Introduction
Ovarian cancer is the second most prevalent cancer
and the leading cause of mortality in women amongst all
gynecological malignancies, with epithelial ovarian cancer (EOC)
accounting for >95% of all ovarian cancer cases (1,2). As it is
difficult to detect the disease at early stages, the majority of
patients with EOC have advanced-stage disease at the time of
diagnosis. EOC metastasizes and transfers easily, is recurrent and
is also resistant to chemotherapy, thus resulting in high mortality
rates (3,4). Currently, the 5-year survival rate of
patients with EOC remains at <50% despite recent advances in
chemotherapeutic agents and cytoreductive surgery (5). Platinum-based therapy is the first-line
chemotherapy regimen for EOC; however, platinum-resistance is a
major factor affecting patient prognosis (6,7). If the
potential sensitivity of platinum chemotherapy and prognosis is
able to be predicted prior to treatment, it may guide
individualized treatment, protect patients from inappropriate
chemotherapy and reduce the occurrence of secondary resistance.
Nucleotide excision repair (NER) is a versatile DNA
repair system that identifies platinum-based therapy-induced DNA
damage (8). The excision repair
cross-complementation group 1 (ERCC1) gene is critical within NER
and serves a leading role in this pathway (9,10).
Cisplatin-resistant ovarian cancer exhibits increased expression of
ERCC1 (11–13). Steffensen et al (13) reported that patients with
ERCC1-negative tumors had a significantly greater response to
platinum-based therapy compared with patients with ERCC1-positive
tumors, while other studies demonstrated that examination of ERCC1
expression fails to identify therapy-responsive or resistant
patients (14,15). Although the overexpression of ERCC1
may function as a prognostic indicator of poor survival in patients
with advanced ovarian cancer, the differences in response rates
cannot be translated into survival rates (16,17).
Muallem et al (18) recently
reported that there were no significant differences in the
progression-free survival time (PFS) of patients with low,
intermediate and high H-scores for ERCC1 expression. The variation
in results of previous studies demonstrates that there is no
conclusive evidence indicating that ERCC1 expression is associated
with platinum-resistance and survival of patients with EOC.
The present study aimed to investigate the
association between ERCC1 expression and the platinum-resistance
and survival of patients with EOC using immunohistochemical
analysis. The results demonstrated that high ERCC1 expression is
associated with clinical resistance to platinum-based chemotherapy,
but not with survival or other clinical characteristics. The
current study also determined that ERCC1 expression is not an
independent or lone factor affecting the prognosis of patients with
EOC.
Materials and methods
Patients
A total of 92 patients diagnosed with EOC were
recruited between January 2008 and December 2008 in The First
Affiliated Hospital of Guangzhou Medical University (Guangzhou,
China). The age of the patients ranged between 21–79 years. The
tumors were classified according to the International Federation of
Gynecology and Obstetrics classification system, with 29 samples
classified as stage I, 9 as stage II, 35 as stage III and 19 as
stage IV. The pathological types of the tumor samples were as
follows: 52 Serous carcinoma samples, 25 mucinous carcinoma, 8
endometrium cancer and 7 clear cell carcinoma, and the pathological
classifications were as follows: 18 High-differentiation, 32
medium-differentiation and 42 low-differentiation. All 92 patients
underwent a comprehensive staging laparotomy and comprehensive or
satisfactory cytoreductive surgery (clean removal/basic
removal/majority removal), and received chemotherapy following
surgery. Chemotherapy regimens consisted of 175 mg/m2
taxol plus 75 mg/m2 cisplatin (or carboplatin calculated
at AUC 5–7). Each treatment cycle lasted 3 weeks and 6–8 cycles
were required. This study was approved by the ethical committee of
The First Affiliated Hospital of Guangzhou Medical University and
written informed consent was obtained from all patients.
