Introduction
Hepatocellular carcinoma (HCC) is the fifth most
common cancer, and it ranks as the third leading cause of
cancer-associated mortality worldwide (1). Surgical resection remains the most
effective curative treatment for HCC (2), but the high incidence of tumor
recurrence makes long-term survival following resection
unsatisfactory (3,4). Reducing postoperative recurrence is one
of the most significant challenges to improving the prognosis of
patients with HCC (5). Several
factors (6,7) are hypothesized to affect the risk of
recurrence, including whether radical treatment has been performed,
what biological characteristics the tumors present, how well the
patient's immune system is functioning, and whether the patient has
active hepatitis due to hepatitis B virus (HBV) replication.
Increasingly, clinicians are exploring ways to boost patient immune
function in order to reduce postoperative recurrence (6).
Thymosin α1 (Tα1), a 28-residue peptide hormone with
an acetylated N terminus, is widely used in the clinic to treat
patients with chronic HBV infection and to enhance immune response
to vaccines in immunocompromised individuals (8,9). Tα1
enhances immunity mainly by inducing the differentiation and
maturation of T cells as well as the production of cytokines
(10). Only two studies (11,12) have
reported that Tα1 may also be effective at reducing risk of
postoperative HCC recurrence subsequent to hepatectomy, leading to
significantly increased long-term survival rates compared with the
absence of Tα1 therapy. The reliability of these studies is limited
by their relatively small samples (19 and 34 patients) and the fact
that the studies did not adjust for potential baseline differences
between Tα1 and control groups that may have contributed to
observed differences in outcomes.
To more rigorously assess the clinical efficacy of
postoperative Tα1 subsequent to radical hepatectomy in HCC
patients, medical records were retrospectively analyzed for
recurrence and prognosis in a larger cohort of patients treated at
the Affiliated Tumor Hospital of Guangxi Medical University
(Nanning, China), comparing those who received postoperative Tα1
therapy with those who did not. Propensity score matching was used
to minimize interference from potential confounders.
Patients and methods
Patients
The present study was approved by the Ethics
Committee of the Affiliated Cancer Hospital of Guangxi Medical
University and patients provided consent as part of the standard
admission procedure. Medical records were retrospectively analyzed
for patients who underwent initial radical hepatectomy for HCC at
the Affiliated Tumor Hospital of Guangxi Medical University between
January 2007 and December 2012. To be included, patients had to
present with: i) A diagnosis confirmed by postoperative
pathological examination; ii) serum hepatitis B e antigen (HBeAg)
positivity; iii) a Child-Pugh score of 5–6 for liver function; iv)
an Eastern Cooperative Oncology Group score of 0; v) preoperative
absence of any cancer embolus in the main portal vein or its
first-level branches, the common bile duct or its first-level
branches, the main hepatic vein, or the inferior vena cava; vi)
absence of intra- and extrahepatic metastases, and total resection
of macroscopic tumors without residual cancer cells on the surgical
margins; vii) absence of any residual tumor by imaging 1 month
subsequent to surgery; and viii) return of α-fetoprotein (AFP)
levels to the normal range within 2 months of surgery in patients
with elevated serum AFP before the operation.
Patients were excluded from the present study if
they: i) Had received transarterial chemoembolization (TACE),
radiotherapy or other anti-tumor therapies prior to hepatectomy;
ii) had undergone emergency surgery; iii) were infected with
hepatitis C virus, hepatitis D virus or HIV; iv) had concomitant
malignant tumors or severe disorders in other organs; or v) had a
history of alcohol or drug abuse.
Patients included in the present study were divided
into two groups: Those who received postoperative Tα1 therapy and
those who did not.
Propensity score matching
Since patients were not assigned randomly to receive
postoperative Tα1 therapy or not, it was highly likely that the two
patient groups would present significant baseline differences that
may confound the analysis of outcomes. In order to reduce the bias
in patient selection, propensity score matching was performed to
balance these baseline differences and thereby simulate random
group allocation (2,13,14).
