | N |
|
|
| 41 | 11 | 37 | F | Y | N |
|
|
| 42 | 12 | 62 | F | Y | N |
|
|
| 43 | 13 | 49 | F | Y | N |
|
|
| 44 | 14 | 49 | F | Y | N |
|
|
| 45 | 16 | 67 | F | Y | N |
|
|
| 46 | 17 | 67 | F | Y | N |
|
|
| 47 | 18 | 62 | M | Y | N |
|
|
| 48 | 19 | 52 | F | Y | N |
|
|
| 49 | 20 | 56 | F | Y | N |
|
|
| 50 | 21 | 51 | F | Y | N |
|
|
| 51 | 22 | 42 | F | Y | N |
|
| Nakagawa et
al, 1999 | 52 | 1 | 63 | F | Y | Y | (21) |
|
| 53 | 2 | 65 | F | N | Y |
|
|
| 54 | 3 | 49 | F | Y | Y |
|
|
|
| Patient no. |
|
| Available for |
|
|
|
|
|
|
|
|
| Author, year | New | Original | Age, years | Gender | Response | Survival | Ref. |
|
| Nakagawa et
al, 1999 | 55 | 4 | 56 | F | Y | Y | (21) |
|
| 56 | 7 | 48 | F | Y | Y |
|
|
| 57 | 8 | 70 | M | Y | Y |
|
|
| 58 | 18 | 53 | F | Y | Y |
|
|
| 59 | 19 | 57 | F | Y | Y |
|
|
| 60 | 20 | 58 | F | Y | Y |
|
|
| 61 | 21 | 73 | M | Y | Y |
|
|
| 62 | 22 | 63 | M | Y | Y |
|
| Nakagawa et
al, 1996 | 63 | 1 | 54 | F | Y | Y | (22) |
|
| 64 | 2 | 57 | M | Y | Y |
|
|
| 65 | 3 | 49 | F | Y | Y |
|
|
| 66 | 8 | 54 | F | Y | Y |
|
|
| 67 | 10 | 51 | F | Y | Y |
|
|
| 68 | 11 | 56 | F | Y | Y |
|
|
| 69 | 12 | 44 | M | Y | Y |
|
| Total | 69 |
|
|
| 68 | 50 |
|
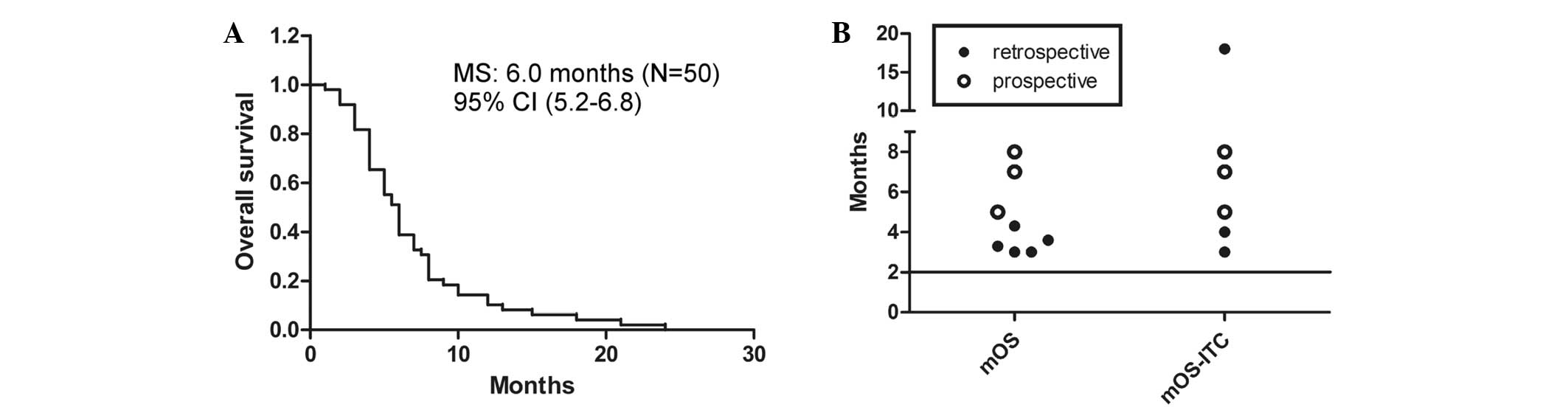
Results of reevaluating patients
The cytological, clinical and neuroradiographic
response rates were 55% (53–60%; n=49), 64% (53–79%; n=58), and 53%
(n=32), respectively (a response was defined as CR plus PR for
clinical and neuroradiological responses). Taking SD into account,
the clinical response rate was 100% when ITC was given by
ventriculolumbar perfusion. The median survival time was 6.0 months
(95% CI, 5.2–6.8; Fig. 2A). The
log-rank test calculated a P-value of 0.017 for the three
comparable groups.
