Introduction
Chronic myelomonocytic leukemia (CMML) is a form of
myeloid neoplasm with dysplastic and proliferative features. It is
defined by the presence of persistent peripheral blood (PB)
monocytosis (≥1×109//), when monocytes account for ≥10%
of the White Blood Cell (WBC) count (1). Other disorders, including Philadelphia
(Ph) chromosome, BCR, RhoGEF and GTPase activating
protein/proto-oncogene tyrosine-protein kinase ABL1 (BCR-ABL1)
fusion gene, and rearrangements of platelet derived growth factor
receptor α (PDGFRα), platelet derived growth factor receptor β
(PDGFRβ) and fibroblast growth factor receptor 1 (FGFR1), require
exclusion prior to diagnosis (2). The
French-American-British (FAB) classification (3) and World Health Organization (WHO)
(4) have classified CMML into 2
subtypes (CMML-I and -II), according to leukocyte count and the
proportion of bone marrow (BM) blasts, respectively.
Due to the heterogeneity of the disease, the
clinical course and outcomes of patients with CMML are variable
(5). A number of prognostic studies
have been performed, in which cytogenetic and molecular
abnormalities were indicated to be important prognostic factors.
Cytogenetic abnormalities, including trisomy 8, complex karyotypes,
monosomy 7, del7q, trisomy 21, and -Y, have been identified to have
prognostic value (6). Patients with
trisomy 8, complex karyotypes, monosomy 7 and del7q are classified
as high-risk according to the majority of prognostic models
(7), and exhibit a higher leukemic
transformation rate and shorter overall survival time (6–8). A number
of molecular abnormalities are commonly exhibited by patients with
CMML, including mutations in additional sex combs like
transcriptional regulator 1 (ASXL1), Tet methylcytosine dioxygenase
2 (TET2), serine and arginine rich splicing factor 2 (SRSF2), NRAS
proto-oncogene, GTPase (NRAS), runt related transcription factor 1
(RUNX1), SET binding protein 1 (SETBP1), Cbl proto-oncogene (CBL),
JAK2 and RUNX1 are common, while mutations in RUNX1, NRAS, SETBP1
and ASXL1, are independently associated with inferior overall
survival (OS) time (9).
The present case study describes a high-risk patient
with CMML, who achieved PR for 2 months with decitabine therapy.
However, the patient demonstrated a sudden transformation to AML
and eventually an inferior outcome, indicating that decitabine
treatment as a single agent may not be satisfactory for CMML cases
that have a tendency to transform to AML. This highlights the
requirement to discover novel treatment strategies for CMML.
Case report
In September 2015, a 53-year-old man was admitted in
The First Affiliated Hospital of Lanzhou University (Lanzhou,
China), having bruised easily for ~5 months. PB analysis revealed a
white blood cell count (WBC) of 35.07×109 cells/l, a
monocyte level of 4.46×109 cells/l, a hemoglobin (Hb)
level of 74 g/l and a platelet count of 44.0×109
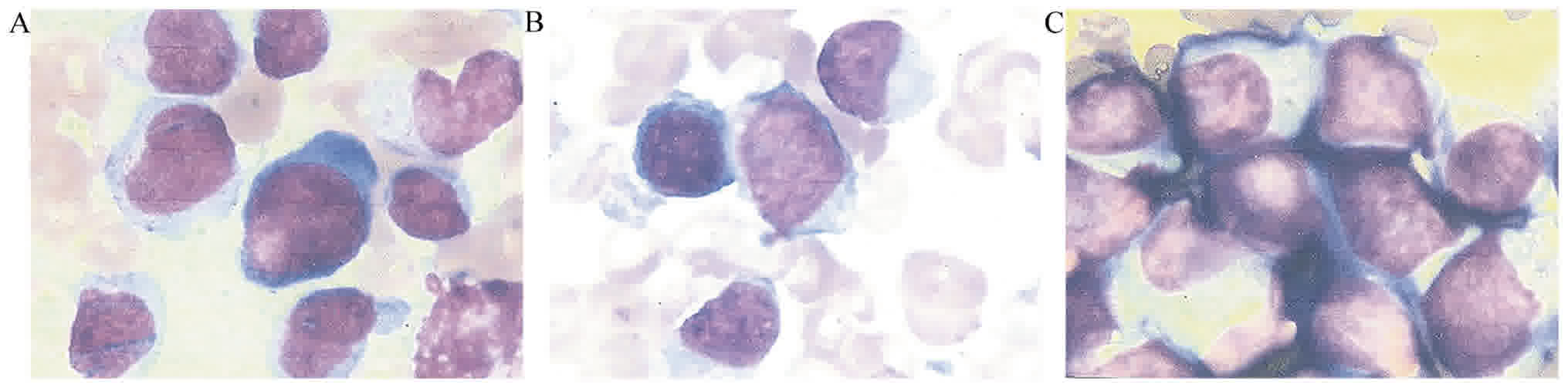
cells/l. A bone marrow aspirate examination using Wright-Giemsa
stain revealed a cell proportion of 6.5% myeloblasts, 2.5%
promyelocyte, 10.5% promonocytes and 20% immature monocytes.