Propensity scores were estimated using a logistic regression model
based on age, gender, presence of HBeAg, presence of diabetes
mellitus, albumin level, total bilirubin level, serum AFP level,
alanine aminotransferase (ALT) level, prothrombin time, platelet
count, tumor size and number, presence of liver cirrhosis, presence
of tumor capsule, microvascular invasion, Edmondson stage,
Barcelona Clinic Liver Cancer classification (15), and antiviral therapy administered.
Subsequently, 1:1 matching without replacement was performed using
a 0.1 caliper width, and the resulting score-matched pairs were
used in subsequent analyses, as previously reported (2).
Treatment
Patients in the Tα1 group were injected
subcutaneously with 1.6 mg Tα1 (Chengdu Diao Jiuhong Pharmaceutical
Factory, Chengdu, China) twice weekly for 6 months.
Follow-up and outcomes
Control and Tα1 patients returned to the Affiliated
Tumor Hospital of Guangxi Medical University for follow-up
assessments every 2–3 months. During these visits, serum levels of
AFP and the following liver function markers were determined:
Albumin level; ALT level; prothrombin time; and total bilirubin
level. In addition, imaging tests were performed using B-mode
ultrasonography, computed tomography or magnetic resonance imaging.
Patients showing the presence of newly developed intra- or
extrahepatic tumors consistent with the characteristics of HCC by
two imaging modalities were considered to have postoperative
recurrence. The outcome measures were postoperative recovery of
liver function and recurrence-free and overall survival rates.
Statistical analysis
SPSS 19.0 (IBM, Armonk, NY, USA) was used for
statistical analysis. Data with a normal or approximately normal
distribution were reported as the mean ± standard deviation. Data
with a non-normal distribution were reported as the median (range).
Means, medians and rates between the two patient groups were
compared using Student's t test, Mann-Whitney U test or
χ2 test, as appropriate. Survival rates were estimated
using Kaplan-Meier analysis, and inter-group differences were
compared using the log-rank test. The threshold of statistical
significance in all cases was defined as P<0.05.
Results
Patients
A total of 558 patients that met the inclusion
criteria were enrolled in the present study, of whom 146 patients
received postoperative Tα1 therapy and 412 patients did not
(Table I). The Tα1 and control groups
were similar for the majority of baseline characteristics, but
there were significant differences in the rates of postoperative
antiviral therapy using lamivudine or other drugs, as well as
marginal differences in the numbers and longest diameter of tumors.
To reduce the risk that these baseline differences may confound the
present results, 1:1 propensity score matching was performed to
generate 106 pairs that showed no significant differences in any of
the baseline parameters (Table
I).
 | Table I.Baseline characteristics of
hepatocellular carcinoma patients who received Tα1 therapy or not
after radical hepatectomy, before and after propensity score
matching. |
Table I.
Baseline characteristics of
hepatocellular carcinoma patients who received Tα1 therapy or not
after radical hepatectomy, before and after propensity score
matching.
