Introduction
Central nervous system (CNS) tumors are the
principal cause of tumor-associated mortality in childhood
(1), and the most common type of
malignant brain tumor in children is medulloblastoma (MB) (2). Craniospinal radiation and chemotherapy
following surgical resection are required for these patients.
Although all these therapies have improved the 5-year survival
rates of patients with MB (3), the
complications of long-term therapy, such as developmental,
neurological and neuroendocrine deficits, should not be neglected
(4,5).
Thus, safer therapies are needed for this disease. Previously, the
consensus was that MB consists of four subgroups: WNT, SHH, group 3
and group 4 (6), and the view that
the subgroups should be treated with diverse approaches is well
accepted (7). However, the respective
underlying molecular mechanisms of these MB subgroups have not been
determined. More accurate predictors and effective therapies are
required for MB.
Speckle-type POZ protein (SPOP), a type of adaptor
protein which may link Cullin-3 E3 ligase to multiple protein
substrates, is a member of the MATH-BTB protein family (8). Previously, multiple studies have
suggested that SPOP inhibits tumors by identifying that the gene
copies of SPOP are lost in certain types of human tumor (9,10).
Multiple studies have also demonstrated that SPOP directly targets
oncogenic proteins, including the Polycomb complex protein
(11), pancreatic and duodenal
homeobox protein 1 (12), apoptosis
factor death domain-associated protein 6 (13), and Hedgehog signaling transcription
factors zinc finger proteins GLI2 and GLI3 (14). Notably, the SPOP-like (SPOPL)
gene has been identified as a SPOP paralog gene (15), sharing an overall 85% sequence
identity with SPOP. The distinct difference between these genes is
that SPOPL exhibits 18 more amino acid residues compared
with SPOP (16). With the
exception of a case report indicating that SPOPL was one of
the deleted genes in a young male with unexplained somatopsychic
illness through array comparative genomic hybridization (17), there is little knowledge of
SPOPL in tumor generation and development. The high
similarity of SPOPL to SPOP may indicate that
SPOPL also functions as a tumor suppressor. However, a
previous study of Cullin-RING ubiquitin ligase demonstrated that
SPOP self-assembly and E3 ubiquitin ligase activity were inhibited
by SPOPL in a dose-dependent manner (16). Therefore, the role of SPOPL in
human malignancy is worth evaluating.
In the present study, the expression of SPOPL
in MB tissue specimens and cell lines was first detected, and it
focused on determining whether SPOPL is associated with the
tumor suppression of MBs, and whether it would be a feasible
indicator for estimating the prognosis of MBs following
treatment.
Materials and methods
Tissue samples
A total of 58 formalin-fixed paraffin-embedded MB
samples and 4 fresh MB surgical samples and matched adjacent normal
human cerebellums were gathered from the Neurosurgery Department of
the First Affiliated Hospital of Sun Yat-Sen University (Guangzhou,
China) between June 2002 and March 2014. The inclusion of patients
in the study was unbiased and depended exclusively on the
availability of sufficient tumor material and clinical follow-up
data. Table I summarizes the clinical
information corresponding to the samples. The following information
was assessed: General information (age and sex) and residual tumor
size. The MB patients were divided into two groups on the basis of
the metastatic phase, age and extent of resection. Infants (≤3
years of age), patients with residual tumor (≥1.5 cm2)
following neurosurgery and patients with leptomeningeal
dissemination at presentation belonged to the high-risk group;
otherwise, patients belonged to the standard-risk group (18). The World Health Organization (WHO)
histological subtype (19),
metastatic status and differentiation level was evaluated by a
pathologist following hematoxylin and eosin staining using the
following procedure: 4-µm thick serial sections were fixed for 20
min at 98°C with sodium citrate buffer (10 mM sodium citrate, 0.05%
Tween-20, pH 6.0), and then stained with hematoxylin (Beijing
Dingguo Changsheng Biotechnology Co., Ltd., Beijing, China) for 45
sec and 1% eosin for 10 sec at room temperature. The evaluation was
performed with a CX31 microscope (abbe condenser with blue filter)
and corresponding Image Analysis system software (CellSens
Standard, version1.16; both from Olympus Corporation, Tokyo,
Japan). A follow-up investigation was performed for all 58
patients, and December 2014 was the final date of follow-up for the
present study. The present study was approved by the Ethics
Committee of Sun Yat-Sen University and written informed consent
was obtained from all subjects.
 | Table I.Clinicopathological characteristics of
patient samples and expression of SPOPL in medulloblastoma. |
Table I.