Immunohistochemical analysis of ERCC1
expression
Tumor specimens were harvested from 92 patients
prior to receiving cisplatin-based treatment. Formalin-fixed and
paraffin-embedded specimens were cut into 5 µm sections for
immunohistochemical analysis. Antigen retrieval was performed using
target retrieval solution (Dako, Carpinteria, CA, USA) at 95°C for
20 min. Specimens were then blocked with 3%
H2O2 for 10 min, rinsed with dH2O
and Tris-buffered saline and incubated with CAS Block™ solution
(Invitrogen; Thermo Fisher Scientific Corporation, Waltham, MA,
USA) for 5 min. Slides were then incubated with monoclonal mouse
anti-human ERCC1 antibody (cat. no. MOB336-05; 1:300; Diagnostic
Biosystems, Pleasanton, CA, USA) for 60 min at room temperature,
followed by incubation with biotinylated goat anti-mouse secondary
antibody (cat. no. M001; 1:500; Diagnostic Biosystems) for 30 min
and DAB for 5 min at room temperature (Vectastain ABC kit; Vector
Laboratories, Burlingame, CA, USA). Identification of brown-yellow
granules in the nuclei and/or plasma of the tumor cells
corresponded with positive ERCC1 expression. A total of 500–1,500
tumor cells were randomly selected from each specimen at a
magnification of ×400. The intensity of positive cell staining was
examined and the percentage of positive cells was calculated. The
cell staining intensity was categorized as follows: 0, No color; 1,
canary yellow; 2, brown-yellow; and 3, brown or dark brown.
Additionally, the composition ratio of positive cell percentage was
scored as follows: 0, <10%; 1, 10–25%; 2, 26–50%; and 3,
>50%. These two scores were added to calculate the total score,
which corresponded with expression as follows: 0–1, negative (−);
2–3, weakly positive (+); 4–5, positive (++); and 6, strongly
positive (+++). The +/− groups were defined as low expression and
the ++/+++ groups as high expression.
Chemotherapy outcome
Clinical curative effect was assessed by routine
gynecological examination, imaging analysis (color ultrasound,
magnetic resonance imaging or positron emission tomography-computed
tomography for abdominal or pelvic regions) and detection of serum
carbohydrate antigen (CA)-125 levels per month. No recurrence at 6
months post-chemotherapy was referred to as ‘clinically sensitive’
and included normal serum CA-125 levels, no new lesions, or the
original residual lesions had decreased in size or disappeared as
identified by pelvic and imaging examination. By contrast, disease
progression during chemotherapy, a continual increase in serum
CA-125 levels or the appearance of new lesions identified by
imaging at 6 months post-chemotherapy was recognized as ‘clinical
resistance’.
Follow-up
The final follow-up (range, 5–62 months) occurred on
June 6, 2014. Out of 92 patients, 1 was lost to suicide and 5 were
lost to follow-up without reason. Disease PFS was described as the
time from ovarian cancer surgery to disease recurrence or
mortality, whichever came first. The time between surgery and
mortality or the end of follow-up was described as the overall
survival time (OS).
Statistical analysis
SPSS 13.0 software (SPSS, Inc., Chicago, IL, USA)
was used for statistical analysis. The χ2 test was
performed to analyze the association between ERCC1 expression and
clinical pathological features or the platinum-resistance of EOC.
Kaplan-Meier survival curve comparison analysis was used for
survival data, and the log-rank test was used for comparing
survival analysis data. Cox proportional hazards regression
analysis of multiple factors was employed to assess the association
between ERCC1 and PFS or OS. P<0.05 was considered to indicate a
statistically significant difference.
