Introduction
Advances in genomic research have revealed various
mutations in cancer-associated genes. One of these mutations is
located in the proto-oncogene B-Raf (BRAF) gene, and has been
detected in a wide range of cancer types, including malignant
melanoma, papillary thyroid carcinoma and colorectal cancer
(1).
BRAF is a serine/threonine kinase and a member of
the RAF family, which consists of three kinases: ARAF, CRAF (RAF-1)
and BRAF. BRAF is a key regulator of the mitogen-activated protein
kinase/extracellular signal-regulated kinase pathway (2). Hyperactivation of this pathway can lead
to cell cycle arrest, while aberrant regulation of the pathway can
trigger carcinogenesis (1).
In total, >40 mutations have been identified in
the BRAF gene, and 90% of these are accounted for by a single base
change of thymine-to-adenine at position 1,799. This missense
mutation in exon 15 results in a change at residue 600, where
glutamine is substituted for valine (V600E). BRAF V600E can lead to
a 500-fold increase in activation of the gene. Additionally, it
also permits signaling cascade activation in the absence of any
extracellular stimuli, such as growth signals, and the cells can
therefore become self-sufficient within this pathway (2).
The BRAF V600E mutation is detected in 4% of primary
and metastatic central nervous system neoplasms. Among metastatic
cases, melanoma, papillary thyroid carcinoma and hepatocellular
carcinoma cerebral metastases have been found to possess this
mutation (3).
Point or fusion mutations in BRAF have also been
identified in glial and glioneuronal tumors, particularly in
pediatric-onset cases. The majority of BRAF mutations are BRAF V600
mutations. BRAF V600E frequently occurs in pleomorphic
xanthoastrocytoma (PXA), ganglioglioma and extra-cerebellar
pilocytic astrocytoma (4). BRAF V600E
is also detected in 1% of primary brain tumors, including
glioblastoma (GBM), gliosarcoma, diffuse astrocytoma and rhabdoid
meningioma (3).
Epithelioid GBM (E-GBM) is a novel entity according
to the World Health Organization (WHO) 2016 brain tumor
classification (5). The composition
of an E-GBM is based on cohesive sheets of closely-packed,
patternless, variably lipidized, small-to medium-sized cells that
have rounded cytoplasmic borders, an eosinophilic cytoplasm and
lack any cytoplasmic stellate processes, with interspersed
neuropils (6–11). The tumors also harbor BRAF V600E
mutations (3,11,12).
Anti-BRAF V600E (clone VE1), a mouse monoclonal
primary antibody [anti-BRAF V600E (VE1)] is used in the
identification of the mutant BRAF V600E protein. BRAF VE1 has been
successfully validated in malignant melanoma, colorectal carcinoma,
papillary thyroid carcinoma, lung cancer and PXA (13–19).
The present study aimed to investigate the presence
of the BRAF V600E mutation and the immunoexpression profiles of
different types of GBMs treated at Bezmialem Vakıf University
(İstanbul, Turkey), and to determine the efficiency of the BRAF
mutation-specific VE1 antibody to detect the V600E hotspot mutation
successfully. In addition, the potential associations between the
clinical parameters of these cases and BRAF status were
analyzed.
Materials and methods
Patients and tumor classification
A total of 20 patients with GBM between January 2015
and January 2017 were included in this study in order to analyze
the immunoexpression of BRAF (BRAF VE1) and the BRAF V600E
mutation. Newly diagnosed glioblastomas were included in the study.
Exclusion criteria were prior chemotherapy, antiangiogenic therapy
and radiotherapy.
This study was approved by the Ethics Committee of
Bezmialem Vakıf University Faculty of Medicine (İstanbul, Turkey).
Written informed consent was obtained from all patients included in
this study. The expression levels of these antigens and their
associations with the clinical follow-up data, including the
patient's age, sex and overall survival status, were assessed.
Clinical information and follow-up data were
obtained from the Department of Neurosurgery. Telephone interviews
of the patients or family members were performed for the study.
Overall survival was defined from the time of diagnosis to
mortality from any cause of death.
All hematoxylin and eosin-stained slides were
reviewed by two pathologists for the confirmation of the diagnoses.
GBMs were considered as having epithelioid features when >30% of
the tumor was composed of epithelioid cells. Tumors with a
predominance of bizarre, multinucleated giant cells and occasional
abundant stromal reticulin networks were considered as giant cell
GBMs. Tumors were further categorized into two types for
statistical analysis: GBMs with epithelioid features and GBMs with
non-epithelioid features.
Mutation analysis
Samples from all 20 patients were analyzed for V600
mutations using the Cobas 4800 BRAF V600 Mutation Test (Roche
Molecular Diagnostics, Pleasanton CA, USA), which is a European
Conformity (CE)-marked and Food and Drug Administration
(FDA)-approved in vitro diagnostics device designed to
detect the BRAF p.Val600Glu mutation in DNA derived from
formalin-fixed, paraffin-embedded (FFPE) melanoma samples. The
method consisted of a quantitative polymerase chain reaction (PCR)
step with two primers that amplified a 116-bp fragment of exon 15
of BRAF (containing codon 600), and two hydrolysis probes labeled
with different fluorochromes [one for the wild-type (WT) allele and
one for the mutant allele, p.Val600Glu and a quencher]. The
quencher absorbed the light from the reporter dye until the DNA
polymerase cleaved it with its 5′-3′ exonuclease activity during
the amplification steps. Once the reporter was free, it emitted
fluorescence at a specific wavelength, which differed for the WT
and p.Val600Glu alleles. The amount of light detected throughout
the PCR for each dye was directly proportional to the original
amount of WT or p.Val600Glu template; therefore, at the end of the
process, the software calculated the ratio of these two signals to
report each sample as ‘mutation detected’ or ‘mutation not
detected’. Selective amplification was achieved by using
uracil-N-glycosylase and dUTP in the reaction mix to thereby
eliminate any potential contamination during the first step of the
reaction prior to PCR amplification. The kit also contained a WT
and a p.Val600Glu control tube that were analyzed in each run to
ensure performance of the test. The Cobas z480 (Roche Molecular
Diagnostics) (offered software for automated analysis and
interpretation of the results. The analysis was performed according
to the manufacturer's protocol.
Immunohistochemistry (IHC)
Sections (4-µm thick) of FFPE tissues were placed on
3-aminopropyletxylene-covered slides. Subsequently, they were
stained with mouse monoclonal antibody against BRAF V600E (catalog
no. 790-4855; 1/100 titer; clone VE1) following the Ventana Medical
Systems' protocol. Briefly, staining was performed on a Ventana
BenchMark Ultra (Ventana Medical Systems, Inc., Tucson, AZ, USA).
