Colorectal cancer (CRC) is the third most commonly
diagnosed cancer in males and the second in females, and it is one
of the most common causes of cancer mortality (1). Localized CRCs are amenable to curative
surgical resection, however, ~25% of patients present with
metastatic disease and ~50% of patients will develop metastases
(2). Fluorouracil-based chemotherapy
remains the primary treatment for metastatic CRC (3). 5-fluorouracil (5-FU) alone has an
objective response rate of ~20% (4).
The addition of irinotecan or oxaliplatin to 5-FU increases the
objective response rate to ~50% (5).
The effects of 5-FU/leucovorin combined with irinotecan (FOLFIRI)
or oxaliplatin (FOLFOX) in the first-line treatment of metastatic
CRC are comparable (6). In the last
decade, the addition of targeted therapies based on these
chemotherapy regimens has improved the therapeutic approach and
significantly increased progression-free survival and overall
survival times (7–9). Fluorouracil-based chemotherapy remains
the primary treatment for metastatic CRC. However, ~50% of patients
are resistant to fluorouracil-based chemotherapy. In addition, the
side effects of systemic chemotherapy, including neurotoxicity,
myelotoxicity and gastrointestinal toxicity, may have a major
impact on the quality of life of the patients and may lead to
life-threatening complications (3).
Therefore, identifying effective strategies that predict response
to chemotherapy are required. Using these strategies, patients that
are predicted to not respond to chemotherapy may receive other
potentially effective treatments as early as possible and avoid
unnecessary side effects. Gene expression profiling is used to