Clinicopathological characteristics of
patient samples and expression of SPOPL in medulloblastoma.
| Clinicopathological
characteristic | No. of cases (%) |
|---|
| Age, years |
|
| ≤3 | 5 (8.6) |
|
>3 | 53 (91.4) |
| Sex |
|
| Male | 46 (79.3) |
|
Female | 12 (20.7) |
| WHO histological
subtype |
|
|
Classic | 44 (75.9) |
|
Desmoplastic | 14 (24.1) |
| Residual tumor
size, cm2 |
|
|
<1.5 | 44 (75.9) |
|
≥1.5 | 14 (24.1) |
| Metastatic
status |
|
| M0 | 25 (43.1) |
| M1 | 33 (56.9) |
| Tumor risk |
|
|
Standard | 17 (29.3) |
|
High | 41 (70.7) |
| Differentiation
level |
|
|
Undifferentiated | 19 (32.8) |
|
Differentiated | 39 (67.2) |
| Expression of
SPOPL |
|
|
Negative | 2 (3.4) |
|
Positive | 56 (96.6) |
|
Low | 42 (75) |
|
High | 14 (25) |
Immunohistochemical staining and
scoring
Each tissue block was cut into 4-µm thick serial
sections on aminopropyltriethoxysilane-coated glass slides, and
fixed as described above. Then the sections were incubated with
anti-SPOPL antibody (1:50 dilution; catalog no. 191175; Abcam,
Cambridge, UK) overnight at 4°C in a humidified chamber. Next, the
slides were processed using a ChemMate EnVision/horseradish
peroxidase kit (Dako; Agilent Technologies, Inc., Santa Clara, CA,
USA) for 30 min at room temperature, which was followed by
processing with diaminobenzidine for visualization. All sections
were counterstained with Mayer's hematoxylin (Beijing Dingguo
Changsheng Biotechnology Co., Ltd.) for 30 sec at room temperature.
Normal human cerebellum was used as a control.
Immunohistochemical staining evaluation was
performed based on the proportion and intensity of positively
stained tumor cells (20,21). The scoring was as follows: 0, 0–5; 1,
6–25; 2, 26–50; 3, 51–75; and 4, >75%. The staining intensity
was scored as one of the following four grades: 0, negative; 1,
weak; 2, moderate; and 3, strong. The final score for each section
was the product of the percentage and intensity score. The SPOPL
protein expression level was categorized as lower (final score
<4) and higher (final score ≥4). Two pathologists separately
scored all immunohistochemical staining. The pathologists were not
familiar with the patient information. The mean scores were the
final score in each case. All evaluation was performed with the
microscope and image analysis software as described above.
Cell culture
The normal human astrocytes (NHAs) were obtained
from the American Type Culture Collection (Manassas, VA, USA) and
human medulloblastoma Daoy, D283 and D341 cell lines were from the
Institute of Basic Medical Sciences of the Chinese Academy of
Medical Sciences (Beijing, China). The Daoy and D283 cell lines
were cultured in Dulbecco's modified Eagle's medium (Gibco; Thermo
Fisher Scientific, Inc., Waltham, MA, USA). The D341 cell line was
cultured in RPMI-1640 medium (Gibco; Thermo Fisher Scientific,
Inc.), and NHA was cultured in Astrocyte medium (#1801; ScienCell
Research Laboratories, Carlsbad, CA, USA) with astrocyte growth
supplement and 10% fetal bovine serum (Thermo Fisher Scientific,
Inc.). All cells were incubated at 37°C in a humidified incubator
in the presence of 5% CO2.
RNA extraction and reverse
transcription-quantitative polymerase chain reaction (RT-qPCR)
Total RNA was isolated using TRIzol reagent
(Invitrogen; Thermo Fisher Scientific, Inc.) according to the
manufacturer's protocol. cDNA was generated using a First-Strand
cDNA Synthesis kit (Thermo Fisher Scientific, Inc.). Real-time PCR
was performed with SYBR-Green qPCR kit on the OpenArray® Real-Time
PCR Platform (both from Thermo Fisher Scientific, Inc.), and
expression levels of the SPOPL gene were calculated by the
2−ΔΔCq method (22) and
normalized to GAPDH (internal control). The PCR program was: 10 min
at 95°C, followed by 40 cycles of 15 sec at 95°C and 60 sec at
60°C. Relative mRNA levels of SPOPL were measured in relation to
NHA and normal human cerebellum as positive control. Primers were
designed using the Primer Express software (version 2.0 software;
Applied Biosystems; Thermo Fisher Scientific, Inc.), and the primer
sequences were as follows: SPOPL forward,
5′-GCTGGAGTCGTAACTCGGAAG-3′ and reverse,
5′-CCCTATCTCCCGCTCCTAAAC-3′; GAPDH forward,
5′-GACTCATGACCACAGTCCATGC-3′ and reverse,
5′-AGAGGCAGGGATGATGTTCTG-3′. The RT-qPCR analysis was performed at
least three times.