Results of comparing studies. For comparison of
therapeutic response, the studies with available response rates
were ranked according to ascending response rate, and then the
detailed design of matched regimens was summarized (Table VII). The percentage of symptomatic
improvement was markedly higher in studies in which the patients
received ITC only (20,22). If SD is taken into account, the
clinical response rate was 100% in these studies. Notably, the
majority of the patients in these particular studies had a poor
performance status (PS) (Table V).
These results reveal that ITC with a suitable regimen may offer a
promising response rate, particularly for the improvement of
clinical symptoms.
| Table VII.Detailed ITC regimen designs of
comparable retrospective and prospective studies. |
Table VII.
Detailed ITC regimen designs of
comparable retrospective and prospective studies.
|
| Response rate
(%) |
|
|
|
|
|
|
|
|
|
|
|---|
|
|
|
|
|
|
|
|
|
|
|
|
|
|---|
| Rate rank | Cytological | Clinical | Author, year | Drugs | Dose | Frequency | Mode | MT | Median rounds | Check
pointa | End point | Ref. |
|---|
| 1 | 14b | – | Lee et al,
2013 | MTX | 15 mg | x2/w | Injection | 1/w × 4 w, 1/2 w ×
3 mg | 9 | CC | MT | (1) |
| 2 | 25c | 13–42c | Gwak et al,
2013 | MTX
(38f) Triple
(62f) | 15 mg Triple | x2/w ×2/w | Injection | – | 5 |
| Progress | (23) |
| 3 | 52b | 50c | Park et al,
2012 | MTX
(48f) Triple
(69f) ThioTEPA
(31f) | 15 mg Triple 10
mg | x2/w ×2/w ×2/w | Injection | 2/w | 1 | CC | Progress | (24) |
| 4 | 53d | 53d | Chamberlain et
al, 1998e | MTX | 2 mg | x5 cds/2 w, ×8
w | Injection | 5 cds/4 w | – | SI | Progress | (7) |
| 5 | 57d | 71d | Nakagawa et
al, 1996 | MTX/Ara-C | 10–30/40 mg | x6 or 9/3 d | Perfusion | 1/wh | – | CC | Progress | (22) |
| 6 | 60d | – | Nakagawa et
al, 1999 | 5-FdUrd | 1–10 mg | 2–7/w | Injection | – | – | – | Progress | (21) |
| 7 | – | 79d | Gwak et al,
2013 | MTX | 24–60 mg | 3 cds | Perfusion | 1/w | – | SI | Progress | (20) |
All matched survival information of the analyzed
patients in different studies is illustrated in Fig. 2B. The total and ITC-related median
survival times of pooled patients were all >2 months (range,
3.0–18.0 months). Notably, all of the total median survival times
of patients receiving multiple interventions (3.0–5.0 months)
(1,7,10,12,23,24) have a
narrower range and are shorter than that of patients receiving ITC
only (7.5 months) (21,22). Furthermore, the start point of
survival in patients receiving ITC only is later than that in
patients receiving multiple interventions. Additionally, the
percentages of each intervention among the different studies were
evidently different.
LM patients with poor PS have a poor prognosis
(19). However, in the study with the
highest percentage of patients having poor PS (Table II), the median survival time was the
longest (8.0 months) (22). These
results indicate that ITC may offer survival benefits under a
suitable regimen. However, the shorter median survival time and
narrower range of patients receiving multiple interventions is not
associated with poor prognosis, as these patients had better PS
(Table V).