| Variable | Tα1 group, n (%) | Control group, n
(%) | P-value | Tα1 group, n (%) | Control group, n
(%) | P-value |
|---|
| Total | 146
(100.0) | 412
(100.0) |
| 106 (100.0) | 106 (100.0) |
|
| Gender |
|
| Male | 127 (87.0) | 359 (87.1) | 0.963 | 93 (87.7) | 95 (89.6) | 0.665 |
|
Female | 19
(13.0) | 53
(12.9) |
| 13 (12.3) | 11 (10.4) |
|
| Age, years | 49.8±9.9 | 50.7±11.6 | 0.786 | 49.0±10.1 | 49.7±10.8 | 0.618 |
| HBeAg |
|
| Yes | 123 (84.2) | 348 (84.5) | 0.950 | 85 (80.2) | 87 (82.1) | 0.726 |
| No | 23
(15.8) | 64
(15.5) |
| 21 (19.8) | 19 (17.9) |
|
| Diabetes
mellitus |
|
| Yes | 14 (9.6) | 23 (5.6) | 0.095 | 8 (7.5) | 8 (7.5) | 1.000 |
| No | 132 (90.4) | 389 (94.4) |
| 98 (92.5) | 98 (92.5) |
|
| HBV-DNA, IU/ml | 8.6×103
(0.0–2.0×107) | 4.2×103
(0.0–1.9×109) | 0.496 | 8.6×103
(0.0–2.0×107) | 7.8×103
(0.0–1.8×107) | 0.875 |
| Total bilirubin,
µmol/l | 12.8 (3.4–68.7) | 13.2 (2.7–63.9) | 0.333 | 12.7 (3.9–46.7) | 12.1 (3.4–29.5) | 0.679 |
| Albumin, g/l | 40.8±4.3 | 40.4±4.7 | 0.283 | 41.0±4.0 | 40.7±4.3 | 0.656 |
| ALT, U/l | 36.5
(8.0–504.0) | 36.0
(8.0–281.0) | 0.959 | 38.0
(12.0–108.0) | 41.0
(8.0–181.0) | 0.654 |
| Prothrombin time,
sec | 12.7 (9.4–22.4) | 12.8 (9.5–20.1) | 0.637 | 12.6 (9.4–18.4) | 12.7
(10.4–16.9) | 0.701 |
| AFP level |
|
| ≥20
ng/ml | 92
(63.0) | 242 (58.7) | 0.365 | 63 (59.4) | 63 (59.4) | 1.000 |
| <20
ng/ml | 54
(37.0) | 170 (41.3) |
| 43 (40.6) | 43 (40.6) |
|
| Number of tumors |
|
|
Multiple | 28
(19.2) | 112 (27.2) | 0.055 | 19 (17.9) | 20 (18.9) | 0.859 |
|
Single | 118 (80.8) | 300 (72.8) |
| 87 (82.1) | 86 (81.1) |
|
| Size of largest
tumor |
|
| ≥5
cm | 70
(47.9) | 235 (57.0) | 0.058 | 55 (51.9) | 52 (49.1) | 0.680 |
| <5
cm | 76
(52.1) | 177 (43.0) |
| 51 (48.1) | 54 (50.9) |
|
| Tumor capsule |
|
|
Incomplete | 77
(52.7) | 189 (45.9) | 0.153 | 49 (46.2) | 48 (45.3) | 0.890 |
|
Complete | 69
(47.3) | 223 (54.1) |
| 57 (53.8) | 58 (54.7) |
|
| Microvascular
invasion |
|
|
Yes | 14 (9.6) | 22 (5.3) | 0.073 | 9 (8.5) | 8 (7.5) | 0.800 |
| No | 132 (90.4) | 390 (94.7) |
| 97 (91.5) | 98 (92.5) |
|
| Liver
cirrhosis |
|
|
Yes | 127 (87.0) | 335 (81.3) |
0.118 | 92 (86.8) | 94 (88.7) | 0.675 |
| No | 19
(13.0) | 77
(18.7) |
| 14 (13.2) | 12 (11.3) |
|
| Portal
hypertension |
|
|
Yes | 58 (39.7) | 152 (36.9) |
0.544 | 38 (35.8) | 41 (38.7) | 0.670 |
| No | 88 (60.3) | 260 (63.1) |
| 68 (64.2) | 65 (61.3) |
|
| BCLC stage |
|
| A | 119 (81.5) | 335 (81.3) |
0.958 | 89 (84.0) | 88 (83.0) | 0.853 |
| B | 27
(18.5) | 77
(18.7) |
| 17 (16.0) | 18 (17.0) |
|
| Edmondson
stage |
|
|
I/II | 13 (8.6)/72
(49.5) | 28 (6.8)/183
(44.4) |
0.062 | 8 (8.0)/51
(48.0) | 7 (6.6)/49
(46.2) | 0.942 |
|
III/IV | 33 (22.6)/28
(19.4) | 141 (34.2)/60
(14.6) |
| 29 (26.9)/18
(17.1) | 33 (30.8)/17
(16.0) |
|
| Antiviral
therapy |
|
|
Yes | 104 (71.2) | 90
(21.8) | <0.001 | 65 (61.3) | 66 (62.3) | 0.888 |
| No | 42
(28.8) | 322 (78.2) |
| 41 (38.7) | 40 (37.7) |
|
Changes in liver function during
follow up
The albumin level was significantly higher in the
Tα1 group compared with the control group at 1, 2 and 3 years
subsequent to hepatectomy, whereas total bilirubin and ALT levels
were significantly lower in the Tα1 group at 2 and 3 years
(Table II). By 3 years subsequent to
surgery, the prothrombin time was significantly shorter in the Tα1
group.
