Introduction
Elucidation of the mechanisms underlying the
metastasis of solid tumors may improve patient outcomes, as the
majority of cancer-associated mortalities are due to tumor
progression and dissemination (1).
Previous studies have investigated the role of immunity in tumor
biology; however, the immune-mediated maintenance of tissue
homeostasis (TH) in cancer has not been thoroughly explored
(2–4). Tumor progression may be influenced by
the immune system (2,3). However, the role of tissue-specific
factors in the outcome of adaptive immune responses remains unclear
(4). Advances in molecular biology
have allowed the investigation of the mechanisms involved in
intercellular interactions. Consequently, there is an increased
understanding of the factors involved in these interactions,
allowing a comprehensive description of tissue development to be
made. A number of immune cells, cytokines, growth factors and
enzymes create a favorable microenvironment for maintaining a
steady state in tissues (5,6). However, which of these are essential in
maintaining a favorable tissue microenvironment remains unknown.
The interchange of signals at the tissue level is maintained by
constant synthesis of various short-lived molecules, including
cytokines, integrins and selectins, and exosomes (7,8). TH is
therefore a complex process. The present review attempted to
analyze the functions of the immune system, not including its
protective role against infection, and establish whether it has a
morphogenetic or regulatory function in maintaining TH (9,10).
Consequently, the present review focused on regulatory T cells, due
to the tissue-specific manner these cells operate in (11,12).
Although T cells reside in tissues, they are functionally monitored
by the thymus, and provide feedback on TH from the peripheral to
the central immune system by their homing capacity (13). Elucidating the central immune
regulation of tumor tissue evolution may aid in the development of
novel immune therapies.
Data sources and searches
PubMed (www.ncbi.nlm.nih.gov/pubmed), Google Scholar
(scholar.google.com), Scopus (www.scopus.com/home.uri) and Web of Science
(login.webofknowledge.com) databases were
searched in November 2017 using a combination of key words and text
words related to ‘solid tumor spread’ and ‘central immune
regulation mechanisms’ of this process. The search was not
restricted by date. The main Medical Subject Headings in PubMed
were as follows: i) Neoplasm/metastasis; ii) neoplasms/immunology;
and iii) T-lymphocytes/immunology. The inclusion criteria were as
follows: i) Peer-reviewed published articles; ii) original research
articles; iii) reviews; iv) meeting abstracts; v) proceedings
papers; and vi) book chapters containing information pertaining to
the central immune regulation of tumor spread/metastasis. Documents
that were not published in the public domain were excluded. A total
of 90 articles which were selected by both authors were included in
the current study. Disagreements were resolved through
consensus.
Central immune regulation in maintaining
homeostasis of normal tissue
The immune system detects pathogen invasion, fights
against infection, prevents malignant transformations and
contributes to permanent tissue renewal and remodeling following
damage to the tissue (10,14). The thymus is a central immune organ
that serves a principal role in post-natal human life by
maintaining the development and homeostasis of T cells (15,16). The
regenerative capacity of the thymus undergoes a significant decline
in the postnatal period compared with its prenatal activity;
however, it continues to perform a pivotal role in T-cell
arrangement in adulthood (17). Stem
cells of the thymic epithelium are constantly generated throughout
the lifespan of a human and their pool is dynamically regulated by
signals from the periphery in response to tissue requirements
(18). The thymus generates clones
of regulatory cells during the process of T-cell development, which
occurs due to the recognition of self-antigens (19). Thymically derived regulatory cells
(T-regs) are considered to serve important roles in maintaining and
re-establishing of normal TH (20,21). The
immune system has a functional presence in every tissue and organ,
as immune cells have the unique ability to travel between
compartments (11). Each organ has a
microenvironment that participates in feedback mechanisms in which
dendritic cells present tissue major histocompatibility complex
(MHC) antigens for recycling lymphocytes (22). The continuous recycling of
lymphocytes from the blood into tissues is a highly sophisticated
bi-directional process that reflects the homing capacity of
migrating cells (19). The migrating
lymphocytes patrol the tissues, thus maintaining homeostasis by a
directional transfer of information, which is beneficial for tissue
development (7,10,23). The
destination of the lymphocytes is predetermined by T-cell receptors
(TCRs), which are located on the surface of migrating cells that
interact with the appropriate ligands of high endothelium venules
for penetration into the tissue (12). TCRs are designed to recognize
different MHC molecules, which are presented by the majority of
cells in the body (24). Using
specific receptors, lymphocytes assess the antigenic immunity in
body tissues, and the binding specificity of the TCRs is important
in the process of recognition (25,26).
Consequently, the movement of lymphocytes into the lymphatic system
and blood circulation, as well as their migration into the tissue,
is an organized process (11). The
endothelial cells of capillaries are not passive membranes that
follow physical and chemical laws, rather they select for active
traffic into tissues by target-binding to the receptor by
antigen-antibody interaction (12).
T-lymphocyte migration directed by TCRs is conducted by
ligand-integrin interactions with adhesive molecules of blood
vessel endothelium (27). Immune
surveillance of peripheral tissues by T cells is performed in
response to homeostatic chemokines that are constitutively
expressed in healthy tissues to recruit lymphoid cells in certain
tissue sites (28).
Tissue disturbance due to injury or inflammation
results in the secretion of cytokines, triggering the hyperactive
expression of specific integrins on the surface of endothelial
cells. The lymphocytes connected to the integrins adhere to the
endothelium, enter between adjacent endothelial cells and exit the
bloodstream (27). Simultaneously,
lymphocytes, macrophages and other lymphoid cells, including
neutrophils and monocytes, penetrate through the intercellular gaps
and re-enter the circulation. Lymphatic tissue is constantly
renewing its cell population in order to continuously recycle
lymphocytes (14,29). Recirculating lymphocytes are a major
part of the population of small lymphocytes, the majority of which
are T-lymphocytes (30).