(Fig. 1), resulting in a diagnosis of
CMML according to the 2008 WHO myelodysplastic
(MDS)/myeloproliferative neoplasms classification system (2). Immunophenotyping analysis revealed that
the blasts were positive for cytoplasmic myeloperoxidase antigens
and cluster of differentiation (CD)64, 11c, 13, 11b and 33, and
negative for CD7, 117, 3, 16, 20, 10, 19, 56, 4 and 34, and
cytoplasmic CD79a and CD3 antigens, which were detected on the
surface of the monoblasts by multiparameter flow cytometry. A total
of 2 ml bone marrow was extracted using a heparin anticoagulation
solution (25 IU heparin sodium; BD Biosciences, Franklin Lakes, NJ,
USA) at 15–25°C for 30 min. The concentration of marrow mononuclear
cells specimen was adjusted to 5×109 cells/l, and
fluorescent labeling antibody reagents, FITC, PE, PerCP or APC (all
from BD Biosciences) were added. The solutions were protected from
light and incubated for 15 min. A total of 2 ml Red Blood Cell
Lysis Buffer was added to each sample and incubated for 10 min at
room temperature in darkness. The sampled were then centrifuged at
40 × g for 6 min, and the supernatant was discarded. The remaining
sample was washed twice in PBS, and cells resuspended in PBS for
detection using a FACSCalibur full automatic multicolor analysis
flow cytometer system (BD Biosciences) using FlowJo version 10.2
software (FlowJo LLC, Ashland, OR, USA).
Giemsa (G) banding analysis required preparation by
adding 3 ml 0.25% trypsin (BD Biosciences) solution to 45 ml 0.85%
saline, with a pH of 6.8–7.2, and warmed to 37° using a water bath.
Chromosome specimens were digested in trypsin solution at 37°C for
2–3 min, then swiftly rinsed with 0.85% saline to terminate trypsin
activity. This was followed by Giemsa staining (5 ml; BD
Biosciences) for 15 min at 32°C and then the slides were rinsed
with tap water and air dried. The staining was observed under a low
power light microscope (magnification, ×10) and the metaphase of
mitosis was observed. Then an oil objective (magnification, ×100)
was used to observe Giemsa (G) banding. G banding analysis did not
detect Ph chromosome.
Total RNA was isolated from the bone marrow aspirate
using TRIzol (Thermo Fisher Scientific, Inc., Waltham, MA, USA,
according to the manufactuerer's protocol. Reverse transcription of
was performed using a reverse transcription kit (Takara Bio, Inc.,
Otsu, Japan). The temperature protocol was as follows: 37°C for 15
min, 85°C for 5 sec and kept at 4°C until use. The fluorophore used
for the reverse transcription-quantitative polymerase chain
reaction (RT-qPCR; Takara Biotechnology Co., Ltd., Dalian, China)
was Dalian's Tap enzyme (Takara Bio, Inc.). The target gene primers
were as follows: BCR-ABL, bcr-abl, forward,
5′-AGGGTGCACAGCCGCAACGGC-3′, reverse 5′-GGCTTCACTCAGACCCTGAGG-3′.
The reference gene was β-actin. The reference gene primers were as
follows: β-actin, forward, 5′-GGAGATTACTGCCCTGGCTCCTA-3′ and
reverse, 5′-GACTCATCGTACTCCTGCTTGCTG-3′. The thermocycling
conditions were as follows: 95°C for 30 sec, then 40 cycles at 95°C
for 5 sec and 60°C for 20 sec. The results were expressed as
2−ΔΔCq (10).. The
quantity of BCR-ABL transcript was normalized to the ABL expression
level. The copy number of BCR-ABL fusion gene and the copy number
of ABL were calculated, and the result was expressed as the ratio
of BCR-ABL copy number to ABL copy number. RT-qPCR did not detect
BCR-ABL1 gene fusion for this patient.
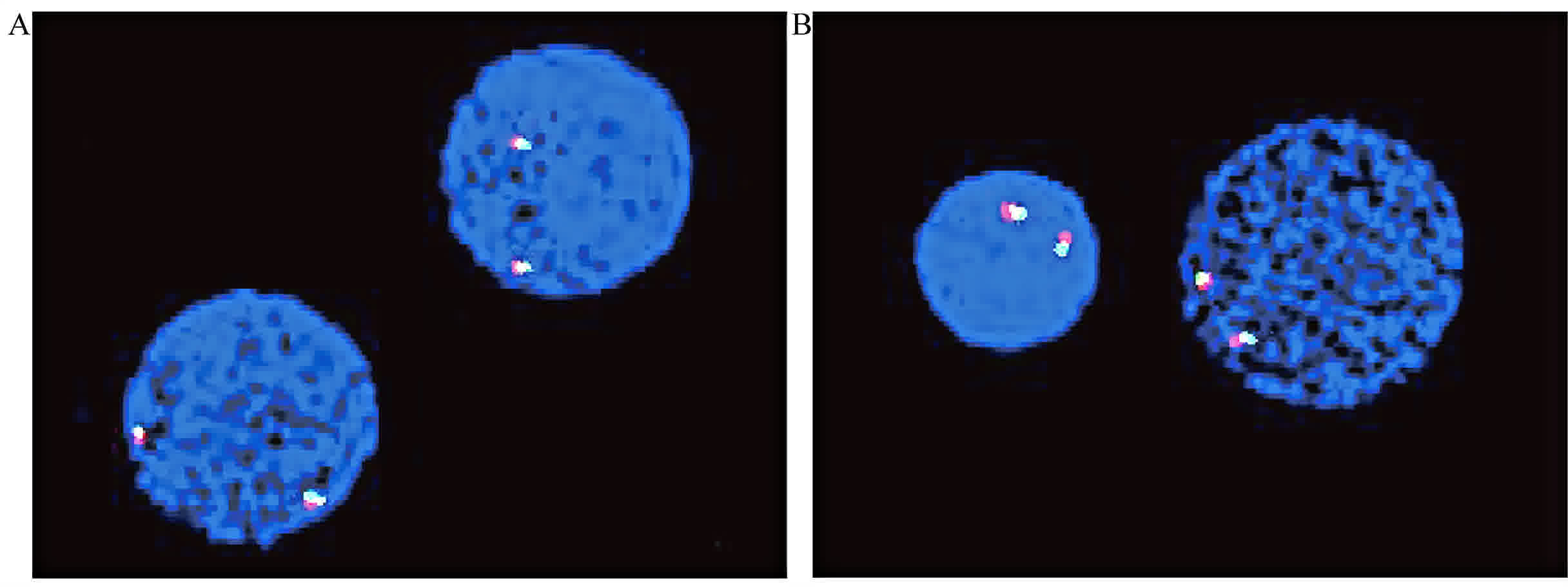
Fluorescence in situ hybridization demonstrated that
PDGFRα, PDGFRβ and FGFR1 were not rearranged (Fig. 2). The method was performed using 4
genes locus specific probes for ASS, PDGFRα, PDGFRβ and FGFR,
localized at 9q34, 4q12, 5q32-33 and 8p12, respectively (all from
Kindstar Global, Hester Clinical Inspection, Beijing, China). Bone
marrow blood (3 ml) was extracted and the sampled centrifuged at
250 × g, room temperaure for 8 min and the supernatant discarded.