predict the clinical outcome of patients with CRC (10–12).
Previous studies have revealed that gene expression profiling may
be used to predict cancer response to chemotherapy, including
breast cancer and CRC (13–15).
The aim of the present study was to develop a
predictor classifier for response to fluorouracil-based
chemotherapy in patients with advanced CRC using microarray gene
expression profiles of primary CRC tissues.
The expression values of DEGs in each sample were
extracted. The LASSO logistic regression model analysis was
performed using the ‘glmnet’ package (CRAN.R-project.org/package=glmnet; version 2.0-16) in
R. The LASSO method is used to select optimal features in
high-dimensional microarray data with a powerful predictive value
and a low correlation between each other to prevent over-fitting
(28). In the training set, the LASSO logistic regression model was
used to select the optimal predictive markers. PCA using the
expression profiles of the DEGs was performed prior to feature
selection using the LASSO method. PCA was subsequently performed
using the expression profiles of the optimal DEGs identified using
by the LASSO method. Samples were plotted in two-dimensional plots
across the first two principal components.
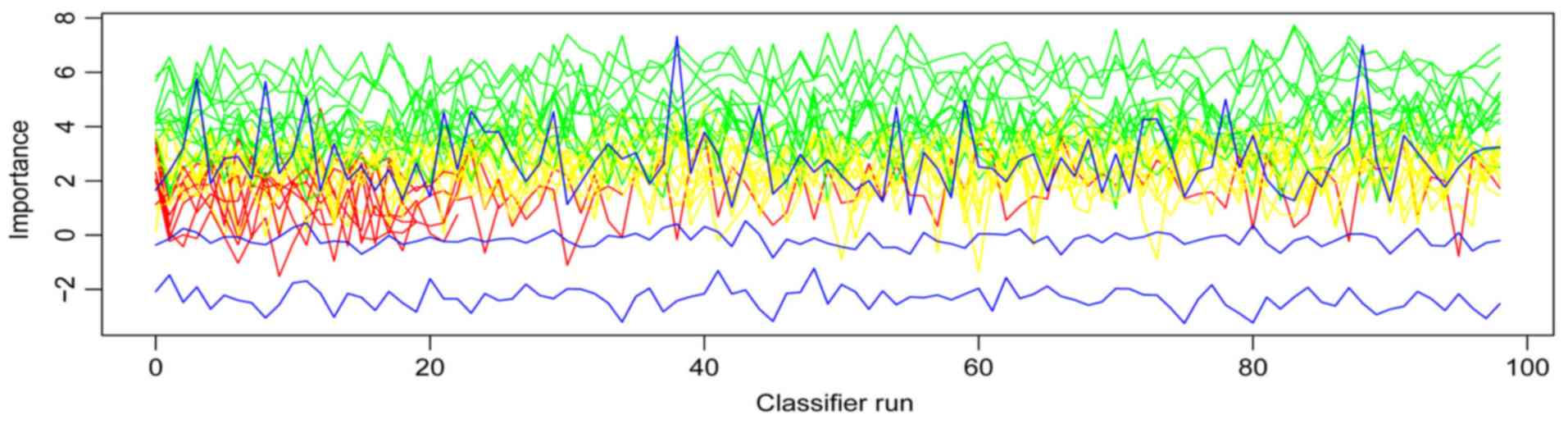
A lower-dimensional model may reduce costs and is
more likely to be used by clinicians (29). Following DEGs selection
by the LASSO method, a feature selection was performed using the
‘Boruta’ package (www.jstatsoft.org/article/view/v036i11; version 6.0.0)
in R. Boruta is a random forest-based feature selection method,
which provides an unbiased and stable selection of important and
non-important attributes from an information system. A variable