The staining protocol included use of Cell Conditioning 1 (Ventana
Medical Systems, Inc.) for 64 min, pre-peroxidase inhibition with
3% hydrogen peroxide for 10 min at 37°C, primary antibody
incubation for 70 min and Amplification kit (catalog no. 760-080;
Ventana Medical Inc.) was applied for 4 min at 37°C to increase the
signal intensity. The OptiView DAB IHC Detection kit (Ventana
Medical Systems, Inc.) was used to detect BRAF V600E protein
expression. Tissues were counterstained with hematoxylin for 16 min
and Bluing Reagent for 4 min. Counterstaining was applied at room
temperature. After the procedure the slides were reviewed using
Nikon Ci-E microscope (Nikon Corporation, Tokyo, Japan) at −40,
−100, −200 and −400 magnifications.
All of the cases were evaluated with an
immunohistochemical panel consisting of glial fibrillary acidic
protein (GFAP), Olig2, epithelial membrane antigene (EMA), CK
(Pancytokeratin) and Ki-67 antibodies at time of initial diagnosis.
The staining was also performed on a Ventana BenchMark Ultra
(Ventana Medical Systems, Inc., Tucson, AZ, USA) with
immunostaining protocols for GFAP (catalog no. RB-087-R7; Thermo
Fisher Scientific, Inc., Waltham, MA, USA) 1:100 dilution for 20
min, Olig2 (catalog no. GTX31569; GeneTex, Irvine, CA, USA) 1:100
dilution for 20 min, EMA (catalog no. MS-348-R7; Thermo Fisher
Scientific, Inc.) 1:200 dilution for 30 min, CK (Keratin Clone
AE1/AE3, catalog no. MS-343-R7; Thermo Fisher Scientific, Inc.)
1:50 for 20 min, Vimentin (catalog no. MS-129-R7; Thermo Fisher
Scientific, Inc.) 1:50 dilution for 20 min and Ki67 (catalog no.
RB-1510-R7; Thermo Fisher Scientific, Inc.) 1:100 dilution for 30
min at room temperature.
Evaluation of immunostaining
Immunostaining with the BRAF VE-1 antibody was
evaluated in 10 representative fields. The cases were considered as
positive when diffuse near-complete cytoplasmic and membranous
staining was visible at scanning magnification. Background staining
and staining in non-tumoral cells was considered as non-specific
staining, and cases with this kind of staining pattern were
interpreted as negative. A PE block prepared from a case of
papillary thyroid carcinoma showing diffuse intense staining with
the BRAF VE1 antibody was also used as an external control
tissue.
Statistical analysis
Statistical analysis was performed using Number
Cruncher Statistical System 2007 (NCSS; LLC, Kaysville, UT, USA).
Quantitative statistics (mean, standard deviation and frequency)
and qualitative data were analyzed. Normally distributed parameters
between groups were analyzed with the unpaired Student's t-test and
the unevenly distributed data were analyzed using the Mann Whitney
U-test. Frequency data were assessed with the χ2 test or
the Fisher's exact test. Survival was evaluated with Kaplan-Meier
survival analysis excluding those lost to follow-up and who
succumbed due to postoperative surgical complications. Log-rank
(Mantel-Cox) analysis was used to compare the prognostic
significance of the antibody staining level for survival. Results
were presented with 95% confidence intervals, and P<0.05 was
considered to indicate a statistically significant difference.
Results
Patients and follow-up
A total of 20 patients (12 men and 8 women) were
included in this study. The age of the patients ranged from 2 to 80
years, and the median age at time of diagnosis was 54 years. The
tumors were parietal (n=3), frontotemporal (n=2), frontal (n=6),
temporal (n=4), frontoparietal (n=4) and occipital (n=1).
Data from clinical follow-up of up to 827 days was
available for 15 out of 20 patients. The mean survival time was
464.0 days (range, 13–827 days). The overall mortality rate of the
patients with GBM was 53.3% (8 of the 15 patients).
Patients with E-GBM ranged in age from 2–74 years.
Of the 6 patients with E-GBM, 5 patients were <50 years old, and
3 were pediatric (≤18 years old). Of the pediatric patients, 1
patient was 2 years old and the others were 17 years old at the
time of diagnosis. In the non-epithelioid GBM (NE-GBM) group, the
majority of the patients were aged >50 years. Only 1 patient
with conventional GBM was pediatric (13 years old) (Table I).
 | Table I.Summary of clinical, morphological
and molecular data of the patients. |
Table I.
Summary of clinical, morphological
and molecular data of the patients.
| Patient no. | Age, years | Sex | Localization | Morphology | BRAF IHC | BRAF V600E
mutation | Survival time,
days | Survival
status |
|---|
| 1 | 44 | M | Parietal | E | – | + | 304 | Alive |
| 2 | 2 | M | Frontotemporal | E | – | – | 185 | Succumbed |
| 3 | 17 | F | Parietal | E | – | – | NA | NA |
| 4 | 49 | M | Frontal | E | – | – | 396 | Alive |
| 5 | 17 | F | Parietal | E | – | – | 211 | Alive |
| 6 | 74 | M | Temporal | E | – | – | NA | NA |
| 7 | 73 | M | Frontoparietal | GC | – | – | 132 | Succumbed |
| 8 | 71 | M | Occipital | GC | – | – | 541 | Succumbed |
| 9 | 62 | F | Frontal | GC | – | – | NA | NA |
| 10 | 30 | F | Frontal | GC | – | – | 710 | Alive |
| 11 | 46 | F | Frontal | GC | – | – | 827 | Alive |
| 12 | 53 | F | Frontoparietal | GC | – | – | 13 | Succumbed |
| 13 | 53 | M | Frontoparietal | C | – | – | 251 | Succumbed |
| 14 | 80 | M | Frontotemporal | C | – | – | 268 | Succumbed |
| 15 | 71 | F | Temporal | C | + | – | 536 | Alive |
| 16 | 61 | M | Frontal | C | + | – | 360 | Succumbed |
| 17 | 13 | M | Temporal | C | + | – | 276 | Alive |
| 18 | 55 | M | Temporal | C | – | – | 166 | Succumbed |
| 19 | 65 | F | Frontal | C | – | – | NA | NA |
| 20 | 69 | M | Frontoparietal | C | – | – | NA | NA |
The associations between age, sex and localization
between the two histological types [E-GBM and NE-GBM) were
analyzed. No significant difference was identified between the two
groups for these parameters (P>0.05). The estimated mean
survival times were 434 and 343 days in NE-GBMs and E-GBMs,
respectively. Although the survival time was shorter in E-GBMs,
there was no statistically significant difference (P>0.05)
Kaplan Meier Analysis, χ2 Test, Log Rank (Mantel Cox)
(Table II).
| Table II.Mean survival times (days). |
Table II.