Results
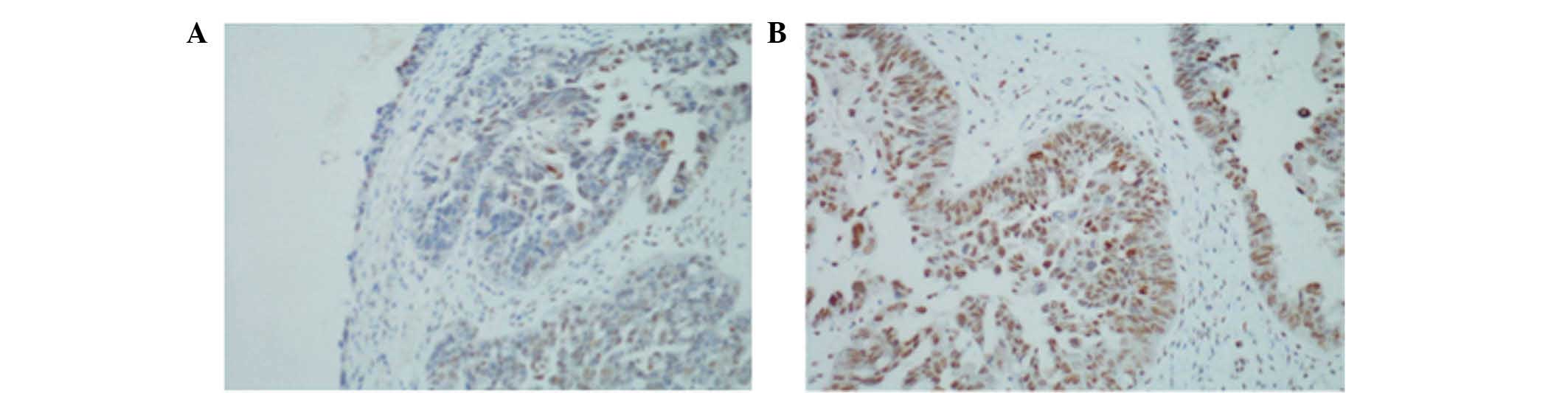
ERCC1 immunohistochemistry
Brown-yellow granules were observed in the majority
of tumor cell cytoplasm and nuclei, and corresponded with positive
ERCC1 expression (Fig. 1).
Immunohistochemistry identified that 82/92 specimens (89.13%) were
ERCC1 positive, with high expression observed in 64 cases (69.57%).
A total of 10 cases (10.87%) were classified as ERCC1(−), 18 cases
(19.57%) as (+), 28 cases (30.43%) as (++) and 36 cases (39.13%) as
(+++).
Association between ERCC1 expression
and clinical pathological features
As presented in Table
I, no significant association was identified between ERCC1
expression and age (P=0.188), pathological type (P=0.681), cell
differentiation (P=0.517) or clinical stage (P=0.418).
 | Table I.Association between ERCC1 expression
and clinicopathological features. |
Table I.
Association between ERCC1 expression
and clinicopathological features.
| Clinical feature | n | Low expression | High expression | χ2 | P-value |
|---|
