Introduction
Urothelial carcinoma of the upper urinary tract
(UC-UUT) tends to be associated with intravesical recurrence, lymph
node metastasis and distant metastasis, even after complete
surgical resection, presumably due to occult micrometastasis
present at the time of surgery and the thin wall and rich lymphatic
drainage of the ureter (1,2). While intravesical recurrence can be
controlled by transurethral resection, lymph node metastasis or
distant metastasis tends to be refractory to chemotherapy,
eventually leading to an unfavorable outcome (3). Advanced tumor stage, a higher nuclear
grade and lymphovascular invasion (LVI) of UC-UUT are pathological
factors conventionally associated with metastases and an
unfavorable outcome (2,4–6). Among
them, we have previously reported that LVI is associated with early
recurrence and an unfavorable outcome after radical
nephroureterectomy (1). Although
gemcitabine- and cisplatin-based chemotherapy is frequently
performed in an adjuvant setting for patients with such risk
factors, its efficacy tends to be disappointing because of not only
advanced age or renal dysfunction resulting from
nephroureterectomy, but also the paucity of established biomarkers
(7–10). Tegafur-uracil (UFT™, Taiho
Pharmaceutical Co., Ltd., Tokyo, Japan) is an oral form of
5-fluorouracil (5-FU) that can be administered to a wide range of
patients because of its lower incidence of severe adverse events
(11,12). 5-FU is generally administered as
adjuvant chemotherapy to patients with cancers of the lung and
colon (13–17), and its antitumor effect is thought to
be associated with the expression of enzymes related to 5-FU
metabolism, such as dihydropyrimidine dehydrogenase (DPD),
orotatephosphoribosyltransferase (OPRT) and thymidylate synthase
(TS) (18). Intravenously or orally
administered 5-FU is phosphorylated by OPRT and converted to
5-fluoro-2′-deoxyuridine 5′-monophosphate (FdUMP). It then inhibits
TS, which is a rate-limiting enzyme for pyrimidine synthesis, and
exerts an antitumor effect by inhibiting the synthesis of DNA.
However, most of the administered 5-FU is broken down by DPD and
thus unable to exert an antitumor effect (18). Therefore, underexpression of OPRT,
overexpression of TS and overexpression of DPD are reported to be
associated with 5-FU resistance in patients with urothelial
carcinoma (19–21). Thus, the efficacy of 5-FU
chemotherapy depends on inter-individual differences in the
activity of these enzymes. Although it has been reported that the
activity of these enzymes is associated with tumor stage or nuclear
grade, their role in carcinogenesis has not yet been elucidated
(19–22). On the other hand, there has been some
controversy regarding the efficacy of 5-FU as adjuvant chemotherapy
for UC-UUT. In the present study, we administered adjuvant 5-FU
chemotherapy to UC-UUT patients with LVI who were at risk of poor
outcome, and then we investigated the relationship between the
efficacy of adjuvant 5-FU chemotherapy for lymphovascular-invasive
UC-UUT and the expression of these enzymes, with the aim of
detecting an effective biomarker.
Materials and methods
Patients and tissues
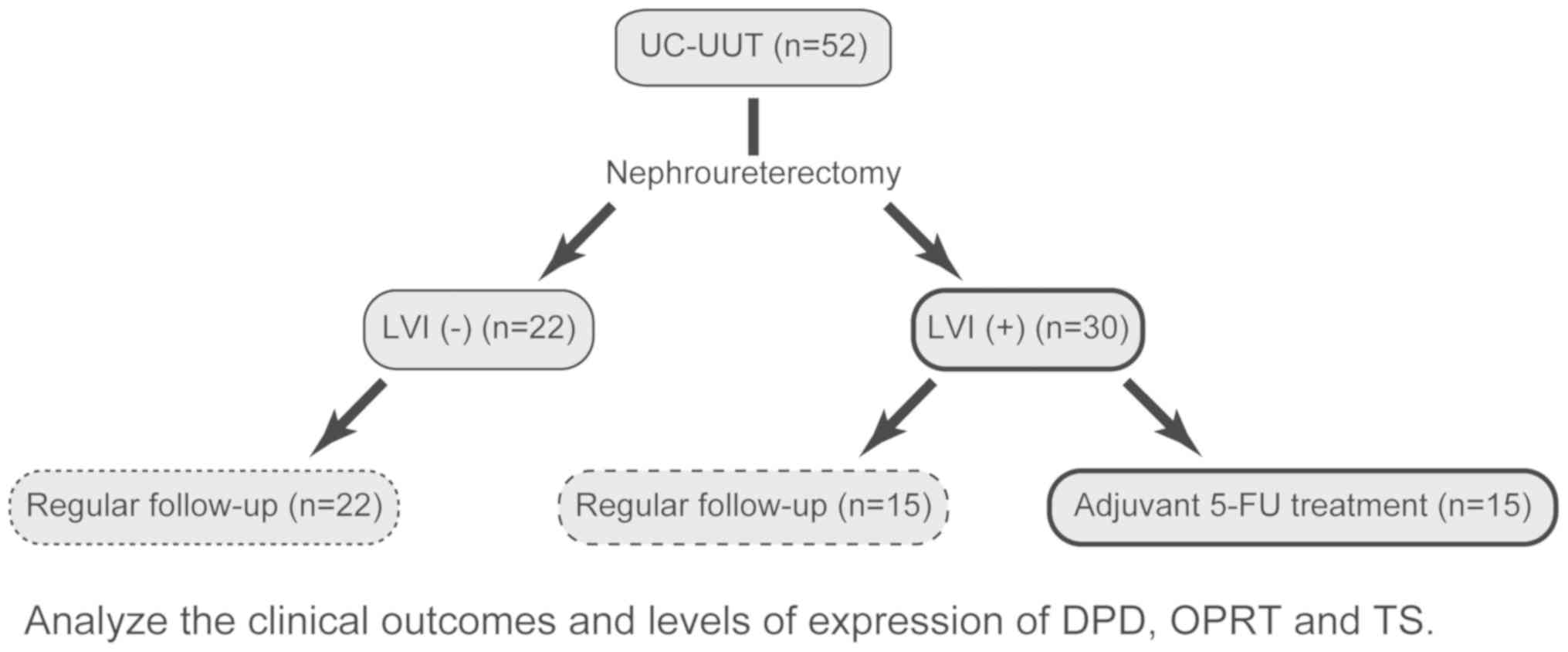
We retrieved archival formalin-fixed,
paraffin-embedded (FFPE) tumor samples from 52 Japanese patients
who had undergone nephroureterectomy for UC-UUT at Dokkyo Medical
University Hospital (Tochigi, Japan) between 2002 and 2015. After
surgical resection, UFT™ was administered at 200 mg/day to 15 of 30
patients with LVI who were ineligible for cisplatin-based adjuvant
chemotherapy (Fig. 1). The median
observation period was 44 months with a range of 1 to 145 months.