Mean survival times (days).
|
|
| Mean |
|---|
|
|
|
|
|---|
|
|
| 95% Confidence
interval |
|---|
|
|
|
|
|---|
| Morphology | Estimatea | Std Error | Lower limit | Upper limit |
|---|
| NE-GBMs | 434,000 | 90,878 | 255,879 | 612,121 |
| E-GBMS | 343,250 | 45,683 | 253,712 | 432,788 |
| All GBMs | 464,030 | 82,945 | 301,459 | 626,602 |
Histopathological evaluation
According to the WHO classification, 8 tumors were
of the conventional type, 6 were giant cell GBMs and 6 had
epithelioid features. Conventional and giant cell GBMs were
considered as NE-GBMs. The mortality rates were 25% in E-GBMs and
63.6% in NE-GBMs.
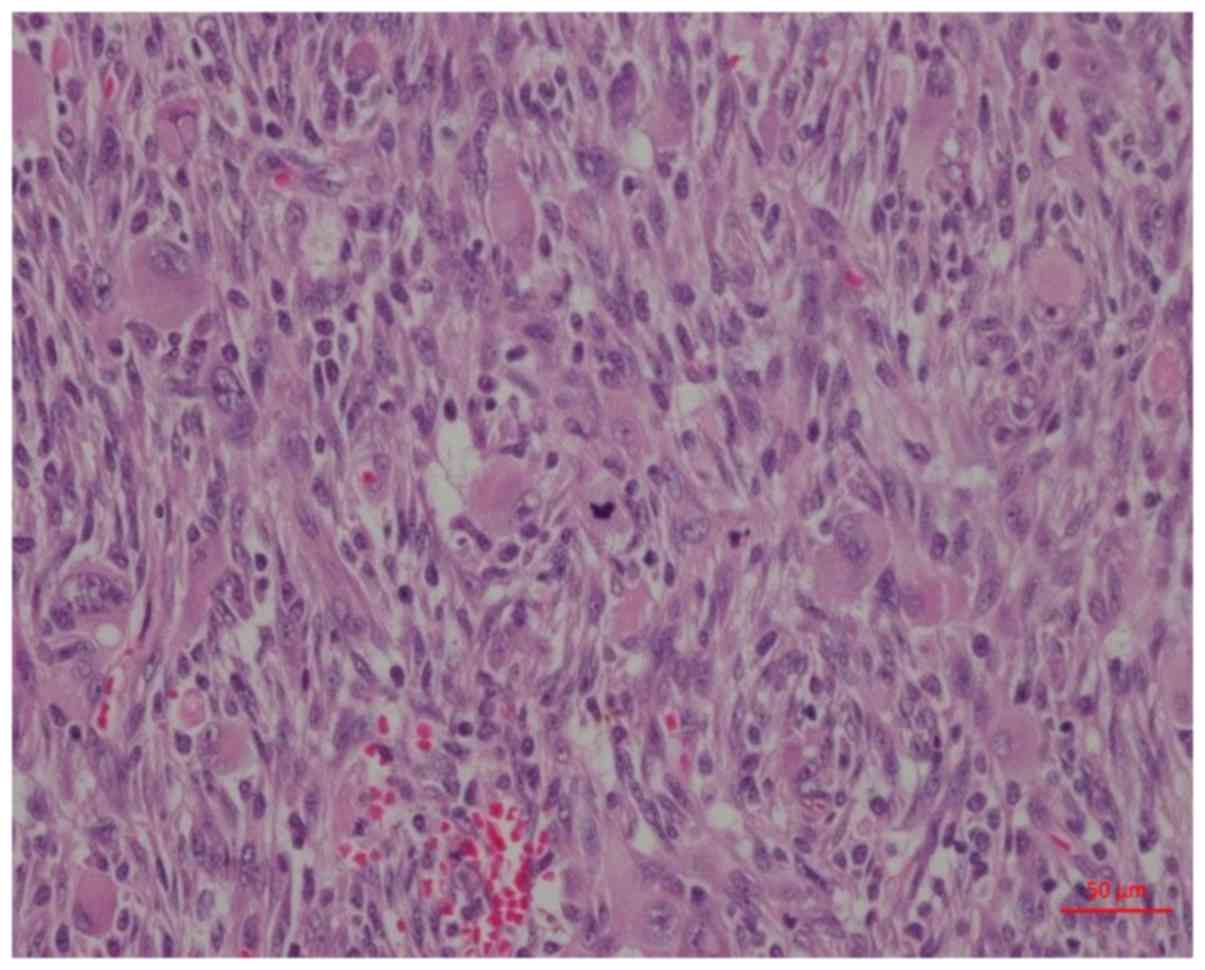
E-GBMs were composed of epithelioid cells with
eosinophilic round cytoplasm devoid of stellate cytoplasmic
processes, and exhibited nuclei with distinct nucleoli that were
eccentrically located. These cells were discohesive and arranged in
patternless and closely packed sheets (Fig. 1). A number of the cells had
intranuclear inclusions. All of the E-GBM cases showed
microvascular proliferation and palisading/confluent necrosis. None
of the E-GBMs showed eosinophilic granular bodies, which are a
distinct feature of PXAs. Mitotic activity was also high in the
E-GBM cases [>7 per 10 high-power fields (HPFs) in each case].