| Age, years |
|
|
>50 | 53 | 19 | 34 | 1.731 | 0.188 |
| ≤50 | 39 | 9 | 30 |
|
|
| Pathological
type |
|
|
Serous | 52 | 14 | 38 | 1.506 | 0.681 |
|
Mucinous | 25 | 10 | 15 |
|
|
|
Endometrium | 7 | 2 | 5 |
|
|
| Clear
cell | 8 | 2 | 6 |
|
|
| Pathological
differentiation |
|
| Good | 16 | 3 | 13 | 1.320 | 0.517 |
|
Medium | 32 | 10 | 22 |
|
|
| Poor | 44 | 15 | 29 |
|
|
| Clinical stage |
|
| I | 29 | 12 | 17 | 2.835 | 0.418 |
| II | 9 | 3 | 6 |
|
|
| III | 35 | 9 | 26 |
|
|
| IV | 19 | 4 | 15 |
|
|
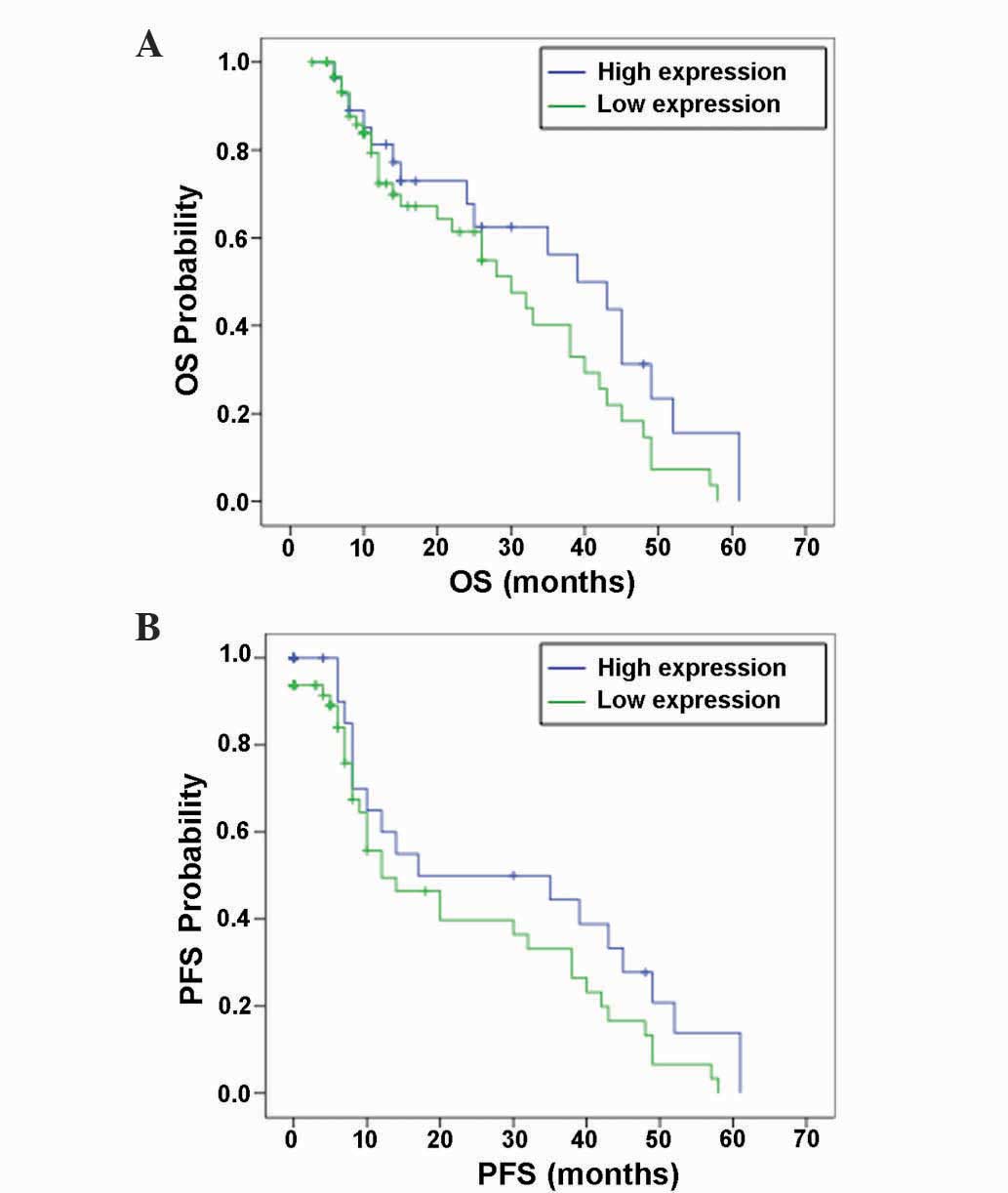
Association between ERCC1 expression
and chemoresistance and survival time
As presented in Table
II, the number of resistant cases with high ERCC1 expression
(27/31; 87.10%) was significantly greater than the number of
sensitive cases with high ERCC1 expression (37/61; 60.77%)
(P<0.05). For the 92 EOC cases, the median OS was 33.0 months
and the median PFS was 14.0 months. The PFS of cases with high
ERCC1 expression was 12.0 months and the median OS was 30.0 months.
