Introduction
Hashimoto's thyroditis (HT), also known as chronic
lymphocytic thyroiditis, is a specific autoimmune disease.
Currently its pathogenesis remains unclear (1). According to literature (2), HT may be associated with genetic
deletions. Congenital immunodeficiency, as a result of genetic
deletions, causes immune dysfunction in patients. Thyroiditis
occurs when thyroid follicular epithelium is damaged. In clinic, HT
is a common form of thyroiditis. Patients with HT do not have
prominent clinical manifestations at the early stage. When patients
are admitted to the hospital, the disease is already serious
(3). HT can be complicated by a
variety of thyroid diseases, of which, thyroid carcinoma (TC) is
the most serious one (4).
TC is a common cancer treated in Department of
General Surgery, accounting for only 1% of all malignant tumors.
However, its incidence ranks first among malignant tumors in the
human endocrine system (5).
Statistics show that the incidence of TC is increasing year by
year, and the patients tend to be diagnosed with TC at a younger
age (6). It was reported that TC
patients are mostly females, and the ratio of male to female is
approximately 1:2.5–3 (7). TC has a
wide age range of onset, ranging from adolescents to elderly, and
the average age of onset is approximately 40 years. Surgical
resection is the major treatment of TC. Surgery combined with
chemotherapy can significantly improve patient survival (8). Due to the absence of prominent clinical
manifestations at the early stage, TC is easily neglected by
patients, resulting in missing the optimal time for treatment.
Misdiagnosis can also occur in clinic due to the occult nature of
TC, such as slow disease progression and similarity to nodular
goiter (9). Therefore, a reliable
biomarker is needed in the diagnosis and treatment of combined HT
and TC.
The role of microRNAs (miRNAs) in various human
diseases has become a hot research topic in recent years. miRNAs
are a class of short non-coding RNA molecules containing 19–22
nucleotides. They are highly conserved molecules and are involved
in the regulation of target genes by binding to 3′ untranslated
regions (3′-UTRs) of the target gene in a completely or
incompletely complementary manner (10). According to literature, a variety of
miRNAs are closely associated with cancer onset and progression,
often playing the role of cancer suppressor genes or cancer
promoting genes (11). It was
reported that miRNA-146b-5p is associated with TC invasion and
migration, but not associated with HT (12). To the best of our knowledge,
association of miRNA-146b-5p with combined TC and HT has not been
reported. In this study, the tissue expression levels of
miRNA-146b-5p in patients with TC in combination with HT were
evaluated, and its clinical significance was analyzed, in order to
provide a reference for clinical practice.
Patients and methods
Eighty-seven patients who underwent thyroid surgery
in The Third Affiliated Hospital of Southern Medical University
(Guangzhou, China) from March 2010 to February 2013 were enrolled
in this study. Fresh specimens of cancer tissues and paracancerous
tissues (5 mm away from the cancer border) were collected and
transferred to liquid nitrogen for storage 5–10 min after surgery.
After pathological tests, 37 of 87 patients were diagnosed with TC
(group A), and 50 were diagnosed with TC in combination with HT
(group B). In group A, there were 10 males and 27 females, and the
patients were aged 33–58 years, with an average age of 44.2±9.9
years. The pathological types in group A included 30 cases of
papillary carcinoma, 5 cases of follicular carcinoma, and 2 cases
of medullary carcinoma. In group B, there were 15 males and 35
females, and the patients were aged 24–62 years, with an average
age of 45.8±8.9 years. The pathological types in group B included
40 cases of papillary carcinoma, 7 cases of follicular carcinoma,
and 3 cases of medullary carcinoma. During the same time period,
further 40 patients with HT only were collected (group C). In group
C, there were 15 males and 25 females, and the patients were aged
30–55 years, with an average age of 44.8±9.1 years. Variables such
as sex and age were comparable in the three groups, and the
differences were not statistically significant. The study was
approved by the Medical Ethics Committee of The Third Affiliated
Hospital of Southern Medical University. The patients and their
families were informed and signed an informed consent.
Inclusion and exclusion criteria
Patients who met the following criteria were
eligible for the study: i) Patients older than 18 years; ii)
patients without preoperative treatment of radiotherapy and
chemotherapy; iii) patients with all limbs and normal cognitive
function; iv) patients with complete medical records; and v)
patients and their families who were cooperative in treatment.
