Introduction
Thyroid cancer is the most frequent thyroid
malignancy, accounting for 90% of all types of endocrine malignant
cancer, and its incidence has increased markedly worldwide within
the last few decades (1).
Differentiated thyroid cancer (DTC) is the most common subtype and
has a relatively good prognosis, with 10-year survival rates of
92–98% (2). Unlike the majority of
malignancies, cervical lymph node metastasis (CLNM) is identified
in 53% patients with DTC at initial surgery (3) and may be present even when the primary
tumor is contained within the thyroid (4). CLNM is considered a risk factor for poor
clinical outcome (5). Increased
mortality rates and decreased survival have been demonstrated among
patients with DTC with lymph node metastasis (6).
Total or subtotal thyroidectomy followed by
radioiodine-131 (131I) therapy and lifelong thyroid
hormone suppressive therapy has been accepted as essential
management for DTC (7). The first
sufficient dose of 131I administration following
thyroidectomy to eradicate the remnant normal thyroid tissue is
termed ‘remnant ablation’ (8). The
goal of remnant ablation is to achieve an undetectable serum
thyroglobulin (Tg) level, which serves as a tumor marker to
facilitate follow-up of biochemical analysis, to eradicate any
neoplastic foci to decrease the risk of recurrence and to detect
any recurrence by 131I scanning (9). Total thyroidectomy, together with
central compartment dissection was recommended for patients with
DTC (10), and if the pathological
results verified the presence of lymph node metastasis, the first
follow-up whole-body iodine scan (WBIS) was performed 6 months
subsequent to the thyroidectomy to confirm the presence or absence
of any CLNM. The patients exhibiting CLNM were then scheduled for a
second ablative dose of 131I (11).
Although131I has been used for over 6
decades, the majority of previously published studies focused on a
single optimal dose of remnant ablation (12). No data in the literature concentrated
on the effect of repetitive 131I administration in the
treatment of DTC with CLNM. The aim of the present study was to
evaluate whether 131I administration has an effect on
the final outcome of patients with DTC with CLNM and to analyze the
associated factors responsible for the clinical outcomes.
Materials and methods
Patients
A total of 562 patients with DTC who received
131I administration following subtotal or total
thyroidectomy were recruited from the Department of Endocrinology,
Qilu Hospital of Shandong University (Shandong, China), from
January 2012 to April 2016. All patients were classified according
to the American Joint Committee on Cancer/Union for International
Cancer Control 2010 risk stratification system (13), and the American Thyroid Association
staging system was designed to assess the risk of recurrence in DTC
(14). All patients had undergone
thyroidectomy, together with neck lymphadenectomy and without
131I treatment prior to enrolment. Histopathology
revealed the diagnosis of papillary or follicular thyroid carcinoma
with known positive CLNM at the time of primary surgery. The
tissues were fixed in 10% neutral buffered formalin (Sakura Finetek
USA, Inc., Torrance, CA, USA) for 20 h, overnight, embedded in
paraffin at 56°C and sectioned at 4 µm for hematoxylin (cat no.
C0107; Biyuntian Biotech Co., Ltd., Shanghai, China.) and eosin
(cat no. C0109; Biyuntian Biotech Co., Ltd.) staining (H&E
staining). Tissue sections were treated with hematoxylin stock
solution (no dilution) for 30 min at room temperature, washed with
double distilled water and followed immediately immersed in eosin
stock solution (no dilution) for 30 min. Images of H&E-stained
sections were captured using a ×20 objective magnification attached
to a Olympus DP71 digital camera Olympus microscope equipped with a
Olympus DP71 digital camera (Olympus Life Science Imaging Systems
Inc., Markham, ON, Canada). The diagnosis was performed by three
veterinary pathologists. Pregnant woman and patients with distant
metastases, white blood cell counts <3.0×109 cells/l
(normal range, 4.0×109-10.0×109 cells/l),
severe hepatic and renal failure, poor wound healing and a recent
history of iodine contamination were excluded. The Medical Ethical
Committee of Qilu Hospital of Shandong University approved the
present study. Due to the retrospective nature of the study,
written informed consent was not available from all
participants.
Preoperative preparation
Iodine scrubbing and scanning with iodine contrast
materials were prohibited for 1 month. All patients were required
to discontinue levothyroxine sodium tablets for at least one month
following surgery, until the serum thyrotropin (TSH) concentration
was >30 mIU/l. Patients were maintained on a low iodine diet for
2 weeks prior to the scan. Serum TSH, Tg, anti-thyroglobulin
(Anti-Tg), routine blood examination, hepatic and renal function,
electrocardiogram, neck ultrasound and chest X-ray were measured
~2–3 days prior to administration of the diagnostic dose. Patients
were hospitalized in the special ward of the Department of
Endocrinology, Qilu Hospital of Shandong University (Jinan,
Shandong), according to European Union legislations (15). The 24-h 131I pre-treatment
uptake value in the neck region was measured using a thyroid
function machine (MN-6110; Zhongke Zhongjia Scientific Instrument
Co., Ltd., Anhui, China). A total of 1mCi of 131I was
administered orally, followed by planar scintigraphy of the neck
region 24 h later. The uptake rate of 131I was used to
avoid unnecessary exposure and local radioiodine side-effects
(16). Uptake rates <5%, between
5–10% and >10% was followed by 100, 80 or 30 mCi of
131I in one dose for remnant ablation, respectively.
