Introduction
Colorectal cancer (CRC) is the third most common
cancer and the fourth leading cause of cancer-related deaths
worldwide, accounting for roughly 1.36 million new people and
690,000 deaths per year in 2012 (1).
The outcome of patients with CRC is related to the stage at
diagnosis: The 5-year relative survival is 95.0% for CRC patients
with stage I, 83.3% for those with stage II, 77.4% for those with
stage III, and 16.9% for those with stage IV (2). Although adjuvant chemotherapy is
recommended for CRC with high risk of relapse, its administration
to patients with stage II and III CRC, in which the 5-year relapse
rates are approximately 20 and 35–50%, respectively, remains
controversial (3,4). Because patients with CRC that is
identical in grade and stage often have significantly different
clinical outcomes or responses to therapy and there are no
established biomarkers to predict relapse, improved tumor
classification is needed for CRC, especially for stage II and III
CRC.
The Wnt/β-catenin signaling pathway plays an
essential role in the development of various tumors (5,6). It is
well known that the Wnt/β-catenin signaling pathway is activated in
most sporadic CRC (up to 80%) (7).
Recently, LGR5 (leucine-rich repeat containing G-protein-coupled
receptor 5) was identified as the target gene of the Wnt/β-catenin
signaling pathway (8,9). LGR5 is reported to be a biomarker of
cancer stem cells of CRC and stem cells in adult intestinal crypts
(10,11). TROY (tumor necrosis factor receptor
superfamily member 19, TNFRSF19, TAJ) is a type I cell surface
receptor protein containing the highly conserved TNFR cysteine-rich
motifs in the extracellular domain and a TNF receptor-associated
factor (TRAF)-binding sequence in the large cytoplasmic domain
required for signaling (12).
Recently, TROY was reported to be a β-catenin target gene
and to form a complex with LGR5 in cellular membranes (13). Although overexpression of TROY is
observed in CRC cell lines (14–17), its
clinical significance for CRC is poorly understood. Because TROY
might be a possible prognostic biomarker of CRC, we performed this
study to investigate the clinical significance of TROY in patients
with CRC and compared its clinical usefulness to that of LGR5.
Materials and methods
Materials
We collected 100 CRC tissues from 100 patients who
underwent surgical treatment at the Department of
Gastroenterological, Breast and Endocrine Surgery, Yamaguchi
University Graduate School of Medicine between March 2000 and May
2008. From them, 36 matched normal-appearing mucosa tissues were
also collected from a site distal to the resected materials. All
samples were immediately frozen in liquid nitrogen after sample
collection from surgically resected materials and then stored at
−80°C. Total RNA was isolated using the AllPrep DNA/RNA Mini Kit
(QIAGEN). The extracted total RNA was reverse transcribed into
single-stranded cDNA using a High-Capacity cDNA Archive Kit
(Applied Biosystems; Thermo Fisher Scientific, Inc., Waltham, MA,
USA).
The clinicopathologic characteristics of the CRC
patients are shown in Table I. The
patient population consisted of 51 men and 49 women with a mean age
of 66.9 years (range, 38–92 years). According to the staging system
of the International Union Against Cancer (UICC) (18), 14 patients were stage I, 36 patients
were stage II, 30 patients were stage III, and 20 patients were
stage IV. After surgical treatments, 66 patients were treated with
adjuvant chemotherapies using tegafur/uracil, cisplatin, or
irinotecan, and 34 patients did not receive any adjuvant
chemotherapy. This study was approved by the Institutional Review
Board of Yamaguchi University Hospital (approval number: H28-073),
and written informed consent was obtained from each patient before
inclusion in the study.
 | Table I.Relation between clinicopathologic
factors and patient outcomes. |
Table I.
