Introduction
Endometriosis is defined as the presence of
functioning endometrial glands and stroma outside the uterus, most
commonly in the pelvic peritoneum and ovaries. This disorder is a
benign estrogen-dependent disease of reproductive age, although
ovarian endometrioma (OE) increases the subsequent risk of
developing endometriosis-associated ovarian cancer (EAOC) (1,2). EAOC
occurs in 0.72% of women with endometriosis in Japan (1). The risk factors for malignant
transformation include older age (>45 years old) and large tumor
size (>7 cm) (2). Ovarian cancer
is an important cause of cancer morbidity and mortality, largely
due to the late stage of presentation. The mechanisms involved in
malignant transformations warrant further investigation.
Repeated bleeding episodes occur in endometriosis
and result in a local accumulation of hemoglobin, heme and iron
species (3), which leads to increased
formation of reactive oxygen species (ROS) (4). Generally, ROS consist principally of
molecules including the superoxide anion
(O2−), hydroxyl radicals (•OH) and hydrogen
peroxide (H2O2). 8-hydroxy-2-deoxyguanosine
(8-OHdG) is considered to be a biomarker of ROS-mediated DNA
damage, as guanosine is the most oxidized among the DNA nucleobases
(5). Toxic heme also induces a
stress-responsive enzyme, heme oxygenase-1 (HO-1), that is
responsible for the degradation of heme to carbon monoxide (CO),
bilirubin and iron (6). HO-1 and
their products exert beneficial effects through protection against
oxidative injury. In response to an excess of ROS, macrophages
secrete antioxidants, and regulate redox signaling and the
inflammatory microenvironment, via control of the expression of a
transcription factor, NRF2 (Nuclear factor erythroid-derived factor
2-related factor 2), during endometriosis regeneration (3). NRF2 also regulates the expression of
HO-1 and antioxidants. HO-1 is thought to be an oxidative stress
marker (6,7). On the other hand, the combined activity
of all antioxidants is measured via the total antioxidant capacity
(TAC), instead of measuring the activity of each agent separately,
for example superoxide dismutase (SOD), catalase (CAT) and
glutathione peroxidase (GSH-Px) (8).
TAC/Heme-iron reflects the antioxidant capacity of water-soluble
molecules, since the majority of iron exists as heme-iron in OE and
EAOC cyst fluid samples (9).
Oxidative stress may be involved in the progression
of the malignant transformation of endometriosis (10,11).
However, no reports on the oxidant-antioxidant profile in the cyst
fluid of patients suffering from OE and EAOC exist, to the best of
our knowledge. The aim of this study was to analyze redox
biomarkers, pro-oxidants (the in vivo DNA damage marker
8-OHdG, and the oxidative stress marker HO-1) and antioxidants
(TAC/Heme-iron) in the cyst fluids of patients with benign OE and
already-growing EAOC.
Materials and methods
Patient selection
Τhe present study was conducted on 14
histopathologically confirmed cases of EAOC and the 44 cases of
benign OE. To avoid selection bias in the EAOC cases, morphological
documentation of the continuous transition from benign
endometriotic epithelial cells to atypical endometriosis, and
finally to invasive carcinoma, was confirmed within the same
specimen. A total of 58 cyst fluid sample specimens were collected
from the Department of Gynecology at Nara Medical University
Hospital, Japan, between January 2006 and December 2012. Specific
exclusion criteria considered for the present study were acute or
chronic diseases, including diabetes, immune dysfunction or any
other malignancy. None of the study subjects were under antioxidant
supplementation, hormonal therapy or chemotherapy prior to the
surgery. The data on patient demographic features and
clinicopathological characteristics were collected from a database
containing comprehensive medical records and pathology reports. The
protocols were approved by The Ethics Committee of Nara Medical
University (reference no. 2012-541). Written informed consent was
obtained from each study subject, and all subjects consented to
donate cyst fluid samples.
Analytical methods
Cyst fluid samples were collected at the time of
surgery. Following centrifugation at 3,000 × g for 15 min,
specimens were immediately aliquoted and frozen at −70°C within 1 h
of collection. A histological diagnosis was confirmed via surgical
pathology.
Estimation of 8-OHdG and HO-1
Cyst fluid samples were used for the measurement of
8-hydroxy-2-deoxy guanosine (8-OHdG) levels using a competitive
in vitro ELISA kit (Catalog# KOG-HS10/EC, NIKKEN SEIL Co.,
Ltd, Shizuoka, Japan), and HO-1 levels using
StressXpress® HO-1 ELISA kits (Catalog# SKT-111-96,
StressMarq Biosciences, Inc., Victoria, BC, Canada). Dilution
linearity and parallelism, in addition to intra- and inter-assay
variability, were assessed using in-house calibrators. The two
ELISA kits exhibited a linear response in the range of ≥3 orders of
magnitude. The assay variances of all methods described above were
<10%.
Assay of total antioxidant status
Total antioxidant capacity (TAC) in the cyst fluid
was measured using the TAC Assay kit (Metallogenics Co., Ltd.,
Chiba, Japan), which uses a copper (II) reduction assay with
bathocuproinedisulfonic acid disodium salt as the chelating agent
(the CUPRAC-BCS assay). This assay was applied to measure the
antioxidants as reductants in a redox-linked colorimetric procedure
using a spectrophotometer (Bio Aquarius; Cecil Instruments Ltd.,
Cambridge, UK), as described previously (12,13).