Potassium chloride (5 ml) was added and the samples incubated at
37°C for 20 min. The chromosome specimens stored at −20°C, were
then fixed with methanol and glacial acetic acid (3:1) for 30 min
at 37°C. The slide obtained from the previous step were bathed in
2× SSC solution (2× SSC solution configuration method: Nacl 175.5
g, trisodium citrate 88.2 g, add 1,000 ml ddH2O, PH
adjusted to 5.3. Add ddH2O and diluted with 1:9,
adjusted pH to 7.0) at 37°C for 10 min, so as to increase cell
permeability, simulate cell physiological environment and ensure
the stability of the test substances, prior to graded dehydration
in 70, 85 and 100% ethanol at room temperature. Denaturation took
place in 70% formamide and 2× SSC, at 72°C for 3 min. A total of 10
µl probe mixture, with 5 µl probe, 3 µl DNA specimen, 0.5 µl salmon
sperm DNA and 1.5 µl H2O was incubated for 10 min in a
water bath at 72°C, then placed in an iced water bath for 5 min,
and finally a 37°C water bath for 5 min. The specimens were mounted
onto glass slides using RubberCement (Kindstar Global, Beijing,
China) and placed at 37°C overnight for hybridization. Specimens
were washed for 5 min at 72°C in 0.4× SSC and then for 2 min with
0.1% TritonX-100 at room temperature. DAPI (Kindstar Global) was
added to PBS and a 10 µg/ml DAPI solution was prepared, and the
specimens incubated at 37°C for 15 min. Fluorescence hybridization
signals of interphase cells were observed under the excitation of
UV/Texas red/FITC trichromatic filters with an Olympus BX60
fluorescence microscope (Olympus Corporation, Tokyo, Japan). A
total of 400 probe mixture cells were analyzed at one time. Image
acquisition was achieved using an autosomal auto analysis system
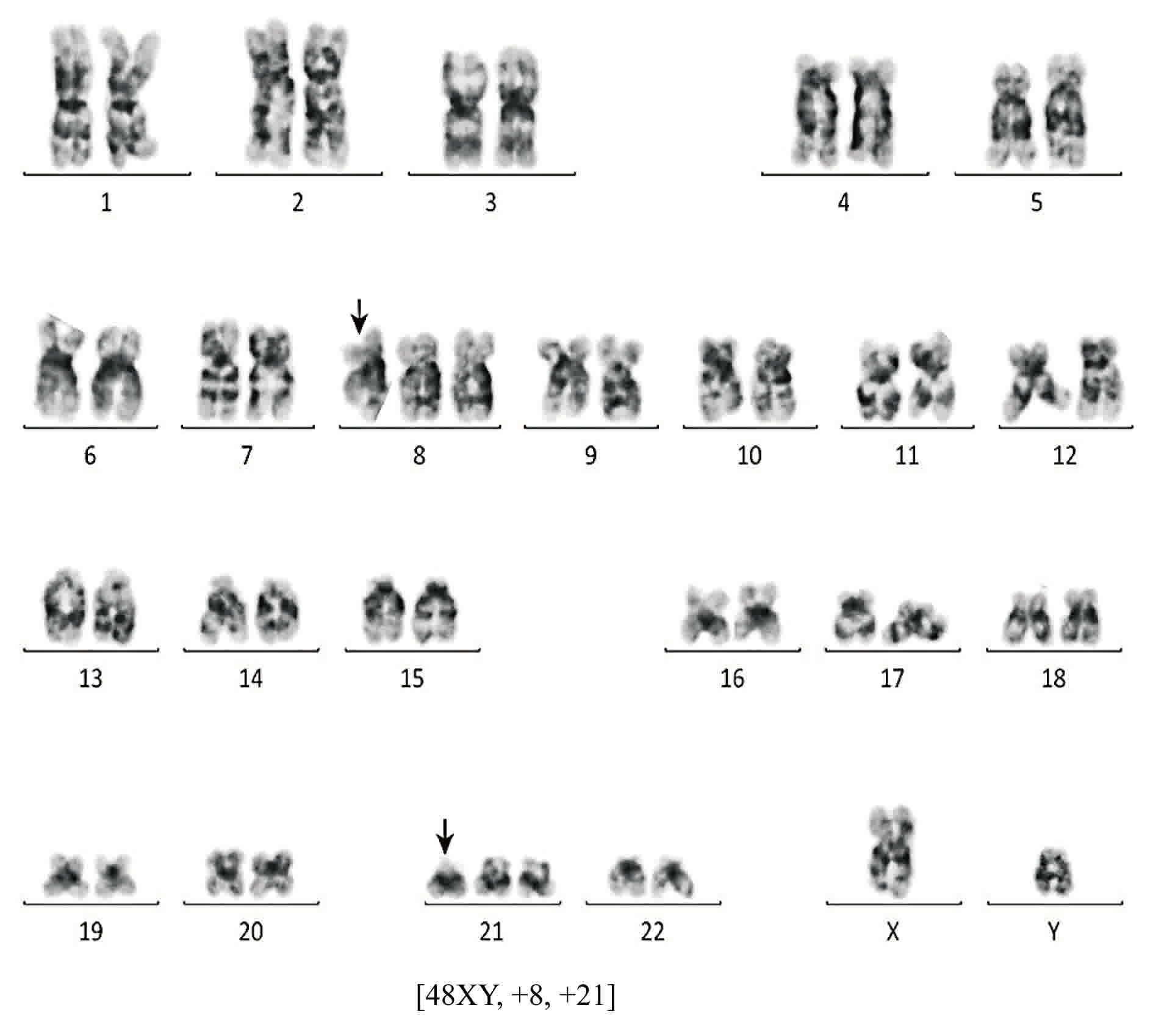
(Kindstar Global). This allowed a CMML diagnosis to be made. In
addition, conventional cytogenetic analysis performed using the G
banding technique revealed a 48, XY, +8 and +21 karyotype in all 20
metaphase cells (Fig. 3).
