Introduction
As the second leading cause of cancer-associated
mortality in men, and the sixth in women worldwide (1), human hepatocellular carcinoma (HCC)
remains a severe global health threat. Chronic infections of
hepatitis B virus (HBV) and hepatitis C virus (HCV) are major risk
factors associated with HCC (2). With
an increased rate of HBV/HCV infection and other risk factors,
including obesity, cigarette smoking, diabetes mellitus and heavy
alcohol consumption, the incidence of HCC has also increased
(3). In order to prevent HCC
progression, tumor resection, liver transplantation and
radiofrequency (thermal) ablation [RF(T)A] are commonly used for
HCC treatment (4–6). Although these treatments have improved
the survival rates of patients with HCC, they are only appropriate
for a minority of patients, and their efficacies are limited by
high recurrence rates (7). Hence, new
systemic therapies for HCC are urgently required.
Sorafenib, an oral multi-kinase inhibitor, can block
certain signaling pathways, including those of Raf kinase and
vascular endothelial growth factor (VEGF) (8). Multiple phase III clinical studies have
indicated its effect of improving the survival of patients with HCC
and delaying radiological progression (9). Therefore, it has been proposed as the
standard treatment for patients with advanced HCC. Considering its
strong effect on the suppression of angiogenesis and the induction
of apoptosis (10), it has also been
approved for the treatment of other types of advanced cancer,
including renal cell carcinoma (11),
breast cancer (12) and leukemia
(13). However, the survival benefits
for patients with HCC treated with sorafenib treatment are modest
due to individual variation and toxicity (14). The establishment of sorafenib-based
therapeutic combination options is required to improve the overall
survival rate of patients with HCC.
Arsenic trioxide (As2O3), a
traditional Chinese medicine, has been widely used to treat acute
promyelocytic leukemia (APL) (15).
It induces differentiation at low concentrations (<0.5 µM) and
increases apoptosis at higher concentrations (0.5–2.0 µM) in APL
cells (16). Previous studies have
used As2O3 to treat various types of solid
cancer, including small cell lung cancer (17) and colon cancer (18). Despite its ability to inhibit
hepatocellular tumor growth and cell apoptosis in vitro
(19), a phase II clinical trial
reported that As2O3 had limited activity
against advanced HCC (20). On the
other hand, a different study demonstrated that
As2O3 potentiated the anticancer activity of
sorafenib in HCC by inhibiting Akt activation (21). As2O3 in
combination with chemotherapy is now considered to have potential
in cancer therapeutics (22).
However, the effect of sorafenib/As2O3
combination on primary HCC cells and the underlying mechanisms
remain to be elucidated.
TNF-related apoptosis-inducing ligand (TRAIL), also
known as Apo2L, is a member of the TNF superfamily with potential
for anticancer therapy (23). TRAIL
induces apoptosis through interacting with its receptors, death
receptor (DR)4 and 5, causing tumor-cell death (24). The upregulation of TRAIL expression is
directly involved in the inhibition of tumor initiation and
metastasis (25,26). However, regulation of the TRAIL ligand
remains poorly understood compared with TRAIL receptor-binding.
To provide a novel solution to sorafenib-resistance
in HCC, the present study aimed to evaluate the efficacy of
As2O3/sorafenib combined treatment against
primary HCC cells and its impact on TRAIL expression. We
hypothesized that the synergistic interaction of
As2O3 and sorafenib would induce apoptosis of
HCC cells via a TRAIL-dependent pathway. Furthermore, this
synergistic effect was analyzed in fresh-isolated HCC cells.
Materials and methods
Isolation of fresh HCC cells
A total of 10 patients with HCC, including 4 females
and 6 males, aged between 48 and 79 years, with a median age of 62
years, who were either HBV- or HCV-positive underwent surgical
resection at Zhongshan Hospital (Shanghai, China) between January
2013 and December 2014. HCC tissues were collected at surgery,
washed in Hank's solution (8.0 g NaCl, 0.2 g KCl, 0.2 g Na2HPO4·H2O
1.56 g, KH2PO4 in 1 l distilled water) and sliced into 0.5–1.0-mm3
sections. Sections were incubated with 5–10 ml collagenase
containing penicillin (100 U/ml)/streptomycin (100 mg/ml) at 37°C
for 30 min, and centrifuged at 4°C, 300 × g for 12 min to achieve a
single-cell suspension. HCC cells were isolated by repeated
trypsinization and adhesion. The present study was approved by the
institutional review board of Zhongshan Hospital, Fudan University
(Shanghai, China). Written informed consent was obtained from all
patients in accordance with the Declaration of Helsinki.
Cell culture
The human HCC cell lines, Huh7, 97H and L-02, were
purchased from the Cell Bank of the Shanghai Institutes for
Biological Science (Shanghai, China). Huh7, 97H, L-02 and
freshly-isolated HCC cells were cultured in Dulbecco's modified
Eagle's medium (DMEM) supplemented with 10% fetal bovine serum
(FBS; Biowest, Nuaillé, France) and penicillin (100
U/ml)/streptomycin (100 mg/ml). Cell cultures were maintained at
37°C in a humidified atmosphere with 5% CO2. HCC cells were seeded
in 6-, 24- or 96-well plates and incubated overnight for
attachment. Following 24-h starvation, cells were treated with
different concentrations of sorafenib (5, 10 and 20 µM) and
As2O3 (0.5, 1 and 2 µM) for 24, 48 and 72 h.
A medium-only group served as a negative control.
Cell Counting Kit-8 (CCK8) assay
The culture medium was discarded and 100 µl
serum-free DMEM was added to each well with 10 µl CCK8 assay
reagent (Dojindo Molecular Technologies, Inc., Kumamoto, Japan).
After a 4-h incubation at 37°C, the absorbance was measured at 450
nM using a microplate reader (Molecular Devices, LLC, Sunnyvale,
CA, USA). A total of 6 replicates were performed for each sample to
obtain a mean value. The drug combination index value was
calculated according to Jin's formula: Q=E(A+B)/(EA+EB-EA*EB)
(27). E(A+B) being the inhibitory
effect of the co-treatment of 2 drugs, while EA and EB are the
inhibitory effects of the single drugs.
Apoptosis assay
Apoptosis was measured using an Annexin-V-FITC
Apoptosis Detection kit (BD Bioscience, Franklin Lakes, NJ, USA),
according to the manufacturer's protocol. Briefly, following
single- or combined-agent drug treatments, 1×105 cells were washed
twice with cold PBS and resuspended in 500 µl binding buffer for
Annexin-V and propidium iodide (PI) staining. After staining,
~20,000 cells were analyzed using a FACS Arial II system (BD
Biosciences). Annexin-V+PI- cells were analyzed as apoptotic and
Annexin-V+PI+ cells were regarded as necrotic cells.
RNA isolation and reverse
transcription-quantitative polymerase chain reaction (RT-qPCR)
Total RNA of HCC cells following single or combined
treatment was isolated using TRIzol (Thermo Fisher Scientific,
Inc., Waltham, MA, USA), according to the manufacturer's protocol.
1 mg total RNA from each sample was reverse-transcribed to cDNA
using a PrimeScript® RT reagent kit (Takara Bio, Inc.,
Otsu, Japan), according to the manufacturer's protocol. RT-qPCR was
performed using SYBR® Premix Ex Taq™ (Takara Bio, Inc.),
according to the manufacturer's protocol, and cDNA amplification
was detected using a 7500 RT-PCR system (Applied Biosystems; Thermo
Fisher Scientific, Inc.) for 40 cycles at 95°C 5 sec and 60°C 30
sec. Relative gene expression was quantified using the
2−ΔΔCq method (28). The
sequences of each primer used are listed in Table I (Invitrogen; Thermo Fisher
Scientific, Inc.).
 | Table I.Primer sequences of TRAIL and GAPDH
for Real-time PCR. |
Table I.