Measurement of heme iron
concentration
Cyst fluids were added to 96-well plates and
alkalized with NaOH to adjust the pH to >10. The resultant
solution was subjected to heme measurement using the Metalloassay
LS Heme Assay kit (Metallogenics Co., Ltd.), based on the
Triton-methanol colorimetric assay (14). The optical density at 400 nm was
determined using a microtiter plate reader.
Statistical analysis
All values are expressed as the mean ± standard
deviation. Differences between the groups of patients were
estimated by Mann-Whitney U test. Categorical variables are
presented as absolute numbers (frequency percentages) and analyzed
via the χ2 test. Correlations between levels of
oxidative stress biomarkers and antioxidant status were evaluated
using Pearson's correlation coefficient. Receiver Operative
Characterisitic (ROC) curve analysis was used to identify the best
discriminating threshold of the cyst fluid iron levels for
differential diagnosis between EAOC and OE. Analyses were performed
using SPSS (v.22.0; IBM Corp., Armonk, NY, USA). P<0.05 was
considered to indicate a statistically significant difference.
Results
Baseline characteristics
The principal clinical and pathological
characteristics of the subjects with benign OE and patients with
EAOC are presented in Table I. Age
(P=0.001), premenopausal status (P=0.001) and the maximum diameter
of the cyst (P=0.006) differed significantly between the two
groups. There were no statistical differences in parity and serum
CA125 levels between the two groups (P>0.05).
 | Table I.Clinical and tumor characteristics of
the study population. |
Table I.
Clinical and tumor characteristics of
the study population.
| Baseline
characteristics of two groups | Benign endometrioma
group |
Endometriosis-associated ovarian cancer
group | P-value |
|---|
| Nο. | 44 | 14 |
|
| Age at
diagnosis, |
| Mean ±
SD | 36.9±8.4 | 50.0±13.2 | 0.001 |
| Median
(range) | 38.0 (21–62) | 44.5 (36–78) |
|
| Nulliparous n
(%) | 19 (43.2%) | 7 (50.0%) | 0.665 |
| Premenopause n
(%) | 42 (95.5%) | 9 (64.2%) | 0.007 |
| Tumor size
(cm)a |
| Mean ±
SD | 7.12±2.78 | 12.0±6.43 | 0.006 |
| Median
(range) | 6.8 (2.7–13.6) | 10.6 (4.2–25.5) |
|
| CA125 |
| Mean ±
SD | 92.1±70.3 | 375.2±658.0 |
|
| Median
(range) | 66.5 (10–316) | 47.0
(7.0–2141) | 0.531 |
| Pathology | Endometriosis | Clear cell
(n=6) |
|
|
|
| Endometrioid
(n=1) |
|
|
|
| Serous (n=3) |
|
|
|
| Mucinous (n=1) |
|
|
|
| Other (n=3) |
|
| The international
federation of gynecology | – | IA (n=3) |
|
| and obstetrics
stage |
| IC (n=10) |
|
|
|
| IIIC (n=1) |
|
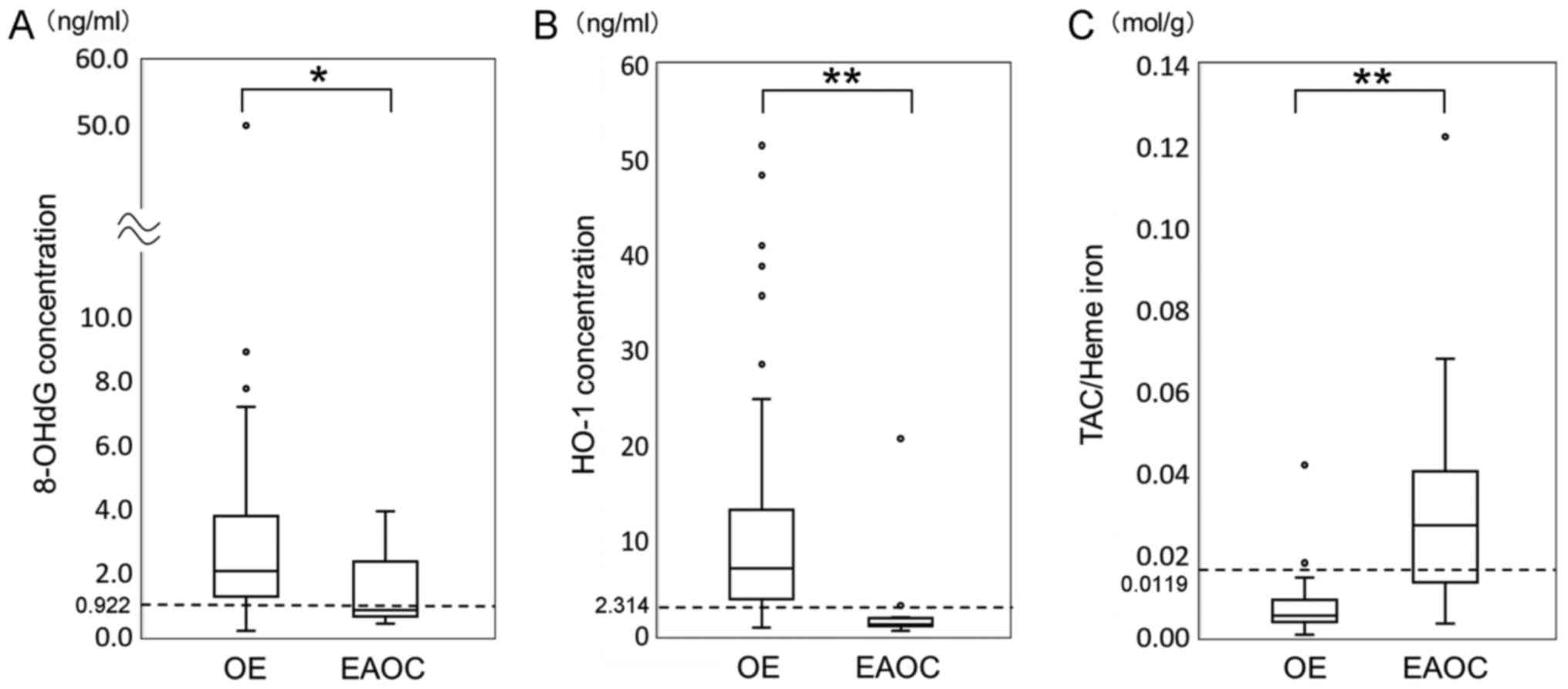
Cyst fluid marker levels in patients
with OE and EAOC
As presented in Fig.