Western blot analysis
The NHA, Daoy, D283 and D341 cells were lysed in
lysis buffer (catalog no. P0013B; Beyotime Institute of
Biotechnology, Haimen, China) on ice and then centrifuged at 12,000
× g for 10 min at 4°C. The protein contents in the supernatants
were determined using a Bicinchoninic Acid protein assay kit
(Pierce; Thermo Fisher Scientific, Inc.). Equal amounts of protein
lysates (50 mg) were separated by SDS-PAGE (10% gels) and
transferred on to polyvinylidene difluoride membranes (EMD
Millipore, Billerica, MA, USA). The membranes were blocked with 1%
bovine serum albumin for 2 h at room temperature, and then
incubated with anti-SPOPL (catalog no. 191175; dilution, 1:1,000;
Abcam, Cambridge, UK) and anti-β-actin primary antibody (catalog
no. AF7018; dilution, 1:1,000; EarthOx Life Sciences, Millbrae, CA,
USA) overnight at 4°C. Then, horseradish peroxidase-conjugated
secondary antibody was added for 2 h at room temperature. Enhanced
chemiluminescence by ECL substrate (Pierce; Thermo Fisher
Scientific, Inc.) was used for detection. Experiments were
performed at least twice.
Statistical analysis
SPSS software (version 16.0 for Windows; SPSS Inc.,
Chicago, IL, USA) was used for statistical analysis. A
χ2 test was used for comparisons between groups.
P<0.05 was considered to indicate a statistically significant
difference. The overall survival (OS) time was measured (months)
from the date of diagnosis to the date of mortality or the last
follow-up prior to study termination. The Kaplan-Meier estimator
method and Cox's regression were used for survival analysis.
Results
Downregulation of SPOPL mRNA and
protein levels in MB cell lines and primary MB tumors
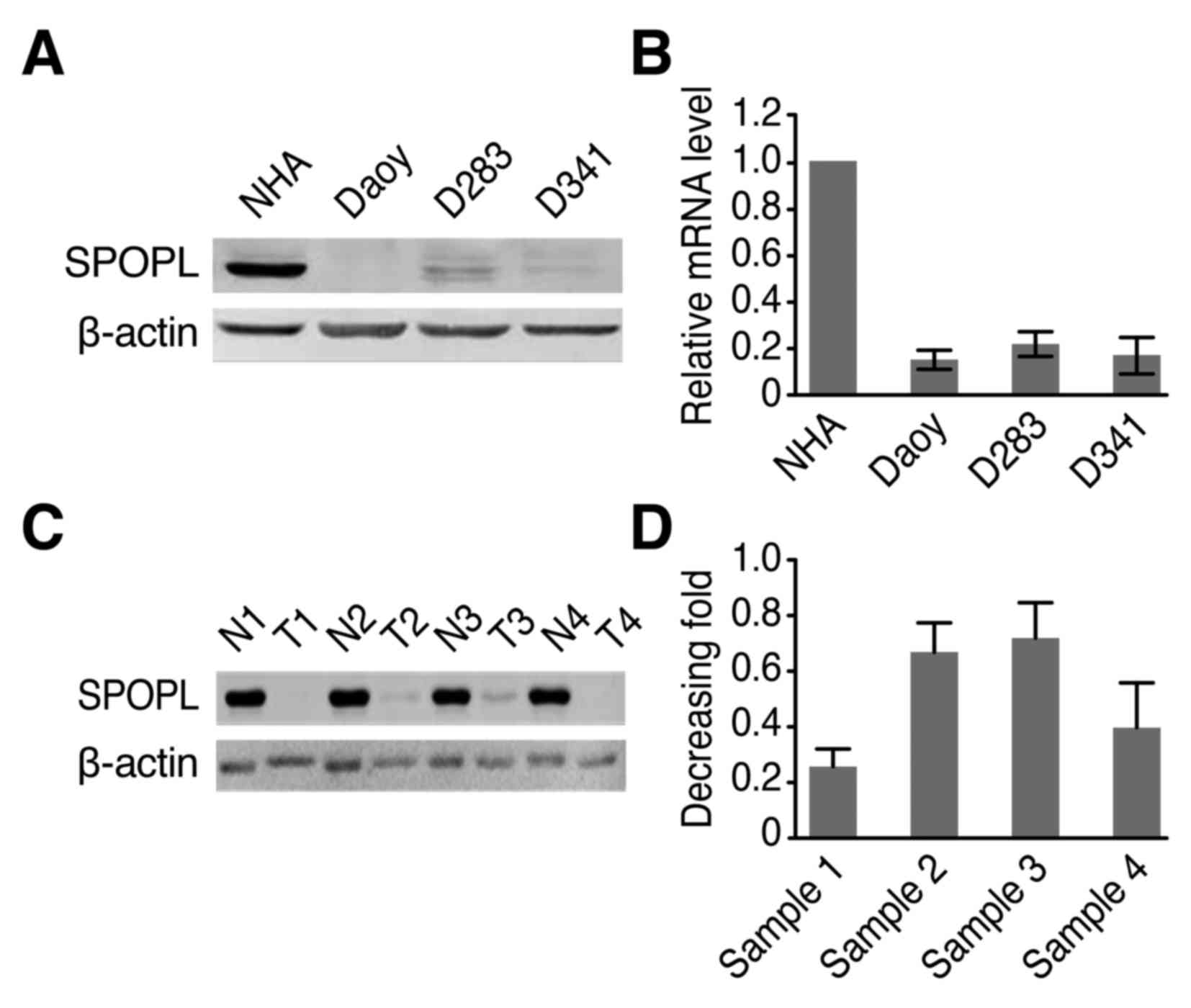
Western blotting results demonstrated that the SPOPL
protein level was significantly decreased in the MB cell lines
compared with the NHA cells (Fig.