Patients who met the following criteria were excluded from the
study: i) Patients with immunodeficiency; ii) patients with
congenital heart disease; iii) patients with other malignant
tumors; iv) patients with serious dysfunction of key organs; and v)
patients not willing to be followed up.
Reagents and instruments
The following reagents and instruments were
purchased: i) TRIzol RNA extraction reagent from Thermo Fisher
Scientific, Inc. (Shanghai, China, A33251); ii) RT-PCR kit for
PrimeScript™ and PrimeScript™ II 1st Strand cDNA Synthesis kit from
Takara Biomedical Technology (Beijing) Co., Ltd. [Beijing, China
(6210A, RR055B)]; and iii) PCR Amplifier ABI7900 from Applied
Biosystems; Thermo Fisher Scientific, Inc. (Waltham, MA, USA). The
miRNA-146b-5p primers were designed and synthesized by Shanghai
Sangon Biotech Co., Ltd. (Shanghai, China). The primer sequences
are shown in Table I.
 | Table I.Primer sequences. |
Table I.
Primer sequences.
| Genes | Upstream primers | Downstream
primers |
|---|
| miRNA-146b-5p |
5′-GCGTGAGAACTGAATTCCA-3′ |
5′-GTGCAGGGTCCGAGGTAT-3′ |
| U6 |
5′-GCGCGTCGTGAAGCGTTC-3′ |
5′-GTGCAGGGTCCGAGGT-3′ |
Reverse transcription-quantitative
polymerase chain reaction (RT-qPCR)
Total RNA reverse transcription was performed in
strict accordance with the PrimeScript™ II 1st Strand cDNA
Synthesis kit instructions. The system was: 2 µl 5X buffer, 0.5 µl
RT Enzyme Mix, 0.5 µl Oligo (dT) primer, 2 µl Random 6 mers, 1 µg
total RNA, and RNase free H2O to 10 µl. The reaction
conditions were: 37°C for 15 min and then 85°C for 5 min. After the
reverse transcription, cDNA was collected. The SYBR Green PCR
reaction system was: (Thermo Fisher Scientific, Inc.): PrimeScript
1 Step Enzyme Mix 1 µl, upstream and downstream primers 0.5 µl
each, 2X 1 step buffer 12.5 µl, and cDNA 1 µl. Finally, cDNA RNase
Free dH2O was used to add up to 25 µl. The PCR reaction
conditions were: 50°C for 30 min, 94°C degeneration for 2 min, 98°C
degeneration for 10 sec, and 68°C for 1 min. Thirty circles were
performed, and U6 was used as the internal reference. The data were
analyzed using the 2−∆∆Cq method (13). The experiment was carried out three
times. The median relative expression of miRNA-146b-5p in patient
tissues was selected and divided into the high expression and low
expression groups.
Follow-up
The patients were followed up for 60 months after
discharge. The recurrence of cancer was tracked by follow-up phone
calls at 1, 3, 6, 12, 24, 36, 48 and 60 months.
Statistical analysis
The SPSS 20.0 statistics software package (IBM
Corp., Armonk, NY, USA) was used for statistical analysis on the
collected data. The GraphPad Prism 7 software was used for figure
drawing. Enumeration data were expressed in rate (%) and compared
using the Chi-square test. Measurement data were expressed in a
mean ± standard deviation (mean ± SD). Independent t-test was used
for inter-group comparison, represented by t. Single-factor ANOVA
was used for multi-group comparison, and LSD t-test was used for
pairwise comparison. P<0.05 was considered to indicate a
statistically significant difference.
