Introduction
Pancreatic cancer is the twelfth most common
malignancy, with 337,872 cases reported in 2012, and the seventh
leading cause of cancer-associated mortality, with 330,391
mortalities reported in 2012, worldwide (1). Pancreatic ductal adenocarcinoma (PDAC)
is one of the most lethal malignancies. PDAC is the fourth leading
cause of cancer-associated mortality in the USA (2); without any substantial improvement in
curative therapies, it is anticipated to be the second leading
cause of cancer-associated mortality by 2030 (3). Surgical resection is currently the only
option to potentially achieve long-term survival (4). However, the 5-year survival rate is only
~10% following surgical therapy (5);
therefore, postoperative adjuvant chemotherapy is being developed
to improve prognosis. In the USA in 1985, the Gastrointestinal
Tumor Study Group reported the use of postoperative adjuvant
therapy for the first time (6).
Later, in 2007, the CONKO-001 trial evaluated the use of
gemcitabine (7). The effectiveness of
postoperative S-1 adjuvant chemotherapy was revealed in Japan in
2016 (8). Nevertheless, the 5-year
survival rate following surgery and adjuvant chemotherapy remains
at only ~20% (5,9). Due to postoperative quality of life
degradation and other factors, there are a number of problems that
result in insufficient adjuvant chemotherapy. Therefore, the
importance of neoadjuvant therapy has recently been the focus of
numerous studies (10). Treatment
options for PDAC will diversify in the future and it will be
necessary to make the optimal choice of therapy.
PDAC is postulated to lead to systemic metastasis,
which is accompanied by an accumulation of various gene mutations
(11,12). However, which gene mutations are
associated with clinicopathological prognostic factors is not
clear. By identifying gene mutations that are associated with
prognostic factors, there is a possibility that the range of
treatment options will be increased. We previously reported that
the preoperative carbohydrate antigen 19-9 (preCA19-9) level and
the dissected peripancreatic tissue margin (DPM) were independent
prognostic factors in PDAC (13). To
date, it has repeatedly been reported that a positive margin and
CA19-9 are prognostic factors in a univariate manner (14–16).
However, each previous study included different clinicopathological
factors and multivariate prognostic analysis revealed different
sets of independent prognostic factors. To the best of our
knowledge, our previous study was the first to report that the two
factors can be simultaneously evaluated as independent prognostic
factors (13). Analysis that combines
these important prognostic factors may be useful in clinical
management. However, our previous study had limitations, including
a small sample size and follow-up period.
The aims of the current study were to validate the
prognostic relevance of preCA19-9 and DPM as independent prognostic
factors in primary PDAC and to clarify the associations between
predictive factors and gene mutation status.
Materials and methods
Registration of patients
From January 1986 to December 2013, 161 patients
(median, 65; range 38–88), including 85 male and 76 female
patients, with histologically confirmed PDAC underwent a
pancreatectomy with D0-D3 lymph node dissection at the Department
of Surgery, Kitasato University Hospital (Kanagawa, Japan).
Patients with histological variants, including mucinous cystic
adenocarcinoma, intraductal papillary adenocarcinoma, acinar cell
carcinoma and endocrine carcinoma were excluded from the study.
Preoperative workup included an ultrasonography, computed
tomography, endoscopic retrograde pancreatography, endoscopic
ultrasonography and magnetic resonance cholangiopancreatography to
evaluate primary and metastatic tumor sites.
The preoperative serum CA19-9 levels were
investigated immediately prior to surgery, avoiding the effects of
obstructive jaundice and/or inflammation of the biliary duct. The
recommended upper limit of a normal CA19-9 level is 37 U/ml, when
CA19-9 levels are determined and defined from the standard
deviations of healthy individuals. CA19-9 levels were determined
using a chemiluminescent enzyme immunoassay kit (LUMIPLSE G; cat.
no., CA19-9-N) obtained from Fujirebio US, Inc. (Malvern, PA,
USA).
The surgical resection tissues were obtained from
pancreaticoduodenectomy (n=39), pylorus-preserving
pancreaticoduodenectomy (n=74), distal pancreatectomy (n=43) and
total pancreatectomy (n=5). Partial resection of the portal vein
was performed if the surgeon observed tumor invasion of the portal
vein. Intraoperative pathologic assessment of the proximal or
distal pancreatic margins was performed using frozen-tissue
sections. If the pancreatic margin was positive for cancerous
cells, further resection of the pancreas was performed. The present
study was approved by the Institutional Review Board for
Observation and Epidemiological Study, Kitasato University Medical
Ethics Organization (approval no. B18-017; Kanagawa, Japan). All
patients agreed to the use of their samples in scientific research
and written informed consent was obtained from all patients.
Pathological investigation
All histological and other clinicopathological
factors were judged independently and blindly by histopathologists,
and all histopathologic factors from the Japanese classification
system (JCS) version 6 (17) were
obtained from medical records. In the current study, stage was
determined according to the 6th edition of the International Union
Against Cancer (UICC) tumor-node-metastasis classification
(18). Assessment of cancer
infiltration at the surgical margin was evaluated according to the
JCS, as DPM, pancreatic cut end margin or bile duct cut end margin.
According to the National Comprehensive Cancer Network guideline
(19), the surgical margin was
defined as a superior mesenteric artery (SMA) margin, posterior
margin, portal vein groove margin, portal vein margin, pancreatic
margin or pancreatic surface and bile duct margin. Details of the
DPM included the SMA margin, posterior margin and portal vein
groove margin. Surgical margin-positive was defined as tumor cells
present in the dissection surface, as judged by histopathologists.
When requested by a pathologist, the gene mutation was investigated
using non-radioisotopic single-strand conformation polymorphism
(SSCP) from each DNA sample (n=97).
DNA examination and search for the
mutated K-ras gene using SSCP
For simultaneous DNA analysis, the previously
described protocols were conducted (20,21).
Briefly, this consisted of five steps. Firstly, to prevent
cross-contamination, small sections of fresh solid tissue were
sampled by scraping with disposable bamboo combs, which are 3×3×120
mm rods made of bamboo with a spatula like ends. Secondly, one-step
DNA extraction with lysis buffer containing proteinase K, Nonidet
P-40 and Tween 20 was performed. Subsequently. polymerase chain
reaction (PCR) was performed with each gene primer presented in
Table I and the conditions presented
in Table II. Next, SSCP analysis
with polyacrylamide gels was performed, and detection was achieved
by silver staining. In this analysis, mutated bands were evident at
1:64 dilutions of the mutated alleles.
 | Table I.Primer sequences used for polymerase
chain reaction. |
Table I.