Generally, uptake rate was <5% following total thyroidectomy. A
total of 2 h later, the patients were encouraged to drink more
water, resulting in increased rates of urination. Oral prednisone
and vitamin C were administered to alleviate the local radioiodine
side effects. The patients continued receiving levothyroxine sodium
tablets replacements 48 h later, to suppress TSH levels to
<0.1–0.5 mIU/l. A WBIS was performed 5–7 days following
131I administration to ensure proper tracer localization
in the residual functioning thyroid tissues in the neck, and to
confirm the presence of any cervical lymph node or distant
functioning metastases. A panel of 3 nuclear medicine physicians
performed the aforementioned procedures. The patients with CLNM, as
identified by WBIS, received a second ablation with oral 120 mCi
131I 6 months following the first ablation. The
preparation for the 6-month post-therapy evaluation was similar to
that for the pre-ablation scan. If the second 131I
treatment failed again, the patients received a third ablation with
150 mCi 131I. The decision of repeat 131I
administration was based on detectable serum Tg levels or on
abnormal uptake in WBIS. Repetitive 131I treatments were
administrated until successful ablation was achieved, or until the
patient did not tolerate or refuse the treatment, subsequent to
which annual check-ups were planned with the measurement of Tg
levels.
Outcome assessment
Successful ablation was defined as stimulated serum
Tg levels of <2 ng/ml with negative Anti-Tg in the absence of
cervical lymph node metastases on the ultrasound scan of the neck
and on WBIS. Patients who did not fulfill these criteria were
considered to exhibit persistent disease. Disease recurrence was
monitored in patients who were in remission for ≥1 year, and if a
follow-up examination revealed evidence of disease recurrence by
imaging and/or raised thyroglobulin levels under either TSH
suppression or stimulation. Persistent and recurrent disease was
defined as unsuccessful ablation.
Hormone measurements
The ARCHITECT TSH assay was used to measure TSH
levels with chemiluminescent microparticle immunoassay (CMIA), with
an analytical sensitivity of 0.0025 µIU/l and functional
sensitivity of 0.01 µIU/l, according to ARCHITECT i system (Abbott
Laboratories, Chicago, IL, USA). Tg serum level was measured by an
immunochemiluminometric two-site immunoassay, with a calibration
range of 0.04–500 ng/ml (Roche Diagnostics GmbH, Mannheim,
Germany). The measurement of Anti-Tg was performed using the
ARCHITECT Anti-Tg assay with a calibration range of 0.0–1,000.0
IU/ml. The assay was supplied by Fisher Diagnostics (Thermo Fisher
Scientific, lnc., Waltham, MA, USA).
Statistical analysis
Statistical analyses were performed with SPSS
statistical software (version 16.0; SPSS, Inc., Chicago, IL, USA).
Categorical values are presented as relative frequencies. A
χ2 test was used to compare categorical data. Univariate
Cox proportional hazards regression analysis was used to determine
the factors affecting survival time. All possible predictive
variables were entered into multivariate logistic model with a
backwards stepwise method to remove the least predictive variable
at each step. A two-tailed P<0.05 was considered to indicate a
statistically significant difference.
Results
General characteristics of the study
population
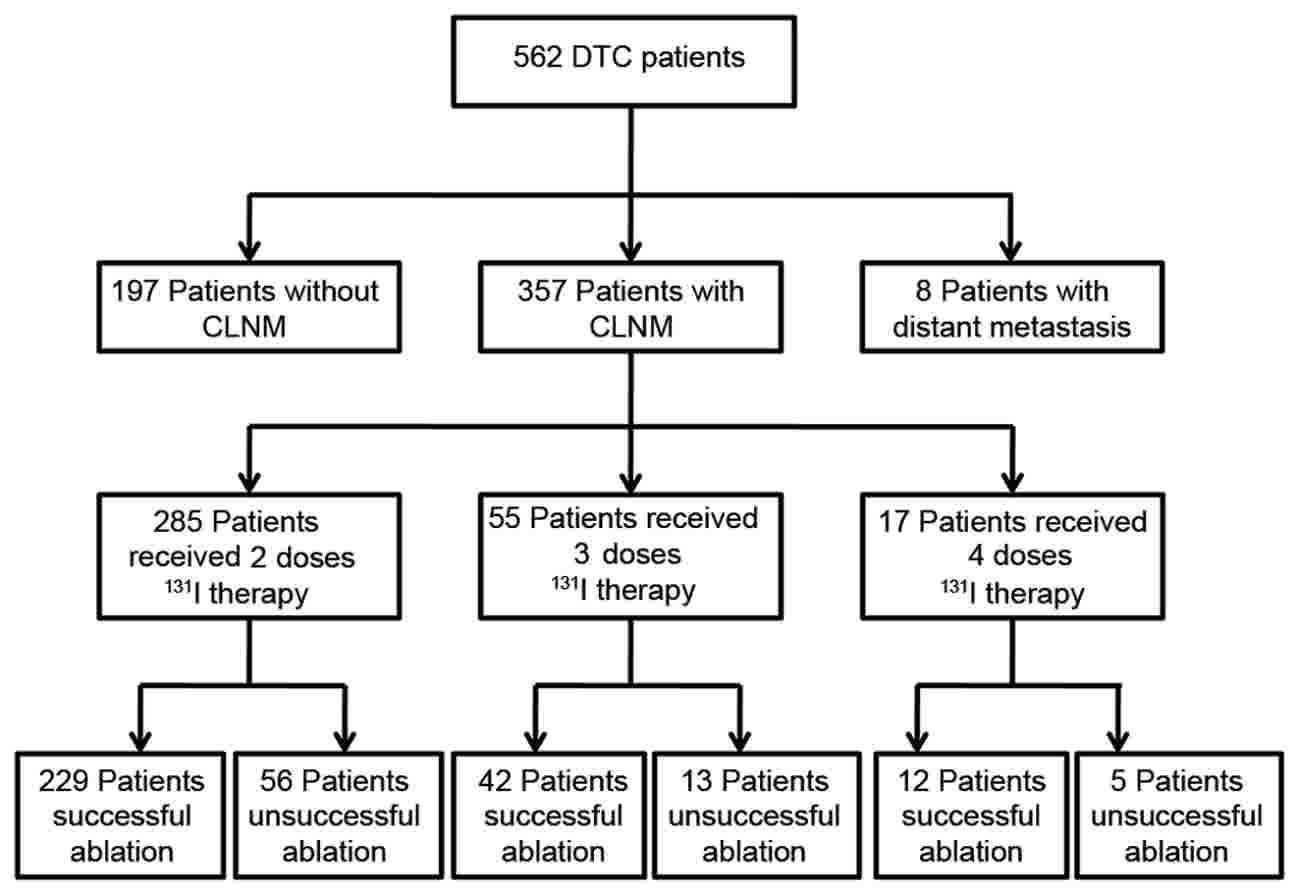
The present study retrospective study involved 562
patients with DTC who were referred to the Department of
Endocrinology, Qilu Hospital of Shandong University (Jinan,
Shandong), for 131I-postoperative ablation, including
197 patients without CLNM, 357 patients with CLNM and 8 patients
with distant metastasis. In general, the patients with DTC with
CLNM received remnant ablation and repetitive administration of
131I. The duration of 131I therapy was based
either on detectable serum Tg levels or abnormal absorbance in
WBIS. A total of 357 patients with DTC with CLNM received
administration of 131I, in which 285, 55 and 17 patients
received 2, 3 or 4 doses of 131I therapy, respectively.