| Table II.Post-hepatectomy liver function in
hepatocellular carcinoma patients with or without postoperative Tα1
therapy. |
Table II.
Post-hepatectomy liver function in
hepatocellular carcinoma patients with or without postoperative Tα1
therapy.
| Years after
surgery | TBIL, µmol/l | ALB, g/l | ALT, U/l | PT, sec |
|---|
| Control group |
|
| 1
year | 12.4
(3.4–506.9) | 42.2±4.9 | 31.0
(8.0–373.0) | 13.3
(10.3–24.2) |
| 2
years | 14.3
(5.2–187.6) | 39.9±4.6 | 33.0
(9.0–219.0) | 13.3
(10.4–17.8) |
| 3
years | 13.3
(5.8–16.0) | 42.3±4.7 | 44.5
(22.0–65.0) | 12.7
(11.0–14.1) |
| Tα1 group |
|
| 1
year | 10.4
(5.0–134.5) |
44.0±4.3a | 31.5
(10.0–558.0) | 13.0
(10.3–19.1) |
| 2
years | 10.7
(3.8–98.7)a |
45.3±3.1a | 27.5
(6.0–159.0)a | 13.0
(10.2–37.9) |
| 3
years | 9.9
(7.3–12.4)a |
48.6±2.7a | 31.5
(25.0–38.0)a | 11.6
(11.2–12.0)a |
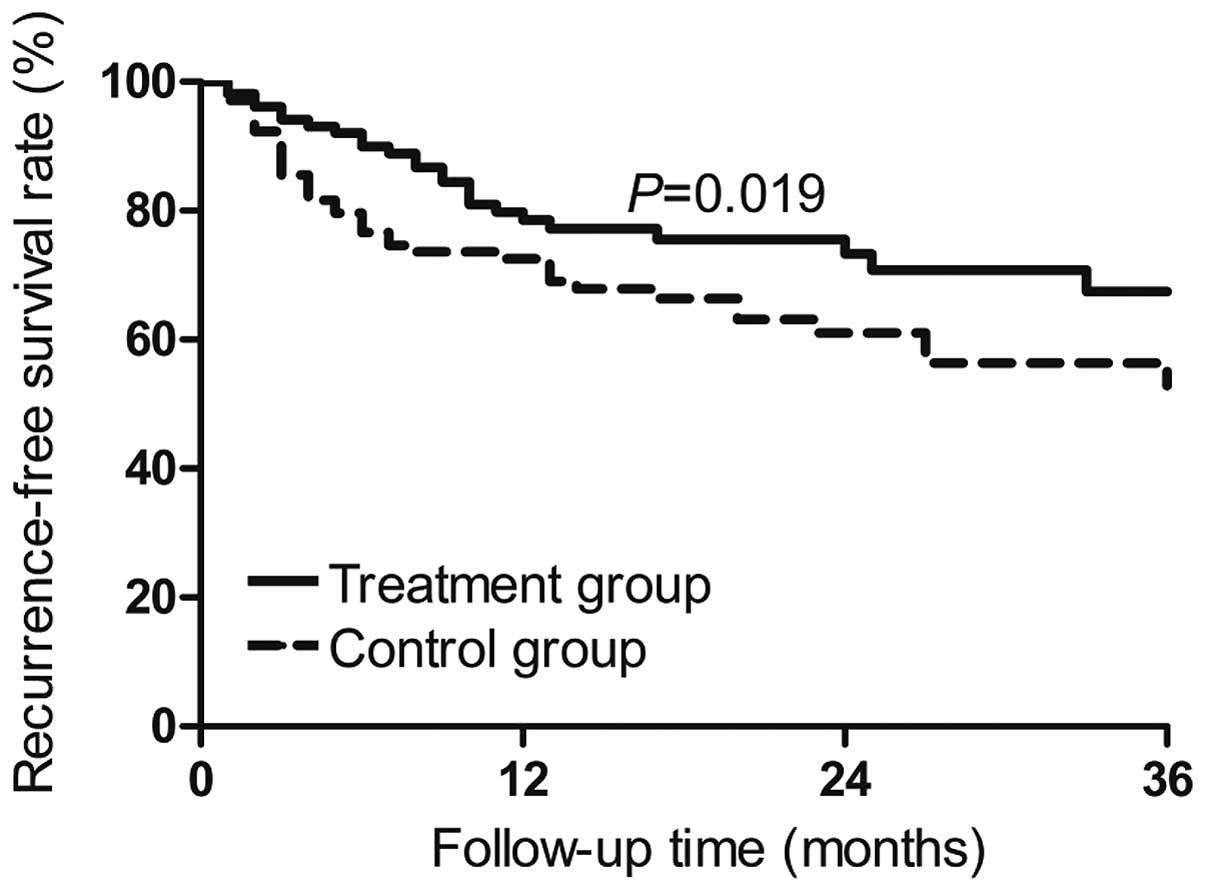
Recurrence-free survival and overall
survival analyses
Cumulative recurrence-free survival rates of the
Tα1-treated patients in the 106 propensity score-matched pairs were