The PFS of cases with low ERCC1 expression was 17.0 months and the
median OS was 39.0 months. There was no significant difference in
PFS and median OS between patients with high ERCC1 expression and
patients with low expression (OS, P=0.103; PFS, P=0.099) (Fig. 2).
| Table II.Association between ERCC1 expression
and chemoresistance. |
Table II.
Association between ERCC1 expression
and chemoresistance.
| Group | n | High ERCC1
expression, n (%) | χ2 | P-value |
|---|
| Total | 92 | 64 (69.57) |
|
|
| Sensitive | 61 | 37 (60.77) | 6.787 | 0.009 |
| Resistant | 31 | 27 (87.10) |
|
|
Independent risk factors for patient
survival time
Cox proportional hazards regression was used to
analyze five possible risk factors, including age,
histopathological type, degree of cancer cell differentiation,
clinical stage and ERCC1 expression. As presented in Table III, pathological differentiation and
clinical stage were identified as independent factors significantly
affecting the prognosis of patients (P=0.005 and P<0.001,
respectively), whilst ERCC1 expression (P=0.056), age (P=0.223) and
pathological type (P=0.276) did not significantly affect
prognosis.
| Table III.Cox proportional hazard regression
analysis for independent risk factors affecting patient survival
time. |
Table III.
Cox proportional hazard regression
analysis for independent risk factors affecting patient survival
time.
|
| 95% CI for Exp
(B) |
|---|
|
|
|
|---|
|
| B | SE | Wald | df | P-value | Exp (B) | Lower | Upper |
|---|
| Age | 0.467 | 0.391 | 1.483 | 1 |
0.223 | 1.609 | 0.748 | 3.460 |
| Pathological
type | 0.255 | 0.234 | 1.187 | 1 |
0.276 | 1.290 | 0.816 | 2.040 |
| Pathological
classification | −1.230 | 0.441 | 7.773 | 1 |
0.005 | 0.292 | 0.123 | 0.694 |
| Clinical stage | 0.985 | 0.265 | 13.782 | 1 | <0.001 | 2.677 | 1.592 | 4.501 |
| Expression of
ERCC1 | −0.782 | 0.409 | 3.662 | 1 |
0.056 | 0.458 | 0.205 | 1.019 |
Discussion
Over 200,000 women are affected by EOC, with 125,000
mortalities each year worldwide (19). Chemotherapy drug resistance is a major
factor restricting the improvement of patient survival rates, with
20–30% of patients with EOC undergoing primary platinum-resistance;
however, 80% of patients are likely to eventually encounter
resistance (20,21). The majority of patients experience
relapse, and may eventually succumb to the disease as a result of
drug resistance.
A key factor impacting the survival of patients with
EOC is the response to initial or subsequent platinum-based
chemotherapy, which is subjected to the development of platinum
resistance. With the rapid development of pharmacogenomics and
molecular biology, the mechanism of cisplatin resistance is closely
associated with NER (22). In DNA
repair, ERCC1 is a key gene of the NER pathway due to its binding
with DNA repair endonuclease ERCC1-xeroderma pigmentosum group F
(XPF) (23,24). In addition, the ERCC1-XPF complex is
required for the removal of DNA interstrand crosslinks (ICLs),
which are highly cytotoxic lesions induced by bifunctional
genotoxins, including cisplatin (25). ERCC1-XPF is the only enzyme that is
essential for ICL repair and NER, and therefore, removal of all
platinum-induced DNA damage.
ERCC1 has been the focus of numerous studies
investigating the mechanisms of platinum-based resistance. A number
of studies have demonstrated an association between high ERCC1
expression and resistance to cisplatin-based chemotherapy, which
determined the survival rate of patients with EOC (11,13,16,17,26).