importance (VIMP) measure may be calculated and visualized based on
Boruta. In the current study, DEGs selected by Boruta were used to
develop a gene-based classifier for response to fluorouracil-based
chemotherapy in advanced CRCs. The random forest classifier was
developed using the ‘randomForest’ package (CRAN.R-project.org/package=randomForest; version
4.6-14) in R. The validation set (GSE69657) was used to confirm the
robustness and transferability of the classifier. The performance
of the classifier was assessed by accuracy, sensitivity (Se),
specificity (Sp), positive predictive value (PPV), negative
predictive value (NPV) and receiver operating characteristic (ROC)
curves in the training and validation sets. The ROC curves were
drawn and compared using the ‘pROC’ (version 1.13.0) package
(30) in R.
The training set included 32 responders and 26
non-responders. According to the cut-off criteria
(|log2FC|≥0.263 and P<0.05), 791 genes were
identified as differentially expressed between responders and
non-responders. A total of 303 genes were upregulated and 488 genes
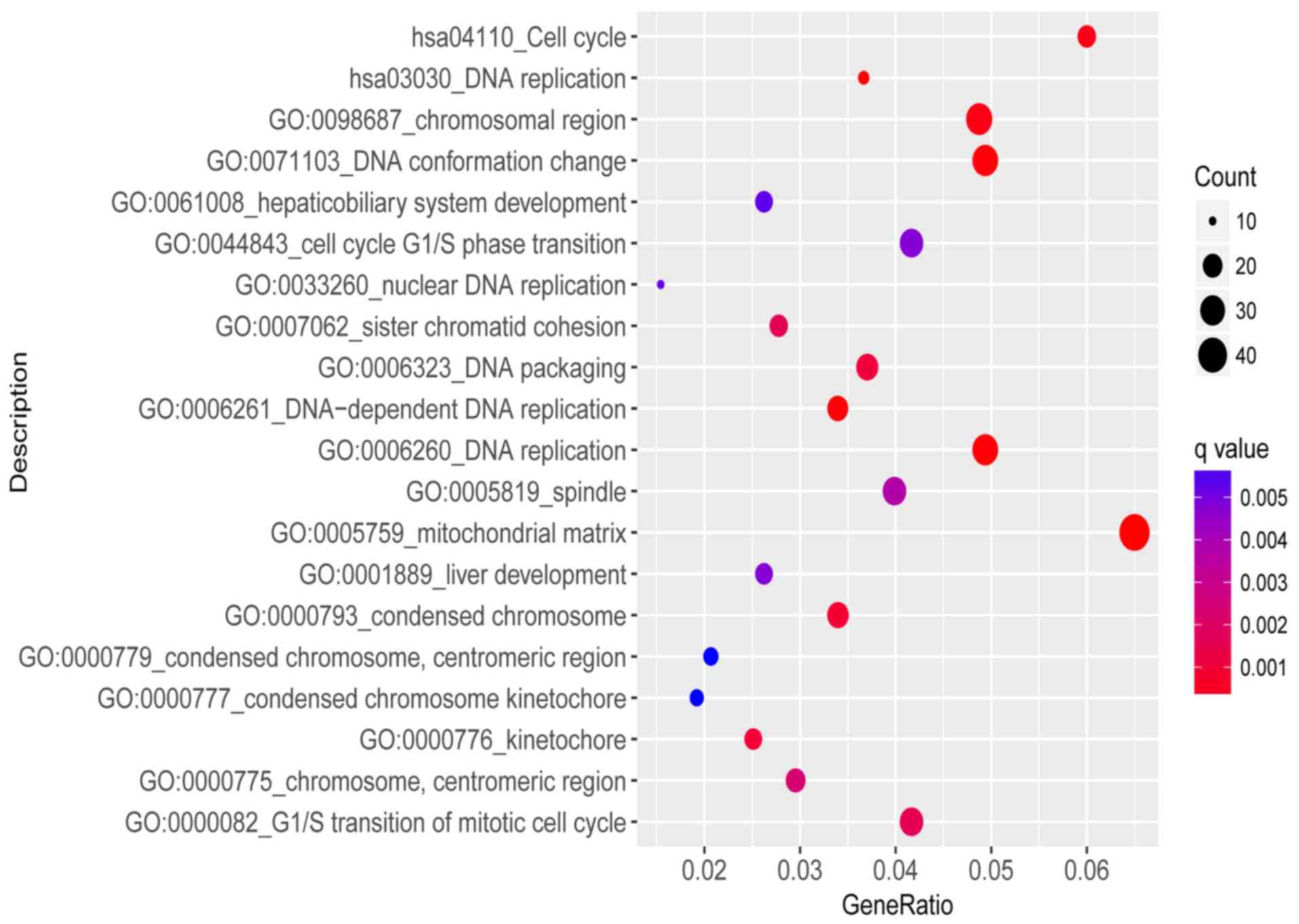
were downregulated in responders. Functional enrichment analysis
revealed that the biological process of DEGs were primarily
involved in ‘cell mitosis’, ‘DNA replication’ and ‘cell cycle’
signaling pathways. The results of enrichment analysis are
presented in Fig. 1.
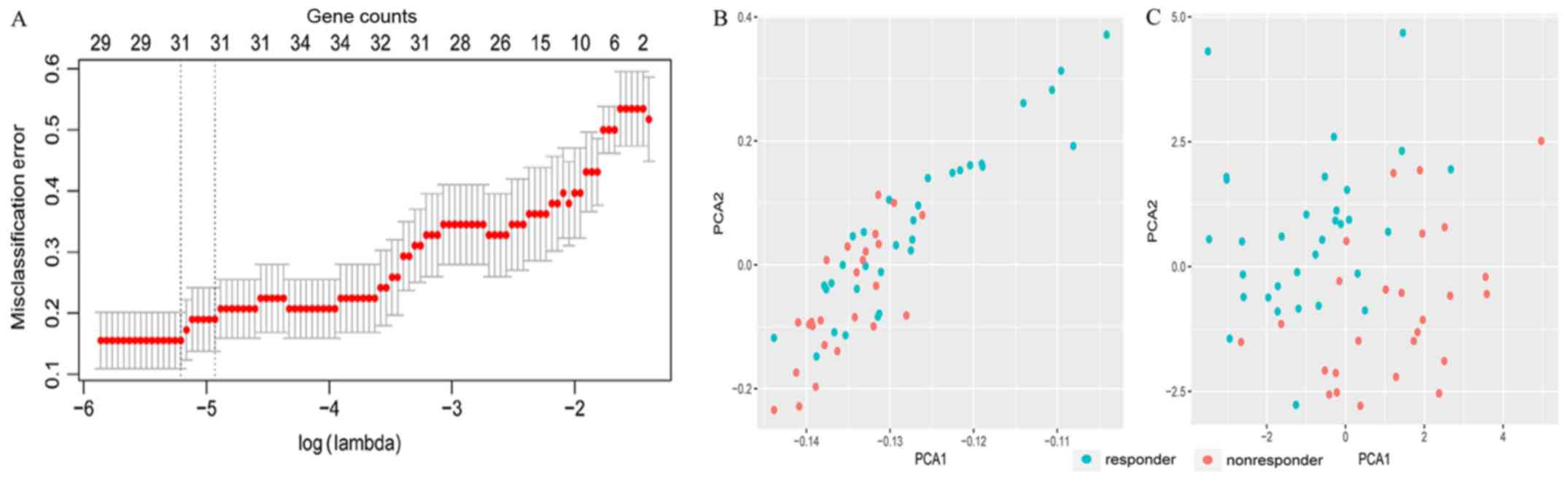
For the first feature selection, LASSO logistic
regression was performed using the expression data of DEGs in the
training set. The group-wise classifications in 10-fold
cross-validations were computed as default. A total of 31 DEGs were
identified as optimal genes (Fig.