Table I shows the adjuvant 5-FU
treatment status and pathological data for the patients.
Pathological factors were assessed in accordance with the TNM tumor
classification (23). The sites of
initial relapse and adjuvant 5-FU treatment status are shown in
Table II. This study was conducted
in accordance with the Helsinki Declaration and approved by the
institutional ethics review board of Dokkyo Medical University
Hospital (approval no. 24023). Each patient signed an informed
consent form that had been approved by our institutional Committee
on Human Rights in Research. All samples were anonymized before
analysis to guarantee protection of patient privacy.
 | Table I.Conventional pathological factors and
adjuvant 5-FU treatment status. |
Table I.
Conventional pathological factors and
adjuvant 5-FU treatment status.
|
| pT | pN | Grade |
|---|
|
|
|
|
|
|---|
| Factors | ≤2 | ≥3 | 0 or X | ≥1 | ≤2 | 3 |
|---|
| LVI (+), 5-FU
(+) | 4 | 11 | 14 | 1 | 6 | 9 |
| LVI (+), 5-FU
(−) | 2 | 13 | 11 | 4 | 4 | 11 |
| LVI (−), 5-FU
(−) | 20 | 2 | 22 | 0 | 18 | 4 |
| Table II.Initial relapse site and adjuvant
5-FU treatment status. |
Table II.
Initial relapse site and adjuvant
5-FU treatment status.
| Variable | Urinary
bladder | Lymph node | Lung | Bone | Liver | Ureter | Local
recurrence | No relapse |
|---|
| LVI (+), 5-FU
(+) | 4 | 5 | 0 | 0 | 0 | 0 | 0 | 6 |
| LVI (+), 5-FU
(−) | 0 | 5 | 3 | 1 | 1 | 0 | 2 | 3 |
| LVI (−), 5-FU
(−) | 6 | 2 | 0 | 0 | 0 | 1 | 0 | 13 |
RNA extraction and quantitative
RT-PCR
Tumor cells were collected from FFPE tissue samples
using laser-capture microdissection. Total RNA was extracted from
the cells using an RNeasy FFPE kit (Qiagen, Inc., Valencia, CA,
USA), and cDNA was prepared using a High Capacity cDNA Reverse
Transcription kit (Applied Biosystems; Thermo Fisher Scientific,
Inc., Waltham, MA, USA) in accordance with the manufacturer's
instructions. The cDNA was then pre-amplified using a TaqMan PreAmp
Master Mix kit (Applied Biosystems; Thermo Fisher Scientific,
Inc.), and quantitative RT-PCR was performed using a TaqMan
low-density array (LDA) (Applied Biosystems; Thermo Fisher
Scientific, Inc.) for determining the relative levels of expression
of mRNAs for DPD, OPRT and TS, as reported previously
(24,25). Briefly, 2.5 µl of cDNA was
pre-amplified using 2× TaqMan PreAmp Master Mix and a pool of 0.2×
TaqMan Gene Expression Assays in a 10-µl PCR reaction volume
(Applied Biosystems; Thermo Fisher Scientific, Inc.).
Pre-amplification was performed under the following thermal cycling
conditions: 95°C for 10 min followed by 14 cycles at 95°C for 15
sec, and 60°C for 4 min. A pre-amplified cDNA sample was diluted
20-fold in Tris-EDTA buffer, then 25 µl of pre-amplified cDNA was
added to 25 µl of nuclease-free water and 50 µl of 2× TaqMan Gene
Expression Master Mix (Applied Biosystems; Thermo Fisher
Scientific, Inc.). The mixture was then applied to the loading port
of the TaqMan LDA. The LDA was centrifuged twice and PCR
amplification was performed using the ABI Prism 7900HT Sequence
Detection System (Applied Biosystems; Thermo Fisher Scientific,
Inc.). The thermal cycling conditions for PCR amplification were as
follows: 50°C for 2 min and 94.5°C for 10 min followed by 40 cycles
at 97°C for 30 sec and 59.7°C for 1 min. The quantitative cycle
(Cq) value detected was inversely proportional to the amount of
cDNA. The Cq value for β-actin (ACTB) included in the LDA
was used as a reference. The expression levels of the 3 genes
relative to that of ACTB were calculated as the ratios
between the differences in the Cq values (26).
Statistical analysis
Differences between two groups were analyzed by
Mann-Whitney U test. Overall survival (OS) and progression-free
survival (PFS) curves were drawn by the Kaplan-Meier method, and
differences in survival were examined by log-rank test with
Bonferroni correction for pairwise multiple comparisons. In all
analyses, P<0.05 (Bonferroni adjusted P<0.0167) was
considered to indicate a statistically significant difference. Data
were analyzed using R version 3.2.2 (www.r-project.org).