1, box and whisker plots represent the median levels and the
interquartile range (box) of 8-OHdG (Fig.
1A), HO-1 (Fig. 1B) and
TAC/Heme-iron (Fig. 1C) for each
studied group. 8-OHdG concentrations in all samples ranged between
0.164 and 49.82 ng/ml. The concentrations were highly divergent
between the patients, with a few having extremely high
concentrations and a few with very low concentrations. Cyst fluid
8-OHdG levels were significantly lower in patients with EAOC
compared with OE (P=0.013; Fig. 1A).
EAOC patients had significantly lower HO-1 levels compared with
subjects with OE (P<0.001; Fig.
1B). Compared with OE, TAC/Heme-iron levels were significantly
higher in EAOC (P<0.001; Fig. 1C).
The marker values by each type of cyst are presented in Table II. Diminished oxidative damage in the
malignant group compared with the benign group was accompanied by
the increase in antioxidant protection.
| Table II.Level of three markers in benign OE
and EAOC. |
Table II.
Level of three markers in benign OE
and EAOC.
|
| Cyst fluid
value |
|
|---|
|
|
|
|
|---|
| Parameter | OE group | EAOC group | P-value |
|---|
| 8-OHdG (ng/ml) | 2.023
(0.16–49.98) | 0.820
(0.39–3.89) | 0.013a |
| HO-1 (ng/ml) | 7.00
(0.83–51.47) | 1.15
(0.42–20.69) | <0.001a |
| TAC/Heme-iron
(mol/g) | 0.0051
(0.0005–0.0420) | 0.0270
(0.0030–0.1226) |
<0.001a |
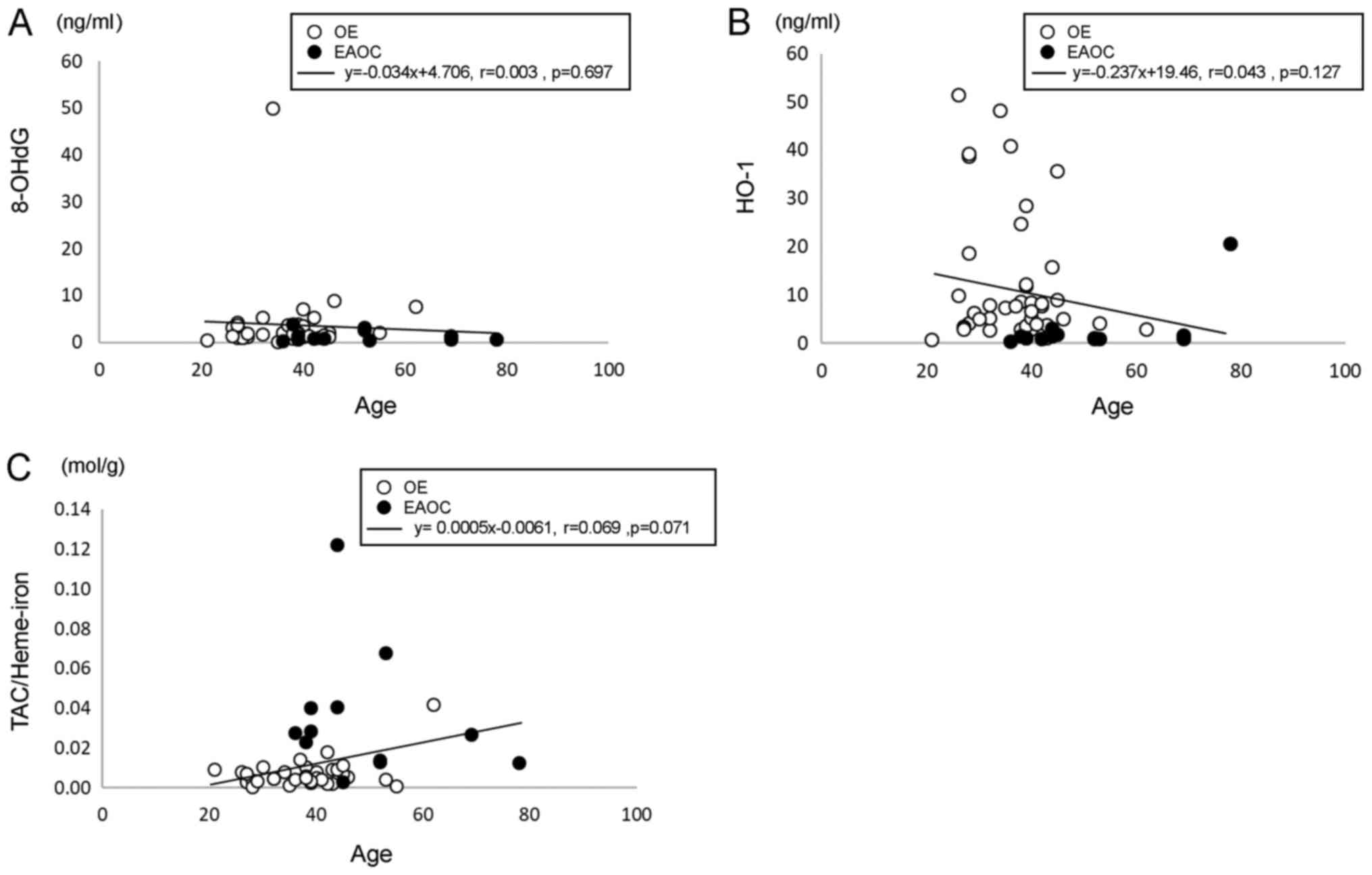
Correlation between patient ages and
cyst fluid marker levels
Since the EAOC group was significantly older
compared with the OE group (P=0.001), the correlation between age
and cyst fluid marker levels was analyzed. No significant
correlation was identified between patient age and the cyst fluid
levels of 8-OHdG, HO-1 or TAC/Heme-iron (Fig. 2).
