Introduction
Cancer stem cells (CSCs) are functionally defined by
their extensive self-renewal capacity. CSC confers increased radio-
and chemoresistance in tumors, resulting in tumor recurrence and
metastatic spread. Therefore, identification of the regulators that
control the tumorigenic potential of CSCs might provide new
therapeutic strategies against CSCs to improve cancer treatment.
The CSC theory suggests that only a few cancer cells with a
capacity for high tumorigenicity, self-renewal, and differentiation
are responsible for the maintenance and growth of tumors. Similar
to normal tissue stem cells, CSCs can also exist within a
supportive niche (1).
Oral squamous cell carcinoma (OSCC) patients in
stage I and II are mainly treated by surgery and almost all
patients show good prognosis, with a 5-year disease free survival
rate of early stage OSCC patients over 90%. However, approximately
10% of these early stage OSCC patients showed poor prognosis
(2) and some cases have shown
cervical lymph node metastasis and distant metastasis, with poor
outcome. Currently, there are no prognostic markers for these stage
I and II OSCC patients who show poor prognosis.
Cluster of differentiation (CD)44 is a cell surface
transmembrane glycoprotein encoded by the CD44 gene, which consists
of 20 exons. The standard isoform of CD44 is encoded by exons 1–5
and exons 16–20, and other CD44 variant (CD44v) protein isoforms
are generated by alternative splicing with variable exons (3). CD44 functions in various biological
processes, such as cell adhesion, cell migration, and cancer
metastasis. More recently, CD44 has been recognized as a CSC marker
in several types of cancers (3).
However, as CD44 is ubiquitously expressed in many cell types, its
usefulness as a CSC marker may be limited. Furthermore, conflicting
data in the field implicate the importance of CD44 in both tumor
suppression and progression, and these discrepancies have been
largely attributed to the expression of alternatively spliced
variants. Among the variants, CD44 variant 9 (CD44v9) may
contribute to cancer survival in harsh environments, such as high
reactive oxygen species-generated conditions from chemotherapy
and/or radiotherapy (4–6).
ATP-binding cassette sub-family G member 2 (ABCG2)
is a member of the ATP-binding cassette transporter protein
superfamily that produces multiple drug-resistant cancers (7) and is a molecular determinant for
maintaining the side population phenotype in stem cells. This
phenotype has been isolated from several primary tumors and cancer
cell lines, including those of the lung, esophagus, nasopharynx,
and oral cavity (8–10). Furthermore, ABCG2 expression has been
found in solid tumors of hepatocellular, lung, pancreas, and head
and neck squamous carcinomas (HNSCC) (8–10). ABCG2 plays a critical
role in the maintenance of the stem cell phenotype and multidrug
resistance of cancer cells (7). ABCG2
also regulates the pattern of cell division in non-small cell lung
cancer cell lines (9). A recent study
suggested that the ABCG2-positive side population cells with the
ability to exclude Hoechst 33342 and the possession of cancer
stem-like properties may play an important role in oral
carcinogenesis (9). Increasing
evidence suggests ABCG2 is a marker in CSC and plays a central role
in tumorigenesis (8–10).
CD24 is a mucin-like cell surface protein that is
expressed in cells of the hematopoietic system, in neuronal
tissues, and in certain epithelial cells such as keratinocytes
(11,12). Several studies have investigated CD24
expression in various malignant tissues; B cell lymphoma, lung,
pancreatic, colorectal, breast, and prostate cancer (13–15).
Although its physiologic functions are not fully elucidated, it
seems to be involved in the regulation of tumor proliferation and
adhesion. In cancer cells, the function of CD24 as a ligand for
P-selection may be important for the metastatic potential of the
tumors by facilitating interactions with endothelial cells.
Previous studies showed that elevation of CD24 expression in
various malignant tumors is associated with prognosis (12–15).
B-cell specific Moloney leukemia virus insert site 1
(BMI-1) is an essential constituent of polycomb repressive complex
1, a key epigenetic regulator. BMI-1 controls the cell cycle and
the self-renewal of tissue stem cells by regulating chromatin and
histone structure, and has been implicated in maintaining the
self-renewal of neural, hematopoietic, and intestinal stem cells.
Elevated Bmi-1 expression was demonstrated to be associated with
dysplastic cell transformation during oral carcinogenesis and to be
required for cancer cell replication and survival (16–18).
Aldehyde dehydrogenase 1 (ALDH1) contributes to the
oxidation of retinol acid in early stem cell differentiation and
also correlates with the number of cells undergoing
epithelial-mesenchymal transition, a process that is considered a
key for the formation of metastasis (19,20).
Several studies proposed ALDH1 as a putative marker for the
identification and isolation of CSCs in many kinds of cancers
including HNSCC (19,21,22).
Little is known regarding the biology or behavior of CD44, CD44V9,
ABCG2, CD24, BMI-1, ALDH1 of stage I and II OSCC. We would choose
those CSC marker among many reports considered important for
survival rates including esophageal, lung, gastric, colorectal, and
head and neck cancer (1–19,21,22). And the significance of
expression of those markers in stage I and II OSCC remains to be
determined. In this study, we evaluated the association between
expression of CSC markers and clinicopathological features of stage
I and II OSCC patients and determined the potential correlation
between CSC marker expression with clinical factors and prognosis.
The aim of the present study was to clarify the prognostic factors
for stage I and II OSCC patients focused on the expression of CSC
markers. Because we need to find the prognostic factor in order to
improve the poor outcome of approximately 10% of early stage OCC
patients.
Materials and methods
Patients
Oral cancer tissues were obtained from 70 OSCC
patients from Tokushima University Hospital at biopsy or surgery.