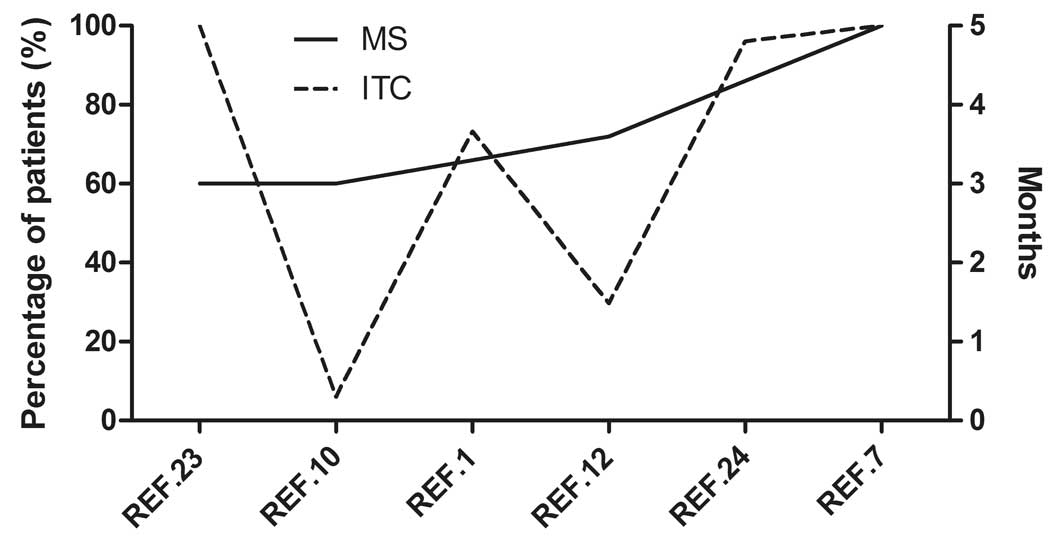
All of the retrospective studies included patients
enrolled between 2000 and 2010 (Table
I). Only two studies (23,24)
excluded some of the patients according to their eligibility
criteria (Table II). Furthermore,
the regimens of ITC among the retrospective studies were also
similar (Tables I and VII). However, the studies involving
multiple interventions had significant heterogeneity with regard to
numerous characteristics, such as race and the percentages of
patients with poor PS and ITC (Tables
I and V; Fig. 3). Additionally, the differences in the
percentages of patients with poor PS and receiving ITC cannot
explain the differences in median survival time among the studies
involving multiple interventions. Hence, there must be other
important factors causing the shortening median survival time and
narrowing of the range in patients receiving multiple
interventions.
For better understanding, the studies with available
survival information were ranked according to the ascending order
of the median survival time values (Table VIII). The matched percentage of
patients receiving each intervention was also calculated and listed
in Table VIII. Notably, the
significant shortening of median survival time was accompanied by a
high percentage of patients receiving multiple interventions. The
effect was enhanced when the interventions were given concurrently.
These results suggest that the shortening of median survival time
and narrowing of the range were caused by the reduction of body
tolerance during repeated treatments, and also the aggravation of
side effects during combination therapy.
| Table VIII.Percentages of intervention in
included studies. |
Table VIII.
Percentages of intervention in
included studies.
| MS rank | MS mOS | mOS-ITC | Author, year | ITC (%) | TKI (%) | SCT (%) | WBRT (%) | SC (%) | Ref. |
|---|
| 1 | 3.0 mo | 3.0 mo | Gwak et al,
2013 | 100.0 | 27.6c | 22.9c | 28.6c | – | (23) |
| 2 | 3.0 mo | 18.0
moa | Morris et
al, 2012 |
6.0 | 14.0 | 16.0 | 45.0 | 30.0 | (10) |
| 3 | 14 wks | 17 wks | Lee et al,
2013 |
73.2 | 16.1 | 16.8 | 43.7 | 13.4 | (1) |
| 4 | 3.6 mo | – | Umemura et
al, 2012 |
29.7 | 56.0 | 29.9 | 23.1 | 25.3 | (12) |
| 5 | 4.3 mo | – | Park et al,
2012 |
96.0 | 28.0 | 24.0 | 42.2c | – | (24) |
| 6 | 5.0 mo | 5.0 mo | Chamberlain et
al, 1998 | 100.0 |
0.0 | 37.5c | 28.1d |
0.0 | (7) |
| 7 | 6.0 mo | 6.0 mo | Present study | 100.0 |
0.0 | 24.0c | 18.0d |
0.0 |
|
| 8 | 7.0 mo | 7.0 mo | Nakagawa et
al, 1999b | 100.0 |
0.0 |
0.0e |
0.0e |
0.0 | (21) |
| 9 | 7.5 mo | 7.5 mo | Present
studyc | 100.0 |
0.0 |
0.0e |
0.0e |
0.0 |
|
| 10 | 8.0 mo | 8.0 mo | Nakagawa et
al, 1996b | 100.0 |
0.0 |
0.0 |
0.0 |
0.0 | (22) |
Bias
The current study is a pooled analysis. All the data
of patients came from published studies. Selection and publication
biases must be considered. Without any doubt, these biases would be
overcome via an RCT. However, the extremely low incidence of LM
makes the implementation of RCTs very challenge and time-consuming.