79.7% at 1 year, 70.8% at 2 years and 67.3% at 3 years subsequent
to surgery. The corresponding rates in the 106 control patients
were 69.9, 61.5 and 51.6% (P=0.019; Fig.
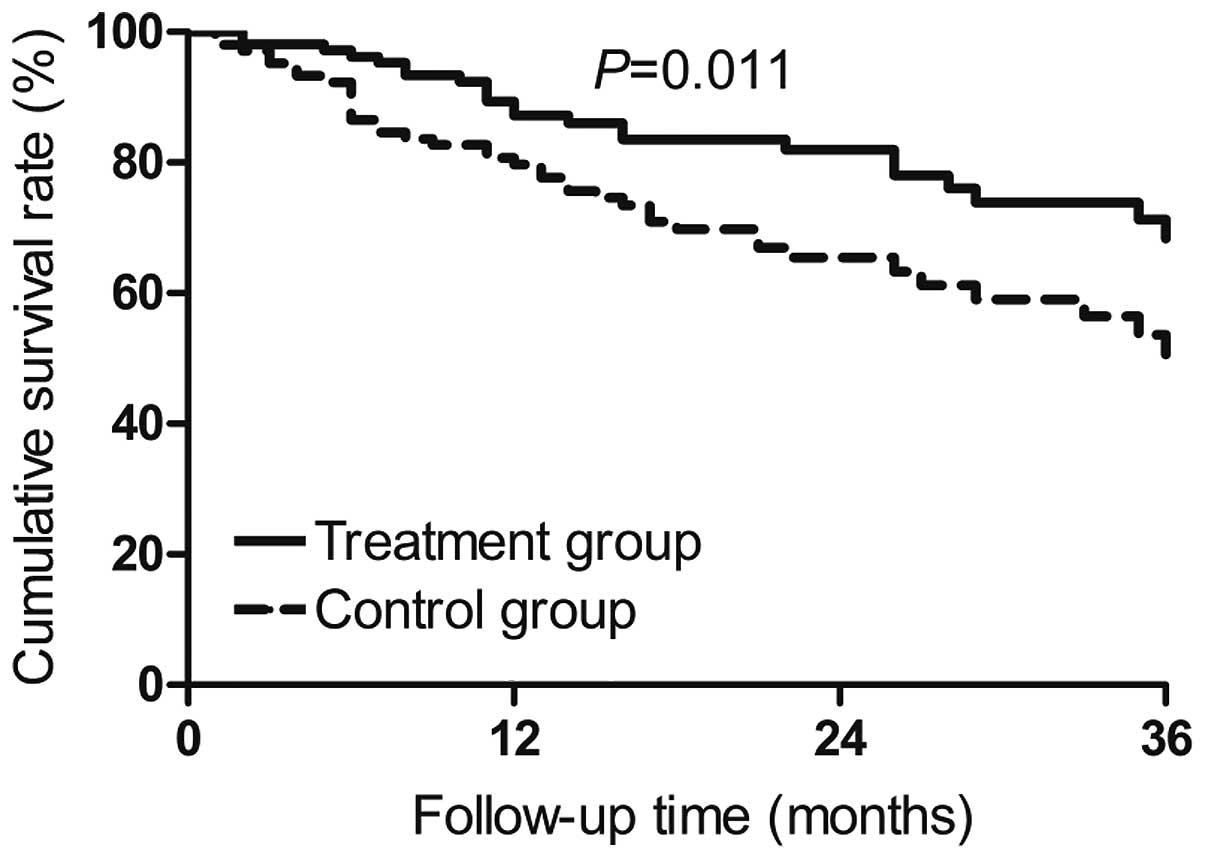
1). Cumulative overall survival at the three time points was
87.2, 82.0 and 68.4% in the propensity score-matched Tα1 patients,
compared to 78.2, 64.2 and 49.7% in the control patients (P=0.011;
Fig. 2).
Discussion
The preferred treatment for early- and
intermediate-stage HCC is radical hepatectomy, but despite
impressive advances in early HCC detection and resection
techniques, 2-year recurrence remains high, at 45% (16). Reducing tumor recurrence and/or
metastasis subsequent to resection is crucial for the long-term
survival of HCC patients. The present study provides evidence that
postoperative therapy using the peptide hormone Tα1 may
significantly increase overall and recurrence-free survival as well
as liver function in patients with HBV-associated HCC.
Impaired immunity subsequent to resection is
considered to contribute to HCC recurrence both soon afterwards and
in the longer term (6). Single-site
HCC recurrence appears to be more common within 2 years of surgery,
while multi-site recurrence is more common >2 years subsequent
to surgery (17). The present
results, with 3-year recurrence-free survival, suggest that Tα1 can
significantly reduce both types of recurrence. Tα1 may exert these
anti-tumor effects mainly by boosting immune function in several
respects (18). Tα1 enhances the
mitogen-triggered maturation of Tα1 lymphocytes in the peripheral
blood, increases the secretion of various T cell lymphokines, such
as interferon (IFN)-α, IFN-γ, interleukin (IL)-2 and IL-3,
increases the number of lymphokine receptors on the T lymphocyte
surface, and activates T4 helper cells to promote lymphocyte
activity. Tα1 also promotes the chemotaxis of NK precursor cells,
thereby increasing cytotoxicity. Previous studies have shown Tα1 to
be useful in the treatment of HCC (11,12), and
the present study complements that literature by demonstrating
significant survival benefits for HCC patients following radical
hepatectomy.