T-lymphocytes are characterized by their rapid migration, which
enables them to constantly move between the blood and peripheral
organs (31,32). As such, small lymphocytes are an
extremely mobile cell population. Due to their mobility,
lymphocytes are able to penetrate into intercellular spaces
(33). Subsequent to passing through
the vessel endothelium, lymphocytes may interact with intercellular
matrix proteins and tissue cells. The complex interactions among
lymphocytes, residing immune cells, stromal components and
tissue-specific factors influence the outcome of the immune
responses at the tissue level (14).
As a result, all functioning tissues have active lymphocytes
located around postcapillary venules (11,34). The
zone of interaction between endothelial cells, lymphocytes and
tissue structures is termed the immune regulatory zone, or the
immune regulatory compartment of an organ (34,35).
Previous studies demonstrated that the majority of tissue
lymphocytes are T-lymphocytes, which originate from the
double-positive helper/suppressor population, and are currently
defined as the regulatory population (13,36).
Through a homing mechanism, T-lymphocytes undergo a settling stage
in the tissue, where they acquire their immunological specificity
(11).
The thymus is an important site for the development
of T-regs during the positive selection process of clones that are
tailored to the tissue in which they complete differentiation
(37). Following this process,
T-regs join the lymphatic system and blood circulation. Circulating
lymphocytes form a pool of cells carrying receptors that are
specific for the particular tissues that created this clone
(11). Once the migration process
has started, a functional complex that includes an adjustable
tissue and regional lymph nodes is formed. It provides a
selectivity of migration, termed homing (12). Such selectivity is associated with
effector lymphocytes acquiring novel properties dictated by the
local tissue microenvironment (38,39).
Therefore, any regenerating/renewing healthy tissue that is
non-inflamed drives the preferential recruitment of a highly
restricted repertoire of specific T-regs for its continued
development (13).
One issue that remains is concerned with the manner
in which recirculating T-cells perform the morphogenetic functions
of the immune system. Cell-to-cell interactions assist
multicellular organisms to function as a stable system (40). Informational support by the transfer
of genetic material in the form of exosomes to developing tissue is
an immunoediting function of T-cells (41), although the transmission mechanism of
information pertaining to regeneration has not been fully
elucidated. Previous studies have indicated that cells can
communicate via the direct exchange of genetic patterns in the form
of exosomes and apoptotic bodies (7,40,42). The
processes of cell-to-cell communications via exosomes are a
potential driving factor of phenotypic changes and cellular
plasticity during tissue regeneration (43). Therefore, specific genetic messages
are designed to be embedded into accepting cells for their
differentiation with subsequent tissue development. The required
level of exosomes is provided by cell activation and apoptosis,
which underlies the effector mechanisms of immune cell action
(44). The genetic information
contained within exosomes in the form of DNA or RNA can influence
the target cell by triggering activation, differentiation or even
by promoting apoptosis (40). In the
immune system, exosomes from T cells can directly fuse with
accepted tissue cells, releasing relevant functional information
(45). The involvement of
lymphocytes in the regulation of tissue development has clearly
been demonstrated by their presence in the microenvironment of
differentiating hematopoietic cells of the bone marrow (46). Furthermore, T-regs have been shown to
serve an important role in maintaining the homeostasis of skin and
various mucosal surfaces, from which epithelial tumors have been
identified to form (13,47).
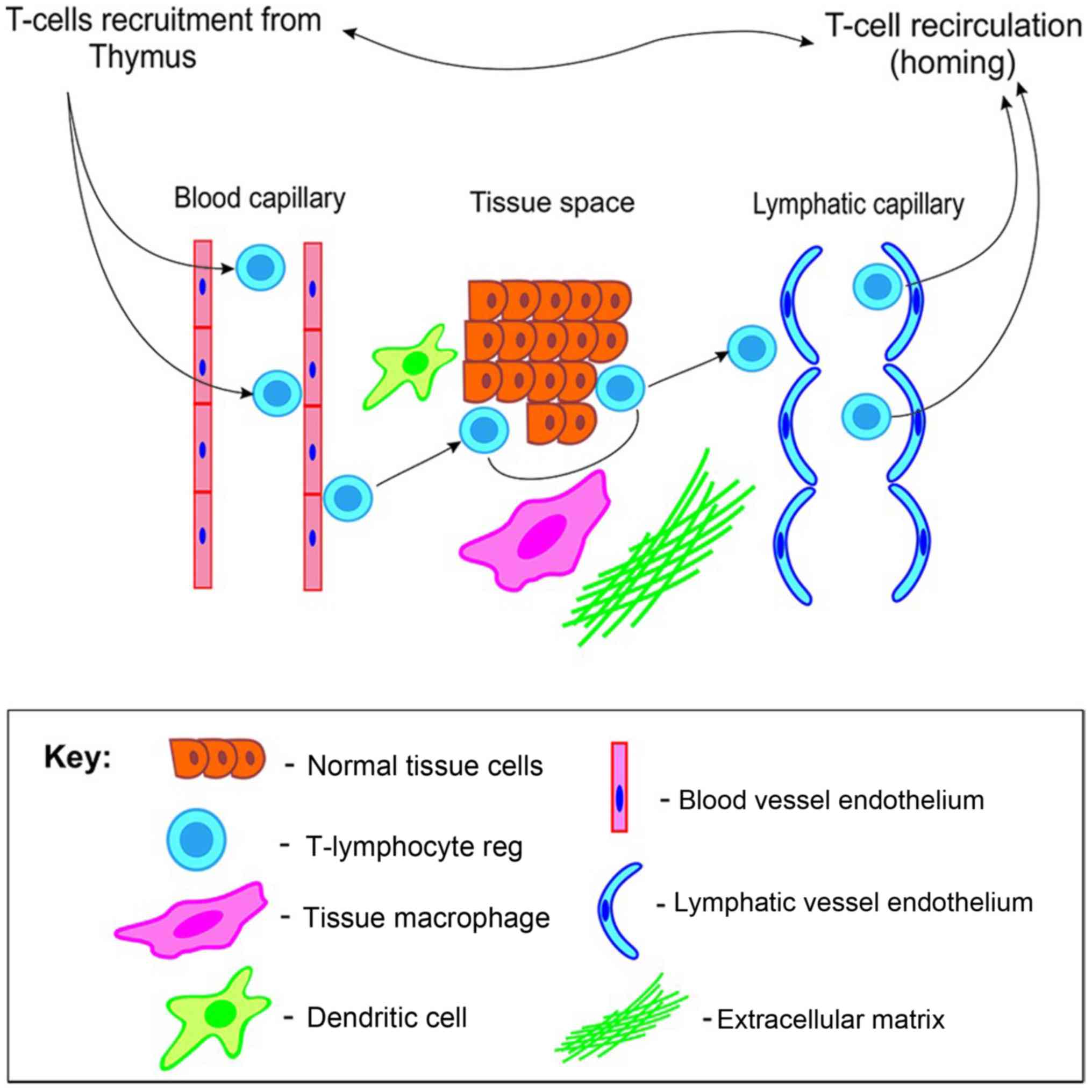
In summary, any functioning tissue is a highly
organized peripheral division of the immune system with a stable
contingent of residing cells and a mobile component comprised of
recycling regulatory T cells that are functionally monitored by the
thymus. These T cells provide a feedback reaction to the thymus as
a central part of the immune system. T-regs actively participate in
the generation of adaptive immune responses. The processes of the
migration and recirculation of immune cells, and their active
interactions with other tissue structures ensure the maintenance of
TH (Fig. 1).
Immune regulation in case of tumor tissue
manifestation and metastatic spread
One topic of note is what happens to the highly