The rate of successful ablation was 80.35 (229/285), 76.36 (42/55)
and 70.59 (12/17) in these three groups, respectively. The
flowchart for the inclusion of all the participants is described in
Fig. 1. The clinical characteristics
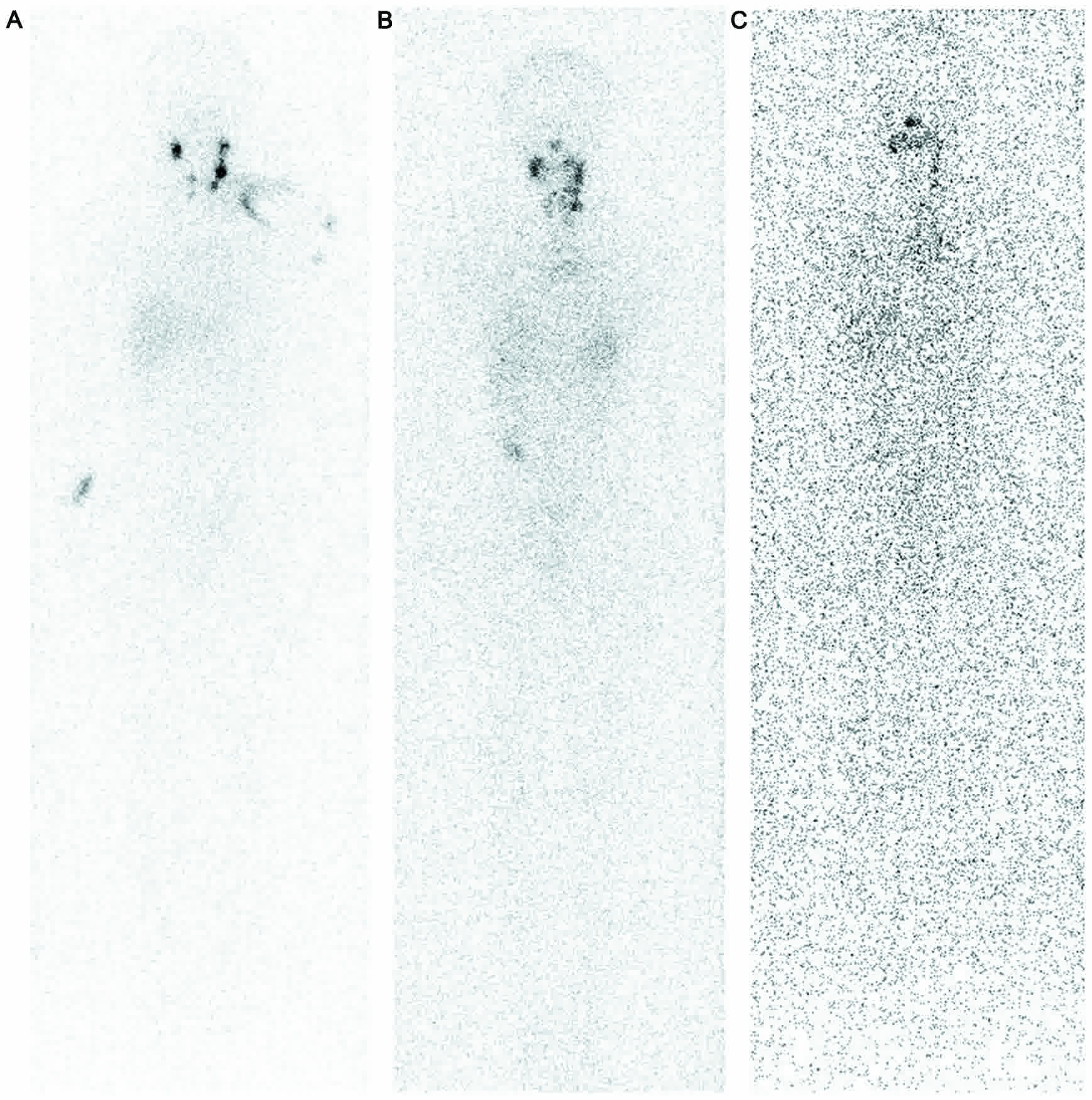
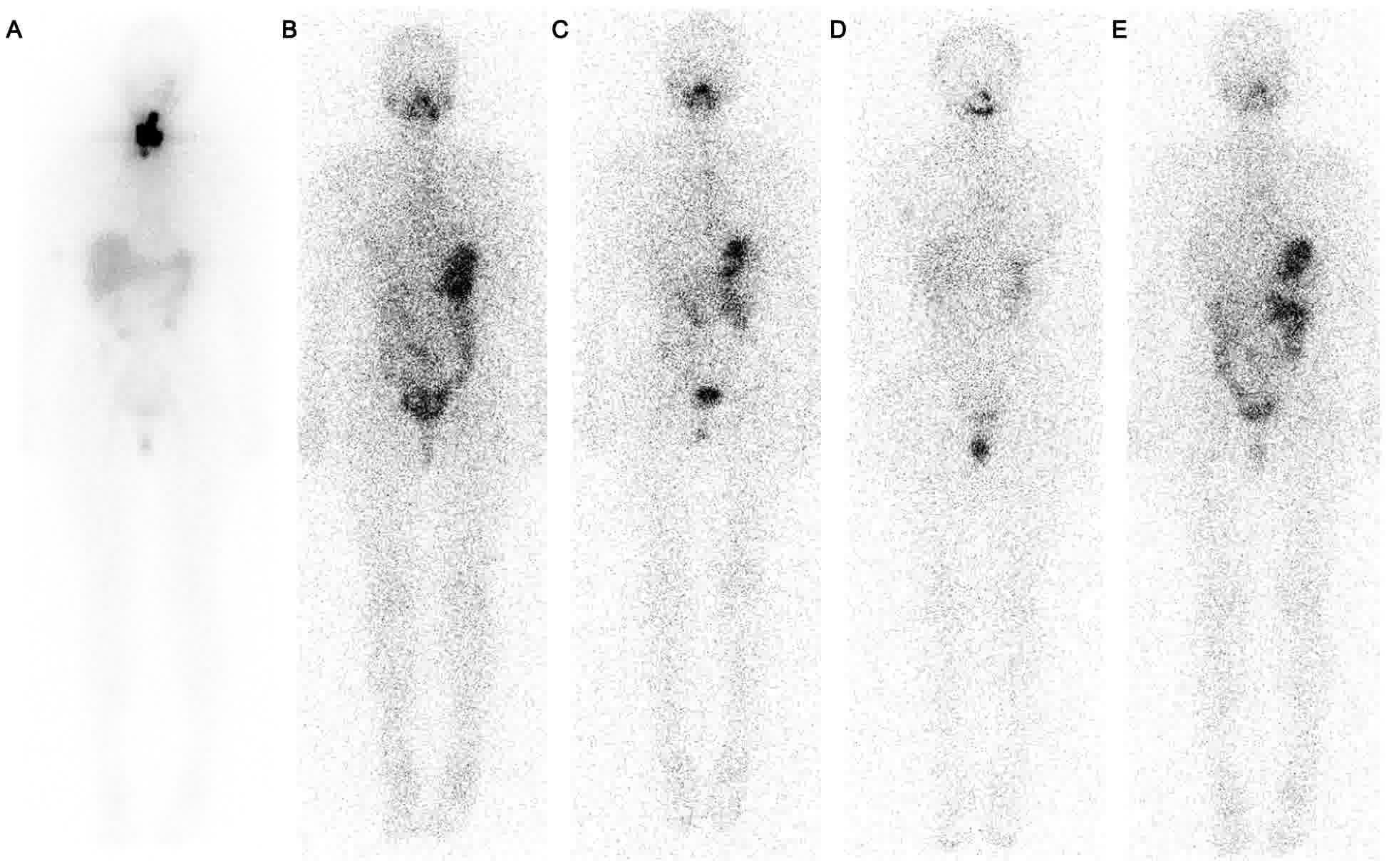
of the participants are summarized in Table I. The typical WBIS scanning of the
process of receiving 131I administration is presented in
Figs. 2–4.
 | Table I.Baseline characteristics of the
patients with differentiated thyroid cancer with cervical lymph
node metastasis. |
Table I.
Baseline characteristics of the
patients with differentiated thyroid cancer with cervical lymph
node metastasis.