1A). RT-qPCR results additionally confirmed that the SPOPL mRNA
level was also decreased in the MB cell lines compared with the NHA
cells (Fig. 1B). A total of four
pairs of MB samples and normal human cerebellum were detected by
western blotting to explore whether they exhibited similar
tendencies. The present study demonstrated that SPOPL was
differentially expressed in all four human MB samples compared with
the normal human cerebellum, as presented in Fig. 1C. This result is similar to the
results obtained for the mRNA level. As demonstrated in Fig. 1D, the tumor/normal ratio of SPOPL
signals exhibited an 0.25–0.7-fold difference in the four tissue
pairs. These results indicate decreased SPOPL expression in
cancer lesions.
Decreased SPOPL expression in archived
MB tissues
On the basis of the aforementioned results, whether
SPOPL exhibits decreased expression levels in a larger
cohort of clinical samples was assessed. In total, 58 archived MB
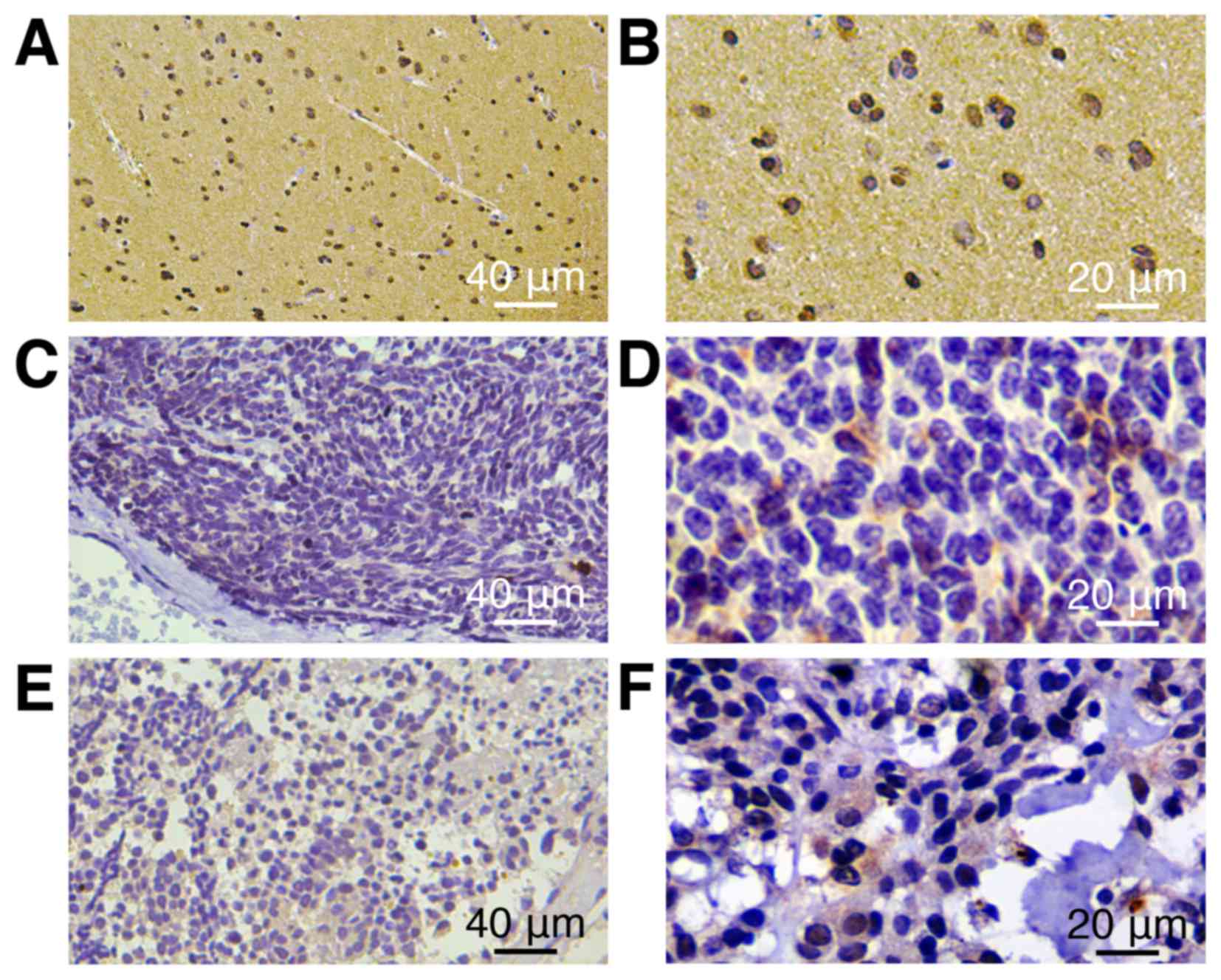
tissues were examined. SPOPL was detected in 56/58 (96.7%)
cases. According to immunohistochemical staining evaluation, the 56
cases were separated into two groups: 42 cases with decreased
expression (75%) and 14 cases with increased expression (25%). In
contrast, more intense SPOPL staining was observed in the
normal human cerebellum (Fig. 2).