2A) with non-zero regression coefficients (Table I). Fig.
2B presents the results of PCA prior to feature selection using
LASSO and Fig. 2C presents the
results of PCA following feature selection using LASSO. As
demonstrated in Fig. 2C, responders
and non-responders are easily distinguished using the 31 DEGs
selected by LASSO.
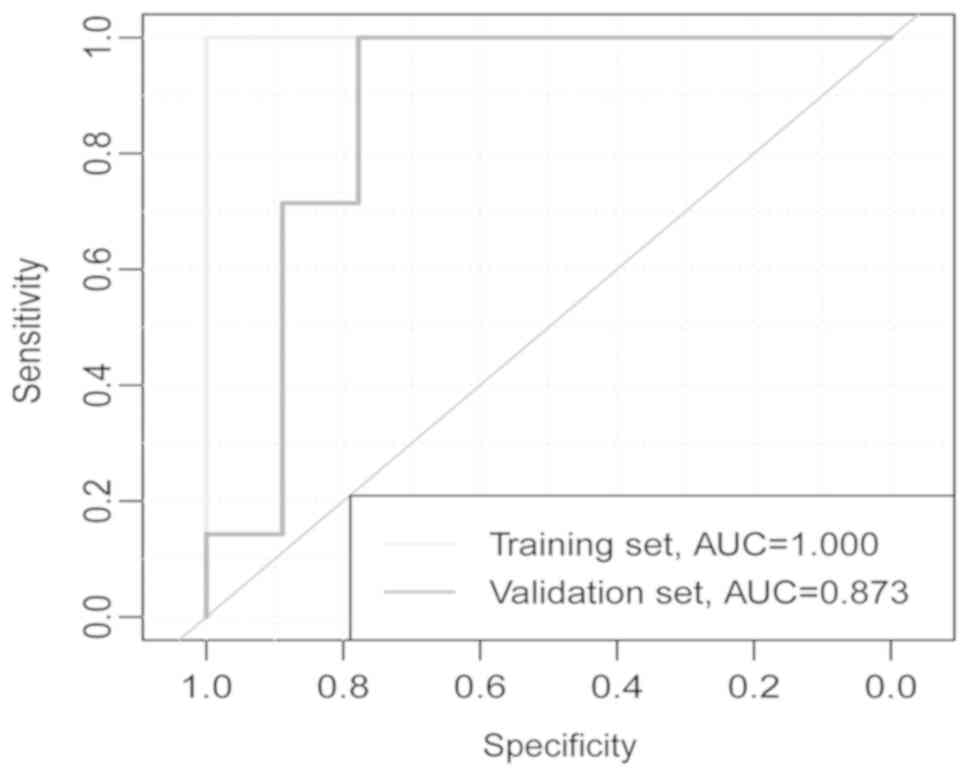
The accuracy of the 13-gene classifier was 0.930 in
the training set and 0.810 in the validation set. Based on
accuracy, Se, Sp, PPV, NPV and area under curve (AUC) values, the
sample recognition efficiency of the classifier was high (Table II). ROC curve analysis revealed that
the AUC was 1.000 in the training set and 0.873 in the validation
set (P=0.227; Fig. 4).
Personalized treatment may improve the treatment
outcome of patients with tumors (31). In CRC, the gene expression levels of
vascular endothelial growth factor (VEGF) and epidermal growth
factor receptor (EGFR) provide the basis for selecting EGFR and
VEGF inhibitor combinations (32–36).
Monoclonal antibodies against VEGF and EGFR have been approved for
treatment of metastatic CRC in combination with 5-FU-based regimens
(3). The identification of subsets
of patients that respond to specific chemotherapy regimens remains
a challenge (3). A previous study
demonstrated that tumors with microsatellite instability (MSI)
respond well to 5-FU-based therapies; however, further studies are
required to substantiate these results (37). Another previously published study
suggested that MSI status does not affect the outcome of the
treatment (38). Therefore,
effective tools for predicting the outcome of chemotherapy are
currently lacking. The present study identified 13 genes from 791
DEGs using two feature selection algorithms and developed a 13-gene
predictor classifier for response to fluorouracil-based
chemotherapy in CRC. The predictor classifier demonstrated high
accuracy in the training and validation sets. The training set
included two datasets from different centers, and the validation
set was from an additional independent center. ROC curve analysis
revealed that the AUC was 1.000 in the training set and 0.873 in
the validation set, and their difference was not significant
(P=0.227). These results suggested that the classifier was robust.