Primer sequences used for polymerase
chain reaction.
| Gene | Exon | Forward
sequence | Reverse
sequence | Amplified fragment
length, bp | Codons |
|---|
| K-ras | 1 |
5′-GACTGAATATAACTTGTGG-3′ |
5′-GCTATTGTTGGATCAATATTC-3′ | 108 | 2–37 |
|
| 2 |
5′-GATTCCTACAGGAAGCAAGT-3′ |
5′-TAATGGTGAATATCTTC-3′ | 185 | 38–97 |
| TP53 | 5 |
5′-TTCCTCTTCCTGCAGTACTC-3′ |
5′-GCCCCAGCTGCTCACCATCGCTA-39 | 214 | 125–186 |
|
| 6 |
5′-GCCTCTGATTCCTCACTGATTG-3′ |
5′-AGTTGCAAACCAGACCTCAG-3′ | 157 | 187–224 |
|
| 7 |
5′-CCTCATCTTGGGCCTGTGTTATC-3′ |
5′-CAAGTGGCTCCTGACCTGGAGTC-3′ | 154 | 225–261 |
|
| 8 |
5′-CCTATCCTGAGTAGTGGTAA-3′ |
5′-GTCCTGCTTGCTTACCTCGC-3′ | 166 | 262–306 |
|
| 9 |
5′-GCCTCTTTCCTAGCACTGCC-3′ |
5′-CCAAGACTTAGTACCTGAAG-3′ | 101 | 307–331 |
| Table II.Polymerase chain reaction cycle
conditions. |
Table II.
Polymerase chain reaction cycle
conditions.
| Fresh samples |
|---|
|
|---|
| Conditions | No. of cycles |
|---|
| 94°C 3 min | 1 |
| 52°C for 1 min,
72°C for 1 min, 94°C for 30 sec | 2 |
| 52°C for 45 sec,
72°C for 30 sec, 94°C for 20 sec | 35 |
| 52°C for 45 sec,
72°C for 3 min | 1 |
Follow-up and postoperative
therapy
A total of 108 patients (67%) received empirical
adjuvant therapy; this consisted of 105 patients who received
chemotherapy and 3 patients who received radiotherapy. Another 23
patients (14%) received therapy for remnant tumor; specifically 22
patients who received chemotherapy and 1 patient who received
radiotherapy. A number of chemotherapy regimens consisted of
5-fluorouracil (5-FU)-based chemotherapy, including 5-FU only
(n=3), 5-FU/cisplatin (n=9) or
5-FU/Adriamycin/mitomycin-C/nimustine hydrochloride (n=2) by
venous, portal or arterial infusion. Other chemotherapy regimens
included tegafur/uracil (n=11), 5′-deoxy-5-fluorouridine (n=3) or
TS-1 (n=3) as oral therapy, or mitomycin-C (n=7). In addition to
gemcitabine (n=83) or gemcitabine+TS-1 (n=6) by venous or arterial
infusion. Radiotherapy consisted of 1.8 Gy per day to a total dose
of 50 Gy. Routine follow-up consisted of physical examination,
laboratory studies and computed tomography imaging at 3- to 4-month
intervals for the first 2 years, at 6-month intervals for years 3
to 5, and followed by annual follow-ups from thereon. Only the
first sites of recurrence were recorded.
Statistical analysis
Continuous variables were compared using the
Student's t-test and nominal variables were compared using
Pearson's chi-square test. The Kaplan-Meier method was used for
disease-specific survival (DSS) analysis and the difference in
survival rate was assessed by log-rank test (22). DSS was measured from the date of
surgery to the date of mortality or last follow-up. Mortality
associated with causes other than PDAC were not counted in this
measurement. The variables that demonstrated prognostic potential
suggested by univariate analysis (P<0.05) were subjected to
multivariate analysis with a Cox proportional hazards model.
Propensity scores were matched using a caliper width of 0.2
multiplied by the standard deviation of values that was calculated
by a logistic regression analysis. A receiver operating
characteristic (ROC) curve was generated using JMP software v.11.0
(SAS institute, Cary, NC, USA) and the area under the curve (AUC)
was used to optimize the best cut-off value. The associations
between K-ras gene mutation and prognostic factors were
examined with the Student's t-test. P<0.05 was considered to
indicate a statistically significant difference. All statistical
analysis was performed using JMP software v.11.0.
Results
Patients' characteristics and
univariate prognostic analysis in PDAC
The first aim of the current study was to validate
the prognostic relevance of preCA19-9 and DPM, which have
previously been identified as independent prognostic factors in
PDAC (12). The characteristics of
161 patients with PDAC and the univariate prognostic factors are
summarized in Table III.
Significant prognostic factors included lymphatic permeation factor
(ly; P=0.036), vascular permeation factor (v; P=0.0087), tumor
differentiation (P=0.0037), intrapancreatic nerve invasion factor
(ne; P=0.00025), retropancreatic tissue invasion factor (RP;
P=0.0053), portal venous system invasion factor (PV; P=0.0133),
extrapancreatic nerve plexus invasion factor (PL; P=0.0004),
arterial system invasion factor (A; P=0.0019), preCA19-9 level
(P<0.0001), DPM (P<0.0001) and UICC 6th stage (P<0.0001).
Arterial invasion was composed of pT4 (celiac artery or superior
mesenteric artery; n=2) and non-pT4 (splenic artery; n=3). By
increasing the number of patients from the previous pilot study
(13), several pathological factors,
which are not UICC staging factors, including ly, v, ne, RP, PV and
A, were newly identified as univariate prognostic factors in
PDAC.
| Table III.Univariate and multivariate
prognostic analysis for 161 patients with PDAC who underwent
pancreatectomy. |
Table III.
Univariate and multivariate
prognostic analysis for 161 patients with PDAC who underwent
pancreatectomy.