Prior to the publication of any convincing RCTs, the current study
indeed offers some suggestions for clinical practice.
Discussion
The current study presented a pooled analysis
including the largest number of NSCLC patients with LM. Although
many prospective studies have been conducted to investigate drug
therapy for LM from solid tumors (including NSCLC) (6,25–37), they were not available according to
the criteria defined in the current study. However, these studies
still offer useful information for selecting suitable experimental
drugs and regimens in clinical trials that are aiming to
investigate ITC for the treatment of NSCLC patients with LM
(Table IX).
| Table IX.Relevant information in prospective
studies investigating ITC. |
Table IX.
Relevant information in prospective
studies investigating ITC.
|
| Number of
patients |
| Response, % | Median survival
time (range) |
|
|---|
|
|
|
|
|
|
|
|---|
| Author, year | Total | Lung (NSCLC) | Regimen | Total | Lung (NSCLC) | Total | Lung / NSCLC | Ref. |
|---|
| Wasserstrom et
al, 1982 | 90 | 23 (17) | RT followed by ITC
[MTX (7 mg/m2) or ara-C (30 mg/m2)] | 51.2 | 17.4 (−) | 5.8 mo (1–29) | 4.0 mo (1–10) / − | (6) |
| Hitchins et
al, 1987 | 42 | 16 (3) | MTX (15 mg), or MTX
plus ara-C (50 mg/m2); concurrent RT when needed | 55.0 | − (−) | 8 wks (1–152) | − / − | (25) |
| Grossman et
al, 1993 | 52 | 12 (−) | MTX (10 mg) or
thioTEPA (10 mg); concurrent RT when needed | 23.0 | 33.3 (−) | 15.86 wks (MTX)
14.14 wks (thioTEPA) | − / − | (26) |
| Kim et al,
2003a | 55 | 33 (−) | MTX (15 mg), or MTX
(15 mg) plus hydrocortisone (15 mg/m2) plus ara-C (30
mg/m2); concurrent RT when needed | 25.5/65.5 | 26.7 (16.0) | 11.9 wks
(2.7–28.7) | − / 10.4 vs. 23.9
wks | (27) |
| Yoshida et
al, 2005b | 58 | 12 (9) | MTX, ara-C and
prednisolone | 62.1/53.4 | 33.3/33.3 (−) | 32.8 mo (lymphoma)
18.4 mo (breast) 15.4 mo (others) | 13.0 mo / − | (29) |
| Glantz et
al, 1999 | 61 | 10 (6) | Sustained-release
ara-C (DepoCyt) or MTX; concurrent RT when needed | 23.0 | 30.0 (16.7) | 105 days (DepoCyt)
78 days (MTX) | − / − | (32) |
| Groves et
al, 2008 | 62 | 13 (12) | Topotecan;
concurrent RT when needed | 21.0 | − (−) | 15 wks (13–24) | − / − | (33) |
| Jaeckle et
al, 2002 | 110 | 28 (14) | Sustained-release
ara-C (DepoCyt); concurrent RT when needed | 40.0 | − (−) | 95 days
(7–791) | − / − | (34) |
| Chamberlain et
al, 2002 | 22 | 5
(4) | α-interferon;
concurrent RT when needed | 45.0 | 0.0 (0.0) | 18 wks (5–69) | − / − | (36) |
| Chamberlain et
al, 2006 | 27 | 9
(8) | Etoposide;
concurrent RT when needed | 26.0 | 0.0 (0.0) | 10 wks (4–52) | 9 wks (5–11) / 9
wks (5–11) | (37) |
As there was no individually assessable information,
it was not possible to reevaluate side effects that occurred in
evaluable patients. According to the reporting of each study, the
incidence of side effects was low, and the symptoms were mild,
usually manifesting as slight headache, nausea and fever. There was
an increasing trend in the incidence of side effects in patients
receiving more treatments (7).
