Introduction
Renal cell carcinoma (RCC), accounts for 2–3% of all
malignancies in adults and is the most lethal type of urological
cancer, with ~63,990 new cases and ~14,400 RCC-associated
mortalities estimated for 2017 in the United States (1). Clear cell renal cell carcinoma (ccRCC)
constitutes 70–80% cases RCC and is the most common and most
aggressive histological RCC subtype (2). Approximately 30% of patients with RCC
present with locally advanced or metastatic disease at the time of
diagnosis, and 30% of patients who undergo surgical resection for
local disease experience recurrence (2). While patients with localized disease
have a 5-year survival rate of 91.7%, patients with metastatic
disease have a 5-year survival rate of 12.3%, according to the
Surveillance, Epidemiology and End Results Program database
(3). Currently, RCC is treatment is
limited by the difficulty of early diagnosis and the lack of
reliable specific diagnostic biomarkers.
Changes at the cellular and subcellular level,
involving DNA, RNA, and protein structure and function, are
initiating factors of cancer development and progression (4). MicroRNAs (miRNAs), a class of non-coding
RNAs of ~22 nucleotides in length, have been demonstrated to serve
roles in cancer initiation and progression, primarily through
interaction with the 3′-untranslated region (3′-UTR) of target
mRNA. This causes posttranscriptional inhibition and mRNA
degradation (5). Specific
miRNA-expression profiles have been established for a number of
types of cancer, including RCC (6,7). Certain
miRNAs released from tumor cells are chemically stable and can be
detected in a broad range of body fluids (8–11).
Therefore, miRNAs have potential to serve as biomarkers for RCC
diagnosis.
A previous study by this group identified 74 miRNAs
that were dysregulated in ccRCC tissues compared with normal
tissues, of which 44 were significantly downregulated in ccRCC and
30 were upregulated (12). Among the
differentially expressed miRNAs in ccRCC, miR-141 and miR-200c were
the most significantly downregulated (≤104- and ≤100-fold,
respectively), whereas miR-210 and miR-224 were the most
upregulated (≤22- and ≤14-fold, respectively). Previous studies
have reported fold changes in miR-141, miR-210 and miR-224
expression in ccRCC vs. normal tissue of 7–100, 3–22 and 4–14,
respectively (13–19). The variability among these fold
changes may be caused by differing construction of microarray
platforms, variability among samples, experimental conditions or
normalization technique. It has been demonstrated that the
expression of miR-141, but not miR-200c, yielded high accuracy in
discriminating ccRCC from normal tissues (12,20).
Therefore, miR-141, miR-210 and miR-224 were selected for further
analysis in the present study.
Materials and methods
Patient samples
Paired cancerous and non-cancerous tissues were
obtained from 78 patients with kidney tumors, including 68 cases of
ccRCC (median age, 55±13 years; range, 22–81 years; 36 males and 32
females), 2 cases of chromophobe RCC, 1 case of sarcoma RCC and 7
cases of renal angiomyolipoma, between October 2008 and December
2013 at the Department of Urology, Union Hospital, Tongji Medical
College (Wuhan, China). The samples were freshly frozen in liquid
nitrogen and stored at −80°C until required for RNA extraction.
Fasting EDTA blood samples were collected from 66 patients (median
age: 56±12 years; range, 26–81 years; 39 males and 27 females) with
ccRCC prior to radical nephrectomy or nephron-sparing surgery and 7
days post-surgery, between November 2011 and January 2015 at Union
Hospital (Wuhan, China). Blood samples were also collected from 67
age-matched healthy controls. Blood was processed within 1 h of
collection by centrifugation at 820 × g at 4°C for 10 min. The
plasma was then transferred to a fresh RNase/DNase-free Eppendorf
tube, followed by further centrifugation at 16,000 × g at 4°C for
10 min. The supernatant was transferred to fresh RNase/DNase-free
tubes and stored at −80°C. Samples exhibiting evidence of hemolysis
were excluded. The clinicopathological information was collected
patient records and are presented in Table I. The tumors were classified according
to the 2009 Tumor-Node-Metastasis system (21), the 2004 World Health Organization
classification (22), and Fuhrman
grading system using the characteristics of the nuclei and nucleoli
of tumor cells (23). The tissue- and
blood plasma-based studies were approved by the Clinical Research
Ethics Committee of Wuhan Union Hospital (Wuhan, China) and the
Institutional Review Board of Huazhong University of Science and
Technology (Wuhan, China), in accordance with the Declaration of
Helsinki. Informed consent was obtained from all participants prior
to tissue and blood collection.
 | Table I.Patient characterization. |
Table I.
Patient characterization.
|
| Number (% all
participants) |
|---|
|
|
|
|---|
| Characteristic | Microarray | Tissues collected
for RT-qPCR | Plasma collected
for RT-qPCR |
|---|
| Age |
|
|
|
| Mean ±
SEM (years) | 58±17 | 55±13 | 56±12 |
| Sex |
|
|
|
|
Male/Female | 3/2 | 36/32 | 39/27 |
| Tumor size |
|
|
|
| Mean ±
SEM (cm) | 4.7±1.6 | 6.1±2.4 | 5.9±2.6 |
| T stage |
|
|
|
|
pT1a | 2 (40.0) | 10 (14.7) | 15 (22.3) |
|
pT1b | 3 (60.0) | 37 (54.4) | 34 (51.5) |
|
pT2a | 0 (0) | 13 (19.1) | 10 (15.2) |
|
pT2b | 0 (0) | 4 (5.9) | 5 (7.6) |
|
pT3 | 0 (0) | 1 (1.5) | 2 (3.0) |
|
pT4 | 0 (0) | 0 (0) | 0 (0) |
|
Missing | 0 (0) | 3 (4.4) | 0 (0) |
| N stage |
|
|
|
| N0 | 5 | 63 (92.6) | 62 (93.9) |
| N1 | 0 (0) | 2 (2.9) | 4 (6.1) |
|
Missing | 0 (0) | 3 (4.4) | 0 (0) |
| M stage |
|
|
|
| M0 | 5 | 64 (94.1) | 66 (100.0) |
| M1 | 0 (0) | 1 (1.5) | 0 (0) |
|
Missing | 0 (0) | 3 (4.4) | 0 (0) |
| Fuhrman grade |
|
|
|
| 1 | 4 (80.0) | 16 (23.5) | 11 (16.7) |
| 2 | 1 (20.0) | 31 (45.6) | 33 (50.0) |
| 3 | 0 (0) | 16 (23.5) | 20 (30.3) |
| 4 | 0 (0) | 3 (4.4) | 2 (3.0) |
|
Missing | 0 (0) | 2 (2.9) | 0 (0) |
RNA extraction
Total RNA was extracted from tissues using TRIzol
(Thermo Fisher Scientific, Inc., Waltham, MA, USA), according to
the manufacturer's instructions. Total RNA was extracted from
plasma using TRI Reagent BD (Molecular Research Center, Inc.,
Cincinnati, USA), according to the manufacturer's protocol with
minor modifications: A total of 200 µl plasma was thawed on ice and
added to 750 µl TRI Reagent BD supplemented with 20 µl acetic acid
(5 mol/l). A total of 25 fmol synthetic cel-miR-39 (Qiagen, Hilden,
Germany) was added prior to chloroform extraction, and RNA was
precipitated at −20°C overnight using isopropanol. RNA was
resuspended in 15 µl RNase-free water, and the quantification and
RNA-quality determination was determined using a Nanodrop 2000c
spectrophotometer (Thermo Fisher Scientific, Inc.). All samples
were stored at −80°C until further analysis.