During chemotherapy, platinum drugs primarily bind to and destroy
tumor cells with negative ERCC1 expression, while having no effect
on tumor cells with high ERCC1 expression exhibiting platinum
resistance. In addition to ovarian cancer, a number of studies have
evaluated the role of ERCC1 in the mechanisms of platinum
resistance in other types of cancer, including head and neck cancer
(27), non-small cell lung cancer
(27,28) and gastrointestinal cancer (29). However, no consistent results have
been obtained regarding the association between ERCC1 expression
and different clinical endpoints.
A previous meta-analysis evaluated whether response
to platinum-based chemotherapy was associated with ERCC1 expression
in patients with ovarian cancer (30). It was observed that patients with
negative ERCC1 expression had a significantly greater response to
platinum-based chemotherapy compared with patients with positive
ERCC1 expression (30), indicating
that ERCC1 protein expression status is correlated with response to
platinum-based chemotherapy in ovarian cancer. Zhao et al
(31) identified a negative
correlation between ERCC1 expression and clinical chemosensitivity
in EOC. Furthermore, Steffensen et al (13) analyzed 100 tumor samples for ERCC1
expression and observed that 45% of ERCC1-positive samples were
significantly less sensitive to chemotherapy than ERCC1-negative
samples, and therefore identified a positive association between
clinical resistance to platinum-based chemotherapy and ERCC1
expression in patients with EOC. Thus, it is considered to be
beneficial to predict the sensitivity of clinical platinum
chemotherapy by examining ERCC1 expression in tumor tissues prior
to chemotherapy. However, Muallem et al (18) demonstrated that there were no
significant differences in the PFS between patients with low,
intermediate and high H-scores for ERCC1 expression. Furthermore,
Rubatt et al (32) reported
that the tumoral expression of ERCC1 prior to chemotherapy in women
with advanced stage EOC is not predictive of clinical outcomes.
Additionally, Steffensen et al (13) observed no association between ERCC1
expression and OS in patients with EOC.
In the present study, ERCC1 expression was analyzed
in the EOC tissues by immunohistochemical staining. The results
demonstrated that 89.13% of the EOC tissues were ERCC1 positive,
and the number of chemoresistant cases with high ERCC1 expression
was significantly greater than the number of chemosensitive cases
with high ERCC1 expression, suggesting that the ERCC1 expression is
associated with cisplatin chemotherapy-sensitivity. As platinum
chemotherapy is the first-line therapy administered for EOC, ERCC1
expression may be widely used as a predictor of clinical
chemotherapy sensitivity to guide individualized treatment, avoid
administration of invalid chemotherapy and eventually improve
treatment for patients with cancer.
Furthermore, when compared with patients with low
ERCC1 expression, PFS and OS were lower in the high ERCC1
expression group in the current study, but this was not significant
(PFS, P=0.099; OS, P=0.103). Additionally, Cox regression analysis
demonstrated that ERCC1 expression level was not an independent
prognostic factor for the survival time of patients with EOC.
Certain factors, such as the use of a comprehensive treatment as
primary tumor treatment, may affect patient survival and require
further analysis. In addition, genetic polymorphisms in ERCC1 genes
may reverse ERCC1 mRNA level, and may also impact the curative
effect and prognosis of platinum-based chemotherapy (33).
In conclusion, the present study demonstrated that
high ERCC1 expression in patients with EOC was associated with
resistance to platinum-based chemotherapy, but not with survival
time. In addition, it was also observed that ERCC1 protein
expression was not an independent or lone factor affecting the
prognosis of patients. Further studies with larger sample sizes and
improved study designs are required to investigate whether or not
ERCC1 may function as a predictor for chemotherapy against EOC.
Acknowledgements
The present study was funded by the Department of
Science and Technology of Guangdong Province (Guangzhou, China;
grant no. 20140212).