Statistical analyses were performed to explore the association
between SPOPL and the clinicopathological characteristics of MB. As
summarized in Table II, SPOPL
expression was markedly associated with the tumor differentiation
level (P=0.011), whereas no association was identified with the
patient age, WHO histological subtype or tumor risk with MB.
| Table II.Association between SPOPL and the
clinicopathological characteristics of patients with MB. |
Table II.
Association between SPOPL and the
clinicopathological characteristics of patients with MB.
|
| SPOPL |
|
|---|
|
|
|
|
|---|
| Characteristic | Low or none | High | χ2
(P-value) |
|---|
| Age, years |
|
|
|
| ≤3 | 4 | 1 | 0.821 |
|
>3 | 40 | 13 |
|
| Sex |
|
|
|
|
Male | 34 | 12 | 0.764 |
|
Female | 10 | 2 |
|
| WHO histological
subtype |
|
|
|
|
Classic | 34 | 10 | 0.931 |
|
Desmoplastic | 10 | 4 |
|
| Residual tumor
size, cm2 |
|
|
|
|
<1.5 | 41 | 14 | 0.756 |
|
≥1.5 | 3 | 0 |
|
| Metastatic
status |
|
|
|
| M0 | 19 | 6 | 0.983 |
| M1 | 25 | 8 |
|
| Tumor risk |
|
|
|
|
Standard | 16 | 5 | 0.965 |
|
High | 28 | 9 |
|
| Differentiation
level |
|
|
|
|
Undifferentiated | 10 | 9 | 0.011 |
|
Differentiated | 34 | 5 |
|
SPOPL expression is associated with
the prognosis of patients with MB
SPOPL expression in patients with MB was
significantly associated with the survival time of patients
(P<0.05) at a coefficient of 0.187, which manifested in
increased SPOPL expression and survival time in patients
with MB (Table III). The effects of
SPOPL and classic clinicopathological characteristics
(including age, sex, WHO histological subtype, residual tumor size,
metastatic status and differentiation level) on the survival rates
by Kaplan-Meier estimator analysis and the log-rank test were
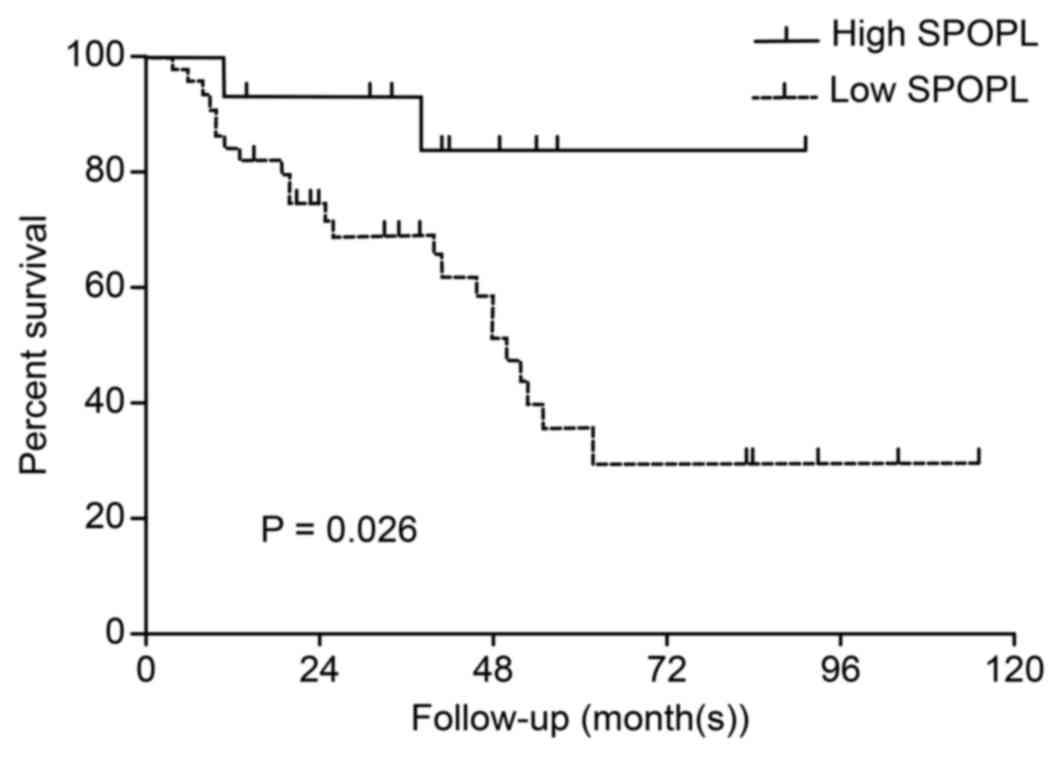
calculated. The results indicated that the survival time
significantly differed between the low and high SPOPL
expression groups (P<0.05). As presented in Fig. 3, the cumulative 5-year survival rate
for the low SPOPL expression group was only 35.1% [95%
confidence interval (CI) 0.439–0.720], whereas it was 83.6% in the
high SPOPL expression group (95% CI 0.668–0.940).