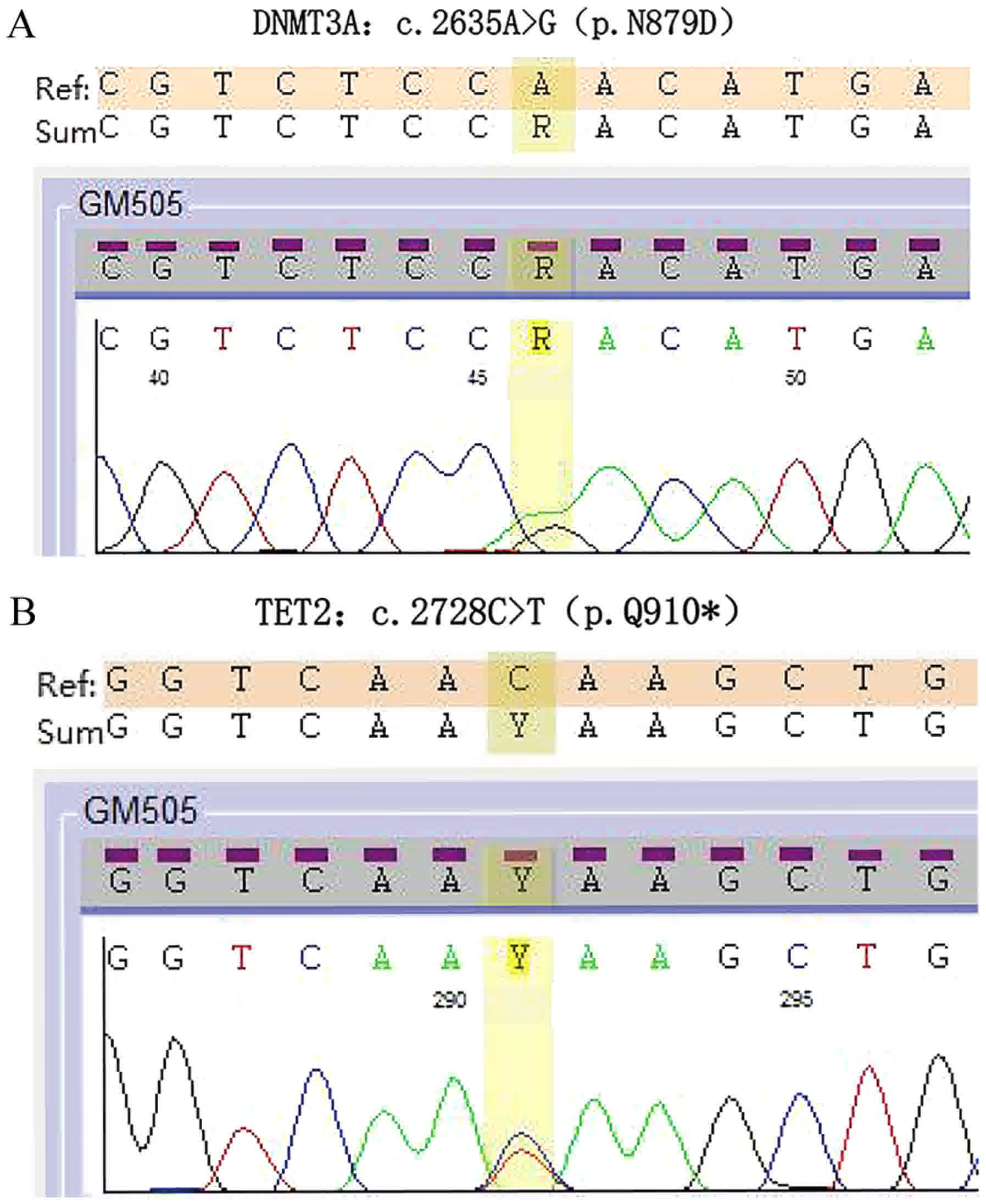
Meanwhile, gene sequencing using a polymerase chain
reaction binding-based sequencing method, performed externally
(Shanghai Di Shuo Becken Ltd Medical Examination, Shanghai, China),
detected a missense mutation in DNMT3A (Fig. 4A) and nonsense mutations in TET2
(Fig. 4B). There was no evidence of
mutations in SF3B1, SRSF2, ASXL1, RUNX1, FLT3-ITD, C-kit/D816V,
NPM1 or CEBPA. According to these cytogenetic abnormalities, the
case was defined as high-risk CMML.
The patient was treated with decitabine,
administered at 25 mg daily for 5 consecutive days every 28 days.