Sixty eight cases were used biopsy samples except surgery samples
of two cases. All patients were treated by surgery. Tumor size and
clinicopathological stage of OSCC were classified according to the
TNM staging system (2011). This study was approved by the Tokushima
University Human Investigations Committee Febuary 2016. The
Yamamoto-Kohama (YK) classification, which is a modified version of
the classification of Jakobsson et al (23) and Willen et al (24), was used for pathological grade of
tumor invasion (25). This
classification has five grades (1, 2, 3, 4C and 4D) and focuses on
the shape of tumor cell aggregation at the invasion front.
Immunohistochemistry: Samples were fixed in neutral
10% formalin and embedded in paraffin after resection. Sections (5
µm-thick) were cut and transferred on slides; sections were
deparaffinized in xylene and dehydrated in graded ethanol.
Endogenous peroxidase activity was blocked by 1% hydrogen peroxide,
and microwave antigen retrieval was carried out in a microwave
oven. Immunostaining was performed using an avidin-biotin
peroxidase enzyme complex (ABC kit; Vector Laboratories,
Burlingame, CA, USA). The sections were incubated with monoclonal
rabbit anti-human CD44 (clone EPR1013Y: dilution 1:100; Abcam,
Cambridge, UK), monoclonal rat anti-human CD44v9 (LKG-M001:
dilution 1:2,000; Funakoshi, Tokyo, Japan), monoclonal mouse
anti-human ABCG2 (clone BXP-21: dilution 1:100; Abcam), monoclonal
mouse anti-human CD24 (clone 8.B.76: dilution 1:50; Abcam),
monoclonal mouse anti-human Bmi-1 (clone 1.T.21: dilution 1:100;
Abcam), and monoclonal rabbit anti-human ALDH1 (clone EP1933Y:
dilution 1:100; Abcam) antibodies overnight at 4°C, and then
subsequently placed in secondary anti-rabbit antibody followed by
avidin-biotin complex reagent. The sections were finally incubated
in the substrate 3,3′diaminobenzidine (0.05%) and 0.1% hydrogen
peroxide for 8 min. The intensity of immunohistochemical staining
was graded as negative and positive; expressions of CSC markers
were considered positive when more than 10% of all tumor cells were
stained. The grade of staining intensity in case of different
biomarkers were not taken into consideration in this study.
Statistical analysis
Statistical analysis was performed by Kruskal-Wallis
test, Mann-Whitney U test between expressions of CSC markers
and clinicopathological factors. Survival analysis was calculated
using the Kaplan-Meier Method and compared using the log-rank test.
Cox hazard regression model was used for the multivariate analysis.
The results were quantified using hazard ratio (HR) with 95%
confidence interval (95% CI). P<0.05 was considered to indicate
a statistically significant difference.
Results
The expression of CD44, CD44v9, ABCG2,
CD24, BMI-1, and ALDH1 in OSCC with stage I and II
This study examined the expression of a panel of CSC
markers in oral cancer tissues from 70 OSCC patients. The
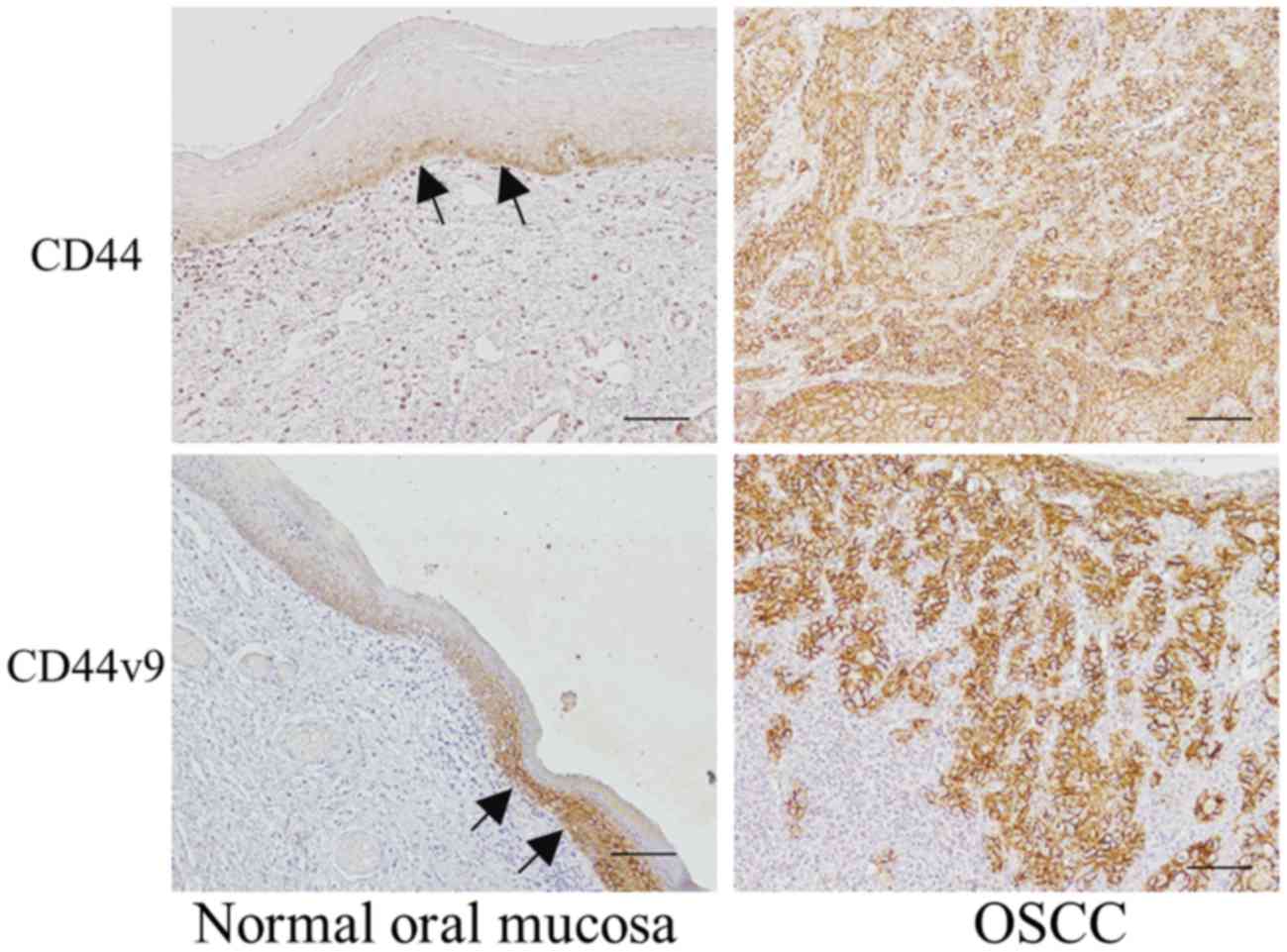
clinicopathological data of all patients are summarized in Table I. CD44 and CD44v9 protein expressions
were detected in all OSCC tissues and were observed in the majority
of tumor cells, as shown in Fig. 1
and Table II. CD44 and CD44v9
proteins were expressed in basal cell layer of normal oral
epithelium and in more than 50% of the cells in epithelial
dysplasia (data not shown). CD44 and CD44V9 proteins were localized
to the plasma membrane and cytoplasm in cancer cells, and tended to
exhibit intense irregular and disorganized staining patterns.