Results
Relative expression levels of
miRNA-146b-5p in patient cancer tissues
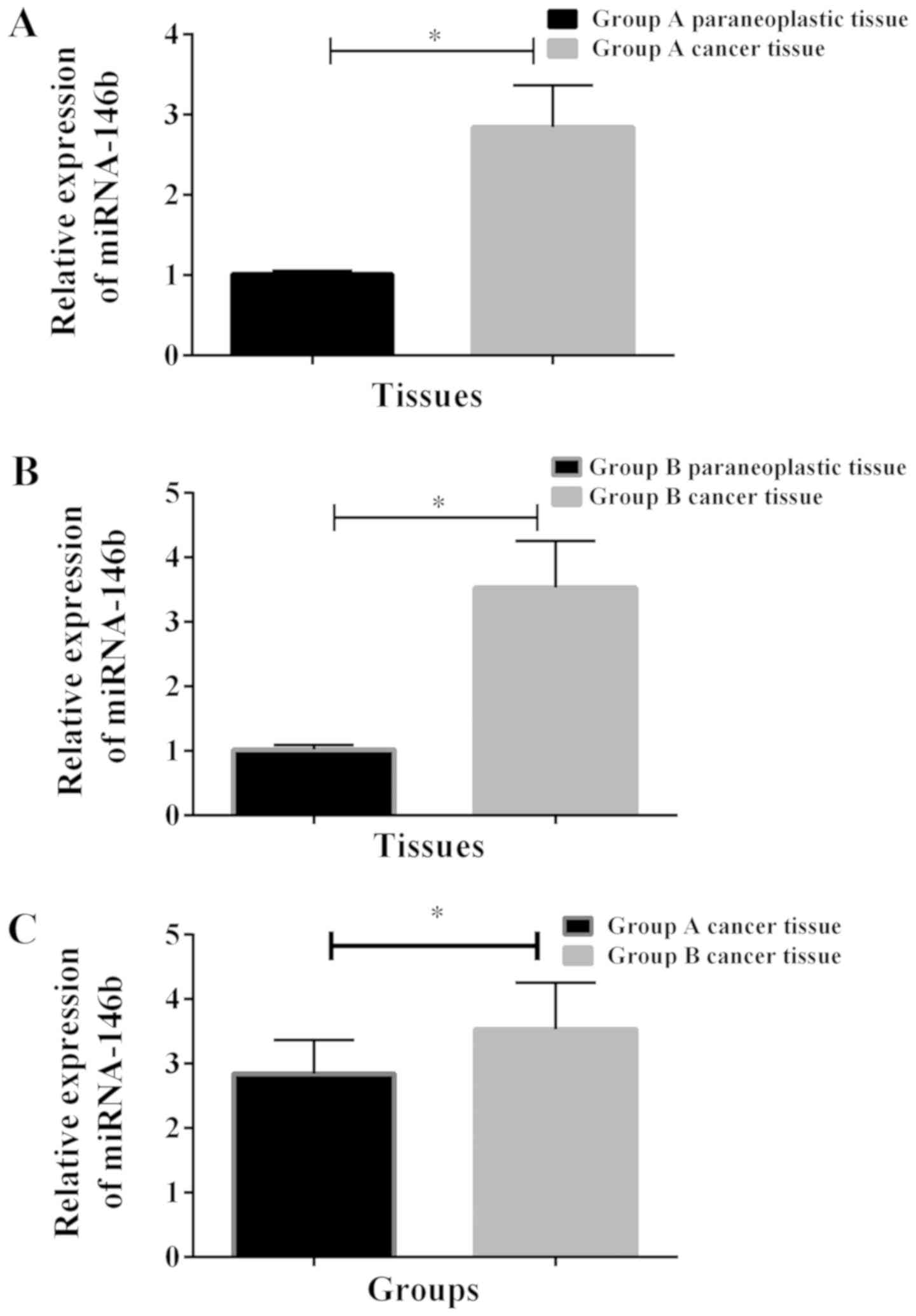
After the detection of miRNA-146b-5p, no significant
difference was found in the expression of miRNA-146b-5p in patient
cancer tissues among the three groups (P<0.05). The
miRNA-146b-5p expression in patient cancer tissues in group B was
significantly higher than those in groups A and C. The
miRNA-146b-5p expression in patient cancer tissues in group A was
significantly higher than that in group C (P<0.05). The
miRNA-146b-5p expression levels in patient cancer tissues in the
three groups were higher than those in para-carcinoma tissues
(P<0.05) (Table II and Fig. 1).
| Table II.Relative expression levels of
miRNA-146b-5p in patient cancer tissues. |
Table II.