Results
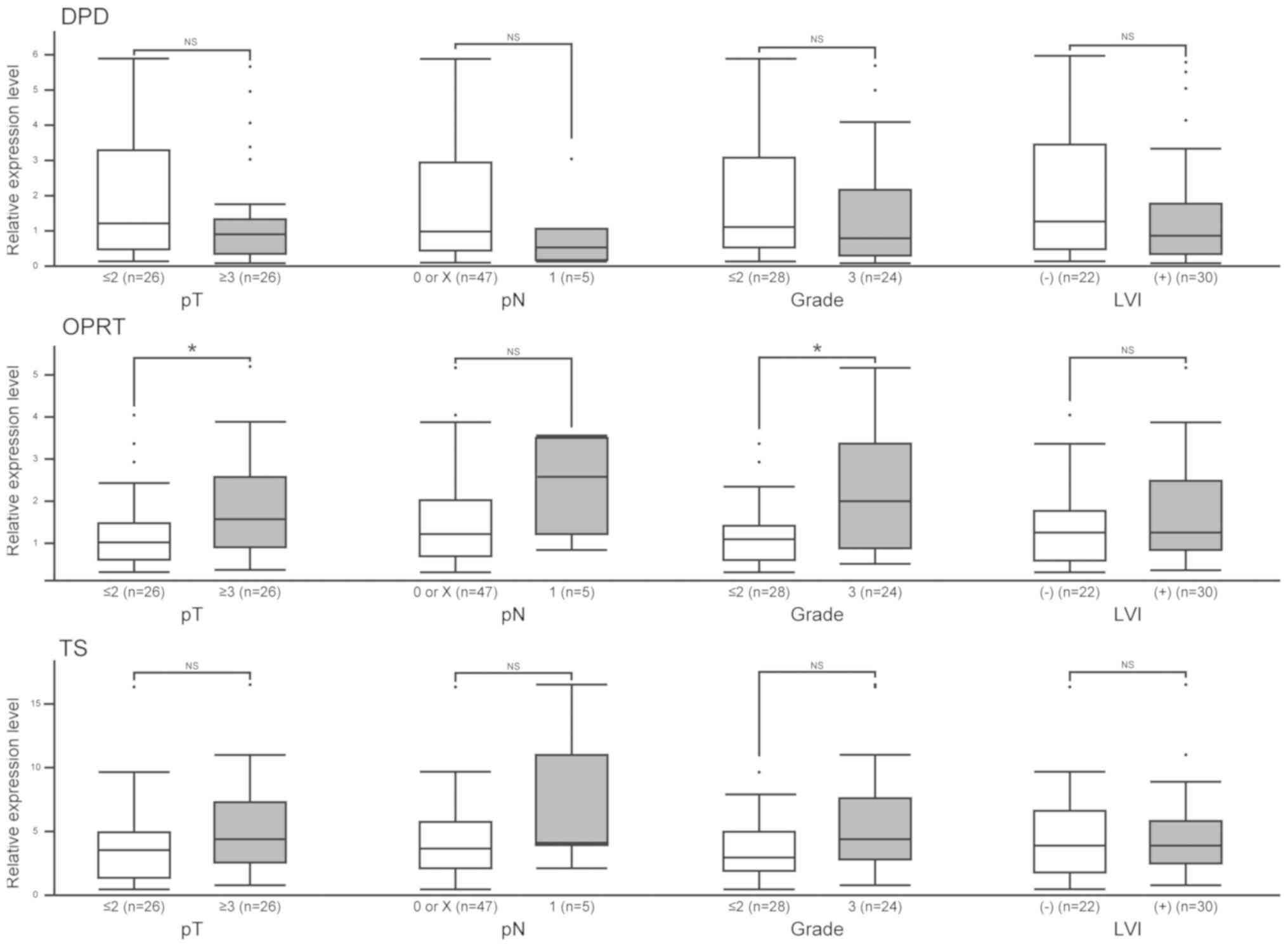
Levels of DPD, OPRT and TS expression
are not associated with pathological factors
Clinicopathological characteristics of the patients
are shown in Table SI. There were
39 male and 13 female patients with a mean age of 70 years (rage
45–85 years). None of them developed any severe adverse events. We
first analyzed the relationship between conventional pathological
factors and the levels of expression of enzymes related to 5-FU
metabolism. The levels of DPD, OPRT and TS expression
were not associated with pT stage, pN stage, nuclear grade or LVI;
however, higher expression of OPRT was associated with high
pT stage and nuclear grade (Fig.
2).
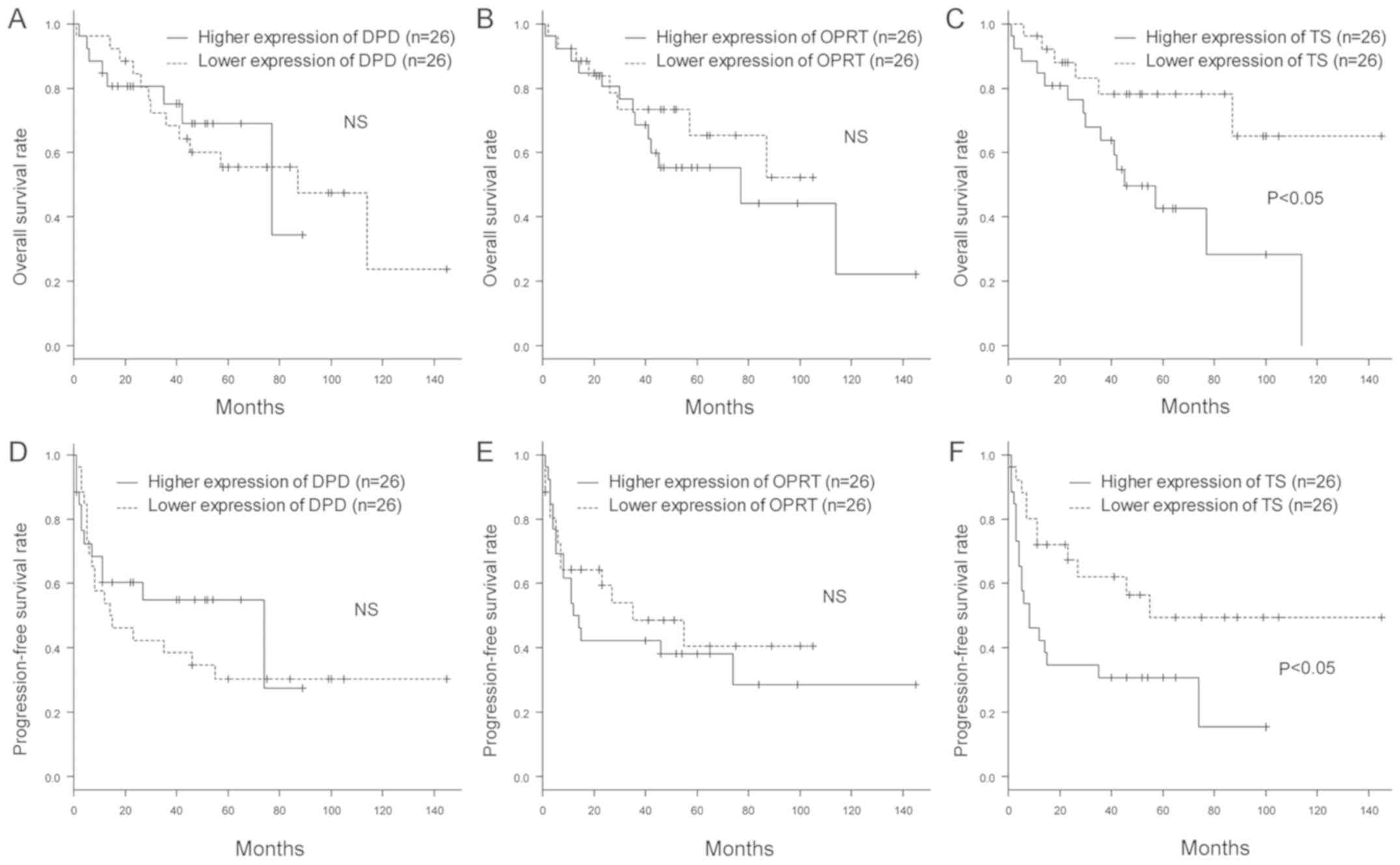
Levels of DPD and OPRT expression are
not associated with clinical outcomes
We then investigated the influences of DPD,
OPRT and TS expression on OS and PFS in UC-UUT patients.
We divided the patients into two groups according to the median
level of expression of each gene, and compared the OS and PFS rates
between them. Kaplan-Meier plots showed that patients with higher
expression of TS had poorer OS and PFS rates than those with
lower expression. On the other hand, the levels of DPD and