References
|
1
|
Siegel R, Naishadham D and Jemal A: Cancer
statistics, 2012. CA Cancer J Clin. 62:10–29. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Desai A, Xu J, Aysola K, Qin Y, Okoli C,
Hariprasad R, Chinemerem U, Gates C, Reddy A, Danner O, et al:
Epithelial ovarian cancer: An overview. World J Transl Med. 3:1–8.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Roett MA and Evans P: Ovarian cancer: An
overview. Am Fam Physician. 80:609–616. 2009.PubMed/NCBI
|
|
4
|
Coleman RL, Monk BJ, Sood AK and Herzog
TJ: Latest research and treatment of advanced-stage epithelial
ovarian cancer. Nat Rev Clin Oncol. 10:211–224. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jemal A, Siegel R, Xu J and Ward E: Cancer
statistics, 2010. CA Cancer J Clin. 60:277–300. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lawrie TA, Rabbie R, Thoma C and Morrison
J: Pegylated liposomal doxorubicin for first-line treatment of
epithelial ovarian cancer. Cochrane Database Syst Rev.
10:CD0104822013.PubMed/NCBI
|
|
7
|
Griffiths RW, Zee YK, Evans S, Mitchell
CL, Kumaran GC, Welch RS, Jayson GC, Clamp AR and Hasan J: Outcomes
after multiple lines of chemotherapy for platinum-resistant
epithelial cancers of the ovary, peritoneum and fallopian tube. Int
J Gynecol Cancer. 21:58–65. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bowden NA: Nucleotide excision repair: Why
is it not used to predict response to platinum-based chemotherapy?
Cancer Lett. 346:163–171. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wijnhoven SW, Hoogervorst EM, de Waard H,
van der Horst GT and van Steeg H: Tissue specific mutagenic and
carcinogenic responses in NER defective mouse models. Mutat Res.
614:77–94. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gossage L and Madhusudan S: Current status
of excision repair cross complementing-group 1 (ERCC1) in cancer.
Cancer Treat Rev. 33:565–577. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Dabholkar M, Bostick-Bruton F, Weber C,
Bohr VA, Egwuagu C and Reed E: ERCC1 and ERCC2 expression in
malignant tissues from ovarian cancer patients. J Natl Cancer Inst.
84:1512–1517. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ferry KV, Hamilton TC and Johnson SW:
Increased nucleotide excision repair in cisplatin-resistant ovarian
cancer cells: Role of ERCC1-XPF. Biochem Pharmacol. 60:1305–1313.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Steffensen KD, Waldstrøm M and Jakobsen A:
The relationship of platinum resistance and ERCC1 protein
expression in epithelial ovarian cancer. Int J Gynecol Cancer.
19:820–825. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Bosmuller H, Haitchi-Petnehazy S,
Webersinke G, Marschon R, Roithmeier F, Stummvoll W, Fehm T,
Klier-Richter M, Bonzheim I, et al: Intratumoral lymphocyte density
in serous ovarian carcinoma is superior to ERCC1 expression for
predicting response to platinum-based therapy. Virchows Arch.
459:183–191. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Stadlmann S, Dirnhofer S, Güth U, Thies S
and Singer G: ERCC1-immunoexpression does not predict
platinum-resistance in ovarian cancer. Gynecol Oncol. 108:252–253.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Milovic-Kovacevic M, Srdic-Rajic T,
Radulovic S, Bjelogrlic S and Gavrilovic D: Expression of ERCC1
protein in biopsy specimen predicts survival in advanced ovarian
cancer patients treated with platinum-based chemotherapy. J BUON.
16:708–714. 2011.PubMed/NCBI
|
|
17
|
Scheil-Bertram S, Tylus-Schaaf P, du Bois
A, Harter P, Oppitz M, Ewald-Riegler N and Fisseler-Eckhoff A:
Excision repair cross-complementation group 1 protein
overexpression as a predictor of poor survival for high-grade
serous ovarian adenocarcinoma. Gynecol Oncol. 119:325–331. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Muallem MZ, Marnitz S, Richter R, Köhler
C, Sehouli J and Arsenic R: ERCC1 expression as a predictive marker
of cervical cancer treated with cisplatin-based chemoradiation.