sophisticated hierarchy of TH regulation in the extreme case of its
imbalance, i.e., during malignant transformation of tissue. Since
tumor cells originate from normal ones, the key principles of
immune regulation are preserved in the transformed tissue.
Therefore, immune mechanisms that regulate tumor tissue function
may be the same as in cases of normal non-metastatic tissues
(48).
When tumors develop, the new tissue evolves and the
metastatic potential of the rapidly dividing cells (cellular
clones) constantly increases. Clinically, metastasis is the last
stage of tumor progression. Prior studies revealed that the process
of cancer spreading is not random, and follows domestic rules and
mechanisms in the ‘host-tumor’ system (49–51).
This was confirmed when certain cancer types elected to metastasize
over their preferred target tissues (52). Previous studies have provided
supporting evidence of the importance a common mechanism involved
in the regulation of tumor progression: i) Tumor cells acquire
metastatic properties prior to migration from the site of the
primary tumor (53); ii) the
systemic circulation of tumor cells may subsequently remain latent
for an extended period of time (54)
and the presence of tumor cells in the blood is not indicative of
metastasis (55,56); iii) the formation of metastatic
niches in the form of restructured stroma in tissues distant from
the site of the primary tumor begins prior to the dissemination of
malignant cells (2,57); and iv) the enhanced vascularization
of blood and lymph vessels in tumors contributes to the process of
metastasis (58,59). Clonal polymorphism, genetic
instability of tumor cells and a hypoxic microenvironment
contribute to the expression of multiple angiogenic factors in
malignant tissues (60–62). Nevertheless, it has been postulated
that stimulation of vessel growth in tumors occurs via the same
mechanism as that in normal tissue (63). As such, blood vessels treat the tumor
as an extra cell mass, which requires nutrition and elimination of
the products of tissue metabolism (64). The aforementioned process supports
the hypothesis that the influence of the host on the formation of
the tumor microenvironment is a factor that determines when the
metastatic process is initiated as the formation of metastatic
niches begins before the spread of malignant cells, and
neoangiogenesis contributes to the process of metastasis. However,
the central regulatory mechanisms that activate selected tumor
cells for metastatic initiation remain poorly defined.
T-regs with the phenotype cluster of differentiation
(CD)4+CD25+forkhead box P3+
(FOXP3+) imitate mediators of immune editing
(surveillance) (65–67). Novel immune checkpoint inhibitors
recognize that T-regs serve a key role in tumor development
(68). Therefore, elucidating the
associations of T-regs and tumor cells may provide insight into the
modulation of the host response to the malignant transformation of
tissues (66). T-reg density within
tumor lesions and the recurrent imbalance of its contents in the
blood has been associated with the clinical outcome of patients in
a number of types of cancer, including breast, cervical,
endometrial, ovarian, colorectal and pancreatic cancer (69–71).
Tumor-specific T-regs may originate in the thymus during T-cell
development and are recruited to the tumor lesion in a preferential
manner from the diverse systemic pool of T-regs (19,48).
The phenotype, differentiation status and function
of regulatory immune cells depend on the anatomical compartment in
which the cells reside. Even immune cells that originated from the
same precursors, but which reside in different tissues, have
diverse functions as they are instructed by different,
organ-specific factors (11).
Consequently, different types of tissue have different antigens
that activate the immune system and generate regional immune
responses, which is associated with the relative stability of the
tissue. In cases of tumor transformation due to immune escape
mechanisms, the immune system may maintain homeostasis in the
newly-formed anatomical site, i.e., the tumor. Therefore, the
immune system allows the tumor to grow rather than destroy it
(65,72), suggesting a mechanism of how tumor
tissue development, and progression may coexist with the normal
function of an organ (2,64). Tumor cells are constantly exposed to
immune cells during each phase of the metastatic process,
suggesting that the immune cells may restrict their development
(73). However, previous studies
have revealed that tumor-infiltrating immune cells may instead
promote the metastatic cascade (2,3,72). T-regs may serve a role in increasing
the number of surviving tumor cells in circulation and metastatic
sites; however, the precise mechanisms underlying this process
remain unknown (2).