Compared with each study, higher response rates are
achieved under suited regimen, particularly under relatively
intensive regimens (e.g., more drug types, higher doses or longer
administration time; Table VII).
Although the higher response rates were predominantly reported by
studies with relative small sample sizes, the low rates reported in
the two retrospective studies with a large sample number (1,23) still
support the need for relatively intensive regimens. Considering
patients also received other kinds of interventions when necessary
(prior to enrolling in the original clinical trial), we speculate
that the need for relatively intensive regimen is determined by the
biological features of NSCLC or the drug tolerance induced by
repeated treatments. As the reported side effects are slight, and
serious side effects are rare, it is worth trying relatively
intensive regimens in patients who are able to tolerate it well. In
fact, Nakagawa et al (21)
attempted to determine patient tolerance by daily dose and weekly
dosage schedule, in order to achieve better efficacy.
The median survival times of pooled patients were
all >2 months. Notably, in patients treated predominantly by
ITC, the longest median survival time was observed (6.0 months).
This may be explained by the type of patients pooled in the current
analysis: Clinical trials reporting shorter median survival times
usually enrolled patients with different types of tumor to expand
the sample size (Table IX) (38).
Tolerance is one of the important factors that
requires consideration when multiple interventions are administered
to a patient. LM from NSCLC indicates the end-stage of disease that
is usually associated with poor PS and low body tolerance. Thus,
suitable combination strategies of multidisciplinary therapy are
extremely important for NSCLC patients with LM. Besides the studies
included in the current analysis, other authors also
retrospectively reported that the median survival time of 30 NSCLC
patients with LM was 6.0 months, with 53% of patients receiving
modern systemic therapy defined as a regimen containing pemetrexed,
bevacizumab or a TKI (39). Another
two Phase II clinical trials also reported that lung cancer
patients receiving concurrent ITC and radiotherapy [3 out of 5
patients (36) and 7 out of 8
patients (37)] exhibited short
survival times without response (36,37). The
indication for radiotherapy in such patients must be better
defined, considering that WBRT does not appear to contribute to
survival (3,10).
EGFR TKI treatment is also considered to be a
significant intervention, particularly to patients with sensitive
mutations (1,11–13,23,24).
Although it was reported that EGFR TKI offered higher response rate
(14) and longer survival time
(12) compared with other
interventions, the studies (12,14) are
still retrospective and has a smaller patient number. Meanwhile,
the selectivity of EGFR TKI treatment limits the scope of
application, and patients are increasingly administered EGFR TKI
treatment prior to the diagnosis of LM, which can lead to the
development of drug tolerance. Incomplete penetration of the drug
is considered to be one of the reasons for treatment failure
(40–42). Although erlotinib exhibits improved
capability of penetration (43) and
disease control (14) compared with
other EGFR TKIs, ITC remains a more direct, less selective and also
well tolerated method of treatment. As the status of EGFR mutation
is not clear for all of the pooled patients, it is not possible to
compare the two interventions in the current study. Future clinical
studies should perform a comparison between ITC and EGFR TKI
treatment.
Recently, experts in LM developed a consensus
proposal [Response Assessment in Neuro-Oncology (RANO) criteria]
for evaluating the response to treatment of patients with LM
(44), considering the lack of
standardization and the importance of criteria for future clinical
trials (38). Unfortunately, this new
criteria was not practicable in the current study. If the new
criteria are used, ITC may not offer such promising response rate,
as the new criteria pay more attention to the cytological and
radiographic responses. However, in NSCLC patients with LM,
survival is the most important indicator of response evaluation,
based on the analyzed results of median survival time. In other
words, symptomatic improvement is the main target for the treatment
of LM in patients with poor prognosis. This must be considered
during the design of future clinical trials, and investigators must
also consider the feasibility of the new RANO criteria in patients
with varying prognoses.
In summary, for NSCLC patients with LM, ITC may
offer promising response rates and survival benefits under suitable
regimen. A suitable combination strategy of multidisciplinary
therapy is important to NSCLC patients with LM.
Acknowledgements
The authors greatly appreciate the valuable comments
and helpful assistance of Dr Kehong Zhang (The Ivy Editing,
Shanghai, China) in preparing the manuscript.