OPRT expression were not associated with the OS and PFS
rates (Fig. 3). Furthermore, to
exclude the influence of adjuvant 5-FU chemotherapy on outcome, we
excluded the patients who had received 5-FU and also compared the
OS and PFS rates between them according to the expression of each
gene. The patients with lower expression of DPD and higher
expression of TS had poorer PFS rates. However, the level of
TS expression was not associated with OS rate (Fig. S1).
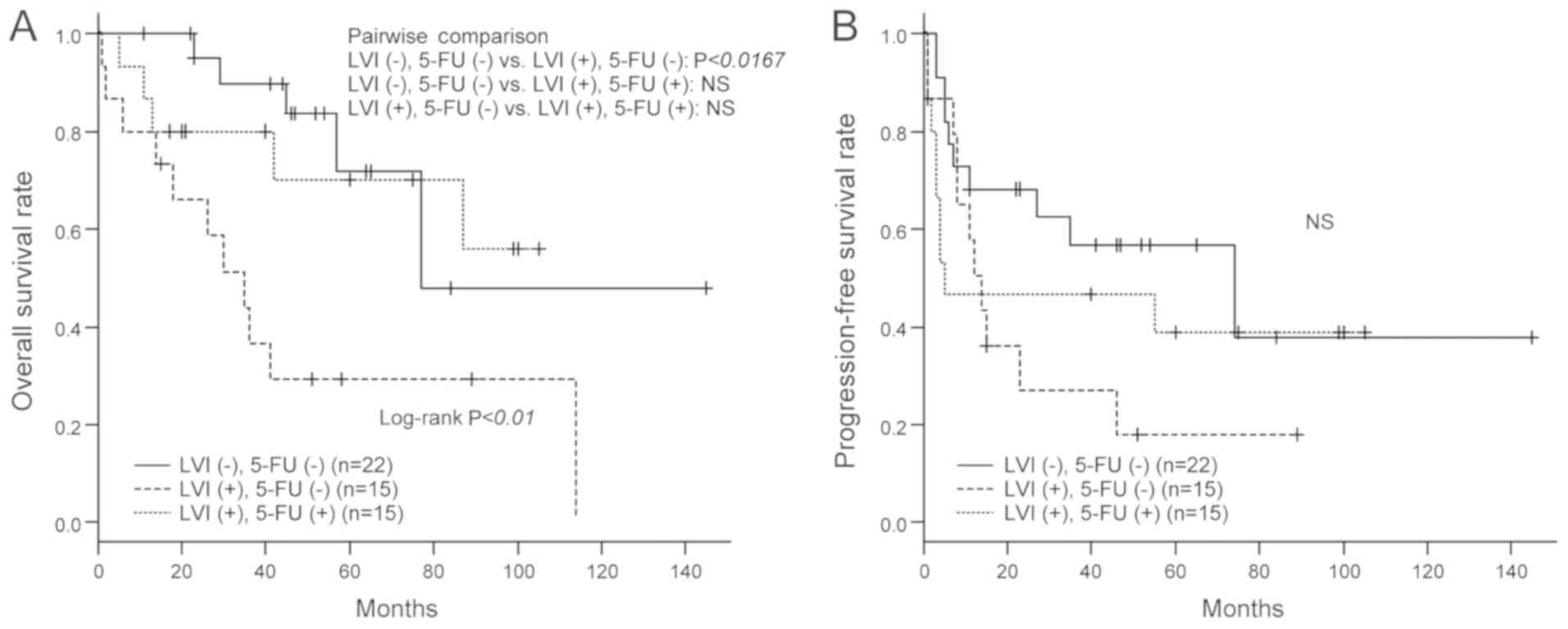
Poor outcome of UC-UUT with LVI and
efficacy of adjuvant 5-FU chemotherapy
To evaluate the efficacy of adjuvant 5-FU
chemotherapy, we compared the OS and PFS rates among the three
groups of patients divided according to LVI and 5-FU treatment
status. As shown in Fig. 4A, UC-UUT
patients with LVI had poorer OS than those without LVI. However,
there were no significant inter-group differences between UC-UUT
patients with LVI and those without LVI when adjuvant 5-FU was
administered to the former. We also investigated the improvement of
OS rates resulting from adjuvant 5-FU administration in UC-UUT
patients with LVI, but the degree of improvement did not reach a
statistically significant level. The PFS rates showed no
significant inter-group differences (Fig. 4B).