Relative expression levels of
miRNA-146b-5p in patient cancer tissues.
|
| Pattern of
organization |
|
|
|---|
|
|
|
|
|
|---|
| Groups | Lesion tissue | Perifocal tissue | t value | P-value |
|---|
| Group A (n=37) | 1.864±0.235 | 1.005±0.022 | 22.138 | <0.001 |
| Group B (n=50) |
2.532±0.422a | 1.009±0.038 | 25.417 | <0.001 |
| Group C (n=40) |
1.384±0.102a,b | 1.002±0.020 | 23.243 | <0.001 |
| F value | 166.929 | 0.663 |
|
|
| P-value | <0.001 | 0.517 |
|
|
Expression of miRNA-146b-5p in
patients with different pathological tissue types
According to the pathological tissue types, 87
patients were divided into the papillary carcinoma group, the
follicular carcinoma group and the medullary carcinoma group. We
found that there was no significant difference in the miRNA-146b-5p
expression in all three groups (P>0.05). (Table III).
| Table III.Relative expression of miRNA-146b-5p
in patients with different histological types. |
Table III.
Relative expression of miRNA-146b-5p
in patients with different histological types.
| Group | Papillary carcinoma
group (n=70) | Follicular carcinoma
group (n=12) | Medullary carcinoma
group (n=5) | F value | P-value |
|---|
| Relative expression
of miRNA-146b-5p | 2.254±0.434 | 2.362±0.634 | 2.358±0.367 | 0.365 | 0.695 |
Association of relative expression
levels of miRNA-146b-5p with clinical records in group B
The patients in group B were further separated into
two subgroups based on the median miRNA-146b-5p relative expression
level: group B high expression subgroup and group B low expression
subgroup. There were 22 patients in group B high expression
subgroup, and 28 patients in group B low expression subgroup. The
miRNA-146b-5p expression level was found to be associated with
tumor size, lymph node metastasis and TNM stage (P<0.05), while
not associated with sex, age, lesion multiplicity, smoking history,
diabetes history and pathological type in group B (P>0.05)
(Table IV).
| Table IV.Association of relative expression
levels of miRNA-146b-5p with clinical records in group B (n=50) [n