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
Reverse transcription of 500 ng tissue RNA or 4 µl
plasma RNA was performed using a RevertAid™ First Strand cDNA
Synthesis kit (Fermentas; Thermo Fisher Scientific, Inc.) and a
reverse transcript primer from Guangzhou RiboBio Co., Ltd.
(Guangzhou, China). RT-qPCR analysis was performed using Platinum
SYBR Green qPCR Supermix UDG (Invitrogen; Thermo Fisher Scientific,
Inc.) using primers synthesized at Guangzhou RiboBio Co., Ltd.
(Guangzhou, China). Mature miRNAs were detected using a
LightCycler® 480 II (Roche Diagnostics, Basel,
Switzerland). The amplification conditions were as follows: 10 min
at 95°C, followed by 45 cycles of 10 sec at 95°C, 20 sec at 60°C
and 1 sec at 72°C. Tissue or plasma samples were normalized to U6
or cel-miR-39, respectively. Relative miRNA expression was
calculated using the 2−ΔΔCq method (24).
Statistical analysis
All data are expressed as the mean ± standard error
of the mean, and all experiments were performed ≥3 times
independently. Student's t-test, one-way ANOVA followed by the
Least-Significant-Difference test, Mann-Whitney test, receiver
operating characteristic (ROC) and Pearson's correlation
coefficient analyses were performed using GraphPad Prism v.6
(GraphPad Software, Inc., La Jolla, CA, USA). Correlation of
miR-141, miR-210 and miR-224 expression was assessed using
Pearson's correlation coefficient. Fisher r-to-z transformation was
used to decide whether 2 correlations were different. ROC curves
were constructed by plotting sensitivity vs. [100%-specificity
(%)]. P<0.05 was considered to indicate a statistically
significant difference.
Results
miRNA expression levels in RCC
tissues
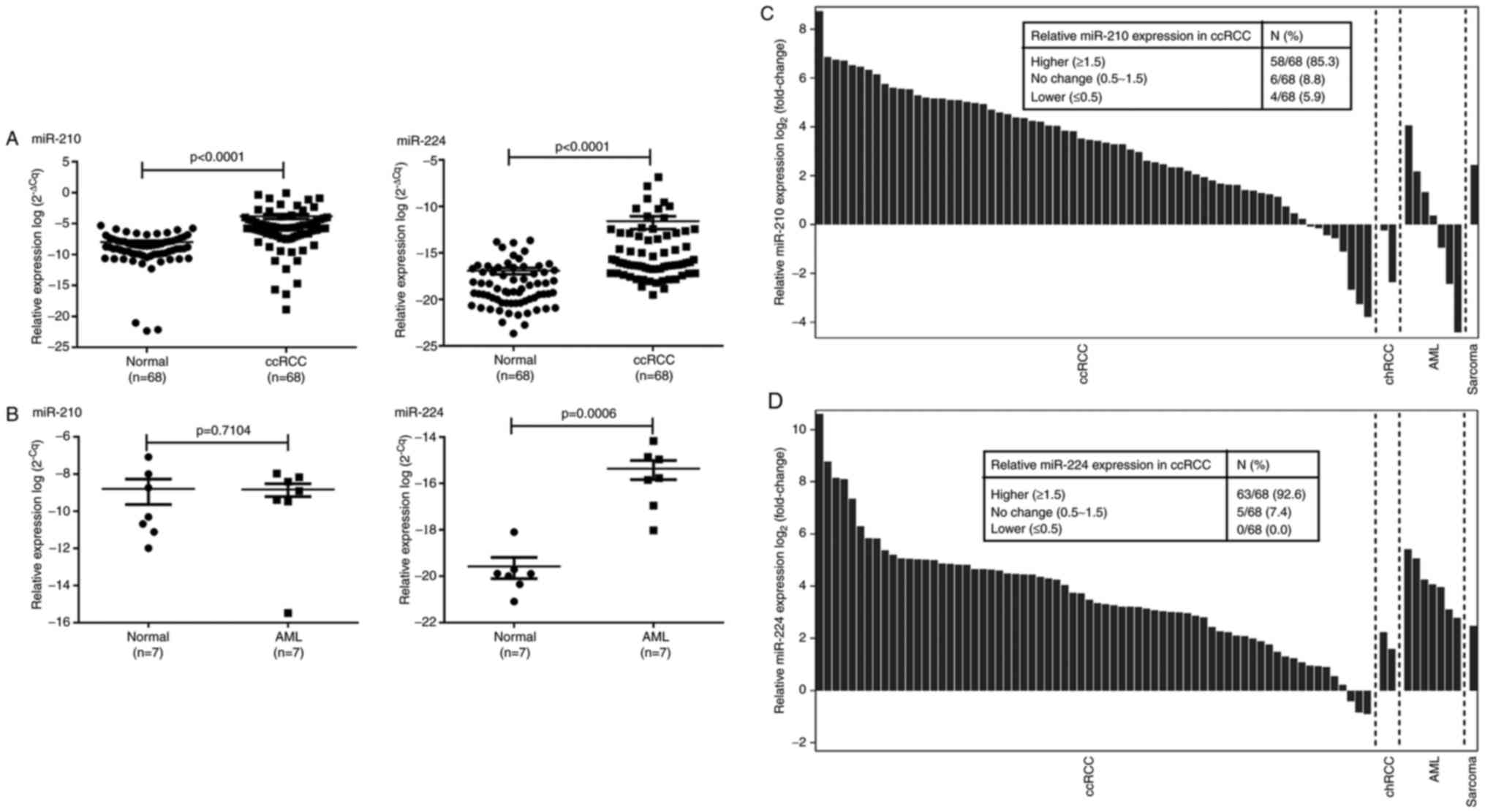
miR-141, miR-210 and miR-224 expression levels were
analyzed in a cohort of 78 patients with renal tumors, including 68
ccRCCs, 2 chromophobe RCCs (chRCCs), 1 sarcoma RCC and 7 renal
angiomyolipomas (AMLs). In accordance with the microarray results,
miR-210 and miR-224 were significantly upregulated in 83.8% (57/68)
and 88.2% (60/68) ccRCC tissues, respectively (P<0.0001;
Fig. 1A and B). miR-210 expression
was decreased in chRCC but markedly increased in sarcoma RCC,
whereas miR-224 expression was significantly increased in both RCC
subtypes (Fig. 1C). Furthermore,
miR-224 overexpression in AML was noted, but there was no
difference in miR-210 expression between AML and normal tissues
(Fig. 1D). Unexpectedly, miR-210 and
miR-224 expression levels in ccRCC were not demonstrated to be
associated with tumor size and stage. However, miR-210 was
significantly associated with tumor grade (P=0.0414, data not
shown).