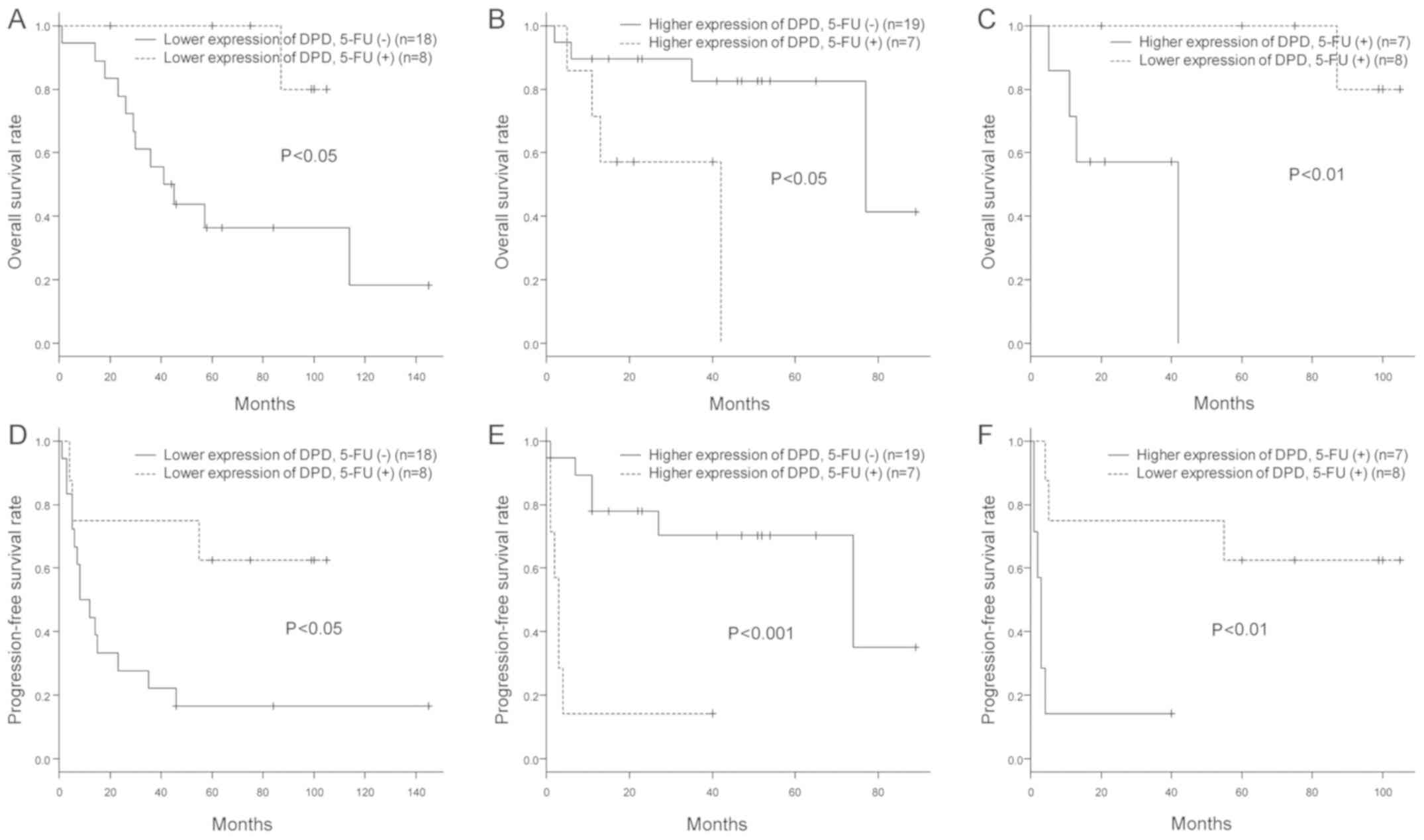
Adjuvant 5-FU chemotherapy improves
the OS and PFS rates of patients with lymphovascular-invasive
UC-UUT and lower DPD expression
We further investigated the relationship between the
efficacy of adjuvant 5-FU chemotherapy for lymphovascular-invasive
UC-UUT and the levels of expression of enzymes related to 5-FU
metabolism. We classified the patients according to their median
level of expression of DPD, OPRT or TS, and then
analyzed their OS and PFS rates in relation to 5-FU administration
status. Interestingly, patients who had received 5-FU, especially
those whose primary tumors had lower levels of DPD
expression, had better OS and PFS rates (Fig. 5A and D). On the other hand, patients
with higher expression of DPD had rather poor OS and PFS
rates, regardless of 5-FU administration (Fig. 5B and E). Furthermore, among the
patients who had received 5-FU, the OS and PFS rates were better
for those who had lower expression of DPD than for those who
had higher expression (Fig. 5C and
F). No significant relationships were found between the
efficacy of adjuvant 5-FU chemotherapy and the levels of
OPRT and TS expression (Figs. S2 and S3).
Discussion
Complete surgical resection is one of the most
important factors for eradication of UC-UUT. However, even when
this has been achieved, some patients, particularly those with LVI,
suffer early recurrence and metastasis, and have poorer clinical
outcomes (1,3–5). In this
study also, patients with LVI showed poorer OS rates than those
without LVI. It is difficult to control distant metastasis of
UC-UUT by surgical resection (27),
and therefore the efficacy of chemotherapy is limited (3,28).