|
|
| Univariate | Multivariate |
|---|
|
|
|
|
|
|---|
| Variable | No. | RR | 95% CI |
P-valuea | RR | 95% CI |
P-valuea |
|---|
| Age, years |
|
|
|
|
|
|
|
|
<65/>65 | 79/82 | 0.8 | 0.6–1.2 | 0.3150 |
|
|
|
| Sex |
|
|
|
|
|
|
|
|
Male/female | 85/76 | 1.2 | 0.8–1.8 | 0.2628 |
|
|
|
| Lymphatic
invasion |
|
|
|
|
|
|
|
|
Absence/presence | 22/139 | 1.8 | 1.1–3.5 | 0.0360 | 1.5 | 0.81–2.95 | 0.2109 |
| Venous
invasion |
|
|
|
|
|
|
|
|
Absence/presence | 13/148 | 4 | 1.5–16.4 | 0.0087 | 1.6 | 0.56–6.91 | 0.4082 |
| Tumor
differentiation |
|
|
|
|
|
|
|
|
Well/other (moderate,
poorly) | 137/24 | 2.1 | 1.2–3.4 | 0.0037 | 1.8 | 0.32–1.01 | 0.0563 |
| Intrapancreatic
nerve invasionth |
|
|
|
|
|
|
|
|
Absence/presence | 17/144 | 3.6 | 1.6–10.2 | 0.0025 | 2 | 0.87–6.1 | 0.1083 |
| Retropancreatic
tissue invasion |
|
|
|
|
|
|
|
|
Absence/presence | 62/99 | 1.8 | 1.2–2.7 | 0.0053 | 1.2 | 0.70–1.94 | 0.5635 |
| Portal venous
system invasion |
|
|
|
|
|
|
|
|
Absence/presence | 131/30 | 1.8 | 1.1–2.9 | 0.0133 | 2 | 1.15–3.22 | 0.0143 |
| Extrapancreatic
nerve plexus invasion |
|
|
|
|
|
|
|
|
Absence/presence | 126/35 | 2.1 | 1.4–3.2 | 0.0004 | 1.5 | 1.15–3.22 | 0.1671 |
| Arterial system
invasion |
|
|
|
|
|
|
|
|
Absence/presence | 156/5 | 3.8 | 1.3–8.6 | 0.0019 | 2.4 | 0.78–6.32 | 0.1173 |
| PreCA19-9 level,
U/ml |
|
|
|
|
|
|
|
|
<37/>37 | 39/122 | 3.5 | 2.1–6.4 | <0.0001 | 2.8 | 1.58–5.46 | 0.0003 |
| Dissected
pancreatic tissue margin |
|
|
|
|
|
|
|
|
Negative/positive | 101/60 | 2.9 | 2.0–4.3 | <0.0001 | 2.5 | 1.58–3.99 | <0.0001 |
| Stageb |
|
|
|
|
|
|
|
|
0–I | 9 | Reference |
| <0.0001 | Reference |
| 0.0032 |
| II | 122 | 9.6 | 2.1–169 |
| 4.5 | 0.92–80.4 |
|
|
III | 7 | 56.7 | 9.9–1067.6 |
| 13.5 | 2.0–268 |
|
| IV | 23 | 30.5 | 6.3–547.8 |
| 9.4 | 1.81–173 |
|
| PreCA19-9 and DPM
combination |
|
|
|
|
|
|
|
| A; Over
37 U/ml and Positive | 51 | Reference |
| <0.0001 |
|
|
|
| B; Over
37 U/ml and Negative | 71 | 2.6 | 1.7–3.9 |
|
|
|
|
| C;
<37 U/ml and Positive | 9 | 2.6 | 1.2–6.3 |
|
|
|
|
| D;
<37 U/ml and Negative | 30 | 10.2 | 5.0–23.8 |
|
|
|
|
Multivariate Cox proportional hazards
model in PDAC
The ten variables that exhibited prognostic
potential identified by univariate prognostic analysis, including
ly, v, tumor differentiation, ne, RP, PV, PL, A, preCA19-9, DPM and
UICC 6th stage, were subjected to multivariate analysis. This
analysis revealed that preCA19-9 [P=0.0002, relative risk
(RR)=2.8], DPM positive (P=0.0002, RR=2.4), PV (P=0.01, RR=2.0) and
A (P=0.035, RR=3.3) were the remaining prognostic factors
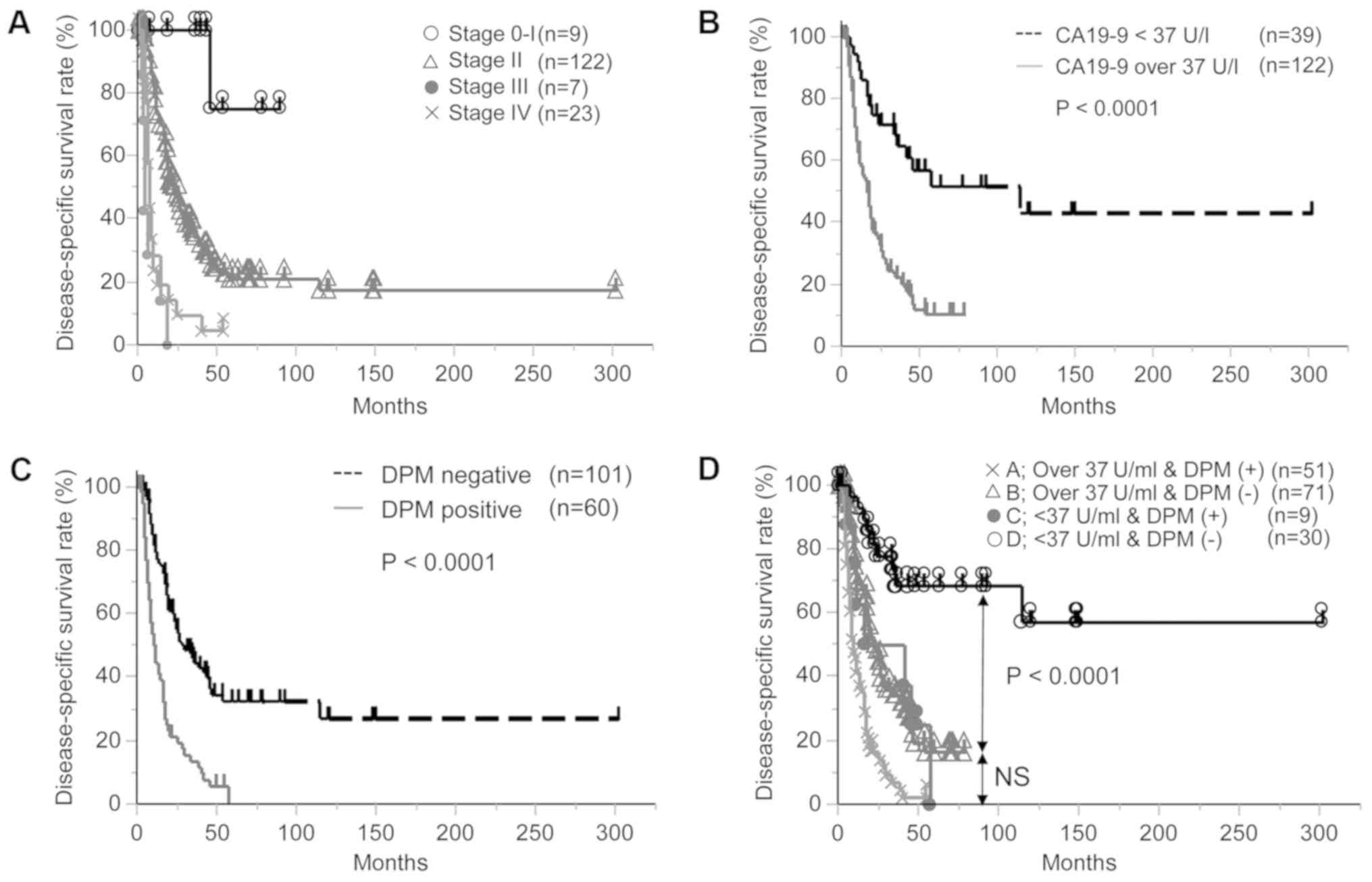
independent of UICC stage (P=0.0015; Table III).