In addition to survival rates, postoperative Tα1
therapy significantly improved liver function indices, such as
total bilirubin, albumin and ALT and prothrombin time, in the
present patients. It was hypothesized that in the current patients,
Tα1 enhanced lymphocyte activity and thereby suppressed viral
replication, leading to improved liver function. The Tα1-mediated
increase in overall survival was possibly due to the combination of
improved liver function and reduction in recurrence.
Strengths of the present study include that it
involved larger patient samples than previous studies on this area
of research (11,12), and that propensity score matching was
used to balance baseline differences between patients who received
postoperative Tα1 therapy and those who did not. At the same time,
the study has several weaknesses. No data on changes in immune
function indices prior and subsequent to hepatectomy were included;
these indices should be included in future studies. Similarly, data
on HBV replication in the present patients was not used, although
the observed significant improvement in liver function suggests
that Tα1 therapy exerted a strong antiviral effect in the present
patients.
The present data provide evidence that Tα1 therapy
may improve overall and recurrence-free survival as well as liver
function in HCC patients following radical hepatectomy. The
survival benefits of Tα1 therapy may be greater than those of other
adjuvant therapies, and the therapy may be compatible with a wider
range of HCC patients. For example, TACE is effective only in HCC
patients at high risk of recurrence (19), while adoptive immunotherapy appears to
have little effect on the overall survival rate (6). Interferons may cause adverse reactions
such as fever, cold-like symptoms, myelosuppression and hair loss,
as well as complications such as hepatic decompensation (20). Lamivudine is indicated only for
patients with high serum titers of HBV DNA (21). Future studies should not only verify
our findings in patients with HBV-associated HCC, but also examine
whether the treatment may benefit other subpopulations of HCC
patients.
Acknowledgements
The authors thank Dr. Armando Chapin Rodríguez for
his language editing, which substantially improved the quality of
the manuscript. This research was funded by the National Natural
Science Foundation of China (grant nos. 81160262 and 81260331), and
National Science and Technology Major Project of the Ministry of
Science and Technology of China (grant no.
2012ZX10002010001009).
References
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Guo Z, Zhong JH, Jiang JH, Zhang J, Xiang
BD and Li LQ: Comparison of survival of patients with BCLC stage a
hepatocellular carcinoma after hepatic resection or transarterial
chemoembolization: A propensity score-based analysis. Ann Surg
Oncol. 21:3069–3076. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Li T, Fan J, Qin LX, Zhou J, Sun HC, Qiu
SJ, Ye QH, Wang L and Tang ZY: Risk factors, prognosis and
management of early and late intrahepatic recurrence after
resection of primary clear cell carcinoma of the liver. Ann Surg
Oncol. 18:1955–1963. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Arnaoutakis DJ, Mavros MN, Shen F,
Alexandrescu S, Firoozmand A, Popescu I, Weiss M, Wolfgang CL,
Choti MA and Pawlik TM: Recurrence patterns and prognostic factors
in patients with hepatocellular carcinoma in noncirrhotic liver: A
Multi-Institutional analysis. Ann Surg Onco. 21:147–154. 2014.