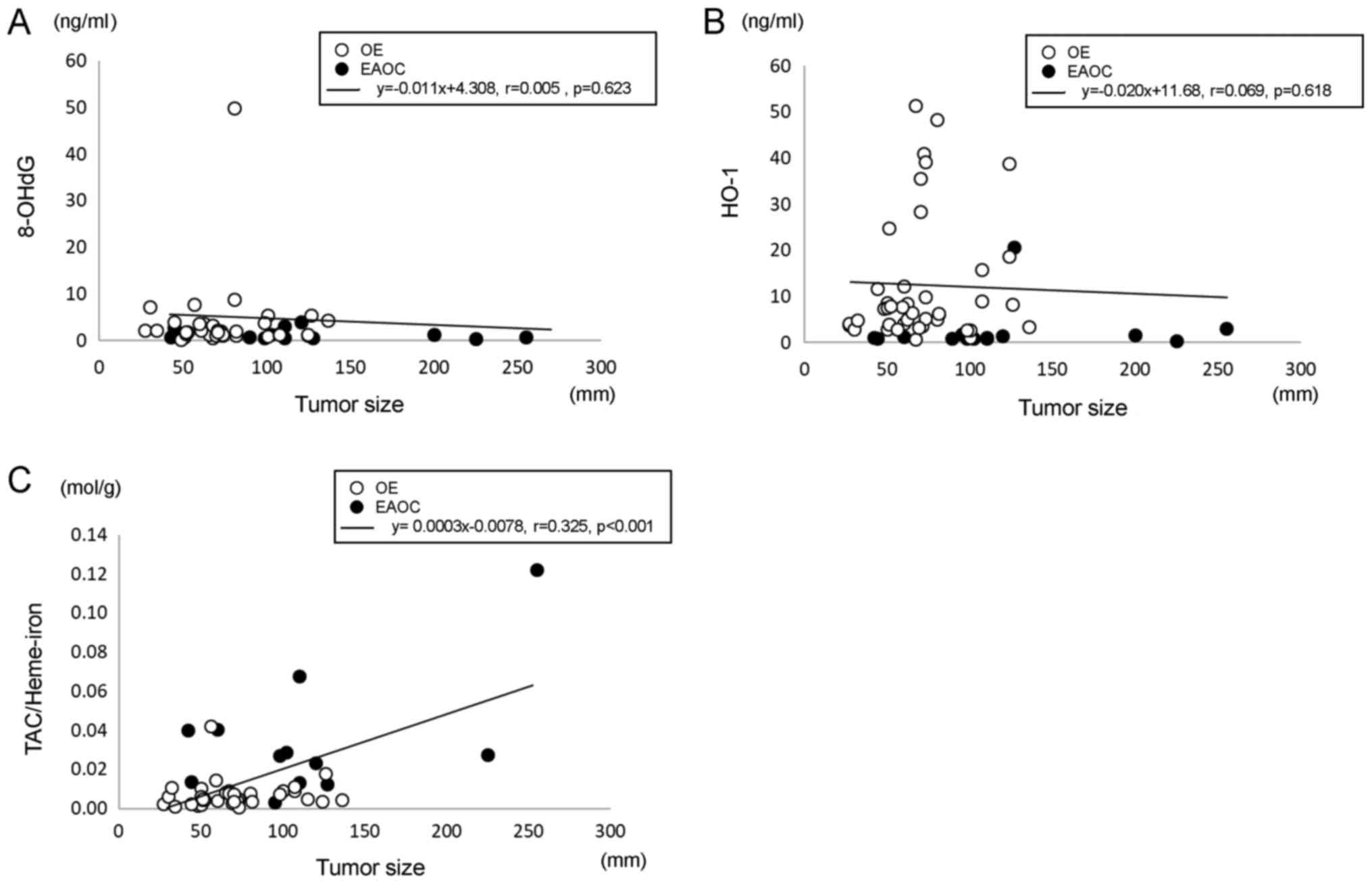
Correlation between tumor size and
cyst fluid marker levels
The present study subsequently analyzed the
correlation between cyst fluid marker levels and tumor size. No
significant differences were observed between 8-OHdG (Fig. 3A) and HO-1 levels (Fig. 3B) and tumor size. Cyst fluid
TAC/Heme-iron levels exhibited a positive association with tumor
size (Fig. 3C).