The study established a foundation for further research into
personalized treatment of CRC.
Previous studies have attempted to identify a single
biomarker to predict response to fluorouracil-based chemotherapy in
CRC (17,39–42).
However, there is currently no single biomarker that is routinely
applied in clinical practice. CRC is a heterogeneous disease, which
is compounded by changes in the molecular profile of the tumor as
it progresses (3). An in
vitro study demonstrated that the measurement of multiple,
rather than single marker genes, may provide a more accurate
assessment of drug response in colon carcinoma (43). Previous studies have been designed to
identify a pattern of gene expression capable of predicting
response to fluorouracil-based chemotherapy in CRC (15,16). One
study identified a set of 14 genes for predicting response to the
FOLFIRI regimen based on 21 samples (15), and an expression profile of 7 genes
was identified in another study (16). Compared with the two aforementioned
studies, the current study performed a comprehensive analysis of
more samples (n=58) from two centers and validated the predictor
classifier in an independent dataset (n=16). Furthermore, to the
best of the authors' knowledge, the current study is the first to
construct a random forest classifier to predict response to
chemotherapy in CRC. Considering the limited ability of Cox
regression analysis to process high-dimensional data (44), it was not performed in the current
study. A random forest algorithm was used to construct the
classifier, which was subsequently validated with an independent
dataset. The results obtained in the current study suggest that the
robust classifier developed warrants further investigation.
Functional enrichment analysis revealed that certain
DEGs identified in the present study are involved in DNA
replication and cell cycle pathways; however, none of the 13 genes
were involved in these two signaling pathways. A previous study
suggested that PHLDA1 may be associated with CRC progression
(45). A previous study demonstrated
that PTGR2-knockdown gastric cancer cells rendered them more
sensitive to cisplatin and 5-FU compared with the
PTGR2-overexpressing cells (46). In
addition, two variants of CHIT1, rs61745299 and rs35920428, may
increase expression of the gene and have been associated with CRC
(47). CHRNB1 may be a biomarker for
the detection of relapsed and early relapsed CRC (48). In addition, LIG4 may mediate Wnt
signaling-induced radioresistance in CRC (49). With the exception of the
aforementioned studies, the association between the 13 genes
identified in the current study and CRC or chemotherapy has not
been investigated. Therefore, it is not clear whether these genes
are causal or merely markers for response to fluorouracil-based
chemotherapy in CRC.
Although the current study provides novel insights
into the treatment of CRC, it has some limitations. The present
study was based on a relatively small sample size; however, it is
worth noting that the sample size in our study is relatively large
compared with previous studies (15,16).
Future studies are required to verify and improve the 13-gene
signature in a larger independent cohort of patients.
In conclusion, the current study identified a
13-gene predictor classifier for the response to fluorouracil-based
chemotherapy in patients with advanced CRC.
Not applicable.
This research was supported by the Youth Science
Foundation of Guangxi Medical University (grant no. GXMUYSF 201716)
and the Basic Ability Enhancement Program for Young and Middle-aged
Teachers of Guangxi (grant no. 2017KY0120).
All data generated or analyzed during the present
study are included in this published article.
YFL designed the study and revised the manuscript.
ZHG and QYZ analyzed the data and wrote the manuscript. YL, ZHX,
ZH, and ZCC assisted with analyzing the data and writing the
manuscript. All authors read and approved the final manuscript.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Torre LA, Bray F, Siegel RL, Ferlay J,
Lortet-Tieulent J and Jemal A: Global cancer statistics, 2012. CA
Cancer J Clin. 65:87–108. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Van Cutsem E, Cervantes A, Nordlinger B
and Arnold D; ESMO Guidelines Working Group, : Metastatic
colorectal cancer: ESMO clinical practice guidelines for diagnosis,
treatment and follow-up. Ann Oncol. 25 Suppl 3:iii1–iii9. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Brenner H, Kloor M and Pox CP: Colorectal
cancer. Lancet. 383:1490–1502. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
de Gramont A, Bosset JF, Milan C, Rougier
P, Bouché O, Etienne PL, Morvan F, Louvet C, Guillot T, François E
and Bedenne L: Randomized trial comparing monthly low-dose
leucovorin and fluorouracil bolus with bimonthly high-dose
leucovorin and fluorouracil bolus plus continuous infusion for
advanced colorectal cancer: A French intergroup study. J Clin
Oncol. 15:808–815. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Goldberg RM, Sargent DJ, Morton RF, Fuchs
CS, Ramanathan RK, Williamson SK, Findlay BP, Pitot HC and Alberts
SR: A randomized controlled trial of fluorouracil plus leucovorin,
irinotecan, and oxaliplatin combinations in patients with
previously untreated metastatic colorectal cancer. J Clin Oncol.