Anticancer Res. 34:401–406. 2014.PubMed/NCBI
|
|
19
|
Parkin DM, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lin H and Changchien CC: Management of
relapsed/refractory epithelial ovarian cancer: Current standards
and novel approaches. Taiwan J Obstet Gynecol. 46:379–388. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Colombo N and Gore M: Treatment of
recurrent ovarian cancer relapsing 6–12 months post platinum-based
chemotherapy. Crit Rev Oncol Hematol. 64:129–138. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Altaha R, Liang X, Yu JJ and Reed E:
Excision repair cross complementing-group 1 Gene expression and
platinum resistance. Int J Mol Med. 14:959–970. 2004.PubMed/NCBI
|
|
23
|
Andrieux LO, Fautrel A, Bessard A,
Guillouzo A, Baffet G and Langouët S: GATA-1 is essential in
EGF-mediated induction of nucleotide excision repair activity and
ERCC1 expression through ERK2 in human hepatoma cells. Cancer Res.
67:2114–2123. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Niedernhofer LJ, Odijk H, Budzowska M, van
Drunen E, Maas A, Theil AF, de Wit J, Jaspers NG, Beverloo HB,
Hoeijmakers JH and Kanaar R: The structure-specific endonuclease
Ercc1-Xpf is required to resolve DNA interstrand cross-link-induced
double-strand breaks. Mol Cell Biol. 24:5776–5787. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kirschner K and Melton DW: Multiple roles
of the ERCC1-XPF endonuclease in DNA repair and resistance to
anticancer drugs. Anticancer Res. 30:3223–3232. 2010.PubMed/NCBI
|
|
26
|
Dabholkar M, Vionnet J, Bostick-Bruton F,
Yu JJ and Reed E: Messenger RNA levels of XPAC and ERCC1 in ovarian
cancer tissue correlate with response to platinum-based
chemotherapy. J Clin Invest. 94:703–708. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Vilmar A and Sorensen JB: Excision repair
cross-complementation group 1 (ERCC1) in platinum-based treatment
of non-small cell lung cancer with special emphasis on carboplatin:
A review of current literature. Lung Cancer. 64:131–139. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Bonanno L, Favaretto A and Rosell R:
Platinum drugs and DNA repair mechanisms in lung cancer. Anticancer
Res. 34:493–501. 2014.PubMed/NCBI
|
|
29
|
Metzger R, Bollschweiler E, Holscher AH
and Warnecke-Eberz U: ERCC1: Impact in multimodality treatment of
upper gastrointestinal cancer. Future Oncol. 6:1735–1749. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Li FY, Ren XB, Xie XY and Zhang J:
Meta-analysis of excision repair cross-complementation group 1
(ERCC1) association with response to platinum-based chemotherapy in
ovarian cancer. Asian Pac J Cancer Prev. 14:7203–7206. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Zhao D, Zhang W, Li XG, Wang XB, Li M, Li
YF, Tian HM, Song PP, Liu J, Chang QY and Wu LY: The mRNA
expression of BRCA1, ERCC1, TUBB3, PRR13 genes and their
relationship with clinical chemosensitivity in primary epithelial
ovarian cancer. Zhonghua Zhong Liu Za Zhi. 34:196–200. 2012.(In
Chinese). PubMed/NCBI
|
|
32
|
Rubatt JM, Darcy KM, Tian C, Muggia F,
Dhir R, Armstrong DK, Bookman MA, Niedernhofer LJ, Deloia J, Birrer
M and Krivak TC: Pre-treatment tumor expression of ERCC1 in women
with advanced stage epithelial ovarian cancer is not predictive of
clinical outcomes: A gynecologic oncology group study. Gynecol
Oncol. 125:421–426. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kiyohara C and Yoshimasu K: Genetic
polymorphisms in the nucleotide excision repair pathway and lung
cancer risk: A meta-analysis. Int J Med Sci. 4:59–71. 2007.
View Article : Google Scholar : PubMed/NCBI
|