Furthermore, multivariate survival analysis was performed to test
the SPOPL expression level, age, sex, WHO histological
subtype, metastatic status and differentiation level to determine
whether SPOPL was an independent prognostic factor of the
outcome of patients with MB. The residual tumor size and SPOPL
expression were independent prognostic factors (Table IV). Thus, it was concluded that the
SPOPL gene is associated with MB prognosis.
| Table III.Kaplan-Meier estimator analysis for
overall survival rate of patients with medulloblastoma. |
Table III.
Kaplan-Meier estimator analysis for
overall survival rate of patients with medulloblastoma.
| Clinicopathological
characteristics | STQ2
(STQ1, STQ3), months |
P-valuea |
|---|
| Age, years |
|
|
| ≤3 | 20 (13, 21) | 0.161 |
|
>3 | 41 (20.5, 55) |
|
| Sex |
|
|
|
Male | 41 (19, 53) | 0.585 |
|
Female | 40 (24, 56) |
|
| WHO histological
subtype |
|
|
|
Classic | 40 (19.75, 55) | 0.820 |
|
Desmoplastic | 37.5 (17.75,
60.75) |
|
| Residual tumor
size, cm2 |
|
|
|
<1.5 | 40 (20, 54) | 0.001 |
|
≥1.5 | 19 (11, 25) |
|
| Metastatic
status |
|
|
| M0 | 32.5 (14.75,
53.25) | 0.562 |
| M1 | 41.5 (20, 55) |
|
| Tumor risk |
|
|
|
Standard | 40 (19.5,
53.5) | 0.352 |
|
High | 26 (19, 57) |
|
| Differentiation
level |
|
|
|
Undifferentiated | 38 (14, 53.5) | 0.273 |
|
Differentiated | 41 (24, 55) |
|
| SPOPL
expression |
|
|
|
Low | 36.5 (19,
53.5) | 0.026 |
|
High | 41.5 (33.25,
57) |
|
| Table IV.Cox regression model for multivariate
analyses of prognostic factor in medulloblastoma. |
Table IV.
Cox regression model for multivariate
analyses of prognostic factor in medulloblastoma.
| Variable | Hazard ratio | 95% confidence
interval | P-value |
|---|
| Age, years (≤3 vs.
>3) | 4.443 | 0.451–43.78 | 0.201 |
| Sex (male vs.
female) | 1.779 | 0.550–5.755 | 0.336 |
| WHO histological
subtype (classic vs. desmoplastic) | 1.454 | 0.507–4.169 | 0.486 |
| Metastatic status
(M0 vs. M1) | 1.089 | 0.083–14.29 | 0.949 |
| Residual tumor
size, cm2 (<1.5 vs. ≥1.5) | 7.639 | 1.663–35.09 | 0.009 |
| Tumor risk
(standard vs. high) | 0.906 | 0.055–14.84 | 0.945 |
| Differentiation
(differentiated vs. undifferentiated) | 0.571 | 0.211–1.546 | 0.270 |
| Speckle-type POZ
protein-like expression (low vs. high) | 0.218 | 0.048–0.982 | 0.047 |
Discussion
To the best of our knowledge, the present study is
the first to demonstrate that decreased SPOPL expression is
associated with the decreased survival time of patients with MB.
SPOPL expression is decreased in MB cell lines at the mRNA
and protein levels, which is in contrast with NHAs. Additionally,
MB lesions and normal human cerebellum tissues express SPOPL
at different levels, and MB tissues exhibit markedly decreased
expression of SPOPL at the mRNA and protein levels.