Relation between clinicopathologic
factors and patient outcomes.
|
|
| Relapse status | Survival
status |
|---|
|
|
|
|
|
|---|
| Factor | n | Disease-free
(n) | Relapse (n) | P-value | Survival (n) | Non-survival
(n) | P-value |
|---|
| Sex |
|
|
|
|
|
|
|
|
Male | 51 | 36 | 15 | 0.9000 | 38 | 13 | 0.5500 |
|
Female | 49 | 34 | 15 |
| 39 | 10 |
|
| Age in years (mean
± SD/range) pStage |
66.9±11.4/38–92 |
67.3±11.6/38–92 |
66.1±11.2/48–89 | 0.4900 |
67.3±11.4/38–92 |
65.5±11.7/49–89 | 0.5100 |
| I | 14 | 14 | 0 | NA | 14 | 0 | NA |
| II | 36 | 27 | 9 | 0.0390 | 30 | 6 | 0.1700 |
|
III | 30 | 21 | 9 | 0.0220 | 24 | 6 | 0.0720 |
| IV | 20 | 8 | 12 | 0.0003 | 9 | 11 | 0.0007 |
| pT |
|
|
|
|
|
|
|
| 1 | 8 | 8 | 0 | NA | 8 | 0 | NA |
| 2 | 9 | 8 | 1 | 0.3300 | 8 | 1 | 0.3300 |
| 3 | 70 | 48 | 22 | 0.0610 | 54 | 16 | 0.1300 |
| 4 | 13 | 6 | 7 | 0.0110 | 7 | 6 | 0.0230 |
| pN |
|
|
|
|
|
|
|
| 0 | 55 | 43 | 12 | NA | 47 | 8 | NA |
| 1 | 23 | 17 | 6 | 0.6800 | 17 | 6 | 0.2300 |
| 2 | 22 | 10 | 12 | 0.0051 | 13 | 9 | 0.0120 |
| pM |
|
|
|
|
|
|
|
| 0 | 80 | 62 | 18 | NA | 68 | 12 | NA |
| 1 | 20 | 8 | 12 | 0.0011 | 9 | 11 | 0.0001 |
| Lymphatic vessel
invasion |
|
|
|
|
|
|
|
|
Negative | 12 | 12 | 0 | NA | 12 | 0 | NA |
|
Positive | 88 | 58 | 30 | 0.0160 | 65 | 23 | 0.0440 |
| Vascular
invasion |
|
|
|
|
|
|
|
|
Negative | 31 | 26 | 5 | NA | 27 | 4 | NA |
|
Positive | 69 | 44 | 25 | 0.0430 | 50 | 19 | 0.1100 |
| Liver
metastasis |
|
|
|
|
|
|
|
|
Negative | 86 | 63 | 23 | NA | 70 | 16 | NA |
|
Positive | 14 | 7 | 7 | 0.0780 | 7 | 7 | 0.0096 |
| Peritoneal
metastasis |
|
|
|
|
|
|
|
|
Negative | 91 | 66 | 25 | NA | 74 | 17 | NA |
|
Positive | 9 | 4 | 5 | 0.0800 | 3 | 6 | 0.0011 |
| Histopathological
type |
|
|
|
|
|
|
|
| Well
differentiated adenocarcinoma | 29 | 25 | 4 | NA | 25 | 4 | NA |
|
Others | 71 | 44 | 26 | 0.0210 | 51 | 19 | 0.1500 |
| Postoperative
adjuvant chemotherapy |
|
|
|
|
|
|
|
| Not
performed | 34 | 31 | 3 | NA | 30 | 4 | NA |
|
Performed | 66 | 39 | 27 | 0.0009 | 47 | 19 | 0.0550 |
Quantitative real-time PCR
Quantitative real-time PCR was performed using
TaqMan Gene Expression Master Mix (Applied Biosystems; Thermo
Fisher Scientific, Inc.). The Applied Biosystems catalog numbers of
the primer and probe set for the endogenous control (β-actin) and
target genes were 4326315E for β-actin, Hs00969422_m1 for
LGR5, and Hs00218634_m1 for TROY. Quantitative
real-time PCR was performed on an ABI Prism 7900HT Sequence
Detection System (Applied Biosystems; Thermo Fisher Scientific,
Inc.). PCR cycling conditions included preheating at 50°C for 2 min
for optimal UDG (uracil-DNA glycosylase) enzyme activity and at
95°C for 10 min for AmpliTaq Gold DNA polymerase and UP enzyme
activation followed by 40 cycles of denaturation at 95°C for 15 sec
and annealing at 60°C for 1 min. All reactions were carried out in
a 20-µl reaction volume in triplicate. The mRNA expression level
was determined using the 2−∆∆CT method, in which
relative quantification of mRNA expression level was calculated
using β-actin as the internal reference (19).