Similar to previous studies (23,24),
preCA19-9 and DPM were identified as independent prognostic
factors. The Kaplan-Meier curves of each factor are presented in
Fig. 1A for UICC stage, Fig. 1B for PreCA19-9 and Fig. 1C for DPM. Notably, all DPM-positive
patients succumbed to the disease within 5 years, while a number of
patients with preCA19-9 levels >37 U/ml were alive with no
recurrence after five years.
In addition, survival outcomes for the combination
of preCA19-9 and DPM are presented in Table III and Fig. 1D. The prognosis of patients with PDAC
was sub-classified into four groups (A, B, C and D) according to
preCA19-9 and DPM (group A, preCA19-9 >37 U/ml and DPM-positive;
group B, preCA19-9 >37 U/ml and DPM-negative; group C, preCA19-9
<37 U/ml and DPM-positive; and group D, preCA19-9 <37 U/ml
and DPM-negative). Of note, group D demonstrated the best clinical
outcome and included long-term survivors (10/30) of PDAC (Fig. 1D).
Prognostic relevance of DPM-positive
status in PDAC following propensity score matching
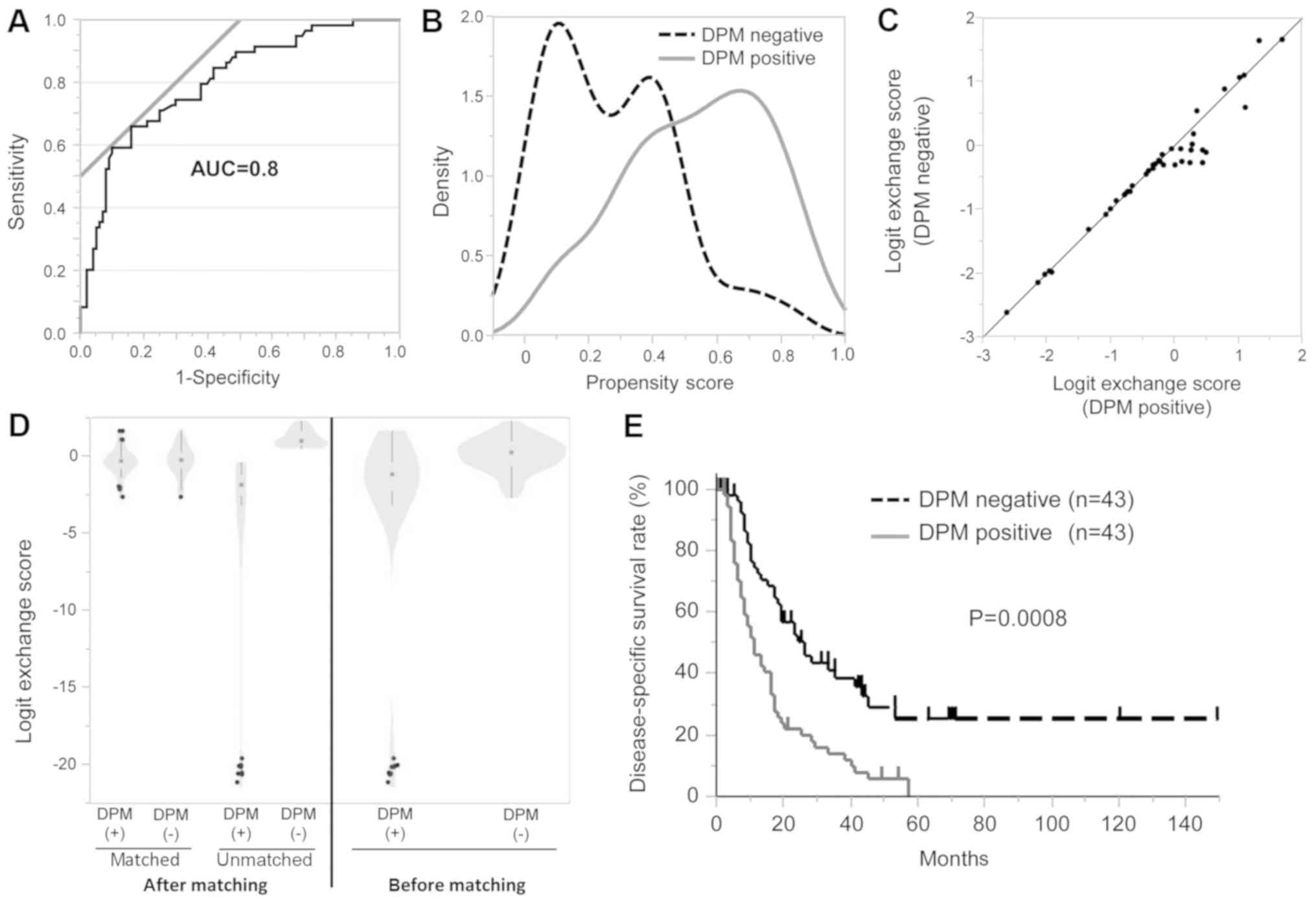
A DPM-positive status may be the best indicator of
highly aggressive tumor characteristics in PDAC; therefore, a risk
model for DPM prediction was generated by logistic regression
analysis. The clinicopathological factors analyzed were as follows:
age, gender, ly, v, ne, RP, PV, A, PL, UICC stage and preCA19-9.
Using this prediction model, an ROC curve was generated and
presented in Fig. 2A (AUC=0.80) and
the propensity score (PS) to predict DPM was calculated. The
density distribution of PS was analyzed between DPM-positive and
DPM-negative patients, and a notable difference in the PS
distribution was identified between the groups (Fig. 2B). The matching of PS was performed by
logit exchange. The logit exchange scores of the matched cases
between both DPM-positive and DPM-negative cases were presented
linearly in a scatter plot (Fig. 2C).
The logit exchange scores of the matched cases between DPM-positive
and DPM-negative were distributed in Kernel density estimation
differently from the unmatched cases (Fig. 2D, left panel), as compared with the
differential ranges prior to matching (Fig. 2D, right panel). Following matching, no
significant differences were identified for factors potentially
affecting DPM between DPM-positive and DPM-negative cases (Table IV). Notably, the factors identified
to be associated with DPM positive were RP and RL, and these
factors were corrected by score matching. As a result, DPM was
demonstrated as a robust prognostic factor in PDAC (P=0.0008;
Fig. 2E).
| Table IV.Distribution of potential factors
associated with DPM between DPM positive and negative cases prior
to and following propensity score matching. |
Table IV.