The thymus orchestrates the arrangement of T-cell
clones and predetermines the function of T-cell populations on the
periphery (27,74). A prior study that observed changes in
the thymus during experimental carcinogenesis revealed that the
development of malignant tumors in the colons of rats was
correlated with significant fluctuations in the morphology of the
thymus, highlighting the role of central immunological regulation
in tumor biology (75). These
variations were manifested in the differentiation and apoptosis of
thymus cells, as well as changes to the components in the
microenvironment of the thymus cells. Notably, significant
transformations in the thymus, including an increase in the number
of thymic cells, active T-lymphocytes and changes in the
microenvironment were observed during the precancerous stage in the
intestinal mucosa (75). The
aforementioned study reported that colonic cancer had a greater
impact on the thymus morphology. It manifested in the elevation of
proliferation and differentiation of thymocytes into mature forms
with their subsequent traffic to the colonic mucosa (75). Experimental data regarding the
increased egress of mature thymocytes and their migration into
peripheral circulation are consistent with clinical data reporting
an increased T-reg lymphocyte population in the peripheral blood of
patients with solid tumors including melanoma and breast, lung,
gastric, ovarian, head and neck, tumors (65,70,76).
Furthermore, T-reg lymphocytes have been detected in lymph nodes
containing micrometastases, but not in healthy lymph nodes
(77). The detection of T-reg
lymphocytes and the formation of new lymphatic vessels precede the
detection of metastatic lesions in the regional lymph nodes
(78). T-lymphocyte clones migrate
and infiltrate a solid tumor (70).
According to numerous studies, they are mainly represented by the
same regulatory thymic subpopulation of lymphocytes, which has been
discussed previously (48,79,80).
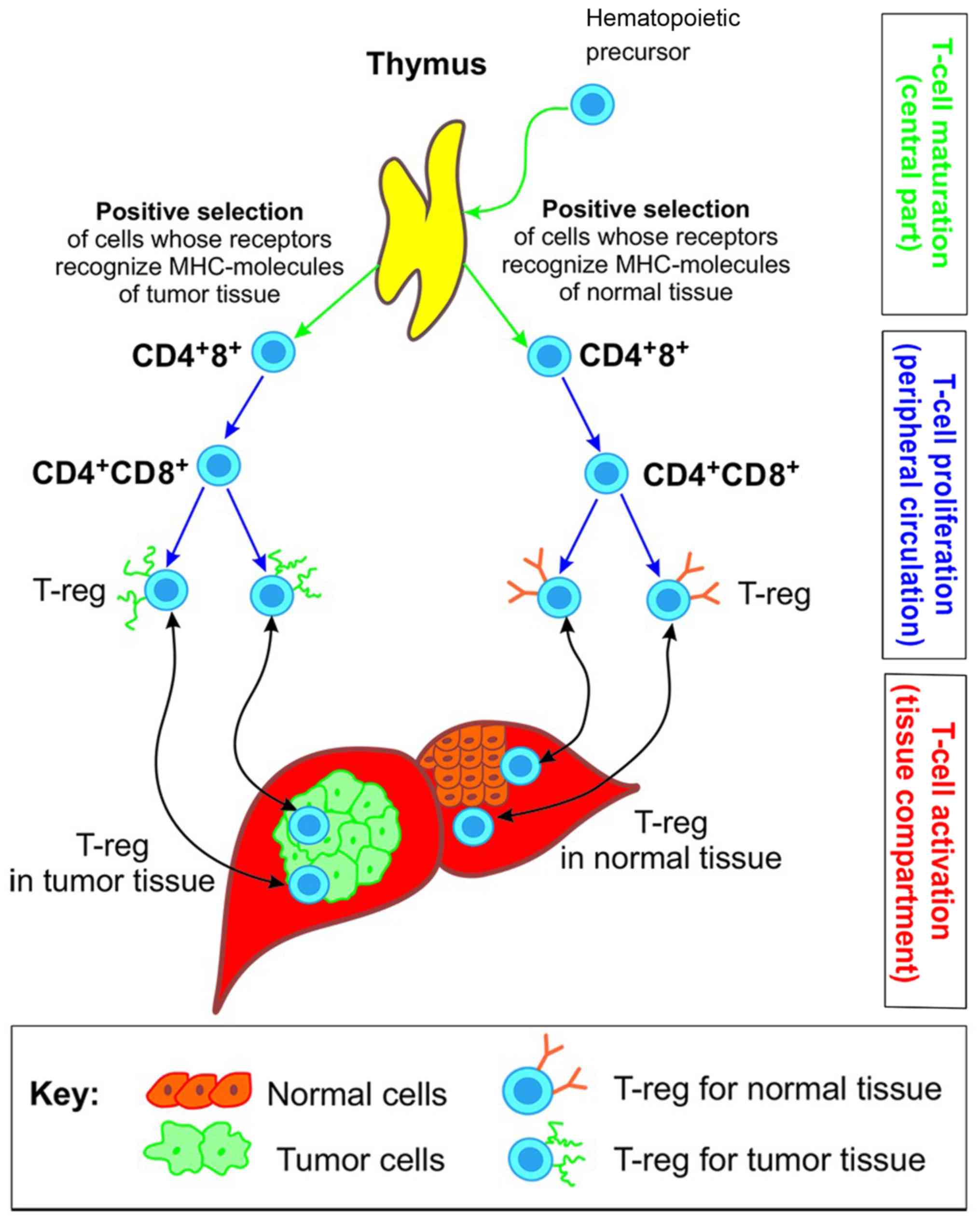
The process of malignant transformation of tissue is
accompanied by the formation of T-lymphocyte clones designed for
that tissue. These lymphocytes begin to differentiate in the thymus
and complete the differentiation process in the tumor tissue, which
is actively involved in the generation of immune signals required
to maintain tissue development (81). Consequently, the tumor tissue may be
considered as a peripheral compartment of the immune system whose
regulatory zone includes vessels, endothelial cells, circulating
and settled pools of T-reg lymphocytes, tumor cells and components
of the extracellular matrix. Therefore, the affected organ consists
of tumor and normal tissues. Each of these tissue types has a zone
infiltrated by T-reg lymphocytes designed for this tissue type.