 | Table I.Clinicopathological characteristics of
the patients. |
Table I.
Clinicopathological characteristics of
the patients.
| Characteristic | Group | No. of patients |
|---|
| Sex | Male | 34 |
| Female | 36 |
| Age (years) | Median | 68 |
|
| Range | 35–97 |
| Primary site | Tongue | 38 |
|
| Oral floor | 5 |
|
| Upper gingiva | 5 |
|
| Lower gingiva | 16 |
|
| Buccal mucosa | 6 |
| T
classification | T1 | 17 |
|
| T2 | 53 |
| Histological
type |
Well-differentiated | 35 |
|
| Moderately
differentiated | 30 |
|
| Poorly
differentiated | 3 |
| YK
classification | YK1 | 5 |
|
| YK2 | 24 |
|
| YK3 | 30 |
|
| YK4C | 6 |
|
| YK4D | 3 |
| N status | N (+) | 14 |
|
| N (–) | 56 |
| Table II.Expression rate of CSC marker. |
Table II.
Expression rate of CSC marker.
| Marker | No. of positive
expression patients/total patients | Percentage |
|---|
| CD44 | 70/70 | 100 |
| CD44V9 | 70/70 | 100 |
| ABCG2 | 22/70 | 31.4 |
| CD24 | 41/70 | 59.0 |
| BMI-1 | 33/70 | 47.1 |
| ALDH1 | 18/70 | 25.7 |
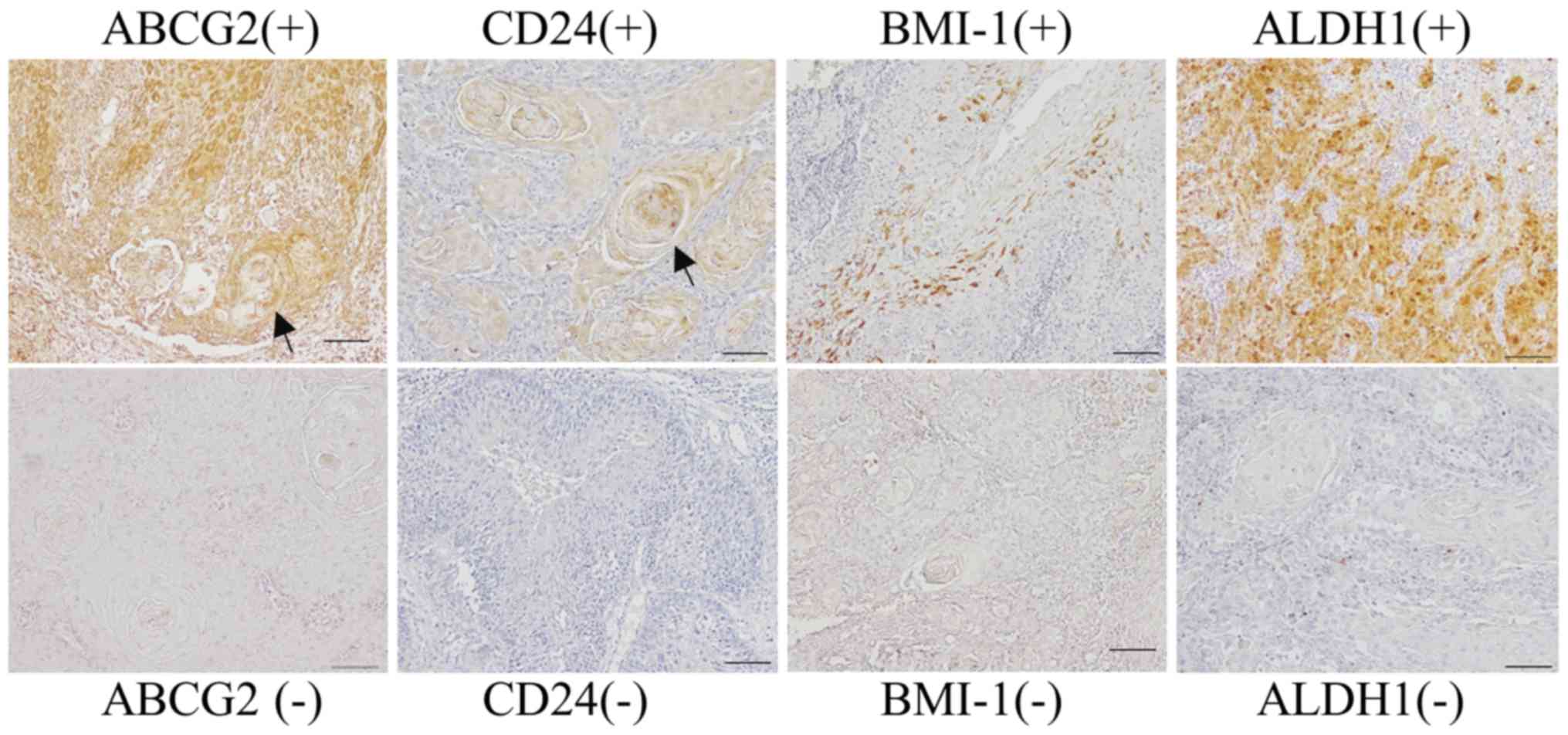
The rates of ABCG2, CD24, BMI-1, and ALDH1 positive
expression in OSCC patients were 31.4, 59.0, 47.1 and 25.7%,
respectively (Table II).