22:23–30. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tournigand C, André T, Achille E, Lledo G,
Flesh M, Mery-Mignard D, Quinaux E, Couteau C, Buyse M, Ganem G, et
al: FOLFIRI followed by FOLFOX6 or the reverse sequence in advanced
colorectal cancer: A randomized GERCOR study. J Clin Oncol.
22:229–237. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Yamazaki K, Nagase M, Tamagawa H, Ueda S,
Tamura T, Murata K, Eguchi Nakajima T, Baba E, Tsuda M, Moriwaki T,
et al: Randomized phase III study of bevacizumab plus FOLFIRI and
bevacizumab plus mFOLFOX6 as first-line treatment for patients with
metastatic colorectal cancer (WJOG4407G). Ann Oncol. 27:1539–1546.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Petrelli F, Borgonovo K, Cabiddu M,
Ghilardi M, Lonati V, Maspero F, Sauta MG, Beretta GD and Barni S:
FOLFIRI-bevacizumab as first-line chemotherapy in 3500 patients
with advanced colorectal cancer: A pooled analysis of 29 published
trials. Clin Colorectal Cancer. 12:145–151. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Saltz LB, Clarke S, Díaz-Rubio E,
Scheithauer W, Figer A, Wong R, Koski S, Lichinitser M, Yang TS,
Rivera F, et al: Bevacizumab in combination with oxaliplatin-based
chemotherapy as first-line therapy in metastatic colorectal cancer:
A randomized phase III study. J Clin Oncol. 26:2013–2019. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wang Y, Jatkoe T, Zhang Y, Mutch MG,
Talantov D, Jiang J, McLeod HL and Atkins D: Gene expression
profiles and molecular markers to predict recurrence of Dukes' B
colon cancer. J Clin Oncol. 22:1564–1571. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Eschrich S, Yang I, Bloom G, Kwong KY,
Boulware D, Cantor A, Coppola D, Kruhøffer M, Aaltonen L, Orntoft
TF, et al: Molecular staging for survival prediction of colorectal
cancer patients. J Clin Oncol. 23:3526–3535. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Notterman DA, Alon U, Sierk AJ and Levine
AJ: Transcriptional gene expression profiles of colorectal adenoma,
adenocarcinoma, and normal tissue examined by oligonucleotide
arrays. Cancer Res. 61:3124–3130. 2001.PubMed/NCBI
|
|
13
|
Wen WH, Bernstein L, Lescallett J,
Beazer-Barclay Y, Sullivan-Halley J, White M and Press MF:
Comparison of TP53 mutations identified by oligonucleotide
microarray and conventional DNA sequence analysis. Cancer Res.
60:2716–2722. 2000.PubMed/NCBI
|
|
14
|
Iwao-Koizumi K, Matoba R, Ueno N, Kim SJ,
Ando A, Miyoshi Y, Maeda E, Noguchi S and Kato K: Prediction of
docetaxel response in human breast cancer by gene expression
profiling. J Clin Oncol. 23:422–431. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Del Rio M, Molina F, Bascoul-Mollevi C,
Copois V, Bibeau F, Chalbos P, Bareil C, Kramar A, Salvetat N,
Fraslon C, et al: Gene expression signature in advanced colorectal
cancer patients select drugs and response for the use of
leucovorin, fluorouracil, and irinotecan. J Clin Oncol. 25:773–780.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Estevez-Garcia P, Rivera F, Molina-Pinelo
S, Benavent M, Gómez J, Limón ML, Pastor MD, Martinez-Perez J,
Paz-Ares L, Carnero A and Garcia-Carbonero R: Gene expression
profile predictive of response to chemotherapy in metastatic
colorectal cancer. Oncotarget. 6:6151–6159. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Li S, Lu X, Chi P and Pan J:
Identification of HOXB8 and KLK11 expression levels as potential
biomarkers to predict the effects of FOLFOX4 chemotherapy. Future
Oncol. 9:727–736. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Therasse P, Arbuck SG, Eisenhauer EA,
Wanders J, Kaplan RS, Rubinstein L, Verweij J, Van Glabbeke M, van
Oosterom AT, Christian MC and Gwyther SG: New guidelines to
evaluate the response to treatment in solid tumors. European
Organization for Research and Treatment of Cancer, National Cancer
Institute of the United States, National Cancer Institute of
Canada. J Natl Cancer Inst. 92:205–216. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Miller AB, Hoogstraten B, Staquet M and
Winkler A: Reporting results of cancer treatment. Cancer.