Statistical analysis
Data analyses were performed using StatFlex v6
(Artech Co., Ltd., Osaka, Japan). Student's t-test, Fisher's exact
test, one-way analysis of variance (ANOVA) followed by Tukey
multiple comparison test, two-tailed Spearman's test, Kaplan-Meier
analysis, stepwise multiple regression analysis, or Cox
proportional hazard regressions analysis was used. Disease-free
survival (DFS) time was defined as the length of time after the
primary surgical treatment for CRC during which no recurrence was
detected. The follow-up period ended on June 30, 2016. Before the
analysis, a logarithmic transformation was performed on LGR5
and TROY mRNA expression values to obtain normally
distributed data sets. P<0.05 was considered to indicate a
statistically significant difference.
Results
LGR5 and TROY mRNA expression levels
in the CRC and non-tumor specimens
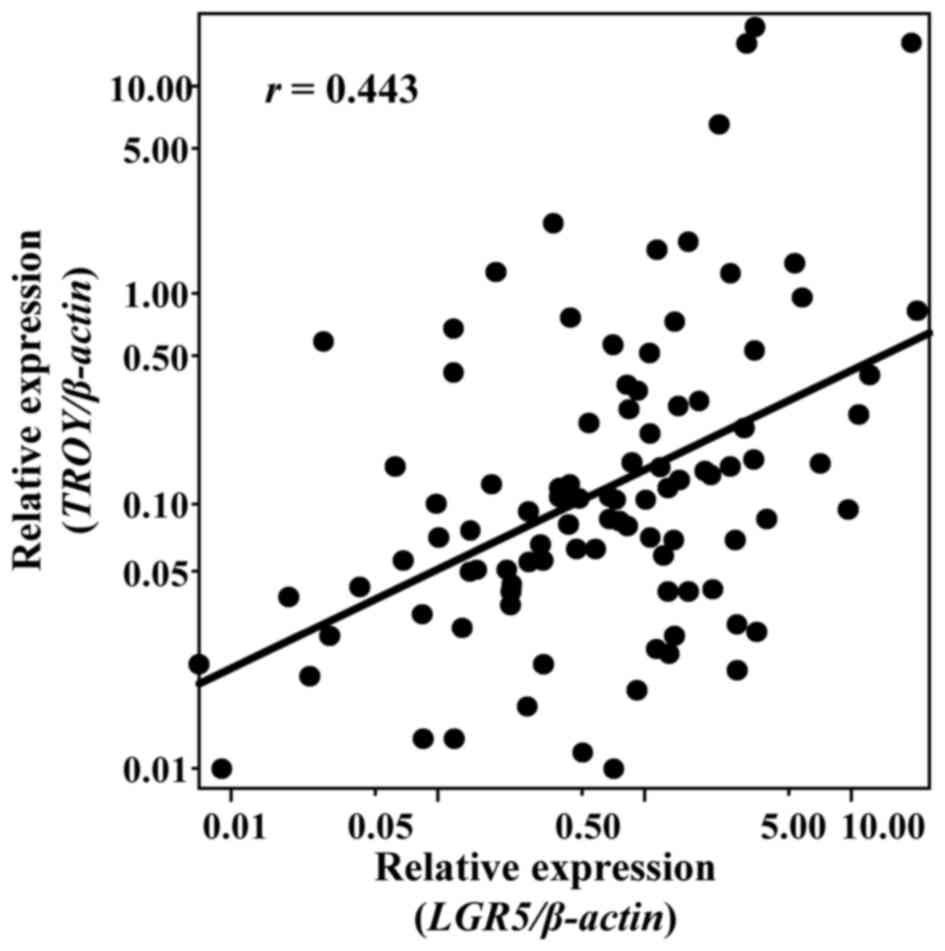
There was a positive correlation of expression level
between TROY and LGR5 (r=0.443, P<0.001 by
two-tailed Spearman's test) (Fig. 1).