Representative staining images of ABCG2, CD24, BMI-1, and ALDH1
proteins are presented in Fig. 2.
ABCG2, CD24, BMI-1, and ALDH1 proteins were expressed in the plasma
membrane and cytoplasm. ABCG2, CD24, and ALDH1 proteins were mainly
localized in the invasive front. The well-differentiated cells
forming keratin pearls tended to show expression of CD24 and BMI-1
proteins. ALDH1-positive cells were scattered and were notably
absent in keratin pearls.
Correlation of CSC marker expressions
and clinicopathologic characteristics
We next examined the correlation of CSC marker
expressions with clinicopathologic features. Although ABCG2
expression was not associated with tumor size (Table III), histological differentiation,
or lymph node metastasis, its expression was significantly
associated with classification of invasion mode (YK classification)
in OSCC. CD24 expression was not associated with tumor size,
histological differentiation, or lymph node metastasis (Table IV). However, there was an association
between CD24 expression and invasion mode (YK classification).
BMI-1 expression was not related with tumor size, histological
differentiation, invasion mode (YK classification), or lymph node
metastasis (Table V). There was
significant association between ALDH1 expression and histological
differentiation, invasion mode or lymph node metastasis (Table VI).
| Table III.Statistical correlation of ABCG2
expression and clinicopathological features. |
Table III.
Statistical correlation of ABCG2
expression and clinicopathological features.
| Clinicopathological
feature | Group | ABCG2 (+) | ABCG2 (–) | P-value |
|---|
| T
classification | T1 | 6 | 11 | 0.71 |
|
| T2 | 16 | 37 |
|
| Histological
type |
Well-differentiated | 12 | 23 |
|
|
| Moderately
differentiated | 8 | 22 | 0.80 |
|
| Poorly
differentiated | 1 | 2 |
|
| YK classification
(invasion mode) | YK 1 | 1 | 4 |
|
|
| YK 2 | 12 | 12 |
|
|
| YK 3 | 3 | 27 | 0.04 |
|
| YK 4C | 3 | 1 |
|
|
| YK 4D | 2 | 1 |
|
| N status | N (+) | 7 | 7 | 0.10 |
|
| N (–) | 15 | 41 |
|
| Table IV.Statistical correlation of CD24
expression and clinicopathological features. |
Table IV.
Statistical correlation of CD24
expression and clinicopathological features.
| Clinicopathological
feature | Group | CD24 (+) | CD24 (–) | P-value |
|---|
| T
classification | T1 | 12 | 5 | 0.25 |
|
| T2 | 29 | 24 |
|
| Histological
type |
Well-differentiated | 24 | 11 |
|
|
| Moderately
differentiated | 15 | 15 | 0.21 |
|
| Poorly
differentiated | 1 | 2 |
|
| YK classification
(invasion mode) | YK 1 | 5 | 0 |
|
|
| YK 2 | 17 | 7 |
|
|
| YK 3 | 12 | 18 | 0.03 |
|
| YK 4C | 3 | 1 |
|
|
| YK 4D | 1 | 2 |
|
| N status | N (+) | 9 | 5 | 0.60 |
|
| N (–) | 32 | 24 |
|
| Table V.Statistical correlation of BMI-1
expression and clinicopathological features. |
Table V.
Statistical correlation of BMI-1
expression and clinicopathological features.
| Clinicopathalogical
feature | Group | BMI-1 (+) | BMI-1 (–) | P-value |
|---|
| T
classification | T1 | 6 | 11 | 0.26 |
|
| T2 | 27 | 26 |
|
| Histological
type |
Well-differentiated | 17 | 18 |
|
|
| Moderately
differentiated | 15 | 15 | 0.25 |
|
| Poorly
differentiated | 0 | 3 |
|
| YK classification
(invasion mode) | YK 1 | 3 | 2 |
|
|
| YK 2 | 12 | 12 |
|
|
| YK 3 | 14 | 16 | 0.55 |
|
| YK 4C | 2 | 2 |
|
|
| YK 4D | 0 | 3 |
|
| N status | N (+) | 4 | 10 | 0.12 |
|
| N (–) | 29 | 27 |
|
| Table VI.Statistical correlation of ALDH1
expression and clinicopathological features. |
Table VI.