Distribution of potential factors
associated with DPM between DPM positive and negative cases prior
to and following propensity score matching.
|
| Prior to
matching | Following
matching |
|---|
|
|
|
|
|---|
| Variable | DPM positive
(n=59) | DPM negative
(n=101) | P-value | DPM positive
(n=43) | DPM negative
(n=43) | P-value |
|---|
| Agea | 63.4±9.4 | 64.4±10.3 | 0.5172c | 64.1±9.1 | 64.7±10.4 | 0.81c |
| Sex |
|
|
|
|
|
|
|
Male/female | 30/29 | 55/46 | 0.6590d | 22/21 | 22/21 | 1.00d |
| PreCA19-9 level,
U/ml |
|
|
|
|
|
|
|
<37/>37 | 9/50 | 30/71 | 0.0400d | 8/35 | 10/33 | 0.59d |
| Stageb |
|
|
|
|
|
|
|
0–I/II/III/IV | 0/42/5/12 | 9/79/2/11 | 0.0097d | 0/33/2/8 | 0/35/2/6 | 0.84d |
| Lymphatic
invasion |
|
|
|
|
|
|
|
Absence/presence | 53/6 | 85/16 | 0.3056d | 38/5 | 37/6 | 0.75d |
| Venous
invasion |
|
|
|
|
|
|
|
Absence/presence | 56/3 | 91/10 | 0.2664d | 41/2 | 39/4 | 0.39d |
| Intrapancreatic
nerve invasion |
|
|
|
|
|
|
|
Absence/presence | 56/3 | 87/14 |
0.00675d | 40/3 | 40/3 | 1.00d |
| Retropancreatic
tissue invasion |
|
|
|
|
|
|
|
Absence/presence | 51/8 | 48/53 |
<0.0010d | 35/8 | 32/11 | 0.44d |
| Portal venous
system invasion |
|
|
|
|
|
|
|
Absence/presence | 12/47 | 18/83 | 0.6939d | 11/32 | 7/36 | 0.28d |
| Extrapancreatic
nerve plexus invasion |
|
|
|
|
|
|
|
Absence/presence | 22/37 | 13/88 | 0.0003d | 9/34 | 11/32 | 0.61d |
| Arterial system
invasion |
|
|
|
|
|
|
|
Absence/presence | 3/56 | 2/99 | 0.2762d | 2/42 | 1/41 | 0.56d |
Subsequently, initial recurrent sites were
investigated in DPM-positive patients with PDAC. Among the 60
DPM-positive patients, 52 recurrences were identified. Liver
metastases were the most prevalent in 21 patients (35%), followed
by lymph node metastases in 13 patients (22%), peritoneal
dissemination in 5 patients (8%), lung metastasis in 1 patient
(35%), nerve plexus of the SMA in 9 patients (15%) and remnant
pancreas in 3 patients (5%).
Molecular association of DPM with
mutational status of K-ras and p53 genes in PDAC
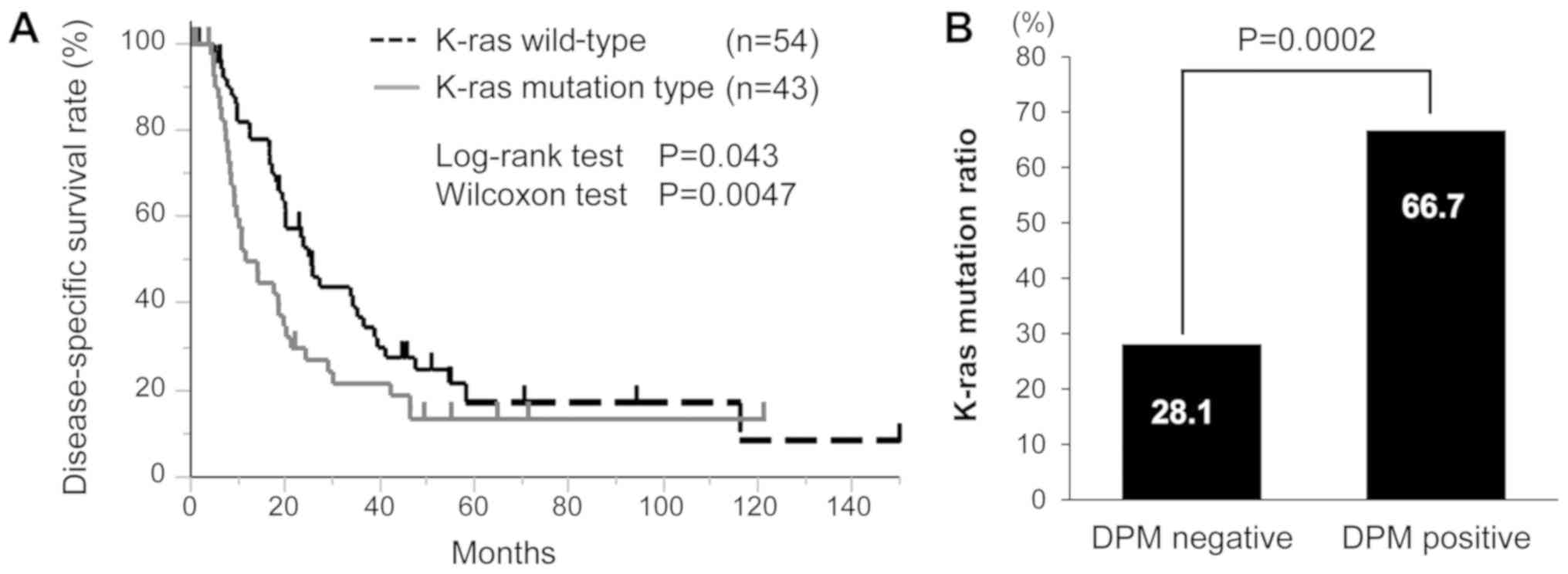
Subsequently, the associations of DPM with the
mutational status of K-ras and TP53 genes in PDAC
were investigated. For K-ras gene mutation, 96 patients with
PDAC were investigated. K-ras gene mutation was identified
in 42 patients (44%), among whom 34 patients possessed mutations in
exon1 (codon 12 or 13). The Kaplan-Meier curve was generated
according to K-ras gene mutation status (P=0.043 by the
log-rank test and P=0.0047 by the Wilcoxon test; Fig. 3A). Since DPM has been cited as a poor
prognostic factor in the present results, univariate analysis was
performed for factors associated with DPM status (Table V). RP (P<0.001), PL (P=0.0003) and
K-ras gene mutation status (P=0.0002) were significantly
associated with DPM-positive status. Multivariate analysis
confirmed that RP (P=0.037), PL (P=0.026) and K-ras gene
mutation status (P=0.0004) remained as independent factors of
DPM-positive statue. A significant association was identified
between DPM and K-ras gene mutation status (Fig. 3B). DPM-positive patients had a
K-ras gene mutation in 66.7% (26/39) of cases, while
DPM-negative patients exhibited a K-ras gene mutation in
28.1% (16/57) of cases. For the TP53 gene mutation, 67
patients with PDAC were examined and a TP53 gene mutation
was identified in 14 (20.9%). Of these, 6 patients were
DPM-positive, and no significant difference was identified with
regard to DPM status (P=0.9275).
| Table V.Univariate and multivariate
prognostic analysis for DPM. |
Table V.