Primer sequences of TRAIL and GAPDH
for Real-time PCR.
| Gene | Chains | Primer
sequence |
|---|
| GAPDH | Sense |
AGAAGGCTGGGGCTCATTT |
|
| Antisense |
AGGGGCCATCCACAGTCTTC |
| TRAIL | Sense |
GAAGCAACACATTGTCTTCTCCAA |
|
| Antisense |
TTGCTCAGGAATGAATGCCC |
Western blot analysis
Western blotting was performed as previously
described (7). Briefly, HCC cells
were harvested following single or combined drug treatment by
scraping. The cells were incubated with lysis buffer (1 mmol/l
EGTA, 150 mmol/l NaCl, 1% Triton X-100, 2.5 mmol/l sodium
pyrophosphate, 1 mmol/l PMSF, 1 mmol/l Na3VO4, 1 mg/ml leupeptin, 1
mg/ml aprotinin, 5 mmol/l NaF in 20 mmol/l Tris-HCl buffer, pH
7.5). Cell lysates were centrifuged at 13,000 × g, 4°C for 30 min.
Protein concentration was determined using the BCA protein analysis
(Thermo Fisher Scientific, Inc.) and 40 µg of protein from each
sample of protein were separated by 10% SDS-PAGE gels. The
separated proteins were transferred onto PVDF membranes. After
blocking with 5% nonfat dry milk in double-distilled water at room
temperature for 1 h, membranes were washed 3 times with TBS
containing 0.1% Tween (TBS-T) at room temperature for 5 min each
time and incubated overnight at 4°C with anti-TRAIL (cat. no.
3219S; Cell Signaling Technology, Danvers, MA, USA) and anti-GAPDH
(cat. no. 5174S; Cell Signaling Technology) at a 1:1,000 dilutions
overnight. The membranes were washed 3 times with TBS-T at room
temperature for 5 min each time, followed by 1 h incubation at room
temperature in a 1:1,000 dilution of horseradish peroxidase
conjugated goat anti-rabbit secondary antibody (cat. no.
111-035-003; Jackson Laboratory for Genomic Medicine, Farmington,
CT, USA). Following incubation, membranes were washed 3 times with
TBS-T and were visualized by enhanced chemiluminescence (Pierce ECL
Western Blotting Substrate; Thermo Fisher Scientific, Inc.).
RNA silencing
TRAIL was downregulated in HCC cells using siRNA
duplexes (GenePharma, Co., Ltd., Shanghai, China). Briefly,
untreated Huh7 cells were seeded in a 6-well plate at 5×105 cells
per well, and incubated overnight for attachment. After growing to
80–90% confluency, the cells were transfected with 20 nM TRAIL
siRNA or negative control (the sequences of all siRNA are listed in
Table II) using Lipofectamine 2000
(Thermo Fisher Scientific, Inc.), according to the manufacturer's
protocol, in Opti-MEM medium (Gibco; Thermo Fisher Scientific,
Inc.) without FBS. A total of 6 h later, the media was replaced by
DMEM containing 10% FBS. A total of 24 h later, mRNA was used to
detect the efficiency of transfection by RT-qPCR. After 48 h, HCC
cells were treated with 1 µM As2O3 and 5 µM
sorafenib for further research.
| Table II.siRNA sequences of TRAIL and Negative
control. |
Table II.
siRNA sequences of TRAIL and Negative
control.
| siRNA | Chains | Primer
sequence |
|---|
| TRAIL | Sense |
UCCGUCAGCUCGUUAGAAATT |
| Negative
control | Sense |
UUCUCCGAACGUGUCACGUdTdT |
Statistical analysis
All analyses were performed using SPSS software
(version 13.0; SPSS Inc., Chicago, IL, USA). Data are expressed as
the mean ± standard error of the mean. Normality was assessed by
Shapiro-Wilk test. One-way analysis of variance or Kruskal Wallis
testing was used for normal or non-normal data, respectively. The
least significant difference test was used for post-hoc multiple
comparisons. P<0.05 was considered to indicate a statistically
significant difference.
Results
Effects of As2O3
and sorafenib, alone and combined, on the proliferation of Huh7 and
97H cells
To investigate the effect of
As2O3 with and without sorafenib on liver
cancer cell lines, Huh7 and 97H, cells were stimulated with drugs
at different concentrations for 72 h. Huh7 proliferation was
significantly inhibited at high doses of
As2O3 (2 µM, 1.174±0.113 vs. 2.882±0.007, in
As2O3-treated and control cells,
respectively; P<0.01; Fig. 1).
Proliferation was suppressed at all concentrations of sorafenib
alone, even at the lowest dose of 5 µM (1.564±0.070 vs. 2.882±0.007
in sorafenib-treated and control cells, respectively; P<0.01,
Fig. 1). Huh7-cell proliferation was
inhibited in an As2O3-concnetration-dependent
manner when treated with sorafenib in the presence of varying
concentrations of As2O3 (Fig. 1). To determine whether the combined
treatment had a synergistic impact on cell proliferation, the
combination index values of each dose were calculated according to
Jin's formula. At a concentration of 5 µM sorafenib and 1 µM
As2O3, a synergistic effect was evident
(Q=1.7>1.4). The effect on proliferation at high doses (20 µM)
of sorafenib and As2O3 resulted in cell death
(Fig. 1). However, a synergistic
effect was not detected in 97H cells. Inhibition of proliferation
of 97H cells was evident only at high concentrations of sorafenib
(0.795±0.052 vs. 1.495±0.015, in 10 µM sorafenib-treated and
control cells, respectively; P<0.01; 0.359±0.034 vs.
1.495±0.01520 in 20 µM sorafenib-treated and control cells,
respectively; P<0.01; Fig. 1).