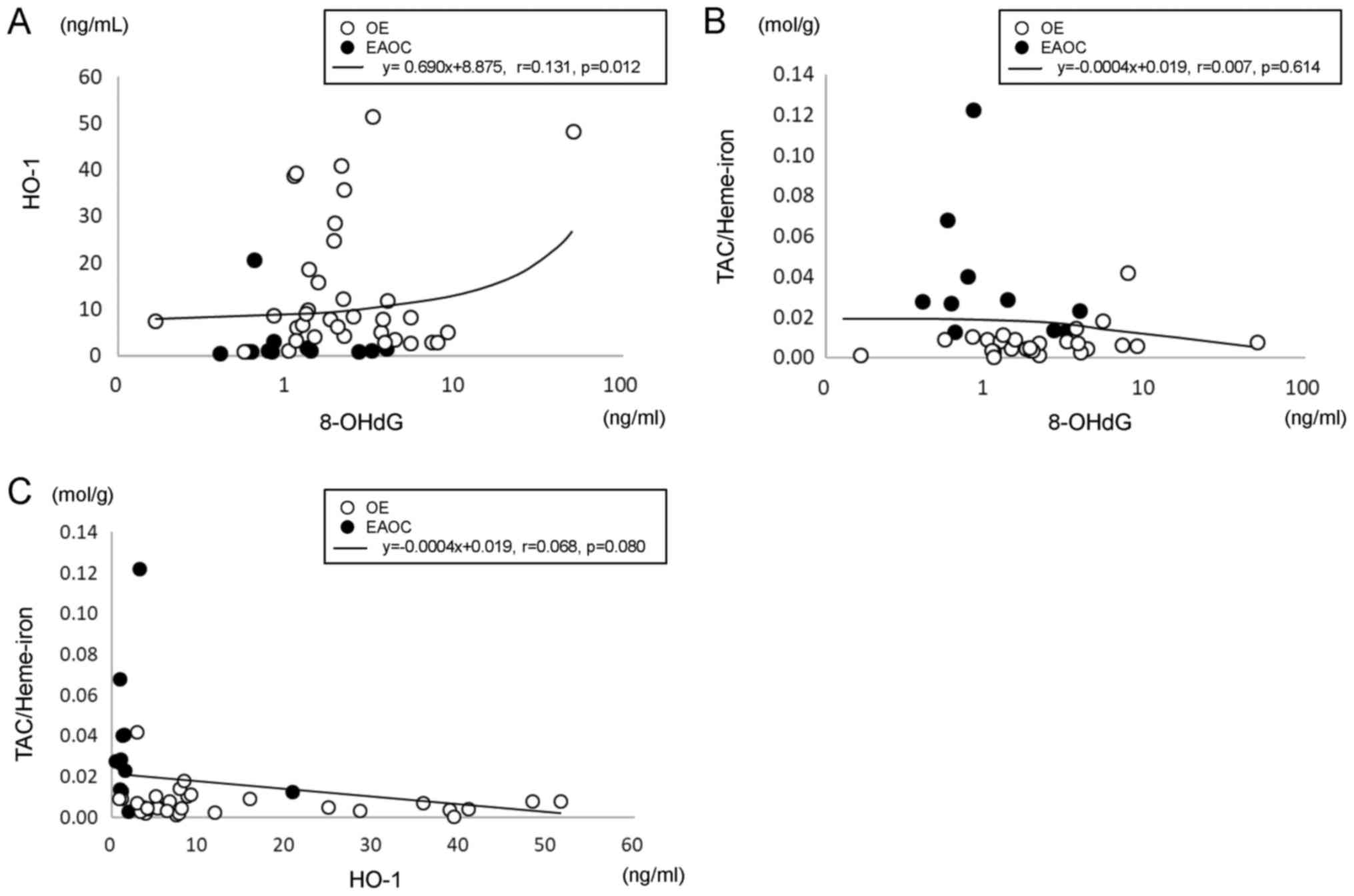
Correlation between cyst fluid 8-OHdG
levels, HO-1 levels and TAC/Heme-iron levels
With the use of Pearson's correlation coefficient
analysis, 8-OHdG levels were demonstrated to be positively
correlated with HO-1 levels (P=0.012; Fig. 4A). The correlation between the
antioxidant marker TAC/Heme-iron, and the levels of the oxidative
stress markers 8-OHdG and HO-1, was assessed. No correlation
existed between TAC/Heme-iron and 8-OHdG levels (Fig. 4B), or between TAC/Heme-iron and HO-1
levels (Fig. 4C).