There are clones for tumor and normal tissues in the peripheral
circulation of an organism with cancer. Phenotypically these clones
are similar, all being T-reg CD4+ FOXP3+
cells (79,82). However, they differ in the direction
of migration to the appropriate tissue, which expresses its own
unique set of histocompatible antigens (Fig. 2).
An increased number of T-regs in tumor tissues is
associated with a higher degree of differentiation and an improved
prognosis (69–71,76),
suggesting that T-regs serve a role in the pace of tumor
progression. A previous study in patients with breast cancer
assessed T-reg lymphocytes profiles in samples of tumor tissue
following the administration of neo-adjuvant chemotherapy, and a
significant reduction in T-regs among infiltrating tumor tissue
lymphocytes was detected (83). This
suggests the possibility of using T-reg lymphocytes as a prognostic
marker for response to chemotherapy and demonstrates a direct
association between tumor regression and a reduction in the
population of T-reg lymphocytes (70,84,85).
Novel immunotherapies may have a greater impact on
T-reg lymphocyte subpopulations than traditional chemotherapy
agents (68,86). The clinical application of targeted
antitumor drugs against cytotoxic T-lymphocyte associated protein 4
and programmed cell death 1 lymphocyte receptors, termed immune
checkpoint inhibitors, has demonstrated efficacy in a subset of
patients with aggressive solid tumors, including disseminated
melanoma, renal cell carcinoma and non-small cell lung cancer
(86,87). Furthermore, patients demonstrated
partial or complete tumor regression following the administration
of the aforementioned immune therapies, which persisted following
the cessation of therapy, which was renewed as an identical
treatment if disease progression occurred (87). Novel immunotherapies have increased
the potential available targets of anticancer drugs, providing
insights into the mechanisms underlying tumor development and
progression. Preceding studies have identified novel agents that
target lymphocytes and alter the immunological microenvironment of
tumors, thus promoting tolerance and changes to the apoptotic
program in tumor tissues (81,88,89).
Tolerance may be considered as the deprivation of the informational
support from the host to the tumor (90). This data implicates T-regs in the
process of tumor progression and the presence of central immune
mechanisms that govern tumor spread (2,3). In
spite of the fact that the tumor promoting role of
tumor-infiltrating immune cells at each step of the metastatic
cascade has been stated, interactions between tumor and immune
cells are traditionally considered in the context of tolerance or
suppression by the immune system only at the tissue level without
the evaluation of central, i.e. thymic, regulation of immune cell
behavior (2,3,88).
Previous studies investigating malignant tissue revealed central
mechanisms of immune regulation that define the character,
direction and outcomes of cellular interactions at the tissue level
(2,48). As this novel therapeutic strategy
with checkpoint inhibitors has demonstrated, a functional blockade
of the lymphocytes regulating homeostasis in tumor tissue leads to
tumor regression due to the deprivation of immunological support
from the host (86,90). Therefore, there is a requirement for
selective therapeutic agents that target the population of
tumor-associated T-regs and not other T-regs in the body.
Conclusion
The current review summarizes the data on the
participation of the immune system in the process of tumor growth
and metastatic spread. Previous studies have demonstrated the
importance of the role of recirculating and tissue-residing
immunocompetent cells in tumor progression. However, even a
detailed phenotypic specification of lymphoid cells and analysis of
their interactions does not completely describe the tumor spread
regulation without considering the central part of T-cell
competency formation. Central regulation mechanisms provide insight
into the predestination and direction of immune reactions in tumor
tissue. We believe that enough data pertaining to the regulatory
levels of tumor metastasis is available to attempt to influence the
process of tumor spread globally, by changing the speed and
direction through therapies that target not only tumor cells, but
also the regulatory mechanisms of the immune system. For example,
the targeted impact on the adaptive immune response with immune
checkpoint inhibitors is a successful strategy in immune system
interventions in patients with cancer. Finally, elucidating the
mechanisms of tumor metastasis with regard to immunological
regulation may aid the identification and development of novel
therapeutic strategies. A limitation of the present review is that
it is purely narrative. Insight into the process of tumor spread
through the prism of central immune regulation may be of interest
to clinicians, and an in-depth explanation of the mechanisms
underlying the efficiency and toxicity of novel immune therapies
with checkpoint inhibitors is a topic for future research.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
NL conceived the study. NS critically revised the
manuscript and contributed to the editing process. The two authors
read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
TH
|
tissue homeostasis
|
|
T-reg
|
thymically derived regulatory cell
|
|
TCR
|
T-cell receptor
|
References
|
1
|
Jiang WG and Ablin RJ: Cancer metastasis,
challenges, progress and the opportunities. Front Biosci (Elite
Ed). 3:391–394. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
2
|
Kitamura T, Qian BZ and Pollard JW: Immune
cell promotion of metastasis. Nat Rev Immunol. 15:73–86. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Smith HA and Kang YT: The
metastasis-promoting roles of tumor-associated immune cells. J Mol
Med (Berl). 91:411–429. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Fridman WH, Pages F, Sautes-Fridman C and
Galon J: The immune contexture in human tumours: Impact on clinical
outcome. Nat Rev Cancer. 12:298–306. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zlotnic A and Yoshie O: The chemokine
superfamily revisited. Immunity. 36:705–716. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Almeida FF and Belz GT: Innate lymphoid
cells: Models of plasticity for immune homeostasis and rapid
responsiveness in protection. Mucosal Immunol. 9:1103–1112. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Corrado C, Raimondo S, Chiesi A, Ciccia F,
De Leo G and Alessandro R: Exosomes as intercellular signaling
organelles involved in health and disease: Basic science and
clinical applications. Int J Mol Sci. 14:5338–5366. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wang CM, Ploia C, Anselmi F, Sarukhan A
and Viola A: Adenosine triphosphate acts as a paracrine signaling
molecule to reduce the motility of T cells. EMBO J. 33:1354–1364.