In 2 cases, 40 mitoses per 10 HPFs were recorded, and the mean
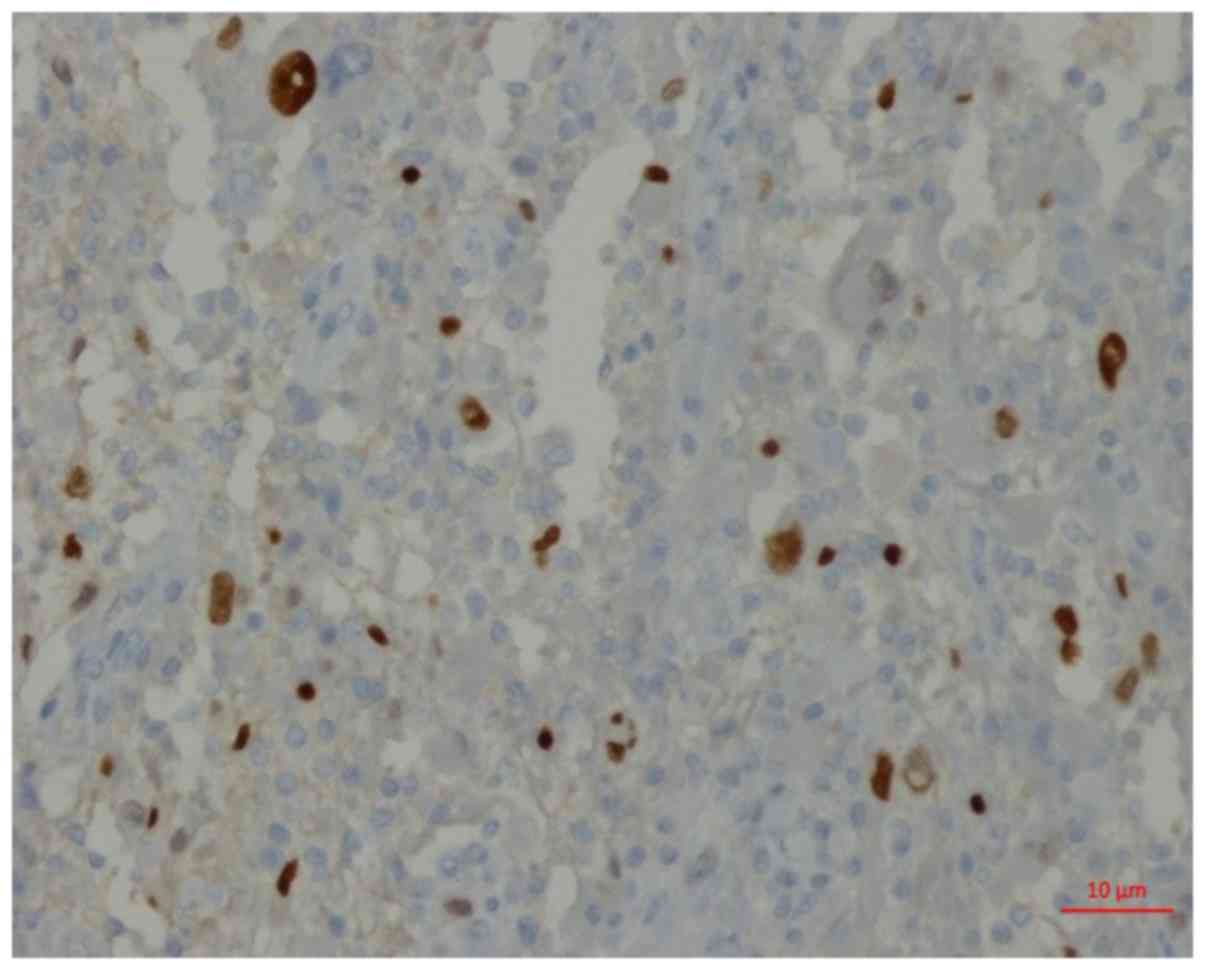
mitotic activity was 23 per 10 HPFs. IHC staining in the 6 cases
showed focal and/or weak staining with GFAP and focal nuclear
staining with oligodendrocyte transcription factor (Olig2)
(Fig. 2). Focal immunoexpression with
epithelial markers, such as cytokeratin and epithelial membrane
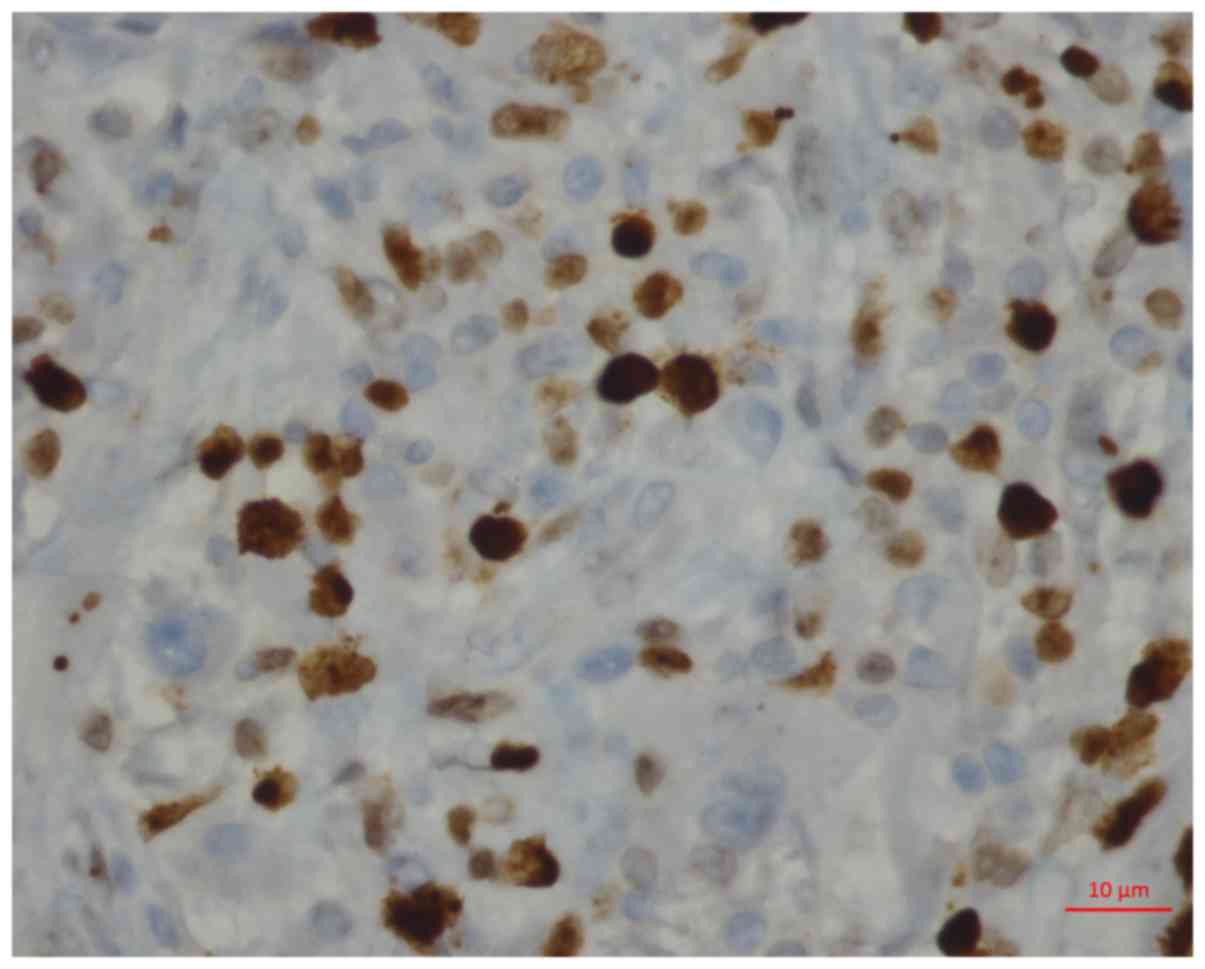
antigen, was present in each E-GBM case. The Ki-67 proliferation
index was also high in these cases. The lowest Ki-67 index was 20%,
the highest was 55% and the mean was 40% (Fig. 3).
NE-GBMs were either conventional or giant cell GBMs.