(%)]. |
Table IV.
Association of relative expression
levels of miRNA-146b-5p with clinical records in group B (n=50) [n
(%)].
|
|
| Group B subgroup |
|
|
|---|
|
|
|
|
|
|
|---|
| Variables | Case (%) | Low expression
(n=28) | High expression
(n=22) | χ2
value | P-value |
|---|
| Sex |
|
|
| 0.990 | 0.319 |
| Male | 15 (30.00) | 10 (35.71) | 5
(22.73) |
|
|
|
Female | 35 (70.00) | 18 (64.29) | 17 (77.27) |
|
|
| Age, years |
|
|
| 0.325 | 0.569 |
|
>45 | 25 (50.00) | 15 (53.57) | 10 (45.45) |
|
|
|
≤45 | 25 (50.00) | 13 (46.43) | 12 (54.55) |
|
|
| Tumor size |
|
|
| 5.864 | 0.015 |
| ≥1
cm | 40 (80.00) | 19 (67.86) | 21 (95.45) |
|
|
| <1
cm | 10 (20.00) | 9
(32.14) | 1 (4.55) |
|
|
| Lesion
multiplicity |
|
|
| 0.487 | 0.485 |
|
Single | 20 (40.00) | 10 (35.71) | 10 (45.45) |
|
|
|
Multiple | 30 (60.00) | 18 (64.29) | 12 (54.55) |
|
|
| Lymph node
metastasis |
|
|
| 4.818 | 0.028 |
|
Yes | 41 (82.00) | 20 (71.43) | 21 (95.45) |
|
|
| No | 9
(18.00) | 8
(28.57) | 1 (4.55) |
|
|
| TNM stage |
|
|
| 5.009 | 0.025 |
| Stage
I–II | 35 (70.00) | 16 (57.14) | 19 (86.36) |
|
|
| Stage
III–VI | 15 (30.00) | 12 (42.86) | 3
(13.64) |
|
|
| Smoking
history |
|
|
| 0.139 | 0.709 |
|
Yes | 15 (30.00) | 9
(32.14) | 6
(27.27) |
|
|
| No | 35 (70.00) | 19 (67.86) | 16 (72.73) |
|
|
| Diabetes
history |
|
|
| 0.033 | 0.856 |
|
Yes | 13 (26.00) | 7
(25.00) | 6
(27.27) |
|
|
| No | 37 (74.00) | 21 (75.00) | 16 (72.73) |
|
|
| Pathological
type |
|
|
| 3.449 | 0.178 |
|
Papillary carcinoma | 40 (80.00) | 25 (89.29) | 15 (68.18) |
|
|
|
Follicular carcinoma | 7
(14.00) | 2 (7.14) | 5
(22.73) |
|
|
|
Medullary carcinoma | 3 (6.00) | 1 (3.57) | 2 (9.09) |
|
|
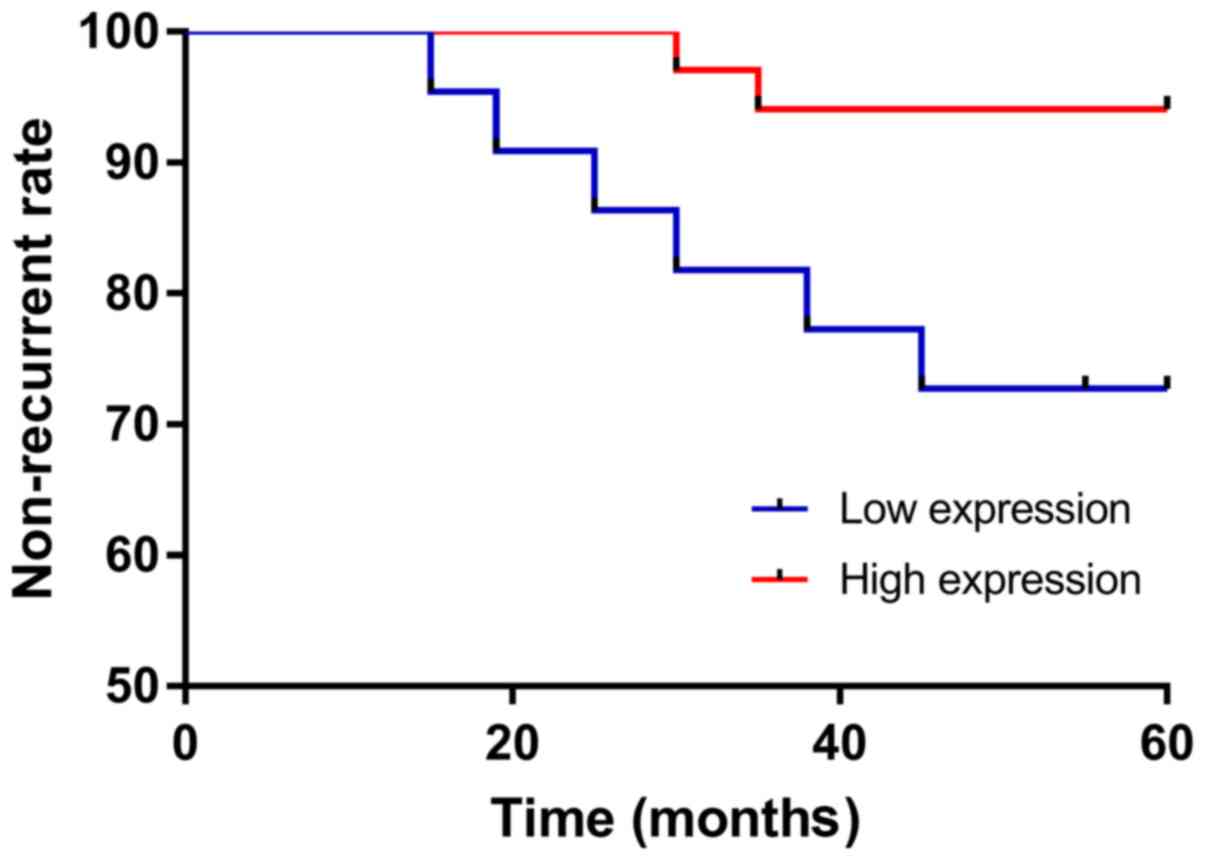
Recurrence rate of group B
Patients in group B were followed up for 5 years.
The 5-year non-recurrence rate of group B high expression subgroup
was lower than that of group B low expression subgroup (P<0.05).
The results are shown in (Table V
and Fig. 2).
| Table V.Group B patients' 1-, 3- and 5-year
non-recurrence rates (%). |
Table V.