Considering these characteristics of UC-UUT, it can be concluded
that reducing the incidence of recurrence and distant metastasis is
the most important consideration if clinical outcomes are to be
improved. Although cisplatin-based adjuvant chemotherapy is often
performed for UC-UUT patients with risk factors for recurrence or
distant metastasis, its efficacy is debatable due to the
nephrotoxicity of cisplatin and the impairment of renal function
caused by nephroureterectomy (7–10).
Furthermore, no biomarkers that can predict the efficacy of
chemotherapy have yet been established.
UFT™ is an oral prodrug of 5-FU that is associated
with less severe adverse events, and can be used for a wider
variety of patients (11,12). In fact, adjuvant chemotherapy with
this oral form of 5-FU, which contains a DPD inhibitor, is commonly
used for patients with lung and colon cancer, and helps to improve
their prognosis (13–17). Some groups have reported the efficacy
of adjuvant chemotherapy with oral 5-FU for urothelial carcinoma of
the urinary bladder, although no unified view has yet emerged
(29–31). Also, the efficacy of adjuvant 5-FU
chemotherapy for UC-UUT has not yet been investigated (21). The present study was designed to
assess the efficacy of 5-FU for reducing the rate of recurrence and
prolonging the survival of UC-UUT patients undergoing radical
nephroureterectomy, especially those with LVI. None of the patients
included developed any severe adverse events associated with the
oral 5-FU agent, suggesting that this form of adjuvant chemotherapy
may be an effective option, especially for UC-UUT patients with LVI
who are not eligible for cisplatin-based adjuvant chemotherapy.
Even though UC-UUT patients with LVI may be at risk of poor
outcome, we found no significant difference in OS rates after 5-FU
administration between them and UC-UUT patients without LVI.
However, despite the importance of reducing the rates of recurrence
and distant metastasis in patients with UC-UUT, we found that
adjuvant 5-FU chemotherapy did not significantly improve the PFS.
This might have been attributable to the small number of patients
we analyzed, and the fact that intravesical recurrence can be
treated easily by transurethral resection. In fact, Harada et
al (31) have reported that
adjuvant chemotherapy using oral 5-FU for urothelial carcinoma of
the urinary bladder did not reduce the incidence of intravesical
recurrence. Interestingly, despite the small number of UC-UUT
patients we studied, those with LVI who had received adjuvant 5-FU
did not develop visceral metastases, in contrast to those who had
not received it. These results suggest that adjuvant 5-FU
chemotherapy might reduce the incidence of visceral metastasis, and
thus improve prognosis.
We also investigated biomarkers that could be
applicable for predicting the efficacy of adjuvant 5-FU
chemotherapy. It is well known that the antitumor effect of 5-FU is
influenced by the activities of enzymes related to its metabolism,
such as DPD, OPRT and TS. In urothelial carcinoma, underexpression
of OPRT, overexpression of TS and overexpression of DPD are
reported to be associated with 5-FU resistance in vitro and
in vivo (19–21). To our knowledge, no previous studies
have investigated the correlation between the efficacy of adjuvant
5-FU chemotherapy and the levels of expression of 5-FU
metabolism-related enzymes in patients with UC-UUT. In this study,
when we focused on the relationship between 5-FU administration and
DPD expression, we found that both the OS and PFS rates for
patients with lower DPD expression were improved by adjuvant
5-FU therapy to a greater degree than in patients who did not
receive 5-FU. Taking into consideration that all of the patients
who received 5-FU chemotherapy were LVI-positive and thus at risk
of a poor outcome, these results suggest that the level of
DPD expression had a major influence on the efficacy of
adjuvant 5-FU chemotherapy for UC-UUT, and that such chemotherapy
would be highly effective for patients with lower expression of
DPD. On the other hand, the patients with higher expression
of DPD showed poorer OS and PFS rates, despite
administration of adjuvant 5-FU. This might have been due to
immediate breakdown of 5-FU by DPD, and the fact that the adjuvant
5-FU group included patients with LVI. In addition, among the
patients who received 5-FU, the OS and PFS rates for those with
lower expression of DPD were better than those for patients
with higher expression. These results support the contention that
the level of DPD expression influences the efficacy of
adjuvant 5-FU chemotherapy for UC-UUT. Although DPD deficiency has
been reported to increase the toxicity of 5-FU (18), none of the present patients developed
any severe adverse events, irrespective of DPD expression.
This may have been attributable to the low dose of 5-FU we
administered.
In association with pathological factors, some
groups have reported that DPD, OPRT and TS are associated with a
high stage and high grade of urothelial carcinoma (19–22), and
that OPRT and TS expression are associated with poor outcome
(19,21,22),
although DPD was not reported to be associated with outcome
(20,21). Despite an apparent association of
OPRT and TS expression with tumor cell proliferation, their role in
carcinogenesis has not yet been confirmed (19,22). The
associations among pathological factors, outcomes, 5-FU sensitivity
and expression of some enzymes demonstrated in the present study
were not concordant with previous reports, possibly because we
analyzed samples of mRNA rather than protein expression or enzyme
activity. Furthermore, biological differences in the cell lines and
patients studied might have affected 5-FU sensitivity. In
particular, TS and DPD expression might have had a
stronger influence on outcome and 5-FU sensitivity than other
factors. However, no definitive conclusion can be drawn at this
stage.
Our present findings suggest that the level of
DPD expression in patients undergoing surgical resection for
UC-UUT might be a useful biomarker for predicting the efficacy of
adjuvant 5-FU chemotherapy. Although this study was designed to
investigate the level of DPD mRNA expression in tumor
specimens, it has been reported that the levels of mRNA expression
and protein activity of DPD are not necessarily correlated
(18). Because the present data were
limited in view of our retrospective design and the small numbers
of patients studied, it will be necessary to conduct a large-scale
randomized controlled trial to investigate the activity of DPD
protein, interactions among enzymes related to 5-FU metabolism, and
the metabolic pathways associated with the efficacy of 5-FU for
treatment of UC-UUT. In addition, an oral 5-FU agent including a
stronger DPD inhibitor, such as tegafur/gimeracil/oteracil (S-1™)
(Taiho Pharmaceutical Co., Ltd.), might be more effective for
patients with higher expression of DPD who do not show a
good response to the UFT™ that was employed in the present study
(32).