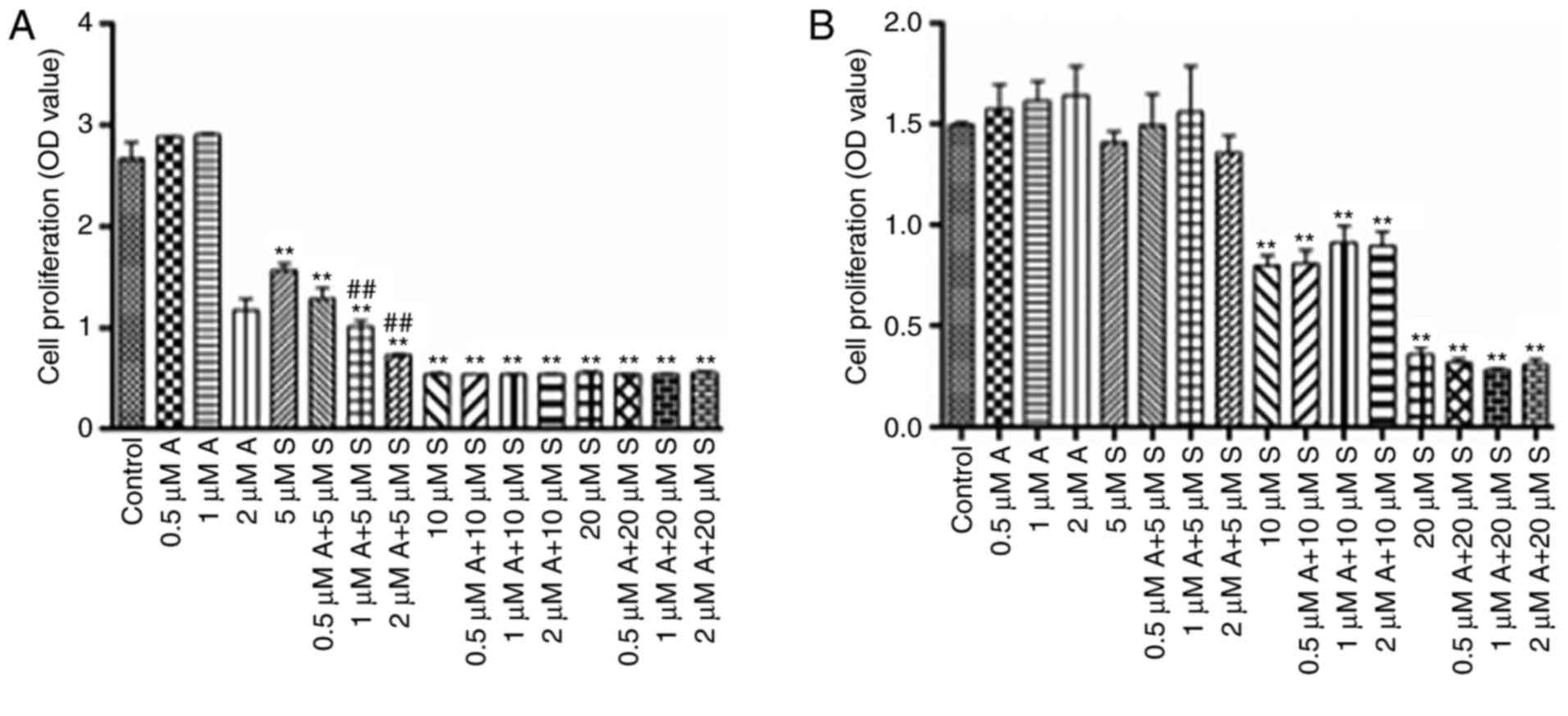 | Figure 1.Effect of As2O3
and sorafenib, alone and combined, on cell proliferation. (A) The
cell proliferation index of Huh7 cells, measured by CCK8 assay. (B)
The cell proliferation index of 97H cells, measured by CCK8 assay.
Data are presented as the mean ± standard deviation and each
experiment was repeated 6 times. **P<0.01, compared with
control, ##P<0.01 compared with 5 µM sorafenib alone. A,
As2O3; As2O3, arsenic
trioxide; S, sorafenib; OD, optical density. |
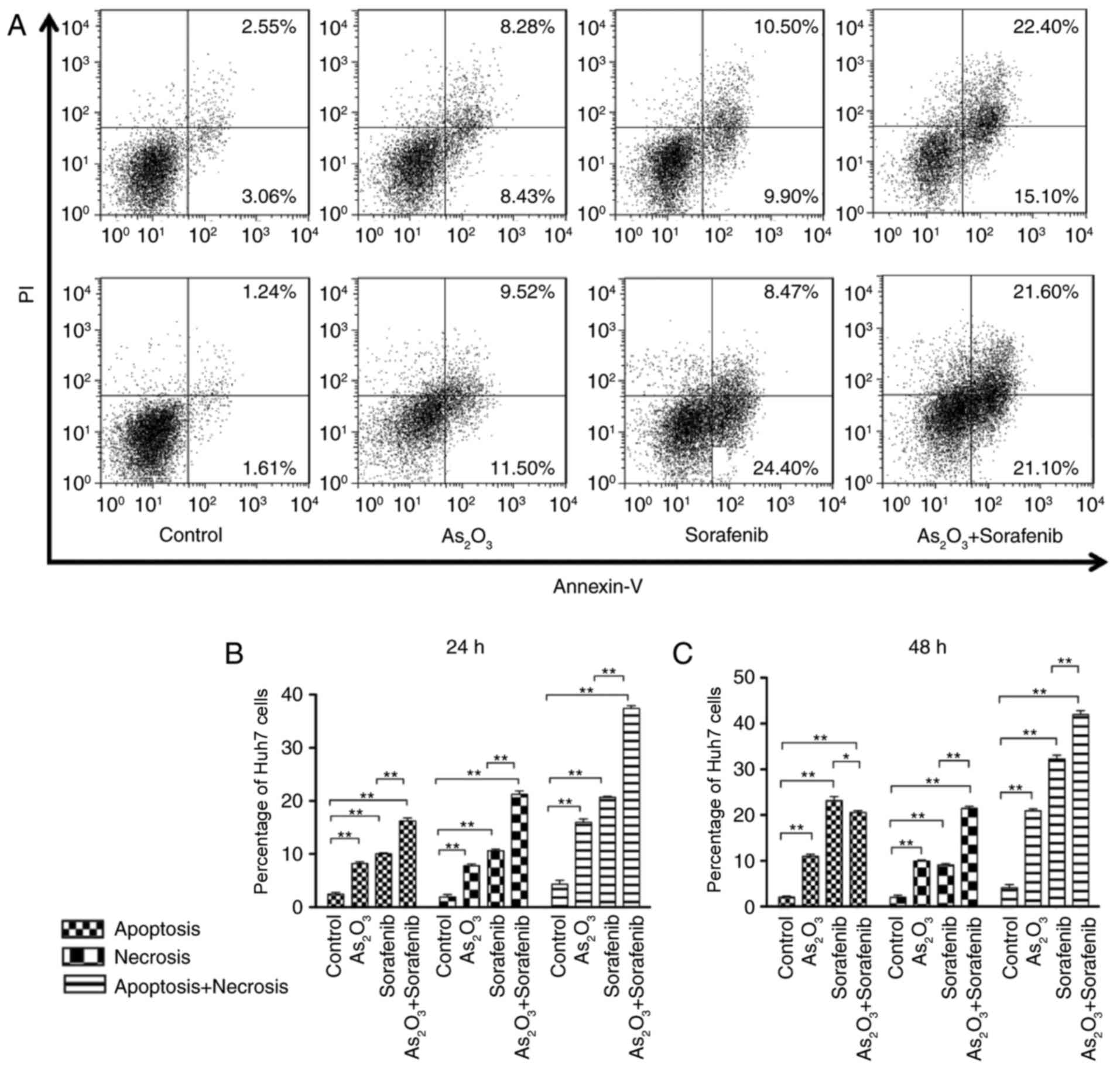
Combined treatment of
As2O3 and sorafenib increases cell death in
Huh7 cells via TRAIL
When treated with 1 µM As2O3,
or 5 µM sorafenib, or a combination of the two drugs, for 24, 48
and 72 h, the apoptotic rate was significantly increased in Huh7
cells. Combination treatment demonstrated a synergistic effect on
apoptosis and necrosis (P<0.01; Fig.