Group B patients' 1-, 3- and 5-year
non-recurrence rates (%).
| Group B
subgroup | 1-year | 3-year | 5-year |
|---|
| High expression
(n=22) | 100.00 | 81.81 | 68.18 |
| Low expression
(n=28) | 100.00 | 92.86 | 92.86 |
| χ2
value | 0 | 1.422 | 5.082 |
| P-value | >0.999 | 0.233 | 0.024 |
Discussion
HT, also known as chronic lymphocytic thyroiditis,
is a human autoimmune disease. Under the microscope, diffuse
lymphocytic infiltration and fibrosis, as well as lymphoid
follicles, are identifiable (14).
In clinic, symmetrical and diffuse enlargement of the thyroid gland
at both sides is typical of HT. Most patients slowly develop
hypothyroidism as the patients' disease course progresses. When
this destruction goes on long enough, permanent hypothyroidism can
be caused, posing a serious threat to patients' health and quality
of life (1). In addition, a variety
of other conditions may develop on the basis of primary HT, of
which TC is the most serious one. Among the pathological types of
combined TC, thyroid papillary carcinoma is the most common
(15).
In clinic, TC is the most common malignancy of the
endocrine system, impacting individuals' life, though its incidence
is lower than many other tumors (16). According to the pathological
classification, TC can be divided into four types: papillary
carcinoma, follicular carcinoma, undifferentiated carcinoma and
medullary carcinoma. Among them, papillary carcinoma accounts for
80–85% of the total incidence of TC (17). The distribution of pathological types
in current study is basically similar to this general distribution.
Although the 35- or 40-year survival rate of TC can reach 80% or
even higher with timely treatment (18), there are currently no effective means
of preventing TC.
Recent technological advances in molecular biology
have allowed a deeper understanding of the mechanisms underlying TC
onset and progression. miRNAs as a new type of molecules are
gradually gaining widespread interest. miRNAs are a type of
endogenous short non-coding single-stranded RNA molecules, which
are highly chronological, conserved and specific (19). It was reported that miRNAs are
involved in disease onset and progression by specific binding to
the target gene of interest, for example, miRNAs play an important
role in cell proliferation, apoptosis and growth in tumor onset and
progression processes (20).
miRNA-146b-5p belongs to the miRNA-146 family and is a newly
discovered immune regulatory factor. It is associated with the
onset and progression of autoimmune diseases. For example,
miRNA-146 may play a role in persistent inflammation in rheumatoid
arthritis through a T cell network (21). According to literature, miRNA-146b-5p
can suppress TC cell invasion by regulating its target gene IRAK1
(22). However, it is unclear if
miRNA-146b-5p is associated with TC complicated by HT. In this
study, the tissue expression levels of miRNA-146b-5p in patients
with TC in combination with HT were evaluated, and possible
association between miRNA-146b-5p and the disease was analyzed, in
order to provide a reference for clinical practice.
In this study, the expression levels of
miRNA-146b-5p in cancer tissues, as well as paracancerous tissues,
of patients with TC (group A), patients with combined TC and HT
(group B) and patients with HT (group C) were evaluated. It was
found that in the three groups, the expression levels of
miRNA-146b-5p in cancer tissues were higher than those in
corresponding paracancerous tissues. The expression level of
miRNA-146b-5p in cancer tissues was higher in group B than those in
groups A and C, and the differences were statistically significant.