In conclusion, adjuvant 5-FU chemotherapy can
improve the outcome of patients with lymphovascular-invasive UC-UUT
and low expression of DPD. Assessment of the DPD
expression level in UC-UUT might therefore be helpful for
predicting the effectiveness of adjuvant 5-FU chemotherapy.
Supplementary Material
Supporting Data
Acknowledgements
The authors would like to thank Dr Kyoko Arai and
Mrs. Hitomi Yamazaki (Department of Urology, Dokkyo Medical
University, Tochigi, Japan) for their technical assistance.
Funding
This work was supported in part by Taiho
Pharmaceutical Co., Ltd.
Availability of data and materials
The datasets analyzed during the present study are
available from the corresponding author on reasonable request.
Authors' contributions
TN and TaK conceived and designed the study. TN,
TsK, HA, TU, YT, IS, KS, KT, DN, GN, HK, HY, HB and TaK acquired
the clinical data and samples. TN and TaK performed the experiments
and statistical analyses, and interpreted the data. TN wrote the
manuscript. TaK critically revised the manuscript for important
intellectual content and supervised the project. All authors read
and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Ethics Review Board of Dokkyo Medical University Hospital (Tochigi,
Japan) and was conducted in accordance with the Helsinki
Declaration. Each patient signed an informed consent form that had
been approved by our Institutional Committee on Human Rights in
Research.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
UC-UUT
|
urothelial carcinoma of the upper
urinary tract
|
|
LVI
|
lymphovascular invasion
|
|
5-FU
|
5-fluorouracil
|
|
DPD
|
dihydropyrimidine dehydrogenase
|
|
OPRT
|
orotatephosphoribosyltransferase
|
|
TS
|
thymidylate synthase
|
|
FdUMP
|
5-fluoro-2′-deoxyuridine
5′-monophosphate
|
|
FFPE
|
formalin-fixed, paraffin-embedded
|
|
LDA
|
low-density array
|
|
Cq
|
quantitative cycle
|
|
ACTB
|
β-actin
|
|
OS
|
overall survival
|
|
PFS
|
progression-free survival
|
References
|
1
|
Kamai T, Shirataki H, Nakanishi K, Furuya
N, Kambara T, Abe H, Oyama T and Yoshida K: Increased Rac1 activity
and Pak1 overexpression are associated with lymphovascular invasion
and lymph node metastasis of upper urinary tract cancer. BMC
Cancer. 10:1642010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Hall MC, Womack S, Sagalowsky AI, Carmody
T, Erickstad MD and Roehrborn CG: Prognostic factors, recurrence,
and survival in transitional cell carcinoma of the upper urinary
tract: A 30-year experience in 252 patients. Urology. 52:594–601.
1998. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Tanaka N, Kikuchi E, Kanao K, Matsumoto K,
Kobayashi H, Miyazaki Y, Ide H, Obata J, Hoshino K, Shirotake S, et
al: Patient characteristics and outcomes in metastatic upper tract
urothelial carcinoma after radical nephroureterectomy: The
experience of Japanese multi-institutions. BJU Int. 112:E28–E34.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kikuchi E, Margulis V, Karakiewicz PI,
Roscigno M, Mikami S, Lotan Y, Remzi M, Bolenz C, Langner C, Weizer
A, et al: Lymphovascular invasion predicts clinical outcomes in
patients with node-negative upper tract urothelial carcinoma. J
Clin Oncol. 27:612–618. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kikuchi E, Horiguchi Y, Nakashima J,
Hatakeyama N, Matsumoto M, Nishiyama T and Murai M: Lymphovascular
invasion independently predicts increased disease specific survival
in patients with transitional cell carcinoma of the upper urinary
tract. J Urol. 174:2120–2124. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Ozsahin M, Zouhair A, Villà S, Storme G,
Chauvet B, Taussky D, Gouders D, Ries G, Bontemps P, Coucke PA and
Mirimanoff RO: Prognostic factors in urothelial renal pelvis and
ureter tumours: A multicentre Rare Cancer Network study. Eur J
Cancer. 35:738–743. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Fujita K, Inamoto T, Yamamoto Y, Tanigawa
G, Nakayama M, Mori N, Tsujihata M, Azuma H, Nonomura N and Uemura
M: Role of adjuvant chemotherapy for lymph node-positive upper
tract urothelial carcinoma and the prognostic significance of
C-reactive protein: A multi-institutional, retrospective study. Int
J Urol. 22:1006–1012. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kim HS, Lee JS, Jeong CW, Kwak C, Kim HH
and Ku JH: Adjuvant chemotherapy for locally advanced upper tract
urothelial carcinoma: Updated results of the Seoul National
University Hospital experience. Int Braz J Urol. 41:1067–1079.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kaag MG, O'Malley RL, O'Malley P, Godoy G,
Chen M, Smaldone MC, Hrebinko RL, Raman JD, Bochner B, Dalbagni G,
et al: Changes in renal function following nephroureterectomy may
affect the use of perioperative chemotherapy. Eur Urol. 58:581–587.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Lane BR, Smith AK, Larson BT, Gong MC,
Campbell SC, Raghavan D, Dreicer R, Hansel DE and Stephenson AJ:
Chronic kidney disease after nephroureterectomy for upper tract
urothelial carcinoma and implications for the administration of
perioperative chemotherapy. Cancer. 116:2967–2973. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ho DH, Pazdur R, Covington W, Brown N, Huo
YY, Lassere Y and Kuritani J: Comparison of 5-fluorouracil
pharmacokinetics in patients receiving continuous 5-fluorouracil
infusion and oral uracil plus
N1-(2′-tetrahydrofuryl)-5-fluorouracil. Clin Cancer Res.