Statistical correlation of ALDH1
expression and clinicopathological features.
| Clinicopathalogical
feature | Group | ALDH1 (+) | ALDH1 (–) | P-value |
|---|
| T
classification | T1 | 4 | 13 | 0.81 |
|
| T2 | 14 | 39 |
|
| Histological
type |
Well-differentiated | 7 | 28 |
|
|
| Moderately
differentiated | 8 | 22 | 0.01 |
|
| Poorly
differentiated | 3 | 0 |
|
| YK classification
(invasion mode) | YK 1 | 0 | 5 |
|
|
| YK 2 | 4 | 20 |
|
|
| YK 3 | 9 | 21 | 0.04 |
|
| YK 4C | 3 | 1 |
|
|
| YK 4D | 2 | 1 |
|
| N status | N (+) | 7 | 7 | 0.02 |
|
| N (–) | 11 | 45 |
|
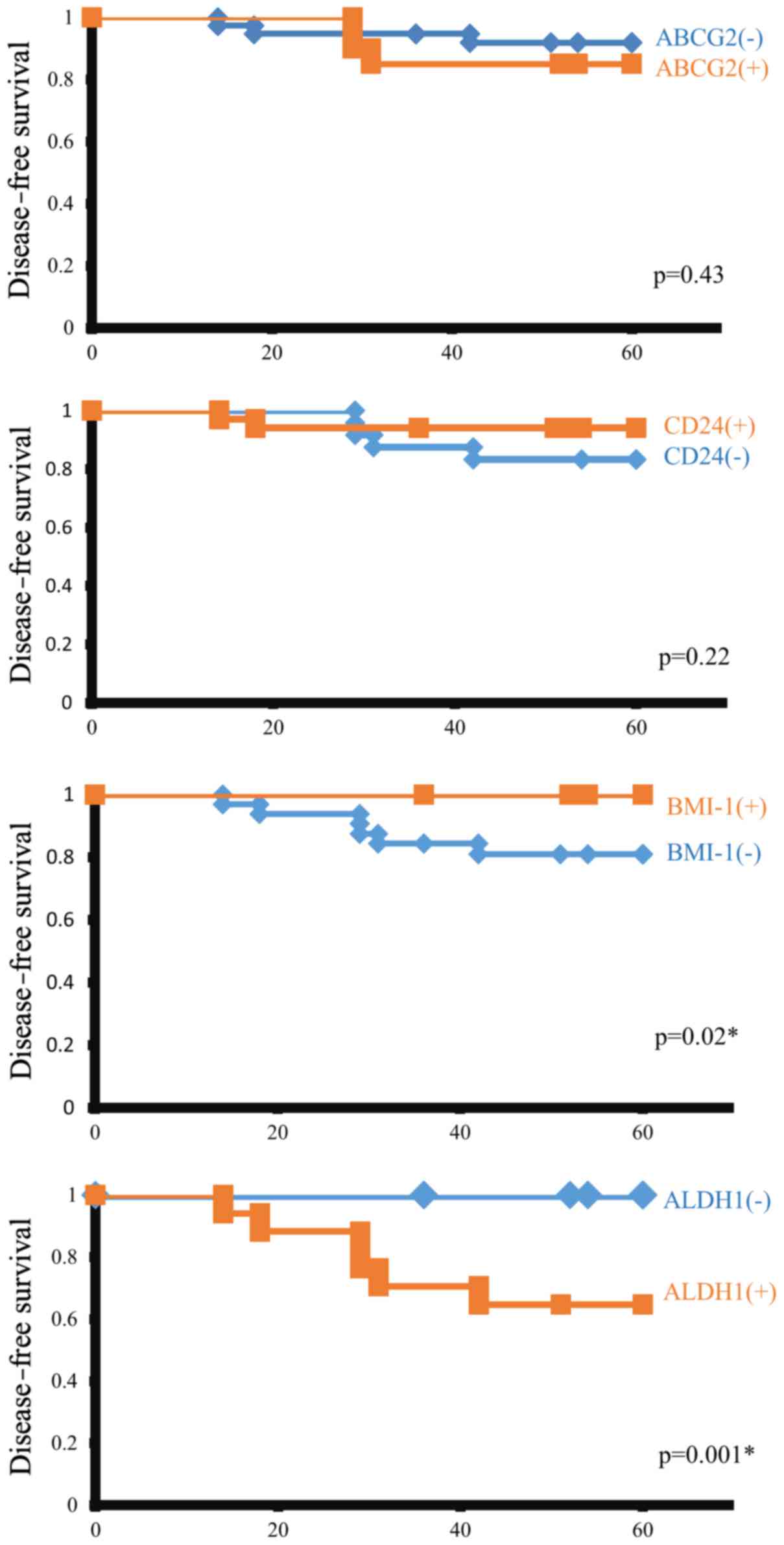
Survival analysis
We further determined the effects of the CSC marker
expression in stage I and II OSCC patients on survival rate
(Fig. 3). The data for overall
survival are almost same of the data for disease free survival,
because only one patients was died at other disease other than
OSCC. So we could not show the data for overall survival. The
expressions of ABCG2 or CD24 did not show an association with
disease-free survival rate. Patients with BMI-1 expression showed
better prognosis, and those who lacked BMI-1 expression showed
worse prognosis. ALDH1 expression was significantly associated with
worse prognosis. Multivariate analysis showed that ALDH1 expression
was the only prognostic factor against disease-free survival rate
(HR, 15.82, 95% CI, 1.08–231.48, P=0.04; Table VII).
| Table VII.Cox regression analysis of CSC marker
expression and disease free survival. |
Table VII.
Cox regression analysis of CSC marker
expression and disease free survival.
| Factor | HR | (95% CI) | P-value |
|---|
| Age | 0.99 | (0.91–1.08) | 0.79 |
| Primary site | 0.71 | (0.27–1.85) | 0.48 |
| Histological
type | 0.85 | (0.22–3.34) | 0.82 |
| YK
classification | 3.09 | (0.80–12.03) | 0.10 |
| ABCG2 | 0.56 | (0.04–7.51) | 0.67 |
| CD24 | 0.83 | (0.09–7.57) | 0.87 |
| BMI-1 | 1.85 | (0.13–25.71) | 0.21 |
| ALDH1 | 15.82 | (1.08–231.48) | 0.04 |
Discussion
This study clearly demonstrated that there was
significant association between ALDH1 expression and histological
differentiation or invasion mode; ABCG2 expression and invasion
mode; and CD24 expression and invasion mode in stage I and II OSCC
patients. In addition, the expression of ALDH1 and lack of BMI-1
expression were significantly associated with survival in stage I
and II OSCC patients.