Tissue miR224/141 as a
robust diagnostic biomarker in ccRCC
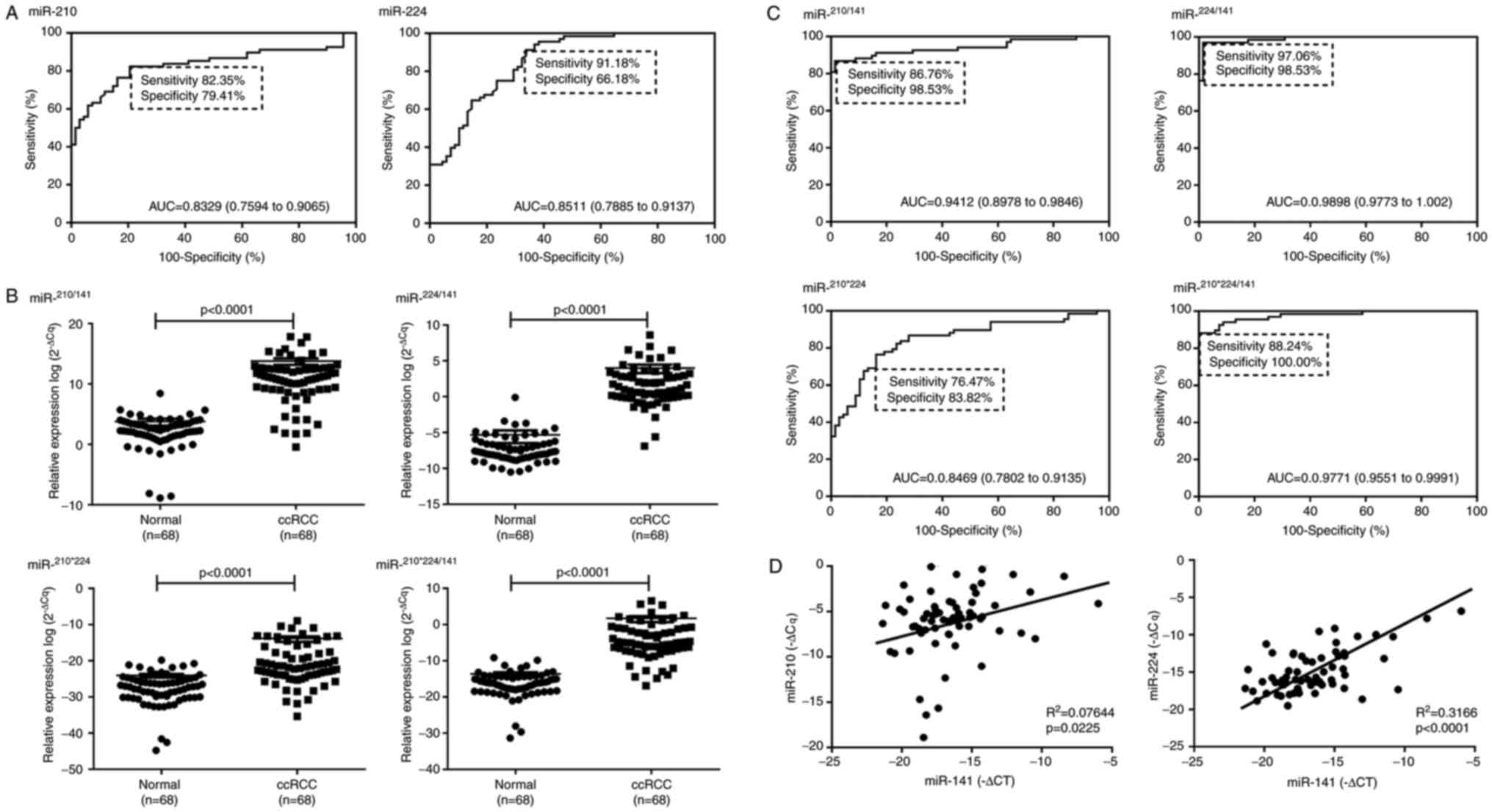
To evaluate the discrimination value of miR-210 and
miR-224 expression levels in ccRCC, receiver operating
characteristic (ROC) analysis was performed. This revealed that the
miR-210/miR-224 ratio served as a useful biomarker for
discriminating ccRCC from normal tissues, with an AUC of 0.8329
(95% confidence intervals (CI), 0.7594–0.9065; P<0.0001) and
0.8511 (95% CI, 0.7885–0.9137; P<0.0001), respectively (Fig. 2A). At a threshold of 0.005373 for
relative miR-210 expression, the sensitivity was 82.35% and the
specificity was 79.41% (Fig. 2A). At
a threshold of 0.00000413 for relative miR-224 expression, the
sensitivity and specificity were 91.18 and 66.18%, respectively
(Fig. 2A). The accuracy of miR-210
and miR-224 in differentiating ccRCC from normal tissues was lower
than that of miR-141 (AUC=0.93) (11).
Subsequently, it was investigated whether the
considering the expression of miR-141, miR-210 and miR-224
together, would provide a more accurate prediction ccRCC diagnosis.
Considering the downregulation of miR-141 expression and
upregulation of miR-210 and miR-224 expression in ccRCC tissues,
the ratio of miR-210/miR-141 (miR210/141),
miR-224/miR-141 (miR224/141), miR-210× miR-224
(miR210×224) and (miR-210× miR-224)/miR-141
(miR(210×224)/141) were analyzed in ccRCC tissues. As
demonstrated in Fig. 2B,
miR210/141, miR224/141, miR210×224
and miR(210×224)/141 were increased in ccRCC tissues
(P<0.0001, Mann-Whitney). ROC curve analyses demonstrated that
the diagnostic accuracy of miR210/141,
miR224/141 and miR(210×224)/141 with AUCs of
0.9412, 0.9898 and 0.9771, respectively, were increased compared
with that of miR-141 (AUC=0.93). However, the diagnostic accuracy
of miR210×224 with AUC of 0.8469 was lower than that of
miR-141 (Fig. 2C). Notably,
miR224/141 demonstrated the highest accuracy with a
sensitivity of 97.06% and a specificity of 98.53% at a threshold of
0.1148 for ccRCC tissues (Fig. 2C).