2). After 72 h with combination treatment, almost all Huh7
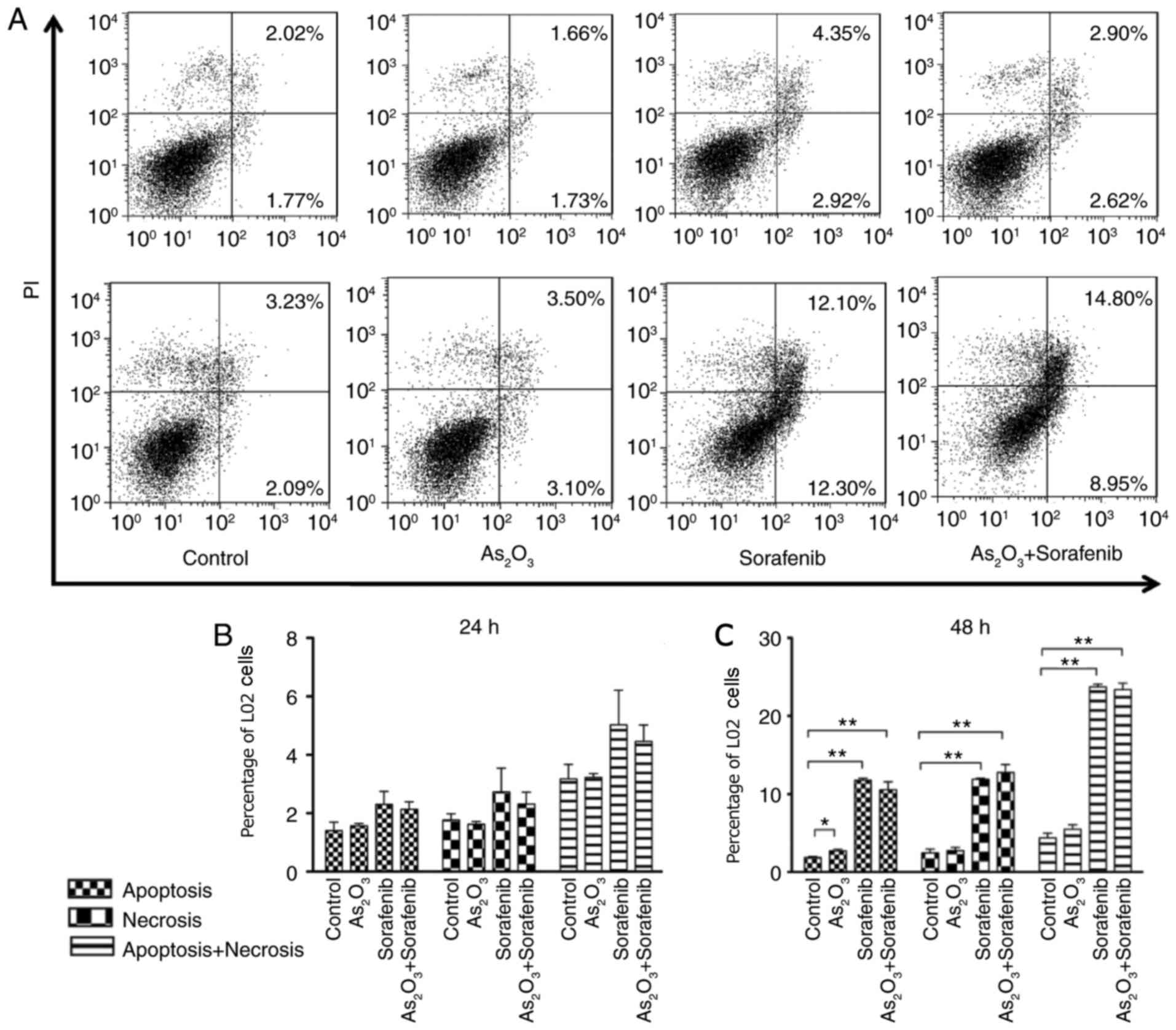
cells were Annexin-V+ (data not shown). Sorafenib resulted in
significantly increased cell death after 48 h in normal liver
(L-02) cells, but not after 24 h (Fig.
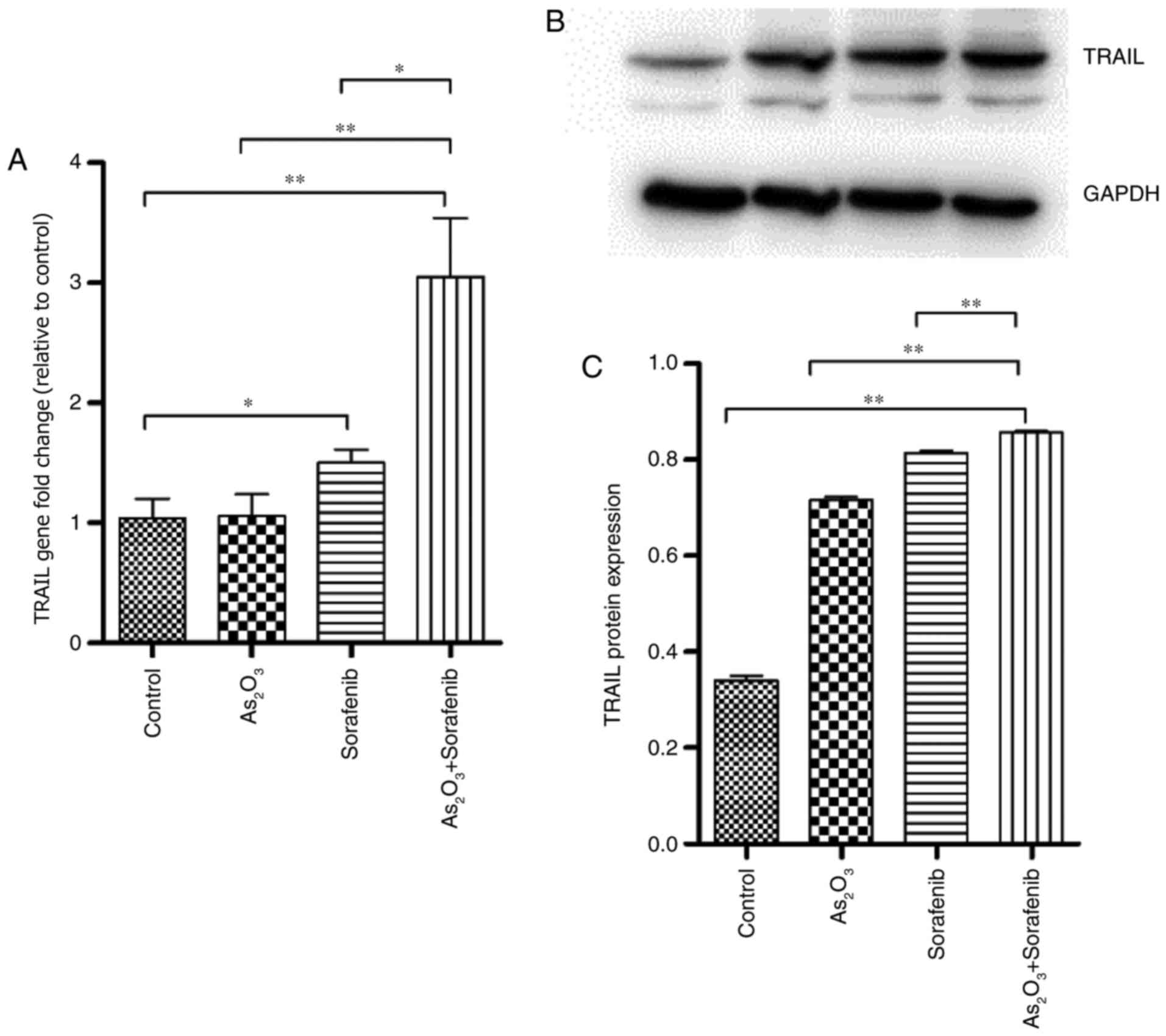
3). A number of genes associated with apoptosis were examined
by RT-qPCR (data not shown), which demonstrated that the gene
expression of TRAIL selectively induced apoptosis in tumor cells
(29). TRAIL expression was
significantly upregulated in the combination treatment group
compared with the control and single treatment groups (Fig. 4A). TRAIL protein expression levels
demonstrated consistent results (Fig. 4B
and C).