The patient underwent 3 courses of this regimen. The BM response
was examined following each treatment cycle. Following 2 cycles of
therapy, the patient achieved partial remission, classified
according to the modified International Working Group response
criteria in myelodysplastic syndromes (MDS) (11). The level of BM blasts had decreased to
<5% and the percentage reduction was >50%. Furthermore, the
patient's diagnosis was altered from CMML-II to CMML-I according to
the FAB subtype criteria. Following 3 cycles of therapy, the
patient maintained PR and displayed hematologic improvement (HI),
including erythroid and platelet responses (11). The majority of parameters had
improved, including an increase in Hb level from 56–168 g/l and an
increase in platelet level from
2.1×1010-6.2×1010/l. BM aspirate analysis
revealed a proportion of 2.5% myeloblasts and 0% promonocytes
(Fig. 1B).
Subsequent to 3 cycles of decitabine therapy, the
level of lactate dehydrogenase progressively increased from 267 to
11,347 U/l and absolute monocytosis (AMC) was detected (from
0.32×109 to 1.86×109 cells/l), potentially
indicating disease progression. PB examination confirmed a WBC of
13.4×109/l, 81 g Hb/l, 32×109 platelets/l and
11347 U lactate dehydrogenase/l. BM aspirate analysis revealed
73.5% myeloblasts and 59% monoblasts (Fig. 1C). BM biopsy demonstrated a trend
towards AML-M5. A diagnosis of disease transformation to AML-M5 was
made, and fatality of the patient occurred 1 month after AML
transformation, and prior to any AML treatment.
Discussion
CMML is a clonal stem cell disorder, with
characteristics of myeloproliferative and myelodysplastic neoplasms
(1). Due to the heterogeneity of the
disease, it is associated with variable clinical courses and
outcomes, and an inherent tendency to transform to AML. CMML-I has
a 14% chance and CMML-II has a 24% chance of developing into AML
within 2 years, increasing to 18 and 63% after 5 years,
respectively (4). To date, a number
of clinical parameters have been reported to be associated with
poor survival time of patients with CMML, including age, sex,
Eastern Cooperative Oncology Group performance status (12), Hb level, WBC count, number of
circulating immature myeloid cells, proportion of BM blasts,
karyotype and β2-microglobulin/lactate dehydrogenase levels
(13,14). Furthermore, previous reports have
demonstrated that a high proportion of BM blasts, elevated lactate
dehydrogenase, male sex and a low Hb level were independent
prognostic factors (15). Most
recently, cytogenetic status and specific gene mutations have been
identified as important prognostic factors, and have been
incorporated into the CMML risk stratification system (7,16).
In the present case, a 48, XY, +8, +21 karyotype was
detected by conventional cytogenetic analysis. Clonal cytogenetic
abnormalities have been reported in >30% CMML cases (17). Multiple prognostic models have been
defined to stratify CMML patients into different risk categories,
based on the Global MD Anderson Prognostic Scoring system (G-MDAPS)
(8,18), Spanish cytogenetic risk stratification
system (14) and CMML-specific
prognostic scoring system (CPSS) (18,19). These
systems stratify patients based on cytogenetic abnormalities and
are effective in predicting survival and leukemic transformation
(17). Furthermore, certain
prognostic models, including The Groupe Francophone des
Myelodysplasies (GFM) (15) and Mayo
Molecular Model (MMM) (15) integrate
gene mutation into risk assessment, which significantly improves
the risk stratification of CMML. In an international collaborative
study, Elena et al (9)
proposed a specific prognostic score based on 260 CMML patients,
called the CPSS-Mol (9). This score
integrated karyotype with genetic mutation, red blood cell
transfusion dependence, WBC count and percentage of BM blasts. It
stratified CMML patients into 4 different risk groups that had
significantly different median OS times and incidences of leukemic
progression (9). The patient
discussed in the present study exhibited cytogenetic abnormalities
of trisomy 8 and trisomy 21, which are classified as high-risk
factors according to the majority of prognostic models, including
the CPSS-Mol. Such cases are considered to have a high leukemic
transformation rate and shorter OS time.
Molecular abnormalities are identified in >90%
CMML patients (20). Genetic
sequencing identified DNMT3A and TET2 mutations in the patient
discussed in the present study. These genes are involved in
epigenetic regulation and DNA methylation. Mutations in DNMT3A,
located on chromosome 2q23.3, are identified in 2–5% patients with
CMML (21). Considering this low
frequency, its prognostic value has not been investigated. Itzykson
et al (16) reported that
DNMT3A does not impact OS or leukemia-free survival (LFS). In
addition, Jaiswal et al (22)
indicated that DNMT3A is associated with age-associated clonal
hematopoiesis and increased overall mortality. However, a recent
study by Patnaik et al (21)
indicated that DNMT3A mutations are independent prognostic factors
of an inferior OS time. Patients with DNMT3A mutations were
demonstrated to be more likely to exhibit low hemoglobin levels,
high monocyte counts, a high proportion of bone marrow blasts and
abnormal karyotypes. Considering rare DNMT3A mutations have an
independent prognostic impact on survival, the gene may be
integrated into CMML prognostic models.
TET2 is a member of the TET family, and is located
on chromosome 4q24. Mutations in this gene are identified in
>60% CMML patients (15). However,
to the best of our knowledge, it has not been associated with OS
nor LFS, and the prognostic value of TET2 mutations in CMML remains
controversial. Previous research has suggested that TET2 mutations
have an adverse effect in patients with CMML (23,24).
However, other studies have suggested a relatively good prognosis
for patients with CMML patients carrying TET2 mutations. For
example, Patnaik et al (25)
demonstrated that the presence of clonal TET2 mutations in the
absence of clonal ASXL1 mutations has a favorable effect on OS
time. In addition, mutations in TET2 are associated with an
improved response to hypomethylating agents (HMAs) (26). However, the prognostic impact of TET2
mutation remains unclear. Furthermore, although the interaction
between TET2 and ASXL1 has been studied, the association between
TET2 and other genes, including DNMT3A, remain unknown. Therefore,
a more comprehensive genomic analysis is required in to study the
interaction between TET2 and DNMT3A, and to confirm the exact role
of these genes.