|
| Doses of 131I
therapy (N) |
|---|
|
|
|
|---|
|
Characteristics | 2 (n=285) | 3 (n=55) | 4 (n=17) |
|---|
| Age, years |
|
|
|
|
<45 | 139 | 28 | 7 |
|
≥45 | 146 | 27 | 10 |
| Sex |
|
|
|
|
Male | 68 | 20 | 6 |
|
Female | 217 | 35 | 11 |
| Previous thyroid
surgery |
|
|
|
|
Near-total thyroidectomy | 19 | 12 | 3 |
| Total
thyroidectomy | 266 | 43 | 14 |
| Histopathological
types |
|
|
|
|
Papillary carcinoma | 276 | 53 | 16 |
|
Follicular carcinoma | 9 | 2 | 1 |
| Size of tumor,
cm |
|
|
|
|
<2 | 171 | 22 | 6 |
|
2-4 | 91 | 28 | 7 |
|
>4 | 23 | 5 | 4 |
| Number of
nodules |
|
|
|
|
Solitary | 97 | 16 | 6 |
|
Multiple | 188 | 39 | 11 |
| Capsular
invasion |
|
|
|
|
Yes | 259 | 52 | 16 |
| No | 26 | 3 | 1 |
| TNM stage |
|
|
|
| Stage
I–II | 140 | 27 | 7 |
| Stage
III–IV | 145 | 28 | 10 |
| RRS |
|
|
|
| Low
risk | 0 | 0 | 0 |
|
Intermediate risk | 259 | 47 | 9 |
| High
risk | 26 | 8 | 8 |
| Time from surgery
to ablation, month |
|
|
|
| ≤1 | 150 | 34 | 5 |
|
>1 | 135 | 21 | 12 |
| Ablation |
|
|
|
|
Successful ablation | 229 | 42 | 12 |
|
Unsuccessful ablation | 56 | 13 | 5 |
Successful ablation was associated
with clinical characteristics in patients with DTC with CLNM who
received 2 doses of 131I therapy
To identify potential effects of the clinical
features on successful ablation, the differences in clinical
pathological characteristics between patients with successful and
unsuccessful ablation were compared. Due to the limited data of the
patients who received 3 and 4 doses of 131I treatment,
the analysis of these results was excluded, and the present study
focused on the patients who received 2 doses of 131I
therapy. The proportion of patients with successful ablation was
80.35% (229/285) in this subgroup. The clinical characteristics,
including sex, age, the type of thyroid surgery, histopathological
type, tumor size, number of tumors, capsular invasion, time
interval from surgery to ablation, TNM stage and recurrence risk
stratification (RRS) risk are summarized in Table II.
| Table II.Comparison of baseline
characteristics of successful and unsuccessful ablation in patients
with differentiated thyroid cancer with cervical lymph node
metastasis who received two doses of radioiodine-131 therapy. |
Table II.
Comparison of baseline
characteristics of successful and unsuccessful ablation in patients
with differentiated thyroid cancer with cervical lymph node
metastasis who received two doses of radioiodine-131 therapy.
|
Characteristics | Successful
ablation, n (%) | Unsuccessful
ablation, n (%) | P-value |
|---|
| Age, years |
|
|
|
|
<45 | 126 (90.65) | 13 (9.35) | <0.001 |
|
≥45 | 103 (70.55) | 43 (29.45) |
|
| Sex |
|
|
|
|
Male | 55 (80.88) | 13 (19.12) | 0.899 |
|
Female | 174 (80.18) | 43 (19.82) |
|
| Previous thyroid
surgery |
|
|
|
|
Near-total thyroidectomy | 14 (73.68) | 5 (26.32) | 0.548 |
| Total
thyroidectomy | 215 (80.83) | 51 (19.17) |
|
| Histopathological
type |
|
|
|
|
Papillary carcinoma | 222 (80.43) | 54 (19.57) | 0.692 |
|
Follicular carcinoma | 7 (77.78) | 2 (22.22) |
|
| Size of tumor,
cm |
|
|
|
|
<2 | 157 (91.81) | 14 (8.19) | <0.001 |
| ≥2 | 72 (63.16) | 42 (36.84) |
|
| Number of
nodules |
|
|
|
|
Solitary | 85 (87.63) | 12 (12.37) | 0.026 |
|
Multiple | 144 (76.60) | 44 (23.40) |
|
| Capsular
invasion |
|
|
|
|
Yes | 205 (79.15) | 54 (20.85) | 0.107 |
| No | 24 (92.31) | 2 (7.69) |
|
| TNM stage |
|
|
|
| Stage
I–II | 128 (91.43) | 12 (8.57) | <0.001 |
| Stage
III–IV | 101 (69.66) | 44 (30.34) |
|
| RRS |
|
|
|
|
Intermediate risk | 211 (81.47) | 48 (18.53) | 0.134 |
| High
risk | 18 (69.23) | 8 (30.77) |
|
| Time from surgery
to ablation, month |
|
|
|
| ≤1 | 122 (81.33) | 28 (18.67) | 0.660 |
|
>1 | 107 (79.26) | 28 (20.74) |
|
There was no significant difference between the rate
of successful and unsuccessful ablation with respect to sex
(P=0.899), type of thyroid surgery (P=0.548), histopathological
type (P=0.692), capsular invasion (P=0.107), RSS risk (P=0.134) and
time interval from surgery to ablation (P=0.660). However, a
significantly higher rate of successful ablation was identified in
patients who were <45 years old compared with patients who were
≥45 years old (P<0.001). There was also a significantly higher
level of successful ablation in patients with tumor size <2 cm
compared with patients with tumor size ≥2 cm (P<0.001). Notably,
successful ablation was significantly higher in patients with
solitary nodules compared with patients with multiple nodules
(P=0.026). Additionally, the patients with stages I–II disease
exhibited a higher successful ablation rate compared with patients
with stage III–IV disease (P<0.001). These results indicated
that successful ablation may be affected, or partly affected, by
certain critical clinical factors, including age, tumor size,
number of nodules and TNM stages in patients with DTC with
CLNM.
Independent risk factor for successful
ablation in DTC patients with CLNM who received two doses of
131I therapy
As the χ2 test for the association of
categorical variables revealed that age, tumor size, number of
nodules and TNM stage are able to affect the rate of successful
ablation, these factors may be independent risk factors for
successful ablation in patients with DTC with CLNM who received 2
doses of 131I therapy.