These findings promoted an investigation of the association between
miR-141, miR-210 and miR-224 expression in ccRCC tissues by
Pearson's correlation analysis. As demonstrated in Fig. 2D, miR-141 was positively correlated
with miR-210 (r=0.2765; 95% CI, 0.04067–0.4831;
R2=0.07644; P<0.05) and miR-224 (r=0.5627; 95%
CI, 0.3744–0.7064, R2=0.3166; P<0.0001) expression.
There was a significant difference between the 2 correlation
coefficients (P=0.044), according to the Fisher
r-to-z transformation test. Overall, these results
suggest that the tissue miR224/141 may be used as a
robust diagnostic biomarker for ccRCC.
Plasma miR-210, miR-224 and miR-210×
miR-224 are not clinically useful biomarkers in ccRCC
Given that a tumor can release miRNAs into the blood
(25), we hypothesized that the high
expression of miR-210 and miR-224 and the low expression of miR-141
in ccRCC tissues would affect their levels in the blood of ccRCC
patients. Considering the lower amount of circulating miRNAs in
serum compared with plasma and the variable range of miRNAs from
different patient samples (26), the
expression levels of plasma miR-210, miR-224 and miR-141 were
analyzed in paired pre- and post-operative blood samples from 66
ccRCC patients and 67 healthy controls.
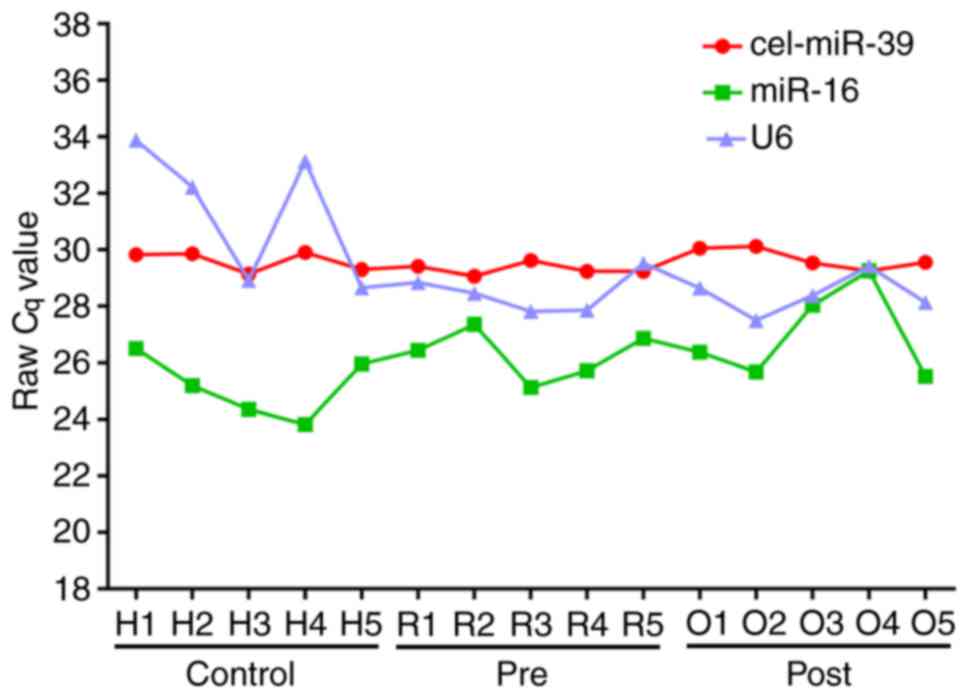
To determine an appropriate endogenous control for
quantification of plasma miRNA, the expression of miR-16, U6 and
cel-miR-39 were analyzed by RT-qPCR in 15 plasma samples (5
pre-operative ccRCCs, 5 post-operative ccRCCs and 5 healthy
controls). The results indicated that the expression of cel-miR-39
was highly consistent between samples (mean Cq=29.54; standard
deviation, 0.34; Fig. 3). However,
the expression of miR-16 and U6 appeared to be unstable (mean
Cq=26.15 and 29.43, SD=1.39 and 2.00, respectively) (Fig. 3). Thus, cel-miR-39 was used as a
normalizing control for RT-qPCR.
RT-qPCR analysis revealed that the Cq values of
miR-141 in the majority of ccRCC patients and healthy control
samples were >40, suggesting that plasma miR-141 expression was
extremely low (data not shown), which is consistent with previous
studies (9,27,28).
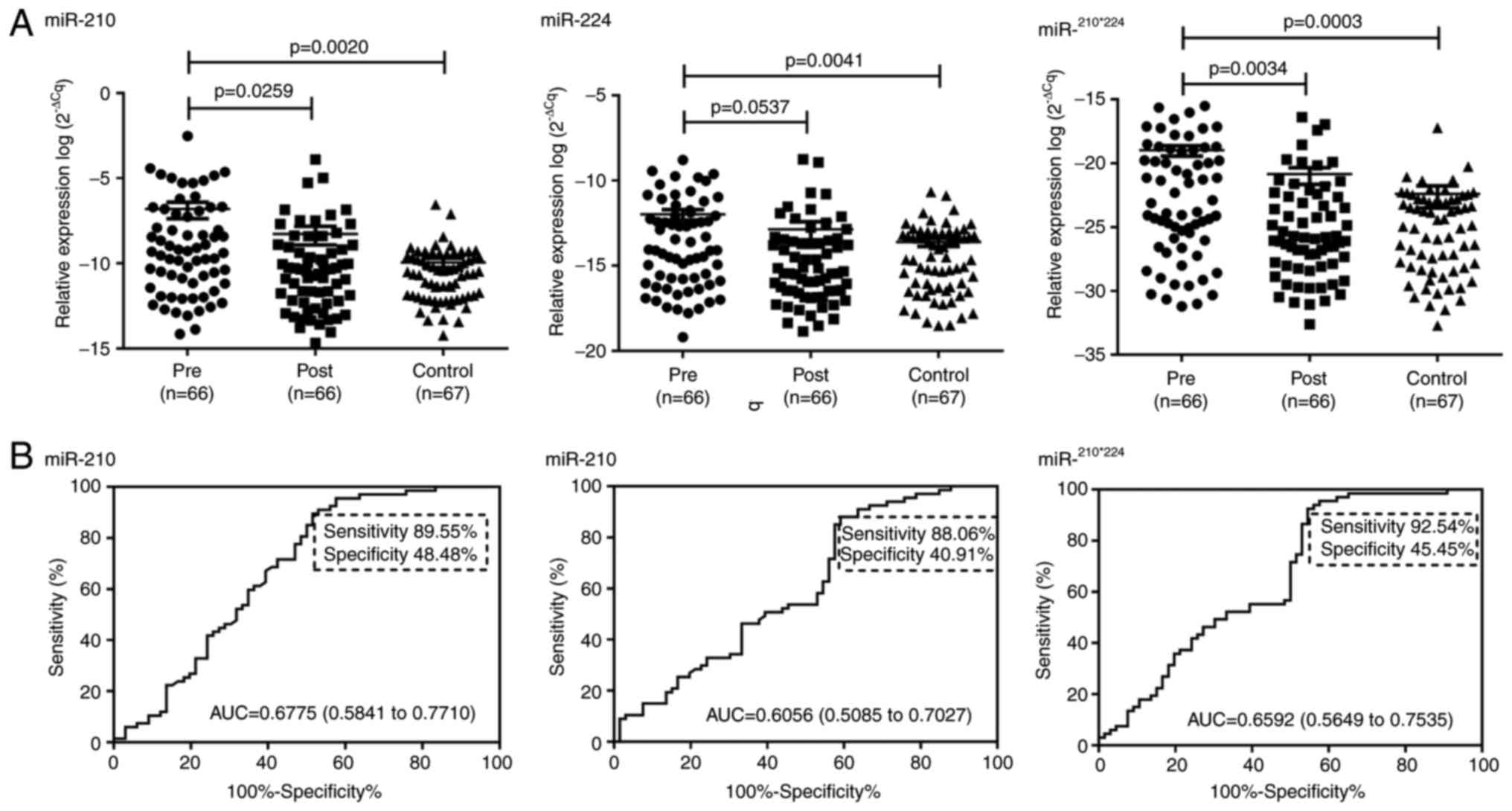
Expression levels of plasma miR-210 and miR-224 in patients with
ccRCC were significantly increased compared with healthy controls
(P<0.05; Fig. 4A). Furthermore,
plasma miR-210 expression was significantly reduced postoperatively
in patients with ccRCC (P<0.05, Fig.