47:207–214. 1981. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Aras M, Erdil TY, Dane F, Gungor S, Ones
T, Dede F, Inanir S and Turoglu HT: Comparison of WHO RECIST 1.1,
EORTC, and PERCIST criteria in the evaluation of treatment response
in malignant solid tumors. Nucl Med Commun. 37:9–15.
2016.PubMed/NCBI
|
|
21
|
Khokher S, Qureshi MU and Chaudhry NA:
Comparison of WHO and RECIST criteria for evaluation of clinical
response to chemotherapy in patients with advanced breast cancer.
Asian Pac J Cancer Prev. 13:3213–3218. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Choi JH, Ahn MJ, Rhim HC, Kim JW, Lee GH,
Lee YY and Kim IS: Comparison of WHO and RECIST criteria for
response in metastatic colorectal carcinoma. Cancer Res Treat.
37:290–293. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Park JO, Lee SI, Song SY, Kim K, Kim WS,
Jung CW, Park YS, Im YH, Kang WK, Lee MH, et al: Measuring response
in solid tumors: Comparison of RECIST and WHO response criteria.
Jpn J Clin Oncol. 33:533–537. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Gautier L, Cope L, Bolstad BM and Irizarry
RA: affy-analysis of Affymetrix GeneChip data at the probe level.
Bioinformatics. 20:307–315. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Leek JT, Johnson WE, Parker HS, Jaffe AE
and Storey JD: The sva package for removing batch effects and other
unwanted variation in high-throughput experiments. Bioinformatics.
28:882–883. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ritchie ME, Phipson B, Wu D, Hu Y, Law CW,
Shi W and Smyth GK: limma powers differential expression analyses
for RNA-sequencing and microarray studies. Nucleic Acids Res.
43:e472015. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yu G, Wang LG, Han Y and He QY:
clusterProfiler: An R package for comparing biological themes among
gene clusters. OMICS. 16:284–287. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Wu TT, Chen YF, Hastie T, Sobel E and
Lange K: Genome-wide association analysis by lasso penalized
logistic regression. Bioinformatics. 25:714–721. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Cuyle PJ and Prenen H: Current and future
biomarkers in the treatment of colorectal cancer. Acta Clin Belg.
72:103–115. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Robin X, Turck N, Hainard A, Tiberti N,
Lisacek F, Sanchez JC and Müller M: pROC: An open-source package
for R and S+ to analyze and compare ROC curves. BMC Bioinformatics.
12:772011. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Stintzing S: Personalized treatment for
colorectal carcinomas. Dtsch Med Wochenschr. 142:1652–1659.