The present study identified the potential risk
factors for successful ablation using univariate and multivariate
logistic regression analysis. As indicated in Table III, univariate logistic regression
identified no significant association of successful ablation with
sex (P=0.899), type of thyroid surgery (P=0.411), histopathological
types (P=0.844), capsular invasion (P=0.316), RSS risk (P= 0.512)
and time interval from surgery to ablation (P=0.497). Notably, age
(P=0.003), tumor size (P<0.001), number of nodules (P=0.029) and
TNM stage (P<0.001) were significantly associated with
successful ablation. Multivariate analysis indicated that age
(P=0.183) was not significantly associated with the rate of
successful ablation, but tumor size (P<0.001), number of nodules
(P=0.012) and TNM stage (P<0.001) remained significantly
associated with the rate of successful ablation. These results
revealed that tumor size, number of nodules and TNM stage may be
independent risk factors associated with successful ablation in
patients with DTC with CLNM who received 2 doses of 131I
therapy.
| Table III.Univariate and multivariate Cox
regression analyses in patients with differentiated thyroid cancer
with cervical lymph node metastasis who received two doses of
radioiodine-131 therapy (n=285) and the effect of successful
ablation. |
Table III.
Univariate and multivariate Cox
regression analyses in patients with differentiated thyroid cancer
with cervical lymph node metastasis who received two doses of
radioiodine-131 therapy (n=285) and the effect of successful
ablation.
| A, Univariate
analysis |
|---|
|
|---|
| Variable | HR | 95% CI | P-value |
|---|
| Age | 0.963 | 0.940–0.987 | 0.003 |
| Sex | 1.046 | 0.524–2.085 | 0.899 |
| Type of thyroid
surgery | 1.521 | 0.560–4.130 | 0.411 |
| Histopathological
type | 1.175 | 0.237–5.814 | 0.844 |
| Tumor size | 0.460 | 0.354–0.600 | <0.001 |
| Number of
nodules | 2.164 | 1.083–4.325 | 0.029 |
| Capsular
invasion | 0.316 | 0.072–1.380 | 0.316 |
| TNM stage | 0.243 | 0.124–0.476 | <0.001 |
| ETA risk | 0.512 | 0.210–1.246 | 0.512 |
| Time from surgery
to ablation | 0.817 | 0.455–1.466 | 0.497 |
|
| B, Multivariate
analysis |
|
|
Variable | HR | 95% CI | P-value |
|
| Age | 1.031 | 0.986–1.079 | 0.183 |
| Sex | – | – | – |
| Type of thyroid
surgery | – | – | – |
| Histopathological
types | – | – | – |
| Tumor size | 0.434 | 0.323–0.585 | <0.001 |
| Number of
nodules | 2.828 | 1.257–6.360 | 0.012 |
| Capsular
invasion | – | – | – |
| TNM stage | 0.243 | 0.116–0.513 | <0.001 |
| RRS risk | – | – | – |
| Time from surgery
to ablation | – | – | – |
Discussion
CLNM is common in DTC, with a frequency of 30–90%
(17) and has been demonstrated to be
closely associated with higher recurrence and poorer survival rates
in patients with DTC (18). The
majority of metastatic sites are located in central compartment
lymph nodes, and complete central lymph node dissection has been
identified to reduce the incidence of disease persistence,
recurrence and mortality (19).
However, when lymph nodes metastasis is not restricted to the
central compartment, post-operative remnant ablation is
supplemented to eradicate remnant CLNM. Previous studies have
demonstrated that remnant ablation is an independent variable that
reduces loco-regional recurrence, distant metastases and
cancer-associated mortality (20).
However, no single group achieved 100% ablation following remnant
ablation (21). The majority of
patients with DTC with CLNM required repetitive 131I
treatments (22). Therefore, the
present retrospective study of 357 patients with DTC with CLNM was
performed to investigate the rate of successful ablation, and to
analyze the effects of possible prognostic factors affecting
successful ablation, including age, tumor size, number of nodules
and TNM stage.
In the present study, although one dose of 100 mCi
131I was administered, successful remnant ablation was
not achieved in any of the patients with DTC and CLNM. This is in
contrast with a number of studies that have demonstrated that the
administration of 100 mCi 131I achieved an acceptable
ablation rate, from 50 to 100% (23–25). The
difference in ablation outcomes was associated with the clinical
characteristics of the participants: The patients recruited in the
present study exhibited CLNM, whereas the patients in the
previously reported studies did not exhibit extra-thyroidal
extension, nor lymph node or distant metastases, suggesting that
lymph node or distant metastases may be an independent risk factor
affecting successful remnant ablation.
In clinical practice, patients who fail to achieve
complete ablation following remnant ablation should receive a
second administration of 131I to achieve successful
ablation (26). In the present study,
all of these patients received ≥2 doses of 131I therapy,
with a maximum of 4 doses. The rate of successful ablation was
80.35% (229/285) at 2 doses, 76.36% (42/55) at 3 doses, 70.58%
(12/17) at 4 doses. The second, third and fourth 131I
treatments were administered orally, with 120, 150 and 150 mCi,
respectively. The rate of successful ablation was in agreement with
results from a previous study, which stated that 30–50 mCi, 75 mCi
or 100 mCi as a second 131I treatment achieved
successful ablation in patients with DTC confined to the thyroid
(27). This may be partially
explained by the change in size of remnant thyroid tissue, which is
expected to become significantly smaller following a high initial
dose of 131I. A low dosage may have an almost equal
ablation outcome compared with high activity in patients with small
remnants of thyroid tissue (12).
Similar to patients with DTC restricted to the thyroid, whether
patients with DTC with CLNM would be able to use a lower dosage as
a second dose to achieve a complete ablation outcome should be
examined in future studies, to alleviate local radioiodine
side-effects.