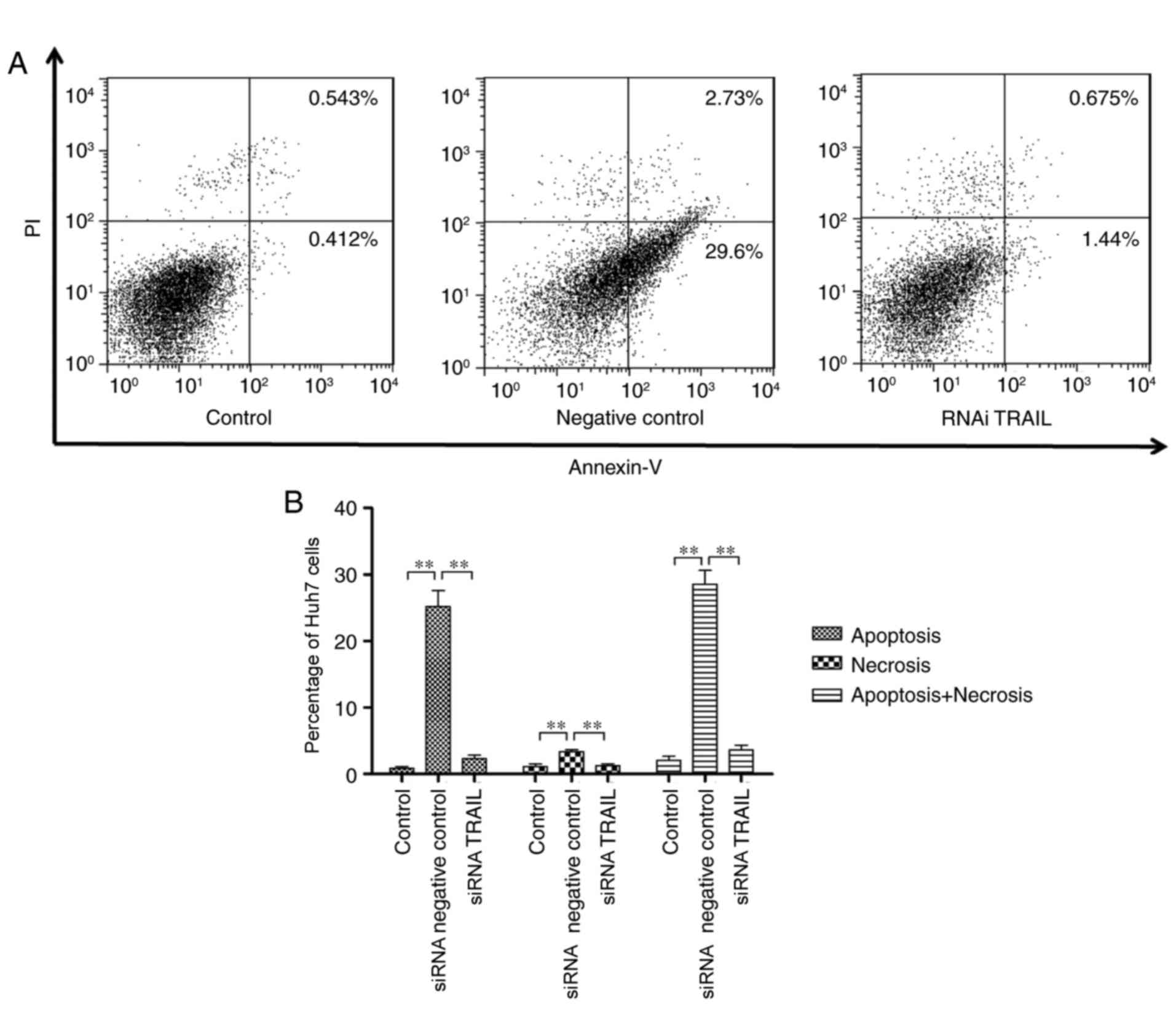
The synergistic effect of
As2O3 and sorafenib on Huh7-cell death is
dependent on TRAIL
In order to investigate whether the synergistic
effect of sorafenib and As2O3 on Huh7-cell
death occurred via a TRAIL-dependent pathway, TRAIL-targeted siRNA
was used to downregulate TRAIL expression for 48 h, after which the
apoptosis of Huh7 cells was analyzed by flow cytometry. The
synergistic effect of As2O3 and sorafenib on
Huh7-cell apoptosis was reversed compared with negative control
(Fig. 5).
As2O3 and
Sorafenib combined treatment enhanced cell death in fresh isolated
HCC cells
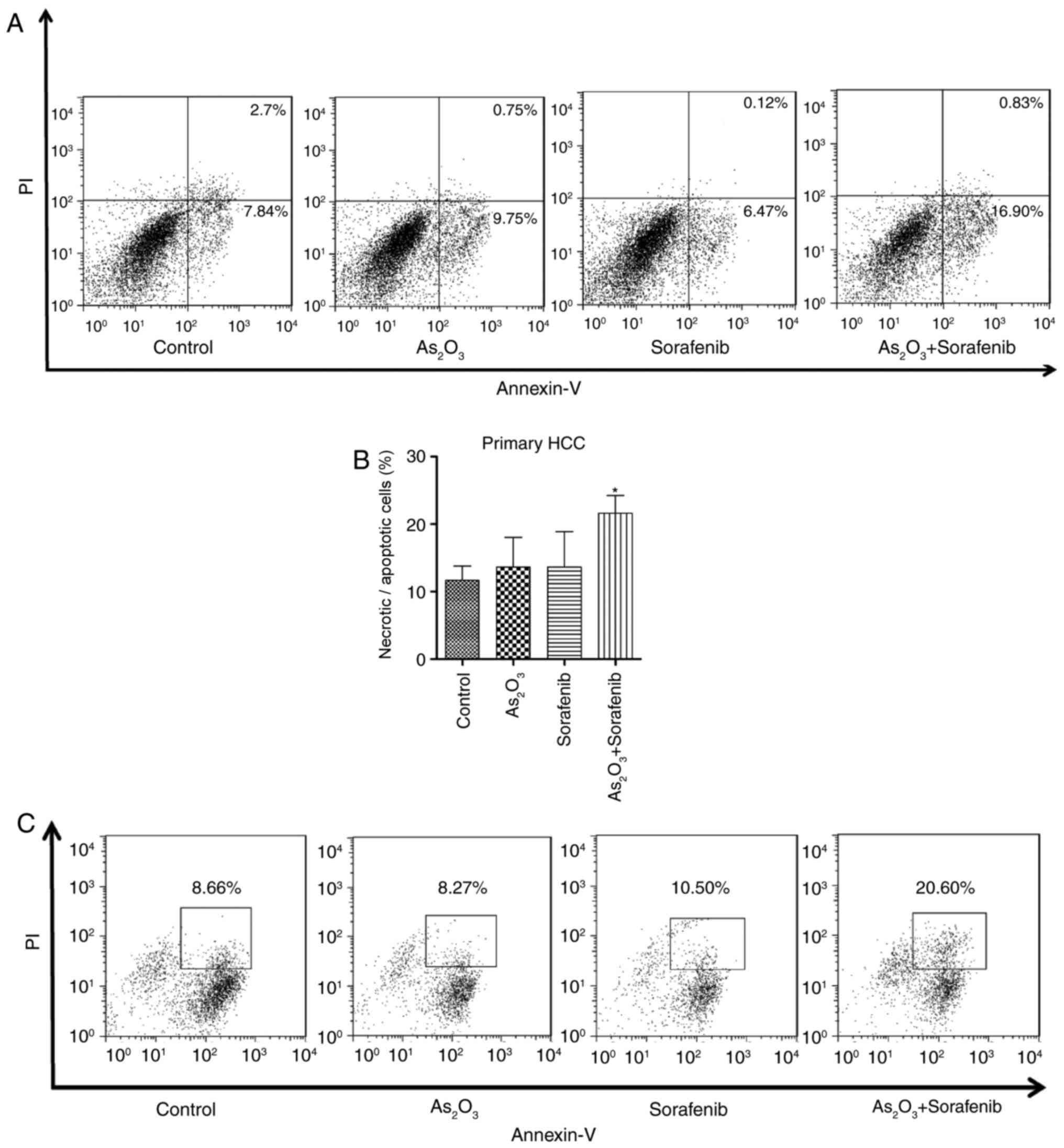
In order to investigate the clinical effect of
As2O3 and sorafenib in combination, the
anti-tumor activity of the combination treatment was analyzed in
freshly isolated HCC cells. Annexin-V/PI staining was performed
after 24 h treatment. The results revealed that cell death was
significantly upregulated in the HCC-patient cells treated with
As2O3 and sorafenib in combination
(P<0.05; Fig. 6). Sorafenib or
As2O3 alone had no effect on tumor cell death
in some of the HCC patients.