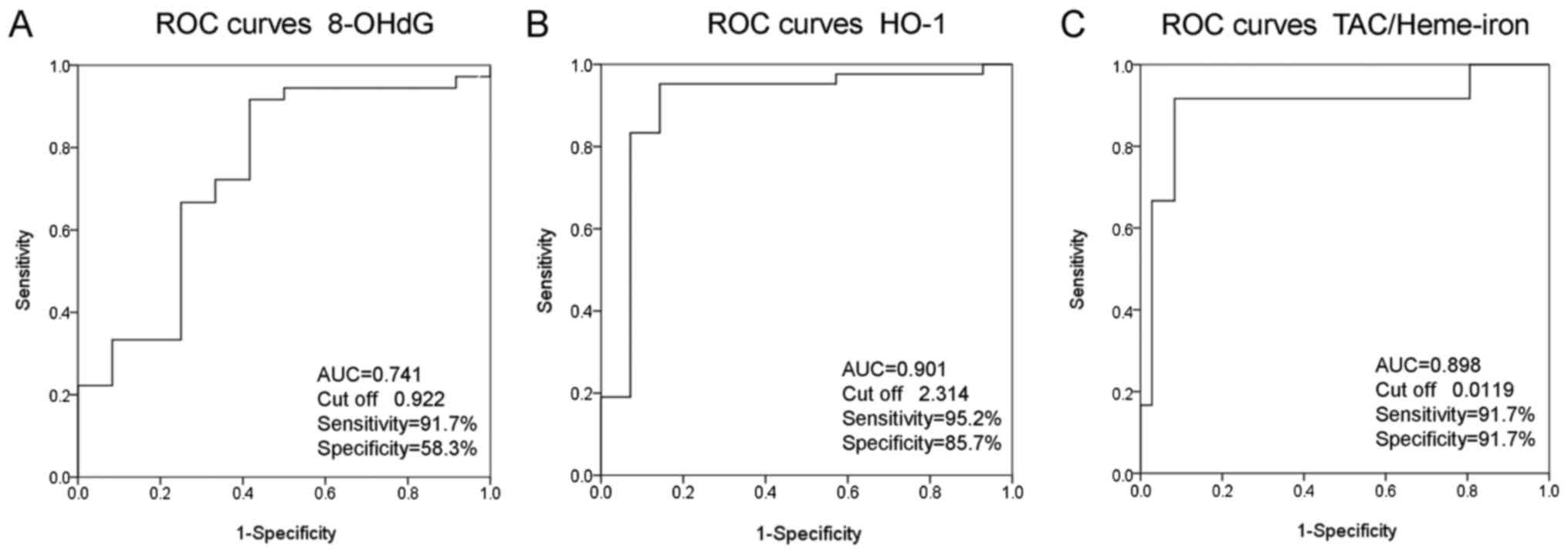
Evaluation of cyst fluid marker levels
as potential biomarkers for differential diagnosis between EAOC and
OE
Following quantitative measurement of each marker in
58 cyst fluid samples, ROC curves were applied to assess the
potential utility of cyst fluid levels in diagnosing EAOC from OE
(Fig. 5). The diagnostic sensitivity
and specificity of 8-OHdG, HO-1 and TAC/Heme-iron were analyzed and
the results are presented in Fig. 5.
The summary ROC curve illustrated that the AUC was 0.741 based on
cyst fluid 8-OHdG levels (Fig. 5A).
The detection sensitivity and specificity of 8-OHdG were 91.7 and
58.3%, respectively. HO-1 exhibited a higher detection sensitivity
(95.2%) and specificity (85.7%). The corresponding AUC and cut-off
point were 0.901 and 2.314, respectively. The ROC curves
demonstrated an optimum cut-off point of 0.0119 (for TAC/Heme-iron)
to distinguish EAOC from OE, yielding 91.7% sensitivity and 91.7%
specificity. The corresponding AUC was 0.898. As presented in
Fig. 1, the dashed horizontal line
represents the cut-off level for each marker. Among the indicators
investigated, HO-1 and Tac/Heme-iron exhibited the highest
discriminant value for EAOC (Fig. 5B and
C).
Discussion
This study evaluated the cyst fluid levels of
oxidative stress markers (8-OHdG and HO-1), and antioxidant
capacity (TAC/Heme-iron), in patients with benign OE and
already-growing EAOC. Lower pro-oxidant (8-OHdG and HO-1) levels
were observed in the cyst fluid of the EAOC group in comparison
with the benign OE group. By contrast, the cyst fluid anti-oxidant
TAC/Heme-iron was upregulated in the EAOC group compared with the
OE group. HO-1 exhibited the highest discriminant value for
differentiating between benign and malignant cyst fluids. The
present study revealed a clear separation of the overall redox
state between OE and EAOC. Therefore, redox imbalance may be
implicated in the etiology of the malignant transformation of
endometriosis.
Firstly, there is increasing evidence that oxidative
stress is one of the key factors in the establishment and
progression of endometriosis (15–17). High
levels of oxidized DNA adduct 8-OHdG were observed in the cyst
fluid from OE cases, suggesting increased oxidative stress and
frequent DNA mutations (18). HO-1
may be expressed in endometriosis, particularly in red lesions
(19), and also in macrophages
accumulated in endometriotic tissues (20). A number of studies have confirmed a
compromised antioxidant capacity in endometriosis (4,10,12,21,22). Total
antioxidant activity scavenges excess intracellular free radicals
and augments cellular antioxidant defenses. These findings support
the idea that higher oxidative stress-induced DNA damage and
mutations, and lower antioxidant capacity, are associated with
endometriosis progression, possibly directing it towards a
pre-malignant phenotype (17). HO-1
may terminate the further expansion of pre-malignant endometriotic
cells.
Secondly, few studies have examined the
oxidant-antioxidant profile in EAOC. An immunohistochemical study
demonstrated that EAOC tumor cells had weaker nuclear and
cytoplasmic 8-OHdG expression compared with tumors adjacent to OE
and benign endometriotic epithelial cells (23), suggesting an alleviation of oxidative
stress during the process of malignant transformation. Contrary to
previous reports (24), the present
results indicated that reduced accumulation of ROS-mediated
oxidative damage may predispose to cancer. In general, HO-1
influences tumor formation and progression, and its overexpression
has been associated with tumor growth, aggressiveness, metastasis
and angiogenetic potential, resistance to therapy, tumor escape and
a poor prognosis (7,25). In contrast to the well-known role of
HO-1 in tumor aggressiveness, the present study suggests that
diminished HO-1 expression may favor the progression from OE to
EAOC. Meanwhile, HO-1 serves a key role in preventing tumor
initiation and carcinogenesis (25,26).