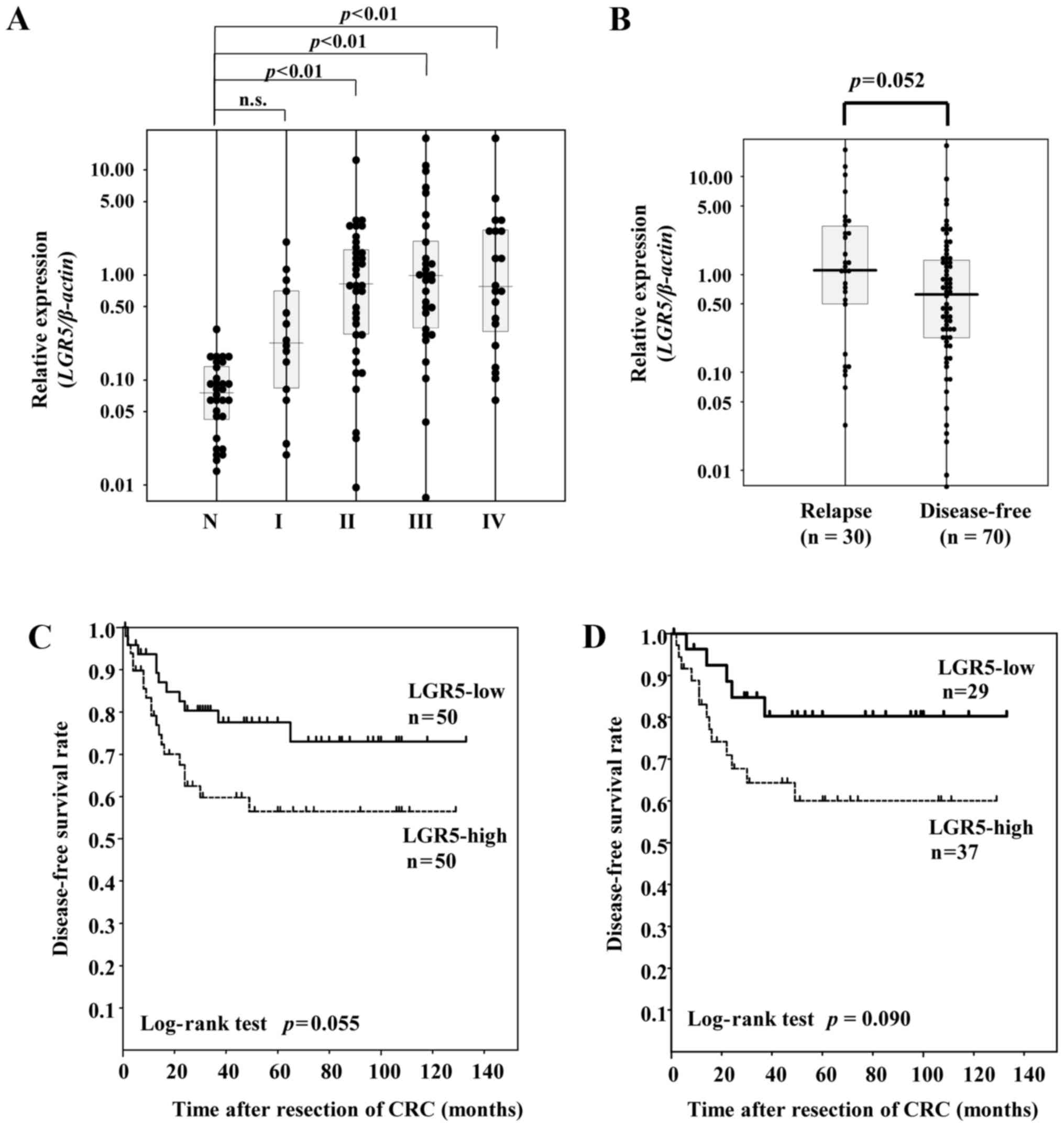
LGR5 mRNA expression levels were significantly higher in the
CRC tissues of each stage except for stage I than those in the
normal-appearing mucosa tissues (P<0.001 by one-way ANOVA; both
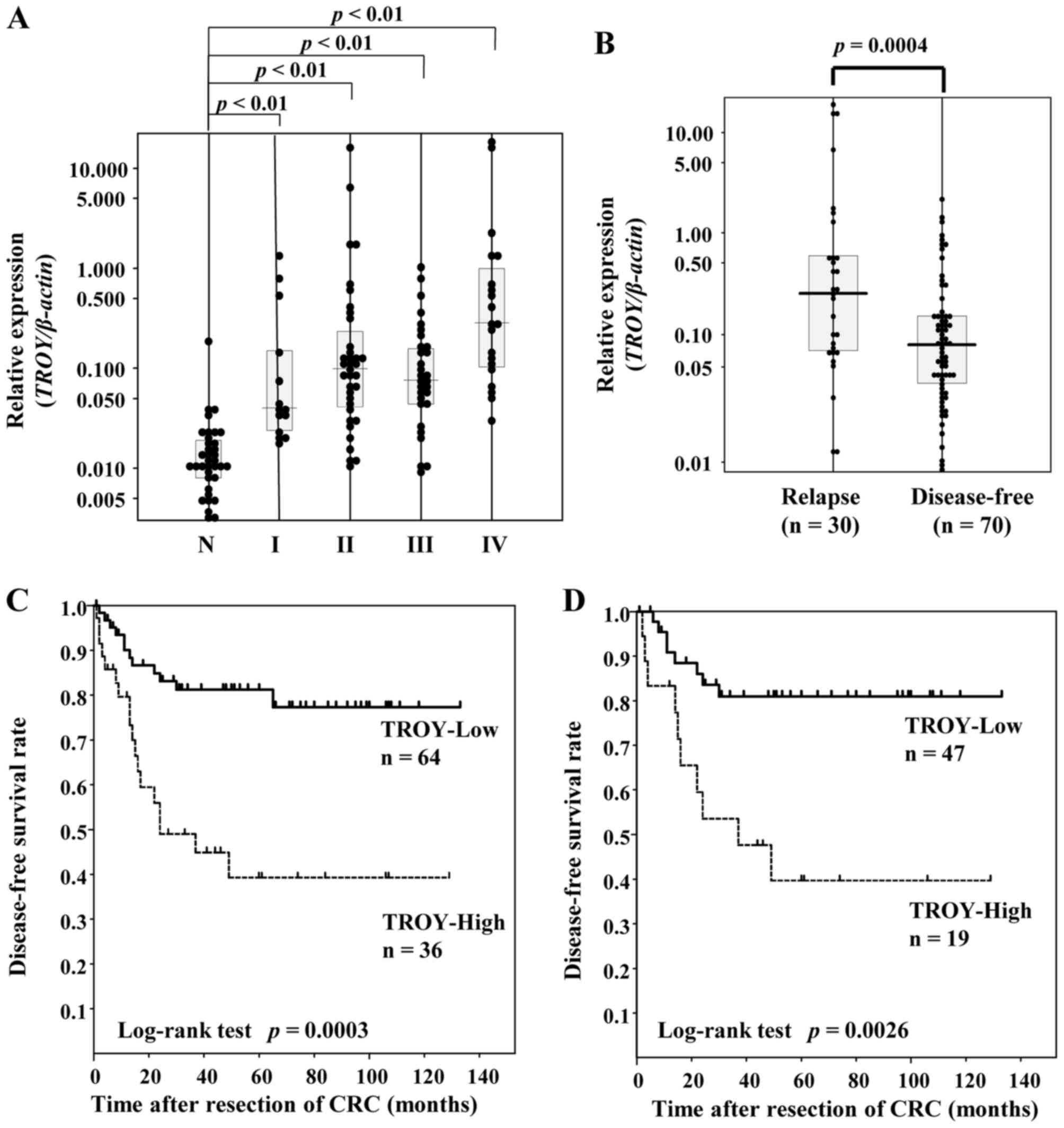
P<0.01 by Tukey multiple comparison test) (Fig. 2A). TROY mRNA expression levels
were significantly higher in the CRC tissues of each stage than
those in the normal-appearing mucosa tissues (P<0.001 by one-way
ANOVA; both P<0.01 by Tukey multiple comparison test) (Fig. 3A).
Prognostic significance of LGR5
LGR5 expression levels were slightly higher
in the relapse group than in the disease-free group (P=0.058 by
Student's t-test) (Fig. 2B). Receiver
operator characteristic (ROC) curves and sensitivity and
specificity curves were plotted using LGR5 mRNA expression values
for differentiating between the disease-free condition and relapse.
As the crossover of the sensitivity and specificity curves was
0.739, we divided the CRC patients into 2 groups on this basis: the
LGR5-high group (≥0.739) and the LGR5-low (<0.739)
group. Univariate analysis showed CRC patients in the
LGR5-low group tended to have improved DFS as compared with
those in the LGR5-high group (P=0.055 by log-rank test)
(Fig. 2C). In contrast, there was no
association between the LGR5 expression level and overall
survival status (P=0.37 by Student's t-test) (data not shown).