Discussion
HCC is a complex and heterogeneous type of tumor,
associated with genomic aberrations (30). A number of signaling cascades,
including mitogen-activated protein kinase (MAPK), VEGF and
phosphoinositide-3-kinase (PI3K) have been demonstrated to be
involved in HCC, and drugs have been designed to target these
signaling pathways (31).
Unfortunately, a number of these drugs, including brivanib,
sunitinib and erlotinib, failed phase III clinical trials (32). Sorafenib, a multikinase inhibitor,
remains the standard treatment for patients with advanced-stage
hepatocellular carcinoma (33). The
standard initial dose of sorafenib is 400 mg, taken orally, twice
daily (34). The high dosage required
can present financial and physical burdens for patients (35). Various adverse effects, including
severe skin rash can occur following sorafenib administration
(36). Therefore, novel therapeutic
approaches to improve sorafenib efficacy at lower dosages are
urgently required.
Previous studies have demonstrated that synergistic
sorafenib therapy such as sorafenib combined with TACE or hepatic
arterial infusion chemotherapy can enhance its antitumor activity
(37). As2O3 is
currently the most effective single agent treatment of APL, with a
dose of 0.16 mg/kg/day allowing complete remission with lower-dose
chemotherapy (38). Furthermore,
As2O3 has been demonstrated to suppress tumor
growth in liver, prostate and breast cancer through
demethylation/apoptosis pathways (39). Research has demonstrated that
As2O3 induced growth arrest of liver cancer,
HepG2 and HepG3B, cells via activation of FOXO3a (39,40).
Furthermore, minimal side effects of As2O3
treatment have been observed (41).
Thus, the combination of As2O3 and sorafenib
has been hypothesized to have potential for effective treatment of
HCC (21).
Although the present study demonstrated that
As2O3 combined with sorafenib executes an
anti-tumor effect by triggering cell death in Huh7 cells, this was
not observed in 97H cells. One reason for this difference may be
different status of cell differentiation. Another is that Huh7
cells are characterized as HBV-negative whereas 97H are
HBV-positive. HBV virus status has been associated with the
effectiveness of sorafenib treatment, HBV-negative patients
receiving sorafenib treatment had an improved OS time (42). HBV virus status may also influence the
effect of As2O3 combined with sorafenib on
HCC cells. Despite the cell type specificity, an advantage of the
combination is the potential for a decreased dosage of sorafenib.
An in vitro dosage of 5 µM sorafenib with
As2O3 corresponds to 50% the therapeutic
plasma level of sorafenib in patients with HCC receiving 400 mg
sorafenib twice daily (43,44). Furthermore, no significant side
effects were demonstrated in the normal liver cell line after 24 h
combination treatment, while sorafenib alone was toxic at 48 h.
This may be associated with the previously reported dose-limiting
toxicities of sorafenib (45). These
findings indicate that even at a low dosage of 5 µM, sorafenib
impacts the viability of normal liver cells, further supporting the
investigation of combined regimens, to achieve improved anti-tumor
efficacy and minimized toxicity.
Programmed cell death (PCD) is an important cellular
mechanism whose dysregulation has been reported to be involved in
tumor formation (46). Induction of
PCD is the best-characterized cause of cell death in most cell
types (47). Seeing as
As2O3 and sorafenib induce apoptosis in human
cancer cell lines (48,49), the synergic effect of sorafenib with
As2O3 on human liver cancer cell apoptosis
pathways was investigated. It was revealed that TRAIL, closely
associated with PCD (50), was
upregulated in the As2O3 and sorafenib
combined-treatment group compared with untreated cells.
Downregulation of TRAIL expression in the combined group
significantly reduced the rate of PCD in HCC cells. These results
indicate a close association between TRAIL and PCD-induction in
HCC. TRAIL not only serves a role in induction of cell death, but
also as a key effector in the immune system (51). It has been demonstrated that TRAIL-/-
mice were more susceptible to autoimmune diseases such as arthritis
and diabetes (52). Further study is
required to investigate whether the As2O3 and
sorafenib combination causes HCC-cell death by impacting the tumor
immune microenvironment as well as inducing tumor-cell PCD.
To determine the value of the combination of
As2O3 and sorafenib in clinical practice,
freshly isolated HCC cells were collected from HCC patients who
underwent surgery. The results confirmed that the combination
treatment induces HCC-cell death. This result supports further
clinical investigations of this combined treatment, particularly as
the primary HCC cells were only sensitive to the combined
treatment, and not to sorafenib or As2O3
alone. Recently, it has been reported that targeted TRAIL gene
therapy may provide a potential strategy for HCC therapy in a
preclinical setting (53). The
results of the present study suggest that targeted TRAIL therapy,
based on the success of sorafenib/As2O3
treatment, may benefit patients with HCC.
The present study demonstrates that
As2O3 and sorafenib combination treatment
causes HCC-cell death via the TRAIL signaling pathway. Furthermore,
the combination had potent anti-tumor activity in freshly isolated
HCC cells from patients with HCC patients, while these cells were
resistant to the treatment of sorafenib or
As2O3 alone. The authors acknowledge that
these findings need to be validated in vivo. However, the
significance of the present study lies with the potential of a
novel therapeutic target. Therefore, clinical research of
As2O3 and sorafenib combination treatment of
HCC should be prioritized. However, the anti-tumor activity of this
combination was demonstrated to be cell type specific, which is
likely associated with the HBV virus infection. The underlying
mechanisms of this effect also require further investigation.
Acknowledgements
Not applicable.
Funding
The present study was supported by grants from
National Natural Science Foundation of China (grant nos. 81470282
and 81170473) and Zhongshan Hospital (grant no., 2015ZSYXGG09).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
YW and YC conceived the study. LW, YW and YC
performed the literature review, and drafted and revised the
manuscript. YW and YC critically revised the manuscript. LW, ZM,
XW, MH, DS and ZR performed the experiments and analyzed data. All
authors read and approved the final manuscript.