Conventional GBMs were composed of neoplastic glial cells, the
majority of which had distinct stellate cytoplasmic processes, and
all were intensely immunostained with GFAP and Olig2. Giant cell
GBMs had a >50% giant cell component throughout the whole tumor.
The giant cells were bizarre and multinucleated. All the giant cell
GBMs had an abundant stromal reticulin network and had glial
regions, stained with GFAP, and sarcomatous regions, stained with
vimentin. The mean mitotic activity of the NE-GBMs was 15 per 10
HPFs and the mean Ki-67 index was 37%.
Immunoexpression of BRAF VE1 and BRAF
V600E mutation
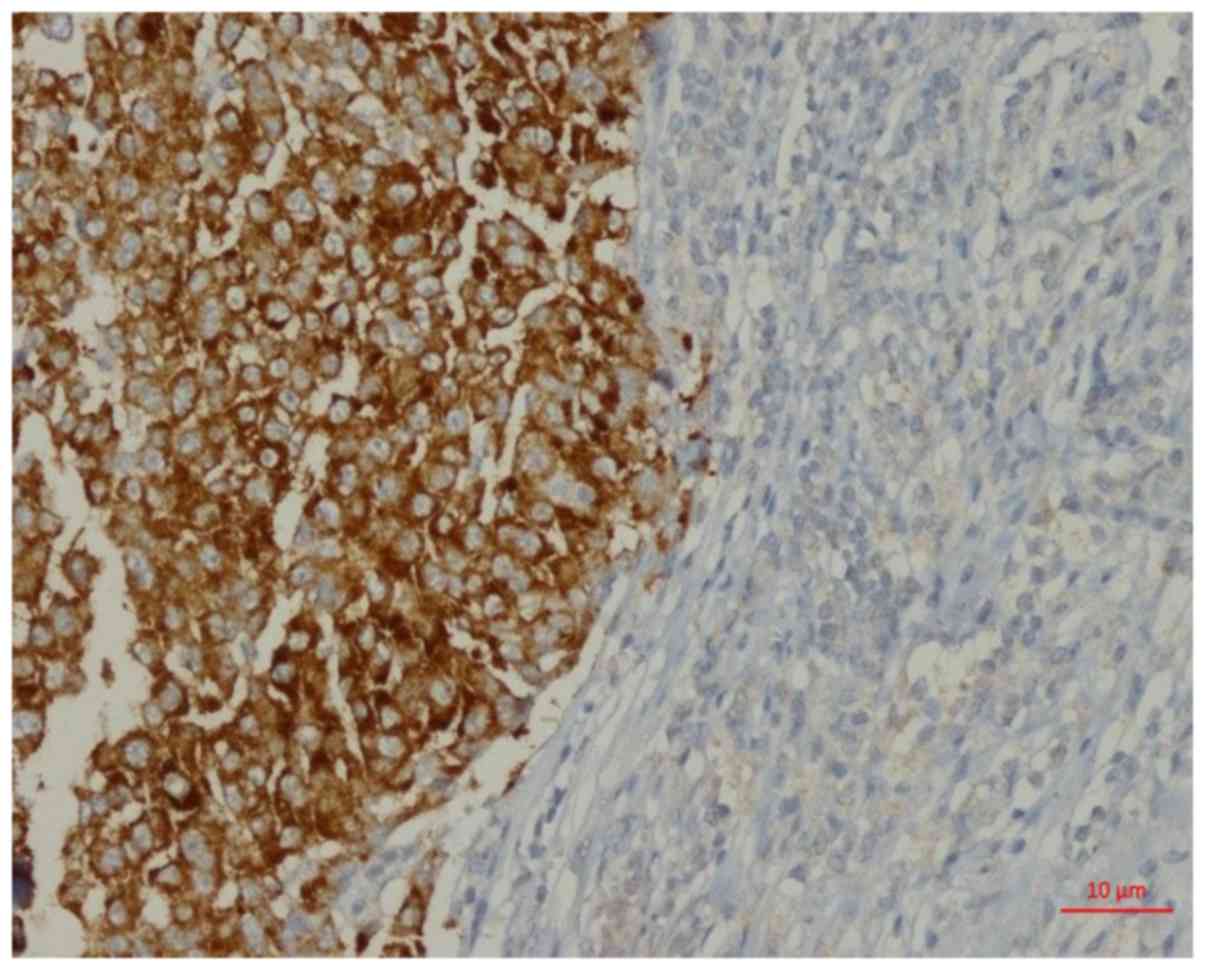
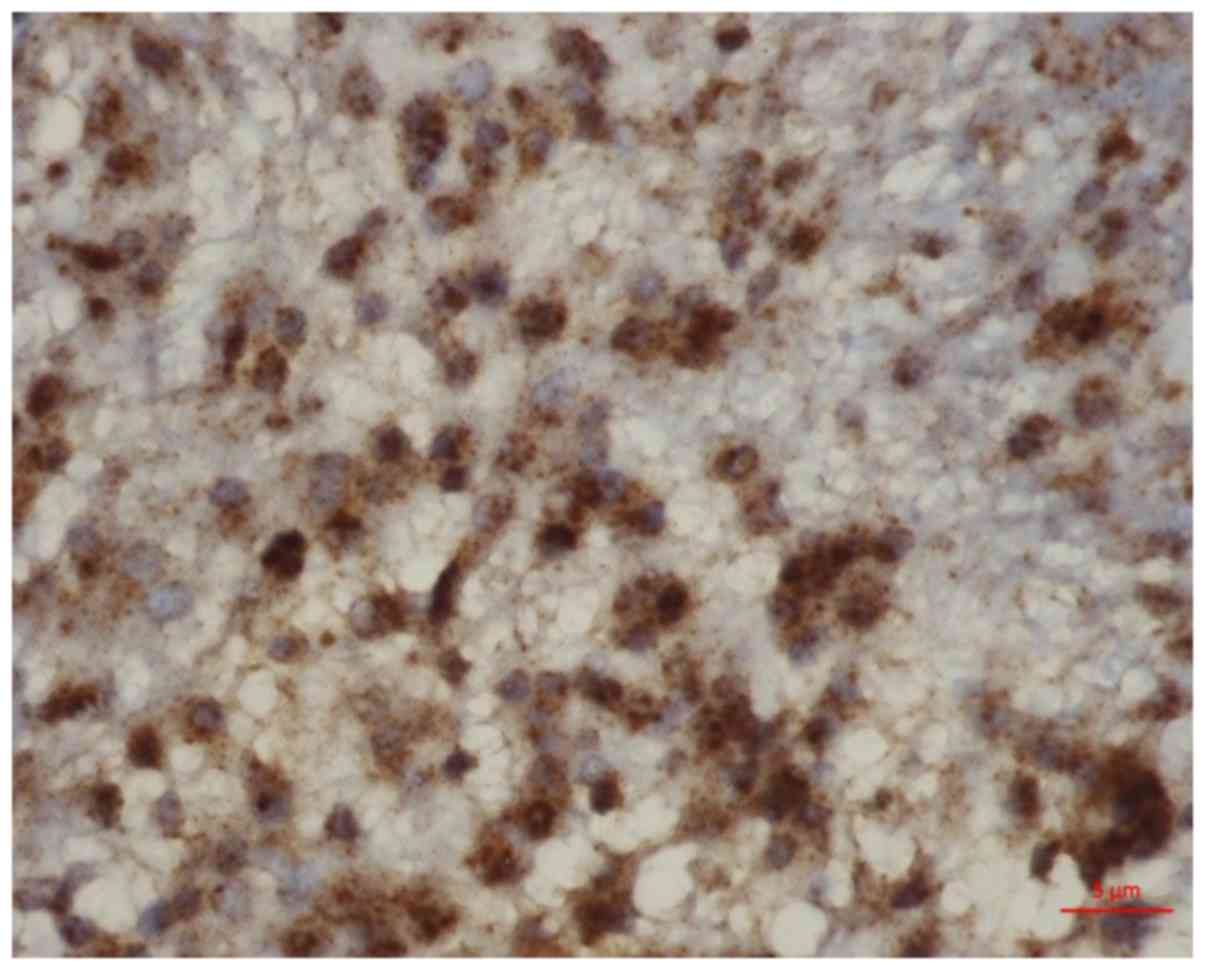
Among the conventional GBMs, 3 showed positive
immunostaining with the BRAF VE1 antibody, while no
immunoreactivity was observed in the other cases (Figs. 4 and 5).