The expression level of miRNA-146b-5p in cancer tissues was higher
in group A than that in group C, and the differences were
statistically significant. The above findings were consistent with
previous studies. For example, the tissue expression of
miRNA-146b-5p in patients with papillary thyroid carcinoma was
higher than that in healthy subjects (23), and the miRNA-146b-5p expression in
cancer tissues of patients with papillary thyroid carcinoma was
also higher than that in corresponding paracancerous tissues
(24). Moreover, higher tissue
expression of miRNA-146b-5p in combined TC and HT than in TC only
suggested that miRNA-146b-5p expression was associated with HT. In
the study of Taganov et al (25), miRNA-146b-5p is a natural immune
protein inhibitor, while TC, an autoimmune disease, is
significantly higher than that in the lesion tissue of HT patients,
suggesting that the expression of miRNA-146b-5p is associated with
the occurrence and development of HT. The possible reason of higher
expression of miRNA-146b-5p in patients with combined TC and HT was
that the miRNA-146b-5p expression was increased in TC with HT
patients under the influence of the dual factors of cancer lesions
and immune inflammatory response. We also analyzed the expression
of miRNA-146b-5p in tissues of patients with different pathological
types and found no significant difference in miRNA-146b-5p
expression in tissues of patients with papillary carcinoma group,
follicular carcinoma group and medullary carcinoma group, but the
small number of sample size may affect the results. The statistical
analysis of the clinical records of patients in group B high
expression subgroup and group B low expression subgroup found that
miRNA-146b-5p expression was associated with tumor size, lymph node
metastasis and TNM stage. At the end of this study, we conducted a
5-year statistical analysis on the recurrence of patients with high
and low expression in group B and found that the recurrence rate of
patients with high expression was higher than that of patients with
low expression. In a recent study, the miRNA-146b-5p expression was
found to be associated with TC tumor size and lymph node
metastasis, suggesting that miRNA-146b-5p could be used as a
potential prognostic indicator for combined TC and HT (26). However, in the study of Lee et
al (26), compared to PTC
patients without HT, patients with HT had favorable
clinicopathologic features by a meta-analysis, which is
inconsistent with our study. It may be due to the small sample size
in this study. Besides, only 2,471 PTC patients of the 10,648 cases
were combined with HT, accounting for 23.2%, while in this study,
57.47% PTC patients had HT. The significant difference between the
two studies may be caused by the exclusion criteria in this
study.
It is undeniable that there are certain limitations
in this study. Both the sample size and the group numbers were
small. In addition, the expression level of miRNA-146b-5p in
patients with HT only was unclear, and it was unclear as to which
target gene played a role in combined TC and HT.
Collectively, miRNA-146b-5p was overexpressed in
tissues of patients with combined TC and HT. It was associated with
tumor size, lymph node metastasis, and TNM staging. miRNA-146b
shows potential as a prognostic indicator for combined TC and
HT.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
NL and XL conceived the study and drafted the
manuscript. LH, RZ and JY acquired the data. GZ and LL analyzed the
data and revised the manuscript. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
The study was approved by the Medical Ethics
Committee of The Third Affiliated Hospital of Southern Medical
University, (Guangzhou, China). The patients and their families
were informed and signed an informed consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Torimoto K, Okada Y, Nakayamada S, Kubo S
and Tanaka Y: Anti-PD-1 antibody therapy induces Hashimoto's
disease with an increase in peripheral blood follicular helper T
cells. Thyroid. 27:1335–1336. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Zaletel K and Gaberšček S: Hashimoto's
thyroiditis: From genes to the disease. Curr Genomics. 12:576–588.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Sendt W, Rippe V, Flor I, Drieschner N and
Bullerdiek J: Monosomy and ring chromosome 13 in a thyroid nodular
goiter - do we underestimate its relevance in benign thyroid
lesions? Cancer Genet. 205:128–130. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Song E, Jeon MJ, Park S, Kim M, Oh HS,
Song DE, Kim WG, Kim WB, Shong YK and Kim TY: Influence of
coexistent Hashimoto's thyroiditis on the extent of cervical lymph
node dissection and prognosis in papillary thyroid carcinoma. Clin
Endocrinol (Oxf). 88:123–128. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wells SA Jr, Asa SL, Dralle H, Elisei R,
Evans DB, Gagel RF, Lee N, Machens A, Moley JF, Pacini F, et al:
American Thyroid Association Guidelines Task Force on Medullary
Thyroid Carcinoma: Revised American Thyroid Association guidelines
for the management of medullary thyroid carcinoma. Thyroid.
25:567–610. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
La Vecchia C, Malvezzi M, Bosetti C,
Garavello W, Bertuccio P, Levi F and Negri E: Thyroid cancer
mortality and incidence: A global overview. Int J Cancer.
136:2187–2195. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhao J, Xu C, Yao J, Yu C, Liao L and Dong
J: Statins and thyroid carcinoma: A meta-analysis. Cell Physiol
Biochem. 47:1422–1431. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fallahi P, Ferrari SM, Camastra S, Politti
U, Ruffilli I, Vita R, Navarra G, Benvenga S and Antonelli A: TSH
normalization in bariatric surgery patients after the switch from
L-thyroxine in tablet to an oral liquid formulation. Obes Surg.