We determined the expression of CD44 and CD44v9 in
the oral mucosa and cancer tissues in 70 stage I and II OSCC
patients. CD44 and CD44v9 expressions were almost in basal layer of
normal epithelium and were abundantly expressed in most tumor
cells. A previous study showed that CD44 expression was detected in
0.1–41.7% HNSCC cases (26). Sato
et al found that increased expression of CD44v9 was
significantly associated with poorer clinical outcome in OSCC
(27). These findings are not in
agreement with the results of this study showing that CD44 and
CD44v9 were abundantly expressed in OSCC. Many reports investigated
the CD44 expression rate (50~80%) and relationship between CD44s
expression and clinicopathological factors (28,29).
However, the results of these studies have been conflicting. Mack
and Gires showed that the possibilities for these discrepancies may
be due to different antibodies used, different cut-offs or
different technologies used, i.e. flow cytometry (30). Clay et al recently suggested
that it was unlikely that CD44+ cells were a pure population of
CSCs, and highlighted the need for its evaluation in combination
with another marker (31). This study
showed that CD44 could not be an important biomarker for stage I
and II OSCC.
ABCG2 expression was observed in 31.4% of OSCC
patients in this study, and our data indicates that ABCG2
expression is related with invasion mode and is not associated with
tumor size, differentiation, metastasis, and survival rate.
However, there were few reports associated with ABCG2 expression
and cancer cell invasion. On the other hand, it has been shown that
ABCG2 expression was associated with malignant transformation of
oral leukoplakia (OL), oral lichen planus (OLP), or oral
erythroplakia (OE) (17,32,33). ABCG2
expression was observed in 36 of 103 patients with untransformed OL
and 22 of 32 patients with malignant transformed OL (32). Additionally, ABCG2 expression was
detected in 21 and 35% untransformed OLP and OE patients,
respectively, and upon malignant transformation, expression rates
markedly increased to 69 and 88%, respectively (17,33).
Although additional experiments are needed to determine whether
ABCG2-positive cells are CSCs in oral potentially malignant
disorders, these patterns of ABCG2 expression may reveal its
potential as an early detection biomarker in precancerous
lesions.
CD24 expressions seemed to be implicated in tumor
cell proliferation, cell-cell interactions, adhesion, and decreased
E-cadherin expression (34,35). The relationship between CD24
expression and YK classification of OSCC observed in this study
might be caused by the decreased E-cadherin expression induced
through CD24 overexpression. In breast tumors, CD24 positive cancer
cells can be spread more rapidly (36). CD24 is also considered a potential
target for treatment, as previous studies showed that CD24-specific
antibodies can inhibit the growth of human colorectal and
pancreatic cancer cell lines (19,34). These
authors had suggested that the shift from the membranous CD24
localization to the cytoplasm found in well-differentiated tumors
could reflect the transition of epithelial cells to a more invasive
phenotype (19,34). However, our study did not reveal any
significant associations between CD24 expression and prognosis or
other clinicopathologic features, and our results are consistent
with other studies in OSCC (12,32).
BMI-1 expression was not associated with tumor size,
differentiation, invasion mode, or lymph node metastasis in this
study. High BMI-1 overexpression was connected to poor prognosis in
nasopharyngeal cancer, breast cancer and hepatocellular carcinoma
(16,18). In this study, BMI-1 expression in the
OSCC patients led to better prognosis, but lack of BMI-1 expression
was related with worse prognosis caused by distant metastasis. The
reason was thought that the Bmi-1 expression would be related with
distant metastasis of OSCC in this study. Several studies have
shown that high BMI-1 expression was associated with poor prognosis
(16,18). However, Pietersen et al also
reported a correlation between high expression of BMI-1 and better
outcome in OSCC patients (26). These
discrepancies may be due to the different types of epithelium in
the population groups, the type of cancers, the population
ethnicities, and differences in the underlying molecular
mechanisms.
The present results show that ALDH1 was
significantly associated with histological differentiation,
invasion mode and lymph node metastasis. Moreover, multivariate
analysis showed that ALDH1 expression was the only prognostic
factor for disease-free survival rate. Overexpression of ALDH1
leads to increased cell proliferation and, notably, to increased
resistance to chemotherapeutic agents (32). Several studies have reported an
association between ALDH1-positive tumors and poor clinical
prognosis in breast, lung, pancreatic, and prostate cancer
(37). In this study, ALDH1
expression was observed in 25.7% of OSCC patients, which is similar
as the ALDH1 expression rate compared with other cancers (37–39).
We also found that increased ALDH1 expression correlated with poor
disease-free survival of OSCC patients. However, contrasting
results have also been reported. For instance, Chang et al
reported that ALDH1 expression correlated with favorable prognosis
in a group of ovarian cancer patients, which included 266 serous
ovarian cancer patients and 176 non-serous ovarian cancer patients
(38). In addition, Dimou et
al reported that non-small cell lung cancer patients with high
expression of ALDH1 had longer survival and lower recurrence rates
(39). Thus, more prospective studies
are needed to draw a definite conclusion. CSCs have major phenotype
and functional heterogeneities, which may help distinguish them
from cancer cells and may be of potential benefit in the
development of anticancer therapies to improve clinical outcomes.
Therefore, the present study supports the idea that ALDH1 could be
a CSC marker, because of the significant correlation between
ALDH1-positive OSCC patients and common clinical parameters, such
as histological differentiation, invasion mode (YK classification),
metastasis, and survival rate. The present findings suggested that
ALDH1 positively in OSCC were likely to correlate with the number
of cells undergoing epithelial mesenchymal transition and a process
for the formation of metastasis.