In the present study, a number of patients that
received 4 doses of 131I treatment did not achieve
successful ablation. These results indicated that the diminution of
remnant lymph node tissues following remnant ablation and the
different 131I activity was not solely associated with
ablation outcomes. Therefore, the factors that may contribute to
successful ablation in patients with DTC with CLNM were
investigated. Due to a large disparity in the numbers of patients
receiving 2, 3 and 4 doses of 131I, the present analysis
concentrated on those receiving 2 doses of 131I. It was
identified that tumor size, number of nodules and TNM stage were
the independent risk factors affecting successful ablation in
patients with DTC with CLNM who received 2 doses of 131I
therapy. Additionally, age was significantly associated with
complete ablation in the univariate analysis, particularly in
patients aged ≤45 years. It has demonstrated that the delay in
initial 131I therapy following total thyroidectomy in
patients with DTC with metastases resulted in poor survival
(28). However, in the present study,
the timing of the first 131I treatment exhibited no
effect on the rate of successful ablation, which was consistent
with the findings of Tsirona et al (29).
There are several limitations with the present
study. Firstly, the assessment time of successful ablation was
between 8 and 55 months. Future recurrence was not addressed due to
short follow-up periods. Long-term follow-up should be performed in
the future studies to examine distant metastasis and recurrence.
Secondly, the participants with CLNM were diagnosed at the entry of
this trial, and the changes in lymph node and distant metastasis
were not observed during follow-up, which may be a factor
contributing to unsuccessful ablation, and should be addressed in
future follow-up. Additionally, as there was a large variation in
the numbers of patients included in the groups, the analysis
between the patients with DTC who received 2, 3 and 4 doses of
131I treatment was not relevant; an increased number of
patients should have been recruited. Finally, as the trial was only
performed in a single center, the Qilu Hospital of Shandong
University, all conclusions should be verified in a multi-center,
large-scale cohort.
In conclusion, the present study demonstrated that
131I administration is a useful therapy to eradicate
remnant thyroid tissue and cervical lymph node metastasis in
patients with differentiated thyroid cancer, and that age, tumor
size, number of nodules and TNM stage were independent risk factors
affecting successful ablation in patients with DTC with CLNM.
Therefore, 131I treatment is preferentially indicated in
patients with DTC with CLNM who are aged <45 years, with tumor
sizes <2 cm, solitary nodules and lower TNM stages in order to
control and prevent recurrence and/or metastases.
Acknowledgements
The authors would like to thank Professor Jun Peng,
Wen Wang and Jinbo Liu (Qilu Hospital of Shandong University) for
their help in revising the manuscript.
Funding
No funding was received.
Availability of data and materials
The data of the present study is be available upon
request from the corresponding author.
Authors' contributions
CJC and CYD contributed to the majority of the
experiments, data collection, study design and drafted the
manuscript. CJC, CYD, JYL and WLX contributed to data analysis.
ZSL, WZ, LC and KHZ contributed to data and figure collection. CJC
and HL conceived the study. HL was responsible for study
supervision
Ethics approval and consent to
participate
The Medical Ethical Committee of Qilu Hospital of
Shandong University approved the present study. Informed consent
was obtained from each patient before entering this experiment.
Consent for publication
Informed consent was obtained from each patient
before entering this experiment.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
DTC
|
differentiated thyroid cancer
|
|
CLNM
|
cervical lymph node metastasis
|
|
131I
|
radioiodine-131
|
|
WBIS
|
whole-body iodine scan
|
|
Tg
|
thyroglobulin
|
|
Anti-Tg
|
anti-thyroglobulin antibodies
|
|
RSS
|
recurrence risk stratification
|
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Mitchell AL, Gandhi A, Scott-Coombes D and
Perros P: Management of thyroid cancer: United kingdom national
multidisciplinary guidelines. J Laryngol Otol. 130:S150–S160. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Shi RL, Qu N, Yang SW, Ma B, Lu ZW, Wen D,
Sun GH, Wang Y and Ji QH: Tumor size interpretation for predicting
cervical lymph node metastasis using a differentiated thyroid
cancer risk model. Onco Targets Ther. 9:5015–5022. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wang TS, Dubner S, Sznyter LA and Heller
KS: Incidence of metastatic well-differentiated thyroid cancer in
cervical lymph nodes. Arch Otolaryngol Head Neck Surg. 130:110–113.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hay ID, Grant CS, van Heerden JA, Goellner
JR, Ebersold JR and Bergstralh EJ: Papillary thyroid
microcarcinoma: A study of 535 cases observed in a 50-year period.
Surgery. 112:1139–1147. 1992.PubMed/NCBI
|
|
6
|
Lang BH, Ng SH, Lau LL, Cowling BJ, Wong
KP and Wan KY: A systematic review and meta-analysis of
prophylactic central neck dissection on short-term locoregional
recurrence in papillary thyroid carcinoma after total
thyroidectomy. Thyroid. 23:1087–1098. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hundahl SA, Cady B, Cunningham MP,
Mazzaferri E, McKee RF, Rosai J, Shah JP, Fremgen AM, Stewart AK
and Hölzer S: Initial results from a prospective cohort study of
5583 cases of thyroid carcinoma treated in the united states during
1996. U.S. and German thyroid cancer study group. An American
college of surgeons commission on cancer patient care evaluation
study. Cancer. 89:202–217. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ain KB: Radioiodine-remnant ablation in
low-risk differentiated thyroid cancer. Pros Endocrine. 50:61–66.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Schlumberger M, Catargi B, Borget I,
Deandreis D, Zerdoud S, Bridji B, Bardet S, Leenhardt L, Bastie D,
Schvartz C, et al: Strategies of radioiodine ablation in patients
with low-risk thyroid cancer. N Engl J Med. 366:1663–1673. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lee YM, Cho JY, Sung TY, Kim TY, Chung KW,
Hong SJ and Yoon JH: Clinicopathological risk factors and
biochemical predictors of safe discharge after total thyroidectomy
and central compartment node dissection for thyroid cancer: A
prospective study. Int J Endocrinol. 2015:2145252015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jia Q, Meng Z, Tan J, Zhang G, He Y, Sun
H, Yu C, Li D, Zheng W, Wang R, et al: Retrospective imaging study
on the diagnosis of pathological false positive iodine-131 scans in
patients with thyroid cancer. Exp Ther Med. 10:1995–2001. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hackshaw A, Harmer C, Mallick U, Haq M and
Franklyn JA: 131I activity for remnant ablation in patients with
differentiated thyroid cancer: A systematic review. J Clin
Endocrinol Metab. 92:28–38. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Edge SB and Compton CC: The American Joint
Committee on Cancer: The 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
American Thyroid Association (ATA)
Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid
Cancer, . Cooper DS, Doherty GM, Haugen BR, Kloos RT, Lee SL,
Mandel SJ, Mazzaferri EL, McIver B, Pacini F, et al: Revised
American Thyroid Association management guidelines for patients
with thyroid nodules and differentiated thyroid cancer. Thyroid.