TROY as a prognostic biomarker of
CRC
There was a significant difference in the expression
level of TROY between the disease-free and recurrence groups
(P=0.0004 by Student's t-test) (Fig.
3B). ROC analysis revealed the area under the ROC curve to be
0.694, and an optimal cut-off point to discriminate between the
disease-free and recurrence groups was 0.15 according to the
crossover of the sensitivity and specificity curves, resulting in a
sensitivity of 60.0% and a specificity of 77.1%. Univariate
survival analysis showed patients with high TROY expression
(n=36) had a significantly shorter duration of DFS than those with
low TROY expression (n=64) (P=0.0003 by log-rank test)
(Fig. 3C), and this association was
also observed when patients were limited to stage II and III CRC
(P=0.0026 by log-rank test) (Fig.
3D). Multivariate analysis identified stage and TROY
mRNA level as the independent predictive factors of DFS (Table II). In contrast, there was no
association between TROY mRNA level and overall survival
status (P=0.14 by Student's t-test) (data not shown).
| Table II.Results of Cox proportional hazards
regression analysis of risk factors for recurrence in patients with
all stages colorectal cancer (n=100). |
Table II.
Results of Cox proportional hazards
regression analysis of risk factors for recurrence in patients with
all stages colorectal cancer (n=100).
| Variable | P-value | HR | 95% CI |
|---|
| Sexa | 0.6378 | 0.837 | 0.399–1.757 |
| Age | 0.5711 | 1.010 | 0.976–1.046 |
| pStage | 0.0004 | 2.288 | 1.444–3.624 |
| LGR5 mRNA
level | 0.6209 | 0.856 | 0.463–1.583 |
| TROY mRNA
level | 0.0039 | 2.364 | 1.317–4.241 |
Discussion
In the present study, LGR5 mRNA expression
levels were significantly higher in the CRC tissues of stages II–IV
than those in the normal-appearing mucosa tissues, and CRC patients
with higher LGR5 expression tended to have unfavorable
outcomes compared with those with lower LGR5 expression.
LGR5 overexpression has been reported in several cancers
including hepatocellular carcinoma, ovarian cancer, cervical
cancer, and basal cell carcinoma (20–23).
Regarding CRC, many study groups reported that LGR5 is
overexpressed in CRC tissues and is associated with unfavorable
outcome in CRC patients (24–27). In the present study, although
univariate analysis showed overexpression of LGR5 to be a
possible biomarker of unfavorable outcome of CRC, its clinical
usefulness in predicting relapse of CRC was not as expected. Thus,
we continued searching for other biomarkers including
TROY.
In the present study, the overexpression of
TROY was found to be an independent prognostic marker of DFS
in all stages of CRC and even when limited only to stage II and III
CRC. To date, this is, to our knowledge, the first report in the
world of TROY as an independent prognostic marker of DFS of
CRC. TROY has unique aspects in the Wnt signaling pathway.
TROY has the potential of being a negative feedback
mechanism in the canonical Wnt pathway. Because TROY is one
of the β-catenin/TCF4 target genes, TROY expression is
increased in a Wnt-signaling-dependent manner; however, TROY
also reduces Wnt signaling by destabilizing LRP6 (28). Thus, we speculate that the
overexpression of TROY observed in the present study may
reflect a failure of the negative feedback of TROY in Wnt
signaling or a protective effect of TROY to suppress Wnt signaling.
The function of TROY in CRC is poorly understood. One
research group reported that TROY is significantly up-regulated in
neoplastic tissues from mice during intestinal tumorigenesis and is
produced specifically by fast-cycling intestinal stem cells
(13). Another research group
suggested that TROY can contribute to the initiation or progression
of colorectal tumors with deregulated β-catenin activity (17). Regarding the prognostic significance
of TROY, one research group reported no increase in TROY
mRNA in CRC specimens in a small sample of patients (n=20)
(13). In contrast, another group
reported an increase in TROY mRNA expression in 4 of 8 CRC
tissues but did not investigate its prognostic significance
(17). Because the number of samples
analyzed in both reports was small, they were insufficient to
evaluate the prognostic significance of the expression level of
TROY. Further studies are required to confirm the association of
the higher expression of TROY with outcome in patients with CRC. In
cancers other than CRC, higher expression of TROY correlates with
increasing glial tumor grade (15),
glioblastoma cell invasion, and unfavorable outcome of glioblastoma
(16,29). These reports may support our finding
of TROY as a possible prognostic marker in CRC. However, we realize
that limitations exist in our study: We did not measure protein
levels of TROY and did not investigate its localization because of
an insufficient amount of tissue samples. Thus, further studies
incorporating investigation of these issues are required to prove
TROY as a true prognostic factor in CRC.