4A). ROC curve analysis revealed that the AUCs for plasma
miR-210 and miR-224 in differentiating ccRCC patients from healthy
controls were 0.6775 and 0.6056, respectively (Fig. 4B). The optimal sensitivity and
specificity of plasma miR-210 was 89.55 and 48.48%, respectively
(Fig. 4B). The optimal sensitivity
and specificity of plasma miR-224 was 88.06 and 40.91%,
respectively (Fig. 4B). These
specificity values are too low for clinical utility.
Next, it was determined whether the combination of
plasma miR-210 and miR-224 levels could differentiate ccRCC
patients from healthy controls. As demonstrated in Fig. 4A, plasma miR210×224 was
downregulated in postoperative samples from ccRCC patients and
healthy controls, compared with preoperative samples. However, the
AUC, and optimal sensitivity and specificity for plasma
miR210×224 were 0.6592, 92.54 and 45.45%, respectively,
which were not much different from those for plasma miR-210 and
miR-224 alone (Fig. 4B). Plasma
miR-210 and miR-224 expression, and miR210×224, were not
associated with tumor stage, grade or size. These results indicate
that plasma miR-210, miR-224 and miR210×224 may not be
clinically useful biomarkers for ccRCC.
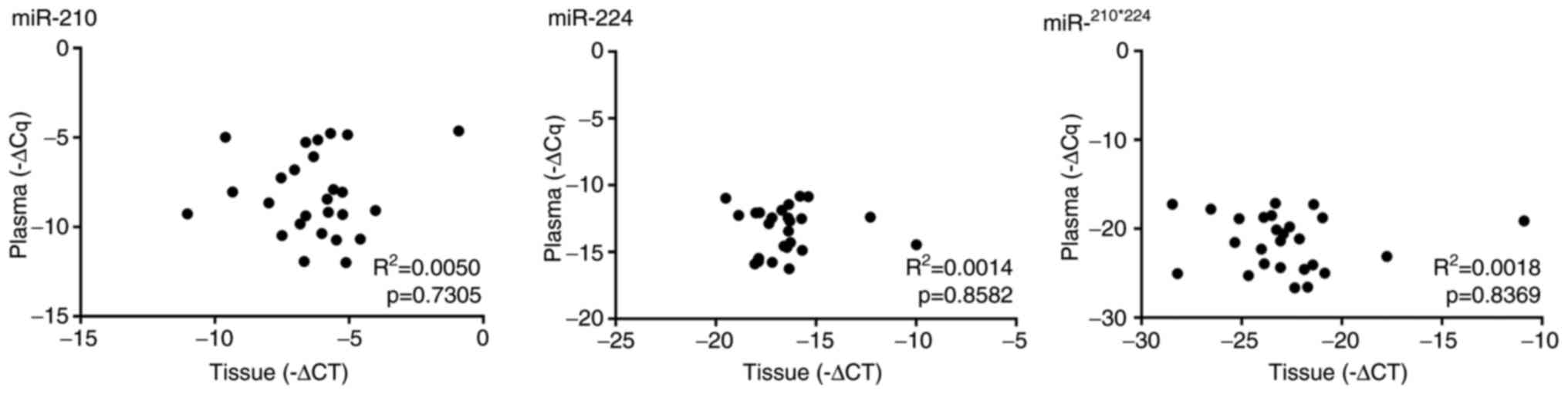
Association between tissue and plasma
miRNA expression
The association between tissue and plasma miR-210,
miR-224 and miR210×224 in 26 ccRCC patients was analysed
using Pearson's correlation coefficient. As indicated by Fig. 5, miR-210, miR-224 and
miR210×224 levels in tumor tissue were not positively
correlated with those in the plasma (miR-210, P=0.7305; miR-224,
P=0.8582, and miR210×224, P=0.8369).
Discussion
DNA, RNA, miRNA and protein are essential in the
routine diagnostic panels for various types of cancer (29). miRNAs are small, noncoding, endogenous
single-stranded RNAs that critically regulate human cancer
development and progression (30).
Altered miRNA expression has been implicated in the pathobiology of
various types of cancer and function as diagnostic markers and
potential therapeutic targets (29,30). The
identification of reliable diagnostic biomarkers remains a major
challenge in cancer research, particularly for RCC (31). Based on previous studies of miRNA
expression in RCC, we selected miR-210, miR-224 and miR-141 for
investigation as potential biomarkers in the present study. It was
demonstrated that miR224/141 had a high accuracy in
predicting the diagnosis of ccRCC (AUC=0.9898). However, plasma
miR-210, miR-224 and miR210×224 demonstrated poor
specificity and relatively low accuracy in the diagnosis of ccRCC.