References
|
1
|
Lee SJ, Lee JI, Nam DH, Ahn YC, Han JH,
Sun JM, Ahn JS, Park K and Ahn MJ: Leptomeningeal carcinomatosis in
non-small-cell lung cancer patients: Impact on survival and
correlated prognostic factors. J Thorac Oncol. 8:185–191. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Christoph DC and Reckamp KL:
Intraventricular chemotherapy for leptomeningeal carcinomatosis
from lung cancer: A feasible and beneficial treatment option? J
Thorac Oncol. 8:523–524. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nagpal S, Riess J and Wakelee H: Treatment
of leptomeningeal spread of NSCLC: A continuing challenge. Curr
Treat Options Oncol. 13:491–504. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Waki F, Ando M, Takashima A, Yonemori K,
Nokihara H, Miyake M, Tateishi U, Tsuta K, Shimada Y, Fujiwara Y
and Tamura T: Prognostic factors and clinical outcomes in patients
with leptomeningeal metastasis from solid tumors. J Neurooncol.
93:205–212. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hustu HO, Aur RJ, Verzosa MS, Simone JV
and Pinkel D: Prevention of central nervous system leukemia by
irradiation. Cancer. 32:585–597. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wasserstrom WR, Glass JP and Posner JB:
Diagnosis and treatment of leptomeningeal metastases from solid
tumors: Experience with 90 patients. Cancer. 49:759–772. 1982.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chamberlain MC and Kormanik P: Carcinoma
meningitis secondary to non-small cell lung cancer: Combined
modality therapy. Arch Neurol. 55:506–512. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Liaw CC, Ng KT, Huang JS, Wang CH, Kiu MC
and Lai GM: Meningeal carcinomatosis from solid tumors: Clinical
analysis of 42 cases. J Formos Med Assoc. 91:299–303.
1992.PubMed/NCBI
|
|
9
|
Taillibert S and Hildebrand J: Treatment
of central nervous system metastases: Parenchymal, epidural, and
leptomeningeal. Curr Opin Oncol. 18:637–643. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Morris PG, Reiner AS, Szenberg OR, Clarke
JL, Panageas KS, Perez HR, Kris MG, Chan TA, DeAngelis LM and Omuro
AM: Leptomeningeal metastasis from non-small cell lung cancer:
Survival and the impact of whole brain radiotherapy. J Thorac
Oncol. 7:382–385. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yi HG, Kim HJ, Kim YJ, Han SW, Oh DY, Lee
SH, Kim DW, Im SA, Kim TY, Kim CS, et al: Epidermal growth factor
receptor (EGFR) tyrosine kinase inhibitors (TKIs) are effective for
leptomeningeal metastasis from non-small cell lung cancer patients
with sensitive EGFR mutation or other predictive factors of good
response for EGFR TKI. Lung Cancer. 65:80–84. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Umemura S, Tsubouchi K, Yoshioka H, Hotta
K, Takigawa N, Fujiwara K, Horita N, Segawa Y, Hamada N, Takata I,
et al: Clinical outcome in patients with leptomeningeal metastasis
from non-small cell lung cancer: Okayama lung cancer study group.
Lung Cancer. 77:134–139. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Nakamura Y, Takahashi T, Tsuya A, Naito T,
Kenmotsu H, Ono A, Shukuya T, Murakami H, Harada H, Watanabe R, et
al: Prognostic factors and clinical outcome of patients with lung
adenocarcinoma with carcinomatous meningitis. Anticancer Res.
32:1811–1816. 2012.PubMed/NCBI
|
|
14
|
Lee E, Keam B, Kim DW, Kim TM, Lee SH,
Chung DH and Heo DS: Erlotinib versus gefitinib for control of
leptomeningeal carcinomatosis in non-small-cell lung cancer. J
Thorac Oncol. 8:1069–1074. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chamberlain MC: Leptomeningeal metastasis.
Curr Opin Oncol. 22:627–635. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Le Rhun E, Taillibert S and Chamberlain
MC: Carcinomatous meningitis: Leptomeningeal metastases in solid
tumors. Surg Neurol Int. 4(Suppl 4): S265–S288. 2013.PubMed/NCBI
|
|
17
|
Berg SL and Chamberlain MC: Systemic
chemotherapy, intrathecal chemotherapy, and symptom management in
the treatment of leptomeningeal metastasis. Curr Oncol Rep.