2014.PubMed/NCBI
|
|
9
|
Fidler IJ: Lymphocytes are not only
immunocytes. Biomedicine. 32:1–3. 1980.PubMed/NCBI
|
|
10
|
Senovilla L, Galluzzi L, Zitvogel L and
Kroemer G: Immunosurveillance as a regulator of tissue homeostasis.
Trends Immunol. 34:471–481. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hu W and Pasare C: Location, location,
location: Tissue-specific regulation of immune responses. J Leukoc
Biol. 94:409–421. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Shechter R, London A and Schwartz M:
Orchestrated leukocyte recruitment to immune-privileged sites:
Absolute barriers versus educational gates. Nat Rev Immunol.
13:206–218. 2013. View
Article : Google Scholar : PubMed/NCBI
|
|
13
|
Schaerli P, Ebert L, Willimann K, Blaser
A, Roos RS, Loetscher P and Moser B: A skin-selective homing
mechanism for human immune surveillance T cells. J Exp Med.
199:1265–1275. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Satija R and Shalek AK: Heterogeneity in
immune responses: From populations to single cells. Trends Immunol.
35:219–229. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Caramalho I, Nunes-Cabaco H, Foxall RB and
Sousa AE: Regulatory T-cell development in the human thymus. Front
Immunol. 6:3952015. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ge Q, Hu H, Eisen HN and Chen J: Different
contributions of thymopoiesis and homeostasis-driven proliferation
to the reconstitution of naive and memory T cell compartments. Proc
Natl Acad Sci USA. 99:2989–2994. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Chinn IK, Blackburn CC, Manley NR and
Semprowski GD: Changes in primary lymphoid organs with aging. Semin
Immunol. 24:309–320. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ucar O, Li K, Dvornicov D, Kreutz C,
Timmer J, Matt S, Brenner L, Smedley S, Travis MA, Hoffman TG, et
al: A thymic epithelial stem cell pool persists throughout ontogeny
and is modulated by TGF-β. Cell Rep. 17:448–457. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Hsieh CS, Lee HM and Lio CW: Selection of
regulatory T cells in the thymus. Nat Rev Immunol. 12:157–567.
2012. View
Article : Google Scholar : PubMed/NCBI
|
|
20
|
Dobrzanski MJ: Expanding roles for CD4 T
cells and their subpopulations in tumor immunity and therapy. Front
Oncol. 3:632013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
von Boehmer H: The thymus in immunity and
in malignancy. Cancer Immunol Res. 2:592–597. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Dong J, Chen Y, Xu X, Jin R, Teng F, Yan
F, Tang H, Li P, Sun X, Li Y, et al: Homeostatic properties and
phenotypic maturation of murine CD4+ pre-thymic
emigrants in the thymus. PLoS One. 8:e563782013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Munoz MA, Biro M and Weninger W: T cell
migration in intact lymph nodes in vivo. Curr Opin Cell Biol.
30:17–24. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Singh NK, Riley TP, Baker SCB, Borrman T,
Weng Z and Baker BM: Emerging concepts in TCR specificity:
Rationalizing and (maybe) predicting outcomes. J Immunol.
199:2203–2213. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Parrish HL, Deshpande NR, Vasic J and
Kuhns MS: Functional evidence for TCR-intrinsic specificity for
MHCII. Proct Natl Acad Sci USA. 113:3000–3005. 2016. View Article : Google Scholar
|
|
26
|
Sethna Z, Elhanati Y, Dudgeon CS, Callan
CG Jr, Levine AJ, Mora T and Walczak AM: Insights into immune
system development and function from mouse T-cell repertoires. Proc
Natl Acad Sci USA. 114:2253–2258. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Muller WA: How endothelial cells regulate
transmigration of leukocytes in the inflammatory response. Am J
Pathol. 184:886–896. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Anders HJ, Romagnani P and Mantovani A:
Pathomechanisms: Homeostatic chemokines in health, tissue
regeneration, and progressive diseases. Trends Mol Med. 20:154–165.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Thiault N, Darrigues J, Adoue V, Gros M,
Binet B, Perals C, Leobon B, Fazilleau N, Joffre OP, Robey EA, et
al: Peripheral regulatory T lymphocytes recirculating to the thymus
suppress the development of their precursors. Nat Immunol.
16:628–634. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Farber DL, Yudanin NA and Restifo NP:
Human memory T cells: Generation, compartmentalization and
homeostasis. Nat Rev Immunol. 14:24–35. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Halkias J, Melichar HJ, Taylor KT and
Robey EA: Tracking migration during human T cell development. Cell
Mol Life Sci. 71:3101–3117. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Dominguez GA, Anderson NR and Hammer DA:
The direction of migration of T-lymphocytes under flow depends upon
which adhesion receptors are engaged. Integr Biol (Camb).