We evaluated 68 biopsy samples and 2 surgery
samples. However, biopsy tissues might not reflect the whole part
of tumors. The present findings of this study might not be the
results of CSC marker expression of the whole tumors. We should
need to investigate the confirmation of this study.
In conclusion, our study indicated that the
expression of ALDH1 could be an effective CSC marker to indicate
the outcome of early stage OSCC patients.
Acknowledgements
Not applicable.
Funding
This study was supported in JSPS KAKENHI (grant no.
15K11294).
Availability of data and materials
The datasets analyzed during the current study are
available from the corresponding author on reasonable request.
Authors' contributions
NT, GO, KA, and TN analyzed and interpreted the
patient data. TT and YM performed the histological examination and
TT was a major contributor in writing the manuscript. All authors
read and approved the final manuscript.
Ethics approval and consent
This study was approved by the Ethics Committee of
Tokushima University Hospital (approval no. 2516).
Consent for publication
Consent was obtained from all patients for the
publication of their data.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Mack B and Gires O: CD44s and CD44v6
expression in head and neck epithelia. PLoS One. 3:e33602008.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Yoshida Y, Sato K, Kin M, Suzuki T, Bessho
H, Tanaka Y and Katakura: Relative factors of late cervical lymph
node metastasis in patients with stage I or II oral squamous cell
carcinoma. J oral Maxillo Surg Med Pathol. 28:156–161. 2016.
View Article : Google Scholar
|
|
3
|
Okudela K, Woo T, Mitsui H, Tajiri M,
Masuda M and Ohashi K: Expression of the potential cancer stem cell
markers, CD133, CD44, ALDH1 and β-catenin, in primary lung
adenocarcinoma-their prognostic significance. Pathol Int.
62:792–801. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hirata K, Suzuki H, Imaeda H, Matsuzaki J,
Tsugawa H, Nagano O, Asakura K, Saya H and Hibi T: CD44 variant 9
expression in primary early gastric cancer as a predictive marker
for recurrence. Br J Cancer. 109:379–386. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kimura Y, Goi T, Nakazawa T, Hirono Y,
Katayama K, Urano T and Yamaguchi A: CD44variant exon 9 plays an
important role in colon cancer initiating cells. Oncotarget.
4:785–791. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Go SI, Ko GH, Lee WS, Kim RB, Lee JH,
Jeong SH, Lee YJ, Hong SC and Ha WS: CD44 Variant 9 serves as a
poor prognostic marker in early gastric cancer, but not in advanced
gastric cancer. Cancer Res Treat. 48:142–152. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Robey RW, To KK, Polgar O, Dohse M, Fetsch
P, Dean M and Bates SE: ABCG2: A perspective. Adv Drug Deliv Rev.
61:3–13. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bhagwandin VJ, Bishop JM, Wright WE and
Shay JW: The Metastatic potential and chemoresistance of human
pancreatic cancer stem cells. PLoS One. 11:e01488072016. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Tang Y, Hou J, Li G, Song Z, Li X, Yang C,
Liu W, Hu Y and Xu Y: ABCG2 regulates the pattern of self-renewing
divisions in cisplatin-resistant non-small cell lung cancer cell
lines. Oncol Rep. 32:2168–2174. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hoe SL, Tan LP, Jamal J, Peh SC, Ng CC,
Zhang WC, Ahmad M and Khoo AS: Evaluation of stem-like side
population cells in a recurrent nasopharyngeal carcinoma cell line.
Cancer Cell Int. 14:1012014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Sano A, Kato H, Sakurai S, Sakai M, Tanaka
N, Inose T, Saito K, Sohda M, Nakajima M, Nakajima T and Kuwano H:
CD24 expression is a novel prognostic factor in esophageal squamous
cell carcinoma. Ann Surg Oncol. 16:506–514. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Oliveira LR, Oliveira-Costa JP, Araujo IM,
Soave DF, Zanetti JS, Soares FA, Zucoloto S and Ribeiro-Silva A:
Cancer stem cell immunophenotypes in oral squamous cell carcinoma.
J Oral Pathol Med. 40:135–142. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kristiansen G, Winzer KJ, Mayordomo E,
Bellach J, Schlüns K, Denkert C, Dahl E, Pilarsky C, Altevogt P,
Guski H and Dietel M: CD24 expression is a new prognostic marker in
breast cancer. Clin Cancer Res. 9:4906–4913. 2003.PubMed/NCBI
|
|
14
|
Karahan N, Güney M, Oral B, Kapucuoglu N
and Mungan T: CD24 expression is a poor prognostic marker in
endometrial carcinoma. Eur J Gynaecol Oncol. 27:500–504.
2006.PubMed/NCBI
|
|
15
|
Sagiv E, Starr A, Rozovski U, Khosravi R,
Altevogt P, Wang T and Arber N: Targeting CD24 for treatment of
colorectal and pancreatic cancer by monoclonal antibodies or small
interfering RNA. Cancer Res. 68:2803–2812. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Choy B, Bandla S, Xia Y, Tan D, Pennathur
A, Luketich JD, Godfrey TE, Peters JH, Sun J and Zhou Z:
Clinicopathologic characteristics of high expression of Bmi-1 in
esophageal adenocarcinoma and squamous cell carcinoma. BMC
Gastroenterol. 12:1462012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Feng JQ, Mi JG, Wu L, Ma LW, Shi LJ, Yang
X, Liu W, Zhang CP and Zhou ZT: Expression of podoplanin and ABCG2
in oral erythroplakia correlate with oral cancer development. Oral
Oncol. 48:848–852. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Allegra E, Caltabiano R, Amorosi A,
Vasquez E, Garozzo A and Puzzo L: Expression of BMI1 and p16 in
laryngeal squamous cell carcinoma. Head Neck. 35:847–851. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Goossens-Beumer IJ, Zeestraten EC, Benard
A, Christen T, Reimers MS, Keijzer R, Sier CF, Liefers GJ, Morreau
H, Putter H, et al: Clinical prognostic value of combined analysis
of Aldh1, Survivin and EpCAM expression in colorectal cancer. Br J
Cancer. 110:2935–2944. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kahlert C, Bergmann F, Beck J, Welsch T,
Mogler C, Herpel E, Dutta S, Niemietz T, Koch M and Weitz J: Low
expression of aldehyde dehydrogenase 1A1 (ALDH1A1) is a prognostic
marker for poor survival in pancreatic cancer. BMC Cancer.