2017.(In German). PubMed/NCBI
|
|
32
|
Gustavsson B, Carlsson G, Machover D,
Petrelli N, Roth A, Schmoll HJ, Tveit KM and Gibson F: A review of
the evolution of systemic chemotherapy in the management of
colorectal cancer. Clin Colorectal Cancer. 14:1–10. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Iwamoto S, Takahashi T, Tamagawa H,
Nakamura M, Munemoto Y, Kato T, Hata T, Denda T, Morita Y, Inukai
M, et al: FOLFIRI plus bevacizumab as second-line therapy in
patients with metastatic colorectal cancer after first-line
bevacizumab plus oxaliplatin-based therapy: The randomized phase
III EAGLE study. Ann Oncol. 26:1427–1433. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Bazarbashi S, Aljubran A, Alzahrani A,
Mohieldin A, Soudy H and Shoukri M: Phase I/II trial of
capecitabine, oxaliplatin, and irinotecan in combination with
bevacizumab in first line treatment of metastatic colorectal
cancer. Cancer Med. 4:1505–1513. 2015. View
Article : Google Scholar : PubMed/NCBI
|
|
35
|
Heinemann V, von Weikersthal LF, Decker T,
Kiani A, Vehling-Kaiser U, Al-Batran SE, Heintges T, Lerchenmüller
C, Kahl C, Seipelt G, et al: FOLFIRI plus cetuximab versus FOLFIRI
plus bevacizumab as first-line treatment for patients with
metastatic colorectal cancer (FIRE-3): A randomised, open-label,
phase 3 trial. Lancet Oncol. 15:1065–1075. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Stremitzer S, Sebio A, Stintzing S and
Lenz HJ: Panitumumab safety for treating colorectal cancer. Expert
Opin Drug Saf. 13:843–851. 2014.PubMed/NCBI
|
|
37
|
Saridaki Z, Souglakos J and Georgoulias V:
Prognostic and predictive significance of MSI in stages II/III
colon cancer. World J Gastroenterol. 20:6809–6814. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Webber EM, Kauffman TL, O'Connor E and
Goddard KA: Systematic review of the predictive effect of MSI
status in colorectal cancer patients undergoing 5FU-based
chemotherapy. BMC Cancer. 15:1562015. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Nakanishi R, Kitao H, Fujinaka Y,
Yamashita N, Iimori M, Tokunaga E, Yamashita N, Morita M, Kakeji Y
and Maehara Y: FANCJ expression predicts the response to
5-fluorouracil-based chemotherapy in MLH1-proficient colorectal
cancer. Ann Surg Oncol. 19:3627–3635. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Simmer F, Venderbosch S, Dijkstra JR,
Vink-Börger EM, Faber C, Mekenkamp LJ, Koopman M, De Haan AF, Punt
CJ and Nagtegaal ID: MicroRNA-143 is a putative predictive factor
for the response to fluoropyrimidine-based chemotherapy in patients
with metastatic colorectal cancer. Oncotarget. 6:22996–23007. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Molina-Pinelo S, Carnero A, Rivera F,
Estevez-Garcia P, Bozada JM, Limon ML, Benavent M, Gomez J, Pastor
MD, Chaves M, et al: MiR-107 and miR-99a-3p predict chemotherapy
response in patients with advanced colorectal cancer. BMC Cancer.
14:6562014. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Candy PA, Phillips MR, Redfern AD, Colley
SM, Davidson JA, Stuart LM, Wood BA, Zeps N and Leedman PJ:
Notch-induced transcription factors are predictive of survival and
5-fluorouracil response in colorectal cancer patients. Br J Cancer.
109:1023–1030. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Mariadason JM, Arango D, Shi Q, Wilson AJ,
Corner GA, Nicholas C, Aranes MJ, Lesser M, Schwartz EL and
Augenlicht LH: Gene expression profiling-based prediction of
response of colon carcinoma cells to 5-fluorouracil and
camptothecin. Cancer Res. 63:8791–8812. 2003.PubMed/NCBI
|
|
44
|
Kursa MB and Rudnicki WR: Feature
selection with the boruta package. J Stat Soft. 36:1–13. 2010.
View Article : Google Scholar
|
|
45
|
Zhang Z and Huang J: Intestinal stem
cells-types and markers. Cell Biol Int. 37:406–414. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Chang EY, Tsai SH, Shun CT, Hee SW, Chang
YC, Tsai YC, Tsai JS, Chen HJ, Chou JW, Lin SY and Chuang LM:
Prostaglandin reductase 2 modulates ROS-mediated cell death and
tumor transformation of gastric cancer cells and is associated with
higher mortality in gastric cancer patients. Am J Pathol.
181:1316–1326. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Li FF, Yan P, Zhao ZX, Liu Z, Song DW,
Zhao XW, Wang XS, Wang GY and Liu SL: Polymorphisms in the CHIT1
gene: Associations with colorectal cancer. Oncotarget.
7:39572–39581. 2016.PubMed/NCBI
|
|
48
|
Chang YT, Yeh YS, Ma CJ, Huang CW, Tsai
HL, Huang MY, Cheng TL and Wang JY: Optimization of a multigene
biochip for detection of relapsed and early relapsed colorectal
cancer. J Surg Res. 220:427–437. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Jun S, Jung YS, Suh HN, Wang W, Kim MJ, Oh
YS, Lien EM, Shen X, Matsumoto Y, McCrea PD, et al: LIG4 mediates
Wnt signalling-induced radioresistance. Nat Commun. 7:109942016.
View Article : Google Scholar : PubMed/NCBI
|