Indeed, HO-1 expression was downregulated in early-stage lung
carcinoma (27), suggesting an
opposing role of HO-1 in different neoplasms or at different times
during tumor progression. Increased expression of HO-1 may protect
benign OE against oxidative stress-induced injury; however, HO-1
has been suggested to be a negative factor contributing to tumor
progression in EAOC. In other words, HO-1 is upregulated in
pre-transformation endometriotic cells, although it remains at the
basal level in already-growing cancer. Another possibility is that
patients with EAOC had much lower levels of hemoglobin, heme and
iron species compared with endometriotic cyst samples (9), supporting the idea that EAOC is
associated with lower HO-1 levels compared with OE. Although the
exact roles of HO-1 in malignant transformation remain
controversial, HO-1 serves a dual (promoting or inhibitory) role at
different stages of tumor initiation and progression (7,27). The
present study presents evidence supporting the idea that the
pre-tumorigenic environment of endometriois induces a redox
signaling switch in the oncogenic process.
Thirdly, an elevation in the TAC status in the
malignant group suggested increased production of antioxidants in
response to an enhanced level of oxidative damage. It was
hypothesized that increased expression of TAC may promote the
proliferation and survival of EAOC cells. The observed result was
comparable to existing results reported in similar studies:
Overexpression of a series of antioxidant genes counters cell and
DNA damage originating from oxidative stress in liver, thyroid,
breast, colon and pancreas cancer (28). Antioxidants alleviate cell death by
scavenging surplus oxidative stress, thus allowing for survival.
Taken together, enhancing antioxidant defenses and reducing
oxidative stress may predispose to malignancy.
It has previously been established that increased
intracellular ROS and decreased antioxidant molecules frequently
initiate carcinogenesis in various types of cancer (24). The patients with EAOC exhibited an
opposite pattern of altered expression of pro- and anti-oxidants.
The present study highlighted certain evidence suggesting a redox
change, which may drive the progression of already-growing cancer,
although not the initiation of carcinogenesis. Therefore,
characteristic alterations in redox parameters may depend on the
investigation of different stages of tumor ‘initiation’ and
‘progression’.
Finally, the present findings emphasize the
requirement to identify risk factors associated with the malignant
transformation of OE to predict it at the earliest stages. Among
redox parameters, HO-1 may be a candidate marker to estimate the
risk of malignant transformation. If there is a close association
between serum and cyst fluid HO-1 levels, HO-1 has potential as a
serum biomarker that may help to stratify the severity of OE, to
improve risk stratification for developing EAOC, and to accurately
predict the prognosis of patients with EAOC.
In conclusion, the present study revealed an
imbalance in the redox system of the tumor microenvironment due to
alterations in oxidative stress markers and antioxidant capacity
between OE and EAOC. HO-1 may protect OE against oxidative
stress-induced injury; however, in already-growing EAOC, excess
antioxidants favor tumor progression. Further study of the
molecular pathways involving redox balance may strengthen the
understanding of how the local intracystic microenvironment
initiates and sustains the transition of benign cells toward
malignant forms. There is a gradient of redox expression and
complexity in malignant transformation from benign OE to EAOC.
Acknowledgements
Not applicable.
Funding
The present study was supported by the Takeda
Science Foundation (JSPS KAKENHI grant no. JP16K11150) and the
Tohoku Bureau of Economy, Trade and Industry (grant no. Tohoku
1607028).
Availability of data and materials
All data generated or analysed during the present
study are included in this published article.
Authors' contributions
SI, KO and NK collected patients samples. FI, YY and
CY collected patients data and performed analyses. YF measured the
samples and performed analyses. HK contributed to conception and
design, acquisition of data, and analysis and interpretation of
data. HK was also involved in drafting the manuscript or revising
it critically for important intellectual content. All authors read
and approved the final manuscript.
Ethics approval and consent to
participate
The protocols were approved by The Ethics Committee
of Nara Medical University (reference no. 2012-541). Written
informed consent was obtained from each study subject, and all
subjects consented to donate cyst fluid samples.
Patient consent for publication
Written informed consent was obtained from each
study subject, and all subjects consented to donate cyst fluid
samples.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Kobayashi H, Sumimoto K, Moniwa N, Imai M,
Takakura K, Kuromaki T, Morioka E, Arisawa K and Terao T: Risk of
developing ovarian cancer among women with ovarian endometrioma: A
cohort study in Shizuoka, Japan. Int J Gynecol Cancer. 17:37–43.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kobayashi H: Ovarian cancer in
endometriosis: Epidemiology, natural history, and clinical
diagnosis. Int J Clin Oncol. 14:378–382. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kobayashi H: Potential scenarios leading
to ovarian cancer arising from endometriosis. Redox Rep.
21:119–126. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Iwabuchi T, Yoshimoto C, Shigetomi H and
Kobayashi H: Oxidative stress and antioxidant defense in
endometriosis and its malignant transformation. Oxid Med Cell
Longev. 2015:8485952015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kasai H: Analysis of a form of oxidative
DNA damage, 8-hydroxy-2′-deoxyguanosine, as a marker of cellular
oxidative stress during carcinogenesis. Mutat Res. 387:147–163.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ryter SW and Choi AM: Heme oxygenase-1:
Redox regulation of a stress protein in lung and cell culture
models. Antioxid Redox Signal. 7:80–91. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Nemeth Z, Li M, Csizmadia E, Döme B,
Johansson M, Persson JL, Seth P, Otterbein L and Wegiel B: Heme
oxygenase-1 in macrophages controls prostate cancer progression.
Oncotarget. 6:33675–33688. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Zamani-Ahari U, Zamani-Ahari S, Fardi-Azar
Z, Falsafi P and Ghanizadeh M: Comparison of total antioxidant
capacity of saliva in women with gestational diabetes mellitus and
non-diabetic pregnant women. J Clin Exp Dent. 9:e1282–e1286.