27:78–82. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Wu ZG, Yan XQ, Su RS, Ma ZS, Xie BJ and
Cao FL: How many contralateral carcinomas in patients with
unilateral papillary thyroid microcarcinoma are preoperatively
misdiagnosed as benign? World J Surg. 41:129–135. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Trzybulska D, Bobjer J, Giwercman A and
Tsatsanis C: Serum microRNAs in male subfertility-biomarkers and a
potential pathogenetic link to metabolic syndrome. J Assist Reprod
Genet. 34:1277–1282. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kasinski AL, Kelnar K, Stahlhut C,
Orellana E, Zhao J, Shimer E, Dysart S, Chen X, Bader AG and Slack
FJ: A combinatorial microRNA therapeutics approach to suppressing
non-small cell lung cancer. Oncogene. 34:3547–3555. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lima CR, Geraldo MV, Fuziwara CS, Kimura
ET and Santos MF: MiRNA-146b-5p upregulates migration and invasion
of different papillary thyroid carcinoma cells. BMC Cancer.
16:1082016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(−Delta Delta C(T)) Method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kagawa T, Watanabe M, Inoue N, Otsu H,
Saeki M, Katsumata Y, Takuse Y and Iwatani Y: Increases of microRNA
let-7e in peripheral blood mononuclear cells in Hashimoto's
disease. Endocr J. 63:375–380. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Girardi FM, Barra MB and Zettler CG:
Papillary thyroid carcinoma: Does the association with Hashimoto's
thyroiditis affect the clinicopathological characteristics of the
disease? Braz J Otorhinolaryngol. 81:283–287. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lang BH, Shek TW, Chan AO, Lo CY and Wan
KY: Significance of size of persistent/recurrent central nodal
disease on surgical morbidity and response to therapy in
reoperative neck dissection for papillary thyroid carcinoma.
Thyroid. 27:67–73. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lu Z, Zhang Y, Feng D, Sheng J, Yang W and
Liu B: Targeted next generation sequencing identifies somatic
mutations and gene fusions in papillary thyroid carcinoma.
Oncotarget. 8:45784–45792. 2017.PubMed/NCBI
|
|
18
|
Hay ID, Johnson TR, Thompson GB, Sebo TJ
and Reinalda MS: Minimal extrathyroid extension in papillary
thyroid carcinoma does not result in increased rates of either
cause-specific mortality or postoperative tumor recurrence.
Surgery. 159:11–19. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Schwarzenbach H, Nishida N, Calin GA and
Pantel K: Clinical relevance of circulating cell-free microRNAs in
cancer. Nat Rev Clin Oncol. 11:145–156. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hill M and Tran N: MicroRNAs regulating
microRNAs in cancer. Trends Cancer. 4:465–468. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Nakasa T, Miyaki S, Okubo A, Hashimoto M,
Nishida K, Ochi M and Asahara H: Expression of microRNA-146 in
rheumatoid arthritis synovial tissue. Arthritis Rheum.
58:1284–1292. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Chou CK, Chi SY, Huang CH, Chou FF, Huang
CC, Liu RT and Kang HY: IRAK1, a target of miR-146b, reduces cell
aggressiveness of human papillary thyroid carcinoma. J Clin
Endocrinol Metab. 101:4357–4366. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chou CK, Yang KD, Chou FF, Huang CC, Lan
YW, Lee YF, Kang HY and Liu RT: Prognostic implications of miR-146b
expression and its functional role in papillary thyroid carcinoma.
J Clin Endocrinol Metab. 98:E196–E205. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Sun M, Fang S, Li W, Li C, Wang L, Wang F
and Wang Y: Associations of miR-146a and miR-146b expression and
clinical characteristics in papillary thyroid carcinoma. Cancer
Biomark. 15:33–40. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Taganov KD, Boldin MP, Chang KJ and
Baltimore D: NF-kappaB-dependent induction of microRNA miR-146, an
inhibitor targeted to signaling proteins of innate immune
responses. Proc Natl Acad Sci USA. 103:12481–12486. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lee YS, Lim YS, Lee JC, Wang SG, Park HY,
Kim SY and Lee BJ: Differential expression levels of plasma-derived
miR-146b and miR-155 in papillary thyroid cancer. Oral Oncol.
51:77–83. 2015. View Article : Google Scholar : PubMed/NCBI
|