Furthermore, no positive correlation between tissue and plasma
miR-210 and miR-224 expression, or miR210×224 was
observed.
miRNA can be used to distinguish normal from
malignant tissues. In consistence with Jung's reports (14,32), our
previous study demonstrated that miR-141 could discriminate ccRCC
tissues from normal kidney tissues with 93% accuracy (12). Combined miR-141 downregulation and
miR-155 upregulation demonstrated 97% accuracy for identification
of ccRCC (14). Fridman et al
(33) defined a two-step
decision-tree classifier that considered the expression levels of 6
miRNAs: The first step used the expression levels of miR-210 and
miR-221 to distinguish between the two pairs of subtypes; the
second step used miR-200c and miR-139-5p to identify oncocytoma
from chRCC. The ccRCC identification sensitivity of the classifier
was 94% (33). Another study devised
a stepwise decision tree to distinguish between normal tissue and
each of the RCC subtypes in a ≤4 steps based on miRNA microarray
analysis (34). The system had a
sensitivity of 97% for distinguishing normal tissue from RCC, and
100% for distinguishing the ccRCC subtype. In the present study it
was demonstrated that miR-210 or miR-224 expression alone yielded
83 and 85% accuracy in discriminating ccRCC tissues from normal
kidney tissues, respectively. Importantly, it was established that
the miR-224/miR-141 ratio is a highly accurate diagnostic biomarker
for ccRCC (AUC=0.9773–1.0002). The expression of miR-224 was not
statistically different between ccRCC and AML, suggesting that it
may not be a specific biomarker for ccRCC. Further studies are
required to validate the expression of miR-210, miR-224 and miR-141
in RCC, using more AML samples.
The concept of miRNA ratios is relatively novel
(35,36), and the prognostic or diagnostic
potentials of miRNA combinations have been suggested by multiple
researchers (14,33,34). Using
this type of ratio as biomarker has many advantages, including
elimination of the requirement for an internal reference,
improvement in discrimination accuracy and specificity, reduced
risk of risk of undetected malignant events, and consideration of
intra-tumor genetic heterogeneity of RCC where various molecules
may be altered by different mechanisms at different foci (35,36). These
characteristics make miRNA ratio biomarkers more attractive in a
clinical setting. In the present study, tissue
miR224/141 was demonstrated to have diagnostic
significance in ccRCC patients. To the best of our knowledge, this
is the first research to investigate a miR-224 and miR-141
combination ratio.
There is limited data available regarding
circulating miRNAs as diagnostic biomarkers of RCC. Wulfken et
al (37) reported that miR-1233
was upregulated in RCC tissue and serum, and that serum miR-1233
could detect RCC with 77.4% sensitivity but only 37.6% specificity.
Redova et al (38)
demonstrated that serum miR-378 and miR-451 were downregulated and
upregulated in patients with RCC, respectively. Serum miR-378,
miR-451 and combination of the two miRNAs served as potential
biomarkers for discriminating patients with RCC from healthy
controls with an AUC of 0.71, 0.77, and 0.86, respectively
(39). Contrasting results were
reported by Hauser et al (39), which demonstrated that there was no
significant difference in serum miR-378 levels between patients
with RCC and control. However, significantly decreased serum
miR-378 levels in patients RCC compared with control was reported
by Wang et al (40). This
group also identified a microRNA panel (serum miR-193a-3p, miR-362,
miR-572, miR-28-5p and miR-378) which demonstrated high diagnostic
accuracy in RCC (AUC=0.807 and 0.796 for training and validation
data sets, respectively). Lou et al (41) reported that plasma miR-144-3p served
as a promising diagnostic biomarker for RCC with an AUC of 0.91, a
sensitivity of 87.10% and a specificity of 83.02%. Recently, Zhao
et al (42) proposed that
upregulated miR-210 in tumor tissues and serum serves as a
diagnostic biomarker for ccRCC with an AUC of 0.874, a sensitivity
of 81.0% and a specificity of 79.4%. This was supported by Iwamoto
et al (43) who demonstrated
serum miR-210 to be a diagnostic biomarker with an AUC of 0.77, 65%
sensitivity and 83% specificity in RCC. Combination of serum
miR-378 and miR-210 has also been indicated to yield high
diagnostic accuracy with an AUC of 0.85, 80% sensitivity and 78%
specificity (44). More recently, Li
et al (45) demonstrated that
urinary miR-210 expression was significantly upregulated in
patients with ccRCC, which yielded an AUC of 0.76 in for
distinguishing ccRCC. In the present study, it was demonstrated
that plasma miR-210, miR-224 and miR210×224 had good
sensitivity, but low accuracy and specificity, for distinguishing
ccRCC patients from healthy individuals. The inconsistency of these
results may be due to the variability/selection of study
participants, or differing methodologies for sample processing,
miRNA extraction and data normalization.
Normalization is a critical step for the accurate
quantification of miRNA levels with RT-qPCR. However, no consensus
regarding internal controls currently exist for the analysis of
circulating miRNA. Literature-based tissue housekeeping genes or
miRNAs in the blood are often selected as references for
normalization of miRNA expression levels, including miR-16, RNU6B
or RNAU6 (46). miR-16 has been
suggested to act as an oncomiRs in certain types of cancer, and
RNU6B is degraded in the blood, rendering these molecules
unsuitable for normalization of serum/plasma sample miRNA data
(46,47). In the present study, it was identified
that miR-16 and U6 were not stable normalization controls.
Recently, Roberts et al (48)
demonstrated that the synthetic spike-in control was less variable
compared with omnipresent expressed miRNAs, including miR-16. In
consistence with Roberts et al (48) and conventional clinical biochemistry
assays, in the present study plasma volume was standardized between
samples rather than standardization of RNA input at the reverse
transcription stage. Sanders et al (49) demonstrated that cel-miR-39 is
effective for normalization of circulating miRNAs in patients with
urological malignancies, including RCC.
Recent studies have revealed that circulating miRNAs
are encapsulated in microparticles that are actively secreted from
cancer cells, and that function in cell-cell communications
(25). Thus, miRNAs upregulated in
tumor tissue may be reflectively overexpressed in the bloodstream.
In the present study, it was observed that tissue and plasma
miR-210 and miR-224 were overexpressed in ccRCC. However, the
expression levels in the plasma were decreased 7 days post-surgery,
suggesting that circulating miR-210 and miR-224 in ccRCC patients
are released in large amounts from ccRCC tumor tissue. However, no
positive correlation between plasma and tissue expression levels of
miR-210 and miR-224 was observed in patients with ccRCC. Therefore,
it remains unclear whether ccRCC cells secrete miR-210 and miR-224
into the bloodstream. It is possible that ccRCC cells stimulate
non-tumoral cells in renal organs and other organs to secrete
miRNAs. Further study is required to determine the source of plasma
miR-210 and miR-224 in patients with ccRCC.
In conclusion, tissue miR224/141 is a
potentially powerful tool for the early detection of ccRCC. Further
investigation is urgently required to identify circulating miRNAs,
which serve as specific biomarkers for ccRCC, and to reveal their
source and roles in ccRCC pathogenesis. Although a number of
studies have reported that circulating miRNAs are stable in blood
serum and plasma, the low level of enrichment in the blood and the
unstandardized isolation and quantification techniques are the
major hurdles in research of circulating miRNAs. Therefore, the
development of improved methods of detecting circulating miRNAs to
identify biomarkers in the future.
Acknowledgements
Not applicable.