7:345–355. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Mrass P, Petravic J, Davenport MP and
Weninger W: Cell-autonomous and environmental contributions to the
interstitial migration of T cells. Semin Immunopathol. 32:257–274.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Ruddle NH: Lymphatic vessels and tertiary
lymphoid organs. J Clin Invest. 124:953–959. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Mai J, Virtue A, Shen J, Wang H and Yang
XF: An evolving new paradigm: Endothelial cells-conditional innate
immune cells. J Hematol Oncol. 6:612013. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Smigiel KS, Srivastava S, Stolley JM and
Campbell DJ: Regulatory T-cell homeostasis: Steady-state
maintenance and modulation during inflammation. Immunol Rev.
259:40–59. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Feinerman O, Jentsch G, Tkach KE, Coward
JW, Hathorn MM, Sneddon MW, Emonet T, Smith KA and Altan-Bonnet G:
Single-cell quantification of IL-2 response by effector and
regulatory T cells reveals critical plasticity in immune response.
Mol Syst Biol. 6:4372010. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Barbi J, Pardoll D and Pan F: Treg
functional stability and its responsiveness to the
microenvironment. Immunol Rev. 259:115–139. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Zhan Y, Bourges D, Dromey JA, Harrison LC
and Lew AM: The origin of thymic CD4+CD25+
regulatory T cells and their co-stimulatory requirements are
determined after elimination of recirculating peripheral
CD4+ cells. Int Immunol. 19:455–463. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Mittelbrunn M and Sánchez-Madrid F:
Intercellular communication: Diverse structures for exchange of
genetic information. Nat Rev Mol Cell Biol. 13:328–335. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Mittelbrunn M, Gutierrez-Vazquez C,
Villarroya-Beltri C, Gonzalez S, Sanchez-Cabo F, González MÁ,
Bernad A and Sanchez-Madrid F: Unidirectional transfer of
microRNA-loaded exosomes from T cells to antigen-presenting cells.
Nat Commune. 2:2822011. View Article : Google Scholar
|
|
42
|
Azmi AS, Bao B and Sarkar FH: Exosomes in
cancer development, metastasis, and drug resistance: A
comprehensive review. Cancer Metastasis Rev. 32:623–642. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Yáñez-Mó M, Siljander PR, Andreu Z, Zavec
AB, Borràs FE, Buzas EI, Buzas K, Casal E, Cappello F, Carvalho J,
et al: Biological properties of extracellular vesicles and their
physiological functions. J Extracell Vesicles. 4:270662015.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Green DR, Droin N and Pinkoski M:
Activation-induced cell death in T cells. Immunol Rev. 193:70–81.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Ventimiglia LN and Alonso MA: Biogenesis
and function of T cell-derived exosomes. Front Cell Dev Biol.
4:842016. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Tang Q, Jiang D, Harfuddin Z, Cheng K, Moh
MC and Schwarz H: Regulation of myelopoiesis by CD137L signaling.
Int Rev Immunol. 33:454–469. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Medler TR and Coussens LM: Duality of the
immune response in cancer: Lessons learned from skin. J Invest
Dermatol. 134:E23–E28. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Savage PA, Leventhal DS and Malchow S:
Shaping the repertoire of tumor-infiltrating effector and
regulatory T cells. Immunol Rev. 259:245–258. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Seyfried TN and Huysentruyt LC: On the
origin of cancer metastasis. Crit Rev Oncog. 18:43–73. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Keskinov AA and Shurin MR: Myeloid
regulatory cells in tumor spreading and metastasis. Immunobiology.
220:236–242. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Kovács KA, Hegedus B, Kenessey I and Tímár
J: Tumor type-specific and skin region-selective metastasis of
human cancers: Another example of the ‘seed and soil’ hypothesis.
Cancer Metastasis Rev. 32:493–499. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Ben-Baruch A: Organ selectivity in
metastasis: Regulation by chemokines and their receptors. Clin Exp
Metastasis. 25:345–356. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Satelli A, Mitra A, Brownlee Z, Xia X,
Bellister S, Overman MJ, Kopetz S, Ellis LM, Meng QH and Li S:
Epithelial-mesenchymal transitioned circulating tumor cells capture
for detecting tumor progression. Clin Cancer Res. 21:899–906. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Dasgupta A, Lim AR and Ghajar CM:
Circulating and disseminated tumor cells: Harbingers or initiators
of metastasis? Mol Oncol. 11:40–61. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Caceres G, Puskas JA and Magliocco AM:
Circulating tumor cells: A window into tumor development and
therapeutic effectiveness. Cancer Control. 22:167–176. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Caixeiro NJ, Kienzle N, Lim SH, Spring KJ,
Tognela A, Scott KF, de Souza P and Becker TM: Circulating tumour
cells-a bona fide cause of metastatic cancer. Cancer Metastasis
Rev. 33:747–756. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Sceneay J, Smyth MJ and Möller A: The
pre-metastatic niche: Finding common ground. Cancer Metastasis Rev.
32:449–464. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Paduch R: The role of lymphangiogenesis
and angiogenesis in tumor metastasis. Cell Oncol (Dordr).
39:397–410. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Coso S, Bovay E and Petrova TV: Pressing
the right buttons: Signaling in lymphangiogenesis. Blood.
123:2614–2624. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Pietras K and Östman A: Hallmarks of
cancer: Interactions with the tumor stroma. Exp Cell Res.
316:1324–1331. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Spano D and Zollo M: Tumor
microenvironment: A main actor in the metastasis process. Clin Exp
Metastasis. 29:381–395. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Spinella F, Caprara V, Cianfrocca R,
Rosanò L, Di Castro V, Garrafa E, Natali PG and Bagnato A: The
interplay between hypoxia, endothelial and melanoma cells regulates
vascularization and cell motility through endothelin-1 and vascular
endothelial growth factor. Carcinogenesis. 35:840–848. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Re RN and Cook JL: An intracrine view of
angiogenesis. Bioessays. 28:943–953. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Egeblad M, Nakasone ES and Werb Z: Tumors
as organs: Complex tissues that interface with the entire organism.