4:2085–2088. 1998.PubMed/NCBI
|
|
12
|
Borner MM, Schoffski P, de Wit R,
Caponigro F, Comella G, Sulkes A, Greim G, Peters GJ, van der Born
K, Wanders J, et al: Patient preference and pharmacokinetics of
oral modulated UFT versus intravenous fluorouracil and leucovorin:
A randomised crossover trial in advanced colorectal cancer. Eur J
Cancer. 38:349–358. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hamada C, Tanaka F, Ohta M, Fujimura S,
Kodama K, Imaizumi M and Wada H: Meta-analysis of postoperative
adjuvant chemotherapy with tegafur-uracil in non-small-cell lung
cancer. J Clin Oncol. 23:4999–5006. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hamada C, Tsuboi M, Ohta M, Fujimura S,
Kodama K, Imaizumi M and Wada H: Effect of postoperative adjuvant
chemotherapy with tegafur-uracil on survival in patients with stage
IA non-small cell lung cancer: An exploratory analysis from a
meta-analysis of six randomized controlled trials. J Thorac Oncol.
4:1511–1516. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kato T, Ohashi Y, Nakazato H, Koike A,
Saji S, Suzuki H, Takagi H, Nimura Y, Hasumi A, Baba S, et al:
Efficacy of oral UFT as adjuvant chemotherapy to curative resection
of colorectal cancer: Multicenter prospective randomized trial.
Langenbecks Arch Surg. 386:575–581. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Akasu T, Moriya Y, Ohashi Y, Yoshida S,
Shirao K and Kodaira S; National Surgical Adjuvant Study of
Colorectal Cancer, : Adjuvant chemotherapy with uracil-tegafur for
pathological stage III rectal cancer after mesorectal excision with
selective lateral pelvic lymphadenectomy: A multicenter randomized
controlled trial. Jpn J Clin Oncol. 36:237–244. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sakamoto J, Hamada C, Yoshida S, Kodaira
S, Yasutomi M, Kato T, Oba K, Nakazato H, Saji S and Ohashi Y: An
individual patient data meta-analysis of adjuvant therapy with
uracil-tegafur (UFT) in patients with curatively resected rectal
cancer. Br J Cancer. 96:1170–1177. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Maring JG, Groen HJ, Wachters FM, Uges DR
and de Vries EG: Genetic factors influencing pyrimidine-antagonist
chemotherapy. Pharmacogenomics J. 5:226–243. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Mizutani Y, Wada H, Fukushima M, Yoshida
O, Nakanishi H, Li YN and Miki T: Prognostic significance of
orotate phosphoribosyltransferase activity in bladder carcinoma.
Cancer. 100:723–731. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mizutani Y, Wada H, Fukushima M, Yoshida
O, Ukimura O, Kawauchi A and Miki T: The significance of
dihydropyrimidine dehydrogenase (DPD) activity in bladder cancer.
Eur J Cancer. 37:569–575. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ide H, Kikuchi E, Hasegawa M, Kozakai N,
Kosaka T, Miyajima A and Oya M: Prognostic significance of
5-fluorouracil metabolism-relating enzymes and enhanced
chemosensitivity to 5-fluorouracil by 5-chloro
2,4-dihydroxy-pyridine in urothelial carcinoma. BMC Cancer.
12:4202012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mizutani Y, Wada H, Ogawa O, Yoshida O,
Fukushima M, Nonomura N and Miki T: Prognostic significance of
thymidylate synthase activity in bladder carcinoma. Cancer.
92:510–518. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sobin LH, Gospodarowicz MK and Wittekind
C: TNM classification of malignant tumours. Wiley-Blackwell. (New
Jersey). 2009.
|
|
24
|
Kimura M, Imamura F, Inoue T, Nishino K,
Uchida J, Kumagai T, Okami J, Higasiyama M and Kamoshida S: Protein
and mRNA expression of folic acid-associated enzymes as biomarkers
for the cytotoxicity of the thymidylate synthase-targeted drugs,
pemetrexed and S-1, in non-small cell lung cancer. Mol Clin Oncol.
7:15–23. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Ichikawa W, Terashima M, Ochiai A, Kitada
K, Kurahashi I, Sakuramoto S, Katai H, Sano T, Imamura H and Sasako
M: Impact of insulin-like growth factor-1 receptor and amphiregulin
expression on survival in patients with stage II/III gastric cancer
enrolled in the adjuvant chemotherapy trial of S-1 for gastric
cancer. Gastric Cancer. 20:263–273. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Abe T, Kitamura H, Obara W, Matsumura N,
Tsukamoto T, Fujioka T, Hara I, Murai S, Shinohara N and Nonomura
K: Outcome of metastasectomy for urothelial carcinoma: A
multi-institutional retrospective study in Japan. J Urol.
191:932–936. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Tanji N, Ozawa A, Miura N, Yanagihara Y,
Sasaki T, Nishida T, Kikugawa T, Ikeda T, Ochi T, Shimamoto K, et
al: Long-term results of combined chemotherapy with gemcitabine and
cisplatin for metastatic urothelial carcinomas. Int J Clin Oncol.
15:369–375. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kubota Y, Noguchi S and Hosaka M: UFT in
bladder cancer. Oncology (Williston Park). 13 (Suppl 3):S112–S115.
1999.
|
|
30
|
Kubota Y, Hosaka M, Fukushima S and Kondo
I: Prophylactic oral UFT therapy for superficial bladder cancer.
Cancer. 71:1842–1845. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Harada K, Miyake H, Terakawa T and
Fujisawa M: Significance of uracil/tegafur for preventing
intravesical recurrence of non-muscle invasive urothelial carcinoma
of the bladder. Curr Urol. 6:27–32. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Takechi T, Fujioka A, Matsushima E and
Fukushima M: Enhancement of the antitumour activity of
5-fluorouracil (5-FU) by inhibiting dihydropyrimidine dehydrogenase
activity (DPD) using 5-chloro-2,4-dihydroxypyridine (CDHP) in human
tumour cells. Eur J Cancer. 38:1271–1277. 2002. View Article : Google Scholar : PubMed/NCBI
|