Due to the heterogeneity of CMML, there exists no
standard therapy. Available treatments include chemotherapy,
allogeneic stem cell transplantation (HCT) and HMAs (decitabine and
azacitidine) (15). Chemotherapies,
including etoposide, cytarabine, topotecan and lonafarnib, have
been reported to have poor response rates and severe toxicities
(15). Although HCT currently remains
the only potentially curative therapeutic strategy for CMML, in the
case of old age, poor cytogenetics or high-risk classification,
this treatment is not effective (27–29). HMAs,
which are approved by the Food and Drug Administration (FDA),
remain the safest and most efficient mode of therapy, and the main
mode of treatment for high risk CMML (30). Compared with HCT, HMAs are often
considered as a first line treatment for patients with CMML-II a
high proportion of BM blasts (31).
Kantarjian et al (32)
demonstrated that decitabine treatment was associated with a
survival advantage in patients with high-risk MDS compared with
intensive chemotherapy. Although these studied (30,31)
confirmed the therapeutic effect of HMA in CMML. However the
overall response rate (ORR) and complete remission rate (CR) are
low, previous studies have indicated that the ORR of patients to
HMAs is ~30–40%, with CR only 15% (15,33). In
addition, the responses may not be sustained, and can lead to poor
OS time and transformation to high risk phenotypes. However, one
study described a patient with AML, transformed from CMML, who
reached complete remission with decitabine combined with a low dose
of cytarabine, aclarubicin and granulocyte colony-stimulating
factor (34). Although the results
did not have statistical significance, they may offer insight into
potential therapeutic strategies for AML, transformed from
CMML.
The case described in the present study is
relatively rarely observed. However, previous research has
demonstrated that loss of response to decitabine in patients who
had reached remission from CMML is not uncommonly. For example,
Padron et al (35) discussed
that while the use of decitabine in CMML is FDA-approved, but HMA
cannot offer meaningful potential to change the natural history of
the disease. In addition, The effectiveness of HMAs is temporary
and survival after loss of response is dismal (15). Patnaik et al (15) demonstrated that the overall response
rates of HMA are about 30–40%, with complete remission rates of
15%. However, the responses are generally not sustained, and the OS
time, subsequent to loss of response, is often poor. The results
inferred from the present study corroborate these conclusions.
Thus, investigation into novel strategies to treat such patients
are urgently required.
A number of targeted therapy drugs are currently in
preclinical studies, including anti-granulocyte-macrophage colony
stimulating factor (GM-CSF) antibodies (36) and JAK inhibitors (35,37). Early
studies have demonstrated that GM-CSF hypersensitivity is a
hallmark of juvenile myelomonocytic leukemia (JMML) (38). A previous study demonstrated that the
majority of CMML cases exhibit GM-CSF hypersensitivity, indicating
a potential therapeutic target in reducing CMML cell proliferation
via GM-CSF neutralization with targeted anti-GM-CSF monoclonal
antibodies or JAK inhibitors (36).
Padron et al (36)
demonstrated that GM-CSF-dependent phosphorylated-signal transducer
and activator of transcription sensitivity has therapeutic
potential in CMML. A phase I trial of ruxolitinib, JAK1/2
inhibitor, conducted by Padron et al (35), identified that ruxolitinib is as safe
to administer as pacritinib and momelotinib, with good tolerance
and minimal toxicity. In addition, the drugs demonstrated a broad
range of activity in hematologic, spleen and symptom response, and
correlative analysis highlighted the ruxolitinib-associated
cytokine depletion in CMML (35). In
addition, a previous study identified that treatment with JAK
inhibitors may be downregulated in several genes, including the
inflammatory response in myeloproliferative neoplasms (39).
However, the current treatment regime for CMML, and
the available therapy for AML transformed from CMML is limited.
Based on its aforementioned success, decitabine requires further
investigation to be used in combination therapies for CMML.
Considering decitabine can temporarily improve CMML and that HCT
remains the only potentially curative therapeutic strategy, we
suggest that timely hematopoietic stem cell transplantation is
necessary. Novel targeted therapies, including JAK inhibitors and
targeted anti-GM-CSF monoclonal antibodies, are being developed.
These are promising for use in patients with high-risk CMML, which
has a tendency to transform to AML.
Conclusion
In the patient presented in the present study, the
trajectory of a sudden transformation from CMML, with a high risk
of molecular and cytogenetic abnormalities, into AML was observed
during decitabine treatment. Although the patient achieved partial
remission, an aggressive clinical course and inferior outcome
followed, indicating that the identified molecular and cytogenetic
abnormalities may have accelerated the course of disease and
resulted in its rapid progression. Thus, decitabine as a single
agent was unable to produce satisfactory results in high-risk CMML,
and novel targeted treatment strategies, are urgently required.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The analyzed data sets generated during the study
are available from the corresponding author, on reasonable
request.
Author contributions
HL contributed to the conception of the study, and
was a major contributor in writing the manuscript. JC designed the
study and conducted the analysis. LZ helped perform the analysis
and discussions. QX, MMX and SLZ were responsible for data
acquisition. BL interpreted the results. The final version of the
manuscript was read and approved by all authors.