View Article : Google Scholar
|
|
5
|
Forner A, Llovet J and Bruix J:
Hepatocellular carcinoma. Lancet. 379:1245–1255. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhong JH, Ma L, Wu LC, Zhao W, Yuan WP, Wu
FX, Zhang ZM, Huang S, You XM and Li LQ: Adoptive immunotherapy for
postoperative hepatocellular carcinoma: A systematic review. Int J
Clin Pract. 66:21–27. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lee SC: Prognostic biomarkers for
prediction of recurrence of hepatocellular carcinoma: Current
status and future prospects. World J Gastroenterol. 20:3112–3124.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
You J, Zhuang L, Cheng HY, Yan SM, Yu L,
Huang JH, Tang BZ, Huang ML, Ma YL, Chongsuvivatwong V, et al:
Efficacy of thymosin alpha-1 and interferon alpha in treatment of
chronic viral hepatitis B: A randomized controlled study. World J
Gastroenterol. 12:6715–6721. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kim BH, Lee YJ, Kim W, Yoon JH, Jung EU,
Park SJ, Kim YJ and Lee HS: Efficacy of thymosin α-1 plus
peginterferon α-2a combination therapy compared with peginterferon
α-2a monotherapy in HBeAg-positive chronic hepatitis B: A
prospective, multicenter, randomized, open-label study. Scand J
Gastroenterol. 47:1048–1055. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Matteucci C, Minutolo A,
Sinibaldi-Vallebona P, Palamara AT, Rasi G, Mastino A and Garaci E:
Transcription profile of human lymphocytes following in vitro
treatment with thymosin alpha-1. Ann N Y Acad Sci. 1194:6–19. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cheng SQ, Wu MC, Chen H, Shen F, Yang JH,
Zhao YX and Mo ZW: Influence of thymosin α1 on postoperative
recurrence of primary liver cancer. Chin J Hepatobil Surg.
10:592–593. 2004.(In Chinese).
|
|
12
|
Palmieri G, Biondi E, Morabito A, Rea A
and Bianco A: Could thymostimulin prevent hepatocellular carcinoma
occurrence in patients with liver cirrhosis? Oncol Rep. 3:655–656.
1996.PubMed/NCBI
|
|
13
|
Zhong J, Ke Y, Gong W, Xiang BD, Ma L, Ye
XP, Peng T, Xie GS and Li LQ: Hepatic resection associated with
good survival for selected patients with intermediate and
advanced-stage hepatocellular carcinoma. Ann Surg. 260:329–340.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Zhong JH, Xiang BD, Gong WF, Ke Y, Mo QG,
Ma L, Liu X and Li LQ: Comparison of long-term survival of patients
with BCLC stage B hepatocellular carcinoma after liver resection or
transarterial chemoembolization. PLoS One. 8:e681932013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Forner A, Reig ME, de Lope CR and Bruix J:
Current strategy for staging and treatment: The BCLC update and
future prospects. Semin Liver Dis. 30:61–74. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chun JM, Kwon HJ, Sohn J, Kim SG, Park JY,
Bae HI, Yun YK and Hwang YJ: Prognostic factors after early
recurrence in patients who underwent curative resection for
hepatocellular carcinoma. J Surg Oncol. 103:148–151. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Poon RT: Differentiating early and late
recurrences after resection of HCC in cirrhotic patients:
Implications on surveillance, prevention, and treatment strategies.
Ann Surg Oncol. 16:792–794. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Garaci E, Pica F, Serafino A, Balestrieri
E, Matteucci C, Moroni G, Sorrentino R, Zonfrillo M, Pierimarchi P
and Sinibaldi-Vallebona P: Thymosin α1 and cancer: Action on immune
effector and tumor target cells. Ann N Y Acad Sci. 1269:26–33.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Nitta H, Beppu T, Imai K, Hayashi H,
Chikamoto A and Baba H: Adjuvant hepatic arterial infusion
chemotherapy after hepatic resection of hepatocellular carcinoma
with macroscopic vascular invasion. World J Surg. 37:1034–1042.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zhong JH, Li H, Li LQ, You XM, Zhang Y,
Zhao YN, Liu JY, Xiang BD and Wu GB: Adjuvant therapy options
following curative treatment of hepatocellular carcinoma: A
systematic review of randomized trials. Eur J Surg Oncol.
38:286–295. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Wu C, Chen Y, Ho HJ, Hsu YC, Kuo KN, Wu MS
and Lin JT: Association between nucleoside analogues and risk of
hepatitis B virus-related hepatocellular carcinoma recurrence
following liver resection. JAMA. 308:1906–1913. 2012. View Article : Google Scholar : PubMed/NCBI
|