Funding
The present study was funded by the National Natural
Science Foundation of China (NSFC; grant nos. 30872924, 81072095
and 81372760), the National High Technology Research and
Development Program of China (863 Program; grant no. 2012AA021101)
and the International Collaborating Project of Hubei Province
(grant no. 2015BH0087). The NSFC (grant no. 81702517) and Natural
Science Foundation of Zhejiang Province (grant No. LY15H160052).
The present study was partially supported by another NSFC grant
(grant no. 81272560), the Open Research Foundation of the State Key
Laboratory of Virology of Wuhan University (grant no. 2014KF007),
the Hubei Provincial Scientific and Technical Project (grant no.
2011CDB366) and the Hubei Provincial Health Project (grant no.
WJ2015MB020).
Availability of data and materials
The datasets used and/or analysed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
XC, XZ and HY made substantial contributions to
conception and design of this study. NL, AR, BQ, YY, XW, HR, QD,
WH, HW collected human samples, analysed and interpreted the data.
XC and QD been involved in drafting the manuscript and revising it
critically for important intellectual content. XC, XZ and HY given
final approval of the version to be published. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
All patients provided written informed consent prior
to their inclusion within the study. The present study was approved
by the Clinical Research Ethics Committee of Wuhan Union Hospital
(Wuhan, China) and the Institutional Review Board of Huazhong
University of Science and Technology (Wuhan, China).
Consent for publication
All patients provided written informed consent for
the publication of their data.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
Statistics, 2017. CA Cancer J Clin. 67:7–30. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Protzel C, Maruschke M and Hakenberg OW:
Epidemiology, aetiology, and pathogenesis of renal cell carcinoma.
Eur Urol Supp. 11:52–59. 2012. View Article : Google Scholar
|
|
3
|
Howlader N, Noone AM, Krapcho M, Garshell
J, Neyman N, Altekruse SF, Kosary CL, Yu M, Ruhl J, Tatalovich Z,
et al: SEER cancer statistics review, 1975–2010. National Cancer
Institute (Bethesda, MD). 2013.http://seer.cancer.gov/csr/1975_2010/December
19–20132013.
|
|
4
|
Hanahan D and Weinberg RA: Hallmarks of
cancer: The next generation. Cell. 144:646–674. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Djuranovic S, Nahvi A and Green R: A
parsimonious model for gene regulation by miRNAs. Science.
331:550–553. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gao Y, Zhao H, Lu Y, Li H and Yan G:
MicroRNAs as potential diagnostic biomarkers in renal cell
carcinoma. Tumour Biol. 35:11041–11050. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Al-Ali BM, Ress AL, Gerger A and Pichler
M: MicroRNAs in renal cell carcinoma: Implications for
pathogenesis, diagnosis, prognosis and therapy. Anticancer Res.
32:3727–3732. 2012.PubMed/NCBI
|
|
8
|
Lawrie CH, Gal S, Dunlop HM, Pushkaran B,
Liggins AP, Pulford K, Banham AH, Pezzella F, Boultwood J,
Wainscoat JS, et al: Detection of elevated levels of
tumour-associated microRNAs in serum of patients with diffuse large
B-cell lymphoma. Br J Haematol. 141:672–675. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mitchell PS, Parkin RK, Kroh EM, Fritz BR,
Wyman SK, Pogosova-Agadjanyan EL, Peterson A, Noteboom J, O'Briant
KC, Allen A, et al: Circulating microRNAs as stable blood-based
markers for cancer detection. Proc Natl Acad Sci USA.
105:10513–10518. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Chen X, Ba Y, Ma L, Cai X, Yin Y, Wang K,
Guo J, Zhang Y, Chen J, Guo X, et al: Characterization of microRNAs
in serum: A novel class of biomarkers for diagnosis of cancer and
other diseases. Cell Res. 18:997–1006. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Weber JA, Baxter DH, Zhang S, Huang DY,
Huang KH, Lee MJ, Galas DJ and Wang K: The microRNA spectrum in 12
body fluids. Clin Chem. 56:1733–1741. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chen X, Wang X, Ruan A, Han W, Zhao Y, Lu
X, Xiao P, Shi H, Wang R, Chen L, et al: miR-141 Is a key regulator
of renal cell carcinoma proliferation and metastasis by controlling
EphA2 expression. Clin Cancer Res. 20:2617–2630. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Nakada C, Matsuura K, Tsukamoto Y,
Tanigawa M, Yoshimoto T, Narimatsu T, Nguyen LT, Hijiya N, Uchida
T, Sato F, et al: Genome-wide microRNA expression profiling in
renal cell carcinoma: Significant down-regulation of miR-141 and
miR-200c. J Pathol. 216:418–427. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jung M, Mollenkopf HJ, Grimm C, Wagner I,
Albrecht M, Waller T, Pilarsky C, Johannsen M, Stephan C, Lehrach
H, et al: MicroRNA profiling of clear cell renal cell cancer
identifies a robust signature to define renal malignancy. J Cell
Mol Med. 13:3918–3928. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yi Z, Fu Y, Zhao S, Zhang X and Ma C:
Differential expression of miRNA patterns in renal cell carcinoma
and nontumorous tissues. J Cancer Res Clin Oncol. 136:855–862.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Juan D, Alexe G, Antes T, Liu H,
Madabhushi A, Delisi C, Ganesan S, Bhanot G and Liou LS:
Identification of a microRNA panel for clear-cell kidney cancer.
Urology. 75:835–841. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Weng L, Wu X, Gao H, Mu B, Li X, Wang JH,
Guo C, Jin JM, Chen Z, Covarrubias M, et al: MicroRNA profiling of
clear cell renal cell carcinoma by whole-genome small RNA deep
sequencing of paired frozen and formalin-fixed, paraffin-embedded
tissue specimens. J Pathol. 222:41–51. 2010.PubMed/NCBI
|
|
18
|
Duns G, van den Berg A, van Dijk MC, van
Duivenbode I, Giezen C, Kluiver J, van Goor H, Hofstra RM, van den
Berg E and Kok K: The entire miR-200 seed family is strongly
deregulated in clear cell renal cell cancer compared to the
proximal tubular epithelial cells of the kidney. Genes Chromosomes
Cancer. 52:165–173. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hidaka H, Seki N, Yoshino H, Yamasaki T,
Yamada Y, Nohata N, Fuse M, Nakagawa M and Enokida H: Tumor
suppressive microRNA-1285 regulates novel molecular targets:
Aberrant expression and functional significance in renal cell
carcinoma. Oncotarget. 3:44–57. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Wang X, Chen X, Han W, Ruan A, Chen L,
Wang R, Xu Z, Xiao P, Lu X, Zhao Y, et al: miR-200c targets CDK2
and suppresses tumorigenesis in renal cell carcinoma. Mol Cancer
Res. 13:1567–1577. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Edge SB and Compton CC: The American Joint
Committee on Cancer: The 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lopez-Beltran A, Scarpelli M, Montironi R
and Kirkali Z: 2004 WHO classification of the renal tumors of the
adults. Eur Urol. 49:798–805. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Fuhrman SA, Lasky LC and Limas C:
Prognostic significance of morphologic parameters in renal cell
carcinoma. Am J Surg Pathol. 6:655–663. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Turchinovich A, Weiz L and Burwinkel B:
Extracellular miRNAs: The mystery of their origin and function.