Ethics approval and consent to
participate
The patient provided informed consent for
participation in the present study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Arber DA, Orazi A, Hasserjian R, Thiele J,
Borowitz MJ, Le Beau MM, Bloomfield CD, Cazzola M and Vardiman JW:
The 2016 revision to the World Health Organization classification
of myeloid neoplasms and acute leukemia. Blood. 127:2391–2405.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Vardiman JW, Thiele J, Arber DA, Brunning
RD, Borowitz MJ, Porwit A, Harris NL, Le Beau MM,
Hellström-Lindberg E, Tefferi A and Bloomfield CD: The 2008
revision of the World Health Organization (WHO) classification of
myeloid neoplasms and acute leukemia: Rationale and important
changes. Blood. 114:937–951. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Bennett JM, Catovsky D, Daniel MT,
Flandrin G, Galton DA, Gralnick H, Sultan C and Cox C: The chronic
myeloid leukaemias: Guidelines for distinguishing chronic
granulocytic, atypical chronic myeloid, and chronic myelomonocytic
leukaemia. Proposals by the French-American-British cooperative
leukaemia group. Br J Haematol. 87:746–754. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Germing U, Strupp C, Knipp S, Kuendgen A,
Giagounidis A, Hildebrandt B, Aul C, Haas R, Gattermann N and
Bennett JM: Chronic myelomonocytic leukemia in the light of the WHO
proposals. Haematologica. 92:974–977. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zandberg DP, Huang TY, Ke X, Baer MR, Gore
SD, Smith SW and Davidoff AJ: Treatment and outcomes for chronic
myelomonocytic leukemia compared to myelodysplastic syndromes in
older adults. Haematologica. 98:584–590. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wassie EA, Itzykson R, Lasho TL, Kosmider
O, Finke CM, Hanson CA, Ketterling RP, Solary E, Tefferi A and
Patnaik MM: Molecular and prognostic correlates of cytogenetic
abnormalities in chronic myelomonocytic leukemia: A Mayo
clinic-french consortium study. Am J Hematol. 89:1111–1115. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Patnaik MM and Tefferi A: Cytogenetic and
molecular abnormalities in chronic myelomonocytic leukemia. Blood
Cancer J. 6:e3932016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Benton CB, Nazha A, Pemmaraju N and
Garcia-Manero G: Chronic myelomonocytic leukemia: Forefront of the
field in 2015. Crit Rev Oncol Hematol. 95:222–242. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Elena C, Galli A, Such E, Meggendorfer M,
Germing U, Rizzo E, Cervera J, Molteni E, Fasan A, Schuler E, et
al: Integrating clinical features and genetic lesions in the risk
assessment of patients with chronic myelomonocytic leukemia. Blood.
128:1408–1417. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cheson BD, Greenberg PL, Bennett JM,
Lowenberg B, Wijermans PW, Nimer SD, Pinto A, Beran M, de Witte TM,
Stone RM, et al: Clinical application and proposal for modification
of the International Working Group (IWG) response criteria in
myelodysplasia. Blood. 108:419–425. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bennett JM, Andersen JW and Cassileth PA:
Long term survival in acute myeloid leukemia: The Eastern
Cooperative Oncology Group (ECOG) experience. Leuk Res. 15:223–227.
1991. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Patnaik MM, Wassie EA, Lasho TL, Hanson
CA, Ketterling R and Tefferi A: Blast transformation in chronic
myelomonocytic leukemia: Risk factors, genetic features, survival,
and treatment outcome. Am J Hematol. 90:411–416. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Tang G, Fu B, Hu S, Lu X, Tang Z, Li S,
Jabbar K, Khoury JD, Medeiros LJ and Wang SA: Prognostic impact of
acquisition of cytogenetic abnormalities during the course of
chronic myelomonocytic leukemia. Am J Hematol. 90:882–887. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Patnaik MM and Tefferi A: Chronic
myelomonocytic leukemia: 2016 update on diagnosis, risk
stratification, and management. Am J Hematol. 91:631–642. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Itzykson R, Kosmider O, Renneville A,
Gelsi-Boyer V, Meggendorfer M, Morabito M, Berthon C, Adès L,
Fenaux P, Beyne-Rauzy O, Vey N, et al: Prognostic score including
gene mutations in chronic myelomonocytic leukemia. J Clin Oncol.
31:2428–2436. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tang G, Zhang L, Fu B, Hu J, Lu X, Hu S,
Patel A, Goswami M, Khoury JD, Garcia-Manero G, et al: Cytogenetic
risk stratification of 417 patients with chronic myelomonocytic
leukemia from a single institution. Am J Hematol. 89:813–818. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Calvo X, Nomdedeu M, Santacruz R, Martinez
N, Costa D, Pereira A, Estrada N, Xicoy B, Esteve J and Nomdedeu B:
Comparison of three prognostic scoring systems in a series of 146
cases of chronic myelomonocytic leukemia (CMML): MD Anderson
prognostic score (MDAPS), CMML-specific prognostic scoring system
(CPSS) and Mayo prognostic model. A detailed review of prognostic
factors in CMML. Leuk Res: S0145-2126(15)30324-6. 2015. View Article : Google Scholar
|
|
19
|
Such E, Cervera J, Costa D, Solé F,
Vallespí T, Luño E, Collado R, Calasanz MJ, Hernández-Rivas JM,
Cigudosa JC, et al: Cytogenetic risk stratification in chronic
myelomonocytic leukemia. Haematologica. 96:375–383. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Patnaik MM, Itzykson R, Lasho TL, Kosmider
O, Finke CM, Hanson CA, Knudson RA, Ketterling RP, Tefferi A and
Solary E: ASXL1 and SETBP1 mutations and their prognostic
contribution in chronic myelomonocytic leukemia: A two-center study
of 466 patients. Leukemia. 28:2206–2212. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Patnaik MM, Barraco D, Lasho TL, Finke CM,
Hanson CA, Ketterling RP, Gangat N and Tefferi A: DNMT3A mutations
are associated with inferior overall and leukemia-free survival in
chronic myelomonocytic leukemia. Am J Hematol. 92:56–61. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Jaiswal S, Fontanillas P, Flannick J,
Manning A, Grauman PV, Mar BG, Lindsley RC, Mermel CH, Burtt N,
Chavez A, et al: Age-related clonal hematopoiesis associated with
adverse outcomes. N Engl J Med. 371:2488–2498. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Jankowska AM, Makishima H, Tiu RV, Szpurka
H, Huang Y, Traina F, Visconte V, Sugimoto Y, Prince C, O'Keefe C,
et al: Mutational spectrum analysis of chronic myelomonocytic
leukemia includes genes associated with epigenetic regulation: UTX,
EZH2, and DNMT3A. Blood. 118:3932–3941. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kosmider O, Gelsi-Boyer V, Ciudad M,
Racoeur C, Jooste V, Vey N, Quesnel B, Fenaux P, Bastie JN,
Beyne-Rauzy O, et al: TET2 gene mutation is a frequent and adverse
event in chronic myelomonocytic leukemia. Haematologica.