5:29–40. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Martins SJ, Azevedo CR, Chinen LT, Cruz
MR, Peterlevitz MA and Gimenes DL: Meningeal carcinomatosis in
solid tumors. Arq Neuropsiquiatr. 69:973–980. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Brem SS, Bierman PJ, Brem H, Butowski N,
Chamberlain MC, Chiocca EA, DeAngelis LM, Fenstermaker RA, Friedman
A, Gilbert MR, et al: Central nervous system cancers. J Natl Compr
Canc Netw. 9:352–400. 2011.PubMed/NCBI
|
|
20
|
Gwak HS, Lim HS, Shin SH, Yoo H, Han JY,
Kim HT, Yun T, Lee JS and Lee SH: Ventriculolumbar perfusion
chemotherapy for the treatment of leptomeningeal carcinomatosis: A
phase I study with pharmacokinetic data. Am J Clin Oncol.
36:491–499. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Nakagawa H, Yamada M, Maeda N, Iwatsuki K,
Hirayama A and Ikenaka K: Clinical trial of intrathecal
administration of 5-fluoro-2′-deoxyuridine for treatment of
meningeal dissemination of malignant tumors. J Neurooncol.
45:175–183. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Nakagawa H, Fujita T, Kubo S, Izumoto S,
Nakajima Y, Tsuruzono K, Tokiyoshi K and Hayakawa T:
Ventriculolumbar perfusion chemotherapy with methotrexate and
cytosine arabinoside for meningeal carcinomatosis: A pilot study in
13 patients. Surg Neurol. 45:256–264. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Gwak HS, Joo J, Kim S, Yoo H, Shin SH, Han
JY, Kim HT, Lee JS and Lee SH: Analysis of treatment outcomes of
intraventricular chemotherapy in 105 patients for leptomeningeal
carcinomatosis from non-small-cell lung cancer. J Thorac Oncol.
8:599–605. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Park JH, Kim YJ, Lee JO, Lee KW, Kim JH,
Bang SM, Chung JH, Kim JS and Lee JS: Clinical outcomes of
leptomeningeal metastasis in patients with non-small cell lung
cancer in the modern chemotherapy era. Lung Cancer. 76:387–392.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Hitchins RN, Bell DR, Woods RL and Levi
JA: A prospective randomized trial of single-agent versus
combination chemotherapy in meningeal carcinomatosis. J Clin Oncol.
5:1655–1662. 1987.PubMed/NCBI
|
|
26
|
Grossman SA, Finkelstein DM, Ruckdeschel
JC, Trump DL, Moynihan T and Ettinger DS: Randomized prospective
comparison of intraventricular methotrexate and thiotepa in
patients with previously untreated neoplastic meningitis. Eastern
Cooperative Oncology Group. J Clin Oncol. 11:561–569.
1993.PubMed/NCBI
|
|
27
|
Kim DY, Lee KW, Yun T, Park SR, Jung JY,
Kim DW, Kim TY, Heo DS, Bang YJ and Kim NK: Comparison of
intrathecal chemotherapy for leptomeningeal carcinomatosis of a
solid tumor: Methotrexate alone versus methotrexate in combination
with cytosine arabinoside and hydrocortisone. Jpn J Clin Oncol.
33:608–612. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kumthekar P, Grimm SA, Avram MJ, Kaklamani
V, Helenowski I, Rademaker A, Cianfrocca M, Gradishar W, Patel J,
Mulcahy M, et al: Pharmacokinetics and efficacy of pemetrexed in
patients with brain or leptomeningeal metastases. J Neurooncol.
112:247–255. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Yoshida S and Morii K: Intrathecal
chemotherapy for patients with meningeal carcinomatosis. Surg
Neurol. 63:52–55; discussion 55. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
List J, Moser RP, Steuer M, Loudon WG,
Blacklock JB and Grimm EA: Cytokine responses to intraventricular
injection of interleukin 2 into patients with leptomeningeal
carcinomatosis: Rapid induction of tumor necrosis factor alpha,
interleukin 1 beta, interleukin 6, gamma-interferon, and soluble
interleukin 2 receptor (Mr 55,000 protein). Cancer Res.