Furthermore, immunostaining demonstrated that the SPOPL
expression in histological sections was significantly associated
with the tumor differentiation level (P=0.011), and increased
survival time of patients with MB. Taken together, these results
indicate that SPOPL potentially represents a novel marker
for determining the prognosis of MB.
As indicated by previous studies, SPOP regulates
signaling pathways that control numerous types of cellular response
that are essential to tumor progression, including proliferation
and differentiation (23,24). Currently, SPOP is considered important
in numerous tumor types, including breast, prostate, liver, gastric
and colorectal cancer (25,26). In brain tumors, Ding et al
(27) identified that decreased
expression of SPOP is associated with a poor prognosis in
glioma. All these results indicate that SPOP serves a role
in tumor suppression. As it shares a high sequence identity with
SPOP, SPOPL may also exhibit similar functions to
those of SPOP, including tumor suppression. Notably,
Errington et al (16)
identified that SPOPL could interact with SPOP and
inhibit its self-assembly and further affect E3 ubiquitin ligase
activity, which indicated that SPOPL may serve the opposite
role in tumorigenesis compared with SPOP. The present study
provided evidence that SPOPL reduction may serve a role in
MB progression, suggesting that SPOPL serves the same role
in tumorigenesis as SPOP
As identified by immunohistochemical detection,
42/56 (75%) paraffin-embedded archival MB biopsies revealed weak
SPOPL staining, whereas strong SPOPL staining was
observed in normal human cerebellum tissues, indicating that
SPOPL loss may accelerate the development and progression of
MB. The present study of the association between SPOPL and
clinical characteristics demonstrated a marked association between
SPOPL and differentiation level of MB cells, suggesting that
SPOPL may be used as a possible valuable marker for
identifying patients with MB. The 35.1% 5-year survival rate of
patients with low SPOPL expression, which was decreased
compared with the 83.6% rate in the high SPOPL expression
group, indicates that SPOPL may be used as a prognosis and
survival predictor for patients with MB. Additional studies are
required to confirm these data, and to verify the significance of
SPOPL. In addition, more functional analyses are also
required to elucidate the role of SPOPL in MB.
In conclusion, the present study assessed the
possibility of using SPOPL as a prognostic marker for MB.
Additionally, SPOPL may be regarded as a novel MB biomarker
for evaluating therapeutic strategies and developing treatment
standards. Therefore, additional studies on the mechanism of SPOPL
and more clinical patients with MB are required.
Acknowledgements
The present study was supported by the National
Natural Science Foundation of China (grant nos. 81370072 and
81572477), the Natural Science Foundation of Guangdong Province for
Distinguished Young Scholars (grant no. S2013050014535), the Key
Project Supported by the Science and Technology Planning Project of
Guangdong Province (grant no. S2012020006147), the Scientific
Research Project of Guangdong Provincial Science and Technology
(grant no. 2013B021800111), the Pearl River New Star Science and
Technology Program of Guangzhou City (grant no. 2013J2200022) and
the Science and Technology Program of Guangzhou City (grant no.
2013J4100060).
References
|
1
|
Pui CH, Gajjar AJ, Kane JR, Qaddoumi IA
and Pappo AS: Challenging issues in pediatric oncology. Nat Rev
Clin Oncol. 8:540–549. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Mueller S and Chang S: Pediatric brain
tumors: Current treatment strategies and future therapeutic
approaches. Neurotherapeutics. 6:570–586. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Packer RJ and Vezina G: Management of and
prognosis with medulloblastoma: Therapy at a crossroads. Arch
Neurol. 65:1419–1424. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Northcott PA, Jones DT, Kool M, Robinson
GW, Gilbertson RJ, Cho YJ, Pomeroy SL, Korshunov A, Lichter P,
Taylor MD and Pfister SM: Medulloblastomics: The end of the
beginning. Nat Rev Cancer. 12:818–834. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Spiegler BJ, Bouffet E, Greenberg ML,
Rutka JT and Mabbott DJ: Change in neurocognitive functioning after
treatment with cranial radiation in childhood. J Clin Oncol.