Diffuse intense cytoplasmic staining, mild membranous staining and
a certain degree of granular staining were present in the positive
cases. Only 1 E-GBM patient (a 44-year-old male) exhibited the BRAF
V600E mutation. In this patient, the tumor was located in the left
parietal lobe, and magnetic resonance imaging results indicated
possible metastasis. The mitotic count was 11 per 10 HPFs and the
Ki-67 proliferation index was 55%. BRAF VE1 immunoexpression was
not observed in this case. IHC testing was repeated, but the second
test invariably showed no staining. The association between BRAF
immunohistochemistry and BRAF mutation was analysed using Fisher's
Exact Test. No statistical association was identified between
mutation and immunohistochemistry (P>0.05).
The BRAF V600E mutation ratio was 16.6% in E-GBMs
and 5% in the total 20 cases of GBM included in the study. The
relation between clinical parameters such as age, sex and
localization of the patients was analysed using Fisher's Exact
Test. No statistically significant associations were found between
the clinical parameters and the BRAF status of the tumors
(P>0.05).
Discussion
The present study demonstrated that 16.7% of E-GBMs
(1/6 cases) possessed the BRAF V600E mutation. BRAF V600E mutations
are relatively common in PXAs (43–66%), anaplastic PXAs (65%) and
gangliogliomas (18–43%), whereas they are more rare in adult
gliomas (4,20–22).
Approximately 22% of gliosarcomas possess a BRAF mutation (23). Kleinschmidt-DeMasters et al
(12) found that 53.8% of E-GBMs
(7/13 cases) exhibited a BRAF V600E mutation.
E-GBMs and PXAs with anaplastically transformed foci
(A-PXAs) show overlapping features, such as epithelioid foci with
the presence of large melanoma-like tumor cells with abundant
eosinophilic cytoplasm and nuclei that are occasionally
eccentrically located. The two tumor types show focal epithelial
and glial marker expression, retained integrase interactor 1 and
Brahma-related gene 1 expression, occasional positivity for cluster
of differentiation 34 and a lack of immunoreactivity for mutant
isocitrate dehydrogenase 1 (R132H), and may have BRAF V600E
mutations. Due to the common histological, immunohistochemical,
molecular and clinical features of E-GBMs and anaplastic PXAs, one
study suggested that they are closely associated or are even the
same entity (24). However, unlike
A-PXAs, eosinophilic granular bodies are not a feature of E-GBMs.
A-PXAs show low-grade regions with more cytologically uniform
cells, while E-GBMs are composed of relatively monotonous,
epithelioid cells in large regions (25).
Tanaka et al (26) also reported an E-GBM with the BRAF
V600E mutation arising from PXA 13 years after the treatment of the
tumor. The findings in this unusual case suggested the possibility
of PXA being a precursor of E-GBM.
A high proportion of pathologists and
neuropathologists diagnose E-GBMs as separate entities (6–10,25). E-GBMs were also introduced as a
separate entity in the WHO 2016 Central Nervous System
Classification guidelines (5). None
of the E-GBMs in the present study had eosinophilic granular bodies
or low-grade areas, which are observed in A-PXAs.
Within the E-GBM cohort (n=6), the patient ages
ranged from 2 to 74 years, with 3/6 patients (50%) being pediatric.
E-GBMs are typically detected within the first three decades of
life (12,27). Behling et al (3) reported 7 cases with BRAF V600E mutations
among 784 cases of primary brain tumors, and 3 of the 7 cases with
BRAF V600E mutations were E-GBMs. Among these cases, 2 patients
were aged <30 years (3).
In a study by Dahiya et al (28), the BRAF V600E mutation was
investigated using the BRAF VE1 antibody in pediatric and adult
cases of glioma and GBM. BRAF VE1 immunoreactivity was detected in
3 out of 25 pediatric GBMs (12.0%) and 3 out of 39 adult GBMs
(7.7%). Of the 3 adult GBMs, 2 were giant cell variants, and mutant
BRAF expression was limited to the giant cells. BRAF mutant tumors
were more commonly detected in younger patients, with a mean age of
39 years (28).
In another study, next-generation sequencing and
BRAF VE1 IHC were performed to detect the BRAF V600E mutation in 11
primary and 2 secondary adult GBMs, among which 1 conventional GBM
exhibited the mutation. The patient was a 49-year-old man with a
huge multicystic mass in the right occipitoparietal area.
Histopathologically, epithelioid or ribbon-like epithelial
structures were not present (29).
One of the aims of the current study was to evaluate
whether IHC results were associated with the mutational analysis
results. IHC staining with the BRAF VE1 antibody was negative in
the only BRAF V600E mutated E-GBM case, and three immunopositive
conventional GBM cases did not harbor the mutation.
IHC is a fast and easy method for the detection of
mutations. However, optimization of IHC depends on several factors,
including tissue preservation, fixation, endogenous peroxidase
activity, temperature, and primary and secondary antibody
concentrations. For the BRAF V600E mutant case, a repeat IHC was
performed, which showed the same negative result, whereas the
external control tissue was intensely stained. The exact
explanations for the false-negative and false-positive results of
these cases are unknown, but PCR failure can be excluded, as all
samples consisted of viable adequate tumor tissues for reliable
examination.