Ethics approval and consent to
participate
The present study was performed in accordance with
the ethical standards formulated in the Declaration of Helsinki,
and was approved by Medical Ethics Committee of Zhongshan Hospital
(Fudan University, Shanghai, China). Written informed consent was
obtained from each patient prior to inclusion in the present
study.
Consent for publication
All participants provided written informed consent
for the publication of any associated data and accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
HCC
|
human hepatocellular carcinoma
|
|
HBV
|
hepatitis B virus
|
|
HCV
|
hepatitis C virus
|
|
RF(T)A
|
radiofrequency (thermal) ablation
|
|
VEGF
|
vascular endothelial growth factor
|
|
As2O3
|
arsenic trioxide
|
|
APL
|
acute promyelocytic leukemia
|
|
TRAIL
|
TNF-related apoptosis-inducing
ligand
|
|
MAPK
|
mitogen-activated protein kinase
|
|
PI3K
|
phosphatidylinostol-3-kinase
|
|
PCD
|
programmed cell death
|
References
|
1
|
Yang Y, Zhao LH, Huang B, Wang RY, Yuan
SX, Tao QF, Xu Y, Sun HY, Lin C and Zhou WP: Pioglitazone, a PPARγ
agonist, inhibits growth and invasion of human hepatocellular
carcinoma via blockade of the rage signaling. Mol Carcinog.
54:1584–1595. 2015. View
Article : Google Scholar : PubMed/NCBI
|
|
2
|
Mgaieth S, Kemp W, Gow P, Fink M, Lubel J,
Nicoll A, Gazzola A, Hong T, Ryan M and Knight V: Impact of viral
hepatitis aetiology on survival outcomes in hepatocellular
carcinoma: A large multicentre cohort study. J Viral Hepat.
24:982–989. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tornai I: Role of environmental factors in
the etiology of hepatocellular carcinoma. Orv Hetil. 151:1132–1136.
2010.(In Hungarian). View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lischalk JW, Repka MC and Unger K:
Radiation therapy for hepatobiliary malignancies. J Gastrointest
Oncol. 8:279–292. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Rich NE, Parikh ND and Singal AG:
Hepatocellular carcinoma and liver transplantation: Changing
patterns and practices. Curr Treat Options Gastroenterol.
15:296–304. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yu WB, Rao A, Vu V, Xu L, Rao JY and Wu
JX: Management of centrally located hepatocellular carcinoma:
Update 2016. World J Hepatol. 9:627–634. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chen CH, Chen MC, Wang JC, Tsai AC, Chen
CS, Liou JP, Pan SL and Teng CM: Synergistic interaction between
the HDAC inhibitor, MPT0E028, and sorafenib in liver cancer cells
in vitro and in vivo. Clin Cancer Res. 20:1274–1287. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zhu YJ, Zheng B, Wang HY and Chen L: New
knowledge of the mechanisms of sorafenib resistance in liver
cancer. Acta Pharmacol Sin. 38:614–622. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S,
Kim JS, Luo R, Feng J, Ye S, Yang TS, et al: Efficacy and safety of
sorafenib in patients in the Asia-Pacific region with advanced
hepatocellular carcinoma: A phase III randomised, double-blind,
placebo-controlled trial. Lancet Oncol. 10:25–34. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Liu LL, Zhang MF, Pan YH, Yun JP and Zhang
CZ: NORE1A sensitises cancer cells to sorafenib-induced apoptosis
and indicates hepatocellular carcinoma prognosis. Tumour Biol.
35:1763–1774. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Karashima T, Komatsu T, Niimura M, Kawada
C, Kamada M, Inoue K, Udaka K, Kuroda N and Shuin T: Novel
combination therapy with imiquimod and sorafenib for renal cell
carcinoma. Int J Urol. 21:702–706. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Luu T, Frankel P, Chung C, Chow W,
Mortimer J, Hurria A and Somlo G: Phase I/II trial of vinorelbine
and sorafenib in metastatic breast cancer. Clin Breast Cancer.
14:94–100. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ravandi F, Yi Arana C, Cortes JE, Levis M,
Faderl S, Garcia-Manero G, Jabbour E, Konopleva M, O'Brien S,
Estrov Z, et al: Final report of phase II study of sorafenib,
cytarabine and idarubicin for initial therapy in younger patients
with acute myeloid leukemia. Leukemia. 28:1543–1545. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wörns MA and Galle PR: HCC
therapies-lessons learned. Nat Rev Gastroenterol Hepatol.
11:447–452. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Emadi A and Gore SD: Arsenic trioxide-An
old drug rediscovered. Blood Rev. 24:191–199. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Miller WH Jr, Schipper HM, Lee JS, Singer
J and Waxman S: Mechanisms of action of arsenic trioxide. Cancer
Res. 62:3893–3903. 2002.PubMed/NCBI
|
|
17
|
Zheng CY, Lam SK, Li YY, Fong BM, Mak JC
and Ho JC: Combination of arsenic trioxide and chemotherapy in
small cell lung cancer. Lung Cancer. 82:222–230. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Thomas-Schoemann A, Batteux F, Mongaret C,
Nicco C, Chéreau C, Annereau M, Dauphin A, Goldwasser F, Weill B,
Lemare F and Alexandre J: Arsenic trioxide exerts antitumor
activity through regulatory T cell depletion mediated by oxidative
stress in a murine model of colon cancer. J Immunol. 189:5171–5177.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yang X, Sun D, Tian Y, Ling S and Wang L:
Metformin sensitizes hepatocellular carcinoma to arsenic
trioxide-induced apoptosis by downregulating Bcl2 expression.
Tumour Biol. 36:2957–2964. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lin CC, Hsu C, Hsu CH, Hsu WL, Cheng AL
and Yang CH: Arsenic trioxide in patients with hepatocellular
carcinoma: A phase II trial. Invest New Drugs. 25:77–84. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Zhai B, Jiang X, He C, Zhao D, Ma L, Xu L,
Jiang H and Sun X: Arsenic trioxide potentiates the anti-cancer
activities of sorafenib against hepatocellular carcinoma by
inhibiting Akt activation. Tumour Biol. 36:2323–2334. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Moloudi K, Neshasteriz A, Hosseini A,
Eyvazzadeh N, Shomali M, Eynali S, Mirzaei E and Azarnezhad A:
Synergistic effects of arsenic trioxide and radiation: Triggering
the intrinsic pathway of apoptosis. Iran Biomed J. 21:330–337.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Xu Y, Li J, Li QJ, Feng YL and Pan F:
Betulinic acid promotes TRAIL function on liver cancer progression
inhibition through p53/Caspase-3 signaling activation. Biomed
Pharmacother. 88:349–358. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kong X, Luo J, Xu T, Zhou Y, Pan Z, Xie Y,
Zhao L, Lu Y, Han X, Li Z and Liu L: Plumbagin enhances
TRAIL-induced apoptosis of human leukemic Kasumi-1 cells through
upregulation of TRAIL death receptor expression, activation of
caspase-8 and inhibition of cFLIP. Oncol Rep. 37:3423–3432. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Clarke N, Jimenez-Lara AM, Voltz E and
Gronemeyer H: Tumor suppressor IRF-1 mediates retinoid and
interferon anticancer signaling to death ligand TRAIL. EMBO J.