Univariate and multivariate
prognostic analysis for DPM.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variable | DPM positive
(n=59) | DPM negative
(n=101) |
P-valuea | Odds ratio | 95% CI |
P-valueb |
|---|
| Lymphatic
invasion |
|
|
|
|
|
|
|
Absence/presence | 53/6 | 85/16 | 0.3148 |
|
|
|
| Venous
invasion |
|
|
|
|
|
|
|
Absence/presence | 56/3 | 91/10 | 0.2820 |
|
|
|
| Intrapancreatic
nerve invasion |
|
|
|
|
|
|
|
Absence/presence | 56/3 | 87/14 | 0.0822 |
|
|
|
| Retropancreatic
tissue invasion |
|
|
|
|
|
|
|
Absence/presence | 51/8 | 48/53 | <0.0010 | 3.1 | 1.1–10.6 | 0.0373 |
| Portal venous
system invasion |
|
|
|
|
|
|
|
Absence/presence | 12/47 | 18/83 | 0.6939 |
|
|
|
| Extrapancreatic
nerve plexus invasion |
|
|
|
|
|
|
|
Absence/presence | 22/37 | 13/88 | 0.0003 | 3.9 | 1.2–14.5 | 0.0264 |
| Arterial system
invasion |
|
|
|
|
|
|
|
Absence/presence | 3/56 | 2/99 | 0.2762 |
|
|
|
| K-ras mutation |
|
|
|
|
|
|
|
Negative/positive | 13/26 | 41/16 | 0.0002 | 5.2 | 2.07–14.2 | 0.0004 |
Discussion
PDAC is one of the most fatal forms of human
malignancy and exhibits a poor 5-year survival rate even following
curative resection and postoperative adjuvant chemotherapy
(5). The present study indicated that
long-term survivors following pancreatectomy can be predicted by a
combination of clinicopathological factors, including preCA19-9 and
DPM, which were prognostic factors independent of the cancer stage.
These factors have been repeatedly reported in previous studies,
therefore, they have been highly validated. However, to the best of
our knowledge, no studies have analyzed a combination of these
factors. In the current study, patients negative for both preCA19-9
and DPM (n=30) demonstrated a 5-year DSS of 68.5% following
surgery, with 25 of the patients undergoing postoperative adjuvant
chemotherapy. This finding recapitulated and validated our previous
study (13) and such prognostic
information may be useful in the development of optimal treatment
strategies for PDAC.
The most established biomarker for PDAC diagnosis
and prognosis is preCA19-9 (14,23–28).
Notably, preCA19-9 level could provide preoperative information and
serve as a preoperative prognostic factor potentially able to
affect the choice of treatment strategy, including the
administration of neoadjuvant therapy. The current study determined
that a pancreatectomy should be considered for patients with a low
preCA19-9 level, while those with a high level of preCA19-9 tend to
exhibit a poorer prognosis and may require neoadjuvant therapy
prior to surgery to improve their survival rate. Previously,
preoperative chemoradiation has been demonstrated to be a promising
strategy to treat aggressive pancreatic cancer, including
borderline resectable pancreatic cancer (10). The present study supports this novel
promising therapeutic strategy for patients with PDAC and a high
level preCA19-9.
By contrast, since DPM is a pathological factor, it
cannot be preoperatively informative and preoperative prediction of
future recurrence by DPM status is impossible. However, the present
study demonstrated that DPM could accurately predict long-term
survivors of PDAC following surgery, in combination with preCA19-9.
Notably, all cases of DPM-positive PDAC inevitably succumbed to the
disease; therefore, DPM status may indicate the tumor
aggressiveness of PDAC and reflect specific molecular features.
To the best of our knowledge, the current study was
the first to demonstrate that K-ras gene mutation is
significantly associated with DPM-positive status, compared with
DPM-negative status. K-ras gene mutation in the resected
margin of PDAC has been reported to be a marker representing a poor
prognosis (29,30). In the present study, K-ras gene
mutation was an independent predictor for DPM-positive status in
multivariate analysis. Supporting these results, PDAC clones with
mutated K-ras gene have previously been demonstrated to be
persistently present in the retroperitoneal margin. K-ras
gene mutation has been identified in pancreatic intraepithelial
neoplasia, which is a precursor lesion (31). In addition, a previous study that used
high-resolution analysis reported >90% of cases have K-ras
gene mutation in PDAC tumors (32,33). By
contrast, but similar to our studies, conventional methods to
investigate K-ras gene mutation have been widely reported.
In a recent meta-analysis (34), the
frequencies of K-ras gene mutations were reported to range
from 47 to 88%. In the present study, the low rate of K-ras
gene mutation is considered to be influenced by component rates of
a small number of tumor cells mixed with a large number of stromal
cells. Using conventional methods, it may be difficult to detect a
small number of K-ras gene mutations in tumors, and the
frequency of K-ras gene mutation therefore appears lower
compared with that observed using high resolution analysis
(35). An inducible
KrasG12D model elucidated that a precursor lesion with
an activated K-ras signal transforms to carcinoma but a precursor
lesion with an inactivated K-ras signal undergoes apoptosis
(36). These findings may support the
hypothesis that mutation of the K-ras gene is associated
with tumor aggressiveness and micrometastases, which have the
potential to disseminate systemically in DPM-positive patients, as
observed in the current study.
The detection rate of K-ras gene mutation in
the present study was low. However, previous studies have
identified the frequencies of K-ras gene mutation in other
cancer types using conventional methods and have repeatedly
demonstrated standard values (20,37–40).
Therefore, it can be suggested that the present result reflects the
conventional mutation rate of PDAC, which may represent dominant
clones in the tumor tissues. With regard to positive association of
DPM with K-ras gene mutation, validation was required for
different patient sets, however the experiments performed in the
current study could not be repeated due to technical reasons.