In a study by Kleinschmidt-DeMasters et al
(11), in which the BRAF V600E
mutation was observed in 46% of cases, a 1:1 correlation was found
between BRAF V600E mutational results and IHC results. However,
limitations were indicated to exist in the immunostaining even
subsequent to multiple attempts to optimize the staining technique
parameters, and heavy background staining resulted in equivocal
results in certain cases.
Behling et al (3) performed BRAF VE1 immunostaining in
metastatic and primary brain tumors with the same antibody clone
and immunostaining apparatus used in the present study, and it was
necessary to repeat the immunostaining process in 12 cases due to
various factors, including insufficient staining or non-specific
background staining. In that study, immunostaining was followed by
Sanger sequencing for the verification of a BRAF V600E mutation,
and Sanger sequencing revealed 6 false-immunopositive cases that
were not mutated. The false-positive cases were breast cancer and
non-small cell lung cancer metastases (3). Previously, pituitary adenomas have also
been demonstrated to exhibit false-positive BRAF VE1 staining
(30).
In metastatic melanoma, although genomic assays are
the gold standard, the sensitivity and specificity of BRAF VE1 for
determining the presence of a BRAF V600 mutation are >94%, and
the use of BRAF IHC followed by genomic assays in patients with
negative IHC results for BRAF is recommended in order to increase
the patient number with detected BRAF mutations compared with that
using either assay alone (19). To
understand the reliability of BRAF VE1 IHC analyses, studies with a
greater number of cases should be performed.
In the present study, the mean estimated survival
time was 343 days in E-GBMs, and this was 101 days shorter than the
median survival time of the NE-GBMs. E-GBMs are considered to be an
aggressive variant of GBM, with early complications and short
survival times (median, 169 days) (27). Nevertheless, long survival times of up
to 10 years have also been reported in a subset of studies
(12,24,28,29).
However, the number of cases available in the literature is too
small to provide meaningful data on survival at present.
PLX4032 (vemurafenib), an FDA-approved kinase
inhibitor, has been used effectively for the targeted treatment of
metastatic melanoma (31,32). Marked responses to BRAF inhibitors
have also been previously reported in V600E mutant PXAs, a
brainstem ganglioglioma and a pediatric GBM (24,33–36). The
patient with the BRAF V600E mutation in the present study received
near-total resection followed by radiotherapy with concomitant
chemotherapy consisting of temozolamide. Unfortunately, 11 months
later, magnetic resonance imaging revealed a recurrent giant tumor
in the previous resection site, and the patient also developed a
subscapular fibrosarcoma as a secondary malignancy. The status of
the patient was not determined to be suitable for vemurafenib
therapy.
Additional studies and literature reviews will aid
in improving our understanding of the molecular signature and
prognosis of this newly introduced epithelioid subtype of GBM.
Routine IHC staining combined with genetic testing can be performed
in young patients with GBMs. A positive test result for BRAF V600E
mutational status in an E-GBM case could potentially provide the
patient with an alternative, targeted treatment in the form of
vemurafenib.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Medical
Research Council of Bezmialem Vakıf University (grant no.
3.2016/8).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
Study conception and design: ZT. Acquisition of
data: ZT, ST and AH. Analysis and interpretation of data: ZT, MOG,
AA and AH. Drafting of the manuscript: ZT and ST. Critical
revision: MOG and AA.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
Bezmialem Vakıf University Faculty of Medicine (İstanbul, Turkey).
Written informed consent was obtained from all patients included in
this study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Davies H, Bignell GR, Cox C, Stephens P,
Edkins S, Clegg S, Teague J, Woffendin H, Garnett MJ, Bottomley W,
et al: Mutations of the BRAF gene in human cancer. Nature.
417:949–954. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cantwell-Dorris ER, O'Leary JJ and Sheils
OM: BRAFV600E: Implications for carcinogenesis and molecular
therapy. Mol Cancer Ther. 10:385–394. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Behling F, Barrantes-Freer A, Skardelly M,
Nieser M, Christians A, Stockhammer F, Rohde V, Tatagiba M,
Hartmann C, Stadelmann C and Schittenhelm J: Frequency of BRAF
V600E mutations in 969 central nervous system neoplasms. Diagn
Pathol. 11:552016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Schindler G, Capper D, Meyer J, Janzarik
W, Omran H, Herold-Mende C, Schmieder K, Wesseling P, Mawrin C,
Hasselblatt M, et al: Analysis of BRAF V600E mutation in 1,320
nervous system tumors reveals high mutation frequencies in
pleomorphic xanthoastrocytoma, ganglioglioma and extra-cerebellar
pilocytic astrocytoma. Acta Neuropathol. 121:397–405. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Louis DN, Perry A, Reifenberger G, von
Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD,
Kleihues P and Ellison DW: The 2016 world health organization
classification of tumors of the central nervous system: A summary.
Acta Neuropathol. 131:803–820. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rosenblum MK, Erlandson RA and Budzilovich
GN: The lipid-rich epithelioid glioblastoma. Am J Surg Pathol.
15:925–934. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Akimoto J, Namatame H, Haraoka J and Kudo
M: Epithelioid glioblastoma: A case report. Brain Tumor Pathol.
22:21–27. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rodriguez FJ, Scheithauer BW, Giannini C,
Bryant SC and Jenkins RB: Epithelial and pseudoepithelial
differentiation in glioblastoma and gliosarcoma: A comparative
morphologic and molecular genetic study. Cancer. 113:2779–2789.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Gasco J, Franklin B, Fuller GN, Salinas P
and Prabhu S: Multifocal epithelioid glioblastoma mimicking
cerebral metastasis: Case report. Neurocirugia (Astur). 20:550–554.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tanaka S, Nakada M, Hayashi Y, Nakada S,
Sawada-Kitamura S, Furuyama N, Suzuki T, Kamide T, Hayashi Y, Yano
S and Hamada J: Epithelioid glioblastoma changed to typical
glioblastoma: The methylation status of MGMT promoter and 5-ALA
fluorescence. Brain Tumor Pathol. 28:59–64. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kleinschmidt-DeMasters BK, Aisner DL and
Foreman NK: BRAF VE1 immunoreactivity patterns in epithelioid
glioblastomas positive for BRAF V600E mutation. Am J Surg Pathol.
39:528–540. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kleinschmidt-DeMasters BK, Aisner DL,
Birks DK and Foreman NK: Epithelioid GBMs show a high percentage of
BRAF V600E mutation. Am J Surg Pathol. 37:685–698. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Capper D, Preusser M, Habel A, Sahm F,
Ackermann U, Schindler G, Pusch S, Mechtersheimer G, Zentgraf H and
von Deimling A: Assessment of BRAF V600E mutation status by
immunohistochemistry with a mutation-specific monoclonal antibody.