11:2752011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Luo WR, Gao F, Li SY and Yao KT: Tumour
budding and the expression of cancer stem cell marker aldehyde
dehydrogenase 1 in nasopharyngeal carcinoma. Histopathology.
61:1072–1081. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Patel M, Lu L, Zander DS, Sreerama L, Coco
D and Moreb JS: ALDH1A1 and ALDH3A1 expression in lung cancers:
Correlation with histologic type and potential precursors. Lung
Cancer. 59:340–349. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Jakobsson PA, Eneroth CM, Killander D,
Moberger G and Mårtensson B: Histologic classification and grading
of malignancy in carcinoma of the larynx. Acta Radiol Ther Phys
Biol. 12:1–8. 1973. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Willén R, Nathanson A, Moberger G and
Anneroth G: Squamous cell carcinoma of the gingiva. Histological
classification and grading of malignancy. Acta Otolaryngol.
79:146–154. 1975. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Yamamoto E, Miyakawa A and Kohama G: Mode
of invasion and lymph node metastasis in squamous cell carcinoma of
the oral cavity. Head Neck Surg. 6:938–947. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Prince ME, Sivanandan R, Kaczorowski A,
Wolf GT, Kaplan MJ, Dalerba P, Weissman IL, Clarke MF and Ailles
LE: Identification of a subpopulation of cells with cancer stem
cell properties in head and neck squamous cell carcinoma. Proc Natl
Acad Sci USA. 104:973–978. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sato S, Miyauchi M, Takekoshi T, Zhao M,
Kudo Y, Ogawa I, Kitagawa S, Fujita M and Takata T: Reduced
expression of CD44 variant 9 is related to lymph node metastasis
and poor survival in squamous cell carcinoma of tongue. Oral Oncol.
36:545–549. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kokko LL, Hurme S, Maula SM, Alanen K,
Grénman R, Kinnunen I and Ventelä S: Significance of site-specific
prognosis of cancer stem cell marker CD44 in head and neck
squamous-cell carcinoma. Oral Oncol. 47:510–516. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Huang CF, Xu XR, Wu TF, Sun ZJ and Zhang
WF: Correlation of ALDH1, CD44, OCT4 and SOX2 in tongue squamous
cell carcinoma and their association with disease progression and
prognosis. J Oral Pathol Med. 43:492–498. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Mack B and Gires O: CD44s and CD44v6
expression in head and neck epithelia. PLoS One. 3:e33602008.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Clay MR, Tabor M, Owen JH, Carey TE,
Bradford CR, Wolf GT, Wicha MS and Prince ME: Single-marker
identification of head and neck squamous cell carcinoma cancer stem
cells with aldehyde dehydrogenase. Head Neck. 32:1195–1201. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Liu W, Feng JQ, Shen XM, Wang HY, Liu Y
and Zhou ZT: Two stem cell markers, ATP-binding cassette, G2
subfamily (ABCG2) and BMI-1, predict the transformation of oral
leukoplakia to cancer: A long-term follow-up study. Cancer.
118:1693–1700. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Shi P, Liu W, Zhou ZT, He QB and Jiang WW:
Podoplanin and ABCG2: Malignant transformation risk markers for
oral lichen planus. Cancer Epidemiol Biomarkers Prev. 19:844–849.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Choi D, Lee HW, Hur KY, Kim JJ, Park GS,
Jang SH, Song YS, Jang KS and Paik SS: Cancer stem cell markers
CD133 and CD24 correlate with invasiveness and differentiation in
colorectal adenocarcinoma. World J Gastroenterol. 15:2258–2264.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Tanaka T, Terai Y, Kogata Y, Ashihara K,
Maeda K, Fujiwara S, Yoo S, Tanaka Y, Tsunetoh S, Sasaki H, et al:
CD24 expression as a marker for predicting clinical outcome and
invasive activity in uterine cervical cancer. Oncol Rep.
34:2282–2228. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Li X, Kong X, Huo Q, Guo H, Yan S, Yuan C,
Moran MS, Shao C and Yang Q: Metadherin enhances the invasiveness
of breast cancer cells by inducing epithelial to mesenchymal
transition. Cancer Sci. 102:1151–1157. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Wakamatsu Y, Sakamoto N, Oo HZ, Naito Y,
Uraoka N, Anami K, Sentani K, Oue N and Yasui W: Expression of
cancer stem cell markers ALDH1, CD44 and CD133 in primary tumor and
lymph node metastasis of gastric cancer. Pathol Int. 62:112–119.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Chang B, Liu G, Xue F, Rosen DG, Xiao L,
Wang X and Liu J: ALDH1 expression correlates with favorable
prognosis in ovarian cancers. Mod Pathol. 22:817–823. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Dimou A, Neumeister V, Agarwal S,
Anagnostou V, Syrigos K and Rimm DL: Measurement of aldehyde
dehydrogenase 1 expression defines a group with better prognosis in
patients with non-small cell lung cancer. Am J Pathol.
181:1436–1442. 2012. View Article : Google Scholar : PubMed/NCBI
|