From 2014 to 2017, 96 patients with PDAC underwent a
pancreatectomy at Kitasato University Hospital and 6 cases were
examined for the K-ras gene mutation. Among the 6 patients
with PDAC, K-ras gene mutation was identified in 2 (33%);
patients with DPM-positive PDAC demonstrated a K-ras gene
mutation in 50% (1/2) of cases, while DPM-negative patients
exhibited a K-ras gene mutation in 25% (1/4) of cases. This
result was consistent with the aforementioned results of the
current study despite the small patient number. In the future,
learning sets should be co-analyzed. Finally, as the recruitment
period of the current study was long, numerous operators were
involved in the study. Therefore, a number of factors could cause
bias and affect the determination of DPM status. Periodical
validation is required to confirm the results of the current
study.
In conclusion, the present study validated and
reiterated the prognostic relevance of DPM and preCA19-9 in
patients with primary PDAC. This finding may be useful in the
development of a novel treatment strategy for patients with PDAC
and a poor prognosis. In addition, the current study revealed an
association of DPM status with K-ras gene mutation in PDAC.
This finding may facilitate the molecular understanding of PDAC and
assist the development of molecular targeted therapy. Similar to
other cancer types associated with a poor prognosis,
multidisciplinary treatment, including preoperative treatment and
aggressive surgery, and postoperative treatment, including
molecular targeted therapy, should be adopted to further improve
the prognosis of patients with PDAC. Thus, the present findings are
important.
Acknowledgements
The authors would like to thank Miss Tomomi Miyake
(Kitasato University School of Medicine) for her technical
assistance.
Funding
No funding was received.
Availability of data and materials
All data generated or analyzed during the present
study are included in this published article.
Authors' contributions
NN, YK and KYa designed the study and wrote the
initial draft of the manuscript. NN, YK and KYa analysed and
interpreted the data and assisted in the preparation of the
manuscript. HK, HU, KYo, TT, SI, KI, HT, TK, TY, MS, YK and MW
contributed to the collection and interpretation of the data and
critically reviewed the manuscript. All authors approved the final
version of the manuscript and agree to be accountable for all
aspects of the work in ensuring that questions related to the
accuracy or integrity of any part of the work are appropriately
investigated and resolved.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Review Board for Observation and Epidemiological Study, Kitasato
University Medical Ethics Organization (approval no. B18-017). All
patients agreed to the use of their samples in scientific research.
And, written informed consents were obtained from all patients.
This study only used these samples. All the data/samples were used
anonymously.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
International Agency for Research on
Cancer WHO. GLOBOCAN2012: Estimated Cancer Incidence, Mortality and
Prevalence. 2012.
|
|
2
|
American Cancer Society. Cancer Facts and
Figures 2014. American Cancer Society. 2014.
|
|
3
|
Rahib L, Smith BD, Aizenberg R, Rosenzweig
AB, Fleshman JM and Matrisian LM: Projecting cancer incidence and
deaths to 2030: The unexpected burden of thyroid, liver, and
pancreas cancers in the United States. Cancer Res. 74:2913–2921.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Hidalgo M: Pancreatic cancer. N Engl J
Med. 362:1605–1617. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Oettle H, Neuhaus P, Hochhaus A, Hartmann
JT, Gellert K, Ridwelski K, Niedergethmann M, Zülke C, Fahlke J,
Arning MB, et al: Adjuvant chemotherapy with gemcitabine and
long-term outcomes among patients with resected pancreatic cancer:
The CONKO-001 randomized trial. JAMA. 310:1473–1481. 2010.
View Article : Google Scholar
|
|
6
|
Kalser MH and Ellenberg SS: Pancreatic
cancer. Adjuvant combined radiation and chemotherapy following
curative resection. Arch Surg. 120:899–903. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Oettle H, Post S, Neuhaus P, Gellert K,
Langrehr J, Ridwelski K, Schramm H, Fahlke J, Zuelke C, Burkart C,
et al: Adjuvant chemotherapy with gemcitabine vs observation in
patients undergoing curative-intent resection of pancreatic cancer:
A randomized controlled trial. JAMA. 297:267–277. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Uesaka K, Boku N, Fukutomi A, Okamura Y,
Konishi M, Matsumoto I, Kaneoka Y, Shimizu Y, Nakamori S, Sakamoto
H, et al: Adjuvant chemotherapy of S-1 versus gemcitabine for
resected pancreatic cancer: A phase 3, open-label, randomised,
non-inferiority trial (JASPAC 01). Lancet. 388:248–257. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Neoptolemos JP, Dunn JA, Stocken DD,
Almond J, Link K, Beger H, Bassi C, Falconi M, Pederzoli P,
Dervenis C, et al: Adjuvant chemoradiotherapy and chemotherapy in
resectable pancreatic cancer: A randomised controlled trial.
Lancet. 358:1576–1585. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kim EJ, Ben-Josef E, Herman JM,
Bekaii-Saab T, Dawson LA, Griffith KA, Francis IR, Greenson JK,
Simeone DM, Lawrence TS, et al: A multi-institutional phase 2 study
of neoadjuvant gemcitabine and oxaliplatin with radiation therapy
in patients with pancreatic cancer. Cancer. 119:2692–2700. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Vogelstein B and Kinzler KW: Cancer genes
and the pathways they control. Nat Med. 10:789–799. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Yachida S, Jones S, Bozic I, Antal T,
Leary R, Fu B, Kamiyama M, Hruban RH, Eshleman JR, Nowak MA, et al:
Distant metastasis occurs late during the genetic evolution of
pancreatic cancer. Nature. 467:1114–1117. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Waraya M, Yamashita K, Katagiri H, Ishii
K, Takahashi Y, Furuta K and Watanabe M: Preoperative serum CA19-9
and dissected peripancreatic tissue margin as determiners of
long-term survival in pancreatic cancer. Ann Surg Oncol.
16:1231–1240. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Mirkin KA, Hollenbeak CS and Wong J:
Prognostic impact of carbohydrate antigen 19-9 level at diagnosis
in resected stage I–III pancreatic adenocarcinoma: A U.S.
population study. J Gastrointest Oncol. 8:778–788. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Allema JH, Reinders ME, van Gulik TM,
Koelemay MJ, Van Leeuwen DJ, de Wit LT, Gouma DJ and Obertop H:
Prognostic factors for survival after pancreaticoduodenectomy for
patients with carcinoma of the pancreatic head region. Cancer.
75:2069–2076. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wenger FA, Peter F, Zieren J, Steiert A,
Jacobi CA and Müller JM: Prognosis factors in carcinoma of the head
of the pancreas. Dig Surg. 17:29–35. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Japan Pancreas Society. Classification of
pancreatic carcinoma Tokyo: Kanahara; 2011
|
|
18
|
Sobin LH and Wittekind C: International
Union Againt Cancer (UICC): TNM classification of malignant tumors.