94:1676–1681. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Patnaik MM, Lasho TL, Vijayvargiya P,
Finke CM, Hanson CA, Ketterling RP, Gangat N and Tefferi A:
Prognostic interaction between ASXL1 and TET2 mutations in chronic
myelomonocytic leukemia. Blood Cancer J. 6:e3852016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Bejar R, Lord A, Stevenson K, Bar-Natan M,
Pérez-Ladaga A, Zaneveld J, Wang H, Caughey B, Stojanov P, Getz G,
et al: TET2 mutations predict response to hypomethylating agents in
myelodysplastic syndrome patients. Blood. 124:2705–2712. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Eissa H, Gooley TA, Sorror ML, Nguyen F,
Scott BL, Doney K, Loeb KR, Martin PJ, Pagel JM, Radich JP, et al:
Allogeneic hematopoietic cell transplantation for chronic
myelomonocytic leukemia: Relapse-free survival is determined by
karyotype and comorbidities. Biol Blood Marrow Transplant.
17:908–915. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Aribi A, Borthakur G, Ravandi F, Shan J,
Davisson J, Cortes J and Kantarjian H: Activity of decitabine, a
hypomethylating agent, in chronic myelomonocytic leukemia. Cancer.
109:713–717. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Courville EL, Wu Y, Kourda J, Roth CG,
Brockmann J, Muzikansky A, Fathi AT, de Leval L, Orazi A and
Hasserjian RP: Clinicopathologic analysis of acute myeloid leukemia
arising from chronic myelomonocytic leukemia. Mod Pathol.
26:751–761. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Wijermans PW, Rüter B, Baer MR, Slack JL,
Saba HI and Lübbert M: Efficacy of decitabine in the treatment of
patients with chronic myelomonocytic leukemia (CMML). Leuk Res.
32:587–591. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Damaj G, Duhamel A, Robin M, Beguin Y,
Michallet M, Mohty M, Vigouroux S, Bories P, Garnier A, El Cheikh
J, et al: Impact of azacitidine before allogeneic stem-cell
transplantation for myelodysplastic syndromes: A study by the
Société Française de Greffe de Moelle et de Thérapie-Cellulaire and
the Groupe-Francophone des Myélodysplasies. J Clin Oncol.
30:4533–4540. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Kantarjian HM, O'Brien S, Huang X,
Garcia-Manero G, Ravandi F, Cortes J, Shan J, Davisson J,
Bueso-Ramos CE and Issa JP: Survival advantage with decitabine
versus intensive chemotherapy in patients with higher risk
myelodysplastic syndrome: Comparison with historical experience.
Cancer. 109:1133–1137. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Duchmann M, Braun T, Micol JB, Platzbecker
U, Park S, Pilorge S, Beyne-Rauzy O, Vey N, Sébert M, Gruson B, et
al: Validation of response assessment according to international
consortium for MDS/MPN criteria in chronic myelomonocytic leukemia
treated with hypomethylating agents. Blood Cancer J. 7:e5622017.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Deng Q, Li JY, Liu PJ and Zhao MF:
Successful management of acute myeloid leukemia transformed from
chronic myelomonocytic leukemia in the elderly by a combination
regimen of decitabine and cytarabine, aclarubicin and granulocyte
colony-stimulating factor: A case report. Oncol Lett. 9:1217–1220.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Padron E, Dezern A, Andrade-Campos M,
Vaddi K, Scherle P, Zhang Q, Ma Y, Balasis ME, Tinsley S, Ramadan
H, et al: A multi-institution phase I trial of ruxolitinib in
patients with chronic myelomonocytic leukemia (CMML). Clin Cancer
Res. 22:3746–3754. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Padron E, Painter JS, Kunigal S, Mailloux
AW, McGraw K, McDaniel JM, Kim E, Bebbington C, Baer M, Yarranton
G, et al: GM-CSF-dependent pSTAT5 sensitivity is a feature with
therapeutic potential in chronic myelomonocytic leukemia. Blood.
121:5068–5077. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Komrokji RS, Seymour JF, Roberts AW,
Wadleigh M, To LB, Scherber R, Turba E, Dorr A, Zhu J, Wang L, et
al: Results of a phase 2 study of pacritinib (SB1518), a
JAK2/JAK2(V617F) inhibitor, in patients with myelofibrosis. Blood.
125:2649–2655. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Emanuel PD, Bates LJ, Castleberry RP,
Gualtieri RJ and Zuckerman KS: Selective hypersensitivity to
granulocyte-macrophage colony-stimulating factor by juvenile
chronic myeloid leukemia hematopoietic progenitors. Blood.
77:925–929. 1991.PubMed/NCBI
|
|
39
|
Savona MR, Malcovati L, Komrokji R, Tiu
RV, Mughal TI, Orazi A, Kiladjian JJ, Padron E, Solary E, Tibes R,
et al: An international consortium proposal of uniform response
criteria for myelodysplastic/myeloproliferative neoplasms (MDS/MPN)
in adults. Blood. 125:1857–1865. 2015. View Article : Google Scholar : PubMed/NCBI
|