19:1167–1214. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Harding LK: Radiation protection
legislation. Eur J Nucl Med. 25:187–191. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Alexander C, Bader JB, Schaefer A, Finke C
and Kirsch CM: Intermediate and long-term side effects of high-dose
radioiodine therapy for thyroid carcinoma. J Nucl Med.
39:1551–1554. 1998.PubMed/NCBI
|
|
17
|
Chang H, Yoo RN, Kim SM, Kim BW, Lee YS,
Lee SC, Chang HS and Park CS: The clinical significance of the
right para-oesophageal lymph nodes in papillary thyroid cancer.
Yonsei Med J. 56:1632–1637. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Gulcelik MA, Ozdemir Y, Kadri Colakoglu M,
Camlibel M and Alagol H: Prognostic factors determining survival in
patients with node positive differentiated thyroid cancer: A
retrospective cross-sectional study. Clin Otolaryngol. 37:460–467.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
American Thyroid Association Surgery
Working Group; American Association of Endocrine Surgeons, American
Academy of Otolaryngology-Head and Neck Surgery, American Head and
Neck Society, . Carty SE, Cooper DS, Doherty GM, Duh QY, Kloos RT,
Mandel SJ, et al: Consensus statement on the terminology and
classification of central neck dissection for thyroid cancer.
Thyroid. 19:1153–1158. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bal CS, Kumar A and Pant GS: Radioiodine
dose for remnant ablation in differentiated thyroid carcinoma: A
randomized clinical trial in 509 patients. J Clin Endocrinol Metab.
89:1666–1673. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
M E, l-Refaei S, W Yassin S, Salman K, Al
Munshy T, Al-Ezzi M, M Al-Sayed Y and Abd Elkareem Husseni M:
Comparison between low and high radioactive iodine (131I)
reablation dose in patients with papillary thyroid cancer. Nucl Med
Commun. 36:114–119. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lim YC, Liu L, Chang JW and Koo BS:
Lateral lymph node recurrence after total thyroidectomy and central
neck dissection in patients with papillary thyroid cancer without
clinical evidence of lateral neck metastasis. Oral Oncol.
62:109–113. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wagieh SM, El-Refaei SM, Salem SS,
Al-Shiekh EA, Al-Ghamdy HA and Al-Juhani NR: Impact of
histopathology of non-neoplastic thyroid tissue on ablation outcome
in patients with papillary thyroid cancer. Nucl Med Commun.
32:597–604. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Pacini F, Schlumberger M, Harmer C, Berg
GG, Cohen O, Duntas L, Jamar F, Jarzab B, Limbert E, Lind P, et al:
Post-surgical use of radioiodine (131I) in patients with papillary
and follicular thyroid cancer and the issue of remnant ablation: A
consensus report. Eur J Endocrinol. 153:651–659. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Tsang RW, Brierley JD, Simpson WJ,
Panzarella T, Gospodarowicz MK and Sutcliffe SB: The effects of
surgery, radioiodine, and external radiation therapy on the
clinical outcome of patients with differentiated thyroid carcinoma.
Cancer. 82:375–388. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
McCowen KD, Adler RA, Ghaed N, Verdon T
and Hofeldt FD: Low dose radioiodide thyroid ablation in
postsurgical patients with thyroid cancer. Am J Med. 61:52–58.
1976. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Prpic M, Dabelic N, Stanicic J, Jukic T,
Milosevic M and Kusic Z: Adjuvant thyroid remnant ablation in
patients with differentiated thyroid carcinoma confined to the
thyroid: A comparison of ablation success with different activities
of radioiodine (I-131). Ann Nucl Med. 26:744–751. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Higashi T, Nishii R, Yamada S, Nakamoto Y,
Ishizu K, Kawase S, Togashi K, Itasaka S, Hiraoka M, Misaki T and
Konishi J: Delayed initial radioactive iodine therapy resulted in
poor survival in patients with metastatic differentiated thyroid
carcinoma: A retrospective statistical analysis of 198 cases. J
Nucl Med. 52:683–689. 2012. View Article : Google Scholar
|
|
29
|
Tsirona S, Vlassopoulou V, Tzanela M,
Rondogianni P, Ioannidis G, Vassilopoulos C, Botoula E, Trivizas P,
Datseris I and Tsagarakis S: Impact of early vs late postoperative
radioiodine remnant ablation on final outcome in patients with
low-risk well-differentiated thyroid cancer. Clin Endocrinol (Oxf).
80:459–463. 2014. View Article : Google Scholar : PubMed/NCBI
|