Acta Neuropathol. 122:11–19. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Colomba E, Hélias-Rodzewicz Z, Von
Deimling A, Marin C, Terrones N, Pechaud D, Surel S, Côté JF,
Peschaud F, Capper D, et al: Detection of BRAF p.V600E mutations in
melanomas: comparison of four methods argues for sequential use of
immunohistochemistry and pyrosequencing. J Mol Diagn. 15:94–100.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Dvorak K, Aggeler B, Palting J, McKelvie
P, Ruszkiewicz A and Waring P: Immunohistochemistry with the
anti-BRAF V600E (VE1) antibody: Impact of pre-analytical conditions
and concordance with DNA sequencing in colorectal and papillary
thyroid carcinoma. Pathology. 46:509–517. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ilie M, Long E, Hofman V, Dadone B,
Marquette CH, Mouroux J, Vignaud JM, Begueret H, Merlio JP, Capper
D, et al: Diagnostic value of immunohistochemistry for the
detection of the BRAFV600E mutation in primary lung adenocarcinoma
Caucasian patients. Ann Oncol. 24:742–748. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ida CM, Vrana JA, Rodriguez FJ, Jentoft
ME, Caron AA, Jenkins SM and Giannini C: Immunohistochemistry is
highly sensitive and specific for detection of BRAF V600E mutation
in pleomorphic xanthoastrocytoma. Acta Neuropathol Commun.
1:202013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ritterhouse LL and Barletta JA: BRAF V600E
mutation-specific antibody: A review. Semin Diagn Pathol.
32:400–408. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Lo MC, Paterson A, Maraka J, Clark R,
Goodwill J, Nobes J, Garioch J, Moncrieff M, Rytina E and Igali L:
A UK feasibility and validation study of the VE1 monoclonal
antibody immunohistochemistry stain for BRAF-V600E mutations in
metastatic melanoma. Br J Cancer. 115:223–227. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Gierke M, Sperveslage J, Schwab D,
Beschorner R, Ebinger M, Schuhmann MU and Schittenhelm J: Analysis
of IDH1-R132 mutation, BRAF V600 mutation and KIAA1549-BRAF fusion
transcript status in central nervous system tumors supports
pediatric tumor classification. J Cancer Res Clin Oncol.
142:89–100. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Gupta K, Orisme W, Harreld JH, Qaddoumi I,
Dalton JD, Punchihewa C, Collins-Underwood R, Robertson T,
Tatevossian RG and Ellison DW: Posterior fossa and spinal
gangliogliomas form two distinct clinicopathologic and molecular
subgroups. Acta Neuropathol Commun. 2:182014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Qaddoumi I, Orisme W, Wen J, Santiago T,
Gupta K, Dalton JD, Tang B, Haupfear K, Punchihewa C, Easton J, et
al: Genetic alterations in uncommon low-grade neuroepithelial
tumors: BRAF, FGFR1, and MYB mutations occur at high frequency and
align with morphology. Acta Neuropathol. 131:833–845. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Ballester LY, Fuller GN, Powell SZ, Sulman
EP, Patel KP, Luthra R and Routbort MJ: Retrospective analysis of
molecular and immunohistochemical characterization of 381 primary
brain tumors. J Neuropathol Exp Neurol. 76:179–188. 2017.PubMed/NCBI
|
|
24
|
Alexandrescu S, Korshunov A, Lai SH,
Dabiri S, Patil S, Li R, Shih CS, Bonnin JM, Baker JA, Du E, et al:
Epithelioid glioblastomas and anaplastic epithelioid pleomorphic
xanthoastrocytomas-same entity or first cousins? Brain Pathol.
26:215–223. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kleinschmidt-DeMasters BK, Alassiri AH,
Birks DK, Newell KL, Moore W and Lillehei KO: Epithelioid versus
rhabdoid glioblastomas are distinguished by monosomy 22 and
immunohistochemical expression of INI-1 but not claudin 6. Am J
Surg Pathol. 34:341–354. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Tanaka S, Nakada M, Nobusawa S, Suzuki SO,
Sabit H, Miyashita K and Hayashi Y: Epithelioid glioblastoma
arising from pleomorphic xanthoastrocytoma with the BRAF V600E
mutation. Brain Tumor Pathol. 31:172–176. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Broniscer A, Tatevossian RG, Sabin ND,
Klimo P Jr, Dalton J, Lee R, Gajjar A and Ellison DW: Clinical,
radiological, histological and molecular characteristics of
paediatric epithelioid glioblastoma. Neuropathol Appl Neurobiol.
40:327–336. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Dahiya S, Emnett RJ, Haydon DH, Leonard
JR, Phillips JJ, Perry A and Gutmann DH: BRAF-V600E mutation in
pediatric and adult glioblastoma. Neuro Oncol. 16:318–319. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Takahashi Y, Akahane T, Sawada T, Ikeda H,
Tempaku A, Yamauchi S, Nishihara H, Tanaka S, Nitta K, Ide W, et
al: Adult classical glioblastoma with a BRAF V600E mutation. World
J Surg Oncol. 13:1002015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Sperveslage J, Gierke M, Capper D,
Honegger J, Sipos B, Beschorner R and Schittenhelm J: VE1
immunohistochemistry in pituitary adenomas is not associated with
BRAF V600E mutation. Acta Neuropathol. 125:911–912. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Chapman PB, Hauschild A, Robert C, Haanen
JB, Ascierto P, Larkin J, Dummer R, Garbe C, Testori A, Maio M, et
al: Improved survival with vemurafenib in melanoma with BRAF V600E
mutation. N Engl J Med. 364:2507–2516. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Sosman JA, Kim KB, Schuchter L, Gonzalez
R, Pavlick AC, Weber JS, McArthur GA, Hutson TE, Moschos SJ,
Flaherty KT, et al: Survival in BRAF V600-mutant advanced melanoma
treated with vemurafenib. N Engl J Med. 366:707–714. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Chamberlain MC: Salvage therapy with BRAF
inhibitors for recurrent pleomorphic xanthoastrocytoma: A
retrospective case series. J Neurooncol. 114:237–240. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Lee EQ, Ruland S, LeBoeuf NR, Wen PY and
Santagata S: Successful treatment of a progressive BRAF
V600E-mutated anaplastic pleomorphic xanthoastrocytoma with
vemurafenib monotherapy. J Clin Oncol. 34:e87–e89. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Robinson GW, Orr BA and Gajjar A: Complete
clinical regression of a BRAF V600E-mutant pediatric glioblastoma
multiforme after BRAF inhibitor therapy. BMC Cancer. 14:2582014.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Rush S, Foreman N and Liu A: Brainstem
ganglioglioma successfully treated with vemurafenib. J Clin Oncol.
31:e159–e160. 2013. View Article : Google Scholar : PubMed/NCBI
|