In conclusion, TROY may be a promising and
better biomarker of predictive relapse of CRC than LGR5. To
support our findings, confirmatory studies using independent data
sets are needed. In addition, to improve the outcome of patients
with CRC, further studies are required to investigate whether the
evaluation of TROY expression level can be useful in
determining whether to introduce adjuvant chemotherapy especially
in patients with stage II and III CRC.
Acknowledgements
The authors would like to thank Reo Kawano (Center
for Clinical Research, Yamaguchi University Hospital) for his help
with the statistical analysis. The present work was supported by
JSPS KAKENHI Grant Numbers JP25931034, JP26893169 and JP16K19195
(to M.N.).
Glossary
Abbreviations
Abbreviations:
|
CRC
|
colorectal cancer
|
|
DFS
|
disease-free survival
|
|
LGR5
|
leucine-rich-repeat-containing
G-protein-coupled receptor 5
|
|
ROC
|
receiver operating characteristic
|
|
TROY
|
TNF receptor superfamily member 19
(TNFRSF19, TAJ)
|
References
|
1
|
GLOBOCAN 2012. 11–June. 2017http://globocan.iarc.fr/
|
|
2
|
CANCERSTATISTICSINJAPAN'15. 11–June.
2017http://ganjoho.jp/en/professional/statistics/brochure/2015_en.html
|
|
3
|
Böckelman C, Engelmann BE, Kaprio T,
Hansen TF and Glimelius B: Risk of recurrence in patients with
colon cancer stage II and III: A systematic review and
meta-analysis of recent literature. Acta Oncol. 54:5–16. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Verhoeff SR, van Erning FN, Lemmens VE, de
Wilt JH and Pruijt JF: Adjuvant chemotherapy is not associated with
improved survival for all high-risk factors in stage II colon
cancer. Int J Cancer. 139:187–193. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Reya T and Clevers H: Wnt signalling in
stem cells and cancer. Nature. 434:843–850. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
MacDonald BT, Tamai K and He X:
Wnt/beta-catenin signaling: Components, mechanisms, and diseases.
Dev Cell. 17:9–26. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Schneikert J and Behrens J: The canonical
Wnt signalling pathway and its APC partner in colon cancer
development. Gut. 56:417–425. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Barker N, van Es JH, Kuipers J, Kujala P,
van den Born M, Cozijnsen M, Haegebarth A, Korving J, Begthel H,
Peters PJ and Clevers H: Identification of stem cells in small
intestine and colon by marker gene Lgr5. Nature. 449:1003–1007.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Barker N and Clevers H: Leucine-rich
repeat-containing G-protein-coupled receptors as markers of adult
stem cells. Gastroenterology. 138:1681–1696. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hirsch D, Barker N, McNeil N, Hu Y, Camps
J, McKinnon K, Clevers H, Ried T and Gaiser T: LGR5 positivity
defines stem-like cells in colorectal cancer. Carcinogenesis.