6th. New York: Wiley and Liss; 2002
|
|
19
|
National Comprehensive Cancer Network.
Clinical practice guidelines in oncology. Pancreatic
Adenocarcinoma. Version 2. 2016.
|
|
20
|
Yamashita K, Tatebayashi T, Shinoda H and
Okayasu I: Simplified rapid non-radioactive PCR-SSCP method applied
to K-ras mutation analysis. Pathol Int. 46:801–804. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yamashita K, Yoshida T, Shinoda H and
Okayasu I: Novel method for simultaneous analysis of p53 and K-ras
mutations and p53 protein expression in single histologic sections.
Arch Pathol Lab Med. 125:347–352. 2001.PubMed/NCBI
|
|
22
|
Kaplan EL and Meier P: Nonparametric
estimation from incomplete observations. J Am Stat Assoc.
53:457–481. 1958. View Article : Google Scholar
|
|
23
|
Piagnerelli R, Marrelli D, Roviello G,
Ferrara F, Di Mare G, Voglino C, Petrioli R, Marini M, Macchiarelli
R and Roviello F: Clinical value and impact on prognosis of
peri-operative CA 19-9 serum levels in stage I and II
adenocarcinoma of the pancreas. Tumour Biol. 37:1959–1966. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Chan A, Prassas I, Dimitromanolakis A,
Brand RE, Serra S, Diamandis EP and Blasutig IM: Validation of
biomarkers that complement CA19.9 in detecting early pancreatic
cancer. Clin Cancer Res. 20:5787–5795. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kondo N, Murakami Y, Uemura K, Hayashidani
Y, Sudo T, Hashimoto Y, Nakashima A, Sakabe R, Shigemoto N, Kato Y,
et al: Prognostic impact of perioperative serum CA 19-9 levels in
patients with resectable pancreatic cancer. Ann Surg Oncol.
17:2321–2329. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Harsha HC, Kandasamy K, Ranganathan P,
Rani S, Ramabadran S, Gollapudi S, Balakrishnan L, Dwivedi SB,
Telikicherla D, Selvan LD, et al: A compendium of potential
biomarkers of pancreatic cancer. PLoS Med. 6:e10000462009.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Berger AC, Garcia M Jr, Hoffman JP, Regine
WF, Abrams RA, Safran H, Konski A, Benson AB III, MacDonald J and
Willett CG: Postresection CA 19-9 predicts overall survival in
patients with pancreatic cancer treated with adjuvant
chemoradiation: A prospective validation by RTOG 9704. J Clin
Oncol. 26:5918–5922. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Hess V, Glimelius B, Grawe P, Dietrich D,
Bodoky G, Ruhstaller T, Bajetta E, Saletti P, Figer A, Scheithauer
W and Herrmann R: CA 19-9 tumour-marker response to chemotherapy in
patients with advanced pancreatic cancer enrolled in a randomised
controlled trial. Lancet Oncol. 9:132–138. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ohigashi H, Ishikawa O, Sasaki Y, Yamada
T, Furukawa H, Imaoka S, Kasugai T, Ishiguro S, Ueda K, Miyoshi Y
and Nakamura Y: K-ras point mutation in the nerve plexuses around
the superior mesenteric artery in resectable adenocarcinoma of the
pancreatic head: Distribution pattern and related factors. Arch
Surg. 135:1450–1455. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kim J, Reber HA, Dry SM, Elashoff D, Chen
SL, Umetani N, Kitago M, Hines OJ, Kazanjian KK, Hiramatsu S, et
al: Unfavourable prognosis associated with K-ras gene mutation in
pancreatic cancer surgical margins. Gut. 55:1598–1605. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ijichi H, Chytil A, Gorska AE, Aakre ME,
Fujitani Y, Fujitani S, Wright CV and Moses HL: Aggressive
pancreatic ductal adenocarcinoma in mice caused by
pancreas-specific blockade of transforming growth factor-beta
signaling in cooperation with active Kras expression. Genes Dev.
20:3147–3160. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Jones S, Zhang X, Parsons DW, Lin JC,
Leary RJ, Angenendt P, Mankoo P, Carter H, Kamiyama H, Jimeno A, et
al: Core signaling pathways in human pancreatic cancers revealed by
global genomic analyses. Science. 321:1801–1806. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Biankin AV, Waddell N, Kassahn KS, Gingras
MC, Muthuswamy LB, Johns AL, Miller DK, Wilson PJ, Patch AM, Wu J,
et al: Pancreatic cancer genomes reveal aberrations in axon
guidance pathway genes. Nature. 491:399–405. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Tao LY, Zhang LF, Xiu DR, Yuan CH, Ma ZL
and Jiang B: Prognostic significance of K-ras mutations in
pancreatic cancer: A meta-analysis. World J Surg Oncol. 14:1462016.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Knijn N, Mekenkamp LJ, Klomp M,
Vink-Börger ME, Tol J, Teerenstra S, Meijer JW, Tebar M, Riemersma
S, van Krieken JH, et al: KRAS mutation analysis: A comparison
between primary tumours and matched liver metastases in 305
colorectal cancer patients. Br J Cancer. 104:1020–1026. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Collins MA, Bednar F, Zhang Y, Brisset JC,
Galbán S, Galbán CJ, Rakshit S, Flannagan KS, Adsay NV and Pasca di
Magliano M: Oncogenic Kras is required for both the initiation and
maintenance of pancreatic cancer in mice. J Clin Invest.
122:639–653. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Onozato W, Yamashita K, Yamashita K, Kuba
T, Katoh H, Nakamura T, Sato T, Ihara A, Okayasu I and Watanabe M:
Genetic alterations of K-ras may reflect prognosis in stage III
colon cancer patients below 60 years of age. J Surg Oncol.
103:25–33. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Yamashita K, Kuba T, Shinoda H, Takahashi
E and Okayasu I: Detection of K-ras point mutations in the
supernatants of peritoneal and pleural effusions for diagnosis
complementary to cytologic examination. Am J Clin Pathol.
109:704–711. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Yamashita K, Kida Y, Shinoda H, Kida M and
Okayasu I: K-ras point mutations in the supernatants of pancreatic
juice and bile are reliable for diagnosis of pancreas and biliary
tract carcinomas complementary to cytologic examination. Jpn J
Cancer Res. 90:240–248. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Kawamata H, Yamashita K, Kojo K, Ushiku H,
Ooki A and Watanabe M: Discrepancies between the K-ras mutational
status of primary colorectal cancers and corresponding liver
metastases are found in codon 13. Genomics. 106:71–75. 2015.
View Article : Google Scholar : PubMed/NCBI
|