Trends Biochem Sci. 37:460–465. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Heneghan HM, Miller N and Kerin MJ:
Circulating miRNA signatures: Promising prognostic tools for
cancer. J Clin Oncol. 28:e573–e576. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Scheffer AR, Holdenrieder S, Kristiansen
G, von Ruecker A, Muller SC and Ellinger J: Circulating microRNAs
in serum: Novel biomarkers for patients with bladder cancer? World
J Urol. 32:353–358. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Westermann AM, Schmidt D, Holdenrieder S,
Moritz R, Semjonow A, Schmidt M, Kristiansen G, Müller SC and
Ellinger J: Serum microRNAs as biomarkers in patients undergoing
prostate biopsy: Results from a prospective multi-center study.
Anticancer Res. 34:665–669. 2014.PubMed/NCBI
|
|
29
|
Sethi S, Ali S, Philip PA and Sarkar FH:
Clinical advances in molecular biomarkers for cancer diagnosis and
therapy. Int J Mol Sci. 14:14771–14784. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Bovell LC, Putcha BD, Samuel T and Manne
U: Clinical implications of microRNAs in cancer. Biotech Histochem.
88:388–396. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ellinger J, Gevensleben H, Muller SC and
Dietrich D: The emerging role of non-coding circulating RNA as a
biomarker in renal cell carcinoma. Expert Rev Mol Diagn.
16:1059–1065. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Wotschofsky Z, Busch J, Jung M,
Kempkensteffen C, Weikert S, Schaser KD, Melcher I, Kilic E, Miller
K, Kristiansen G, et al: Diagnostic and prognostic potential of
differentially expressed miRNAs between metastatic and
non-metastatic renal cell carcinoma at the time of nephrectomy.
Clin Chim Acta. 416:5–10. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Fridman E, Dotan Z, Barshack I, David MB,
Dov A, Tabak S, Zion O, Benjamin S, Benjamin H, Kuker H, et al:
Accurate molecular classification of renal tumors using MicroRNA
expression. J Mol Diagn. 12:687–696. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Youssef YM, White NM, Grigull J, Krizova
A, Samy C, Mejia-Guerrero S, Evans A and Yousef GM: Accurate
molecular classification of kidney cancer subtypes using MicroRNA
signature. Eur Urol. 59:721–730. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Larne O, Martens-Uzunova E, Hagman Z,
Edsjö A, Lippolis G, den Berg MS, Bjartell A, Jenster G and Ceder
Y: miQ-a novel microRNA based diagnostic and prognostic tool for
prostate cancer. Int J Cancer. 132:2867–2875. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Fritz HK, Lindgren D, Ljungberg B, Axelson
H and Dahlback B: The miR(21/10b) ratio as a prognostic marker in
clear cell renal cell carcinoma. Eur J Cancer. 50:1758–1765. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Wulfken LM, Moritz R, Ohlmann C,
Holdenrieder S, Jung V, Becker F, Herrmann E, Walgenbach-Brünagel
G, von Ruecker A, Müller SC and Ellinger J: MicroRNAs in renal cell
carcinoma: Diagnostic implications of serum miR-1233 levels. PLoS
One. 6:e257872011. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Redova M, Poprach A, Nekvindova J, Iliev
R, Radova L, Lakomy R, Svoboda M, Vyzula R and Slaby O: Circulating
miR-378 and miR-451 in serum are potential biomarkers for renal
cell carcinoma. J Transl Med. 10:552012. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Hauser S, Wulfken LM, Holdenrieder S,
Moritz R, Ohlmann CH, Jung V, Becker F, Herrmann E,
Walgenbach-Brünagel G, von Ruecker A, et al: Analysis of serum
microRNAs (miR-26a-2*miR-191, miR-337-3p and miR-378) as potential
biomarkers in renal cell carcinoma. Cancer Epidemiol. 36:391–394.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Wang C, Hu J, Lu M, Gu H, Zhou X, Chen X,
Zen K, Zhang CY, Zhang T, Ge J, et al: A panel of five serum miRNAs
as a potential diagnostic tool for early-stage renal cell
carcinoma. Sci Rep. 5:76102015. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Lou N, Ruan AM, Qiu B, Bao L, Xu YC, Zhao
Y, Sun RL, Zhang ST, Xu GH, Ruan HL, et al: miR-144-3p as a novel
plasma diagnostic biomarker for clear cell renal cell carcinoma.
Urol Oncol. 35:36.e7–36.e14. 2017. View Article : Google Scholar
|
|
42
|
Zhao A, Li G, Peoc'h M, Genin C and
Gigante M: Serum miR-210 as a novel biomarker for molecular
diagnosis of clear cell renal cell carcinoma. Exp Mol Pathol.
94:115–120. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Iwamoto H, Kanda Y, Sejima T, Osaki M,
Okada F and Takenaka A: Serum miR-210 as a potential biomarker of
early clear cell renal cell carcinoma. Int J Oncol. 44:53–58. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Fedorko M, Stanik M, Iliev R,
Redova-Lojova M, Machackova T, Svoboda M, Pacik D, Dolezel J and
Slaby O: Combination of MiR-378 and MiR-210 serum levels enables
sensitive detection of renal cell carcinoma. Int J Mol Sci.
16:23382–23389. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Li G, Zhao A, Peoch M, Cottier M and
Mottet N: Detection of urinary cell-free miR-210 as a potential
tool of liquid biopsy for clear cell renal cell carcinoma. Urol
Oncol. 35:294–299. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Brase JC, Wuttig D, Kuner R and Sultmann
H: Serum microRNAs as non-invasive biomarkers for cancer. Mol
Cancer. 9:3062010. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Huang E, Liu R and Chu Y: miRNA-15a/16: As
tumor suppressors and more. Future Oncol. 11:2351–2363. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Roberts TC, Coenen-Stass AM and Wood MJ:
Assessment of RT-qPCR normalization strategies for accurate
quantification of extracellular microRNAs in murine serum. PLoS
One. 9:e892372014. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Sanders I, Holdenrieder S,
Walgenbach-Brunagel G, von Ruecker A, Kristiansen G, Müller SC and
Ellinger J: Evaluation of reference genes for the analysis of serum
miRNA in patients with prostate cancer, bladder cancer and renal
cell carcinoma. Int J Urol. 19:1017–1025. 2012. View Article : Google Scholar : PubMed/NCBI
|