23:3051–3060. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Cretney E, Takeda K, Yagita H, Glaccum M,
Peschon JJ and Smyth MJ: Increased susceptibility to tumor
initiation and metastasis in TNF-related apoptosis-inducing
ligand-deficient mice. J Immunol. 168:1356–1361. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Zhang H, Liu K, Xue Z, Yin H, Dong H, Jin
W, Shi X and Wang H and Wang H: High-voltage pulsed electric field
plus photodynamic therapy kills breast cancer cells by triggering
apoptosis. Am J Transl Res. 10:334–351. 2018.PubMed/NCBI
|
|
28
|
Livak KJ and Scmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Hellwig CT and Rehm M: TRAIL signaling and
synergy mechanisms used in TRAIL-based combination therapies. Mol
Cancer Ther. 11:3–13. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Cho HJ, Kim SS, Wang HJ, Kim BW, Cho H,
Jung J, Cho SS, Kim JK, Lee JH, Kim YB, et al: Detection of novel
genomic markers for predicting prognosis in hepatocellular
carcinoma patients by integrative analysis of copy number
aberrations and gene expression profiles: Results from a long-term
follow-up. DNA Cell Biol. 35:71–80. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ho DW, Lo RC, Chan LK and Ng IO: Molecular
pathogenesis of hepatocellular carcinoma. Liver Cancer. 5:290–302.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Llovet JM and Hernandez-Gea V:
Hepatocellular carcinoma: Reasons for phase III failure and novel
perspectives on trial design. Clin Cancer Res. 20:2072–2079. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Abeni E, Salvi A, Marchina E, Traversa M,
Arici B and De Petro G: Sorafenib induces variations of the DNA
methylome in HA22T/VGH human hepatocellular carcinoma-derived
cells. Int J Oncol. 51:128–144. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Kobayashi S, Ohkawa S, Kondo M, Morimoto
M, Numata K, Matsunaga K, Okuse C, Suzuki M, Hidaka H, Takada J, et
al: Influence of body surface area on efficacy and safety of
sorafenib in advanced hepatocellular carcinoma. Gan To Kagaku
Ryoho. 39:1065–1070. 2012.(In Japanese). PubMed/NCBI
|
|
35
|
Ziogas IA and Tsoulfas G: Evolving role of
Sorafenib in the management of hepatocellular carcinoma. World J
Clin Oncol. 8:203–213. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Tsuchiya N, Narita S, Inoue T, Hasunuma N,
Numakura K, Horikawa Y, Satoh S, Notoya T, Fujishima N, Hatakeyama
S, et al: Risk factors for sorafenib-induced high-grade skin rash
in Japanese patients with advanced renal cell carcinoma. Anticancer
Drugs. 24:310–314. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Kudo M: Signaling pathway/molecular
targets and new targeted agents under development in hepatocellular
carcinoma. World J Gastroenterol. 18:6005–6017. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Breccia M and Lo-Coco F: Arsenic trioxide
for management of acute promyelocytic leukemia: Current evidence on
its role in front-line therapy and recurrent disease. Expert Opin
Pharmacother. 13:1031–1043. 2102. View Article : Google Scholar
|
|
39
|
Wang X, Jiang F, Mu J, Ye X, Si L, Ning S,
Li Z and Li Y: Arsenic trioxide attenuates the invasion potential
of human liver cancer cells through the demethylation-activated
microRNA-491. Toxicol Lett. 227:75–83. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Fei M, Lu M, Wang Y, Zhao Y, He S, Gao S,
Ke Q, Liu Y, Li P, Cui X, et al: Arsenic trioxide-induced growth
arrest of human hepatocellular carcinoma cells involving FOXO3a
expression and localization. Med Oncol. 26:178–185. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Rangwala F, Williams KP, Smith GR, Thomas
Z, Allensworth JL, Lyerly HK, Diehl AM, Morse MA and Devi GR:
Differential effects of arsenic trioxide on chemosensitization in
human hepatic tumor and stellate cell lines. BMC Cancer.
12:4022012. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Jackson R, Psarelli EE, Berhane S, Khan H
and Johnson P: Impact of viral status on survival in patients
receiving sorafenib for advanced hepatocellular cancer: A
meta-analysis of randomized phase III trials. J Clin Oncol.
35:622–628. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Alsaied OA, Sangwan V, Banerjee S, Krosch
TC, Chugh R, Saluja A, Vickers SM and Jensen EH: Sorafenib and
triptolide as combination therapy for hepatocellular carcinoma.
Surgery. 156:270–279. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Hu S, Niu H, Inaba H, Orwick S, Rose C,
Panetta JC, Yang S, Pounds S, Fan Y, Calabrese C, et al: Activity
of the multikinase inhibitor sorafenib in combination with
cytarabine in acute myeloid leukemia. J Natl Cancer Inst.
103:893–905. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Abou-Alfa GK, Schwartz L, Ricci S, Amadori
D, Santoro A, Figer A, De Greve J, Douillard JY, Lathia C, Schwartz
B, et al: Phase II study of sorafenib in patients with advanced
hepatocellular carcinoma. J Clin Oncol. 24:4293–4300. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Mishra AP, Salehi B, Sharifi-Rad M,
Pezzani R, Kobarfard F, Sharifi-Rad J and Nigam M: Programmed cell
death, from a cancer perspective: An overview. Mol Diagn Ther. Mar
20–2018.(Epub ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Voigt S, Philipp S, Davarnia P,
Winoto-Morbach S, Röder C, Arenz C, Trauzold A, Kabelitz D, Schütze
S, Kalthoff H and Adam D: TRAIL-induced programmed necrosis as a
novel approach to eliminate tumor cells. BMC Cancer. 14:742014.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Oh SJ, Erb HH, Hobisch A, Santer FR and
Culig Z: Sorafenib decreases proliferation and induces apoptosis of
prostate cancer cells by inhibition of the androgen receptor and
Akt signaling pathways. Endocr Relat Cancer. 19:305–319. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Zhang XH, Feng R, Lv M, Jiang Q, Zhu HH,
Qing YZ, Bao JL, Huang XJ and Zheng XL: Arsenic trioxide induces
apoptosis in B-cell chronic lymphocytic leukemic cells through
down-regulation of survivin via the p53-dependent signaling
pathway. Leuk Res. 37:1719–1725. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Liu JJ, Wang W, Dicker DT and El-Deiry WS:
Bioluminescent imaging of TRAIL-induced apoptosis through detection
of caspase activation following cleavage of DEVD-aminoluciferin.
Cancer Biol Ther. 4:885–892. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Diao Z, Shi J, Zhu J, Yuan H, Ru Q, Liu S,
Liu Y and Zheng D: TRAIL suppresses tumor growth in mice by
inducing tumor-infiltrating CD4(+)CD25 (+) Treg apoptosis. Cancer
Immunol Immunother. 62:653–663. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Lamhamedi-Cherradi SE, Zheng SJ, Maguschak
KA, Peschon J and Chen YH: Defective thymocyte apoptosis and
accelerated autoimmune diseases in TRAIL-/- mice. Nat Immunol.
4:255–260. 2003. View
Article : Google Scholar : PubMed/NCBI
|
|
53
|
Galal El-Shemi A, Mohammed Ashshi A, Oh E,
Jung BK, Basalamah M, Alsaegh A and Yun CO: Efficacy of combining
ING4 and TRAIL genes in cancer-targeting gene virotherapy strategy:
First evidence in preclinical hepatocellular carcinoma. Gene Ther.
25:54–65. 2018. View Article : Google Scholar : PubMed/NCBI
|