52:1123–1128. 1992.PubMed/NCBI
|
|
31
|
Chen YM, Chen MC, Tsai CM and Perng RP:
Intrathecal gemcitabine chemotherapy for non-small cell lung cancer
patients with meningeal carcinomatosis-a case report. Lung Cancer.
40:99–101. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Glantz MJ, Jaeckle KA, Chamberlain MC,
Phuphanich S, Recht L, Swinnen LJ, Maria B, LaFollette S, Schumann
GB, Cole BF and Howell SB: A randomized controlled trial comparing
intrathecal sustained-release cytarabine (DepoCyt) to intrathecal
methotrexate in patients with neoplastic meningitis from solid
tumors. Clin Cancer Res. 5:3394–3402. 1999.PubMed/NCBI
|
|
33
|
Groves MD, Glantz MJ, Chamberlain MC,
Baumgartner KE, Conrad CA, Hsu S, Wefel JS, Gilbert MR, Ictech S,
Hunter KU, et al: A multicenter phase II trial of intrathecal
topotecan in patients with meningeal malignancies. Neuro Oncol.
10:208–215. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Jaeckle KA, Batchelor T, O'Day SJ,
Phuphanich S, New P, Lesser G, Cohn A, Gilbert M, Aiken R, Heros D,
et al: An open label trial of sustained-release cytarabine
(DepoCyt) for the intrathecal treatment of solid tumor neoplastic
meningitis. J Neurooncol. 57:231–239. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Sun JM, Nam MH, Chung JY, Im B, Lee SY,
Suh YL, Ahn JS, Park K and Ahn MJ: Safety and pharmacokinetics of
intrathecal administration of pemetrexed in rats. Cancer Chemother
Pharmacol. 68:531–538. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Chamberlain MC: A phase II trial of
intra-cerebrospinal fluid alpha interferon in the treatment of
neoplastic meningitis. Cancer. 94:2675–2680. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Chamberlain MC, Tsao-Wei DD and Groshen S:
Phase II trial of intracerebrospinal fluid etoposide in the
treatment of neoplastic meningitis. Cancer. 106:2021–2027. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Chamberlain M, Soffietti R, Raizer J, Rudà
R, Brandsma D, Boogerd W, Taillibert S, Groves MD, Le Rhun E, Junck
L, et al: Leptomeningeal metastasis: A Response Assessment in
Neuro-Oncology critical review of endpoints and response criteria
of published randomized clinical trials. Neuro Oncol. 16:1176–1185.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Riess JW, Nagpal S, Iv M, Zeineh M, Gubens
MA, Ramchandran K, Neal JW and Wakelee HA: Prolonged survival of
patients with non-small-cell lung cancer with leptomeningeal
carcinomatosis in the modern treatment era. Clin Lung Cancer.
15:202–206. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Heimberger AB, Learn CA, Archer GE,
McLendon RE, Chewning TA, Tuck FL, Pracyk JB, Friedman AH, Friedman
HS, Bigner DD and Sampson JH: Brain tumors in mice are susceptible
to blockade of epidermal growth factor receptor (EGFR) with the
oral, specific, EGFR-tyrosine kinase inhibitor ZD1839 (iressa).
Clin Cancer Res. 8:3496–3502. 2002.PubMed/NCBI
|
|
41
|
Omuro AM, Kris MG, Miller VA, Franceschi
E, Shah N, Milton DT and Abrey LE: High incidence of disease
recurrence in the brain and leptomeninges in patients with nonsmall
cell lung carcinoma after response to gefitinib. Cancer.
103:2344–2348. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Palmieri D, Chambers AF, Felding-Habermann
B, Huang S and Steeg PS: The biology of metastasis to a sanctuary
site. Clin Cancer Res. 13:1656–1662. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Togashi Y, Masago K, Masuda S, Mizuno T,
Fukudo M, Ikemi Y, Sakamori Y, Nagai H, Kim YH, Katsura T and
Mishima M: Cerebrospinal fluid concentration of gefitinib and
erlotinib in patients with non-small cell lung cancer. Cancer
Chemother Pharmacol. 70:399–405. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Chamberlain MC, Junck L, Brandsma D,
Soffietti R, Raizer JJ, Ruda R, Boogerd W, Taillibert S, Groves MD,
Le Rhun E, et al: Leptomeningeal metastases: A rano proposal for
response criteria. J Clin Oncol (suppl). 32:abstr e13019. 2014.
|