Dev Cell. 18:884–901. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Wolf D, Sopper S, Pircher A, Gastl G and
Wolf AM: Treg(s) in cancer: Friends or foe? J Cell Physiol.
230:2598–2605. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Nishikawa H and Sakaguchi S: Regulatory T
cells in tumor immunity. Int J Cancer. 127:759–767. 2010.PubMed/NCBI
|
|
67
|
Bhatia A and Kumar Y: Cellular and
molecular mechanisms in cancer immune escape: A comprehensive
review. Expert Rev Clin Immunol. 10:41–62. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Dyck L and Mills KHG: Immune checkpoints
and their inhibition in cancer and infectious diseases. Eur J
Immunol. 47:765–779. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Curiel TJ: Regulatory T cells and
treatment of cancer. Curr Opin Immunol. 20:241–246. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
70
|
deLeeuw RJ, Kost SE, Kakal JA and Nelson
BH: The prognostic value of FoxP3+ tumor-infiltrating
lymphocytes in cancer: A critical review of the literature. Clin
Cancer Res. 18:3022–3029. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Mailloux AW and Young MR: Regulatory
T-cell trafficking: From thymic development to tumor-induced immune
suppression. Crit Rev Immunol. 30:435–447. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
De Visser KE, Eichten A and Coussens LM:
Paradoxical roles of the immune system during cancer development.
Nat Rev Cancer. 6:24–37. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Quail DF and Joyce JA: Microenvironmental
regulation of tumor progression and metastasis. Nat Med.
19:1423–1437. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Josefowicz SZ, Lu LF and Rudensky AY:
Regulatory T cells: Mechanisms of differentiation and function.
Annu Rev Immunol. 30:531–564. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Struchko GY, Меrkulova LМ and Moskvichev
YV: Morphological and immunohistochemical characteristics of the
thymus during chemical carcinogenesis induced by
1,2-dimethylhydrazine administration. Morfologiia. 146:35–39.
2014.(In Russian). PubMed/NCBI
|
|
76
|
Hamidinia M, Ghafourian Boroujerdnia M,
Talaiezadeh A, Solgi G, Roshani R, Iranprast S and Khodadadi A:
Increased P-35, EBI3 transcripts and other Treg markers in
peripheral blood mononuclear cells of breast cancer patients with
different clinical stages. Adv Pharm Bull. 5:261–267. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Lee JH, Chen Y, Chan JL, Qian YW and
Goydos JS: Molecular analysis of melanoma-induced sentinel lymph
node immune dysfunction. Cancer Immunol Immunother. 60:685–692.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Lagios MD: Clinical significance of
immunohistochemically detectable epithelial cells in sentinel lymph
node and bone marrow in breast cancer. J Surg Oncol. 83:1–4. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Vasco C, Canazza A, Rizzo A, Mossa A,
Corsini E, Silvani A, Fariselli L, Salmaggi A and Ciusani E:
Circulating T regulatory cells migration and phenotype in
glioblastoma patients: An in vitro study. J Neurooncol.
115:353–363. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Zhang X, Kelaria S, Kerstetter J and Wang
J: The functional and prognostic implications of regulatory T cells
in colorectal carcinoma. J Gastrointest Oncol. 6:307–313.
2015.PubMed/NCBI
|
|
81
|
Protti MP, De Monte L and Di Lullo G:
Tumor antigen-specific CD4+ T cells in cancer immunity:
From antigen identification to tumor prognosis and development of
therapeutic strategies. Tissue Antigens. 83:237–246. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Chen X and Oppenheim JJ: Resolving the
identity myth: Key markers of functional
CD4+FoxP3+ regulatory T cells. Int
Immunopharmacol. 11:1489–1496. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Ladoire S, Arnould L, Apetoh L, Coudert B,
Martin F, Chauffert B, Fumoleau P and Ghiringhelli F: Pathologic
complete response to neoadjuvant chemotherapy of breast carcinoma
is associated with the disappearance of tumor-infiltrating
Foxp3+ regulatory T cells. Clin Cancer Res.
14:2413–2420. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Teng MW, Ngiow SF, von Scheidt B,
McLaughlin N, Sparwasser T and Smyth MJ: Conditional regulatory
T-cell depletion releases adaptive immunity preventing
carcinogenesis and suppressing established tumor growth. Cancer
Res. 70:7800–7809. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Liu Y, Gu Y and Cao X: The exosomes in
tumor immunity. Oncoimmunology. 4:e10274722015. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Bersanelli M and Buti S: From targeting
the tumor to targeting the immune system: Transversal challenges in
oncology with the inhibition of the PD-1/PD-L1 axis. World J Clin
Oncol. 8:37–53. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Dolan DE and Gupta S: PD-1 pathway
inhibitors: Changing the landscape of cancer immunotherapy. Cancer
Control. 21:231–237. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Rei M, Pennington DJ and Silva-Santos B:
The emerging protumor role of γδ T lymphocytes: Implications for
cancer immunotherapy. Cancer Res. 75:798–802. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Pennock GK and Chow LQ: The evolving role
of immune checkpoint inhibitors in cancer treatment. Oncologist.
20:812–822. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Zhu J, Powis de Tenbossche CG, Cane S,
Colau D, van Baren N, Lurquin C, Schmitt-Verhulst AM, Liljestrom P,
Uyttenhove C and Van den Eynde BJ: Resistance to cancer
immunotherapy mediated by apoptosis of tumor-infiltrating
lymphocytes. Nat Commun. 8:14042017. View Article : Google Scholar : PubMed/NCBI
|