35:849–858. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Barker N, Ridgway RA, van Es JH, van de
Wetering M, Begthel H, van den Born M, Danenberg E, Clarke AR,
Sansom OJ and Clevers H: Crypt stem cells as the cells-of-origin of
intestinal cancer. Nature. 457:608–611. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hu S, Tamada K, Ni J, Vincenz C and Chen
L: Characterization of TNFRSF19, a novel member of the tumor
necrosis factor receptor superfamily. Genomics. 62:103–107. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Fafilek B, Krausova M, Vojtechova M,
Pospichalova V, Tumova L, Sloncova E, Huranova M, Stancikova J,
Hlavata A, Svec J, et al: Troy, a tumor necrosis factor receptor
family member, interacts with lgr5 to inhibit wnt signaling in
intestinal stem cells. Gastroenterology. 144:381–391. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Spanjaard RA, Whren KM, Graves C and
Bhawan J: Tumor necrosis factor receptor superfamily member TROY is
a novel melanoma biomarker and potential therapeutic target. Int J
Cancer. 120:1304–1310. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Paulino VM, Yang Z, Kloss J, Ennis MJ,
Armstrong BA, Loftus JC and Tran NL: TROY (TNFRSF19) is
overexpressed in advanced glial tumors and promotes glioblastoma
cell invasion via Pyk2-Rac1 signaling. Mol Cancer Res. 8:1558–1567.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Loftus JC, Dhruv H, Tuncali S, Kloss J,
Yang Z, Schumacher CA, Cao B, Williams BO, Eschbacher JM and Ross
JT: TROY (TNFRSF19) promotes glioblastoma survival signaling and
therapeutic resistance. Mol Cancer Res. 11:865–874. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Schön S, Flierman I, Ofner A, Stahringer
A, Holdt LM, Kolligs FT and Herbst A: β-catenin regulates NF-κB
activity via TNFRSF19 in colorectal cancer cells. Int J Cancer.
135:1800–1811. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Sobin LH, Gospodarowicz MK and Wittekind
C: TNM classification of malignant tumours. 7th. Hoboken
Wiley-Blackwell; pp. 3362009
|
|
19
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Yamamoto Y, Sakamoto M, Fujii G, Tsuiji H,
Kenetaka K, Asaka M and Hirohashi S: Overexpression of orphan
G-protein-coupled receptor, Gpr49, in human hepatocellular
carcinomas with beta-catenin mutations. Hepatology. 37:528–533.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Tanese K, Fukuma M, Yamada T, Mori T,
Yoshikawa T, Watanabe W, Ishiko A, Amagai M, Nishikawa T and
Sakamoto M: G-protein-coupled receptor GPR49 is up-regulated in
basal cell carcinoma and promotes cell proliferation and tumor
formation. Am J Pathol. 173:835–843. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Sun B, Ye X, Li Y and Zhang W: Lgr5 is a
potential prognostic marker in patients with cervical carcinoma.
Int J Clin Exp Pathol. 8:1783–1789. 2015.PubMed/NCBI
|
|
23
|
Sun Y, Jia X and Wu X: High expressions of
Lgr5 and ALDH1 in primary epithelial ovarian cancer correlate with
advanced tumor stage and grade as well as poor prognosis of the
patients. Gynecol Obstet Invest. 20–Jun;2015.(Epub ahead of print).
View Article : Google Scholar
|
|
24
|
Takahashi H, Ishii H, Nishida N, Takemasa
I, Mizushima T, Ikeda M, Yokobori T, Mimori K, Yamamoto H, Sekimoto
M, et al: Significance of Lgr5(+ve) cancer stem cells in the colon
and rectum. Ann Surg Oncol. 18:1166–1174. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wu XS, Xi HQ and Chen L: Lgr5 is a
potential marker of colorectal carcinoma stem cells that correlates
with patient survival. World J Surg Oncol. 10:2442012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Saigusa S, Inoue Y, Tanaka K, Toiyama Y,
Kawamura M, Okugawa Y, Okigami M, Hiro J, Uchida K, Mohri Y and
Kusunoki M: Significant correlation between LKB1 and LGR5 gene
expression and the association with poor recurrence-free survival
in rectal cancer after preoperative chemoradiotherapy. J Cancer Res
Clin Oncol. 139:131–138. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Hsu HC, Liu YS, Tseng KC, Hsu CL, Liang Y,
Yang TS, Chen JS, Tang RP, Chen SJ and Chen HC: Overexpression of
Lgr5 correlates with resistance to 5-FU-based chemotherapy in
colorectal cancer. Int J Colorectal Dis. 28:1535–1546. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Barker N, Tan S and Clevers H: Lgr
proteins in epithelial stem cell biology. Development.
140:2484–2494. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Dhruv HD, Roos A, Tomboc PJ, Tuncali S,
Chavez A, Mathews I, Berens ME, Loftus JC and Tran NL:
Propentofylline inhibits glioblastoma cell invasion and survival by
targeting the TROY signaling pathway. J Neurooncol. 126:397–404.
2016. View Article : Google Scholar : PubMed/NCBI
|