22:706–713. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Taylor MD, Northcott PA, Korshunov A,
Remke M, Cho YJ, Clifford SC, Eberhart CG, Parsons DW, Rutkowski S,
Gajjar A, et al: Molecular subgroups of medulloblastoma: The
current consensus. Acta Neuropathol. 123:465–472. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Samkari A, White JC and Packer RJ:
Medulloblastoma: Toward biologically based management. Semin
Pediatr Neurol. 22:6–13. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zhuang M, Calabrese MF, Liu J, Waddell MB,
Nourse A, Hammel M, Miller DJ, Walden H, Duda DM, Seyedin SN, et
al: Structures of SPOP-substrate complexes: Insights into molecular
architectures of BTB-Cul3 ubiquitin ligases. Mol Cell. 36:39–50.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Berger MF, Lawrence MS, Demichelis F,
Drier Y, Cibulskis K, Sivachenko AY, Sboner A, Esgueva R, Pflueger
D, Sougnez C, et al: The genomic complexity of primary human
prostate cancer. Nature. 470:214–220. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kan Z, Jaiswal BS, Stinson J, Janakiraman
V, Bhatt D, Stern HM, Yue P, Haverty PM, Bourgon R, Zheng J, et al:
Diverse somatic mutation patterns and pathway alterations in human
cancers. Nature. 466:869–873. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hernández-Muñoz I, Lund AH, van der Stoop
P, Boutsma E, Muijrers I, Verhoeven E, Nusinow DA, Panning B,
Marahrens Y and van Lohuizen M: Stable X chromosome inactivation
involves the PRC1 Polycomb complex and requires histone MACROH2A1
and the CULLIN3/SPOP ubiquitin E3 ligase. Proc Natl Acad Sci USA.
102:pp. 7635–7640. 2005; View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Liu A, Desai BM and Stoffers DA:
Identification of PCIF1, a POZ domain protein that inhibits PDX-1
(MODY4) transcriptional activity. Mol Cell Biol. 24:4372–4383.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kwon JE, La M, Oh KH, Oh YM, Kim GR, Seol
JH, Baek SH, Chiba T, Tanaka K, Bang OS, et al: BTB
domain-containing speckle-type POZ protein (SPOP) serves as an
adaptor of Daxx for ubiquitination by Cul3-based ubiquitin ligase.
J Biol Chem. 281:12664–12672. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wang C, Pan Y and Wang B: Suppressor of
fused and Spop regulate the stability, processing and function of
Gli2 and Gli3 full-length activators but not their repressors.
Development. 137:2001–2009. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Choo KB, Chuang TJ, Lin WY, Chang CM, Tsai
YH and Huang CJ: Evolutionary expansion of SPOP and associated
TD/POZ gene family: Impact of evolutionary route on gene expression
pattern. Gene. 460:39–47. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Errington WJ, Khan MQ, Bueler SA,
Rubinstein JL, Chakrabartty A and Privé GG: Adaptor protein
self-assembly drives the control of a cullin-RING ubiquitin ligase.
Structure. 20:1141–1153. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Mulatinho MV, de Carvalho Serao CL, Scalco
F, Hardekopf D, Pekova S, Mrasek K, Liehr T, Weise A, Rao N and
Llerena JC Jr: Severe intellectual disability, omphalocele,
hypospadia and high blood pressure associated to a deletion at
2q22.1q22.3: Case report. Mol Cytogenet. 5:302012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ellison DW, Clifford SC, Gajjar A and
Gilbertson RJ: What's new in neuro-oncology? Recent advances in
medulloblastoma. Eur J Paediatr Neurol. 7:53–66. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Louis DN, Ohgaki H, Wiestler OD, Cavenee
WK, Burger PC, Jouvet A, Scheithauer BW and Kleihues P: The 2007
WHO classification of tumours of the central nervous system. Acta
Neuropathol. 114:97–109. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Song LB, Liao WT, Mai HQ, Zhang HZ, Zhang
L, Li MZ, Hou JH, Fu LW, Huang WL, Zeng YX and Zeng MS: The
clinical significance of twist expression in nasopharyngeal
carcinoma. Cancer Lett. 242:258–265. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Fukuoka J, Fujii T, Shih JH, Dracheva T,
Meerzaman D, Player A, Hong K, Settnek S, Gupta A, Buetow K, et al:
Chromatin remodeling factors and BRM/BRG1 expression as prognostic
indicators in non-small cell lung cancer. Clin Cancer Res.
10:4314–4324. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression using real time quantitative PCR and the
2(−Delta Delta C(T)) method. Methods. 25:402–408. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Zhang D, Wang H, Sun M, Yang J, Zhang W,
Han S and Xu B: Speckle-type POZ protein, SPOP, is involved in the
DNA damage response. Carcinogenesis. 35:1691–1697. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Mani RS: The emerging role of speckle-type
POZ protein (SPOP) in cancer development. Drug Discov Today.
19:1498–1502. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kim MS, Je EM, Oh JE, Yoo NJ and Lee SH:
Mutational and expressional analyses of SPOP, a candidate tumor
suppressor gene, in prostate, gastric and colorectal cancers.
APMIS. 121:626–633. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kim MS, Kim MS, Yoo NJ and Lee SH: Somatic
mutation of SPOP tumor suppressor gene is rare in breast, lung,
liver cancers, and acute leukemias. APMIS. 122:164–166. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ding D, Song T, Jun W, Tan Z and Fang J:
Decreased expression of the SPOP gene is associated with poor
prognosis in glioma. Int J Oncol. 46:333–341. 2015.PubMed/NCBI
|