2017.PubMed/NCBI
|
|
9
|
Yoshimoto C, Iwabuchi T, Shigetomi H and
Kobayashi H: Cyst fluid iron-related compounds as useful markers to
distinguish malignant transformation from benign endometriotic
cysts. Cancer Biomark. 15:493–499. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Scutiero G, Iannone P, Bernardi G,
Bonaccorsi G, Spadaro S, Volta CA, Greco P and Nappi L: Oxidative
stress and endometriosis: A systematic review of the literature.
Oxid Med Cell Longev. 2017:72652382017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Worley MJ, Welch WR, Berkowitz RS and Ng
SW: Endometriosis-associated ovarian cancer: A review of
pathogenesis. Int J Mol Sci. 14:5367–5379. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Nasiri N, Moini A, Eftekhari-Yazdi P,
Karimian L, Salman-Yazdi R and Arabipoor A: Oxidative stress
statues in serum and follicular fluid of women with endometriosis.
Cell J. 18:582–587. 2017.PubMed/NCBI
|
|
13
|
Campos C, Guzmán R, López-Fernández E and
Casado A: Evaluation of the copper(II) reduction assay using
bathocuproinedisulfonic acid disodium salt for the total
antioxidant capacity assessment: The CUPRAC-BCS assay. Anal
Biochem. 392:37–44. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pandey AV, Joshi SK, Tekwani BL and
Chauhan VS: A colorimetric assay for heme in biological samples
using 96-well plates. Anal Biochem. 268:159–161. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Di Emidio G, D'Alfonso A, Leocata P,
Parisse V, Di Fonso A, Artini PG, Patacchiola F, Tatone C and Carta
G: Increased levels of oxidative and carbonyl stress markers in
normal ovarian cortex surrounding endometriotic cysts. Gynecol
Endocrinol. 30:808–812. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Polak G, Wertel I, Barczyński B,
Kwaśniewski W, Bednarek W and Kotarski J: Increased levels of
oxidative stress markers in the peritoneal fluid of women with
endometriosis. Eur J Obstet Gynecol Reprod Biol. 168:187–190. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Carvalho LF, Abrão MS, Biscotti C, Sharma
R, Nutter B and Falcone T: Oxidative cell injury as a predictor of
endometriosis progression. Reprod Sci. 20:688–698. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yamaguchi K, Mandai M, Toyokuni S,
Hamanishi J, Higuchi T, Takakura K and Fujii S: Contents of
endometriotic cysts, especially the high concentration of free
iron, are a possible cause of carcinogenesis in the cysts through
the iron-induced persistent oxidative stress. Clin Cancer Res.
14:32–40. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Van Langendonckt A, Casanas-Roux F,
Dolmans MM and Donnez J: Potential involvement of hemoglobin and
heme in the pathogenesis of peritoneal endometriosis. Fertil
Steril. 77:561–570. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Nishie A, Ono M, Shono T, Fukushi J,
Otsubo M, Onoue H, Ito Y, Inamura T, Ikezaki K, Fukui M, et al:
Macrophage infiltration and heme oxygenase-1 expression correlate
with angiogenesis in human gliomas. Clin Cancer Res. 5:1107–1113.
1999.PubMed/NCBI
|
|
21
|
Hevir N, Ribič-Pucelj M and Lanišnik
Rižner T: Disturbed balance between phase I and II metabolizing
enzymes in ovarian endometriosis: A source of excessive
hydroxy-estrogens and ROS? Mol Cell Endocrinol. 367:74–84. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Singh AK, Chattopadhyay R, Chakravarty B
and Chaudhury K: Markers of oxidative stress in follicular fluid of
women with endometriosis and tubal infertility undergoing IVF.
Reprod Toxicol. 42:116–124. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sova H, Kangas J, Puistola U, Santala M,
Liakka A and Karihtala P: Down-regulation of
8-hydroxydeoxyguanosine and peroxiredoxin II in the pathogenesis of
endometriosis-associated ovarian cancer. Anticancer Res.
32:3037–3044. 2012.PubMed/NCBI
|
|
24
|
Nourazarian AR, Kangari P and Salmaninejad
A: Roles of oxidative stress in the development and progression of
breast cancer. Asian Pac J Cancer Prev. 15:4745–4751. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Nitti M, Piras S, Marinari UM, Moretta L,
Pronzato MA and Furfaro AL: HO-1 induction in cancer progression: A
matter of cell adaptation. Antioxidants (Basel). 6:pii: E29.
2017.PubMed/NCBI
|
|
26
|
Skrzypek K, Tertil M, Golda S, Ciesla M,
Weglarczyk K, Collet G, Guichard A, Kozakowska M, Boczkowski J, Was
H, et al: Interplay between heme oxygenase-1 and miR-378 affects
non-small cell lung carcinoma growth, vascularization, and
metastasis. Antioxid Redox Signal. 19:644–660. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
De Palma G, Mozzoni P, Acampa O,
Internullo E, Carbognani P, Rusca M, Goldoni M, Corradi M, Tiseo M,
Apostoli P and Mutti A: Expression levels of some antioxidant and
epidermal growth factor receptor genes in patients with early-stage
non-small cell lung cancer. J Nucleic Acids. 2010:pii: 147528.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kong B, Qia C, Erkan M, Kleeff J and
Michalski CW: Overview on how oncogenic Kras promotes pancreatic
carcinogenesis by inducing low intracellular ROS levels. Front
Physiol. 4:2462013. View Article : Google Scholar : PubMed/NCBI
|